

Abstract
Background:
Diabetes is the fifth leading cause of death in the world, which reduces the patients' quality of life (QOL) and is considered as an important subject especially in medicine and medical community. The present study aimed at investigating the QOL of diabetic patients in Iran through meta-analysis.
Methods:
The search was conducted using relevant keywords in national and international databases including Iranmedex, SID, Magiran, IranDoc, Medlib, Science Direct, PubMed, Scopus, Cochrane, Embase, Web of Science. Questionnaires WHOQOL, SF-36, SF-20, DQOL, QOL, PedsQL, ADDQOL, D-39, DQOL-BCI, SWED-QUAL, IRDQOL, PHG-2, EQ-5D, and IDQOL-BCI were used to assess the QOL. Heterogeneity of studies was assessed using I2 index. Data were analyzed using STATA version 11.
Results:
In 96 studies of 17,994 people, the mean score of QOL in diabetic patients was based on the questionnaires WHOQOL [66.55 (95% CI: 45.83, 87.26)], D-39 [129.43 (95%CI: 88.77, 170.10)], SF-36 [65.64 (95% CI: 59.82, 71.46)], SF-20 [46.50 (95% CI: 37.19, 55.81], DQOL [61.19 (95% CI: 35.73, 86.66)], QOL [117.91 (95% CI: -62.97, 298.79)], PedsQL [34.36 (95% CI: -31.49, 100.22)], ADDQOL [41.76 (95% CI: 12.01-71.50)], SWED-QUAL [59.19 (95% CI: 21.15, 97.23)], IRDQOL [105.92 (95% CI: 102.73, 109.10)], PHG-2 [61.00 (95%CI: 59.63, 62.37)], EQ-5D [0.62 (95% CI: 0.61, 0.64)], DQOL-BCI [3.40 (95% CI: 3.31, 3.49)], and IDQOL-BCI [22.63 (95% CI: -2.38, 47.64)].
Conclusions:
The QOL of diabetic patients was evaluated according to different types of questionnaires and the QOL of diabetic patients was found to be lower than normal population.
Keywords: Diabetes, meta-analysis, quality of life, systematic review
Introduction
World Health Organization defines quality of life (QOL) as an individuals' understanding of living condition in terms of culture and the prevailing community values following their goals, expectations, standards, and interests. Hence, QOL is closely related to physical, psychological, and mental condition, personal beliefs, level of self-reliance, mass communication, and environment.[1,2,3,4,5,6] One reason for the multidimensional complexity of QOL is that it includes different aspects of an individual's life. Another reason is that each individual has his/her own unique characteristics and his/her perception of a good or poor QOL is unique to that person.[1,2,3,4,5,6,7,8,9] The subject of QOL is important since it may lead to frustration, lack of motivation for any attempt and reduction of social, economic, cultural, and health activities. QOL influences the socioeconomic development of a country in deeper dimensions. Modifying the QOL is considered as a part of disease control program.[7,8,9]
Diabetes is known as a “silent epidemic” and is considered a major public health problem in the United States and other parts of the world, including Iran. It is the most prevalent metabolic disease with an increasing incidence, which shortens life expectancy by one third[10,11,12] and affects various aspects of a patient's life, including psychological, physical, social, and economic condition, family life and sexual function.[13,14,15,16] Type 1 and type 2 diabetes are two major forms of this disease and include about 10--90% of the diabetes population, respectively.[17]
According to the latest available data, about 171 million people suffer from diabetes worldwide. Asia is one of the regions with a high prevalence of diabetes.[18] Two percent of the Iranian population are suffering from the disease.[19] Due to the large proportion of diabetic patients in Iran and the direct impact of diabetes on the QOL of patients with diabetes, the present study aims to evaluate the QOL in diabetic patients in Iran. Considering that a meta-analysis study of the same title was published in 2016[20] and evaluated only two questionnaires (SF-20 and SF-36). Also the previous meta-analysis included only the results of 10 studies. The present meta-analysis was performed with the aim of updating the previous study and without considering the time limit, limiting the type of questionnaire and covering all studies published in this field. In the present meta-analysis, the QOL of diabetic patients was evaluated in the form of levels: Good, Moderate, and Poor. This issue was not presented in previous meta-analysis.
Methods
Search strategy
This is a systematic review and meta-analysis aimed at investigating the QOL of diabetic patients in Iran. In order to achieve the related documentation in Persian and English, two researchers independently searched both national and international databases, including Iranmedex, SID, Magiran, Iran-Doc, Med-Lib, Science-Direct, PubMed, Scopus, Cochrane, Embase, Web of Science, and Medline using related Persian keywords and their English equivalents: “Iran,” “meta-analysis,” “diabetes,” and “quality of life,” The keywords were searched using AND/OR operators. The search was performed without time limit until 22.04.2020. However, the articles in question were published between 2003 and 2020. The previous meta-analysis article published in this field belonged to 2016[20] and only examined the SF-20 and SF-36 questionnaires, while the current meta-analysis did not impose any restrictions on the type of questionnaires used in the reviewed articles. For this reason, various questionnaires such as: WHOQOL, SF-36, SF-20, DQOL, PedsQL, ADDQOL, D-39, DQOL-BCI, SWED-QUAL, and IRDQOL were evaluated. In cases of lack of access to the article's full text, the researchers asked the corresponding author for the full-text articles via email. To complete the search, Google Scholar was also searched.
Inclusion and exclusion criteria
Inclusion criteria included mentioning the QOL of diabetic patients in Iran in Persian and English. Exclusion criteria included non-random sampling, inadequate information in the article's text, and population other than diabetic patients.
Study selection
In the first phase of the search, 501 articles related to QOL of diabetic patients were found. After reviewing the titles, 289 duplicate and overlapping articles were excluded. Abstracts of all remaining articles were reviewed and 59 irrelevant articles were excluded. The full text of the remaining articles was reviewed then 57 studies were excluded due to having the exclusion criteria. Finally, 96 articles entered the qualitative evaluation stage.[Chart 1]
Chart 1.
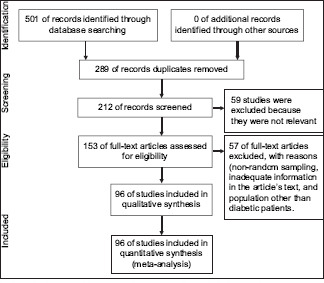
Flowchart of the entrance of studies into the systematic review and meta-analysis
Qualitative evaluation of studies
To check the quality of studies, the STROBE checklist (strengthening the reporting of observational studies in epidemiology)[21] was applied. This checklist includes 22 items that cover different parts of a report (sampling, measuring variables, objectives of the study, and statistical analysis). Each item was given one point and higher points were given to other items that we considered more important. In this phase, four unqualified articles were excluded and finally 96 articles entered the meta-analysis stage.
Data extraction
To reduce bias in reporting and error in data collection, two researchers independently extracted data from articles and entered the data into a checklist, which included the following items: The first author's name, title of study, sample size, year of publication, city of study, diabetes type, questionnaire title, the subjects' average age, mean and standard deviation of the QOL of diabetic patients, mean and standard deviation of quality of life dimensions, etc.
Statistical analysis
Considering that the QOL in diabetic patients score and its subgroups score were quantitative, the mean and standard deviation of these indices were extracted in each study and the variance of the mean was calculated using normal distribution. Considering the heterogeneity of the studies, a random effects model was used to combine the results of the studies. The I2 index was used to investigate the heterogeneity of the studies. A random effects meta-analysis was used to give a pooled estimate of prevalence of QOL for each measure. Metaregression was used to check heterogeneity among the studies and to find any association between the year of publication and the sample size with QOL in diabetic patients. Subgroup analysis was done according to sex, components, and questionnaire. All statistical analyses were performed using STATA ver 14. The significance level of the tests was considered to be P < 0.05.
Results
In 96 reviewed studies with a sample of 17,994, the mean QOL score in diabetic patients was based on WHO Quality of Life-BREF (WHOQOL-BREF) [66.55 (95% CI: 45.83, 87.26)], D-39 [129.43 (95% CI: 88.77, 170.10)], Short Form-36 (SF-36) [65.64 (95% CI: 59.82, 71.46)], Short Form-20 (SF-20) [46.50 (95% CI: 37.19, 55.81)], Diabetes Quality of Life (DQOL) [61.19 (95% CI: 35.73, 86.66)], Quality of Life [QOL) (117.91 (95% CI: -62.97, 298.79)], PedsQL [34.36 (95% CI: -31.49, 100.22)], Audit of Diabetes Dependent Quality of Life (ADDQOL) [41.76 (95% CI: 12.01-71.50)], SWED-QUAL [59.19 (95% CI: 21.15, 97.23)], IRDQOL [105.92 (95% CI: 102.73, 109.10)], PHG-2 [61.00 (95% CI: 59.63, 62.37)], EQ-5D [0.62 (95% CI: 0.61, 0.64)], DQOL-BCI [3.40 (95% CI: 3.31, 3.49)], and Iranian version of the Diabetes Quality of Life Brief Clinical Inventory (IDQOL-BCI) [22.63 (95% CI: -2.38, 47.64)]. Considering the heterogeneity between the studies, the confidence interval for each study based on random-effects model is shown in Table 1.
