

Abstract
Objectives
The objective of this study is to evaluate the effect of vitrectomy timing on anatomical and functional outcomes in cases with open-globe injuries caused by improvised explosive devices (IEDs).
Methods
A retrospective review of ocular injuries caused by IEDs was undertaken. The eyes were classified into four groups based on the timing of vitrectomy: early (Group-1; 2–4 days), delayed (Group-2; 5–7 days), late (Group-3; 8–14 days) and very late (Group-4; >14 days).
Results
The medical records of 351 patients were reviewed, and 212 patients were excluded. A total of 189 eyes of the remaining 139 patients were analysed. Visual improvements were statistically significant compared to the baseline values in all groups (p < 0.001). The early group showed better functional and structural outcomes when compared to the other groups. There was also no proliferative vitreoretinopathy (PVR) in the early group, while PVR was at the highest rate (25%) in the very late group and constituted the most significant reason for recurrent retinal detachment.
Conclusion
Both functional and anatomical outcomes were better in the early group. Delayed surgery may be indicated for some cases, but 1-week interval seems to be an optimal time-frame in open globe injuries due to IEDs.
Subject terms: Trauma, Eye manifestations, Outcomes research
Introduction
Explosive weapons can cause devastating injuries for the whole body. The impact of explosive weapons is highly correlated with the magnitude of the explosion and the proximity of potential victims. Victims of blast are usually severely injured due to the proximity of the explosion. The mechanism of trauma is primary blast injuries and objects colliding with high speed and energy [1]. Improvised explosive devices (IEDs) are strongly associated with severe ocular morbidity due to the effect of additional materials, such as glass and metallic objects that increase the lethal effects of shrapnel propelled by the explosion. They are commonly used during terrorist activities and irregular warfare.
Ocular trauma related to IEDs is often in the form of open-globe injury, in which both anterior and posterior segments are affected. In these cases, the suture closure of the globe should be performed as soon as possible. However, the management of posterior segment involvement is the main challenge for the ophthalmologist. It is highly controversial whether early or deferred vitrectomy is better for posterior segment involvement [2]. Previous reports showed that patients with the posterior segment involvement of ocular injuries tended to result in proliferative vitreoretinopathy (PVR) due to scar formation [3], which could lead to the development of phthisis bulbi if not operated. On the other hand, functional visual improvements can be achieved using pars plana vitrectomy (PPV) [4]. Some reports focus on the timing of vitreoretinal surgery in cases with ocular injuries [5, 6]. However, there is still no consensus on the timing of vitrectomy in these cases.
In this study, we aimed to present the effect of PPV timing on the functional and anatomic results of patients with deadly weapon-related open-globe injuries at a tertiary ocular trauma centre.
Methods
This retrospective study was approved by the institutional review and ethics boards of the Gülhane Training and Research Hospital, Ankara, Turkey and followed the tenets of the Declaration of Helsinki. We conducted a retrospective review of patients presenting with open-globe injuries caused by IEDs during security operations between April 2004 and 2018. We included only cases who underwent PPV due to open-globe injury related to IEDs. Primary open-globe repair was performed either at a regional hospital or at our department. Following urgent medical and/or surgical interventions at the scene of injury, all patients were transferred to our centre by an air ambulance. Systemic levofloxacin and topical moxifloxacin treatments were applied in all patients. Full-thickness wound of the eyewall (sclera, cornea or both) was defined as open-globe injury, and the Ocular Trauma Classification Group criteria were applied to divide the patients into groups according to the type (mechanism), grade (visual acuity at presentation) and zone (location and extent) of injury, and the presence or absence of a relative afferent pupillary defect [7]. In addition, the time to primary repair, subsequent surgical procedures and PPV were recorded. Fundus photography was performed depending on each patient’s general health status and media opacity. Posterior segment photos were captured by the Optos ultra-widefield system (Optomap, Dunfirmline, UK) (Fig. 1). Patients diagnosed with traumatic evisceration, optic nerve avulsion or optic nerve laceration due to trauma were excluded from the study. Those with delayed transportation of more than 7 days due to unstable general health status related to trauma were also excluded.
