

Abstract
Objective:
This study examined the effects of the Protecting Strong African American Families (ProSAAF) prevention program on children’s outcomes more than 2 years after enrollment, including direct effects of the intervention and indirect effects through couple functioning and parent-child relations.
Method:
Three hundred forty-six African American couples with an early adolescent child participated; all families lived in rural, low-income communities in the southern United States. Families were randomly assigned to ProSAAF or control conditions and completed four waves of data collection. Couples reported couple functioning at baseline (Wave 1) and at 9-month follow-up (Wave 2), and parent-child relations at 17-month follow-up (Wave 3). Children reported their conduct problems, affiliation with deviant peers, substance use, sexual onset, depressive symptoms, and self-control at 25-month follow-up (Wave 4).
Results:
Path analyses indicated significant indirect effects of ProSAAF on children’s outcomes through improvements in couple functioning and better parent-child relations. There were no significant direct effects of the intervention on children’s outcomes or significant indirect effects through couple functioning alone.
Conclusions:
This couple-focused prevention program has positive indirect effects on several child outcomes through the intervening processes of promoting improvements in couple functioning and better parent-child relations. These findings provide cautious optimism regarding the possible benefits of couple-focused programming on participants’ children while suggesting ways in which future couple-focused interventions could yield stronger effects on these youth.
Keywords: Couple functioning, couple intervention, parent-child relations, prevention, youth
A large, longstanding body of research indicates that couples’ relationship quality is associated with their children’s well-being (e.g., Brown, 2010; Cummings & Davies, 2002; Grych & Fincham, 1990). These robust correlational associations have contributed to a great deal of enthusiasm for the idea that interventions that enhance couples’ functioning will also lead to benefits for their children. In the United States, for example, the Administration for Children and Families has devoted at least $75 million annually since 2006 for the delivery of healthy marriage and relationship education activities for low-income families (Carter, 2018), under the assumption that improving couples’ romantic relationships through couple-focused programming should improve children’s well-being (e.g., Knox & Fein, 2008). To date, however, there has been surprisingly little research testing this assumption (for discussion, see Cowan & Cowan, 2019; Zemp, Bodenmann, & Cummings, 2016). Few studies have examined children’s outcomes following their parents’ involvement in a couples-focused intervention and even fewer intervention studies have tested the systemic theory underlying these programs whereby improvements in couple and family functioning lead to better child functioning. The current study was designed to address these critical gaps by using four waves of data from the Protecting Strong African American Families (ProSAAF) randomized clinical trial (Barton et al., 2018) to examine direct and indirect effects of couple-focused preventive intervention on long-term child outcomes.
Couples’ Interventions and Child Outcomes
Although the effects of couple and relationship education (CRE) programs on couples’ relationship outcomes have been well-documented, with several meta-analyses examining such effects (e.g., Cowan & Cowan, 2014; Hawkins, Blanchard, Baldwin, & Fawcett, 2008), there has been much less attention to their effects on child outcomes. One meta-analysis of over 150 CRE programs (Cowan & Cowan, 2014) found just 9 (6%) that included assessments of child outcomes. All were with parents of younger children, with 3 of the 9 studies focusing on parents during the transition to parenthood and the remainder focusing on parents of preschoolers and early elementary school years. Statistically significant effects on child outcomes were found for at least some of the child outcome measures in 8 of the 9 studies, though results were not consistent within or across studies. Ultimately, the authors concluded that “although these nine CRE trials are not sufficient to draw a general conclusion about the impact of couples-group participation on children, they provide some support for what had been an untested assumption— that parents’ participation in these groups can have a positive effect on their children” (p. 375). Further support is provided by a more recent study showing positive effects on sleep habits and internalizing behavior problems among the 2-year-old children of parents who participated in a transition to parenthood intervention during pregnancy relative to control (Jones et al., 2018), as well as from two other recent trials of couple-focused prevention programs indicating positive effects on child outcomes (Casey et al., 2017; Doss, Roddy, Llabre, Georgia Salivar, & Jensen-Doss, 2019), though conclusions from these two studies must be interpreted cautiously given their lack of control group data. Together, previous studies provide some support for the idea that couple-focused preventive interventions are associated with positive outcomes for participating couples’ children, though the amount and degree of such support is substantially weaker than that from the basic research literature on couples’ functioning and child outcomes.
These studies examining direct effects on children’s outcomes, though informative, provide an incomplete test of how couple-focused prevention benefits children. The key assumption underlying these programs – consistent with longstanding systemic theories of marital functioning and child development (e.g., Burman, John, & Margolin, 1987; Conger et al., 1992; Davies & Cummings, 1994; Fauber, Forehand, Thomas, & Wierson, 1990) – is that improvements in couple functioning will lead to better parent-child relations, which in turn lead to better child outcomes. For example, the Supporting Healthy Marriage (SHM) project, a large-scale evaluation of prevention programming for low-income married couples with children supported by the Administration for Children and Families’ Healthy Marriage Initiative, was described as “test(ing) the effectiveness of a skills-based relationship education program designed to help low-income married couples strengthen their relationships and, in turn, to support more stable and more nurturing home environments and more positive outcomes for parents and their children” (Hsueh et al., 2012, p. v, emphasis added). Explicitly testing these pathways to determine whether couple-focused interventions have significant indirect effects on child outcomes through their effects on couple functioning and/or parent-child relations has conceptual and methodological advantages (for additional discussion, see Feinberg & Jones, 2018). Conceptually, it allows for a more precise test of the theoretical model underlying these programs and can provide experimental evidence for these linkages. Methodologically, examining indirect effects on distal outcomes through multiple pathways has more statistical power than solely examining direct effects, particularly when associations are small, allowing for the possibility that mediation can exist in the absence of a significant direct association between intervention and outcome (e.g., Hayes, Preacher, & Myers, 2011; MacKinnon & Fairchild, 2009).
Unfortunately, such mechanistic tests are rare. In one study from the aforementioned review, changes in marital functioning among parents during the period their child was in prekindergarten to kindergarten were associated with child outcomes at the end of first grade (Cowan, Cowan, & Heming, 2005, as described in Cowan & Cowan, 2014). Another study among parents of children aged 2-12 (mean age = 7) participating in a relationship-enhancement program found that improvements in couples’ relationship quality from pre-to-post treatment mediated effects on child adjustment 2 weeks post-treatment (Zemp, Milek, Cummings, Cina, & Bodenmann, 2016). Finally, recent work examined the effects of participation in the Supporting Father Involvement group intervention on couple conflict, anxious/harsh parenting, and child behavior problems 2 months (Post 1) and 11 months (Post 2) post-treatment among child welfare-involved families (Pruett, Cowan, Cowan, Gillette, & Pruett, 2019). Results indicated direct effects of intervention only on Post 1 couple conflict, reflected in greater declines in couple conflict among the intervention group. However, there were significant indirect effects of intervention on Post 2 parenting quality through Post 1 and Post 2 couple conflict, such that intervention-related decreases in couple conflict were subsequently associated with lower levels of couple conflict and lower levels of anxious/harsh parenting. Better parenting quality at Post 2 was also associated with lower levels of concurrently measured children’s externalizing behaviors. These studies provide tentative support for the hypothesis that intervention-induced changes in couple functioning lead to positive child outcomes, but such support is limited in scope.
