

Abstract
The present study was undertaken in order to investigate the use of calcaneal ultrasonic backscatter for the application of diagnosis of osteoporosis. Broadband ultrasonic attenuation (BUA), speed of sound (SOS), average backscatter coefficient (ABC), and hip bone mineral density (BMD) were measured in calcanea in forty-seven women (average age: 58 years, standard deviation: 13 years). All three ultrasound variables had comparable correlations with hip BMD (around 0.5). As reported previously by others, BUA and SOS were rather highly correlated with each other. The logarithm of ABC was only moderately correlated with the other two. The three ultrasound parameters exhibited similar moderate negative correlations with age. These results taken collectively suggest that ABC may carry important diagnostic information independent of that contained in BUA and SOS and therefore may be useful as an adjunct measurement in the diagnosis of osteoporosis.
Keywords: ultrasound, backscatter, osteoporosis, cancellous bone
Introduction
Ultrasound-based methods for bone assessment are less expensive, faster, simpler, and more portable than their x-ray counterparts: dual-energy x-ray absorptiometry (DEXA) and quantitative computed tomography (QCT). In addition, they produce no ionizing radiation. The diagnostic capability of ultrasound to predict fracture risk has been documented in many studies. Calcaneal broadband ultrasonic attenuation1–4 (BUA) and speed of sound2,3,5–11 (SOS) correlate highly with calcaneal bone mineral density (BMD) which is in turn an indicator of osteoporotic fracture risk in the hip.12 Linear combinations of BUA and SOS are thought to have greater diagnostic capability than either parameter by itself and have been demonstrated to be predictive of hip and other fractures in women in prospective13,14 and retrospective15–18 studies.
In general, ultrasonic backscatter is known to provide information regarding size, shape, number density, and elastic properties of scatterers.19–23 In trabecular bone applications, trabeculae are likely candidates for scattering sites due to the high contrast in acoustic properties between mineralized trabeculae and marrow.24–27 The diminished number and thicknesses of trabeculae within bone that are associated with increased fracture risk would be expected to reduce backscatter. Several preliminary studies have established diagnostic promise and/or clinical feasibility of this measurement.28–34 A recent study has suggested that backscatter increases significantly upon decollagenization (with 7% sodium hypochlorite) and decreases or remains the same upon demineralization (with ethylenediaminetetraacetic acid, disodium salt dihydrate or EDTA).35
The present study was undertaken to further investigate the use of ultrasonic backscatter as a diagnostic measurement. This study is an extension to a larger population of subjects of an earlier preliminary investigation of 10 subjects. The initial study was performed using a clinical imaging system designed for abdominal applications. A center frequency of 2.25 MHz was used. In the present work a lower frequency (1 MHz, more suitable for highly attenuating bone) system, but without imaging capability, was employed and applied to a much larger set of subjects.
Methods
Forty-seven normal adult women (3 African American, 1 African European, 1 Asian, 1 Hispanic, and 41 non-Hispanic Caucasian; average age 58 years with a standard deviation of 13 years) were studied at the National Naval Medical Center (NNMC) in Bethesda, MD. These nonpregnant women were free of known disorders of skeletal metabolism, with no known history of nontraumatic bone fractures, and free of disorders whose treatment or medication promotes loss of bone such as diabetes, emphysema, and asthma. In addition, women with a history of bilateral hip replacement, Paget’s disease of the bone, renal failure, hyperthyroidism, or treated hypothyroidism were excluded. All participants provided informed consent (approved by both FDA and NNMC).
Ultrasound measurements were performed on each subjects’ left calcaneus. While sitting upright in a chair, the subject rested her left foot on her right knee as shown in Figure 1. A standoff pad (Cone Instruments, Solon, OH) was placed on the foot in order that data could be acquired in the focal zone of the transducer. The standoff pad also created a situation in which multiple reverberations between the transducer and the calcaneal surface were not received until well after the backscatter from the calcaneus and therefore could be excluded from the analysis.
Figure 1.

Data Acquisition. The subject rested her left heel upon her right knee. A standoff pad was so that the region of interest coincided with the focal zone of the transducer. Coupling gel was used at the transducer/standoff-pad and standoff-pad/skin interfaces.
Backscatter measurements were performed using a Panametrics (Waltham, MA) 5800 pulser/receiver and Panametrics V302 1” diameter, focussed (focal length = 2”), broadband transducer with center frequency of 1 MHz. Received signals were digitized (8 bit, 10 MHz) using a LeCroy (Chestnut Ridge, NY) 9310C Dual 400 MHz oscilloscope and stored on computer (via GPIB) for offline analysis.
Backscatter coefficients were measured using a reference phantom method.36 Good agreement between experimental measurements using this method and theoretical predictions based on Faran’s theory of scattering19 for ultrasonic backscatter coefficients from phantoms consisting of glass spheres embedded in gelatin has previously been reported by this laboratory.37 Over a band of frequencies corresponding to the system usable bandwidth (700 kHz to 1.5 MHz), backscatter coefficient vs. frequency data were least-squares fit to a power law relationship. The average backscatter coefficient (ABC) was computed from the midband (1 MHz) value of the fit. In order to compute backscatter coefficients it was necessary to compensate backscattered spectra for the effects of attenuation. For this compensation, the attenuation coefficient was taken to be linear with frequency and computed as the ratio of BUA (dB/MHz) and assumed constant value for calcaneal thickness for all subjects (3 cm).
A Lunar Achilles Plus bone sonometer was used for measurements of broadband ultrasonic attenuation (BUA) and speed of sound (SOS). The Achilles estimate of SOS was based on transit time of the leading edge rather than the center of the pulse propagating through the calcaneus and therefore provided an estimate closely related to signal velocity rather than group velocity.38,39 This device also provided measurements of a parameter commonly (but not rigorously) referred to “stiffness” which is an linear combination of BUA and SOS and is thought to be a more robust indicator of bone status than either parameter by itself.
