

Abstract
Non-traumatic osteonecrosis of the femoral head (ONFH) usually affects adults younger than 50 years and frequently leads to femoral head collapse and subsequent arthritis of the hip. It is becoming more prevalent along with increasing use of corticosteroids for the adjuvant therapy of leukemia and other myelogenous diseases as well as management of organ transplantation. This review updated knowledge on the pathogenesis, classification criteria, staging system, and treatment of ONFH.
Keywords: Hip, Femoral Head, Osteonecrosis, Avascular Necrosis
Graphical Abstract
INTRODUCTION
Around 1830, Jean Cruveilhier, a French anatomist and pathologist, described necrosis of the femoral head as a late complication of hip trauma. He presumed vascular injury was the etiology of the necrosis.1 In early and middle 20th century, various non-traumatic factors were identified to induce the disease or to involve in its development.2,3 This disease entity had been called as avascular necrosis, ischemic necrosis or aseptic necrosis of the femoral head. In 1992, the Committee on Nomenclature and Staging of the Association Research Circulation Osseous (ARCO) agreed to use ‘osteonecrosis’ as a uniform terminology for necrotic lesions of the femoral head.
Non-traumatic osteonecrosis of the femoral head (ONFH) usually affects adults younger than 50 years. In the United States, more than 10,000 new patients are affected with the disease every year, and it accounts for up to 10% of total hip arthroplasties (THAs).4 In South Korea, the annual incidence of ONFH increased from 9,870 in 2002 to 18,691 in 2006.5 The annual incidence rate in Japan was 1.91/100,000 and the annual incidence was estimated to be more than 2,400 in the survey from 2010 to 2013.6 In China, the cumulative number of ONFH patients reached 8.12 million in 2013.7
In this review, we provide up-to-date knowledge on the etiology, pathogenesis, classification criteria, staging system, and treatment of non-traumatic ONFH.
ETIOLOGY
In 1913, osteonecrotic lesions were found in divers and this disease entity was known as “Caisson disease” and later as dysbaric osteonecrosis.8 Osteonecrosis in patients with sickle cell disease was recognized in the 1960s.9 As Chandler called the disease “coronary arterial disease of the hip”,10 embolism seemed to play the central role in the development of ONFH in patients with hemoglobinopathies and those with dysbaric osteonecrosis.
In 1962, the first case of ONFH after the use of corticosteroid was reported.11 By the 1970s, it was known that excessive-alcohol consumers had increased incidence of ONFH.12
In the 1970s and 1980s, ONFHs after pelvic radiation therapy were reported.13,14
During last three decades, thrombophilia, hypofibrinolysis, and hypoangiogenesis were found to involve in the pathogenesis of ONFH,15,16 and familial ONFHs were reported.15,16
The pathogenesis of non-traumatic ONFH is perplexing, and it remains to be investigated and scrutinized. Nevertheless, there are three general agreements. First, local ischemia due to compromised blood flow is the final common pathway in the pathogenesis of ONFHs other than radiation induced osteonecrosis. Second, alcohol- or steroid-associated ONFH is not an embolic infarction. It is a kind of intraosseous compartment syndrome. Third, the disease has a multifactorial etiology including genetic predispositions and exposure to risk factors. In most ONFH patients, both of genetic and non-genetic risk factors reciprocally interact and play roles together in the pathogenesis.17,18,19 The genetic predisposition explains why only some of steroid users and alcohol abusers acquire the disease, while others do not.
Genetic factors are implicated in hypercoagulability/hypofibrinolysis and/or hypoangiogenesis. Protein C and protein S deficiencies,16,20,21,22,23 mutations in the factor V Leiden or the prothrombin 20210A gene,20 polymorphisms of the plasminogen activator inhibitor-1 gene,21,24,25 and presence of antiphospholipid antibodies26,27 and decreased activity of 5,10-methylenetetrahydrofolate reductase25 have been known to be associated with hypercoagulability. Polymorphism of the endothelial nitric oxide synthase gene and vascular endothelial growth factor have been known to impair angiogenesis and to be associated with ONFH.28,29,30,31
Corticosteroid use and alcohol overuse are well known risk factors for ONFH. Besides, smoking, systemic lupus erythematosus, dysbaric disorders, pelvic radiation therapy, non-steroidal chemotherapeutic agents for leukemia and other myelogenous diseases, sickle cell disease, Gaucher's disease, human immunodeficiency virus infection, and pancreatitis have been known as risk factors or associated conditions of ONFH.32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49
Even though corticosteroids and alcohol are leading causes of ONFH, there have been no unified criteria to classify corticosteroid-associated ONFH and alcohol-associated ONFH. In 2017, ARCO develop a classification scheme of corticosteroid-associated and alcohol-associated ONFH to standardize clinical studies on ONFH through Delphi surveys. The ARCO classification criteria of corticosteroid-associated ONFH included the following: 1) patients should have a history of corticosteroid use > 2 g of prednisolone or its equivalent within a 3-month period; 2) osteonecrosis should be diagnosed within 2 years after corticosteroid usage, and 3) patients should not have other risk factor(s) besides corticosteroids.50 The criteria of alcohol-associated ONFH included the following: 1) patients should have a history of alcohol intake > 400 mL/week (320 g/week, any type of alcoholic beverage) of pure ethanol for more than 6 months; 2) ONFH should be diagnosed within 1 year after alcohol intake of this dose; and 3) patients should not have other risk factor(s) than alcohol abuse.51
ARCO recommends using these criteria for studies about ONFH.
PATHOGENESIS
Embolism plays the central role in vascular occlusion and consequent ONFH in hemoglobinopathies and dysbaric disorders.37,38,46
However, alcohol- and corticosteroid-associated ONFHs are not embolic infarctions and have different mechanisms in the pathogenesis. In 2019, ARCO task force developed a plausible model to explain the pathogenetic of non-traumatic ONFH.52
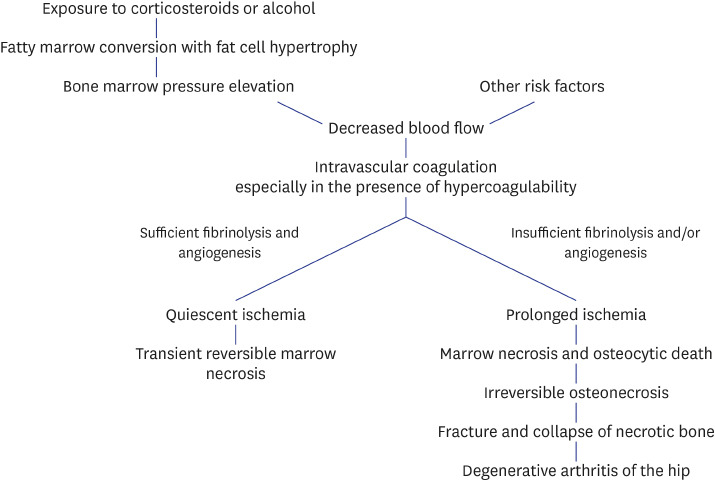
Corticosteroids and alcohol promote differentiation of mesenchymal stem cells to adipocytes. They also induce hypertrophy of the adipocyte through increasing intracellular lipid synthesis.53,54,55,56,57,58 The increments of number and volume of marrow fat cell induce intra-osseous hypertension in the proximal femur. Venous sinusoids are compressed due to the intra-osseous hypertension, and intravascular coagulation occurs. Then, arterial blood flow is blocked, and an ischemia occurs in the femoral head.6,59,60,61,62
Corticosteroid- and alcohol-associated ONFHs are kinds of intra-osseous compartment syndrome inside the femoral head due to an ischemic cascade: 1) hyperplasia of marrow fat cell; 2) intra-osseous hypertension; 3) vascular compression and intravascular coagulation; 4) impaired blood flow; 5) marrow necrosis and osteocytic death; and 6) fibrovascular reparative process around the necrotic zone and saponification of necrotic marrow.17,63,64
Once, this reparative zone is formed, the lesion is irreversible. Thus, the presence of encapsulating fibrovascular reparative tissue around the necrotic bone is the histologic criteria to make a definite diagnosis of ONFH.63,64,65
The necrotic bone becomes saponified and mechanically weak. Thus, stress fracture occurs in the necrotic bone, followed by collapse of the femoral head and subsequent arthritis of the hip.50,66,67
Ischemic lesions do not always progress to irreversible osteonecrosis. Whether the ischemic lesion progresses to osteonecrosis or not depends on the degree of restoration of vascular perfusion and the creeping substitution of dead bone by new bone.63,67,68,69 Genetic predispositions of hypercoagulability/hypo-fibrinolysis and/or hypo-angiogenesis play role in the restoration of vascular perfusion (Fig. 1).16,20,21,22,23
Fig. 1. Pathogenesis of non-traumatic osteonecrosis of the femoral head.