The Current Study
The current study aims to address these gaps and expand the limited research base on child outcomes following couple-focused prevention programs by building on earlier findings from the ProSAAF randomized clinical trial. ProSAAF was a family-centered prevention program for two-parent African American families with a preadolescent child living in the rural South (see Barton et al., 2018). As described in this earlier work, ProSAAF was designed to improve couples’ functioning in the short-to-moderate term, which in turn was expected to affect parenting and parent-child relationship quality and ultimately produce secondary long-term benefits for children’s well-being. Earlier results from this study indicated that the program was successful in achieving its primary aims, leading to significant improvements in couples’ functioning in the intervention group relative to control (Barton et al., 2018). The current study extends this work using four waves of data spanning 25 months to examine ProSAAF’s direct and indirect effects on several long-term child-reported outcomes, including conduct problems, affiliation with deviant peers, substance use, sexual onset, depressive symptoms, and self-control. Indirect effects are tested in accordance with traditional systemic models of influence in which changes in couple functioning are expected to influence the parent-child relationship and ultimately affect child outcomes; we also consider whether improvements in couple functioning alone predict child outcomes. Specifically, we test the following models:
Direct effects of ProSAAF on child outcomes at Wave 4;
Indirect effects of ProSAAF on child outcomes at Wave 4 through improvements in couple functioning from pre-to-post intervention (Wave 1 to 2); and
Indirect effects of ProSAAF on child outcomes at Wave 4 through improvements in couple functioning from Wave 1 to 2 and better parent-child relations at Wave 3.
This successive model testing approach and multi-year, multi-wave, multi-reporter design provide a rigorous test of direct effects of couple-focused prevention on child outcomes, a test of the hypothesis that intervention-induced change in couple functioning will predict later child outcomes, and a test of the broader underlying conceptual model that has guided the field (i.e., a multi-stage indirect effect on child outcomes through change in couple functioning and, subsequently, better parent-child relations). The design also allows us to examine whether any direct and/or indirect effects of ProSAAF on child outcomes are limited to one domain of child functioning (e.g., conduct problems) or generalize across multiple domains of functioning.
Method
Participants and Procedures
Couples with an African American child between the ages of 9 and 14 years took part in the study.1 The study received approval from the Institutional Review Board at the University of Georgia (study title: “Protecting Strong African American Families”; institutional review board approval number: 2012104112) and was not pre-registered. Subject enrollment began in 2013 and continued into 2014. All participants lived in small towns and communities in the southern US, where poverty rates are among the highest in the nation and unemployment rates are above the national average (DeNavas-Walt & Proctor, 2014). To be eligible, couples had to be in a relationship for 2 years or more, living together, and coparenting an African American child in the targeted age range for at least 1 year. Couples had to be willing to spend 6 weeks engaged in a family-centered prevention program and not be planning to move out of the study area during that period. Families were recruited by mail and phone via advertisements distributed in their communities as well as through lists that local schools provided. Schools in 16 counties provided information on youths in grades 4 through 6.
Participant recruitment, randomization, and progress through the study are illustrated in the CONSORT flowchart in Figure 1. A total of 1897 families were screened for eligibility. Of these families, 1145 were ineligible (e.g., household was headed by a single parent, the child was not in the targeted age range, the child was not African American, the family was enrolled in another program, the child had a sibling/stepsibling in the same grade). Of the 752 eligible families, 347 did not respond to the solicitation and 59 were unable to schedule an assessment. The remaining 346 families were randomized to intervention (n = 172) or control (n = 174) conditions. For parents and children in the intervention condition, respective retention of at least one parent was 84% and 83% at Wave 2 (W2) and Wave 3 (W3), respectively; retention of the target child was 79% at Wave 4 (W4). For parents and children in the control condition, respective retention of at least one parent was 89% and 93% at W2 and W3, respectively; retention of the target child was 95% at W4. Retention did not vary by primary study variables or sociodemographic variables (i.e., marital status, children in the home, income, education, and child age). At W3 and W4, families assigned to the control condition were more likely to be retained in the sample than families assigned to the ProSAAF condition (p < .05).
Figure 1.
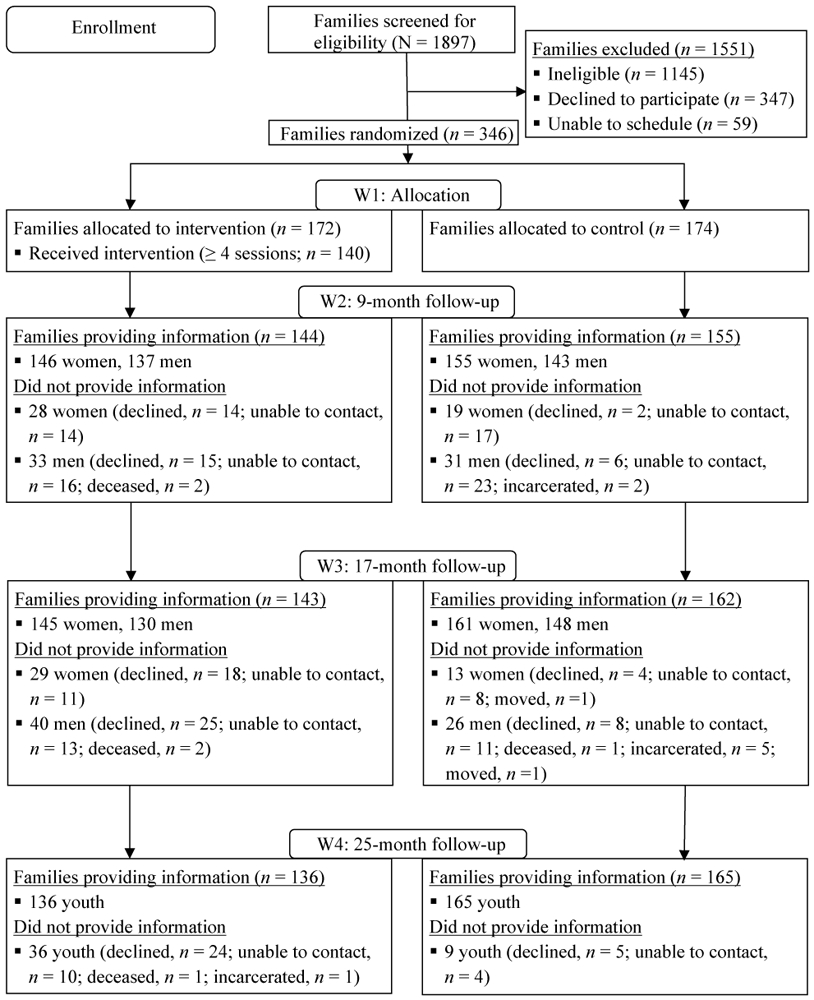
Participant flow chart following CONSORT guidelines
Of the couples in the randomized sample, 63% were married, with a mean length of marriage of 9.8 years (SD = 7.48; range < 1 year to 56 years). Unmarried couples had been living together for an average of 6.7 years (SD = 5.42; range < 1 year to 24 years). Adults’ mean ages were 39.9 years (SD = 9.6; range 21 to 83 years) for men and 36.6 years (SD = 7.45; range 23 to 73 years) for women. Children’s mean age was 10.9 (SD = 0.90; range 9 to 14 years). The majority of families in the study could be classified as working poor: 51% had incomes below 100% of the federal poverty level and an additional 17% had incomes between 100% and 150% of that level. The majority of both men (74% [65% full-time]) and women (61% [45% full-time]) were employed. Median monthly income was $1,375 (SD = $1,375; range $1 to $7,500) for men and $1,220 (SD = $1,440; range $1 to $10,000) for women. Median education levels were high school or GED (ranging from less than grade 9 to a doctorate or professional degree) for men and some college or trade school (ranging from less than grade 9 to a master’s degree) for women. The total number of children residing in the home ranged from 1 to 8, with a median of 3 and a mode of 2 (M = 2.97; SD = 1.48). In families for whom more than one child was in the targeted range (Grades 4-6), the child who was closer to age 11 was identified as the target child. Ninety-four percent of women were biological mothers and 49% of men were biological fathers (and 38% were stepfathers) for the target child. Nearly all couples were heterosexual (n = 344 [99.4%]); two families were headed by a female same-sex couple.
