

ABSTRACT
Introduction:Mediators of immunity and inflammation are playing a crucial role in COVID-19 pathogenesis and complications as demonstrated by several genetic and clinical studies. Thus, repurposing of drugs that possess anti-inflammatory and/or immune-modulatory effects for COVID-19 is considered a rational approach.
Areas covered:We analyze selected studies that correlated COVID-19 with dysregulated interferon and inflammatory responses while reflecting on our academic and real-life experience using non-steroidal anti-inflammatory drugs, nitazoxanide and azithromycin for management of COVID-19. Moreover, we interpret the results that suggested a potential survival benefit of low-dose aspirin and colchicine when used for COVID-19.
Expert opinion:Nitazoxanide/azithromycin combination has been first hypothesized by the author and practiced by him and several researchers to benefit COVID-19 patients due to a potential ability to augment the natural interferon response as well as their positive immunomodulatory effects on several cytokines. Furthermore, NSAIDs, that are unfortunately currently at best of second choice after paracetamol, have been early postulated and clinically practiced by the author to prevent or ameliorate COVID-19 complications and mortality due to their anti-inflammatory and immunomodulatory properties. Finally, we repeat our previous call to adopt our observational study that used these drugs in sufficiently powered double blind randomized clinical trials.
KEYWORDS: COVID-19, Interferons, nitazoxanide, azithromycin, NSAIDS, ibuprofen, Diclofenac, IL-6 amplifier, NF-kB, monocytic immunological dysrhythmia
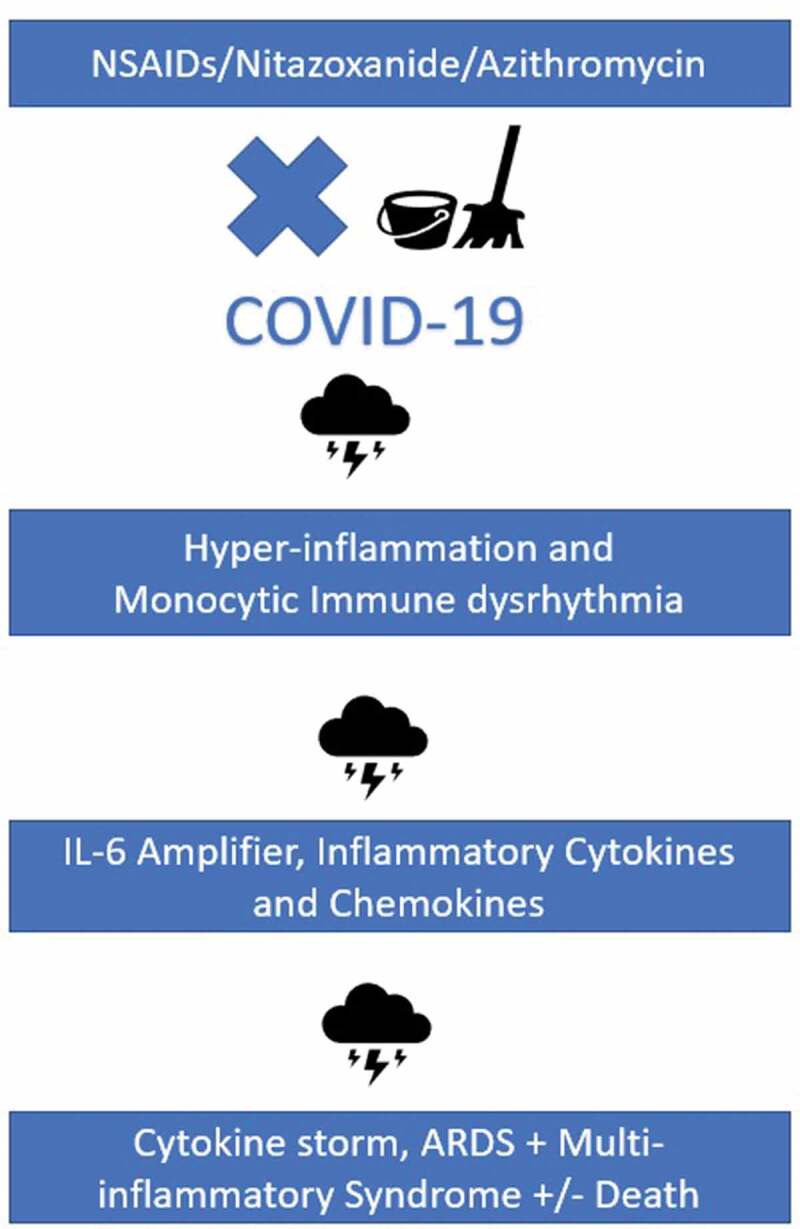
GRAPHICAL ABSTRACT
1. Introduction
The hyper-inflammation and immunopathogenesis of COVID-19 have been well described [1–3] and the study results published by Pairo-Castineira et al. [4], together with its formal interpretation as regards to the potential pharmacological interventions [https://www.ed.ac.uk/edinburgh-infectious-diseas–es/news/news/genes-key-to-new-covid-19-treatments], might be considered as a promising step toward a better understanding of the genetic basis by which mediators of immunity and inflammation determine the pathophysiology of COVID-19.