Based on a wealth of empirical data showing that BMD is positively correlated with both BUA and SOS, the first two coefficients in this equation were obtained by doing regression analysis to obtain those coefficients which make the contributions of the first two terms roughly equal in magnitude (on the average) over the range of clinical values. The constant term was designed to make the average value of “stiffness” for young normal adult women to be equal to 100. (This terminology should not be confused with the more standard and formal use of the term stiffness, which corresponds to the coefficient of proportionality between displacement and restorative force,40 as in a spring, and may be expressed in units of N/m). The Achilles has been reported to yield estimates of BUA which are somewhat higher than those provided with comparable clinical calcaneal ultrasound devices.41 In order to calibrate the Achilles, separate measurements of BUA were performed on two commercial phantoms using the Achilles and a laboratory apparatus previously described.42 The phantoms were manufactured by CIRS Inc. (Norfolk, VA). One was designed to mimic normal bone (normalized BUA = 20.4 dB/cmMHz, SOS = 1562 m/s). The other was designed to mimic osteoporotic bone (normalized BUA = 14.2 dB/cmMHz, SOS = 1503 m/s). The normalized BUA values specified by the manufacturer were obtained over the frequency range from 250 kHz to 550 kHz. Six repeated measurements were acquired for each phantom for each measurement system. In the case of the laboratory system, each measurement was based on 8 RF lines. The average offset of the Achilles obtained from this comparison was subtracted from each of the clinical measurements of BUA.
A Hologic QDR-2000 DEXA scanner was used to measure BMD of the total hip, femoral neck, trochanter, and Ward’s triangle. Only total hip BMD measurements are reported here.
Results
The average values and standard deviations for the measurements performed on the 47 subjects are given in Table I. The correlations between pairs of measurements are given in Table II. As reported by others, BUA and SOS were rather highly correlated with each other. The Alogarithm of the average backscatter coefficient was only moderately correlated with the other two. All three ultrasound variables had comparable correlations with hip BMD (around 0.5). The three ultrasound parameters exhibited similar moderate negative correlations with age. These results taken together suggest that ABC may carry important diagnostic information independent of that contained in BUA and SOS. Scatter plots of the three ultrasound parameters against Hip BMD and age are given in Figures 2 through 7.
Table I.
Means and standard deviations of measurements. Acronyms are BUA (broadband ultrasonic attenuation), SOS (speed of sound), ABC (average backscatter coefficient), and BMD (bone mineral density).
| Parameter | Mean ± Standard Deviation |
|---|---|
| BUA (dB/MHz): | 87.7 ± 13.6 |
| SOS (m/s): | 1539.1 ± 34.2 |
| “Stiffness”: | 89 ± 18 |
| Log(ABC): | −0.3 ± 0.24 |
| BMD (g/cm2): | 0.873 ± 0.120 |
| Age (years): | 58 ± 12.8 |
| Height (inches): | 64.8 ± 2.8 |
| Weight (lb.s): | 148.6 ± 27.3 |
Table II.
Correlation matrix for measurements and age. Acronyms are BUA (broadband ultrasonic attenuation), SOS (speed of sound), ABC (average backscatter coefficient), and BMD (bone mineral density).
| Parameter | BUA | SOS | “Stiffness” | ABC | BMD | AGE | HGT | WGT |
|---|---|---|---|---|---|---|---|---|
| BUA | 1.00 | 0.81 | 0.95 | 0.43 | 0.56 | −0.44 | 0.17 | 0.19 |
| SOS | 0.81 | 1.00 | 0.96 | 0.46 | 0.51 | −0.46 | −0.06 | −0.04 |
| “Stiffness” | 0.95 | 0.96 | 1.00 | 0.47 | 0.56 | −0.47 | 0.05 | 0.08 |
| ABC | 0.43 | 0.46 | 0.47 | 1.00 | 0.50 | −0.42 | 0.17 | 0.08 |
| BMD | 0.56 | 0.51 | 0.56 | 0.50 | 1.00 | −0.31 | 0.06 | 0.30 |
| Age | −0.44 | −0.46 | −0.47 | −0.42 | −0.31 | 1.00 | −0.29 | 0.03 |
| Height | 0.17 | −0.06 | 0.05 | 0.17 | 0.06 | −0.29 | 1.00 | 0.35 |
| Weight | 0.19 | −0.04 | 0.08 | 0.08 | 0.30 | 0.03 | 0.35 | 1.00 |
Figure 2.
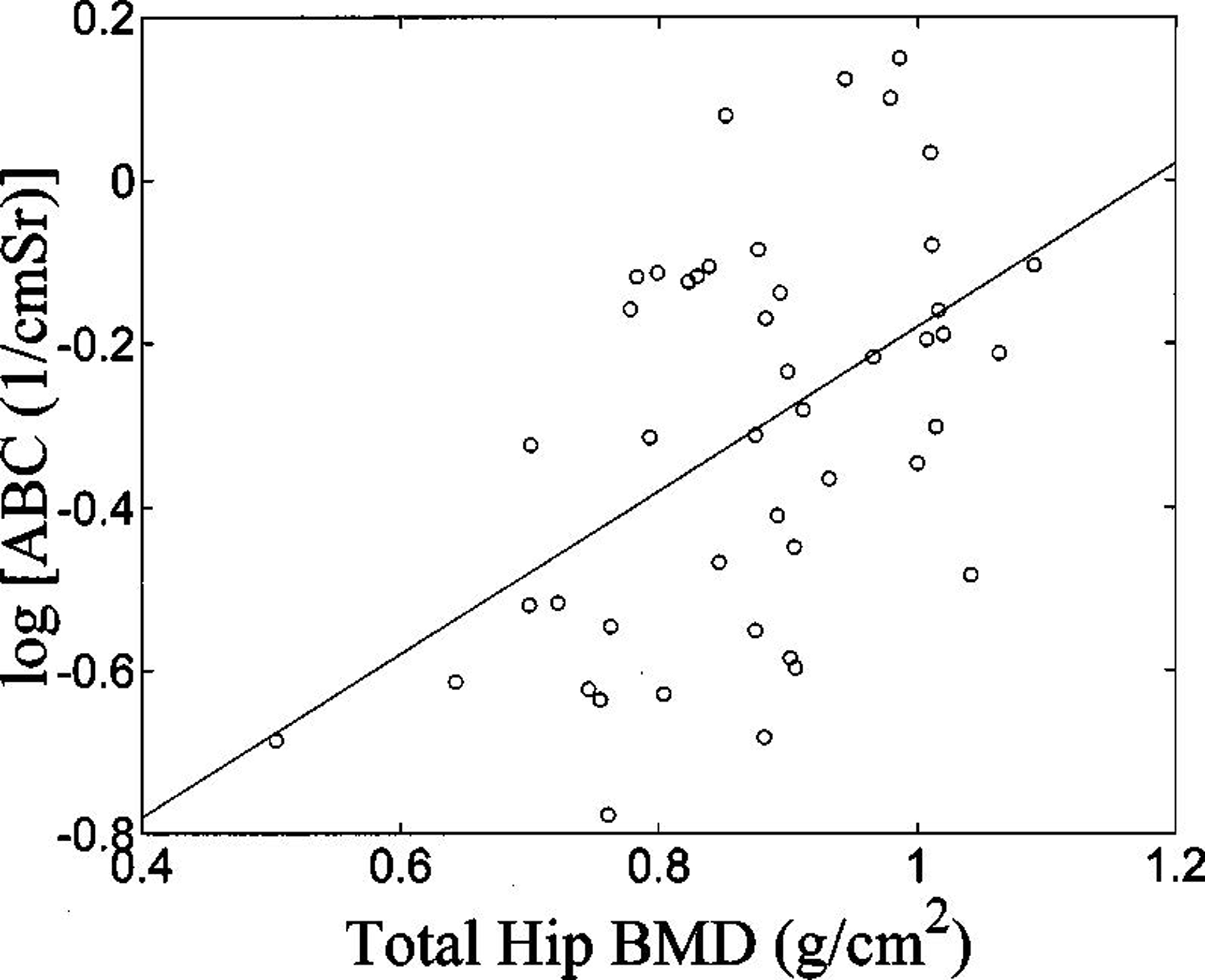
Logarithm of average backscatter coefficient (ABC) vs. total hip bone mineral density (BMD).