Project staff visited couples’ homes, explained the study in greater detail, and obtained informed consent from adult participants and assent and parental permission for child participants. Each participating family member then completed the W1 assessment using audio computer-assisted self-interview software installed on laptop computers. Participants completed surveys on separate laptops and, if possible, in separate rooms. Participants did not talk to one another or see one another’s responses while completing the surveys. Families were visited for W2, W3, and W4 assessments a mean of 9.4 months, 17.0 months, and 24.5 months respectively after W1. Each adult was compensated with a $50 check for completing each assessment. Randomization took place after couples completed pretest measures. Block randomization by marital status was performed within each county to facilitate group equivalence.
The Protecting Strong African American Families (ProSAAF) Program
Program overview (for additional detail, see Barton et al., 2018).
ProSAAF was informed by social learning theory and cognitive-behavioral therapy (CBT) approaches to prevention of couple and family problems (e.g., Stanley et al. 1999) and specifically designed to meet the needs of two-parent African American families residing in the rural South. Each session focused on a specific stressor that rural African American couples experience (e.g., work, racism, finances, extended family), and couples were instructed in cognitive and behavioral techniques for handling the stressor together and responding in mutually supportive and effective ways. Sessions were organized around DVD presentations that taught program content and depicted scenarios of program-targeted interactions and behaviors. In each of the sessions, the facilitator guided the couple through the video instruction and modeling, structured activities, and discussions of specific topics. The first 60 min of each session focused on the adult romantic-partner dyad (i.e., the couple relationship), and the next 30 min focused on parenting/coparenting topics. The facilitator then met with the target youth for a 15-min individual activity, while the couple took a break in a different room. After the youth activity, the entire family met with the facilitator for a 15-min joint activity, such as a discussion or a game. This session structure was modeled after the Strengthening Families Program (Kumpfer, Molgaard, & Spoth, 1996).
Details about each session of the curriculum can be found in Supplemental Table S1. Sample couple-focused content included recognizing positive aspects of the partnership, identifying “beneath the surface” issues, strengthening couple identity and unity, and enhancing quality time together. Sample coparenting/parenting issues included empathy with children, discipline, and supporting children. Youth issues included empathy with parents, resisting temptation, and qualities of good friends; and parent-child issues included understanding each other, effective communication, and working together.
ProSAAF implementation.
Intervention facilitators were African American community members who participated in several initial days of training on the curriculum and subsequently received ongoing supervision on implementation. The facilitator visited the couple in their home for six consecutive weeks to conduct the 2-hour intervention sessions. Two booster sessions were scheduled to reinforce the material covered during the main intervention. If a couple separated or divorced, an alternative booster session was offered that focused on the coparenting relationship and protecting children from the stress of separation and divorce. Booster session 1 was scheduled approximately 3 months after program completion (approximately 2 months before the W2 assessment) and booster session 2 was scheduled approximately 9 months after program completion (approximately 4 months before the W3 assessment).
Following each intervention session, each adult was compensated for their time (Sessions 1 and 2 = $25, Sessions 3 and 4 = $30, Sessions 5 and 6 = $35, Booster Sessions 1 and 2 = $35). A total of 28 facilitators implemented the program; the total number of families with whom each facilitator worked ranged from 1 to 15.
Attendance.
Of the 172 families assigned to the intervention condition, 81% (n = 139) completed all six sessions. Total sessions attended by remaining families were as follows: 5 sessions, 0.6% (n = 1); 3 sessions, 2.9% (n = 5); 2 sessions, 2.3% (n = 4); 1 session, 4.1% (n = 7); and no sessions, 9.3% (n = 16). For booster sessions, 73% (n = 126) of intervention families participated in booster session 1 and 59% (n = 101) participated in booster session 2. Seven families (4% of intervention families) were offered the alternative booster session focused on the coparenting relationship and protecting children from the stress of separation and divorce; all seven families attended. With the possible exception of the alternative booster, sessions were attended by all family members.
Fidelity.
All sessions were audiotaped to allow implementation to be monitored. A sample of sessions (n = 220, corresponding to 25% of all project sessions) was coded using an 87- to 143-point checklist (depending on the session) for fidelity to intervention guidelines. All facilitators were assessed at least once. Of the 220 sessions reviewed, 10% (n = 22) were coded by more than one rater (ICC = .94). The mean fidelity score across facilitators on a scale of 0-100% was 91% (SD = 9.0%).
Control group.
Couples in the control group were assessed on the same schedule as those in the intervention group, thereby controlling for effects of repeated measurements, maturation, individual differences, and external social changes. After the pretest, couples were mailed the book 12 Hours to a Great Marriage (Markman, Stanley, Blumberg, Jenkins, & Whaley, 2004) and an accompanying workbook that presented reasons for enhancing the couple’s relationship, guidelines, examples of communication and problem-solving strategies, and exercises designed to enrich relationships. Use of the book/workbook was not assessed at follow-up assessments.
Measures
Couple functioning.
To provide a global assessment of couple functioning at Wave 1 and at Wave 2, we used a composite variable from our previous work (citation withheld for review) that included partners’ ratings of effective communication, relationship confidence, relationship satisfaction, and perceived partner support. All four variables were significantly correlated at each assessment (rs = .52 to .83, all ps < .001) and showed significant improvement following the intervention (Barton et al., 2018). All scales were standardized within sex (separately at W1 and W2), then averaged, and were scored such that higher scores indicated more positive couple functioning.2
Effective communication
was assessed using a seven-item version of the Communication Skills Test (Jenkins & Saiz, 1995). This measure has been used in prior studies with evidence for its internal consistency and validity (e.g., Stanley et al., 2001), including studies specifically with African American samples (e.g., Barton et al., 2016). Items were rated on a scale ranging from 1 (almost never) to 7 (almost always) and summed to assess the frequency of effective communication patterns between partners (sample item: “When discussing an issue, my mate and I both take responsibility to keep us on track”; men: α ≥ .84; women: α ≥ .86).
Relationship confidence
was rated using the sum of four items from the Relationship Confidence Scale (RCS; Stanley, Hoyer, & Trathen, 1994). The RCS assesses partners’ confidence in the future of their relationship (sample item: “I am very confident when I think of my future with [partner name]”). Similar versions of the current scale have demonstrated good reliability and predictive validity (e.g., Whitton, Rhoades, & Whisman, 2014), including studies with predominantly African American samples (e.g., Owen et al., 2012). In the current study, items were rated on a Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree) (men: α ≥ .87; women: α ≥ .90).
Relationship satisfaction
was assessed using the Quality of Marriage Index (QMI; Norton, 1983), one of the most widely-used measures of relationship satisfaction, including studies with African Americans couples (e.g., Fincham, Ajayi, & Beach, 2011). This six-item scale measures global perceptions of relationship satisfaction (sample question: “[Partner name] and I have a good relationship”) using a Likert scale ranging from 1 (strongly disagree [questions 1-5] and very unhappy [question 6]) to 5 (strongly agree [questions 1-5] and perfectly happy [question 6]) (men: α ≥ .92; women: α ≥ .93).
Perceived partner support
was assessed using items from the Spouse Specific Social Support Scale (Culp & Beach, 1998). This scale was previously shown to be a reliable and valid measure of perceived spousal support among couples (including African American samples, e.g., Barton et al., 2016), showing associations with relationship and individual well-being (Culp & Beach, 1998). Five items were summed and used to assess partners’ perceptions of their ability to confide in and receive support from one another (sample item: “[Partner’s name] is someone I can confide in”); the response set ranged from 1 (almost never) to 5 (almost always) (men: α ≥ .81; women: α ≥ .87).
Parent-child relations.