STAGING
The first ARCO staging system of ONFH was established in 1994. In 2019, ARCO revised the staging system. In the first version, marrow necrosis was defined as stage 0 (marrow necrosis without reparative process, no low-signal band on magnetic resonance imaging [MRI]). In the revised system, stage 0 (marrow necrosis without reparative process, no low-signal band on MRI) was deleted, stage III was divided into early (IIIA) and late stage (IIIB) according to the depth (2 mm) of head depression, and subclassification of location/size was not incorporated (Table 1).64
Table 1. The 2019 revised ARCO staging for osteonecrosis of the femoral head.
| ARCO stage | Image findings | ||
|---|---|---|---|
| I | X-ray: normal | ||
| MRI: low-signal band on T1-weighted MRI | |||
| II | X-ray: abnormal | ||
| MRI: abnormal | |||
| III | Subchondral fracture on X-ray or CT | ||
| IIIA (early) | Femoral head depression ≤ 2 mm | ||
| IIIB (late) | Femoral head depression > 2 mm | ||
| IV | X-ray: osteoarthritis | ||
ARCO = Association Research Circulation Osseous, MRI = magnetic resonance imaging, CT = computed tomography.
SIZE/LOCATION OF NECROTIC PORTION AND NATURAL COURSE
The size/location of necrosis predicts further collapse of the femoral head and is the major determinant in the treatment of ONFH. Various classification systems have been developed to characterize the size/location of necrosis. Currently, three classification systems: Steinberg classification, Japanese Investigation Committee (JIC) classification and modified Kerboul classification, are widely used.
The Steinberg system categorized the extent of involvement into 3 subsets: mild (< 15% of articular surface or head affected), moderate (15–30%), and severe (> 30%) (Fig. 2).70
Fig. 2. Steinberg classification system of femoral head osteonecrosis. Three subsets: mild (< 15% of articular surface or head affected), moderate (15–30%), and severe (> 30%).

The JIC classification is based on the mid-coronal T1-weighted magnetic resonance (MR) image of the femoral head. In the JIC classification, necrotic lesions were classified into four types: type A lesion < medial 1/3 of the weight-bearing portion; type B lesion < medial 2/3 of the weight-bearing portion; type C1 lesion > medial 2/3 of the weight-bearing portion but not extending laterally to the acetabular edge; and type C2 lesion extending laterally to the acetabular edge. The prevalence of collapse was < 10% in type A, 40% in type B, 80% in type C1, and > 90% in type C2 (Fig. 3).71,72
Fig. 3. Japanese Investigation Committee classification system of femoral head osteonecrosis. Four types: type A lesion < medial 1/3 of the weight-bearing portion; type B lesion < medial 2/3 of the weight-bearing portion; type C1 lesion > medial 2/3 of the weight-bearing portion but not extending laterally to the acetabular edge; and type C2 lesion extending laterally to the acetabular edge.

In 1974, Kerboul et al.73 developed a method to quantify the extent of necrosis by measuring the arc of the necrotic portion on anteroposterior and lateral radiographs and then calculating the sum of these two angles. In 2006, Ha et al.74 modified the method by measuring the necrotic arc on the midcoronal and midsagittal MR images (Fig. 4). The authors classified the necrotic lesions into 3 categories: small lesion (combined necrotic angle < 190°), medium-sized lesion (combined necrotic angle between 190° and 240°), and large lesion (combined necrotic angle > 240°). There was a strong correlation between the combined necrotic angle and the risk of femoral head collapse. None of small lesions collapsed, all large lesions collapsed, while 50% of medium-sized lesions collapsed within 3 years from the diagnosis of ONFH.74
Fig. 4. Modified Kerboul classification system of femoral head osteonecrosis. A: necrotic angle in mid-coronal MR image. B: necrotic angle in mid-sagittal MR image. Combined necrotic angle: A + B. Three categories: small lesion (combined necrotic angle ≤ 190°), medium-sized lesion (combined necrotic angle between 190° and 240°), and large lesion (combined necrotic angle ≥ 240°).

MR = magnetic resonance.
There is no agreement as to which method is most reliable and valid. Unified classification system of necrotic size/location should be developed.
TREATMENTS
The risk of collapse depends on the size/location of the necrotic portion. Small lesions seldom develop collapse even without any medical or surgical treatment, while most of large lesions are progressive.75,76,77 The extent of necrotic portion is determined at the ischemic attack. Once ONFH develops, the lesion does not increase in size regardless of the disease progression in the stage.78 Thus, the size of necrotic portion should be evaluated prior to treating ONFH, and any treatment should not be done in small lesions. The efficacy of certain treatment should be determined cautiously considering the different natural courses according to the size of necrosis.
Medical treatments
To date, various pharmacological agents including enoxaparin, statins, bisphosphonates, iloprost and acetylsalicylic acid have been tried to retard or reverse the disease progression.79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95
However, none of them have been proven to be effective by high level evidence, and most of them have adverse reactions.96
At this moment, no pharmacological prevention or treatment is recommendable.
Core decompression (CD) with bone marrow aspirate concentration (BMAC)
CD has been used in early-stage (pre-collapse) ONFH with the assumption that it prevents femoral head collapse and hopefully reverses the disease progression. However, the results of CD were not consistent, and the effectiveness of CD was questioned.97
Recently, injection of BMAC was combined to traditional CD to improve the results. While earlier studies have supported the effectiveness of additional cell therapy,98,99,100,101,102,103 later studies reported no differences in outcomes between CD with BMAC and CD alone. Both of CD and BMAC therapy had high rates of progression in large lesions.104,105,106 Whether BMAC is effective or not is a controversial issue, which needs further investigation.