Table 1.
Specifications of reviewed articles on the status of the quality of life of diabetic patients in Iran
| ID | Author | Year of publication | City of study | Type of diabet | Sample size | Age mean | Questionnaire | Mean score of QOL | SD of QOL |
|---|---|---|---|---|---|---|---|---|---|
| [22] | Aghamolaei T | 2003 | Hormozgan | type 2 | 80 | 32-72 | WHOQOL-BREF | ||
| [23] | Aghamolaei T | 2005 | Hormozgan | type 2 | 71 | 51.3 | WHOQOL-BREF | ||
| [24] | Sadeghie Ahari S | 2008 | Ardebil | type 2 | 110 | 52.5 | SF-36 | ||
| [25] | Ahmadi A | 2011 | Chaharmahal& Bakhtiari | type 2 | 254 | 30-65 | Developed by reserch team | ||
| [26] | Alavi A | 2010 | Chaharmahal& Bakhtiari | type 1 | 22 | 15.33 | PedsQL | 0.78 | 0.48 |
| [27] | Baghianimoghadam MH | 2008 | Yazd | type 2 | 120 | 25-75 | SF-20 | 51.03 | 17.04 |
| [28] | Bazzazian S | 2010 | Tehran | type 1 | 300 | 18-30 | D-39 | 109.47 | 45.31 |
| [29] | Borzou SR | 2010 | Hamedan | type 2 | 165 | SF-36 | |||
| [30] | Safarabadi-Farahani T | 2010 | Tehran | type 1 | 70 | 14.94 | DQOL for youth | 56.28 | 12.2 |
| [31] | Ghanbari A | 2004 | Guilan | type 2 | 90 | >40 | SWED-QUAL | 18.37 | 12.5 |
| [32] | Ghanbari A | 2005 | East-Azerbaijan | type 2 | 117 | >35 | SWED-QUAL | 28 | 8.1 |
| [33] | Haririan HR | 2009 | East-Azerbaijan | type 2 | 150 | 20-60 | SWED-QUAL | ||
| [34] | Heydari M | 2007 | Zanjan | type 1 | 47 | 11-20. | Developed by reserch team | 106.65 | 45.75 |
| [35] | Jafari P | 2011 | Fars | type 1 | 94 | 8-.18 | PedsQL | 67.98 | 14.03 |
| [36] | Ghavami H | 2005 | west-Azerbaijan | type 2 | 74 | 40-65 | Developed by reserch team | 98 | |
| [37] | Shahab-Jahanlou AR | 2011 | Hormozgan | type 2 | 256 | 27-72 | WHOQOL-BREF26 | ||
| [38] | Shahab-Jahanlou AR | 2011 | Hormozgan | typ1& type 2 | 76 | 49.15 | IRDQOL | ||
| [1] | Darvishpour-Kakhaki A | 2005 | Tehran | typ1& type 2 | 131 | 47.3 | SF-36 | ||
| [39] | Sedaghati-Kasbakhi M | 2008 | Mazandaran | type 2 | 70 | SWED-QUAL | 131.72 | 25.88 | |
| [40] | Kermansaravi F | 2012 | Sistan and Baluchestan | type 1 | 100 | 14.6 | DQOL for youth | 52.65 | 14.58 |
| [41] | Khaledi S | 2011 | Kurdestan | type 2 | 198 | >18 | SF-36 | 70.82 | 18.97 |
| [42] | Khamseh MA | 2011 | Tehran | type 1 | 150 | 22.14 | Developed by reserch team | 69.01 | 13.03 |
| [43] | Peymani M | 2007 | Tehran | typ 1 and type 2 | 302 | >18 | Developed by reserch team | ||
| [44] | Rakhshanderu S | 2006 | Tehran | type 2 | 40 | 40-65 | DQOL | 35.2 | 9.1 |
| [45] | Rasouli D | 2011 | Tehran | patients with deiabetic foot ulcer | 120 | 54.23 | DFS | ||
| [46] | Safavi M | 2011 | Ardebil | type 2 | 123 | 30-70 | QOL | 234.27 | 5.18 |
| [47] | Sanjari M | 2011 | Kerman | typ 1 and type 2 | 132 | 52.98 | SF-36 | 314.18 | 138.24 |
| [48] | Shahrjerdi S | 2009 | Markazi | type 2 | 27 | >35 | SF-36 | 83.08 | 11.06 |
| [49] | Sayadi N | 2011 | Khuzestan | type 2 | 31 | 58.35 | SF-36 | 1775.81 | 955.4 |
| [50] | Taghdisi MH | 2011 | Golestan | type 2 | 78 | 49 | WHOQOL | 80.39 | 11.35 |
| [51] | Timareh M | 2012 | Kermanshah | typ 1 and type 2 | 350 | >18 | SF-36 | ||
| [52] | Vares Z | 2010 | Isfahan | typ 1 and type 2 | 310 | >18 | IRDQOL | 105.8 | 44.1 |
| [53] | Vazirinezhad R | 2010 | Kerman | 101 | 50.8 | SF-36 | |||
| [54] | Yekta Z | 2011 | West-Azerbaijan | type 2 | 250 | 60.73 | SF-36 | 57.52 | 17.1 |
| [38] | Shahab-Jahanlou AR | 2011 | Hormozgan | typ 1 and type 2 | 76 | 49.15 | WHOQOL | ||
| [55] | Mirfeizi M | 2012 | Karaj | 180 | 53.47 | IDQOL-BCI | 9.89 | 2.51 | |
| [56] | Shahi M | 2017 | Semnan | type 2 | 60 | 57.82 | QOL | ||
| [57] | Najafi-Ghezeljeh T | 2017 | Tehran | type 2 | 65 | 54.3 | IDQOL-BCI | 35.41 | 7.8 |
| [58] | Shamshirgaran SM | 2016 | Ardebil | type 2 | 300 | 54.13 | WHOQOL | 53.07 | 7.09 |
| [59] | Hajian-Tilaki K | 2016 | Babol | 750 | 67.85 | SF-36 | |||
| [60] | Dadgostar H | 2016 | Tehran | type 2 | 74 | 49.65 | SF-36 | ||
| [61] | Jafari N | 2014 | Isfahan | type 2 | 203 | 55.42 | PHG-2 | 61 | 9.97 |
| [62] | Abdoli S | 2015 | Malayer | type 2 | 40 | 35-85 | WHOQOL-BREF | ||
| [63] | Hadi N | 2013 | Shiraz | typ 1 and type 2 | 300 | 50.98 | SF-36 | ||
| [64] | Shavandi N | 2010 | Markazi | type 2 | 17 | 48.52 | SF-36 | 74.58 | 11.34 |
| [65] | Shayeghian Z | 2013 | Tehran | type 2 | 100 | 55.4 | ADDQoL | 26.63 | 12.01 |
| [66] | Alipour A | 2012 | Yaza | type 2 | 80 | 46.2 | ADDQoL | 56.98 | 18.63 |
| [67] | Afshar M | 2014 | Kashan | type 2 | 56 | 14.75 | IRDQOL | 106 | 15.95 |
| [68] | Derakhshanpour F | 2015 | Gorgan | type 2 | 330 | 50.6 | WHOQOL-BREF | 54.79 | 13.7 |
| [69] | Zaker MR | 2016 | Urmia | 80 | DQOL | 46.04 | 4.3 | ||
| [70] | Didarloo AR | 2016 | Khoy | type 2 | 352 | 43 | WHOQOL-BREF | 58.02 | 17.63 |
| [71] | Gholami A | 2013 | Neishabour | type 2 | 1847 | 59.65 | WHOQOL-BREF | 12.18 | 2.3 |
| [72] | Torabi M | 2014 | Hamedan | type 2 | 110 | 47.4 | SF-36 | ||
| [73] | Izadi A | 2014 | Khoram Abad | type 2 | 80 | 30-70 | SF-20 | ||
| [74] | Khodabakhsi-Kulaei A | 2015 | Tafresh | type 2 | 24 | 50.58 | WHOQOL | 68 | 11.08 |
| [75] | Mohammad-Shahi A | 2014 | Ahvaz | type 2 | 110 | 53.69 | SF-36 | ||
| [76] | Saeedpour J | 2013 | Tehran | 60 | 40 | SF-36 | 43.5 | 15.7 | |
| [4] | Masoudi-Alavi N | 2004 | Tehran | typ 1 and type 2 | 104 | 50.5 | QOL | 116.7 | 18.8 |
| [77] | Ghasemipour M | 2009 | Khoram Abad | 150 | 18-65 | QOL | 2.77 | 0.79 | |
| [78] | Eydi-Bayegi M | 2014 | Ahvaz | type 2 | 50 | 46.2 | WHOQOL-26 | 73.91 | 14.85 |
| [79] | Sadeghi T | 2012 | Rafsanjan | 70 | 18-65 | SF-36 | |||
| [80] | Zaree-Bahramabadi M | 2012 | Sanandaj | type 2 | 48 | 30-50 | SF-36 | 53.3 | 10.76 |
| [81] | Qashqaei S | 2014 | Shiraz | type 2 | 42 | 35-65 | SF-36 | 56.37 | 18.25 |