Figure 7.
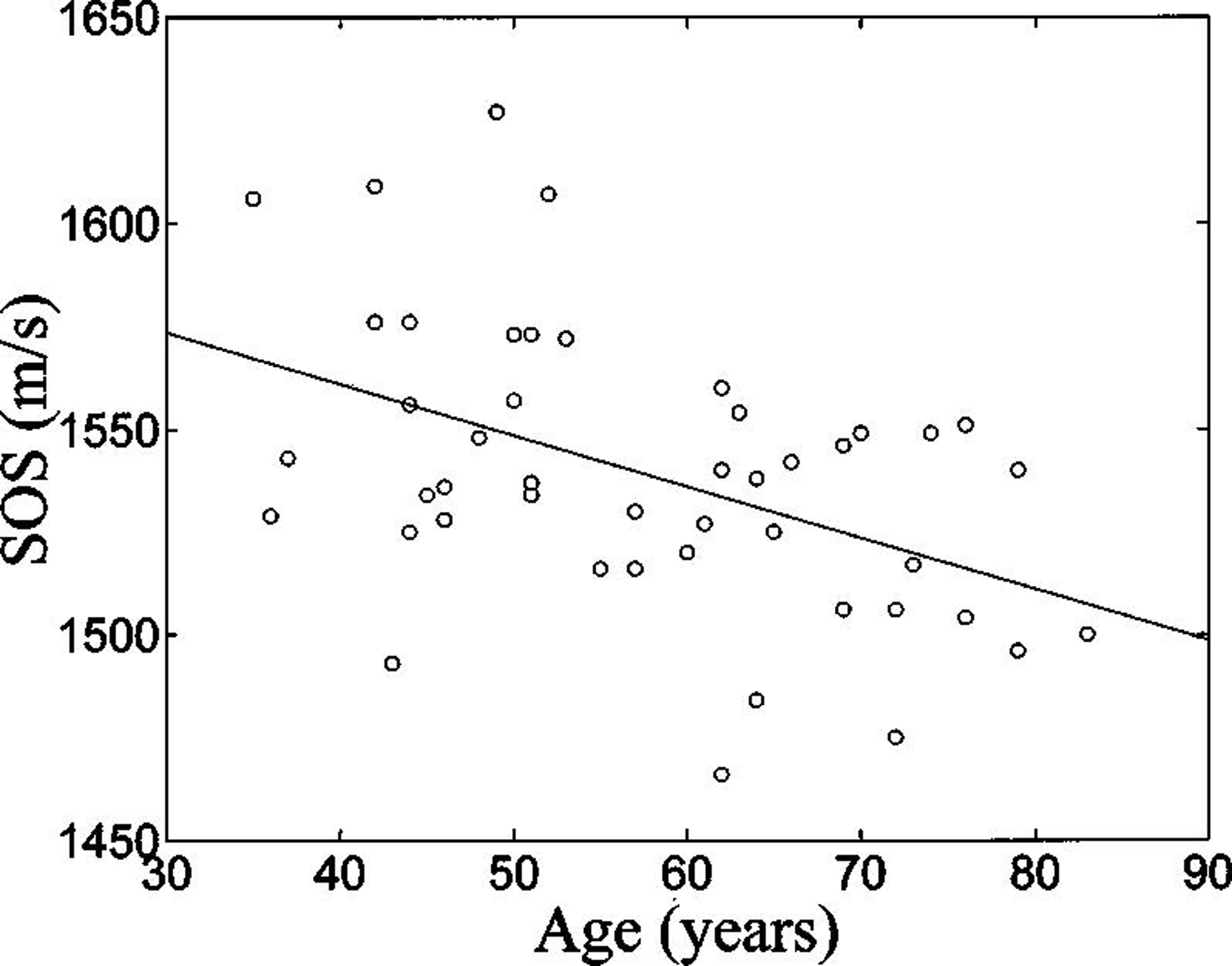
Speed of Sound (SOS) vs. age.
The sharpest decline in BMD occurs shortly following menopause. The age related drop in BUA between subjects ranging in age from 45–54 and those ranging from 55–64 was 93.3 dB/MHz (average of 12 subjects) to 84.6 dB/MHz (average of 11 subjects). These values are quite similar to those reported by Cheng et al.,43 namely 88.5 dB/MHz (average of 20 subjects) to 78.0 dB/MHz (average of 20 subjects) in the same age brackets. Similarly a drop in SOS from 1561 m/s to 1523 m/s was observed in the present study (Cheng et al did not measure SOS).
A linear regression between BUA and age was applied to the subset of subjects over 55, yielding a postmenopausal average annual rate of decline of 0.49 dB/MHz. This is similar to the value of 0.35 dB/MHz per year reported by Frost and co-workers.44 The corresponding values for SOS are 0.30 m/s per year (present study) and 0.56 m/s per year (Frost et al.).