Interestingly and more clinically important, an exaggerated inflammatory response was described as the culprit of the majority of COVID-19 deaths and it was attributed to a weak, irregular or inhibited early interferon response to SARS CoV-2 infection that causes an excessive viral replication triggering this exaggerated inflammatory response and leading to unconstrained immune response which is responsible for COVID-19 associated mortality, rather than the virus itself [5–7].
Furthermore, type I interferon response was shown to contribute to the pathogenesis of critical COVID-19 through domination of gene expression changes in peripheral blood mononuclear cells [8] and specific interferon therapy was shown to be crucial in management of selected COVID-19 cases [9]. Thus, exploration of the immuno-inflammatory response to SARS CoV-2 might help us to insightfully repurpose some existing drugs for early management of COVID-19.
2. COVID-19 cytokine storm: role of IL-6 amplifier and monocytic immunological dysrhythmia
Interestingly, interleukin 6 is a multifunctional cytokine that plays important roles in both the immune and inflammatory body responses [10] and irregular IL-6 production was described to be implicated in the development of various immune-inflammatory diseases including rheumatic arthritis [11] and was correlated to its disease activity [12]. Furthermore, interleukin 6 amplifier (IL-6 Amp) which is an amplification mechanism for the production of IL-6 and a variety of other cytokines and chemokines through a synergic interaction between STAT3 and nuclear factor-kappa B (NF-kB), plays a key role in development of cytokine storm syndromes [13].
Importantly, IL-6 also shares significantly in the formation of the intravascular coagulation that causes multiorgan injury and failure [14] while aging, obesity, and diabetes, which are known risk factors to develop severe COVID-19, are also associated with a lower threshold of the activation of IL-6 Amp [13]. Notably, infected immunologically dysregulated circulating monocytes were described to trigger an acute inflammatory responses leading to cytokine storm and death [15].
Taken together, we provide a concise analysis and interpretations of selected genetic, experimental, and clinical results that correlated COVID-19 with interferon and immune-inflammatory responses according to our real-life and academic experience that used non-steroidal anti-inflammatory drugs (NSAIDs), nitazoxanide and azithromycin to manage COVID-19 patients and illustrate their potential beneficial mechanisms that might mitigate or reverse the IL-6 amplifier and the dysregulated monocytic immunological response or dysrhythmia as we would like to describe it.
3. Nitazoxanide/azithromycin combination for COVID-19
We agree with Pairo-Castineira et al. [4] in their recommendation that clinical trials should focus on drugs that target specific antiviral and anti-inflammatory pathways after they have confirmed that increased expression of the interferon receptor subunit IFNAR2 reduced the odds of severe COVID-19. Interestingly, Blocking of interferons production by the N protein of SARS-CoV was previously shown to be directly important for viral survival [16]. Importantly, we would like to mention that we have previously, on April 2020, suggested a pioneering combination of the FDA approved inexpensive drugs; nitazoxanide/azithromycin to be used for early COVID-19 management basing on a hypothesis attributing their potential benefit to the ability to augment and restore our natural interferon homeostasis [17]. Later, some clinical studies started to prove the validity of our recommendation for this combination [18–20]. Interestingly, nitazoxanide was shown to inhibit the production of several pro-inflammatory cytokines including IL-6, IL-8 and TNF- α in peripheral blood mononuclear cells [21] and it was also shown, in an in vivo murine model and macrophage cell line, to decrease IL-6 production induced by thioglycollate and lipopolysaccharide, respectively to be suggested as a promising lead drug for diseases associated with overproduction of IL-6 [11] and for its anti-IL-6 properties and other potential effects, nitazoxanide was suggested to be tested, either acting alone or as coadjuvant, in the treatment of ovarian carcinoma [22].