| [82] | Saadatjuo SAR | 2012 | Birjand | type 2 | 100 | 42.82 | SF-36 | 57.29 | 26.09 |
| [83] | Behrooz B | 2016 | Kermanshah | type 2 | 16 | 49.47 | WHOQOL-26 | 137.92 | 12.9 |
| [84] | Ebrahimi H | 2014 | Shahrood | type 2 | 156 | 48.11 | DQOL | 164.53 | 63.21 |
| [85] | Mohammadshahi GHR | 2016 | Taybad | type 2 | 20 | 47.75 | SF-36 | ||
| [86] | Shams S | 2015 | Urmia | 80 | SF-36 | ||||
| [87] | Mohammadpour Y | 2008 | Tabriz | type 2 | 150 | Self-made | |||
| [88] | Ganjluo J | 2015 | Sabzevar | type 2 | 75 | 35-65 | ADDQOL-19 | ||
| [89] | Bidi F | 2012 | Bojnord | type 2 | 40 | 52.17 | SF-20 | 41.52 | 16.28 |
| [90] | Derakhshanpour F | 2015 | Gorgan | type 2 | 330 | 51 | WHOQOL | ||
| [91] | Bahadori-Khosroshahi J | 2011 | Tabriz | 100 | 20-60 | WHOQOL-26 | 47.48 | 16.33 | |
| [92] | Fooladvandi M | 2014 | Kerman | type 2 | 96 | 53.08 | SF-36 | 54.21 | 15.16 |
| [93] | Shahraki-Vahed A | 2010 | Zabol | typ 1 and type 2 | 100 | >7 | SF-36 | ||
| [94] | Taghdisi MH | 2011 | Minudasht | type 2 | 78 | 49 | WHOQOL-BREF | 80.39 | 11.35 |
| [95] | Sepehrnia I | 2011 | Karaj | 30 | 40-65 | SF-36 | 53.97 | 13.09 | |
| [96] | Fathi-Ahmadsaraee N | 2016 | Karaj | type 2 | 40 | 42.83 | DQOL | 26.37 | 4.51 |
| [97] | Moein M | 2014 | Kashan | type 2 | 96 | 51.45 | DQOL | 105.23 | 16.06 |
| [98] | Khalili M | 2016 | Isfahan | type 2 | 123 | 52 | DQOL | 1.88 | 0.36 |
| [99] | Hadipour M | 2013 | type 2 | 3472 | 59.4 | EQ-5D | 0.623 | 0.387 | |
| [100] | Daneshvar S | 2018 | Ilam | typ 1 and type 2 | 122 | 57.74 | SF-36 | ||
| [101] | Soleimani Z | 2016 | Sabzevar | typ 1 and type 2 | 189 | 51.7 | DQOL-BCI | 3.4 | 0.62 |
| [102] | Kaveh MH | 2018 | Shiraz | type 2 | 207 | 55.35 | DQOL | 45.95 | 9.67 |
| [103] | Shafiee-Kandjani AR | 2018 | Tabriz | type 2 | 263 | SF-36 | 57.52 | 20.18 | |
| [104] | Sotodeh-Asl N | 2020 | Semnan | type 2 | 50 | >18 | SF-36 | 75.66 | 12.97 |
| [105] | Tafazoli M | 2017 | Mashhad | type 2 | 90 | 43.58 | SF-36 | 58.75 | 16.24 |
| [106] | Tavakkoli L | 2017 | Kerman | type 2 | 198 | 54.91 | WHOQOL-BREF | ||
| [107] | Borhaninejad, VR | 2016 | Kerman | 120 | 71.32 | SF-36 | 46.48 | 20.45 | |
| [108] | Zareipour MA | 2017 | type 2 | 250 | 35-65 | SF-36 | 58.32 | 19.62 | |
| [109] | Soleymanian T | 2017 | Tehran | 219 | 62.2 | SF-36 | 45.7 | 20.9 | |
| [110] | Barzegar Damadi MA | 2018 | Sari | type 2 | 15 | 43.5 | D-39 | 151 | 33.17 |
| [111] | Shakeri M | 2018 | Bojnord | type 2 | 18 | 53.5 | SF-36 | ||
| [112] | Marzban A | 2018 | Yazd | type 2 | 600 | 56.11 | DQOL | 79.34 | 11.02 |
| [113] | Ghaedrahmati A | 2019 | Isfahan | type 2 | 12 | 44 | SF-36 | 54.25 | 4.78 |
According to the results, the mean QOL score in diabetic patients is presented in Table 2. In the WHOQOL-BREF questionnaire, the highest and lowest scores of QOL score in diabetic patients were related to Social Activity (48.36) and the Mental (36.29), respectively. In the SF-36 questionnaire, the highest and lowest quality of life scores of diabetic patients were related to Limitation of Activity (52.72) and Peripheral (24.10), respectively. The mental dimension (20.75) and the Peripheral (9.60) had the highest and lowest QOL scores of diabetic patients in the SF-20 questionnaire. In the DQOL questionnaire, the highest and lowest QOL scores of diabetic patients were related to General Health dimension (41.25) and Social Activity (13.46), respectively. In the QOL questionnaire, the Peripheral dimension (20.23) and the Social Activity dimension (5.18) had the highest and lowest QOL scores of diabetic patients, respectively. In the PedsQL questionnaire, the highest and lowest QOL scores of diabetic patients were related to Emotion dimension (59.84) and Peripheral dimension (33.15), respectively. In the SWED-QUAL questionnaire, the highest and lowest QOL scores of diabetic patients were related to Physical dimension (21.84) and Physical Pain dimension (8.07), respectively. In the IRDQOL questionnaire, the highest and lowest QOL scores of diabetic patients were related to Social Activity dimension (69.53) and Physical dimension (57.03), respectively. In the PHG-2 questionnaire, the highest and lowest QOL scores of diabetic patients were related to Physical dimension (16.43) and Emotion dimension (9.84), respectively.
Table 2.
The mean QOL score in diabetic patients in Iran based on separate reviewed questionnaires
| Questionnaire | Subgroups: Diabetic Patients’ Quality of Life | Number of studies | The quality of life of diabetic patients (CI 95%) | P | I2 (%) |
|---|---|---|---|---|---|
| WHOQOL | Total | 10 | 66.55 (45.83, 87.26) | <0.0001 | 100 |
| Men | 4 | 46.41 (14.76, 78.06) | <0.0001 | 99.8 | |
| Women | 4 | 42.33 (13.92, 70.73) | <0.0001 | 99.9 | |
| Physical Aspect | 15 | 41.06 (26.35, 55.78) | <0.0001 | 100 | |
| Mental Aspect | 14 | 36.29 (22.26, 50.33) | <0.0001 | 100 | |
| Social Activity Aspect | 14 | 48.36 (34.63, 62.09) | <0.0001 | 100 | |
| Peripheral Aspect | 11 | 36.73 (29.46, 44) | <0.0001 | 99.9 | |
| General Health Aspect | 2 | 31.70 (-24.34, 87.73) | <0.0001 | 100 | |
| SF-36 | Total | 19 | 65.64 (59.82, 71.46) | <0.0001 | 98.3 |
| Men | 1 | 49.86 (42.34, 57.38) | - | - | |
| Women | 1 | 63.62 (56.64, 70.60) | - | - | |
| Physical Aspect | 32 | 51.97 (42.75, 61.19) | <0.0001 | 100 | |
| Mental Aspect | 31 | 46.68 (38.99, 54.36) | <0.0001 | 99.9 | |
| Social Activity Aspect | 28 | 48.42 (41.37, 55.46) | <0.0001 | 99.9 | |
| Peripheral Aspect | 2 | 24.10 (22.94, 25.26) | 0.143 | 53.4 | |
| Vitality Aspect | 24 | 49.69 (43.26, 56.11) | <0.0001 | 99.5 | |
| General Health Aspect | 24 | 43.62 (37.0, 50.24) | <0.0001 | 99.6 | |