Discussion
This study indicates that calcaneal ultrasonic backscatter exhibits correlations with hip BMD and age that are comparable to those exhibited by BUA and SOS. The correlation between backscatter and the other two ultrasonic variables is only about 0.5, suggesting that backscatter may reveal substantial information not contained in the other two and therefore may have some potential value as a substitute or an adjunct for BUA and SOS for assessment of bone status. This study represents the first clinical evaluation of a contact-based (as opposed to water-bath based30) method for measurement of calcaneal backscatter near 1 MHz. The correlation between backscatter and hip BMD in these the contact-based and water-bath-based studies are essentially identical (0.50).30
The correlation between backscatter and BMD observed here at 1 MHz (r = 0.50; 95% CI: 0.24 – 0.69) is smaller than previously reported at 2.25 MHz (r = 0.87).29 In addition to the difference in center frequencies, there are numerous differences between these two studies that may account for this. Most importantly, the earlier study correlated calcaneal backscatter with calcaneal BMD (volumetric BMD, in g/cm3, measured with QCT) while the current investigation correlated calcaneal backscatter with hip BMD (areal BMD, in g/cm2, measured with DEXA). It is not surprising that choosing two different sites rather than using the same site resulted in a decrease in the correlation. In addition, the orientation of the transducer relative to the calcaneus was different in the two studies. In the earlier study, the transducer was placed on the inferior surface of the foot, below the calcaneus, while in the present study, data were acquired in the mediolateral orientation. In addition, unlike the earlier study, the current study incorporated compensation for calcaneal attenuation. Finally, applying the method of Hoel,45 the 95% CI for the correlation coefficient in the earlier study may be computed to be 0.54 – 0.97, indicating some overlap in the 95% CI’s for the two studies.
Preliminary in vitro studies28,29,32 have demonstrated that ultrasonic backscatter increases with BMD in human calcaneus. Variations in BMD accounted for 66% – 68% (correlation coefficient near 0.8) of variations in the backscatter coefficient, suggesting that backscatter measurements give some indication of BMD, but also may convey some structural information not already contained in BMD measurements. Another study in bovine tibia trabecular bone34 reported “apparent” (not compensated for attenuation) integrated (averaged over a range of frequencies) backscatter to actually decrease with density in the mediolateral and superoinferior orientations and to show no change with density in the anteroposterior orientation. It is plausible that compensation for attenuation (which demonstrated a significant increase with BMD in the AP and ML directions) in this study34 could have yielded backscatter results more similar to the two above mentioned in vitro studies on human calcaneus. Differences between human calcaneus and bovine tibia trabecular bone46 as well as different frequency ranges of analysis (700 kHz to 1.5 MHz in the present study, 200 kHz – 600 kHz,28 and 1 – 3 MHz34) may also partially account for some disparity in results.
Fracture risk, not BMD, is the fundamental clinical end-point in the diagnosis of osteoporosis. Ideally, the utility of any diagnostic measurement for the prediction of fracture risk should be compared in populations with and without fractures, either prospectively or retrospectively. However, such a study can be somewhat more difficult as individuals either with fractures or with high propensity for fracture can be harder to find and recruit than normals. The current study demonstrates feasibility and some clinical promise for the contact method.
Figure 3.
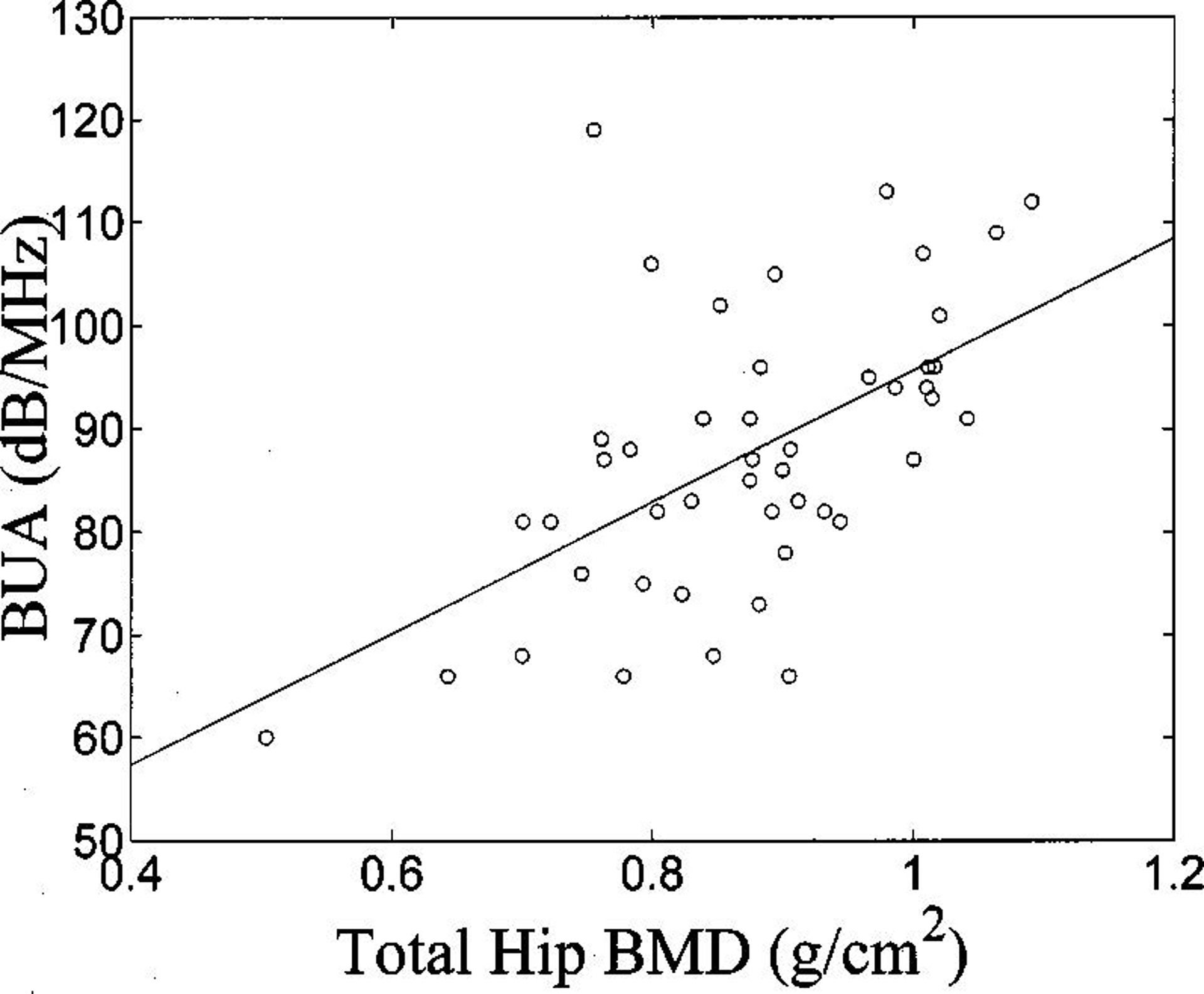
Broadband ultrasonic attenuation (BUA) vs. total hip bone mineral density (BMD).