Similarly, azithromycin was remarkably shown to significantly inhibit the inflammatory IL-1 α and TNF-α cytokines in human monocytes [23]. Moreover, only when azithromycin was added to ceftriaxone in a murine model of polymicrobial sepsis, the lung concentrations of IL-6, TNF-α, and IL-1β were significantly decreased providing a survival benefit [24]. Notably, the positive immunomodulatory effects of several macrolides including azithromycin were shown in several diseases including bronchial asthma and chronic obstructive pulmonary disease [25,26].
Importantly, as regards to the inconsistent results, mentioned by Pairo-Castineira et al., as regards to the efficacy of interferons to manage COVID-19, we suggest to only focus on certain types of interferons in treatment of COVID-19 and we recommend more larger-scale clinical trials using IFN β-1b to be tested for severe COVID-19 cases as evidence coming from several randomized clinical trials show significant recovery as well as morality benefits [27–29]. On the other hand, we suggest, from a pharmacovigilant risk-benefit ratio, that interferons themselves should not be readily administered to early cases of COVID-19, as might be interpreted from Pairo-Castineira et al. in their manuscript.
4. NSAIDs potential therapeutic role in management of COVID-19
Importantly, Pairo-Castineira et al have demonstrated that reduction in the activity of the pro-inflammatory TYK2 gene protects against COVID-19 but they have suggested that barictinib, a second-line therapy used for moderate to severe active rheumatoid arthritis in adults, might be of benefit in selected COVID-19 cases as it targets TYK2, a recommendation that was also previously published [30]. We would like to disagree, also from a pharmacovigilant point of view, with this recommendation as we also suggest that the risk benefit ratio of this drug to be used in an undergoing active viral infectious disease is outbalanced [30,31].
Alternatively, we have previously published two articles to justify the use of NSAIDs including diclofenac potassium and ibuprofen for early management of COVID-19 [32,33]. We suggested that NSAIDs might prevent, especially when early administered, or reverse COVID-19 associated hyperinflammatory response which is correlated with the immuno-pathologically induced SARS CoV-2 morbidity and mortality [5] and to prevent the cytokine induced lymphocyte distraction into or away from the lungs that is laboratory manifested through lymphopenia [32].
Furthermore, we suggest that NSAIDs might possess a beneficial COVID-19 immunomodulatory effect through induction of the release of a number of anti-inflammatory cytokines and mitigate the formation of several proinflammatory cytokines including some important monocytic proinflammatory cytokines (TNF- α, IL-1 β, IL-6, IL-8) [34–36] and this might help to prevent the development of the cytokine storm [14]. Interestingly, diclofenac 50 mg bid for five days has been previously shown to downregulate the production of IL-6 in response to surgical dental trauma [37] and diclofenac, administered for two days, was also demonstrated to significantly and temporarily decrease serum IL-6 peak developed 12 h post skin incision and to increase the anti-inflammatory IL-10, 6 h post skin incision, as compared to placebo in patients undergoing major surgery [38]. Furthermore, lornoxicam, another NSAID, was demonstrated to dose dependently inhibit IL-6 formation and was suggested to inhibit post transcriptional or translational mechanisms of IL-6 gene expression in several human cell lines [39]. Additionally, celecoxib and ibuprofen were shown to significantly reduce the IL-6 and TNF-alpha levels in the synovial fluid of patients suffering from knee osteoarthritis [40].
Moreover, besides their well-known potent analgesic antipyretic properties, other potential beneficial effects of NSAIDs when given early in COVID-19 might include mitigating formation of the inflammatory nitric oxide derived from iNOS [39]; decrease activation of the NF-κB pathway [38] which is of vital importance in development of cytokine storm [14]; caspases inhibition [41] which are described in COVID-19 pathogenesis [42]; limiting the production of prostaglandins associated with edema [37] that would impair lung oxygenation and gas transfer.