Osteotomies
Various osteotomies of the proximal femur were introduced to preserve osteonecrotic hips. These procedures move the necrotic portion from the weight-bearing dome to a non-weight-bearing region. Among them, transtrochanteric curved varus osteotomy (TCVO)107 and transtrochanteric rotational osteotomy (TRO)108 have been done mainly in Japan and South Korea.
In 2017, Lee et al.109 compared the results of 91 TROs and 65 TCVOs. In their comparison, TCVO was better than TRO in terms of operation time, the amount of blood, postoperative collapse, osteoarthritic change (20% vs. 37.4%), and THA conversion rate (10.8% vs. 16.5%). Thus, they recommended TCVO rather than TRO.
In the selection of candidate for the osteotomy, patient's age (< 40 years), body mass index (< 24 kg/m2), stage of the disease (ARCO stage 3A or 3B),64 size of necrotic portion (medium-size lesion),74,75,76 should be counted.
Vascularized bone grafts
Vascularized fibular grafting was first described by Judet et al.110 in 1980 and subsequently popularized by Urbaniak et al.111 and Yoo et al.112 Vascularized iliac bone grafting including a pedicle of the iliac circumflex artery has been favored because the iliac bone is in vicinity of the femoral head and the process needs no microsurgical anastomosis.113 However, vascularized bone grafts have been criticized for the technical difficulties and donor site morbidities. Currently, these procedures are only performed at several centers throughout the world.
Resurfacing arthroplasty
Hemi-resurfacing and total resurfacing arthroplasties were once considered as bone sparing alternatives to THA in young ONFH patients.114,115 However, hemi-resurfacing has been abandoned and total resurfacing is rarely done due to complication related with the metal-on-metal bearing and risk of periprosthetic femoral neck fracture.116
THA using highly cross-linked polyethylene liners
Excessive wear rates and subsequent osteolysis associated with conventional polyethylene have prompted more durable bearings in young patients.117
Highly cross-linked polyethylene, which has enhanced wear-resistant properties, has rapidly replaced conventional polyethylene. Ionizing radiation during the manufacturing process increases the number of crosslinks and thereby reduces the polyethylene wear. Current cross-linking techniques use gamma-rays in place of electron beam irradiation and subsequent annealing or remelting of the polyethylene.118
Highly cross-linked polyethylene liners can be coupled with either cobalt chromium or ceramic femoral head. There are short-term follow-up studies to suggest that the clinical and radiological results of the highly cross-linked polyethylene liners are promising in patients with ONFH.119,120 However, the long-term results remain unknown. There is a concern over the risk of fracture in these liners with time. To prevent fracture, a minimum liner thickness > 6 mm has been advocated.121
THA using ceramic-on-ceramic (CoC) bearings
CoC bearings have the lowest wear rates among various bearing.117 However, there are complications specifically associated with the use of CoC bearings. Fractures of ceramic parts and squeak appeared as matters of concern after the use of these bearings.122,123
Several studies showed that CoC THA had promising outcomes at mid-term follow-up in patients with ONFH.124,125,126 Even though the newest Delta ceramic is expected to reduce the rate of ceramic fracture,127 the long-term outcomes of the CoC THA remain unknown.
SUMMARY
ONFH has a multifactorial etiology including genetic predispositions and exposure to risk factors. The size/location of necrosis is the predictor for collapse of the femoral head and should be the major determinant in the treatment of ONFH patients. The extent of necrosis is determined at the initial ischemic attack, and the size of the lesion does not change with time. Small lesions do not progress even without any intervention and need no treatment. Any treatment, medical or surgical, should be done in medium-sized to large lesions with pain. To date, no pharmacological prevention or treatment has been proven to be effective and is not recommendable. CD combined with BMAC therapy does not work in large lesions and needs further investigations to verify its effectiveness. Osteotomy should be done cautiously in selected patients. Resurfacing arthroplasties are not recommendable in ONFH patients. THA using highly cross-linked polyethylene liners or CoC bearings showed excellent outcomes at early to medium term follow-up studies. However, the long-term follow-up results are unrevealed, yet.
Footnotes
Disclosure: The authors have no potential conflicts of interest to disclose.
- Conceptualization: Koo KH, Lee YK.
- Writing - original draft: Hines J, Jo WL.
- Writing - review & editing: Cui Q, Mont M, Koo KH, Cheng E, Goodman S, Ha YC, Hernigou P, Jones LC, Kim SY, Sakai T, Sugano N, Yamamoto T, Lee MS, Zhao D, Drescher W, Kim TY, Lee YK, Yoon BH, Baek SH, Ando W, Kim HS, Park JW.
References
- 1.Dubois EL, Cozen L. Avascular (aseptic) bone necrosis associated with systemic lupus erythematosus. JAMA. 1960;174(8):966–971. doi: 10.1001/jama.1960.03030080028005. [DOI] [PubMed] [Google Scholar]
- 2.Freund E. Bilateral aseptic necrosis of the femoral head: problems arising in a compensation case. Ann Surg. 1936;104(1):100–106. doi: 10.1097/00000658-193607000-00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Phemister DB. Changes in bones and joints resulting from interruption of circulation. I. General consideration and changes resulting from injury. Arch Surg. 1940;41(2):436. [Google Scholar]
- 4.Mont MA, Cherian JJ, Sierra RJ, Jones LC, Lieberman JR. Nontraumatic osteonecrosis of the femoral head: Where do we stand today? A ten-year update. J Bone Joint Surg Am. 2015;97(19):1604–1627. doi: 10.2106/JBJS.O.00071. [DOI] [PubMed] [Google Scholar]
- 5.Kang JS, Park S, Song JH, Jung YY, Cho MR, Rhyu KH. Prevalence of osteonecrosis of the femoral head: a nationwide epidemiologic analysis in Korea. J Arthroplasty. 2009;24(8):1178–1183. doi: 10.1016/j.arth.2009.05.022. [DOI] [PubMed] [Google Scholar]