Figure 4.
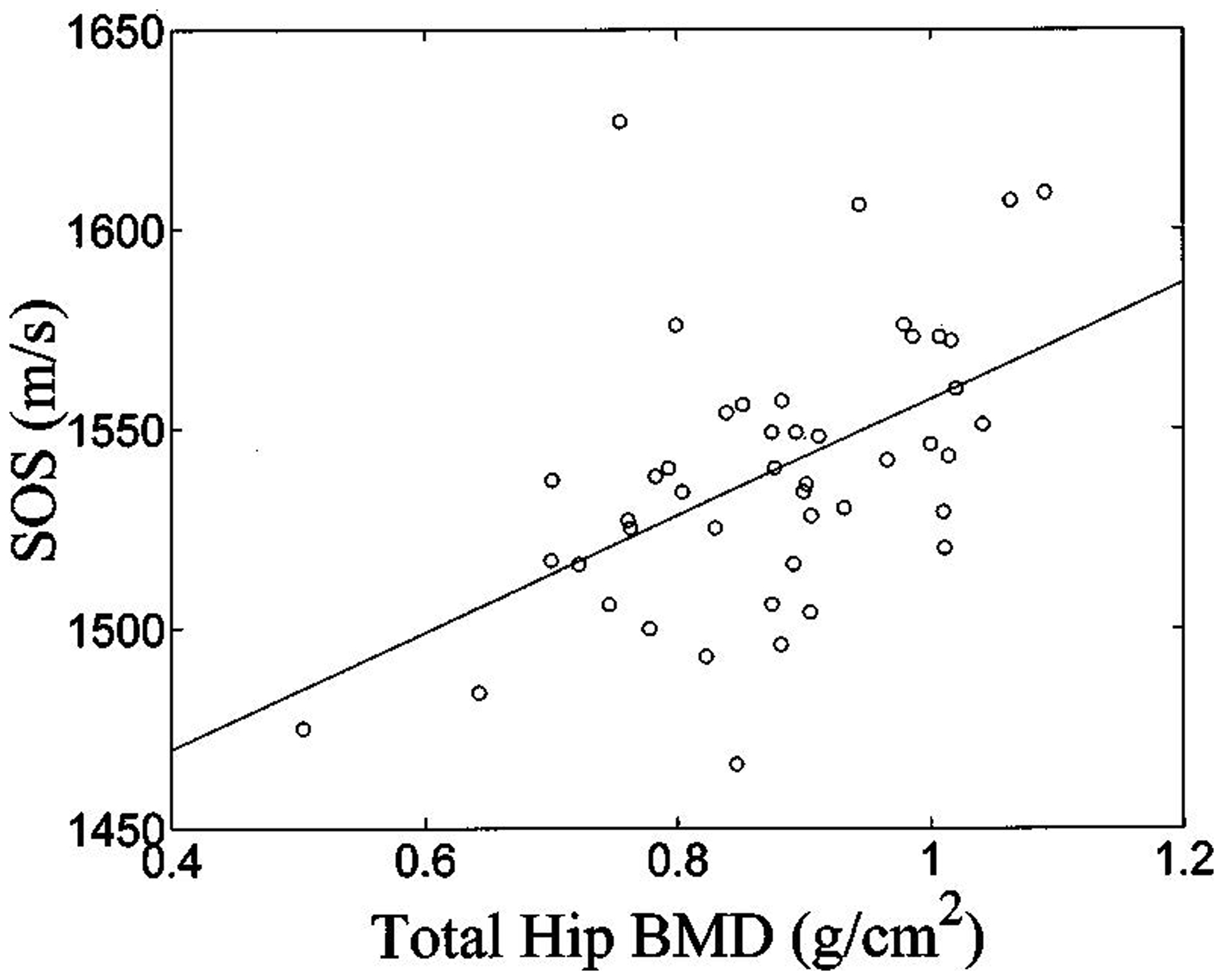
Speed of Sound (SOS) vs. total hip bone mineral density (BMD).
Figure 5.