5. Expert opinion
COVID-19 has many mysteries which are waiting to be resolved in its pathogenesis, progression, and management that witnessed repurposing of several drugs including experimental and potentially toxic ones without significant outcomes [43]. We suggest that the drugs mentioned in this manuscript which are readily available, relatively safe, and very much economic possess a solid theoretical basis that should be always considered before repurposing any drug for COVID-19 and the upcoming anticipated pandemics.
In our opinion, it was a real misfortune that NSAIDs have been practically discriminated against globally as regards to COVID-19 management, as apart from the complex pieces of evidence represented in this manuscript, they possess a very simple obvious potential to combat the well-described hyperinflammatory process associated with COVID-19 and correlated with its morbidity and/or mortality and, unlike glucocorticoids [43], when used early to manage COVID-19 they do possess beneficial immunomodulatory effects. Moreover, we postulate that NSAIDs, when given early, might prevent SARS CoV-2 induced dysregulated humoral immune reaction and improve the durability of SARS CoV-2 induced antibodies [44] to be noted that the effect of NSAIDs on the humoral immunity is far from considered conclusive whether in academia or as regards to its clinical significance [45].
Interestingly, though we welcomed a recently advertised breakthrough that low-dose aspirin, one of the NSAIDs, has shown a significant COVID-19 survival benefit [46], we have heavily criticized the integrity of its analysis according to our academic experience [47]. Similarly, we consider that colchicine, which is used mainly in treatment of gout, similarly advertised breakthrough [https://app.cyberimpact.com/newsletter-view-online?ct=guhsMu_jogsWK5zuKuZWMiFdWXxrNhn6Nkcjb1fm-HUAuS81ZbwD0N6bKX9bJ23ALFDAfrG83CWBnSzT41zxRA] might also prove valid, yet we wish to suggest that colchicine acts via an anti-inflammatory and immune-modulatory mechanisms [48] which are better achieved using the safer and more effective NSAIDs [49].
Unfortunately, six months have elapsed until our paper revoking the original claims that led to the current NSAIDs situation has been eventually sent for peer review, accepted and published [33], yet until today, NSAIDs are avoided in many countries all over the world especially in the developing ones and, even in the most favorable situations, they are considered of second choice to manage COVID-19 after paracetamol that does not possess major peripheral anti-inflammatory effects as compared to NSAIDs [50].
Ironically, our real-life experience using NSAIDs (ibuprofen, diclofenac potassium, ketorolac, lornoxicam, celecoxib, and naproxen), nitazoxanide, and azithromycin to treat COVID-19 patients safely and effectively has been dealt likewise and much worse for almost a year [51]. However, it is currently represented in a much-updated preprint , in which we also cite numerous references of clinical studies performed by other researchers that further support the safety and/or potential efficacy of NSAIDs, nitazoxanide and azithromycin in COVID-19 management while we also fully explain our personalized and pharmacovigilant approach to use these drugs either separately or collectively in management of COVID [52].
Finally, we suggest that the risk benefit ratio for these FDA approved drugs, which are well known and familiar to clinicians all over the world, is in favor of performance of large randomized clinical trials against a standard care protocol at the earliest opportunity as COVID-19 potential safe and economic cure might be available and unfortunately repeatedly ignored for one year.
Acknowledgments
This humble work is dedicated to a noble professor, immunologist, Prof. Toshio Hirano (National Institutes for Quantum and Radiological Science and Technology, Chiba, Japan). Apart from IL-6 discovery, without his devout, brilliant, and relentless research most of our knowledge about IL-6 and IL-6 Amp would not become as lucid and readily available as it is. I wish also to express my deepest gratitude to Expert Review of Anti-infective Therapy and to the commissioning editor; Ms. Felicity Poole as highly constructive comments that came from four honorable anonymous peer reviewers have significantly improved the quality of knowledge represented in this manuscript and no words would perfectly convey my utmost respect and gratitude.
Funding Statement
This paper was not funded.
