

Abstract
Background:
The present study was aimed at evaluating the effectiveness of BNT162b2 among HCWs of a university hospital while a recrudescence of pandemics was hitting the province, with a high rate of the B.1.1.7 variant.
Methods:
The study was performed in the context of health surveillance at the workplaces. We monitored the SARS-CoV-2 infection and COVID-19 symptoms among HCWs classified by having received the entire vaccine schedule or not; the latter further classified in not vaccinated workers and workers who had received the first shot more than 14 days earlier. The SARS-CoV-2 infection was diagnosed by conventional RT-PCR on rhino-pharyngeal swabs, followed by gene sequencing in positive vaccinated HCWs. The cumulative incidence of infections in the period was normalised to 100,000 people.
Results:
At the end of the observation period, HCWs that had completed the full schedule were at lower infection risk than both unvaccinated HCWs and the workforce who had not yet gained the complete theoretical protection from the vaccine (by 2.4-folds). Overall, ninety-two SARS-CoV-2 infections were observed among HCWs, mostly among not protected workers (52 cases) but none of them showed symptoms requiring hospitalisation.
Conclusions:
The vaccination campaign effectively reduced the appearance of symptoms and the incidence of infections among vaccinated HCWs. Among vaccinated HCWs, gene sequencing was possible in five cases only, 4 B.1.1.7 and 1 B1.525 variants. The high rate of unsuccessful gene sequencing observed among infected vaccinated workers could be explained by a low viral burden. Vaccination for COVID-19 should be mandatory in occupational settings with a high infective risk.
Keywords: COVID-19 Pandemic, Vaccination, Follow-up, Health Surveillance
Introduction
Brescia, a city in Northern Italy, was strongly hit by the SARS-COV-2 pandemic since its beginning in Italy in February 2020. The Occupational Health Unit at the university hospital “ASST Spedali Civili di Brescia”, one of the leading European COVID-19 hospital and the local reference hub for such disease, was intensely engaged in the setting-up and management of preventive measures, including testing and trace strategies (1) and, from 27th December 2020 (European Vaccine Day) in the vaccination of healthcare workers (HCWs). Because of the high risk and their crucial role in tackling the COVID-19 pandemic, HCW were the first target population group and notably the first occupational group. HCWs were vaccinated with a two-dose (21-day interval) schedule of BNT162b2 vaccine (Pfizer®), which had shown an efficacy of 95% in the prevention of COVID-19 (2).
Given the limited time for vaccine development and the emergence of SARS-CoV-2 variants worldwide, the effectiveness of vaccines in the “real world” has yet to be demonstrated. Reports dealing with in-mass vaccination campaigns on HCWs in Israel and the USA (3-5) have recently highlighted encouraging data. The present study aimed to evaluate the effectiveness of BNT162b2 among healthcare workers, while a resurgence of pandemics was affecting the county of Brescia, with a high rate of variant B.1.1.7.
Methods
We performed the study relying on data gathered from health and epidemiological surveillance at the workplaces performed on the ASST “Spedali Civili di Brescia” workforce. Owing to the mandatory character of such an activity in Italy, the Ethics Committee’s approval was not necessary. However, all workers gave written consent to the vaccination and the data processing policy. All data were analysed anonymously. The follow-up covers the period between 25th January 2021 (when the first vaccinated workers theoretically gained protection, i.e. after at least seven days from the second dose) and 13th April 2021, 6904 HCWs (78% of the workforce) had gained protection. We monitored the SARS-CoV-2 infection and COVID-19 symptoms among HCWs classified as having received the full vaccine schedule (two shots – full vaccinated - infection detected more than seven days after the second shot), having received half vaccine schedule since more than 14 days (one shot - half vaccinated - infection occurring between 14 and 27 days after the first shot) and not vaccinated workers. The SARS-CoV-2 infection was diagnosed by conventional RT-PCR on rhino-pharyngeal swabs, as previously described, with minimal changes (6), followed by gene sequencing in positive vaccinated HCWs, as suggested by the relevant ECDC Technical Report (7). The incidence of infections in the period was normalised to 100,000 people to allow comparison whenever needed.
Dichotomous variables were analysed by contingency tables followed by the chi-square test and Odds Ratio (OR) along with 95% Confidence Interval (CI) calculation. Continuous variables with skewed distribution were compared by the Mann-Whitney test. The areas under the epidemiological curves (AUC) were evaluated by the GraphPad Prism 9.0 statistical package. All other calculations were performed by means of the IBM® SPSS® 26 software platform.