Fig. 1. Retinal images of the same patient with standart fundus camera and ultra-widefield fundus camera.

a Dilated fundus photography showing vitreous haemorrhage and incarcerated vitreous bands. b Ultra-widefield infrared image of the vitreous bands and exit wound.
Three-port PPV was performed using conventional 23- or 25-gauge instrumentation with/without scleral buckling. Lensectomy using aspiration or a vitrectomy probe was added if visualisation was obscured or the lens capsule was not intact. Core vitrectomy followed by central posterior vitreous detachment was achieved. Perfluorocarbon was used in cases with retinal detachment and intraocular foreign bodies (IOFB). Prophylactic chorioretinectomy (PCR) was performed if there was an exit wound or compromised choroid following IOFB removal. Intraoperative endolaser retinopexy was applied to any retinal break. IOFB removal covered through the entry port, an enlarged sclerotomy or the cornea according to dimensions of IOFB. Air–perfluorocarbon exchange was undertaken following a silicone oil injection of 1000 cs, 5000 cs or heavy silicone oil. Relaxing retinotomy was added to the surgery plan of cases with excessive PVR preventing retinal reattachment. Some surgical procedures were performed endoscopically or with temporary keratoprosthesis due to media opacities preventing the visualisation of the posterior segment.
According to Kuhn’s review, we divided the patients into four groups based on the time between the injury and vitrectomy: early (Group-1; 2–4 days), delayed (Group-2; 5–7 days), late (Group-3; 8–14 days) and very late (Group-4; >14 days) [8]. In addition, patients who underwent evisceration following unsuccessful surgical efforts were evaluated separately as Group-5.
Statistical analysis was performed using SPSS version 20.0 (SPSS, Chicago, IL, USA). Student’s t test was used to compare the parameters before and after surgery, and the one-way analysis of variance was used for intergroup comparisons. Test requirements were not met for univariate analysis and linear regression models. A binary logistic regression analysis was used to determine the relationship between the preoperative categorical variables and the final visual outcome. Statistical significance was set at p < 0.05.
Results
We reviewed the medical records of 490 patients admitted to our clinic for eye trauma due to explosions. The excluded cases were 175 patients with eye trauma related to non-IED explosive devices, 20 patients with superficial corneal foreign bodies that did not require PPV, 7 patients with traumatic evisceration, 5 with orbital foreign bodies but an intact globe, 2 with optic nerve avulsion and 2 with a delayed transfer due to the medical condition of patients being unsuitable for an air ambulance. As a result, 189 eyes of 139 patients (all male) were analysed. Forty-four (33.8%) right eyes and 34 (26.2%) left eyes were injured, whereas 51 (40%) patients experienced bilateral eye injuries. The average age was 26 ± 6 years. All eyes had open-globe injuries, while 48 (25.4%) had perforating eye injuries, 10 (5.3%) had penetrating eye injuries, 109 (57.7%) had IOFB and 22 (11.6%) had rupture related to blunt trauma due to the explosion of IEDs. The eyes with IOFB were evaluated in the IOFB group even if they had additional penetrating or perforating ocular injuries. The distribution of the eyes was similar between the groups (Fig. 2). None of the patients confirmed the use of eye protection at the time of injury. Of all patients, 109 (78.4%) presented to our clinic within 48 h of injury and 30 (21.6%) within 2–7 days after injury. These patients had been examined and undergone first ocular surgery at a local medical centre by an ophthalmologist but needed to wait for transportation due to safety issues. The ocular trauma scores and injury zones are shown in Tables 1 and 2, respectively.
Fig. 2.