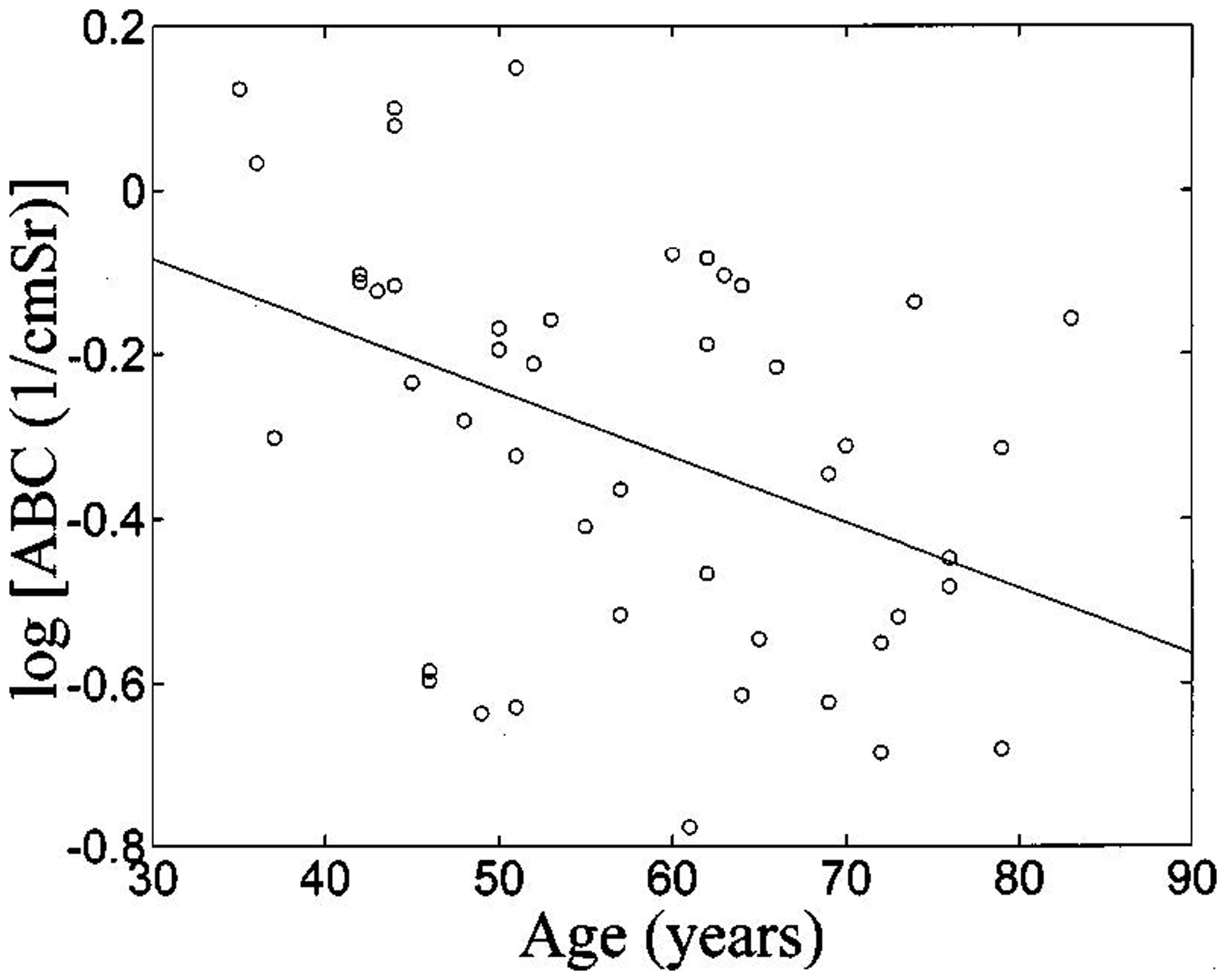
Logarithm of average backscatter coefficient (ABC) vs. age.
Figure 6.
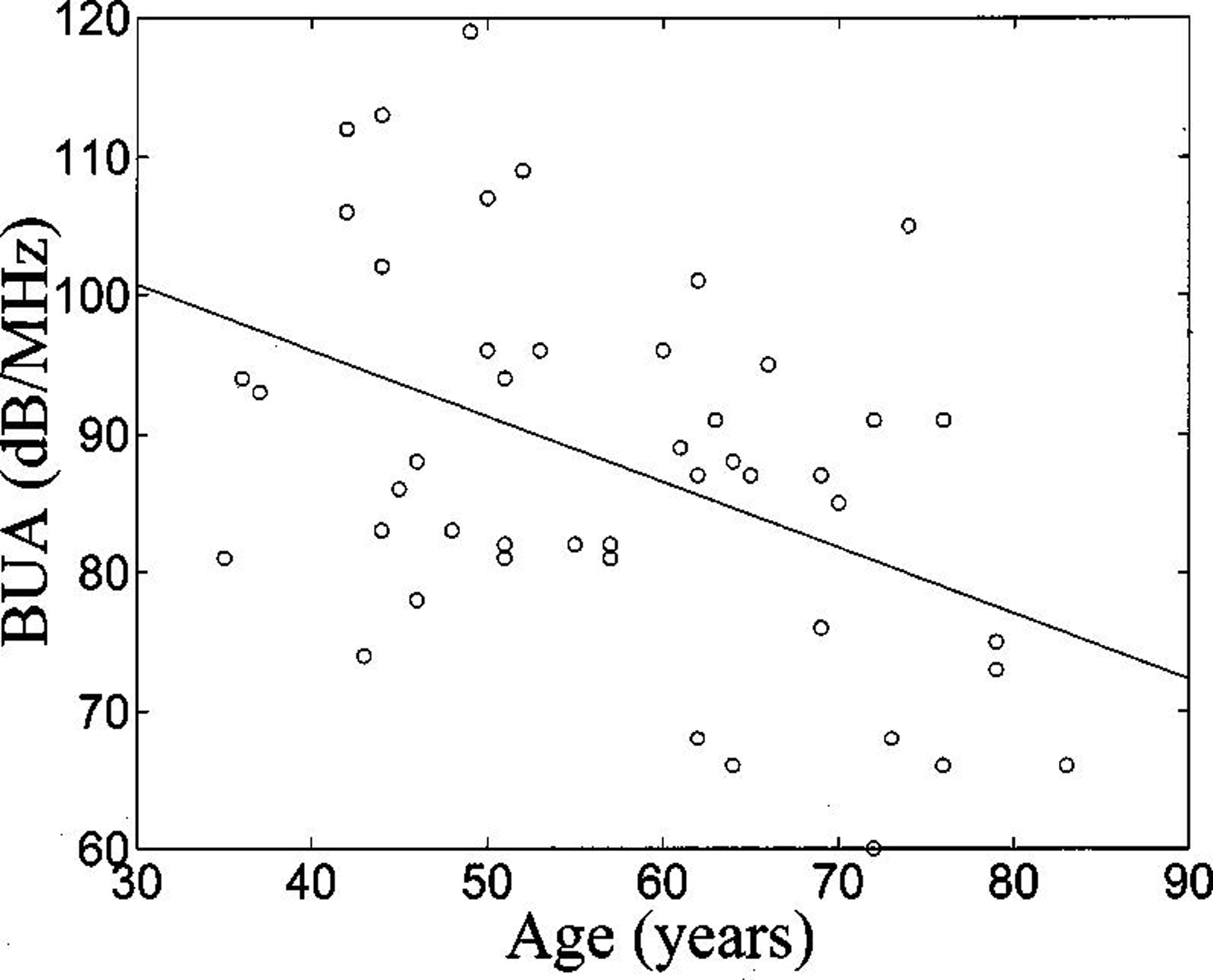
Broadband ultrasonic attenuation (BUA) vs. age.
Acknowledgements
The guidance of Dr. Mona S. Calvo, US Food and Drug Administration, is greatly appreciated. The authors are grateful for funding provided by the US Food and Drug Administration Office of Women’s Health. Gratitude is also expressed for Dr. A. J. Drake, III, MC, U.S.N. Endocrinology Clinic, National Naval Medical Center for serving as a sponsor for this research and authorizing the use of the Hologic DEXA scanner located in the Endocrinology Clinic at the National Naval Medical Center, Bethesda, MD.