Parent-child relations were measured at Wave 3 using a modified version of the 20-item short form of Interaction Behavior Questionnaire (Prinz, Foster, Kent, & O’Leary, 1979). This self-report measure assesses the quality of the parent-child relationship (sample items: “For the most part, your child likes to talk to you” and “In general, you don't think you and your child get along very well” [reverse scored]). The validity of this measure is well-established, including with African American samples (see Jones et al., 2008). The response set ranged from 1 (really false) to 4 (really true). Responses were summed such that higher scores indicated more positive parent-child relations (men: α = .83; women: α = .81)
Child outcomes.
Child adjustment at Wave 4 was measured across six different outcomes, all reported on by the target child: conduct problems, affiliation with deviant peers, substance use, sexual onset, depressive symptoms, and self-control.
Conduct problems.
Conduct problems were assessed using 13 items adapted from the Self-Report Delinquency scale (SRD; Elliott & Ageton, 1980). This adapted measure has demonstrated good reliability and convergent validity in prior research with African Americans (Kogan, Yu, Allen, Pocock, & Brody, 2015). Thirteen items from the SRD were used to assess the number of times in the past 6 months youth reported engaging in mild acts of delinquency (e.g., shoplifting, vandalism, getting into fights). The total score for each individual was calculated by summing the number of acts that the child reported committing at least once. The observed range was from 0 to 10.
Affiliation with deviant peers.
Affiliation with deviant peers was assessed through youths’ reports of the proportion of their close friends who engaged in deviant or risk-taking behaviors, drawn from Elliot’s work with delinquent youth (Elliott, Ageton, & Huizinga, 1985). A total of 11 behaviors were assessed, including selling drugs, getting in trouble with the police, skipping school, and damaging property. Response options ranged from 0 = none of them to 2 = all of them. Responses to items were summed, with higher scores indicating more deviant peer affiliation (α = .91).
Substance use.
To assess substance use, youth reported their past 3-month frequencies of cigarette smoking, alcohol use, heavy drinking, and marijuana use on a widely-used instrument from the Monitoring the Future Study (Johnston et al., 2007). A response set ranging from 0 (not at all) to 6 (more than two packs a day) was used for cigarette smoking; a scale ranging from 0 (none) to 6 (30 or more times) was used to measure alcohol use, heavy drinking, and marijuana use. Responses were summed to form a substance use composite, a procedure that is consistent with prior research (Brody & Ge, 2001; Newcomb & Bentler, 1988).
Sexual onset.
To assess onset of sexual activity, youth were asked “Have you ever had sex?” Response options were 0 = No and 1 = Yes.
Depressive symptoms.
Youths’ reports of depressive symptomatology were assessed using the 20-item Center for Epidemiological Studies-Depression scale (CES-D; Radloff, 1977; sample item: “how often did you feel depressed?” in the past week). Response options ranged from 0 (Rarely or none of the time [0-1 days]) to 3 (Most or all of the time [6-7 days]). Items were summed, with higher scores indicating more depressive symptoms (α = .79).
Self-control.
Youths’ reports of self-control were assessed using 13 items adapted from the Self-Control Rating Scale (Kendall & Wilcox; 1979; sample item: “You usually think before you act”). Youth were asked “how true each statement is for you,” with response options ranging from 1 (not all true) to 3 (very true). Items were summed, with higher scores indicating greater self-control (α = .81).
Descriptive statistics and correlations among all measures are depicted in Table 1.
Table 1.
Descriptive Statistics and Correlations of Measures (N = 346 families)
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| 1. Couple functioning (W1; Couple average) | --- | ||||||||
| 2. Couple functioning (W2; Couple average) | .53** | --- | |||||||
| 3. Parent-child relations (W3; Couple average) | .17** | .21** | --- | ||||||
| 4. Youth conduct problems (W4; Child report) | −.04 | −.02 | −.15** | --- | |||||
| 5. Youth deviant peer affiliation (W4; Child report) | −.12* | −.01 | −.15* | .57** | --- | ||||
| 6. Youth substance use (W4; Child report) | .04 | .07 | −.13* | .36** | .36** | --- | |||
| 7. Youth sexual onset a (W4; Child report) | −.10 | −.02 | −.11 | .19** | .19** | .30** | --- | ||
| 8. Youth depressive symptoms (W4; Child report) | −.08 | −.01 | −.10 | .29** | .28** | .10 | .06 | --- | |
| 9. Youth self-control (W4; Child report) | .05 | −.02 | .16** | −.31** | −.34** | −.25** | −.17** | −.44** | --- |
| M | .00 | −.04 | 63.87 | .86 | 2.00 | .23 | .15 | 12.55 | 30.49 |
| SD | 2.73 | 2.94 | 7.13 | 1.48 | 3.96 | .94 | --- | 8.01 | 5.02 |
Note. Spearman correlation coefficient reported for binary variables. W1 = Wave 1. W2 = Wave 2. W3 = Wave 3. W4 = Wave 4.
0 = No. 1 = Yes.
p < .05 (two-tailed).
p < .01 (two-tailed).
Analytic Plan
Analyses were conducted using path analysis in Mplus version 7.4 (Muthén & Muthén, 1998-2015). We ran three increasingly complex models; each model accommodated all 6 child outcomes simultaneously (i.e., conduct problems, affiliation with deviant peers, substance use, sexual onset, depressive symptoms, and self-control), and all models included child age and sex as control variables. In Model 1, we examined direct effects of ProSAAF participation on child outcomes at Wave 4 (i.e., ProSAAF assignment → W4 Child Outcome). In Model 2, we added Wave 1 and Wave 2 couple functioning to examine if ProSAAF predicted changes in couple functioning, and if post-intervention couple functioning predicted later child outcomes (i.e., ProSAAF assignment → W2 Couple Functioning [controlling for W1] → W4 Child Outcome). In Model 3, we added Wave 3 parent-child relations as an additional intervening variable to examine if ProSAAF predicted changes in couple functioning, if post-intervention couple functioning predicted later parent-child relations, and if parent-child relations predicted later child outcomes (i.e., ProSAAF assignment → W2 Couple Functioning [controlling for W1 levels] → Parent-Child Relations W3 → Child Outcome W4). This type of model where intervention variables are operating “in series” is useful when multiple intervening processes are assumed to transmit the effect of an independent variable to a dependent variable (Hayes et al. 2011; Hayes, 2012). For Models 2 and 3, if there were significant associations between the intervening variable(s) and outcomes, we proceeded to test indirect effects from intervention to long-term child outcomes. Indirect effects were examined using 2,000 bias-corrected bootstrapped sampling with 95% confidence intervals (CIs) involving unstandardized parameter estimates given the non-normal distribution of the product term comprising the indirect effect (Hayes, 2009).
All analyses were conducted according to an intent-to-treat (ITT) approach in which all couples assigned to the ProSAAF condition (regardless of program attendance) were compared to all couples assigned to the control condition. The ITT approach is recommended because it preserves randomization, provides a conservative estimate of program effects, and reflects practical community scenarios of noncompliance (Gupta, 2011). Missing data (12% of all valid cases) were handled using full information maximum likelihood estimation. Overall model fit followed criteria by Marsh, Hau, and Wen (2004).
Given our interest in testing ProSAAF’s effects at the family level (i.e., ProSAAF’s effects on child outcomes; ProSAAF’s effects on couple functioning predicting child outcomes; ProSAAF’s effects on couple functioning predicting parent-child relations predicting child outcomes) and the lack of sex-specific hypotheses for parents, we created a family-level variable for couple functioning and for parent-child relations by averaging male and female partner reports for each family. Averaging partners’ response is a common approach to creating dyadic/family-level variables (e.g., Acock, 1999) and was necessary in this case given that a model involving latent variables with separate indicators for men’s and women’s scores did not converge. Thus, our primary analyses included a couple average for relationship functioning at Wave 1 and at Wave 2 and for parent-child relations at Wave 3.3 We also conducted separate analyses for mothers and fathers; results are summarized in Supplemental Tables S3 and S4.