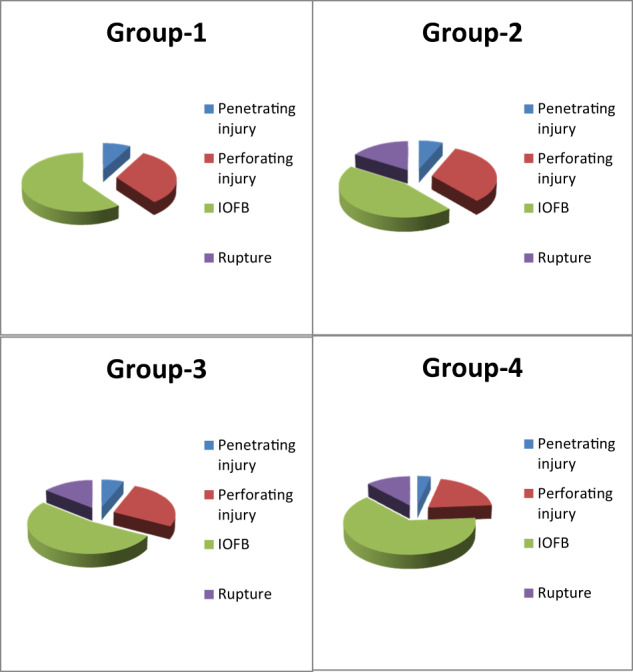
Distribution of the eyes with traumatic injury among the PPV timing groups.
Table 1.
Ocular trauma score calculation.
| Initial visual factor | Raw points |
| A—initial score (based on initial visual acuity) |
NPL = 60 PL/HM = 70 1/200 to 19/200 = 80 20/200 to 20/50 = 90 ≥20/40 = 100 |
| B—globe rupture | −23 |
| C—endophthalmitis | −17 |
| D—perforating injury | −14 |
| E—retinal detachment | −11 |
| F—relative afferent pupillary defect | −10 |
| Raw score sum | OTS category |
| 0–44 | 1 (36.5%) |
| 45–65 | 2 (29.1%) |
| 66–80 | 3 (16.4%) |
| 81–91 | 4 (10.1%) |
| 92–100 | 5 (7.9%) |
Adapted from Kuhn et al. [7]. The percentages of our patients are shown in the relevant category.
NPL non-perception of light, PL perception of light, HM hand movement.
Table 2.
Initial visual acuity after deadly weapon-related open-globe injuries.
| Zone of injury | Initial visual acuity | % | p | ORa (95% CI) | ||
|---|---|---|---|---|---|---|
| Better than 1.0 in logMAR | Worse than 1.0 in logMAR | |||||
| n | % | n | ||||
| 1 | 24 | 36.9 | 41 | 63.1 | <0.001 | 3.58 (1.72–7.44) |
| 2 | 5 | 71.4 | 2 | 28.6 | 0.005 | 10.37 (1.92–55.87) |
| 3 | 1 | 50 | 1 | 50 | 0.32 | 3.75 (0.22–61.49) |
| 1 + 2 | 5 | 3.2 | 26 | 96.8 | 0.42 | 0.65 (0.23–1.84) |
| 2 + 3 | 2 | 13.3 | 13 | 86.7 | 0.53 | 0.53 (0.11–2.49) |
| 1 + 2 + 3 | 1 | 1.7 | 57 | 98.3 | <0.001 | 0.03 (0.005–0.29) |
aThe relative odds of the variable having outcome of interest, compared with the other variables in the category.
Twenty-one patients (11%) underwent evisceration due to irreparable posterior segment defects by blast munitions and fragments traversing the eye. This procedure was undertaken within the first 10 days after injury for 11 (52%) patients and within a month following unsuccessful surgical efforts for the remaining 10 (48%). Patients that underwent evisceration following unsuccessful PPV surgery were included in the corresponding to PPV timing group. The initial details of the patients undergoing evisceration are shown in Table 3. Thirteen patients (7%) required one surgical procedure to recover, while 2 patients (1%) required more than ten operations. IOFB was seen in 109 patients (58%), and had both intraocular and intraorbital foreign bodies in 11 (6%) patients. In 16 of IOFB cases, there was retinal penetration, and the choroid was located at the posterior pole (33% nasally and 51% temporally). All IOFBs were removed, but only six patients with intraorbital foreign bodies underwent the surgical removal procedure. Five of these patients were inoperable due to the deep location of the foreign bodies in the orbit.