Results
Figure 1 shows the cumulative daily standardized (to 105 subjects) incidence of SARS-CoV-2 infections among not vaccinated and vaccinated HCWs, the latter classified as full and half vaccinated, as before specified. Noteworthy, during the last two weeks of February, the incidence of infection among partially vaccinated HCWs receiving one shot exceeded that of non-vaccinated HCWs. At the end of the observation period, HCWs who had received two shots were at lower infection risk than the other groups by 2.4 folds. In contrast, the infection rates among not vaccinated HCWs and those receiving only one shot were overlapping.
Figure 1.
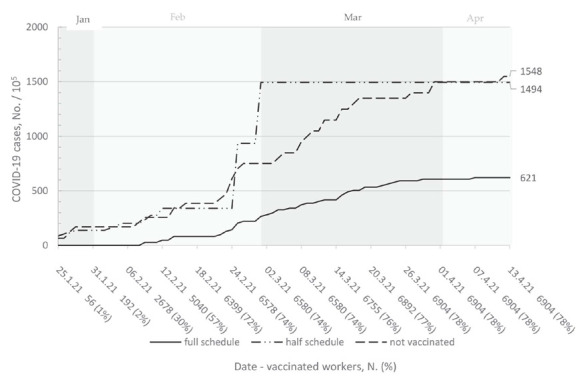
Cumulative standardised incidence (No./100,000/day) of SARS-CoV-2 positive cases among workers receiving the full vaccination (infection detected ≥7 days after the second shot), workers receiving half vaccination (infection detected between 14 and 27 days after the first shot) and not vaccinated workers, between January 25th and April 13th 2021. Total number of workers which had received the full schedule is reported on the horizontal axis along with its percentage.
The diverging trend from the general population and HCWs is shown in figure 2, that highlights the impact of the vaccination campaign among HCWs. Despite the national and regional restrictive measures enacted, the second wave of pandemics in Autumn caused a notable in-hospital rise of SARS-CoV-2 cases, which came to an end as soon as fully vaccinated HCW started to emerge among the workforce, around week 13th. Conversely, the third pandemic wave, starting in February 2021 and mainly supported by the SARS-CoV-2 B.1.1.7 variant, despite its magnitude, did not result in a similar rise among HCWs, supporting the protective vaccination (full schedule) effects. The area under the curve (AUC) of the standardized incidence was 2.1 times higher among HCWs than in the general population during weeks 5-13 (Dec-Jan). In contrast, it was 4.1 times lower in the period between weeks 13th and 23rd.
Figure 2.
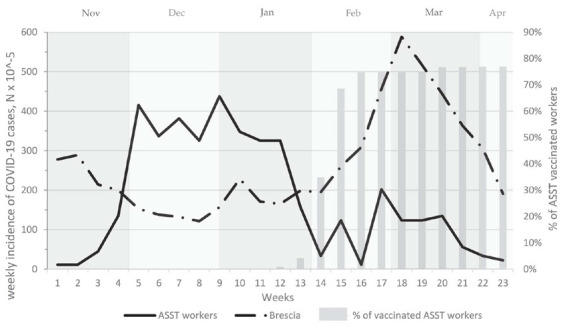
Weekly incidence per 100.000 people of SARS-CoV-2 positive cases among ASST workers and general population (lines, left axis) and percentage of workers who had received the full vaccination schedule (bars, right axis) between November 2nd and April 12th.
When comparing the 7 day-means of incident SARS-CoV-2 infections between groups (half and full vaccinated HCWs, not vaccinated HCWs and the general population) at the beginning, at the third pandemic peak and at the end of the observation, significant differences were apparent between full vaccinated HCWs and the general population at all the considered times (p<0.01). Interestingly, both half vaccinated and not vaccinated HCWs showed a significantly lower SARS-CoV-2 incidence as compared to the general population at the third wave pandemic peak and at the end of the observation period (p<0.05 for the comparison of half vaccinated vs general population at the peak; p<0.01 for all the other comparisons), when the percentage of the full vaccinated HCWs was ≥75%.