Results
Preliminary Analyses
Equivalence analyses testing whether experimental groups differed at W1 are shown in Table 2, and revealed no differences between ProSAAF and control conditions at W1 for family characteristics (i.e., marital status, number of children in the home, income, education, parent age, child age, or child sex) or couple functioning.
Table 2.
Equivalence of Treatment and Control Groups at Wave 1 (N = 346 families)
| Variables | Treatment (n = 172) |
Control (n = 174) |
Test statistic e |
p value | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| Family characteristics | ||||||
| Percent married a | 65% | N/A | 61% | N/A | 0.22 | .66 |
| Number of children in the home a | 3.07 | 1.50 | 2.87 | 1.45 | 1.22 | .22 |
| Income b | 2.89 | 2.11 | 2.77 | 2.13 | 0.52 | .60 |
| Education c, d | 5.48 | 1.84 | 5.46 | 1.66 | 1.88 | .17 |
| Parent age d | 38.12 | 8.64 | 38.25 | 8.87 | 1.63 | .20 |
| Child age | 10.85 | 0.92 | 10.90 | 0.88 | 1.61 | .11 |
| Percent child female | 51% | N/A | 42% | N/A | 0.50 | .62 |
| Couple functioning d | −0.20 | 2.90 | 0.19 | 2.54 | 1.34 | .18 |
Notes.
Based on female caregiver report.
Gross family monthly income divided by 1,000.
Range: 1 = Below grade 9; 11 = Doctorate or professional degree.
Couple average.
t-test for continuous and ordinal variables; chi-square cross-tab statistic for binary variables.
Direct and Indirect Effects of ProSAAF on Child Outcomes
Table 3 summarizes results for the three models. As indicated by the results for Model 1, there were no significant direct effects of ProSAAF assignment on any of the child outcomes, indicating that youth whose families participated in the ProSAAF program did not differ from control group youth at long-term follow-up. In Model 2, we examined whether ProSAAF-induced changes in couple functioning were sufficient as an intervening variable to produce significant effects on child outcomes. These models indicated that ProSAAF participation had a significant effect on changes in couple functioning from Wave 1 to Wave 2, with ProSAAF couples reporting greater improvements in couple functioning compared to control participants (B(β) = .84(.14), se = .30, p < .01). However, post-intervention couple functioning at Wave 2 was not significantly associated with any of the child outcomes at Wave 4.
Table 3.
Summary of Analytic Models Testing ProSAAF’s Effects on Child Outcomes
| W2 | W3 | W4 | ||||||
|---|---|---|---|---|---|---|---|---|
| Couple Functioning (CF) |
Parent-Child Relations (PC) |
Conduct Problems |
Deviant Peers |
Substance Use |
Sexual Onset a |
Depressive Symptoms |
Self- Control |
|
| β (se) | β (se) | β (se) | β (se) | β (se) | OR (se) | β(se) | β(se) | |
| Model 1: ProSAAF → Child Outcomes W4 | ||||||||
| ProSAAF | --- | --- | −0.01 (.06) | −0.10 (.07) | −0.08 (.07) | 0.70 (.21) | −0.01 (.06) | 0.01 (.06) |
| Child sex b | --- | --- | −0.12 (.07) | −0.06 (.07) | −0.03 (.07) | 0.33 (.25)** | 0.15 (.06)** | −0.05 (.06) |
| Child age | --- | --- | 0.07 (.05) | 0.12 (.06) | 0.15 (.06)* | 1.58 (.12)** | 0.04 (.07) | −0.10 (.06) |
| Model 2: ProSAAF → Couple Functioning W2 (controlling for W1) → Child Outcomes W4 | ||||||||
| ProSAAF | 0.14 (.05)** | --- | −0.01 (.06) | −0.11 (.07) | −0.09 (.07) | 0.70 (.21) | −0.01 (.06) | 0.02 (.06) |
| CF W2 | --- | --- | −0.02 (.07) | 0.03 (.07) | 0.09 (.08) | 1.01 (.03) | 0.00 (.07) | −0.04 (.06) |
| Child sex b | --- | --- | −0.12 (.07) | −0.07 (.07) | −0.02 (.07) | 0.32 (.25)** | 0.15 (.06)** | −0.05 (.06) |
| Child age | --- | --- | 0.07 (.05) | 0.10 (.06) | 0.16 (.07)* | 1.55 (.11)** | 0.04 (.07) | −0.09 (.06) |
| CF W1 | 0.55 (.04)** | --- | --- | --- | --- | --- | --- | --- |
| Model 3: ProSAAF → Couple Functioning W2 (controlling for W1) → Parent-Child Relations W3 → Outcomes W4 | ||||||||
| ProSAAF | 0.14 (.05)** | 0.02 (.06) | −0.00 (.06) | −0.10 (.07) | −0.07 (.07) | 0.72 (.21) | −0.01 (.06) | 0.01 (.06) |
| CF W2 | --- | 0.19 (.06)** | --- | --- | --- | --- | --- | --- |
| PC W3 | --- | --- | −0.16 (.06)** | −0.13 (.05)* | −0.11 (.05)* | 0.97 (.03)* | −0.08 (.05) | 0.13 (.05)** |
| Child sex b | --- | --- | −0.12 (.07) | −0.07 (.06) | −0.02 (.07) | 0.32 (.25)** | 0.15 (.06)** | −0.05 (.06) |
| Child age | --- | --- | 0.07 (.05) | 0.10 (.06) | 0.16 (.07)* | 1.05 (.11)** | 0.04 (.07) | −0.09 (.06) |
| CF W1 | 0.56 (.04)** | --- | --- | --- | --- | --- | --- | --- |
Notes. Standardized coefficients.
p < .05 (two-tailed).
p < .01 (two-tailed). Significant effects are shown in bold.
0 = No. 1 = Yes.
0 = Male. 1= Female. CF = Couple Functioning. PC = Parent-Child Relations. OR = Odds Ratio. W1 = Wave 1. W2 = Wave 2. W3 = Wave 3. W4 = Wave 4.
Model 3 introduced parent-child relations at Wave 3 to test the full conceptual model (see Figure 2). In addition to the aforementioned positive effect of ProSAAF on changes in couple functioning, results from this model indicated that higher levels of post-intervention couple functioning at Wave 2 predicted more positive parent-child relations at Wave 3 (B(β) = .46(.19), se = .14, p < .01). In turn, Wave 3 parent-child relations predicted a wide range of child outcomes at Wave 4, with more positive parent-child relations predicting lower levels of youths’ conduct problems (B(β) = −.03(−.16), se = 01., p = .01), deviant peer affiliation (B(β) = −.07(−.13), se = .03, p = .02), substance use (B(β) = −.02(−.11), se = 01., p = .02), lower likelihood of sexual onset (Odds Ratio = .97, se = .14, p = .042), and higher levels of youth self-control (B(β) = .10(.13), se = .04, p < .01). Parent-child relations were not significantly associated with youth depressive symptoms (B(β) = −.09(−.08), se = .06, p = .15). Building on these results, indirect effect (IE) analyses indicated significant IEs linking ProSAAF participation to lower levels of conduct problems (standardized [std] IE = −.004, 95% CI [−.012,−.001]), lower levels of deviant peer affiliation (std IE = −.003, 95% CI [−.011,−.001]), lower levels of substance use (std IE = −.003, 95% CI [−.010,−.001]), lower likelihood of sexual onset (std IE = −.004, 95% CI [−.015, −.001]), and higher levels of self-control (std IE = .004, 95% CI [.001,.011]) through the intervening pathways of positive changes in couple functioning and more positive parent-child relations.
Figure 2. Indirect Effects Linking ProSAAF to Child Outcomes.