Table 3.
Clinical characteristics of patients that underwent evisceration following unsuccessful surgical efforts.
| Initial vision | |
| NPL | 100% |
| OTS | |
| 25 | 85.6% |
| 35 | 4.80% |
| 36 | 4.80% |
| 37 | 4.80% |
| Zone 3 injury | 100% |
| Type of injury | |
| Perforating | 95.20% |
| Penetrating | 4.80% |
All eyes were in OTS category 1 and had injuries involving zone 3.
All of the patients underwent globe exploration and primary open-globe repair within 24 h, and lens removal was performed in 21 (11%) of these patients during the same session as primary open-globe repair. Eight (4%) patients underwent penetrating keratoplasty (PKP) following the use of a temporary keratoprosthesis during the first PPV surgery session. Six (3%) patients required endoscopic PPV due to visualisation problems (Table 4). We did not observe any postoperative complications in the eyes that had been operated on using endoscopic PPV. However, among the patients that underwent keratoprosthesis-assisted PPV, two eyes developed graft failure and one eye required glaucoma shunt surgery. There was no graft failure in the eyes in which PKP was undertaken following other surgical procedures to restore the vision.
Table 4.
Surgical procedures of pars plana vitrectomy in the study population.
| Endoscopic (n = 6) |
Keratoprosthesis (n = 8) |
Conventional (n = 175) |
|
|---|---|---|---|
| Initial VA | |||
| Grade 1 (≥20/40) | – | – | 19 (10.8%) |
| Grade 2 (20/50 to 20/200) | – | – | 27 (15.4%) |
| Grade 3 (19/200 to 1/200) | – | – | 16 (9.1%) |
| Grade 4 (HM/LP) | 3 (50%) | 7 (87.5%) | 84 (46.8%) |
| Grade 5 (NLP) | 3 (50%) | 1 (12.5%) | 29 (17.9%) |
| Final VA | |||
| Grade 1 (≥20/40) | 1 (16.6%) | – | 72 (41.1%) |
| Grade 2 (20/50 to 20/200) | – | 1 (12.5%) | 26 (14.8%) |
| Grade 3 (19/200 to 1/200) | 1 (16.6%) | 1 (12.5%) | 17 (9.7%) |
| Grade 4 (HM/LP) | 3 (50%) | 1 (12.5%) | 26 (14.8%) |
| Grade 5 (NLP) | 1 (16.6%) | 5 (62.5%) | 34 (19.6%) |
| Zone I involvement | 6 (100%) | 8 (100%) | 152 (86%) |
| OTS 1 | 4 (66.7%) | 6 (75%) | 59 (33.7%) |
| OTS 2 | 1 (16.7%) | 1 (12.5%) | 53 (30.3%) |
| OTS 3 | 1 (16.7%) | 1 (12.5%) | 29 (16.6%) |
| OTS 4 | – | – | 19 (10.9%) |
| OTS 5 | – | – | 15 (8.6%) |
VA visual acuity, HM hand movements, LP light perception, NLP no light perception.