In the follow-up period, we observed 92 SARS-CoV-2 infections among HCWs, mostly among non-vaccinated workers. None of the HCWs required hospitalisation. The vaccine also showed a protective effect against symptom development (Table 1).
Table 1.
Distribution of COVID-19 symptoms in SARS-COV-2 positive healthcare workers (HCWs) classified by having or not completed the full vaccine schedule (two doses with a 21-day interval) in the period January 25th – April 13th 2021.
| HCWs who have completed vaccine schedule, No. (%) | SARS-CoV-2 positive HCWs, No. (%) | OR (95% CI) | |
| Symptomatic | Asymptomatic | ||
| Yes 40 (43%) | 15 (38%) | 25 (62%) | 0.38 (0.16-0.88) |
| No 52 (57%) | 32 (62%) | 20 (38%) | |
Interestingly, the overall rate of asymptomatic infection in the study period is about three times higher than that declared by the workforce who tested positive to the first SARS-CoV-2 serological screening performed in the same Hospital between April and July 2020 (8).
Among vaccinated HCWs, gene sequencing was successful in five cases only, 4 B.1.1.7 and 1 B1.525 variants. Overall, in the same period, in the Lombardy Region (10,025,503 inhabitants) there were 244,641 confirmed COVID-19 cases, 48,056 of which in the Province of Brescia (1,247,583 inhabitants); the prevalence of the B.1.1.7 variant rose from 70% (18th February) to 97% (28th March) (9).
Discussion
The present study confirms the protective effects of BNT162b2 against SARS-CoV-2 infection (3-6). Noteworthily, these results were observed while a recrudescent wave of the SARS-CoV-2 pandemic hit our country and particularly the Brescia local community, where the B.1.1.7 variant was highly prevalent. Thus, our results are in good agreement with those of a recent study showing that B.1.1.7 is not a neutralization escape variant that would be a major concern for current vaccines (10). Between 15th February and 15th April 2021, there were 1880 admissions for COVID-19 at the Hospital, with 211 deaths. None of the 92 HCWs positive for SARS-CoV-2 at the nasopharyngeal swab required hospitalization.
Data gathered from health surveillance show that the vaccination campaign was effective not only in reducing the appearance of symptoms but also in decreasing the incidence of infections among other HCWs. The incidence of infection among non-vaccinated HCWs was overlapping that of their colleagues receiving only one shot. In both cases, the incidence was much lower than in the general population in the same period, thus suggesting a positive interaction between in-mass vaccination and the complex of protective measures operating in the hospital.
Apparently, our data disagree with those from previous studies showing a reduced incidence of SARS-CoV-2 infection among HCWs two weeks after the first vaccine shot (3-5). In our series, HCWs receiving one shot and non-vaccinated workers show an overlapping cumulative incidence. Paradoxically, for a couple of weeks, the incidence of infection among HCWs receiving one shot was higher than that of non-vaccinated colleagues, possibly because of reduced observance of protective measures. Indeed, although the rise of specific IgGs is thought to be possible starting from the third week of infection (11), there is still lack of evidence to consider as immunized those individuals who have not completed the full vaccine schedule. To the best of our knowledge, the present study assesses the effectiveness of vaccination campaign performed with BNT162b2 according to the sole evidence of efficacy (2) available to date, thus considering as immunized against SARS-CoV-2 only those workers who had completed the two-shot schedule. The high rate of unsuccessful gene sequencing observed among infected vaccinated workers could be explained by a low viral burden, possibly related to a lower risk of SARS-CoV-2 transmission possibly conferred by vaccination.
A direct comparison with the trend observed in the general population is impossible because health surveillance would be asymmetrical. However, a comparison between the AUCs of the same HCWs relative to the AUCs of the general population in two different periods (Dec 2020-Jan 2021 and Feb 2021-Mar 2021, respectively) is interesting because the vaccination campaign is the only difference introduced in the health surveillance programme. The AUC of HCWs relative to that of the general population was 2.1 times higher before vaccination. It became 4.1 times lower during the vaccination campaign, thus supporting its effectiveness.
Occupational Health physicians are playing a pivotal role in the COVID-19 pandemic, fully collaborating with the management staff in the setup and management of all necessary primary (procedures, personal protective equipment, vaccine administration) and secondary (health surveillance) preventive and protective measures, including testing and tracing of infections. A further effort required by vaccination was to maintain high attention towards preventive and protective measures in vaccinated subjects who tend to underestimate them. At the time we were preparing this manuscript, the vaccine campaign involved about 90% of the Hospital workforce. A catch-up campaign is ongoing to vaccinate people not yet vaccinated due to individual situations (illness, pregnancy, other reasons) at the time of the main campaign.