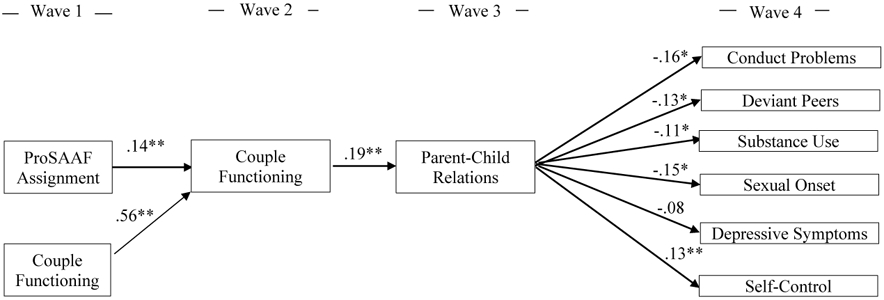
Notes. Standardized coefficients. Pathways from control variables of child age and sex to child outcomes, as well ProSAAF effects on Wave 3 and Wave 4 outcomes, were included in the model but are not shown in the figure for clarity. *p < .05. **p < .01.
Discussion
Couple-focused preventive interventions are being widely disseminated in the hopes of bettering children’s long-term outcomes (Carter, 2018), but little research has examined whether these programs achieve their intended effects on youth either directly or indirectly through their theorized effects on couple and family functioning. These data from African American families participating in the ProSAAF program show that this couple-focused program yields small positive indirect effects on several youth outcomes through the intervening processes of promoting improvements in couple functioning and better parent-child-relations. These results are consistent with the conceptual model underlying ProSAAF and with longstanding systemic theories regarding linkages between couple functioning, parenting, and child outcomes (e.g., Conger et al., 1992).
These findings provide cause for cautious optimism regarding the possible benefits of couple-focused programming on children’s outcomes. By evaluating a mediational model drawing from systemic theory, the study provides a roadmap for how couple-focused programming can ultimately benefit children: by improving their parents’ romantic relationship and in turn parent-child relationships. This mediational framework has guided intervention efforts in this area (e.g. Knox & Fein, 2008) but has rarely been tested in the context of couples’ interventions (Cowan & Cowan, 2014, 2019). Our study did so using multi-wave, multi-reporter data among an ethnic minority, low-income population similar to that being included in recent federal initiatives (e.g., Hsueh et al., 2012), strengthening our conclusions. Further highlighting the promise of this couple-focused approach, these patterns were robust across five of the six child-reported outcomes (i.e., conduct problems, deviant peer affiliation, substance use, sexual onset, self-control) more than 2 years after initial randomization. At the same time, the results also reveal some limits of ProSAAF’s benefits on youth, as there were no significant direct effects on child outcomes or significant indirect effects through couple functioning alone. These non-significant findings suggest that although there is evidence for the underlying systemic theory, the spillover from one level of the model to the next is not sufficiently great, nor the intervention effects sufficiently strong, to produce reliable effects on child outcomes if all pathways from the full conceptual model are not considered. Moreover, the significant indirect effects we did find were small, underscoring the need for caution before drawing the conclusion that programs yielding benefits for couples will necessarily yield substantial benefits for youth.
These findings suggest that there are two primary avenues through which future couple-focused interventions may yield stronger effects on participating couples’ children. First, these programs must do more to strengthen linkages across domains (couple to parent-child relations to youth). One way of doing so is through more of a focus on content that educates parents on the spillover effects of couple relationship functioning, parent-child relations, and child outcomes and instructs families on how to foster positive spillover across these domains. Program material could also be refined to include more of a focus on content that is broadly applicable to the entire family system, rather than solely addressing specific subsystems like the couple or the parent-child relationship. Doing so could enhance cohesion in the family as a whole and increase the likelihood that functioning in one domain affects functioning in another, which in turn would lead to stronger overall intervention effects.
Second, these programs may need to include more content focused specifically on the parent-child relationship, given that functioning in this domain – but not couple functioning – was significantly associated with youth outcomes. In ProSAAF, roughly half of each session was devoted to the couple’s relationship, a quarter of each session was devoted to parenting/coparenting, and the remaining time was evenly split between a youth activity and an activity focused on the family as a whole. Adjustments to the relative balance of time on each topic may lead to stronger intervention effects on downstream parent-child relations (which were not significant in the current investigation), which would lead to stronger overall effects on youth. In adopting this approach, however, it will be important to ensure that enough couple-focused content remains so that the program still yields the intended effects on couple-level outcomes. Achieving the correct balance between couple- and parent-child-focused program material will be a critical issue for the next generation of family-centered prevention programming designed to promote long-term positive youth development, as results from this study and others (e.g., Cowan, Cowan, & Barry, 2011) indicate that improving child outcomes will require programs to reduce the siloed approach to families that has characterized many prevention efforts to date (Cowan & Cowan, 2019).
Limitations and Future Directions
Despite the many strengths of the study, it is important to acknowledge some limitations. First, this study involved 346 African American couples and their pre-adolescent child. As such, it cannot speak to whether these results would generalize to other demographic groups or to children at different developmental stages. Conducting indirect effect analyses using data from existing studies and planning for such analyses in future studies will allow for important tests of the robustness of these effects and provide conceptual clarity regarding the conditions under which children’s outcomes are most strongly tied to couple functioning and/or the parent-child relationship. Second, our analytic model only included parent-child relations at Wave 3 and child outcomes at Wave 4; our parent-child relations measure was not administered earlier in the study and several of the youth outcomes were not developmentally appropriate at earlier ages. Accordingly, our model represents later functioning in these domains, not change over time. Future research using measures of these constructs at earlier waves (as appropriate) will allow for tests of whether changes in one domain lead to changes in another and expand on the analyses described here. Relatedly, we note that although this analytic approach had the advantage of allowing us to examine how couple functioning and parent-child relationship preceded youth outcomes (which was the central question), it does not allow us to examine how they covary with youth outcomes at the same time point (Wave 4). Third, although the youth outcomes and the couple and parent-child outcomes were collected from different reporters (youth self-report for youth outcomes; couple report for couple and parent-child outcomes), all measures were self-report. Observational data of couple and family interactions and ratings of outcomes by independent evaluators (e.g., teacher ratings of youth outcomes) would provide another useful lens into family and youth functioning. Fourth, although we considered a broad set of six child outcomes that were only moderately correlated, there are several other youth outcomes that we did not assess that are also influenced by couple dynamics, including children’s own romantic relationships (e.g., Bryant & Conger, 2002) and children’s physical health (e.g., Troxel & Matthews, 2004). Future research examining indirect effects in these domains, particularly as youth transition into later adolescence and early adulthood, could highlight other clinically meaningful outcomes. Fifth, the control group did not receive the personalized attention that the intervention group received, raising the possibility that non-specific factors (including participants’ expectations of benefit) could have contributed to the changes observed in the ProSAAF participants. Lastly, like most CRE programs, the intervention design does not allow for dismantling of which intervention components contributed to its effectiveness. Further, because our analyses focused on global assessments of couple functioning and of parent-child relationship quality, they cannot speak to specific processes that prove most important. We note, however, that similar results were found when we analyzed specific aspects of couple functioning such as effective communication and relationship satisfaction (see Supplemental Table S2), indicating that the results observed here were not driven by a specific couple process but rather by overall improvements in the couple subsystem. Nonetheless, future research examining which processes link couple functioning with better parent-child relationship quality and better parent-child relationship quality with better youth outcomes would be valuable.
Notwithstanding these limitations, results from this four-wave, multi-year trial indicate that the ProSAAF intervention yields small positive indirect effects on child outcomes through improvements in couples’ functioning and in turn better parent-child relations. The findings represent an important practical and conceptual advance in demonstrating that couple-focused programming can benefit children’s long-term outcomes and in providing experimental evidence for the systemic model underlying this approach. Future research examining direct and indirect effects of couple-focused programs on child outcomes among diverse populations at different development stages is needed, as is research examining even longer-term effects of these programs on children’s health, well-being, and social functioning as they transition into adolescence and early adulthood.