Declaration of interest
The author has no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Reviewer disclosures
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
References
- 1.Dhama K, Patel SK, Pathak M, et al. An update on SARS-CoV-2/COVID-19 with particular reference to its clinical pathology, pathogenesis, immunopathology and mitigation strategies. Travel Med Infect Dis. 20202020/09/01/;37:101755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Prompetchara E, Ketloy C, Palaga T.. Immune responses in COVID-19 and potential vaccines: lessons learned from SARS and MERS epidemic. Asian Pac J Allergy Immunol. 2020. March;38(1):1–9. [DOI] [PubMed] [Google Scholar]
- 3.Attia YA, El-Saadony MT, Swelum AA, et al. COVID-19: pathogenesis, advances in treatment and vaccine development and environmental impact—an updated review. Environ Sci Pollut Res. 2021;28(18):22241–22264. . 2021/ 03/18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.*Pairo-Castineira E, Clohisey S, Klaric L, et al. Genetic mechanisms of critical illness in Covid-19. Nature. 2020;591(7848):92–98. . 2020/12/11 [DOI] [PubMed] [Google Scholar]
- 5.Karaderi T, Bareke H, Kunter I, et al. Host Genetics at the Intersection of Autoimmunity and COVID-19: a Potential Key for Heterogeneous COVID-19 Severity [Perspective]. Front Immunol. 2020. December;22(11):3314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.*Schreiber G. The Role of Type I Interferons in the Pathogenesis and Treatment of COVID-19. Front Immunol. 2020;11:595739-595739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.King C, Sprent J. Dual Nature of Type I Interferons in SARS-CoV-2-Induced Inflammation. Trends Immunol. 2021;42(4):312–322. . 2021/02/12/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lai Wei, Siqi Ming, Bin Zou, et al. Viral Invasion and Type I Interferon Response Characterize the Immunophenotypes during Q6 Covid-19 Infection. SSRN (Preprint). 2020;10.2139/ssrn.3564998
- 9.Haji Abdolvahab M, Moradi-kalbolandi S, Zarei M, et al. Potential role of interferons in treating COVID-19 patients. Int Immunopharmacol. 2021;90:107171. . 2021/01/01/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.*Hirano T. Interleukin HT. 6 in autoimmune and inflammatory diseases: a personal memoir. Proc Jpn Acad Ser B Phys Biol Sci. 2010;86(7):717–730. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hong SK, Kim HJ, Song CS, et al. Nitazoxanide suppresses IL-6 production in LPS-stimulated mouse macrophages and TG-injected mice. Int Immunopharmacol. 2012;13(1):23–27. . 2012/05/01/ [DOI] [PubMed] [Google Scholar]
- 12.Houssiau FA, Devogelaer J-P, Damme JV, et al. Interleukin-6 in synovial fluid and serum of patients with rheumatoid arthritis and other inflammatory arthritides. Arthritis Rheumatism. 1988;31(6):784–788. .1988/06/01 [DOI] [PubMed] [Google Scholar]
- 13.*Hirano T. IL- 6 in inflammation, autoimmunity and cancer. Int Immunol. 2021; 33(3): 127–148 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hojyo S, Uchida M, Tanaka K, et al. How COVID-19 induces cytokine storm with high mortality. Inflamm Regen. 2020;40(1):37. . 2020/10/01 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Meidaninikjeh S, Sabouni N, Marzouni HZ, et al. Monocytes and macrophages in COVID-19: friends and foes. Life Sci. 2021;269:119010. . 2021/03/15/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Tsang HF, Chan LWC, Cho WCS, et al. An update on COVID-19 pandemic: the epidemiology, pathogenesis, prevention and treatment strategies. Expert Rev Anti Infect Ther 2020. 1–12 10.1080/14787210.2021.1863146 [DOI] [PubMed] [Google Scholar]
- 17.**Kelleni MT. Nitazoxanide/azithromycin combination for COVID-19: a suggested new protocol for early management. Pharmacol Res. 2020. July;157:104874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Cadegiani FA, Goren A, Wambier CG, et al. Early COVID-19 Therapy with Azithromycin Plus Nitazoxanide, Ivermectin or Hydroxychloroquine in Outpatient Settings Significantly Reduced Symptoms Compared to Known Outcomes in Untreated Patients. medRxiv. 2020;2020. DOI: 10.1101/2020.10.31.20223883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.*Rocco PRM, Silva PL, Cruz FF, et al. Early use of nitazoxanide in mild Covid-19 disease: randomised, placebo-controlled trial. Eur Respir J 2020. 2003725 10.1183/13993003.03725-2020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Mendieta Zerón H, Meneses Calderón J, Paniagua Coria L, et al. Nitazoxanide as an early treatment to reduce the intensity of COVID‑19 outbreaks among health personnel. World Acad Sci J.. 2021;3(3):23. 2021/03/01. [Google Scholar]