Vaccination for COVID-19 should be made mandatory in all occupational contexts in which there is a high infection risk. In Italy, a Legislative Decree (44/2021) made the vaccination compulsory for HCWs. HCWs refusing vaccination should be temporarily suspended from work or, if possible, relocated in a job without any personal (both colleagues and patients) contact. Transition to the endemicity of SARS-CoV-2 is thought to be the most probable epilogue to this pandemic (12).
Acknowledgements:
we wish to thank Mrs Teresa Diaferia for her skilled and keen work on SARS-CoV-2 tracing.
Conflict of interest:
No potential conflict of interest relevant to this article was reported by the authors
References
- 1.Boffetta P, Violante F, Durando P, et al. Determinants of SARS-CoV-2 infection in Italian healthcare workers: a multicenter study. Sci Rep. 2021;11(1):5788. doi: 10.1038/s41598-021-85215-4. doi:10.1038/s41598-021-85215-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Polack FP, Thomas SJ, Kitchin N, et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N Engl J Med. 2020;383(27):2603–2615. doi: 10.1056/NEJMoa2034577. doi:10.1056/NEJMoa2034577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Benenson S, Oster Y, Cohen MJ, Nir-Paz R. BNT162b2 mRNA Covid-19 Vaccine Effectiveness among Health Care Workers [published online ahead of print, 2021 Mar 23] N Engl J Med. 2021:NEJMc2101951. doi: 10.1056/NEJMc2101951. doi:10.1056/NEJMc2101951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Daniel W, Nivet M, Warner J, Podolsky DK. Early Evidence of the Effect of SARS-CoV-2 Vaccine at One Medical Center. N Engl J Med. 2021 Mar 23:NEJMc2102153. doi: 10.1056/NEJMc2102153. doi: 10.1056/NEJMc2102153. Epub ahead of print. PMID: 33755374; PMCID: PMC8008752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Keehner J, Horton LE, Pfeffer MA, et al. SARS-CoV-2 Infection after Vaccination in Health Care Workers in California [published online ahead of print, 2021 Mar 23] N Engl J Med. 2021:NEJMc2101927. doi: 10.1056/NEJMc2101927. doi:10.1056/NEJMc2101927. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wölfel R, Corman VM, Guggemos W, Seilmaier M, Zange S, Müller MA, et al. Virological assessment of hospitalized patients with COVID-2019. Nature. 1 April, 2020 doi: 10.1038/s41586-020-2196-x. [DOI] [PubMed] [Google Scholar]
- 7. ECDC Technical report 3 Mar 2021. Methods for the detection and identification of SARS-CoV-2 variants, available at: https://www.ecdc.europa.eu/en/publications-data/methods-detection-and-identification-sars-cov-2-variants .
- 8.Comelli A, Focà E, Sansone E, et al. Serological Response to SARS-CoV-2 in Health Care Workers Employed in a Large Tertiary Hospital in Lombardy, Northern Italy. Microorganisms. 2021 Feb 25;9(3):488. doi: 10.3390/microorganisms9030488. doi: 10.3390/microorganisms9030488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. https://statistichecoronavirus.it/coronavirus-italia/ consulted on-line on April 1st 2021.
- 10.Shen X, Tang H, et al. SARS-CoV-2 variant B.1.1.7 is susceptible to neutralizing antibodies elicited by ancestral Spike vaccines. bioRxiv. 2021 Jan 29 doi: 10.1016/j.chom.2021.03.002. 2021.01.27.428516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Nandini S, Sundararaj SJ, Akihide R. Interpreting Diagnostic Tests for SARS-CoV-2. JAMA. 2020;323(22):2249–2251. doi: 10.1001/jama.2020.8259. doi:10.1001/jama.2020.8259. [DOI] [PubMed] [Google Scholar]
- 12.Lavine JS, Bjornstad OJ, Antia R. Immunological characteristics govern the transition of COVID-19 to endemicity. Science. 12 Feb 2021;371(6530):741–745. doi: 10.1126/science.abe6522. [DOI] [PMC free article] [PubMed] [Google Scholar]