| Physical Pain Aspect | 26 | 51.16 (40.61, 61.70) | <0.0001 | 99.9 | |
| Physical Role Aspect | 12 | 48.31 (42.53, 54.10) | <0.0001 | 96.5 | |
| Emotion Aspect | 15 | 51.32 (45.18, 57.47) | <0.0001 | 98.7 | |
| Limitation of Activity Aspect | 12 | 52.72 (33.13, 72.31) | <0.0001 | 99.7 | |
| SF-20 | Total | 2 | 46.50 (37.19, 55.81) | 0.002 | 90 |
| Men | 1 | 54.80 (49.87, 59.73) | - | - | |
| Women | 1 | 48.47 (44.71, 52.23) | - | - | |
| Physical Aspect | 1 | 16.05 (15.42, 16.68) | - | - | |
| Mental Aspect | 1 | 20.75 (19.99, 21.51) | - | - | |
| Social Activity Aspect | 1 | 18.05 (17.43, 18.67) | - | - | |
| Peripheral Aspect | 1 | 9.60 (9.06, 10.14) | - | - | |
| DQOL | Total | 10 | 61.19 (35.73-86.66) | <0.0001 | 100 |
| Physical Aspect | 3 | 19.81 (8.70, 30.92) | <0.0001 | 99.9 | |
| Mental Aspect | 3 | 23.67 (10.00, 37.34) | <0.0001 | 99.9 | |
| Social Activity Aspect | 3 | 13.46 (7.03, 19.89) | <0.0001 | 99.6 | |
| Peripheral Aspect | 2 | 15.26 (-0.92, 31.44) | <0.0001 | 99.9 | |
| General Health Aspect | 1 | 41.25 (37.54, 44.96) | - | - | |
| QOL | Total | 3 | 117.91 (-62.97-298.79) | <0.0001 | 100 |
| Physical Aspect | 2 | 9.95 (-5.40, 25.29) | <0.0001 | 99.8 | |
| Mental Aspect | 2 | 8.84 (-3.54, 21.23) | <0.0001 | 99.7 | |
| Social Activity Aspect | 2 | 5.18 (2.09, 8.26) | <0.0001 | 98.8 | |
| Peripheral Aspect | 1 | 20.23 (19.13, 21.33) | - | - | |
| PedsQL | Total | 2 | 34.36 (-31.49, 100.22) | <0.0001 | 100 |
| Physical Aspect | 2 | 35.06 (-31.78, 101.89) | <0.0001 | 99.9 | |
| Mental Aspect | 2 | 34.29 (-30.44, 99.03) | <0.0001 | 99.9 | |
| Social Activity Aspect | 2 | 38.62 (-36.12, 113.37) | <0.0001 | 99.9 | |
| Peripheral Aspect | 2 | 33.15 (-30.76, 97.07) | <0.0001 | 99.9 | |
| Emotion Aspect | 1 | 59.84 (55.71, 63.97) | - | - | |
| ADDQOL | Total | 2 | 41.76 (12.01, 71.50) | <0.0001 | 99.4 |
| Physical Aspect | 1 | -1.81 (-1.96, -1.66) | - | - | |
| Mental Aspect | 1 | -0.94 (-1.11, -0.76) | - | - | |
| Social Activity Aspect | 1 | -0.96 (-1.07, -0.85) | - | - | |
| D-39 | Total | 2 | 129.43 (88.77, 170.10) | <0.0001 | 95.4 |
| SWED-QUAL | Total | 3 | 59.19 (21.15, 97.23) | <0.0001 | 99.8 |
| Physical Aspect | 2 | 21.84 (14.66, 29.02) | <0.0001 | 98.9 | |
| Physical Pain Aspect | 2 | 8.07 (3.89, 12.26) | <0.0001 | 98.8 | |
| Physical Role Aspect | 1 | 9.70 (8.89, 10.51) | - | - | |
| Emotion Aspect | 2 | 20.48 (9.50, 31.47) | <0.0001 | 99.5 | |
| IRDQOL | Total | 2 | 105.92 (102.73, 109.10) | 0.952 | 0 |
| Physical Aspect | 1 | 57.03 (56.65, 57.41) | - | - | |
| Mental Aspect | 1 | 59.54 (59.29, 59.79) | - | - | |
| Social Activity Aspect | 1 | 69.53 (69.16, 69.90) | - | - | |
| PHG-2 | Total | 2 | 22.63 (-2.38, 47.64) | <0.0001 | 99.9 |
| Physical Aspect | 1 | 16.43 (15.60, 17.26) | - | - | |
| Social Activity Aspect | 1 | 16.04 (15.30, 16.78) | - | - | |
| Emotion Aspect | 1 | 9.84 (9.13, 10.55) | - | - | |
| IDQOL-BCI | Total | 1 | 3.40 (3.31, 3.49) | - | - |
| Mental Aspect | 2 | 11.82 (11.36, 12.29) | 0.690 | 0 | |
| Social Activity Aspect | 2 | 11.82 (11.36, 12.29) | 0.690 | 0 |
In the Sf-36 questionnaire, 15% of diabetic patients had a good QOL and 46% had a poor QOL. In the Sf-20 questionnaire, 29% of diabetic patients had a good QOL and 36% had a low QOL. In the QOL questionnaire, 36% of diabetic patients had a desirable QOL and 45% had a poor QOL. In the WHOQOL questionnaire, 55% of diabetic patients had an acceptable QOL and 37% had a poor QOL. In the SWED-QUAL questionnaire, 62% of diabetic patients had an acceptable QOL and 38% had a poor QOL. In the IRDQOL questionnaire, 11% of diabetic patients had an acceptable QOL and 66% had a poor QOL [Table 3].
Table 3.
The QOL of diabetic patients in Iran in three levels (good, fair, and poor)
| Questionnaire | Subgroups | Number of study | The QOL in diabetic patients (95%CI) | P | I2 (%) |
|---|---|---|---|---|---|
| SF-36 | Good | 3 | 15 (-2, 32) | <0.0001 | 100 |
| Fair | 3 | 68 (53, 83) | <0.0001 | 100 | |
| Poor | 3 | 46 (0, 92) | <0.0001 | 100 | |
| SF-20 | Good | 3 | 29 (14, 44) | <0.0001 | 100 |
| Fair | 3 | 35 (30, 39) | <0.0001 | 99.5 | |
| Poor | 3 | 36 (32, 41) | <0.0001 | 99.5 | |
| QOL | Good | 2 | 36 (24, 47) | <0.0001 | 100 |
| Fair | 1 | 29 (29, 30) | - | - | |
| Poor | 2 | 45 (20, 71) | <0.0001 | 100 | |
| WHOQOL | Good | 1 | 55 (55, 55) | - | - |
| Fair | 1 | 56 (55, 56) | - | - | |
| Poor | 1 | 37 (37, 37) | - | - | |
| SWED-QUAL | Good | 2 | 62 (19, 105) | <0.0001 | 100 |
| Poor | 2 | 38 (-5, 81) | <0.0001 | 100 | |
| IRDQOL | Good | 1 | 11 (11, 11) | - | - |
| Fair | 1 | 23 (22, 23) | - | - | |
| Poor | 1 | 66 (66, 66) | - | - |
In order to perform additional analyzes, we plotted the meta-regression diagram. There was no significant statistical relationship in the study of meta-regression score of quality of life in diabetic patients based on the year of study (P = 0.565) [Figure 1]. This means that over time, the QOL of diabetic patients has not decreased. The relationship between QOL score in diabetic patients and the number of research samples was not statistically significant (P = 0.106) [Figure 2].
Figure 1.
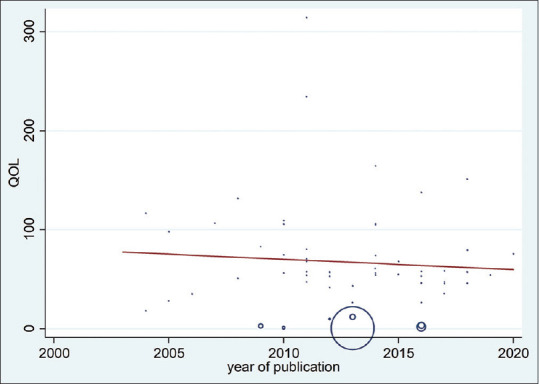
The relationship between quality of life score in diabetic patients and the year of publication
Figure 2.
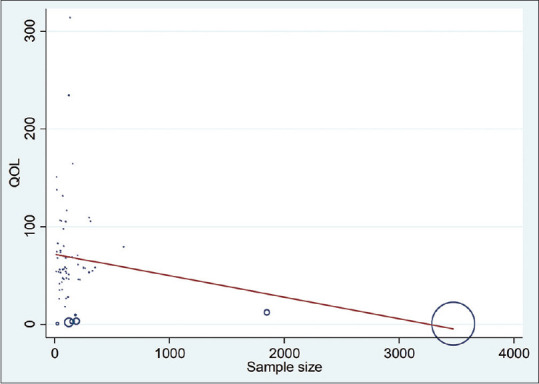
The relationship between quality of life score in diabetic patients and the sample size
Discussion
In 96 reviewed studies with a sample of 17,994, the QOL score in diabetic patients was 66.55 in WHOQOL, 65.64 in SF-36, 46.50 in SF-20, 61.19 in DQOL, 117.91 in QOL,129.43 in D-39, 34.36 in PedsQL, 41.76 in ADDQOL, 22.63 in IDQOL-BCI, 3.40 in DQOL-BCI, 0.62 in EQ-5D, 61.00 in PHG-2, 105.92 in IRDQOL, 59.19 in SWED-QUAL.