Supplementary Material
Public Health Significance:
This study demonstrates that a couple-focused prevention program improves couple functioning and in turn promotes better parent-child relations and child psychosocial functioning two years after enrollment. These findings are important in suggesting that couple-focused programming can yield small benefits for children’s long-term outcomes when they enhance couple and parent-child relationships.
Author Acknowledgment:
This research was supported by award R01 AG059260 funded by the National Institute on Aging and R01 HD069439 funded by the National Institute of Child Health and Human Development to Steven R. H. Beach, and by award P30 DA027827 to Gene H. Brody funded by the National Institute on Drug Abuse. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors thank the families for their willingness to participate in this research and the staff at the Center for Family Research for their assistance implementing this study.
Footnotes
Eligibility guidelines required the target child to be African American, but not both parents. Racial and ethnicity information was not assessed in surveys completed by participants. Notes from research staff indicated that two caregivers (from different families) were not African American. All participants were comfortable being identified as part of an African American family.
The pattern of results for the final indirect effect analyses was the same for the composite and for each of the four couple functioning variables when examined independently (see Supplemental Table S2).
Correlations between partners’ relationship functioning scores: raverage = .28 (range of .11 < r < .41), p < .05, across measures at W1 and W2. Correlations between partners’ parent-child relations scores at W3: r = .15, p = .05.
References
- Acock AC (1999). Quantitative methodology for studying families. In Sussman MB, Steinmetz SK, & Peterson GW (Eds.), Handbook of Marriage and the Family (pp. 263–289). Boston, MA: Springer. [Google Scholar]
- Barton AW, Beach SRH, Hurt TR, Fincham FD, Stanley SM, Kogan SM, & Brody GH (2016). Determinants and long-term effects of attendance levels in a marital enrichment program for African American couples. Journal of Marital and Family Therapy, 42, 272–287. 10.1111/jmft.12126 [DOI] [PubMed] [Google Scholar]
- Barton AW, Beach SRH, Wells AC, Ingels JB, Corso PS, Sperr MC,…Brody GH (2018). The Protecting Strong African American Families Program: A randomized controlled trial with rural African American couples. Prevention Science, 19, 904–913. 10.1007/s11121-018-0895-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brody GH, & Ge X (2001). Linking parenting processes and self-regulation to psychological functioning and alcohol use during early adolescence. Journal of Family Psychology, 15, 82–94. 10.1037/0893-3200.15.1.82 [DOI] [PubMed] [Google Scholar]
- Brown SL (2010). Marriage and child well-being: Research and policy perspectives. Journal of Marriage and Family, 72, 1059–1077. 10.1111/j.1741-3737.2010.00750.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bryant CM, & Conger RD (2002). An intergenerational model of romantic relationship development. In Vangelisti AL, Reis HT, & Fitzpatrick MA (Eds.), Stability and Change in Relationships. (pp. 57–82). New York, NY: Cambridge University Press. 10.1017/CBO9780511499876.005 [DOI] [Google Scholar]
- Burman B, John RS, & Margolin G (1987). Effects of marital and parent-child relations on children’s adjustment. Journal of Family Psychology, 1, 91–108. 10.1037/h0080439 [DOI] [Google Scholar]
- Carter CH (2018). Healthy marriage and relationship education: Strengthening family bonds and increasing economic independence. Retrieved from https://www.hhs.gov/blog/2018/08/23/healthy-marriage-and-relationship-education.html [Google Scholar]
- Casey P, Cowan PA, Cowan CP, Draper L, Mwamba N, & Hewison D (2017). Parents as partners: A UK trial of a US couples-based parenting intervention for at-risk low-income families. Family Process, 56, 589–606. 10.1111/famp.12289 [DOI] [PubMed] [Google Scholar]
- Conger RD, Conger KJ, Elder GH Jr, Lorenz FO, Simons RL, & Whitbeck LB (1992). A family process model of economic hardship and adjustment of early adolescent boys. Child Development, 63, 526–541. 10.1111/j.1467-8624.1992.tb01644.x [DOI] [PubMed] [Google Scholar]
- Cowan PA, & Cowan CP (2014). Controversies in couple relationship education (CRE): Overlooked evidence and implications for research and policy. Psychology, Public Policy, and Law, 20, 361–383. 10.1037/law0000025 [DOI] [Google Scholar]
- Cowan CP, & Cowan PA (2019). Enhancing parenting effectiveness, fathers' involvement, couple relationship quality, and children's development: Breaking down silos in family policy making and service delivery. Journal of Family Theory & Review, 11, 92–111. 10.1111/jftr.12301 [DOI] [Google Scholar]
- Cowan CP, Cowan PA, & Barry J (2011). Couples' groups for parents of preschoolers: Ten-year outcomes of a randomized trial. Journal of Family Psychology, 25, 240–250. 10.1037/a0023003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cowan CP, Cowan PA, & Heming G (2005). Two variations of a preventive intervention for couples: effects on parents and children during the transition to elementary school. In Cowan PA, Cowan CP, Ablow J, Johnson VK & Measelle J (Eds.), The family context of parenting in children's adaptation to elementary school (pp. 277–312). Mahwah, NJ: Lawrence Erlbaum Associates. [Google Scholar]
- Culp LN, & Beach SRH (1998). Marriage and depressive symptoms. Psychology of Women Quarterly, 22, 647–663. 10.1111/j.1471-6402.1998.tb00183.x [DOI] [Google Scholar]
- Cummings EM, & Davies PT (2002). Effects of marital conflict on children: Recent advances and emerging themes in process-oriented research. Journal of Child Psychology and Psychiatry, 43, 31–63. 10.1111/1469-7610.00003 [DOI] [PubMed] [Google Scholar]
- Davies PT, & Cummings EM (1994). Marital conflict and child adjustment: An emotional security hypothesis. Psychological Bulletin, 116, 387–411. 10.1037/0033-2909.116.3.387 [DOI] [PubMed] [Google Scholar]
- DeNavas-Walt C, & Proctor BD (2014). Income and poverty in the United States: 2013 (Current Population Reports P60-249). Washington, DC: U.S. Census Bureau. [Google Scholar]
- Doss BD, Roddy MK, Llabre MM, Georgia Salivar E, & Jensen-Doss A (2019). Improvements in coparenting conflict and child adjustment following an online program for relationship distress. Journal of Family Psychology. Advance online publication. 10.1037/fam0000582 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elliott DS, & Ageton SS (1980). Reconciling race and class differences in self-reported and official estimates of delinquency. American Sociological Review, 45, 95–110. 10.2307/2095245 [DOI] [Google Scholar]
- Elliott DS, Ageton SS, Huizinga D (1985). Explaining delinquency and drug use. Beverly Hills, CA: Sage. [Google Scholar]
- Fauber R, Forehand R, Thomas AM, & Wierson M (1990). A mediational model of the impact of marital conflict on adolescent adjustment in intact and divorced families: The role of disrupted parenting. Child Development, 61, 1112–1123. 10.1111/j.1467-8624.1990.tb02845.x [DOI] [PubMed] [Google Scholar]
- Feinberg ME, & Jones DE (2018). Experimental support for a family systems approach to child development: Multiple mediators of intervention effects across the transition to parenthood. Couple and Family Psychology: Research and Practice, 7, 63–75. 10.1037/cfp0000100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fincham FD, Ajayi C, & Beach SR (2011). Spirituality and marital satisfaction in African American couples. Psychology of Religion and Spirituality, 3, 259–268. 10.1037/a0023909 [DOI] [Google Scholar]