- 6.Ikeuchi K, Hasegawa Y, Seki T, Takegami Y, Amano T, Ishiguro N. Epidemiology of nontraumatic osteonecrosis of the femoral head in Japan. Mod Rheumatol. 2015;25(2):278–281. doi: 10.3109/14397595.2014.932038. [DOI] [PubMed] [Google Scholar]
- 7.Zhao DW, Yu M, Hu K, Wang W, Yang L, Wang BJ, et al. Prevalence of nontraumatic osteonecrosis of the femoral head and its associated risk factors in the Chinese population: results from a nationally representative survey. Chin Med J (Engl) 2015;128(21):2843–2850. doi: 10.4103/0366-6999.168017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bassoe P. The late manifestations of compressed air disease. Am J Med Sci. 1913;145(4):526–542. [Google Scholar]
- 9.Chung SM, Ralston EL. Necrosis of the femoral head associated with sickle-cell anemia and its genetic variants. A review of the literature and study of thirteen cases. J Bone Joint Surg Am. 1969;51(1):33–58. [PubMed] [Google Scholar]
- 10.Chandler FA. Coronary disease of the hip. J Int Coll Surg. 1948;11(1):34–36. [PubMed] [Google Scholar]
- 11.Pietrogrande V, Mastromarino R. Osteopatia da prolunga trattamento cortisonico. ORTOP Traumatol. 1957;25:791. [Google Scholar]
- 12.Hungerford DS, Zizic TM. Alcoholism associated ischemic necrosis of the femoral head. Early diagnosis and treatment. Clin Orthop Relat Res. 1978;(130):144–153. [PubMed] [Google Scholar]
- 13.Duparc J, Frot B, Gastambide D. Radiation-induced lesions of the hip. Chirurgie. 1974;100(12):837–853. [PubMed] [Google Scholar]
- 14.Gun'ko RI, Krasnov AS. Radiation injuries of the bones during treatment of uterine cancer. Vopr Onkol. 1988;34(10):1188–1195. [PubMed] [Google Scholar]
- 15.Arlet J, Franck JL, Nghiem L, Solera ML, de Graeve J. Multiple bone necroses and familial type I hyperlipemia. Apropos of a case report. Rev Rhum Mal Osteoartic. 1983;50(2):149–153. [PubMed] [Google Scholar]
- 16.Pierre-Jacques H, Glueck CJ, Mont MA, Hungerford DS. Familial heterozygous protein-S deficiency in a patient who had multifocal osteonecrosis. A case report. J Bone Joint Surg Am. 1997;79(7):1079–1084. doi: 10.2106/00004623-199707000-00017. [DOI] [PubMed] [Google Scholar]
- 17.Arlet JD, Fauchier C, Hungerford DS. Bone Circulation. Baltimore, MD, USA: Williams & Wilkins; 1984. Histopathology of nontraumatic necrosis of the femoral head: topographic and evolutive aspects. [Google Scholar]
- 18.Hauzeur JP, Perlmutter N, Appelboom T, Pasteels JL. Medullary impairment at early stage of non-traumatic osteonecrosis of the femoral head. Rheumatol Int. 1991;11(4-5):215–217. doi: 10.1007/BF00332565. [DOI] [PubMed] [Google Scholar]
- 19.Mont MA, Salem HS, Piuzzi NS, Goodman SB, Jones LC. Nontraumatic osteonecrosis of the femoral head: Where do we stand today?: A 5-year update. J Bone Joint Surg Am. 2020;102(12):1084–1099. doi: 10.2106/JBJS.19.01271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Björkman A, Svensson PJ, Hillarp A, Burtscher IM, Rünow A, Benoni G. Factor V leiden and prothrombin gene mutation: risk factors for osteonecrosis of the femoral head in adults. Clin Orthop Relat Res. 2004;(425):168–172. [PubMed] [Google Scholar]
- 21.Glueck CJ, Freiberg R, Tracy T, Stroop D, Wang P. Thrombophilia and hypofibrinolysis: pathophysiologies of osteonecrosis. Clin Orthop Relat Res. 1997;(334):43–56. [PubMed] [Google Scholar]
- 22.Jones LC, Mont MA, Le TB, Petri M, Hungerford DS, Wang P, et al. Procoagulants and osteonecrosis. J Rheumatol. 2003;30(4):783–791. [PubMed] [Google Scholar]
- 23.Zalavras CG, Vartholomatos G, Dokou E, Malizos KN. Genetic background of osteonecrosis: associated with thrombophilic mutations? Clin Orthop Relat Res. 2004;(422):251–255. [PubMed] [Google Scholar]
- 24.Glueck CJ, Fontaine RN, Gruppo R, Stroop D, Sieve-Smith L, Tracy T, et al. The plasminogen activator inhibitor-1 gene, hypofibrinolysis, and osteonecrosis. Clin Orthop Relat Res. 1999;(366):133–146. doi: 10.1097/00003086-199909000-00017. [DOI] [PubMed] [Google Scholar]
- 25.Glueck CJ, Freiberg RA, Fontaine RN, Tracy T, Wang P. Hypofibrinolysis, thrombophilia, osteonecrosis. Clin Orthop Relat Res. 2001;(386):19–33. doi: 10.1097/00003086-200105000-00004. [DOI] [PubMed] [Google Scholar]
- 26.Korompilias AV, Gilkeson GS, Ortel TL, Seaber AV, Urbaniak JR. Anticardiolipin antibodies and osteonecrosis of the femoral head. Clin Orthop Relat Res. 1997;(345):174–180. [PubMed] [Google Scholar]
- 27.Seleznick MJ, Silveira LH, Espinoza LR. Avascular necrosis associated with anticardiolipin antibodies. J Rheumatol. 1991;18(9):1416–1417. [PubMed] [Google Scholar]
- 28.Glueck CJ, Freiberg RA, Boppana S, Wang P. Thrombophilia, hypofibrinolysis, the eNOS T-786C polymorphism, and multifocal osteonecrosis. J Bone Joint Surg Am. 2008;90(10):2220–2229. doi: 10.2106/JBJS.G.00616. [DOI] [PubMed] [Google Scholar]
- 29.Koo KH, Lee JS, Lee YJ, Kim KJ, Yoo JJ, Kim HJ. Endothelial nitric oxide synthase gene polymorphisms in patients with nontraumatic femoral head osteonecrosis. J Orthop Res. 2006;24(8):1722–1728. doi: 10.1002/jor.20164. [DOI] [PubMed] [Google Scholar]
- 30.Kim T, Hong JM, Lee J, Oh B, Park EK, Lee C, et al. Promoter polymorphisms of the vascular endothelial growth factor gene is associated with an osteonecrosis of the femoral head in the Korean population. Osteoarthritis Cartilage. 2008;16(3):287–291. doi: 10.1016/j.joca.2007.06.017. [DOI] [PubMed] [Google Scholar]
- 31.Lee YJ, Lee JS, Kang EH, Lee YK, Kim SY, Song YW, et al. Vascular endothelial growth factor polymorphisms in patients with steroid-induced femoral head osteonecrosis. J Orthop Res. 2012;30(1):21–27. doi: 10.1002/jor.21492. [DOI] [PubMed] [Google Scholar]
- 32.Rueda JC, Duque MA, Mantilla RD, Iglesias-Gamarra A. Osteonecrosis and antiphospholipid syndrome. J Clin Rheumatol. 2009;15(3):130–132. doi: 10.1097/RHU.0b013e31819dbd20. [DOI] [PubMed] [Google Scholar]