So far, several meta-analyzes have been conducted on the status of QOL in diabetic patients in Iran, which we will examine below: In a meta-analysis of T. Schram et al. (2009)[114] in The Netherlands, the aim was to investigate the relationship between depression and quality of life in diabetic patients. All studies suggest a negative association between depressive symptoms and at least one aspect of QOL in people with diabetes. People with diabetes with depressive symptoms also had a much lower QOL than diabetes.
In meta-analysis of Kiadaliri et al. (2013),[115] 46 studies found that people with diabetes were less likely to have health-related quality of life (HRQoL) without diabetes. The study covered 20 of Iran's 30 provinces. Of these 46 studies, 5 were type 1 diabetes and 23 were type 2 diabetes, and other studies were a combination of different types of diabetes. However, our study covered the studies published until 2017, and therefore the number of studies studied in our study is about twice that of the 2013 meta-analysis.In 2016, Soleimannejad et al.[20] Studied the QOL of diabetic patients in 10 studies. And we decided to update this study: In the previous meta-analysis the number of studies studied was 10, whereas in the present study 82 studies were reviewed.
In previous meta-analysis, only studies using questionnaires SF-36 and SF-20 were evaluated. However, in the present meta-analysis, all available questionnaires (WHOQOL-BREF, SF-36, SF-20, DQOL, QOL, PedsQL, ADDQoL, Youth Diabetes QOL and IDQOL-BCI) have been reviewed and no restrictions have been imposed on the questionnaire.
The number of samples studied in the previous meta-analysis was 1,082, while in the present study 15,571 diabetic patients were evaluated.
In the present meta-analysis, the QOL score of diabetic patients was examined by type of questionnaire and by dimensions of questionnaires and compared with each other, whereas this was not the case in previous meta-analysis.
Current meta-analysis covers studies published as of December 31, 2016, while previous meta-analysis has carried out resource search for year 2015
-
Current meta-analysis, in addition to the databases used by the previous meta-analysis, it has also examined the Cochrane, Embase, and Medline databases.
Given the above, the present study is more complete than the previous meta-analysis study.
In the present meta-analysis, the QOL of diabetic patients was evaluated in the form of levels: Good, Moderate, and Poor. This issue was not presented in previous meta-analysis.
Recently, two meta-analysis has been published in this regard, which we refer to: In meta-analysis Mokhtari et al. (2018)[116] of 5,472 samples, the mean physical dimension score in patients with type 2 diabetes (53.5, 95% CI: 43.1--63.9) and the mean mental dimension score (54.5, 95% CI: 47--61.9) was less. As the age of the samples increased, the mean HRQoL score in diabetic patients in Iran decreased significantly.
In a meta-analysis of Dehvan et al.) 2019(,[117] the QOL of type 2 diabetes patients in Iran was examined. The mean QOL of patients with type 2 diabetes was 61.90 (95% CI: 54.40--6940.). The highest and lowest QOL was achieved in terms of social support (49.19) and mental health (42.96). In this study, the WHOQOL-BREF questionnaire was used to assess the QOL of diabetic patients and therefore the number of studies studied was limited (16 studies). However, in our study, we did not have any restrictions on the type of diabetes or the type of questionnaire. A meta-analysis of Khunkaew et al. (2018),[118] 12 studies in Australia found this conclusion. Overall, the HRQOL of participants in the studies was poor on four of eight subscales in the SF-36: Physical functioning (42.75); role physical (20.61); general health (39.52); and vitality (45.73). The results of this study are almost consistent with the results of the present meta-analysis.[113,114,115,116]
Thommasen et al. conducted a study on the people of China, Malaysia, and India. In China, the mean scores of physical functioning was 83.3, public health was 69.3, social functioning was 83.9, and mental health was 72.9. In Malaysia, the mean scores of physical functioning was 86.6, public health was 68.6, social functioning was 78.8, and mental health was 75. In India, the mean scores of physical functioning was 73.9, public health was 70.1, social functioning was 86.1, and mental health was 71.5.[119]
QOL[1,118,119] Given that varied data have been archived for QOL of diabetic patients, the present meta-analysis was used to obtain an accurate estimate of the QOL of diabetic patients.
Conclusions
In this study, the QOL of diabetic patients was evaluated according to different types of studied questionnaires. We found that QOL of diabetic patients was lower than normal society. According to the results, the highest and lowest mean QOL score in diabetic patients in Iran were related to the D-39 questionnaire (129.43) and the EQ-5D questionnaires (0.62), respectively.
Limitations of the study
The limitations of the present study include lack of access to the full text of articles, lack of sufficient data in some articles, lack of reference to mean and standard deviation of QOL score in diabetic patients in some studies, and lack of uniform distribution of studies in different regions of Iran.
Authors' contribution
MF, MR, MA and DS searched the literature and analyzed the papers. The extraction stage was performed by MR, MA and DS. DS, MF, AHD prepared the manuscript. All authors read and signed the final paper.
Supplement
S1: Abbreviated table
| Full name | Abbreviated name |
|---|---|
| Quality of life | QOL |
| WHO Quality of Life-BREF | WHOQOL-BREF |
| Short Form-36 | SF-36 |
| Short Form-20 | SF-20 |
| Diabetes Quality of Life | DQOL |
| Quality of Life | QOL |
| The World Health Organization Quality of Life | WHOQOL |
| Pediatric Quality of Life Inventory | PedsQL |
| Audit of Diabetes Dependent Quality of Life | ADDQoL |
Iranian version of the Diabetes Quality of Life IDQOL-BCI Brief Clinical Inventory
Ethical considerations
Ethical issues (including plagiarism, data fabrication, double publication) have been completely observed by the authors.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Footnotes
Quality of life
WHO Quality of Life-BREF
Short Form
Diabetes Quality of Life
Quality of Life
Pediatric Quality of Life Inventory
Audit of Diabetes Dependent Quality of Life
Iranian version of the Diabetes Quality of Life Brief Clinical Inventory
References
- 1.Darvish Poor Kakhki A, Saeedi J, Yaghmaie F, Majd H, Montazeri A. Quality of life of diabetic patients referred to Tehran hospitals in 2004. Int J Endocrinol Metab. 2006;8:49–56. [Google Scholar]
- 2.Sayari A, Gari D, Asadai Lari M. Assessing quality of life, global experiences and the need for action in Iran. Teb va Tazkiye. 2001:30–5. [Google Scholar]
- 3.Cote I, Gregoire J, Moisan J, Chabot I. Quality of life in hypertension: The SF-12 compared to the SF-36. Can J Clin Pharmacol. 2004;11:232–8. [PubMed] [Google Scholar]
- 4.Masoudi-Alavi N, Ghofranipor F, Ahmadi F, Rajab A, Babai G. Quality of life in diabetic patient refers to diabetic association of Iran Behbood Journal. 2004;8:47–56. [Google Scholar]
- 5.Leininger M. Quality of life from a transcultural nursing perspective. Nurs Sci Q. 1994;7:22–8. doi: 10.1177/089431849400700109. [DOI] [PubMed] [Google Scholar]
- 6.Karlson I, Berglin E, Larson P. Sense of coherence: Qol before and after coronary artery bypass surgery alongitudinal study. J Aadv Nurs. 2000;31:1383–92. doi: 10.1046/j.1365-2648.2000.01408.x. [DOI] [PubMed] [Google Scholar]
- 7.Monica S, Clare M, Lesley B. Diabetic foot care: Assessing the impact of care on the whole patient. Practical Diabetes Int. 2000;17:147–51. [Google Scholar]
- 8.Glasgow R, Ruggiero L, Eakin E, Dryfoos J, Chobanian I. Quality of life associated characteristics in a large national sample of adults with diabetes. Diabetes Care. 1997;20:562–7. doi: 10.2337/diacare.20.4.562. [DOI] [PubMed] [Google Scholar]