- 21.Rossignol J-F. Nitazoxanide, a new drug candidate for the treatment of Middle East respiratory syndrome coronavirus. J Infect Public Health. 2016;9(3):227–230. . 2016/05/01/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Di Santo N, Ehrisman J. Research Perspective: potential Role of Nitazoxanide in Ovarian Cancer Treatment. Old Drug, New Purpose? Cancers (Basel). 2013;5(4):3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Khan A, Slifer T, Araujo F, et al. Effect of clarithromycin and azithromycin on production of cytokines by human monocytes. Int J Antimicrob Agents. 1999;11(2):121–132. . 1999/02/01/ [DOI] [PubMed] [Google Scholar]
- 24.Patel A, Joseph J, Periasamy H, et al. Azithromycin in Combination with Ceftriaxone Reduces Systemic Inflammation and Provides Survival Benefit in a Murine Model of Polymicrobial Sepsis. Antimicrob Agents Chemother. 2018;62(9):e00752–18. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.*Zimmermann P, Ziesenitz VC, Curtis N, et al. The Immunomodulatory Effects of Macrolides—A Systematic Review of the Underlying Mechanisms [Systematic Review]. Front Immunol. 2018-March-13. 2018;9(302). 10.3389/fimmu.2018.00302 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hodge S, Hodge G, Brozyna S, et al. Azithromycin increases phagocytosis of apoptotic bronchial epithelial cells by alveolar macrophages. Eur Respir J. 2006;28(3):486–495. . 2006/09// [DOI] [PubMed] [Google Scholar]
- 27.*Rahmani H, Davoudi-Monfared E, Nourian A, et al. Interferon β-1b in treatment of severe COVID-19: a randomized clinical trial. Int Immunopharmacol. 2020;88:106903. . 2020/11/01/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Shalhoub S. Interferon beta-1b for COVID-19. Lancet. 2020;395(10238):1670–1671. (London, England). . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.*Mary A, Hénaut L, Macq PY, et al. Rationale for COVID-19 Treatment by Nebulized Interferon-β-1b–Literature Review and Personal Preliminary Experience [Hypothesis and Theory]. Front Pharmacol. 2020-November-30. 2020;11(1885). 10.3389/fphar.2020.592543 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Zhang X, Zhang Y, Qiao W, et al. Baricitinib, a drug with potential effect to prevent SARS-COV-2 from entering target cells and control cytokine storm induced by COVID-19. Int Immunopharmacol. 2020;86:106749-106749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Jorgensen SCJ, Tse CLY, Burry L, et al. Baricitinib: a Review of Pharmacology, Safety, and Emerging Clinical Experience in COVID-19. Pharmacother J Human Pharmacol Drug Ther. 2020;40(8):843–856. .2020/08/01 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.**Kelleni MT. Early use of non-steroidal anti-inflammatory drugs in COVID-19 might reverse pathogenesis, prevent complications and improve clinical outcomes. Biomed Pharmacother. 2021;133:110982. . 2021/01/01/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.*Kelleni MT. ACEIs, ARBs, ibuprofen originally linked to COVID-19: the other side of the mirror. Inflammopharmacology. 2020. December;28(6):1477–1480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Atzeni F, Masala IF, Sarzi-Puttini PA. Review of Chronic Musculoskeletal Pain: central and Peripheral Effects of Diclofenac. Pain Ther. 2018;7(2):163–177. . 2018/12/01 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Housby JN, Cahill CM, Chu B, et al. NON-STEROIDAL ANTI-INFLAMMATORY DRUGS INHIBIT THE EXPRESSION OF CYTOKINES AND INDUCE HSP70 IN HUMAN MONOCYTES. Cytokine. 1999 1999/05/01/;11(5):347–358. . [DOI] [PubMed] [Google Scholar]