- 33.Tektonidou MG, Moutsopoulos HM. Immunologic factors in the pathogenesis of osteonecrosis. Orthop Clin North Am. 2004;35(3):259–263. vii. doi: 10.1016/j.ocl.2004.02.003. [DOI] [PubMed] [Google Scholar]
- 34.Abu-Shakra M, Buskila D, Shoenfeld Y. Osteonecrosis in patients with SLE. Clin Rev Allergy Immunol. 2003;25(1):13–24. doi: 10.1385/CRIAI:25:1:13. [DOI] [PubMed] [Google Scholar]
- 35.Hedri H, Cherif M, Zouaghi K, Abderrahim E, Goucha R, Ben Hamida F, et al. Avascular osteonecrosis after renal transplantation. Transplant Proc. 2007;39(4):1036–1038. doi: 10.1016/j.transproceed.2007.02.031. [DOI] [PubMed] [Google Scholar]
- 36.Horiuchi H, Hashikura Y, Hisa K, Saito N, Ikegami T, Nakazawa Y, et al. Osteonecrosis of the femoral head in Japanese adults after liver transplantation: a preliminary report. J Orthop Sci. 2004;9(2):119–121. doi: 10.1007/s00776-003-0757-0. [DOI] [PubMed] [Google Scholar]
- 37.Hutter CD. Dysbaric osteonecrosis: a reassessment and hypothesis. Med Hypotheses. 2000;54(4):585–590. doi: 10.1054/mehy.1999.0901. [DOI] [PubMed] [Google Scholar]
- 38.Jones JP. Epidemiological risk factors for non-traumatic osteonecrosis. Orthopade. 2000;29(5):370–379. doi: 10.1007/s001320050458. [DOI] [PubMed] [Google Scholar]
- 39.Katz K, Horev G, Grunebaum M, Yosipovitch Z. The natural history of osteonecrosis of the femoral head in children and adolescents who have Gaucher disease. J Bone Joint Surg Am. 1996;78(1):14–19. doi: 10.2106/00004623-199601000-00003. [DOI] [PubMed] [Google Scholar]
- 40.Li H, Zhang J, He JW, Wang K, Wang GS, Jiang N, et al. Symptomatic osteonecrosis of the femoral head after adult orthotopic liver transplantation. Chin Med J (Engl) 2012;125(14):2422–2426. [PubMed] [Google Scholar]
- 41.Lieberman JR, Roth KM, Elsissy P, Dorey FJ, Kobashigawa JA. Symptomatic osteonecrosis of the hip and knee after cardiac transplantation. J Arthroplasty. 2008;23(1):90–96. doi: 10.1016/j.arth.2007.01.006. [DOI] [PubMed] [Google Scholar]
- 42.Rodrigue SW, Rosenthal DI, Barton NW, Zurakowski D, Mankin HJ. Risk factors for osteonecrosis in patients with type 1 Gaucher's disease. Clin Orthop Relat Res. 1999;(362):201–207. [PubMed] [Google Scholar]
- 43.Sayarlioglu M, Yuzbasioglu N, Inanc M, Kamali S, Cefle A, Karaman O, et al. Risk factors for avascular bone necrosis in patients with systemic lupus erythematosus. Rheumatol Int. 2012;32(1):177–182. doi: 10.1007/s00296-010-1597-9. [DOI] [PubMed] [Google Scholar]
- 44.Shibatani M, Fujioka M, Arai Y, Takahashi K, Ueshima K, Okamoto M, et al. Degree of corticosteroid treatment within the first 2 months of renal transplantation has a strong influence on the incidence of osteonecrosis of the femoral head. Acta Orthop. 2008;79(5):631–636. doi: 10.1080/17453670810016641. [DOI] [PubMed] [Google Scholar]
- 45.Tauchmanovà L, De Rosa G, Serio B, Fazioli F, Mainolfi C, Lombardi G, et al. Avascular necrosis in long-term survivors after allogeneic or autologous stem cell transplantation: a single center experience and a review. Cancer. 2003;97(10):2453–2461. doi: 10.1002/cncr.11373. [DOI] [PubMed] [Google Scholar]
- 46.Toklu AS, Cimşit M. Dysbaric osteonecrosis in Turkish sponge divers. Undersea Hyperb Med. 2001;28(2):83–88. [PubMed] [Google Scholar]
- 47.Torii Y, Hasegawa Y, Kubo T, Kodera Y, Minami S, Morishita Y, et al. Osteonecrosis of the femoral head after allogeneic bone marrow transplantation. Clin Orthop Relat Res. 2001;(382):124–132. doi: 10.1097/00003086-200101000-00019. [DOI] [PubMed] [Google Scholar]
- 48.Winquist EW, Bauman GS, Balogh J. Nontraumatic osteonecrosis after chemotherapy for testicular cancer: a systematic review. Am J Clin Oncol. 2001;24(6):603–606. doi: 10.1097/00000421-200112000-00015. [DOI] [PubMed] [Google Scholar]
- 49.Dzik-Jurasz AS, Brooker S, Husband JE, Tait D. What is the prevalence of symptomatic or asymptomatic femoral head osteonecrosis in patients previously treated with chemoradiation? A magnetic resonance study of anal cancer patients. Clin Oncol (R Coll Radiol) 2001;13(2):130–134. doi: 10.1053/clon.2001.9236. [DOI] [PubMed] [Google Scholar]
- 50.Yoon BH, Jones LC, Chen CH, Cheng EY, Cui Q, Drescher W, et al. Etiologic classification criteria of ARCO on femoral head osteonecrosis part 1: glucocorticoid-associated osteonecrosis. J Arthroplasty. 2019;34(1):163–168.e1. doi: 10.1016/j.arth.2018.09.005. [DOI] [PubMed] [Google Scholar]
- 51.Yoon BH, Jones LC, Chen CH, Cheng EY, Cui Q, Drescher W, et al. Etiologic classification criteria of ARCO on femoral head osteonecrosis part 2: alcohol-associated osteonecrosis. J Arthroplasty. 2019;34(1):169–174.e1. doi: 10.1016/j.arth.2018.09.006. [DOI] [PubMed] [Google Scholar]
- 52.Cui Q, Jo WL, Koo KH, Cheng EY, Drescher W, Goodman SB, et al. ARCO consensus on the pathogenesis of non-traumatic osteonecrosis of the femoral head. J Korean Med Sci. 2021;36(10):e65. doi: 10.3346/jkms.2021.36.e65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Cui Q, Wang GJ, Balian G. Steroid-induced adipogenesis in a pluripotential cell line from bone marrow. J Bone Joint Surg Am. 1997;79(7):1054–1063. doi: 10.2106/00004623-199707000-00012. [DOI] [PubMed] [Google Scholar]
- 54.Cui Q, Wang Y, Saleh KJ, Wang GJ, Balian G. Alcohol-induced adipogenesis in a cloned bone-marrow stem cell. J Bone Joint Surg Am. 2006;88(Suppl 3):148–154. doi: 10.2106/JBJS.F.00534. [DOI] [PubMed] [Google Scholar]
- 55.Miyanishi K, Yamamoto T, Irisa T, Yamashita A, Jingushi S, Noguchi Y, et al. Bone marrow fat cell enlargement and a rise in intraosseous pressure in steroid-treated rabbits with osteonecrosis. Bone. 2002;30(1):185–190. doi: 10.1016/s8756-3282(01)00663-9. [DOI] [PubMed] [Google Scholar]
- 56.Motomura G, Yamamoto T, Miyanishi K, Yamashita A, Sueishi K, Iwamoto Y. Bone marrow fat-cell enlargement in early steroid-induced osteonecrosis--a histomorphometric study of autopsy cases. Pathol Res Pract. 2005;200(11-12):807–811. doi: 10.1016/j.prp.2004.10.003. [DOI] [PubMed] [Google Scholar]
- 57.Peckett AJ, Wright DC, Riddell MC. The effects of glucocorticoids on adipose tissue lipid metabolism. Metabolism. 2011;60(11):1500–1510. doi: 10.1016/j.metabol.2011.06.012. [DOI] [PubMed] [Google Scholar]