- 9.Kotsanos J, Marrfero D, Viginati J, Mathias A, Huster W, Boggs M, et al. Health related quality of life results from multinational clinical trial of insulin lispro. Diabetes Care. 1997;20:948–58. doi: 10.2337/diacare.20.6.948. [DOI] [PubMed] [Google Scholar]
- 10.Andrew J. Guideline and performance measures for diabetes. Am J Manag Care. 2007;13(Suppl 2):S41–6. [PubMed] [Google Scholar]
- 11.Gambert S. Are we up to the challenge? Clin Geriatr. 2002;10:14–7. [Google Scholar]
- 12.Wild S, Ruglie G, Grcon A, Sicree R, king H. Glohal prevalence of diabetes: Estimates for the Year 2000 and projections for 2030. Diabetes Care. 2004;27:1047–53. doi: 10.2337/diacare.27.5.1047. [DOI] [PubMed] [Google Scholar]
- 13.Lustman PJ, Anderson RJ, Freedland KE, de Groot M, Carney RM, Clouse RE. Depression and poor glycemic control: A meta-analytic review of the literature. Diabetes Care. 2000;23:934–42. doi: 10.2337/diacare.23.7.934. [DOI] [PubMed] [Google Scholar]
- 14.Michael J. Diabetes foundation, clinical diabetes. Am Diabetes Assoc. 2008;26:77–82. [Google Scholar]
- 15.Graham JE, Stoebner-May DG, Ostir GV, Snih SA, Peek MK, Markides K, et al. Health related quality of life in older Mexican Americans with diabetes. Health Qual Life Outcomes. 2007;5:39. doi: 10.1186/1477-7525-5-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Abdel Gawad E. Quality of life In Saudis with diabetes. Saudi J Disabil. 2002;8:163–8. [Google Scholar]
- 17.Heine J. Diabetes in the next century: Challenges and opportunities. Neth J Med. 1999;55:265–70. doi: 10.1016/s0300-2977(99)00092-3. [DOI] [PubMed] [Google Scholar]
- 18.Sabiha I. WHO study group. Prevention of diabetes mellitus: Report of a WHO study group. Pak Dev Rev. 1995;34:91. [Google Scholar]
- 19.Azizi F, Gouya MM, Vazirian P, Dolatshahi P, Habibian S. Screening for type 2 diabetes in the Iranian national programme: A preliminary report la revue de sant'de la me'diterrane'e orientale. East Mediterr Health J. 2003;9:1122–7. [PubMed] [Google Scholar]
- 20.Soleimannejad K, Sarokhani D, Sarokhani M, Sayehmiri K, Ahmadi N. Quality of life in diabetes patients in Iran: A systematic review and meta-analysis method. Int J Pharm Tech. 2016;8:21608–18. [Google Scholar]
- 21.Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. The Strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Prev Med. 2007;45:247–51. doi: 10.1016/j.ypmed.2007.08.012. [DOI] [PubMed] [Google Scholar]
- 22.Aghamollaei T, Eftekhar H, Shojaeizadeh D, Mohammad K, Nakhjavani M, Pour F. Behavior, metabolic control and health-related quality of life in diabetic patients at Bandar Abbas diabetic clinic. Iranian J Publ Health. 2003;32:54–9. [Google Scholar]
- 23.Aghamolaei T, Eftekhar H, Mohammad K, Sobhani A, Shojaeizadeh D, Nakhjavani M, et al. Influence of educational intervention using interaction approach on behavior change, hemoglobin AlC and health-related quality of life in diabetic patients. J School Pub Health Int Pub Health Res. 2005;3:1–2. [Google Scholar]
- 24.Sadeghie-Ahari S, Arshi S, Iranpour M, Amani F, Siahpush H. The effect of complications of type 2 diabetes in quality of life in diabetic patients. J Ardabil Univ Med Sci. 2008;8:394–402. [Google Scholar]
- 25.Ahmadi A, Hasanzadeh J, Rahimi M, Laskari L. Factors affecting quality of life in type 2 diabetics in Chaharmahal va Bakhtiari province. J North Khorasan Univ Med Sci. 2011;3:7–11. [Google Scholar]
- 26.Alavi A, Parvin N, Salehian T, Samipour V. Comparing quality of life of children and adolescents with diabetes mellitus and healthy group from patient and parents perspective in Shahrekord. J Kordestan Univ Med Sci. 2010;15:46–52. [Google Scholar]
- 27.Baghianimoghadam M, Afkhami-Ardakani M. The effect of educational intervention on quality of life of diabetic patients type 2, referee to diabetic research centre of Yazd. Horizon Med Sci. 2008;13:21–8. [Google Scholar]
- 28.Bazzazian S, Besharat M, Ehsan H, Rajab A. The moderating role of coping strategies in relationship between illness perception, quality of life and HbA1c in patients with type I diabetes. Iranian J Endocrinol Metab. 2010;12:213–21. [Google Scholar]
- 29.Borzou S, Salavati M, Safari M, Hadadinejad S, Zandieh M, Torkaman B. Quality of life in type II diabetic patients referred to Sina Hospital, Hamadan. Zahedan J Res Med Sci. 2011;13:42–6. [Google Scholar]
- 30.Safarabadi-Farahani T, Ali-Akbar M, Safarabadi-Farahani A, Haghani H. Quality of life in young people with type 1 diabetes in relation to age and gender. Iran J Nurs. 2011;23:73–9. [Google Scholar]
- 31.Ghanbari A, Kazemnezhad E. A comparative study on the quality of life not insulin dependent diabetic melitus (niddm) patients of the razi hospital of rasht. Modares J Med Sci. 2004;7:69–80. [Google Scholar]
- 32.Ghanbari A, Yekta Z, Roushan Z, Lakeh N. Assessment of factors affecting quality of life in diabetic patients in Iran. Public Health Nurs. 2005;22:311–22. doi: 10.1111/j.0737-1209.2005.220406.x. [DOI] [PubMed] [Google Scholar]
- 33.Haririan H, Moghadasian S, Aghajanlou A. Quality of life and its dimensions in diabetic patients referring to diabetes center, Tabriz university of medical sciences, 2007. J Diabetes Metab Disord. 2009;9:152–60. [Google Scholar]
- 34.Heydari M, Alhani F, Kazemnejad A, Moezi F. The effect of empowerment model on quality of life of diabetic adolescents. Iran J Pediatr. 2007;17:87–94. [Google Scholar]
- 35.Jafari P, Forouzandeh E, Bagheri Z, Karamizadeh Z, Shalileh K. Health related quality of life of Iranian children with type 1 diabetes: Reliability and validity of the Persian version of the PedsQL™ generic core scales and diabetes module. Health Qual Life Out. 2011;9:104. doi: 10.1186/1477-7525-9-104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ghavami H, Ahmadi F, Entezami H, Memarian R. The effect of continuous care model on quality of life in diabetic patients. J Urmia Univ Med Sci. 2005;16:22–7. [Google Scholar]
- 37.Jahanlou AS, Karami NA. The effect of literacy level on health related-quality of life, self-efficacy and self-management behaviors in diabetic patients. Acta Med Iran. 2011;49:153–8. [PubMed] [Google Scholar]
- 38.Jahanlou AS, Ghofranipour F, Kimmiagar M, Vafaei M, Heydarnia A, Sobhani A. Can quality of life questionnaires be used in diabetics to assess the relation between HbA1c and patients' domain aspects? Acta Med Iran. 2011;49:246–51. [PubMed] [Google Scholar]
- 39.Sedaghti-Kasbakhi M, Ehsani M, Ghanbari A. Comparison of quality of life in patients with type 2 diabetes with non-diabetic patients. J Babol Univ Med Sci. 2007;9:55–60. [Google Scholar]
- 40.Kermansaravi F, Navidian A, Ansarymoghadamn A. Quality of life in type 1 diabetic adolescents in Zahedan (2011) Iranian J Endocrinol Metab. 2012;13:651–7. [Google Scholar]
- 41.Khaledi S, Moridi G, Gharibi F. Survey of eight dimensions quality of life for patients with diabetes type II, referred to Sanandaj diabetes center in 2009. J Fasa Univ Med Sci. 2011;1:29–37. [Google Scholar]
- 42.Khamseh M, Monavari A, Malek M, Shafiee G, Baradaran H. Health- related quality of life in patients with type 1 diabetes. Iranian J Endocrinol Metab. 2011;13:249–56. [Google Scholar]
- 43.Peymani M, Monjamed Z, Aliasghapour M, Mehran A. Surveying the quality of life of diabetic patients with cardiovascular complications referring to the endocrinology clinic of selected hospitals of Tehran university of medical sciences in 2004-2005. J Med Council IRI. 2007;25:142–8. [Google Scholar]
- 44.Rakhshanderu S, Heydarnia A, Rajab A. The effect of health education on quality of life in diabetic patients. Daneshvar Med. 2006;13:15–20. [Google Scholar]
- 45.Rasouli D, Nasiriziba F, Nabiamjad R, Haghani H. Comparison of life quality in men and women with diabetic foot ulcer in selected hospitals of Tehran universities, 1387. Pars J Med Sci. 2011;9:38–45. [Google Scholar]
- 46.Safavi M, Samadi N, Mahmoodi M. Effect of quality of life improvement on type 2 diabetes patients' self-esteem. Saudi Med J. 2011;32:954–7. [PubMed] [Google Scholar]
- 47.Sanjari M, Safari S, Shokoohi M, Safizade H, Rashidinezhad H, Mashrouteh M, et al. A cross-sectional study in Kerman, Iran, on the effect of diabetic foot Ulcer on health-related quality of life. Int J Low Extrem Wounds. 2011;10:200–2006. doi: 10.1177/1534734611428728. [DOI] [PubMed] [Google Scholar]