The mention of commercial products, their sources, or their use in connection with material reported herein is not to be construed as either an actual or implied endorsement of such products by the Food and Drug Administration.
The views expressed in this article are those of the authors and do not reflect the official policy or position of the Department of the Navy, Department of Defense, nor the U. S. Government. The Chief, Navy Bureau of Medicine and Surgery, Washington, D.C., Clinical Investigation Program was a sponsor of this study, B99-044. This research was supported by the Office of Naval Research and the National Naval Medical Center.
Acronyms:
- ABC
Average Backscatter Coefficient
- BMD
Bone Mineral Density
- BUA
Broadband Ultrasonic Attenuation
- SOS
Speed of Sound
References
- 1.Langton CM, Palmer SB, and Porter RW. “The measurement of broadband ultrasonic attenuation in cancellous bone.” Eng. in Med 13, 89–91, (1984). [DOI] [PubMed] [Google Scholar]
- 2.Rossman P, Zagzebski J, Mesina C, Sorenson J, and Mazess R, “Comparison of Speed of Sound and Ultrasound Attenuation in the Os Calcis to Bone Density of the Radius, Femur and Lumbar Spine,” Clin. Phys. Physiol.Meas, 10, 353–360, (1989). [DOI] [PubMed] [Google Scholar]
- 3.Tavakoli MB and Evans JA. “Dependence of the velocity and attenuation of ultrasound in bone on the mineral content,” Phys. Med. Biol, 36, 1529–1537, (1991). [DOI] [PubMed] [Google Scholar]
- 4.Langton CM, Njeh CF, Hodgskinson R, and Currey JD. “Prediction of Mechanical Properties of the Human Calcaneus by Broadband Ultrasonic Attenuation,” Bone, 18, 495–503, (1996). [DOI] [PubMed] [Google Scholar]
- 5.Zagzebski JA, Rossman PJ, Mesina C, Mazess RB, and Madsen EL. “Ultrasound transmission measurements through the os calcis,” Calcif Tissue Int. 49, 107–111, (1991). [DOI] [PubMed] [Google Scholar]
- 6.Njeh CF, Hodgskinson R, Currey JD, and Langton CM. “Orthogonal relationships between ultrasonic velocity and material properties of bovine cancellous bone,” Med. Eng. Phys, 18, 373–381, (1996). [DOI] [PubMed] [Google Scholar]
- 7.Laugier P, Droin P, Laval-Jeantet AM, and Berger G. “In vitro assessment of the relationship between acoustic properties and bone mass density of the calcaneus by comparison of ultrasound parametric imaging and quantitative computed tomography.” Bone, 20, 157–165, 1997. [DOI] [PubMed] [Google Scholar]
- 8.Bouxsein ML and Radloff SE. “Quantitative ultrasound of the calcaneus reflects the mechanical properties of calcaneal trabecular bone,” J. Bone Miner. Res 12, pp. 839–846, (1997). [DOI] [PubMed] [Google Scholar]
- 9.Nicholson PHF, Muller R, Lowet G, Cheng XG, Hildebrand T, Ruegsegger P, Van Der Perre G, Dequeker J, and Boonen S. “Do quantitative ultrasound measurements reflect structure independently of density in human vertebral cancellous bone?,” Bone. 23, 425–431, (1998). [DOI] [PubMed] [Google Scholar]
- 10.Hans D, Wu C, Njeh CF, Zhao S, Augat P, Newitt D, Link T, Lu Y, Majumdar S, and Genant HK. “Ultasound velocity of cancellous cubes reflects mainly bone density and elasticity,” Calcif. Tissue Intl 64, 18–23, (1999). [DOI] [PubMed] [Google Scholar]
- 11.Trebacz H, and Natali A. “Ultrasound velocity and attenuation in cancellous bone samples from lumbar vertebra and calcaneus,” Osteo. Int’l, 9, 99–105, (1999). [DOI] [PubMed] [Google Scholar]
- 12.Cummings SR SR et al. The study of osteoporotic fractures research group: Bone density at various sites for the prediction of hip fractures. Lancet 341, 72–75, (1993). [DOI] [PubMed] [Google Scholar]
- 13.Hans D, Dargent-Molina P, Schott AM, Sebert JL, Cormier C, Kotzki PO, Delmas PD, Pouilles JM, Breart G, and Meunier PJ. “Ultrasonographic heel measurements to predict hip fracture in elderly women: the EPIDOS prospective study,” Lancet, 348, 511–514, (1996). [DOI] [PubMed] [Google Scholar]
- 14.Bauer DC, Gluer CC, Cauley JA, Vogt TM, Ensrud KE, Genant HK, and Black DM. “Broadband ultrasound attenuation predicts fractures strongly and independently of densitometry in older women,” Arch. Intern, Med 157, 629–634, (1997). [PubMed] [Google Scholar]
- 15.Schott M, Weill-Engerer S, Hans D, Duboeuf F, Delmas PD, and Meunier PJ, “Ultrasound discriminates patients with hip fracture equally well as dual energy X-ray absorptiometry and independently of bone mineral density,” J. Bone Min. Res, 10, 243–249, (1995). [DOI] [PubMed] [Google Scholar]
- 16.Turner H, Peacock M, Timmerman L, Neal JM, and Johnston CC Jr., “Calcaneal ultrasonic measurements discriminate hip fracture independently of bone mass,” Osteo. International, 5, 130–135, (1995). [DOI] [PubMed] [Google Scholar]
- 17.Glüer C, Cummings SR, Bauer DC, Stone K, Pressman A, Mathur A, and Genant HK. “Osteoporosis: Association of recent fractures with quantitative US findings,” Radiology, 199, 725–732, (1996). [DOI] [PubMed] [Google Scholar]
- 18.Thompson P, Taylor J, Fisher A, and Oliver R, “Quantitative heel ultrasound in 3180 women between 45 and 75 years of age: compliance, normal ranges and relationship to fracture history,” Osteo. Int’l, 8, 211–214, (1998). [DOI] [PubMed] [Google Scholar]
- 19.Faran JJ, Sound scattering by solid cylinders and spheres, J. Acoust. Soc. Am, 23, 405–418 (1951) [Google Scholar]
- 20.Morse PM and Ingard KU, Theoretical Acoustics. Princeton, NJ, Princeton University Press, 1986. [Google Scholar]
- 21.Madsen L, Insana MF, and Zagzebski JA, Method of data reduction for accurate determination of acoustic backscatter coefficients, J. Acoust. Soc. Am, 76, 913–923, (1984). [DOI] [PubMed] [Google Scholar]