- 58.Wang GJ, Sweet DE, Reger SI, Thompson RC. Fat-cell changes as a mechanism of avascular necrosis of the femoral head in cortisone-treated rabbits. J Bone Joint Surg Am. 1977;59(6):729–735. [PubMed] [Google Scholar]
- 59.Hungerford DS, Lennox DW. The importance of increased intraosseous pressure in the development of osteonecrosis of the femoral head: implications for treatment. Orthop Clin North Am. 1985;16(4):635–654. [PubMed] [Google Scholar]
- 60.Koo KH, Dussault R, Kaplan P, Kim R, Ahn IO, Christopher J, et al. Age-related marrow conversion in the proximal metaphysis of the femur: evaluation with T1-weighted MR imaging. Radiology. 1998;206(3):745–748. doi: 10.1148/radiology.206.3.9494495. [DOI] [PubMed] [Google Scholar]
- 61.Kricun ME. Red-yellow marrow conversion: its effect on the location of some solitary bone lesions. Skeletal Radiol. 1985;14(1):10–19. doi: 10.1007/BF00361188. [DOI] [PubMed] [Google Scholar]
- 62.Lausten GS, Arnoldi CC. Blood perfusion uneven in femoral head osteonecrosis. Doppler flowmetry and intraosseous pressure in 12 cases. Acta Orthop Scand. 1993;64(5):533–536. doi: 10.3109/17453679308993686. [DOI] [PubMed] [Google Scholar]
- 63.Koo KH, Jeong ST, Jones JP., Jr Borderline necrosis of the femoral head. Clin Orthop Relat Res. 1999;(358):158–165. [PubMed] [Google Scholar]
- 64.Yoon BH, Mont MA, Koo KH, Chen CH, Cheng EY, Cui Q, et al. The 2019 revised version of association research circulation osseous staging system of osteonecrosis of the femoral head. J Arthroplasty. 2020;35(4):933–940. doi: 10.1016/j.arth.2019.11.029. [DOI] [PubMed] [Google Scholar]
- 65.Goetz JE, Robinson DA, Pedersen DR, Conzemius MG, Brown TD. Cryoinsult parameter effects on the histologically apparent volume of experimentally induced osteonecrotic lesions. J Orthop Res. 2011;29(6):931–937. doi: 10.1002/jor.21342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Arlet J. Nontraumatic avascular necrosis of the femoral head. Past, present, and future. Clin Orthop Relat Res. 1992;(277):12–21. [PubMed] [Google Scholar]
- 67.Seamon J, Keller T, Saleh J, Cui Q. The pathogenesis of nontraumatic osteonecrosis. Arthritis. 2012;2012:601763. doi: 10.1155/2012/601763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Jones JP., Jr Concepts of etiology and early pathogenesis of osteonecrosis. Instr Course Lect. 1994;43:499–512. [PubMed] [Google Scholar]
- 69.Jones JP, Jr, Peltier LF. Alcoholism, hypercortisonism, fat embolism and osseous avascular necrosis. 1971. Clin Orthop Relat Res. 2001;(393):4–12. doi: 10.1097/00003086-200112000-00002. [DOI] [PubMed] [Google Scholar]
- 70.Steinberg ME, Brighton CT, Steinberg DR, Tooze SE, Hayken GD. Treatment of avascular necrosis of the femoral head by a combination of bone grafting, decompression, and electrical stimulation. Clin Orthop Relat Res. 1984;(186):137–153. [PubMed] [Google Scholar]
- 71.Nishii T, Sugano N, Ohzono K, Sakai T, Sato Y, Yoshikawa H. Significance of lesion size and location in the prediction of collapse of osteonecrosis of the femoral head: a new three-dimensional quantification using magnetic resonance imaging. J Orthop Res. 2002;20(1):130–136. doi: 10.1016/S0736-0266(01)00063-8. [DOI] [PubMed] [Google Scholar]
- 72.Nakasone S, Takao M, Sakai T, Nishii T, Sugano N. Does the extent of osteonecrosis affect the survival of hip resurfacing? Clin Orthop Relat Res. 2013;471(6):1926–1934. doi: 10.1007/s11999-013-2833-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Kerboul M, Thomine J, Postel M, Merle d'Aubigné R. The conservative surgical treatment of idiopathic aseptic necrosis of the femoral head. J Bone Joint Surg Br. 1974;56-B(2):291–296. [PubMed] [Google Scholar]
- 74.Ha YC, Kim HJ, Kim SY, Kim KC, Lee YK, Koo KH. Effects of age and body mass index on the results of transtrochanteric rotational osteotomy for femoral head osteonecrosis. J Bone Joint Surg Am. 2010;92(2):314–321. doi: 10.2106/JBJS.H.01020. [DOI] [PubMed] [Google Scholar]
- 75.Sugano N, Atsumi T, Ohzono K, Kubo T, Hotokebuchi T, Takaoka K. The 2001 revised criteria for diagnosis, classification, and staging of idiopathic osteonecrosis of the femoral head. J Orthop Sci. 2002;7(5):601–605. doi: 10.1007/s007760200108. [DOI] [PubMed] [Google Scholar]
- 76.Ha YC, Jung WH, Kim JR, Seong NH, Kim SY, Koo KH. Prediction of collapse in femoral head osteonecrosis: a modified Kerboul method with use of magnetic resonance images. J Bone Joint Surg Am. 2006;88(Suppl 3):35–40. doi: 10.2106/JBJS.F.00535. [DOI] [PubMed] [Google Scholar]
- 77.Steinberg ME, Hayken GD, Steinberg DR. A quantitative system for staging avascular necrosis. J Bone Joint Surg Br. 1995;77-B(1):34–41. [PubMed] [Google Scholar]
- 78.Koo KH, Ahn IO, Kim R, Song HR, Jeong ST, Na JB, et al. Bone marrow edema and associated pain in early stage osteonecrosis of the femoral head: prospective study with serial MR images. Radiology. 1999;213(3):715–722. doi: 10.1148/radiology.213.3.r99dc06715. [DOI] [PubMed] [Google Scholar]
- 79.Ajmal M, Matas AJ, Kuskowski M, Cheng EY. Does statin usage reduce the risk of corticosteroid-related osteonecrosis in renal transplant population? Orthop Clin North Am. 2009;40(2):235–239. doi: 10.1016/j.ocl.2009.01.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Chotanaphuti T, Thongprasert S, Laoruengthana A. Low molecular weight heparin prevents the progression of precollapse osteonecrosis of the hip. J Med Assoc Thai. 2013;96(10):1326–1330. [PubMed] [Google Scholar]
- 81.Glueck CJ, Freiberg RA, Sieve L, Wang P. Enoxaparin prevents progression of stages I and II osteonecrosis of the hip. Clin Orthop Relat Res. 2005;(435):164–170. doi: 10.1097/01.blo.0000157539.67567.03. [DOI] [PubMed] [Google Scholar]