- 48.Shahrjerdi S, Shavandi N, Golpaygani M, Sheykhhoseini R. Effect of endurance and strength training on blood glucose control, quality of life and mental health in women with type 2 diabetes. Iranian J Diabetes Metab. 2009;9:35–44. [Google Scholar]
- 49.Sayadi N, Fayazi S, Ramazani A. Comparison of quality of life among diabetic and non diabetic patients after open heart surgery (Short report) J Rafsanjan Univ Med Sci Health Serv. 2011;10:144–50. [Google Scholar]
- 50.Taghdisi M, Borhani M, Solhi M, Afkari M, Hosseini F. The effect of an education program utilising PRECEDE model on the quality of life in patients with type 2 diabetes. Health Educ J. 2012;71:229–38. [Google Scholar]
- 51.Timareh M, Rahimi M, Abbasi P, Rezaei M, Hyaidarpoor S. Quality of life in diabetic patients referred to the diabete research center in Kermanshah. J Kermanshah Univ Med Sci (BEHBOOD) 2012;16:63–9. [Google Scholar]
- 52.Vares Z, Zandi M, Baghaei P, Alavi N, Ajorpaz N. Quality of life and related factors in diabetic patients attending a diabetes center in Kashan. Nurs Res. 2010;5:14–22. [Google Scholar]
- 53.Vazirinejad R, Sajadi MA, Maghool N. A historical cohort study assessing the effect of diabetes on the quality of life of patients. Res Med. 2010;34:35–40. [Google Scholar]
- 54.Yekta Z, Pourali R, Ghasemi-Rad M. Comparison of demographic and clinical characteristics influencing health-related quality of life in patients with diabetic foot ulcers and those without foot ulcers. Diabetes Metab Syndr Obes. 2011;4:393–9. doi: 10.2147/DMSO.S27050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Mirfeizi M, Jafarabadi M, Toorzani Z, Mohammadi S, Azad M, Mohammadi A, et al. Feasibility, reliability and validity of the Iranian version of the diabetes quality of life brief clinical inventory (IDQOL-BCI) Diabetes Res Clin Pract. 2012;96:237–47. doi: 10.1016/j.diabres.2011.12.030. [DOI] [PubMed] [Google Scholar]
- 56.Shahi M, Mohammadyfar M. Comparison of depression, anxiety, stress, quality of life, and alexithymia between people with type II diabetes and non-diabetic counterparts. Pers Individ Differ. 2017;104:64–8. [Google Scholar]
- 57.Najafi-Ghezeljeh T, Kohandany M, Oskouei F, Malek M. The effect of progressive muscle relaxation on glycated hemoglobin and health-related quality of life in patients with type 2 diabetes mellitus. Appl Nurs Res. 2017;33:142–8. doi: 10.1016/j.apnr.2016.11.008. [DOI] [PubMed] [Google Scholar]
- 58.Shamshirgaran S, Ataei J, Alamdari M, Safaeian A, Aminisani N. Predictors of health-related quality of life among people with type II diabetes Mellitus in Ardabil, Northwest of Iran, 2014. Prim Care Diabetes. 2016;10:244–50. doi: 10.1016/j.pcd.2015.11.004. [DOI] [PubMed] [Google Scholar]
- 59.Hajian-Tilaki K, Heidari B, Hajian-Tilaki A. Solitary and combined negative influences of diabetes, obesity and hypertension on health-related quality of life of elderly individuals: A population-based cross-sectional study. Diabetes Metab Syndr. 2016;10:37–42. doi: 10.1016/j.dsx.2016.01.018. [DOI] [PubMed] [Google Scholar]
- 60.Dadgostar H, Firouzinezhad S, Ansari M, Younespour S, Mahmoudpour A, Khamseh M. Supervised group-exercise therapy versus home-based exercise therapy: Their effects on quality of life and cardiovascular risk factors in women with type 2 diabetes. Diabetes Metab Syndr. 2016;10:30–6. doi: 10.1016/j.dsx.2016.01.016. [DOI] [PubMed] [Google Scholar]
- 61.Jafari N, Farajzadegan Z, Loghmani A, Majlesi M, Jafari N. Spiritual well-being and quality of life of Iranian adults with type 2 diabetes. Evid Based Complement Alternat Med. 2014;2014:8. doi: 10.1155/2014/619028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Abdoli S, Abdoli S. Quality of life in people with type 2 diabetes living in rural and remote areas, Iran. Int J Diabetes Dev Ctries. 2015;35:290–7. [Google Scholar]
- 63.Hadi N, Ghahramani S, Montazeri A. Health related quality of life in both types of diabetes in Shiraz, Iran. Shiraz E Medical J. 2013;14:112–22. [Google Scholar]
- 64.Shavandi N, Sharjerdi S, Sheikh Hoseini R, Ghorbani A. The effect of strengthening exercises on metabolic factors, quality of life and mental health in women with type 2 diabetes. Iranian J Endocrinol Metab. 2010;12:222–30. [Google Scholar]
- 65.Shayeghian Z, Aguilar-Vafaie M, Besharat M, Parvin M, Roohi Gilani K. The association between self-care and control of blood sugar and health-related quality of life in type II diabetes patients. Iranian J Endocrinol Metab. 2014;15:545–51. [Google Scholar]
- 66.Alipour A, Zare H, Poursharifi H, Sheibani K, Ardekani M. The intermediary role of self-efficacy in relation with stress, glycosylated haemoglobin and health-related quality of life in patients with type 2 diabetes. Iran J Public Health. 2012;41:76–80. [PMC free article] [PubMed] [Google Scholar]
- 67.Afshar M, Memarian R, Mohammadi E. The effect of group discussion on the quality of life and HbA1c levels of adolescents with diabetes. Iran Red Crescent Med J. 2014;16:e21110. doi: 10.5812/ircmj.21110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Derakhshanpour F, Vakili M, Farsinia M, Mirkarimi K. Depression and quality of life in patients with type 2 diabetes. Iran Red Crescent Med J. 2015;17:e27676. doi: 10.5812/ircmj.17(5)2015.27676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Zaker M, Moghadam A, Shams S, Moradi Y. Effect of self-management education package on specific quality of life among diabetic patients in Urmia diabetes centers. J Chem Pharm Sci. 2016;9:1396–9. [Google Scholar]
- 70.Didarloo A, Alizadeh M. Health-related quality of life and its determinants among women with diabetes mellitus: A cross-sectional analysis. Nurs Midwifery Stud. 2016;5:e28937. doi: 10.17795/nmsjournal28937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Gholami A, Azini M, Borji A, Shirazi F, Sharafi Z, Zarei E. Quality of life in patients with type 2 diabetes: Application of WHOQOL-BREF scale. Shiraz E Medical J. 2013;14:162–71. [Google Scholar]
- 72.Torabi M, Izadi A, Naderi F, Shamsaei F. Sleep quality and quality of life in adults with type 2 diabetes. J Diabetes Nurs. 2014;2:51–61. [Google Scholar]
- 73.Izadi A, Sepahvand F, Naderifar M, Mohammadipour F. The effect of an educational intervention on quality of life in patients with type 2 diabetes referring to Tamin Ejtemaei hospital in 2013. J Diabetes Nurs. 2014;2:18–28. [Google Scholar]
- 74.Khodabakhshi-Koolaei A, Navidian A, Baiati Z, Rahmatizadeh M. Effectiveness of supportive psychotherapy on quality of life in patients with type 2 diabetes. J Diabetes Nurs. 2015;3:31–41. [Google Scholar]
- 75.Mohammadshahi M, Shirani F, Elahi S, Ghasemi S, Shahni M, Haidari F. Evaluation of relationship between dietary patterns and quality of life in patients with type 2 diabetes. Daneshvar Med. 2015;22:1–12. [Google Scholar]
- 76.Saeedpour J, Jafari M, Asgar M, Dardashti H, Teymoorzadeh E. The impact of self-care education on life quality of diabetic patients. J Health Admin. 2013;16:26–36. [Google Scholar]
- 77.Ghasemipour M, Ghasemi V, Zamani A. Evaluation of quality of life and its dimensions in diabetic patients referring to Khorramabad Shohada hospital (in 2008) Yafteh. 2009;11:125–33. [Google Scholar]
- 78.EydiBaygi M, Mehrabizade M, Davoudi I, Ahmadi V, Dehghanizade Z. Comparison the quality of life in patients with diabetes type 2 and non-diabetic individuals. Sci J Ilam Uni Med Sci. 2014;22:55–62. [Google Scholar]
- 79.Sadeghi T, Derakhshan R. The effect of nurse telephone follow up on quality of life in diabetic patients. Payesh. 2012;11:711–7. [Google Scholar]
- 80.Zaree-Bahramabadi M, Vafaei-Baneh F, Ghaderi E, Taghvaei D. The Effectiveness of cognitive-behavioral therapy on quality of life in patients with type 2 diabetes. J Diabetes Metab Disord. 2013;12:225–32. [Google Scholar]
- 81.Ghashghaie S, Farnam R. The effectiveness of mindfulness-based cognitive therapy on quality-of-life in outpatients with diabetes. Iranian J Diabetes Metab. 2014;13:319–30. [Google Scholar]
- 82.Saadatjoo S, Rezvanee M, Tabyee S, Oudi D. Life quality comparison in type 2 diabetic patients and none diabetic persons. Mod Care Sci Qtly Birjand Nurs Midwifery Fac. 2012;9:24–31. [Google Scholar]