- 22.O’Donnell M and Miller JG, Quantitative broadband ultrasonic backscatter: An approach to nondestructive evaluation in acoustically inhomogeneous materials, J. Appl. Phys 52, 1056–1065 (1981). [Google Scholar]
- 23.Wear KA, Milunski MR, Wickline SA, Perez JE, Sobel BE, and Miller JG, Differentiation between acutely ischemic myocardium and zones of completed infarction in dogs on the basis of frequency-dependent backscatter, J. Acoust. Soc. Am, 85, no. 6, 2634–2641, June, (1989). [DOI] [PubMed] [Google Scholar]
- 24.Luo G, Kaufman JJ, Chabrera A et al. , Computational methods for ultrasonic bone assessment. Ultrasound Med. & Biol, 25, 823–830; 1999. [DOI] [PubMed] [Google Scholar]
- 25.Wear KA. Frequency dependence of ultrasonic backscatter from human trabecular bone: theory and experiment. J. Acoust. Soc. Am 106, 3659–3664, 1999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Wear KA. Anisotropy of ultrasonic backscatter and attenuation from human calcaneus: Implications for relative roles of absorption and scattering in determining attenuation. J. Acoust. Soc. Am, 107, 3474–3479, 2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Chaffai S, Roberjot V, Peyrin F, Berger G, and Laugier P. Frequency dependence of ultrasonic backscattering in cancellous bone: Autocorrelation model and experimental results. J. Acoust. Soc. Am 108, 2403–2411, (2000). [DOI] [PubMed] [Google Scholar]
- 28.Roberjot V, Laugier P, Droin P, Giat P, and Berger G. Meaurement of integrated backscatter coefficient of trabecular bone. Proc. 1996 IEEE Ultrason. Symp Vol. 2, 1123–1126, (1996). [Google Scholar]
- 29.Wear KA and Garra BS. Assessment of bone density using broadband ultrasonic backscatter, Proc. 22nd Int. Symp Ultrason. Imag. and Tissue Char, Washington, DC., 14 (1997), (Abstract). [Google Scholar]
- 30.Giat P, Chappard C, Roux C, Laugier P, and Berger G. Preliminary clinical assessment of the backscatter coefficient in osteoporosis, Proc. 22nd Int. Symp Ultrason. Imag. and Tissue Char, Washington, DC, 16, 1997, (Abstract). [Google Scholar]
- 31.Wear KA and Garra BS. Assessment of bone density using ultrasonic backscatter. Ultrason. Med. & Biol 24, 689–695, (1998). [DOI] [PubMed] [Google Scholar]
- 32.Wear KA and Armstrong DW, The relationship between ultrasonic backscatter and bone mineral density in human calcaneus, IEEE Trans. Ultrason. Ferro. Freq. Cont, 47, 777–780, 2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Wear KA, Stuber AP, and Reynolds JC, Relationships of ultrasonic backscatter with ultrasonic attenuation, sound speed, and bone mineral density in human calcaneus, Ultrason. Med. & Biol, 26, 1311–1316, (2000). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Hoffmeister BK, Whitten SA, and Rho JY, Low-megahertz ultrasonic properties of bovine cancellous bone, Bone, 26, (2000). [DOI] [PubMed] [Google Scholar]
- 35.Hoffmeister BK, Whitten SA, Kaste SC, and Rho JY, Effect of collagen and mineral content on the high frequency ultrasonic properties of human cancellous bone, Bone, in press. [DOI] [PubMed] [Google Scholar]
- 36.Zagzebski JA, Yao LX, Boote EJ, and Lu ZF. Quantitative Backscatter Imaging in Ultrasonic Scattering in Biological Tissues, edited by Shung KK and Thieme GA, CRC Press, Boca Raton, FL, (1993). [Google Scholar]
- 37.Wear KA, Garra BS, and Hall TJ, Measurements of ultrasonic backscatter coefficients in human liver and kidney in vivo, J. Acoust. Soc. Am, 98, 1852–1857, (1995). [DOI] [PubMed] [Google Scholar]
- 38.Wear KA, “The effects of frequency-dependent attenuation and dispersion on sound speed measurements: applications in human trabecular bone,” IEEE Trans Ultrason. Ferro. Freq. Cont, 47, 265–273, (2000). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Wear KA. “Measurements of phase velocity and group velocity in human calcaneus,” Ultrason. Med. Biol, 26, 641–646, (2000). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Kinsler LE, Frey AR, Coppens AB, and Sanders JV. Fundamentals of Acoustics. Third Ed., John Wiley & Sons, Inc. Toronto, 1982, chapter 1. [Google Scholar]
- 41.Njeh CF, Hans D, Li J, Fan B, Fuerst T, He YQ, Tsuda-futami E, Lu Y, Wu CY, and Genant HK, Comparison of six calcaneal quantitative ultrasound devices: precision and hip fracture discrimination, Osteo. Int, 11, 1051–1062, 2000. [DOI] [PubMed] [Google Scholar]
- 42.Wear KA, Ultrasonic attenuation in human calcaneus from 0.2 to 1.7 MHz, IEEE Trans. Ultrason Ferro. Freq. Cont., 48, (2001). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Cheng S, Fan B, Wang L, Fuerst T, Lian M, Njeh C, He Y, Kern M, Lappin M, Tylavsky F, Casal D, Harris S, and Genant HK. Factors affecting broadband ultrasound attenuation results of the calcaneus using a gel-coupled quantitative ultrasound scanning system. Osteo. Int 10, 495–504, 1999. [DOI] [PubMed] [Google Scholar]
- 44.Frost ML, Blake GM, and Fogelman J, Contact quantitative ultrasound: an evaluation of precision, fracture discrimination, age-related bone loss and applicability of the WHO criteria, Osteo. Int 10, 441–449, 1999. [DOI] [PubMed] [Google Scholar]
- 45.Hoel PA, Introduction to Mathematical Statistics, John Wiley & Sons, Inc., New York,167, (1962). [Google Scholar]
- 46.Alves JM, Xu W, Lin D, Siffert RS, Ryaby JT, and Kaufmann JJ. “Ultrasonic assessment of human and bovine cancellous bone: a comparison study,” IEEE Trans. Biomed. Eng 43, 249–258, (1996). [DOI] [PubMed] [Google Scholar]