- 82.Glueck CJ, Freiberg RA, Wissman R, Wang P. Long term anticoagulation (4-16 years) stops progression of idiopathic hip osteonecrosis associated with familial thrombophilia. Adv Orthop. 2015;2015:138382. doi: 10.1155/2015/138382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Pengde K, Fuxing P, Bin S, Jing Y, Jingqiu C. Lovastatin inhibits adipogenesis and prevents osteonecrosis in steroid-treated rabbits. Joint Bone Spine. 2008;75(6):696–701. doi: 10.1016/j.jbspin.2007.12.008. [DOI] [PubMed] [Google Scholar]
- 84.Pritchett JW. Statin therapy decreases the risk of osteonecrosis in patients receiving steroids. Clin Orthop Relat Res. 2001;(386):173–178. doi: 10.1097/00003086-200105000-00022. [DOI] [PubMed] [Google Scholar]
- 85.Agarwala S, Shetty V, Karumuri LK, Vijayvargiya M. Patellar resurfacing versus nonresurfacing with patellaplasty in total knee arthroplasty. Indian J Orthop. 2018;52(4):393–398. doi: 10.4103/ortho.IJOrtho_512_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Chen CH, Chang JK, Lai KA, Hou SM, Chang CH, Wang GJ. Alendronate in the prevention of collapse of the femoral head in nontraumatic osteonecrosis: a two-year multicenter, prospective, randomized, double-blind, placebo-controlled study. Arthritis Rheum. 2012;64(5):1572–1578. doi: 10.1002/art.33498. [DOI] [PubMed] [Google Scholar]
- 87.Lai KA, Shen WJ, Yang CY, Shao CJ, Hsu JT, Lin RM. The use of alendronate to prevent early collapse of the femoral head in patients with nontraumatic osteonecrosis. A randomized clinical study. J Bone Joint Surg Am. 2005;87(10):2155–2159. doi: 10.2106/JBJS.D.02959. [DOI] [PubMed] [Google Scholar]
- 88.Lee YK, Ha YC, Cho YJ, Suh KT, Kim SY, Won YY, et al. Does zoledronate prevent femoral head collapse from osteonecrosis? A prospective, randomized, open-label, multicenter study. J Bone Joint Surg Am. 2015;97(14):1142–1148. doi: 10.2106/JBJS.N.01157. [DOI] [PubMed] [Google Scholar]
- 89.Nishii T, Sugano N, Miki H, Hashimoto J, Yoshikawa H. Does alendronate prevent collapse in osteonecrosis of the femoral head? Clin Orthop Relat Res. 2006;443(443):273–279. doi: 10.1097/01.blo.0000194078.32776.31. [DOI] [PubMed] [Google Scholar]
- 90.Albers A, Carli A, Routy B, Harvey EJ, Séguin C. Treatment with acetylsalicylic acid prevents short to mid-term radiographic progression of nontraumatic osteonecrosis of the femoral head: a pilot study. Can J Surg. 2015;58(3):198–205. doi: 10.1503/cjs.016814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Claßen T, Becker A, Landgraeber S, Haversath M, Li X, Zilkens C, et al. Long-term clinical results after iloprost treatment for bone marrow edema and avascular necrosis. Orthop Rev (Pavia) 2016;8(1):6150. doi: 10.4081/or.2016.6150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Jäger M, Zilkens C, Bittersohl B, Matheney T, Kozina G, Blondin D, et al. Efficiency of iloprost treatment for osseous malperfusion. Int Orthop. 2011;35(5):761–765. doi: 10.1007/s00264-010-0998-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Pazianas M, Abrahamsen B. Safety of bisphosphonates. Bone. 2011;49(1):103–110. doi: 10.1016/j.bone.2011.01.003. [DOI] [PubMed] [Google Scholar]
- 94.Pountos I, Giannoudis PV. The role of iloprost on bone edema and osteonecrosis: safety and clinical results. Expert Opin Drug Saf. 2018;17(3):225–233. doi: 10.1080/14740338.2018.1424828. [DOI] [PubMed] [Google Scholar]
- 95.U.S. Food and Drug Administration. FDA drug safety communication: important safety label changes to cholesterol-lowering statin drugs. [Updated 2016]. [Accessed January 7, 2019]. https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-important-safety-label-changes-cholesterol-lowering-statin-drugs.
- 96.Lee YJ, Cui Q, Koo KH. Is there a role of pharmacological treatments in the prevention or treatment of osteonecrosis of the femoral head?: A systematic review. J Bone Metab. 2019;26(1):13–18. doi: 10.11005/jbm.2019.26.1.13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Yoon BH, Lee YK, Kim KC, Ha YC, Koo KH. No differences in the efficacy among various core decompression modalities and non-operative treatment: a network meta-analysis. Int Orthop. 2018;42(12):2737–2743. doi: 10.1007/s00264-018-3977-9. [DOI] [PubMed] [Google Scholar]
- 98.Hernigou P, Dubory A, Homma Y, Guissou I, Flouzat Lachaniette CH, Chevallier N, et al. Cell therapy versus simultaneous contralateral decompression in symptomatic corticosteroid osteonecrosis: a thirty year follow-up prospective randomized study of one hundred and twenty five adult patients. Int Orthop. 2018;42(7):1639–1649. doi: 10.1007/s00264-018-3941-8. [DOI] [PubMed] [Google Scholar]
- 99.Kang JS, Suh YJ, Moon KH, Park JS, Roh TH, Park MH, et al. Clinical efficiency of bone marrow mesenchymal stem cell implantation for osteonecrosis of the femoral head: a matched pair control study with simple core decompression. Stem Cell Res Ther. 2018;9(1):274. doi: 10.1186/s13287-018-1030-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Li X, Xu X, Wu W. Comparison of bone marrow mesenchymal stem cells and core decompression in treatment of osteonecrosis of the femoral head: a meta-analysis. Int J Clin Exp Pathol. 2014;7(8):5024–5030. [PMC free article] [PubMed] [Google Scholar]
- 101.Ma Y, Wang T, Liao J, Gu H, Lin X, Jiang Q, et al. Efficacy of autologous bone marrow buffy coat grafting combined with core decompression in patients with avascular necrosis of femoral head: a prospective, double-blinded, randomized, controlled study. Stem Cell Res Ther. 2014;5(5):115. doi: 10.1186/scrt505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Sen RK, Tripathy SK, Aggarwal S, Marwaha N, Sharma RR, Khandelwal N. Early results of core decompression and autologous bone marrow mononuclear cells instillation in femoral head osteonecrosis: a randomized control study. J Arthroplasty. 2012;27(5):679–686. doi: 10.1016/j.arth.2011.08.008. [DOI] [PubMed] [Google Scholar]
- 103.Zhao D, Cui D, Wang B, Tian F, Guo L, Yang L, et al. Treatment of early stage osteonecrosis of the femoral head with autologous implantation of bone marrow-derived and cultured mesenchymal stem cells. Bone. 2012;50(1):325–330. doi: 10.1016/j.bone.2011.11.002. [DOI] [PubMed] [Google Scholar]