- 83.Behrouz B, Bavali F, Heidarizadeh N, Farhadi M. The effectiveness of acceptance and commitment therapy on psychological symptoms, coping styles, and quality of life in patients with type-2 diabetes. J Health. 2016;7:236–53. [Google Scholar]
- 84.Ebrahimi H, Sadeghi M, Bazghaleh M, Shaker S, Ghasemi M. Relationship between metabolic control indexes and quality of life in patients with type II diabetes mellitus. Iran J Nurs. 2014;27:73–82. [Google Scholar]
- 85.Mohammad Rahimi G, Attarzadeh Hosseini S. Effect of aerobic training and diet on insulin resistance and quality of life in type II diabetic patients. Horizon Med Sci. 2016;21:277–84. [Google Scholar]
- 86.Shams S, Zaker M, Ghavami H. Effect of self management educative package on quality of life among diabetic patients in Urmia diabetes centers between in the years of 2013. J Urmia Nurs Midwifery Fac. 2016;13:863–8. [Google Scholar]
- 87.Mohammadpour Y, Haririan H, Moghadasian S, Ebrahimi H. Study of quality of life and its dimensions in diabetic patients referring to diabetes center of Tabriz university of medical sciences in 2007. J Urmia Nurs Midwifery Fac. 2008;6:26–37. [Google Scholar]
- 88.Ganjlo J, Talebi Z, Assarroudi A, Rakhshani M. Comparative assessment of effect of education in the OREM's self care model way with current method on the quality of life of diabetic type 2 patients. Bimonthly J Sabzevar Univ Med Sci. 2015;22:748–57. [Google Scholar]
- 89.Bidi F, Hassanpour K, Ranjbarzadeh A, Kheradmand A. Effectiveness of educational program on knowledge, attitude, self care and life style in patients with type II diabetes. J Sabzevar Univ Med Sci. 2013;19:336–44. [Google Scholar]
- 90.Derakhshanpoor F, Farsinia M, Shahini N. Relationship between anxiety disorders and life quality in type two diabetic patients. J Res Dev Nurs Midw. 2015;12:94–102. [Google Scholar]
- 91.Bahadori-Khosroshahi J, Khanjani Z. Depression and quality of life between diabetic and non-diabetic patients. J Health Psychol. 2011;1:61–77. [Google Scholar]
- 92.Fuladvandi M, Aziz Zadeh Foroozi M, Asad Abadi A, Fuladvandi G, Lashkari T, Malekian L. Effectiveness of stress management training on improved quality of life in patients with type 2 diabetes. J Health Promot Manag. 2014;3:16–24. [Google Scholar]
- 93.Shahraki-Vahed A, Hamedi-Shahraki S, Masinaeinezhad N, Shahdadi H. Survey of life's quality in diabetic patients referred to diabet's clinic of Zabol 2010. J Rostamineh. 2011;3:21–9. [Google Scholar]
- 94.Taghdisi M, Borhani M, Solhi M, Afkari M, Hosseini M. Effect of educational program based on PRECED model on quality of life in patients with typeII diabetes. J Gorgan Univ Med Sci. 2011;13:29–36. [Google Scholar]
- 95.Sepehrnia E, Ranjbar F, Hosseinzadeh-Taghvaei M, Peymani J. The effectiveness of life skills training on the subscale of quality of life in people with diabetes. J Health Psychol. 2011;1:81–102. [Google Scholar]
- 96.Fathi Ahmadsaraei N, Neshat Doost H, Manshaee G, Nadi M. The effectiveness of acceptance and commitment therapy on quality of life among patients with type 2 diabetes. Iran J Health Educ Health Promot. 2016;4:31–9. [Google Scholar]
- 97.Moein M, Aghajani M, Mirbagher-Ajorpaz N. Effects of the empowerment program on the quality of life in patients with type II diabetes. J Diabetes Nurs. 2015;3:29–41. [Google Scholar]
- 98.Khalili M, Sabouhi F, Abazari P, Aminorroaya A. Comparing the quality of life in insulin recipient and refusal patients with type 2 diabetes. Iran J Nurs Midwifery Res. 2016;21:351–6. doi: 10.4103/1735-9066.185571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Hadipour M, Aboalhasani F, Molavi-Vardanjani H. Health related quality of life in patients with of type II diabetes in Iran. Payesh. 2013;12:135–41. [Google Scholar]
- 100.Daneshvar S, Khodamoradi A, Ghazanfari Z, Montazeri A. Quality of life in diabetic patients: A comparative study. Payesh. 2018;17:541–50. [Google Scholar]
- 101.Solimani Z, Barati H, Mozafari J, Ershadi M, Mohammadi M. The quality of life of patients with diabetes from the city of Sabzevar during year 2016. Military Caring Sci. 2017;3:264–71. [Google Scholar]
- 102.Kaveh M, Ghahremani L, Nazari M, Zare S. Quality of life in diabetic patients: The predicting role of personal resources. J Health Sci Surveillance Sys. 2018;6:142–8. [Google Scholar]
- 103.Shafiee-Kandjani AR, Hosseinpour M, Shoja H, Daneshamouz H, Mohammad-Alizadeh S. Assessing quality of life and general health status in married women with type II diabetes in Tabriz. Depiction Health. 218(9):195–205. [Google Scholar]
- 104.Sotodeh Asl N, Avazabadian M, Ghorbani R, Malek F. Quality of life in patients with hypertension and type 2 diabetes mellitus. Koumesh. 2020;22:263–8. [Google Scholar]
- 105.Tafazoli M, Parnan A, Azmoude E. Sexual function and quality of life in diabetic women referring to health care centers in Mashhad. J Edu Health Promot. 2017;6:25. doi: 10.4103/jehp.jehp_33_15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Tavakkoli L, Dehghan A. Compare the quality of life in type 2 diabetic patients with healthy individuals (Application of WHOQOL-BREF) Zahedan J Res Med Sci. 2017;19:e5882. [Google Scholar]
- 107.Borhaninejad V, Kazazi L, Haghi M, Chehrehnegar N. Quality of life and its related factors among elderly with diabetes. Iran J Ageing. 2016;11:162–73. [Google Scholar]
- 108.Zareipour M, Ghelichi Ghojogh M, Mahdi-Akhgar M, Alinejad M, Akbari S. The quality of life in relationship with glycemic control in people with type 2 diabetes. J Community Health Res. 2017;6:141–9. [Google Scholar]
- 109.Soleymanian T, Kokabeh Z, Mahjoub A, Ramaghi R, Argani H. Clinical outcomes and quality of life in hemodialysis diabetic patients versus non-diabetics. J Nephropathol. 2017;6:81–9. doi: 10.15171/jnp.2017.14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Barzegar Damadi M, Mirzaian B, Akha O, Hosseini S, Jadidi M. Effect of cognitive-behavioral group therapy on HbA1C, selfefficacy, depression, illness perception, and quality of life in patients with type II diabetes. J Mazandaran Univ Med Sci. 2018;27:87–100. [Google Scholar]
- 111.Shakeri M, Hatami M, Hasani J, Shakeri HS. The Effectiveness of Mindfulness-Based Stress Reduction (MBSR) on mental health and quality of life of the patients with type 2 diabetes. JNKUMS. 2018;10:31–40. [Google Scholar]
- 112.Marzban A. Relationship between spiritual health and quality of life in type II diabetic patients: A crosssectional study in Yazd. J Diabetes Nurs. 2018;6:641–52. [Google Scholar]
- 113.Ghaedrahmati A, Jabalameli S. Effect of acceptance and commitment therapy on the quality of life and physical indices of patients with diabetes. J Diabetes Nurs. 2019;7:915–28. [Google Scholar]
- 114.Schram M, Baan C, Pouwer F. Depression and quality of life in patients with diabetes: A systematic review from the European depression in diabetes (EDID) research consortium. Curr Diabetes Rev. 2009;5:112–9. doi: 10.2174/157339909788166828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Kiadaliri AA, Najafi B, Mirmalek-Sani M. Quality of life in people with diabetes: A systematic review of studies in Iran. J Diabetes Metab Disord. 2013;12:54. doi: 10.1186/2251-6581-12-54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Mokhtari Z, Gheshlagh RG, Kurdi A. Health-related quality of life in Iranian patients with type 2 diabetes: An updated meta-analysis. Diabetes Metab Syndr. 2019;13:402–7. doi: 10.1016/j.dsx.2018.10.007. [DOI] [PubMed] [Google Scholar]
- 117.Dehvan F, Saeid DM, Dehkordi AH, Gheshlagh RG. Quality of life of Iranian patients with type 2 diabetes: A systematic review and meta-analysis. Nurs Pract Today. 2019;6:167–75. [Google Scholar]
- 118.Khunkaew S, Fernandez R, Sim J. Health-related quality of life among adults living with diabetic foot ulcers: A meta-analysis. Qual Life Res. 2019;28:1413–27. doi: 10.1007/s11136-018-2082-2. [DOI] [PubMed] [Google Scholar]
- 119.Thommasen HV, Zhang W. Impact of chronic disease on quality of life in the Bella Coola valley. Rural Remote Health. 2006;6:528. [PubMed] [Google Scholar]