- 36.Grant RA, Morales-Nebreda L, Markov NS, et al. Circuits between infected macrophages and T cells in SARS-CoV-2 pneumonia. Nature. 2021;590(7847):635–641. . 2021/01/11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Singh P, Rastogi S, SSSBansal M, et al. A prospective study to assess the levels of interleukin-6 following administration of diclofenac, ketorolac and tramadol after surgical removal of lower third molars. J Maxillofac Oral Surg. 2015;14(2):219–225. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Mahdy AM, Galley HF, Abdel‐Wahed MA, et al. Differential modulation of interleukin‐6 and interleukin‐10 by diclofenac in patients undergoing major surgery. Br J Anaesth. 2002;88(6):797–802. . 2002/06/01/ [DOI] [PubMed] [Google Scholar]
- 39.Berg J, Fellier H, Christoph T, et al. The analgesic NSAID lornoxicam inhibits cyclooxygenase (COX)-1/-2, inducible nitric oxide synthase (iNOS), and the formation of interleukin (IL)-6 in vitro. Inflammation Res. 1999;48(7):369–379. . [DOI] [PubMed] [Google Scholar]
- 40.Gallelli L, Galasso O, Falcone D, et al. The effects of nonsteroidal anti-inflammatory drugs on clinical outcomes, synovial fluid cytokine concentration and signal transduction pathways in knee osteoarthritis. A randomized open label trial. Osteoarthritis Cartilage. 2013. September;21(9):1400–1408. [DOI] [PubMed] [Google Scholar]
- 41.Smith CE, Soti S, Jones TA, et al. Non-steroidal Anti-inflammatory Drugs Are Caspase Inhibitors. Cell Chem Biol. 2017;24(3):281–292. . 1999/07/01 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Kelleni M. NSAIDs Immunomodulation in COVID-19 Might Inhibit SARS CoV-2 ORF Proteins Induced Caspase Activation, Necroptosis and Endoplasmic Reticulum Stress. Authorea. 2021. Preprint. DOI: 10.22541/au.162126663.38675715/v2 [DOI] [Google Scholar]
- 43.*Kelleni MT. Tocilizumab, Remdesivir, Favipiravir, and Dexamethasone Repurposed for COVID-19: a Comprehensive Clinical and Pharmacovigilant Reassessment. SN Compr Clin Med. 2021;3(4):919–923. . 2021/04/01 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Kaneko N, Kuo -H-H, Boucau J, et al. Loss of Bcl-6-Expressing T Follicular Helper Cells and Germinal Centers in COVID-19. Cell. 2020;183(1):143–157.e13. . 2020/10/01/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Saleh E, Moody MA, Walter EB. Effect of antipyretic analgesics on immune responses to vaccination. Hum Vaccin Immunother. 2016;12(9):2391–2402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Chow JH, Khanna AK, Kethireddy S, et al. Aspirin Use Is Associated With Decreased Mechanical Ventilation, Intensive Care Unit Admission, and In-Hospital Mortality in Hospitalized Patients With Coronavirus Disease 2019. Anesthesia Analg. 2021;132(4):4. . [DOI] [PubMed] [Google Scholar]
- 47.*Kelleni M. Potential Crucial Role of COX-1 and/or COX-2 Inhibition, NSAIDs or Aspirin Triggered Lipoxins and Resolvins in Amelioration of COVID-19 Mortality. Authorea. 2021. Preprint. DOI: 10.22541/au.162126683.31375600/v1 [DOI] [Google Scholar]
- 48.Leung YY, Yao Hui LL, Kraus VB. Colchicine--Update on mechanisms of action and therapeutic uses. Semin Arthritis Rheum. 2015;45(3):341–350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Roddy E, Clarkson K, Blagojevic-Bucknall M, et al. Open-label randomised pragmatic trial (CONTACT) comparing naproxen and low-dose colchicine for the treatment of gout flares in primary care. Ann Rheum Dis. 2020;79(2):276–284. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Anderson BJ. Paracetamol (Acetaminophen): mechanisms of action. Pediatr Anesthesia. 2008;18(10):915–921. .2008/10/01 [DOI] [PubMed] [Google Scholar]
- 51.Kelleni M. Breakthrough: ibuprofen/nitazoxanide/azithromycin: a battle changer personalized COVID-19 telemedicine five days protocol. Authorea . 2020. June 22. (Preprint). DOI: 10.22541/au.159285564.49698842 [DOI] [Google Scholar]
- 52.**Kelleni M. NSAIDs/Nitazoxanide/Azithromycin Immunomodulatory Protocol Used in Adults, Geriatric, Pediatric, Pregnant, and Immunocompromised COVID-19 Patients: a Prospective Observational Study and Case-Series. Authorea. 2021. May:14. (Preprint). Doi: 10.22541/au.162126601.15715282/v2. [DOI] [Google Scholar]