- 104.Lim YW, Kim YS, Lee JW, Kwon SY. Stem cell implantation for osteonecrosis of the femoral head. Exp Mol Med. 2013;45(11):e61. doi: 10.1038/emm.2013.128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Nally FJ, Zanotti G, Buttaro MA, Diaz Dilernia F, Mansilla IG, Comba FM, et al. THA conversion rate comparing decompression alone, with autologous bone graft or stem cells in osteonecrosis. Hip Int. 2018;28(2):189–193. doi: 10.5301/hipint.5000552. [DOI] [PubMed] [Google Scholar]
- 106.Pepke W, Kasten P, Beckmann NA, Janicki P, Egermann M. Core decompression and autologous bone marrow concentrate for treatment of femoral head osteonecrosis: a randomized prospective study. Orthop Rev (Pavia) 2016;8(1):6162. doi: 10.4081/or.2016.6162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Nishio A, Sugioka Y. A new technique of the varus osteotomy at the upper end of the femur. Orthop Traumatol. 1971;20(3):381–386. [Google Scholar]
- 108.Sugioka Y. Transtrochanteric anterior rotational osteotomy of the femoral head in the treatment of osteonecrosis affecting the hip: a new osteotomy operation. Clin Orthop Relat Res. 1978;(130):191–201. [PubMed] [Google Scholar]
- 109.Lee YK, Park CH, Ha YC, Kim DY, Lyu SH, Koo KH. Comparison of surgical parameters and results between curved varus osteotomy and rotational osteotomy for osteonecrosis of the femoral head. Clin Orthop Surg. 2017;9(2):160–168. doi: 10.4055/cios.2017.9.2.160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Judet J, Judet H, Gilbert A. Trial revascularization of the femur head with a pediculed fibular transplant. Rev Chir Orthop Reparatrice Appar Mot. 1980;66(Suppl 2):65. [PubMed] [Google Scholar]
- 111.Urbaniak JR, Coogan PG, Gunneson EB, Nunley JA. Treatment of osteonecrosis of the femoral head with free vascularized fibular grafting. A long-term follow-up study of one hundred and three hips. J Bone Joint Surg Am. 1995;77(5):681–694. doi: 10.2106/00004623-199505000-00004. [DOI] [PubMed] [Google Scholar]
- 112.Yoo MC, Chung DW, Hahn CS. Free vascularized fibula grafting for the treatment of osteonecrosis of the femoral head. Clin Orthop Relat Res. 1992;(277):128–138. [PubMed] [Google Scholar]
- 113.Zhao D, Xu D, Wang W, Cui X. Iliac graft vascularization for femoral head osteonecrosis. Clin Orthop Relat Res. 2006;442:171–179. doi: 10.1097/01.blo.0000181490.31424.96. [DOI] [PubMed] [Google Scholar]
- 114.Amstutz HC, Le Duff MJ. Current status of hemi-resurfacing arthroplasty for osteonecrosis of the hip: a 27-year experience. Orthop Clin North Am. 2009;40(2):275–282. doi: 10.1016/j.ocl.2008.12.001. [DOI] [PubMed] [Google Scholar]
- 115.De Smet KA, Van Der Straeten C, Van Orsouw M, Doubi R, Backers K, Grammatopoulos G. Revisions of metal-on-metal hip resurfacing: lessons learned and improved outcome. Orthop Clin North Am. 2011;42(2):259–269. ix. doi: 10.1016/j.ocl.2011.01.003. [DOI] [PubMed] [Google Scholar]
- 116.Zustin J, Sauter G, Morlock MM, Rüther W, Amling M. Association of osteonecrosis and failure of hip resurfacing arthroplasty. Clin Orthop Relat Res. 2010;468(3):756–761. doi: 10.1007/s11999-009-0979-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Kamath AF, Prieto H, Lewallen DG. Alternative bearings in total hip arthroplasty in the young patient. Orthop Clin North Am. 2013;44(4):451–462. doi: 10.1016/j.ocl.2013.06.001. [DOI] [PubMed] [Google Scholar]
- 118.Muratoglu OK, Bragdon CR, O'Connor DO, Jasty M, Harris WH. A novel method of cross-linking ultra-high-molecular-weight polyethylene to improve wear, reduce oxidation, and retain mechanical properties. Recipient of the 1999 HAP Paul Award. J Arthroplasty. 2001;16(2):149–160. doi: 10.1054/arth.2001.20540. [DOI] [PubMed] [Google Scholar]
- 119.Min BW, Lee KJ, Song KS, Bae KC, Cho CH. Highly cross-linked polyethylene in total hip arthroplasty for osteonecrosis of the femoral head: a minimum 5-year follow-up study. J Arthroplasty. 2013;28(3):526–530. doi: 10.1016/j.arth.2012.07.010. [DOI] [PubMed] [Google Scholar]
- 120.Kim YH, Choi Y, Kim JS. Cementless total hip arthroplasty with alumina-on-highly cross-linked polyethylene bearing in young patients with femoral head osteonecrosis. J Arthroplasty. 2011;26(2):218–223. doi: 10.1016/j.arth.2010.03.010. [DOI] [PubMed] [Google Scholar]
- 121.Kim YH, Park JW, Patel C, Kim DY. Polyethylene wear and osteolysis after cementless total hip arthroplasty with alumina-on-highly cross-linked polyethylene bearings in patients younger than thirty years of age. J Bone Joint Surg Am. 2013;95(12):1088–1093. doi: 10.2106/JBJS.L.01211. [DOI] [PubMed] [Google Scholar]
- 122.Koo KH, Ha YC, Jung WH, Kim SR, Yoo JJ, Kim HJ. Isolated fracture of the ceramic head after third-generation alumina-on-alumina total hip arthroplasty. J Bone Joint Surg Am. 2008;90(2):329–336. doi: 10.2106/JBJS.F.01489. [DOI] [PubMed] [Google Scholar]
- 123.Lee YK, Ha YC, Yoo JI, Jo WL, Kim KC, Koo KH. Mid-term results of the BIOLOX delta ceramic-on-ceramic total hip arthroplasty. Bone Joint J. 2017;99-B(6):741–748. doi: 10.1302/0301-620X.99B6.BJJ-2016-0486.R3. [DOI] [PubMed] [Google Scholar]
- 124.Park YS, Park SJ, Lim SJ. Ten-year results after cementless THA with a sandwich-type alumina ceramic bearing. Orthopedics. 2010;33(11):796. doi: 10.3928/01477447-20100924-11. [DOI] [PubMed] [Google Scholar]
- 125.Baek SH, Kim SY. Cementless total hip arthroplasty with alumina bearings in patients younger than fifty with femoral head osteonecrosis. J Bone Joint Surg Am. 2008;90(6):1314–1320. doi: 10.2106/JBJS.G.00755. [DOI] [PubMed] [Google Scholar]
- 126.Kang BJ, Ha YC, Ham DW, Hwang SC, Lee YK, Koo KH. Third-generation alumina-on-alumina total hip arthroplasty: 14 to 16-year follow-up study. J Arthroplasty. 2015;30(3):411–415. doi: 10.1016/j.arth.2014.09.020. [DOI] [PubMed] [Google Scholar]
- 127.Konan S, Alazzawi S, Yoon BH, Cha YH, Koo KH. A focused update on preventing ceramic fractures in hip arthroplasty: is the ‘cup’ half full? Bone Joint J. 2019;101-B(8):897–901. doi: 10.1302/0301-620X.101B8.BJJ-2019-0309.R1. [DOI] [PubMed] [Google Scholar]