- Grych JH, & Fincham FD (1990). Marital conflict and children's adjustment: A cognitive-contextual framework. Psychological Bulletin, 108, 267–290. 10.1037/0033-2909.108.2.267 [DOI] [PubMed] [Google Scholar]
- Gupta SK (2011). Intention-to-treat concept: A review. Perspectives in Clinical Research, 2, 109–112. doi: 10.4103/2229-3485.83221 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hawkins AJ, Blanchard VL, Baldwin SA, & Fawcett EB (2008). Does marriage and relationship education work? A meta-analytic study. Journal of Consulting and Clinical Psychology, 76, 723–734. 10.1037/a0012584 [DOI] [PubMed] [Google Scholar]
- Hayes AF (2009). Beyond Baron and Kenny: Statistical mediation analysis in the new millennium. Communication Monographs, 76, 408–420. 10.1080/03637750903310360 [DOI] [Google Scholar]
- Hayes AF (2012). PROCESS: A versatile computational tool for observed variable mediation, moderation, and conditional process modeling. Retrieved from http://www.afhayes.com/public/process2012.pdf [Google Scholar]
- Hayes AF, Preacher KJ, & Myers TA (2011). Mediation and the estimation of indirect effects in political communication research. In Bucy EP and Holbert RL (Eds). Sourcebook for political communication research: Methods, measures, and analytical techniques (pp. 434–465). New York, NY: Routledge. [Google Scholar]
- Hsueh J, Alderson DP, Lundquist E, Michalopoulos C, Gubits D, Fein D, & Knox V (2012). The Supporting Healthy Marriage Evaluation: Early impacts on low-income families. OPRE Report 2012-11. Washington, DC: Office of Planning, Research and Evaluation, Administration for Children and Families, U.S. Department of Health and Human Services. [Google Scholar]
- Jenkins NH, & Saiz CC (1995). The Communication Skills Test. Unpublished manuscript, University of Denver. Denver, CO. [Google Scholar]
- Johnston LD, O'Malley PM, Bachman JG, & Schulenberg JE (2007). Monitoring the Future national survey results on drug use, 1975-2006. Volume I: Secondary school students (NIH Publication No. 07-6205). Bethesda, MD: National Institute on Drug Abuse. [Google Scholar]
- Jones DE, Feinberg ME, Hostetler ML, Roettger ME, Paul IM, & Ehrenthal DB (2018). Family and child outcomes 2 years after a transition to parenthood intervention. Family Relations, 67, 270–286. 10.1111/fare.12309 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones DJ, Forehand R, Rakow A, Colletti CJ, McKee L, & Zalot A (2008). The specificity of maternal parenting behavior and child adjustment difficulties: A study of inner-city African American families. Journal of Family Psychology, 22, 181–192. 10.1037/0893-3200.22.2.181 [DOI] [PubMed] [Google Scholar]
- Kendall P, & Wilcox L (1979). Self-control in children: Development of a rating scale. Journal of Consulting & Clinical Psychology, 47, 1020–1029. 10.1037/0022-006X.47.6.1020 [DOI] [PubMed] [Google Scholar]
- Knox V, & Fein D (2008). Designing a marriage education demonstration and evaluation for low-income married couples. Retrieved from https://www.mdrc.org/publication/designing-marriage-education-demonstration-and-evaluation-low-income-married-couples [Google Scholar]
- Kogan SM, Yu T, Allen KA, Pocock AM, & Brody GH (2015). Pathways from racial discrimination to multiple sexual partners among male African American adolescents. Psychology of Men & Masculinity, 16, 218–228. 10.1037/a0037453 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kumpfer KL, Molgaard V, & Spoth R (1996). The Strengthening Families Program for the prevention of delinquency and drug use. In Peters RD & McMahon RJ (Eds.), Banff international behavioral science series, Vol. 3. Preventing childhood disorders, substance abuse, and delinquency (p. 241–267). Sage Publications, Inc. [Google Scholar]
- Lavner JA, Barton AW, & Beach SRH (2019). Improving couples’ relationship functioning leads to improved coparenting: A randomized controlled trial with rural African American couples. Behavior Therapy, 50, 1016–1029. doi: 10.1016/j.beth.2018.12.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon DP, & Fairchild AJ (2009). Current directions in mediation analysis. Current Directions in Psychological Science, 18, 16–20. 10.1111/j.1467-8721.2009.01598.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Markman HJ, Stanley SM, Blumberg S, Jenkins NH, & Whaley C (2004). Twelve Hours to a Great Marriage. San Francisco: Jossey-Bass. [Google Scholar]
- Marsh HW, Hau K-T, & Wen Z (2004). In search of golden rules: Comment on hypothesis-testing approaches to setting cutoff values for fit indexes and dangers in overgeneralizing Hu and Bentler's (1999) findings. Structural Equation Modeling: A Multidisciplinary Journal, 11, 320–341. 10.1207/s15328007sem1103_2 [DOI] [Google Scholar]
- Muthén LK, & Muthén BO (1998–2015). Mplus User's Guide (7th ed.). Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Newcomb MD, & Bentler PM (1988). Impact of adolescent drug use and social support on problems of young adults: a longitudinal study. Journal of Abnormal Psychology, 97, 64–75. 10.1037/0021-843X.97.1.64 [DOI] [PubMed] [Google Scholar]
- Norton R (1983). Measuring marital quality: A critical look at the dependent variable. Journal of Marriage and Family, 45, 141–151. 10.2307/351302 [DOI] [Google Scholar]
- Owen J, Quirk K, Bergen C, Inch LJ, & France T (2012). The effectiveness of PREP with lower-income racial/ethnic minority couples. Journal of Marital and Family Therapy, 38, 296–307. 10.1111/j.1752-0606.2012.00294.X [DOI] [PubMed] [Google Scholar]
- Prinz RJ, Foster S, Kent RN, & O’Leary KD (1979). Multivariate assessment of conflict in distressed and nondistressed mother–adolescent dyads. Journal of Applied Behavior Analysis, 12, 691–700. 10.1901/jaba.1979.12-691 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pruett MK, Cowan PA, Cowan CP, Gillette P, & Pruett KD (2019). Supporting father involvement: An intervention with community and child welfare–referred couples. Family Relations, 68, 51–67. 10.1111/fare.12352 [DOI] [Google Scholar]
- Radloff LS (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1, 385–401. 10.1177/014662167700100306 [DOI] [Google Scholar]
- Stanley SM, Hoyer L, & Trathen DW (1994). The Confidence Scale. Unpublished manuscript. University of Denver. Denver, CO. [Google Scholar]
- Stanley SM, Blumberg S, & Markman HJ (1999). Helping couples fight for their marriages: The PREP approach. In Berger R & Hannah M (Eds.), Handbook of preventive approaches in couple therapy (pp. 279–303). New York: Brunner/Mazel. [Google Scholar]
- Stanley SM, Markman HJ, Prado LM, Olmos-Gallo PA, Tonelli L, St. Peters M, et al. (2001). Community-based premarital prevention: Clergy and lay leaders on the front lines. Family Relations, 50, 67–76. 10.1111/j.1741-3729.2001.00067.x [DOI] [Google Scholar]
- Troxel WM, & Matthews KA (2004). What are the costs of marital conflict and dissolution to children's physical health? Clinical Child and Family Psychology Review, 7, 29–57. 10.1023/B:CCFP.0000020191.73542.b0 [DOI] [PubMed] [Google Scholar]
- Whitton SW, Rhoades GK, & Whisman MA (2014). Fluctuation in relationship quality over time and individual well-being: Main, mediated, and moderated effects. Personality and Social Psychology Bulletin, 40, 858–871. 10.1177/0146167214528988 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zemp M, Bodenmann G, & Cummings EM (2016). The significance of interparental conflict for children. European Psychologist, 21, 99–108. 10.1027/1016-9040/a000245 [DOI] [Google Scholar]
- Zemp M, Milek A, Cummings EM, Cina A, & Bodenmann G (2016). How couple-and parenting-focused programs affect child behavioral problems: A randomized controlled trial. Journal of Child and Family Studies, 25, 798–810. 10.1007/s10826015-0260-1 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.