Preoperative visual acuity in logMAR was 1.90 ± 1.61 in Group-1, 2.26 ± 1.59 in Group-2, 2.75 ± 1.29 in Group-3 and 2.70 ± 1.47 in Group-4 (p > 0.05). There was a statistically significant visual improvement compared to the baseline values in all groups over 12 months (p < 0.001) (Fig. 3). The visual improvement also statistically significantly differed between all groups (p < 0.05). The analysis of the visual improvements between the groups showed that the statistically significant differences were caused by the improved outcomes in Group-1 compared to the other groups. There was no incidence of PVR development in Group-1, while the PVR rates were calculated as 7%, 15% and 7% for Group-2, Group-3 and Group-4, respectively. The ophthalmic examination revealed retinal detachment in 131 (69%) patients at baseline. The use of endotamponade during surgery was mostly seen in Group-3 and Group-4. The rate of patients not requiring endotamponade during surgery was 52% in Group-1, 31% in Group-2 and 20% in Group-3 and Group-4. Retinal reattachment was achieved in 90 of 131 eyes (69%). The highest surgical success was obtained from Group-1. Anatomical improvement outcomes statistically significantly differed between the groups (p < 0.001). This was related to the high PVR rates (15%) causing recurrent retinal detachment and multiple surgery requirements in the late group (Fig. 4). A binary logistic regression analysis was performed to analyse the association between the final visual acuity (FVA) and preoperative factors (Table 5). The results showed that OTS category 1 (p = 0.018) and zone 3 injuries (p = 0.006) were associated with an FVA of <1.0 in logMAR. Twenty-one eyes with surgical failure subsequently underwent evisceration surgery due to irreparable posterior segment problems. Ten (5%) eyes became phthisic and lost light perception. Eight patients (4%) had scleral buckling surgery following the surgical failure of PPV. Only four patients, two in Group-1 and two in Group-2, achieved retinal reattachment. The median time from the injury to the scleral buckling procedure was 186 days. Three patients had an Ahmed valve device implanted due to the failure of maximal tolerated medical therapy for traumatic glaucoma, and none of the patients had a diagnosis of endophthalmitis during the routine follow-ups.
Fig. 3. Baseline and postoperative visual improvements.
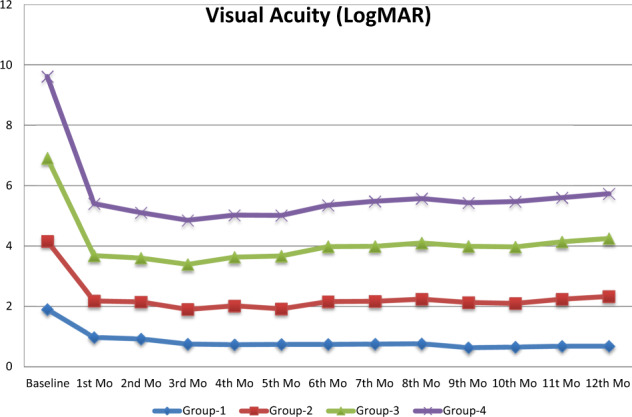
Patients with delayed presentation and surgery had worse visual acuity at baseline. Group-1 (early), Group-2 (delayed), Group-3 (late), Group-4 (very late).
Fig. 4. The 6th-month fundus images of a patient in the late group.

a Massive vitreous haemorrhage with no IOFB or retinal laceration. There is subretinal fibrosis with no tPVR activity. b, c The fundus image of another patient in the late group presenting with IOFB and retinal laceration. The image of PVR following multiple surgical operations with the use of endotamponade.
Table 5.
Binary logistic regression analysis between the final visual acuity and preoperative factors.
| B | p | OR | CI (95%) | |
|---|---|---|---|---|
| IVA | 0.38 | 0.086 | 1.47 | 0.94–2.28 |
| PPV timing (<7 days) | 0.22 | 0.71 | 1.24 | 0.38–4.01 |
| Retinal detachment | 0.9 | 0.18 | 0.4 | 0.10–1.54 |
| IOFB | 0.17 | 0.73 | 0.83 | 0.30–2.29 |
| Zone 3 injury | 1.34 | 0.006 | 3.82 | 1.47–9.29 |
| OTS 1 | 1.35 | 0.018 | 3.89 | 1.26–11.98 |
IVA initial visual acuity, IOFB intraocular foreign body, OTS ocular trauma score, B regression coefficient, OR odds ratio, CI confidence interval.
Statistically significant correlations (p < 0.05) were written in italics.
Discussion
Performing primary open-globe repair as early as possible is the standard practice worldwide; however, the timing of vitrectomy for open-globe injuries involving the posterior segment has remained controversial for decades. Clinical studies that have investigated the early or delayed timing of vitrectomy to date have only limited value due to their retrospective nature. In addition, the wide range of cases related to trauma makes it very difficult to assess risk factors or treatment modalities for a better clinical outcome. A randomised trial with a large number of patients and a long follow-up period would be ideal; however, this seems to be unlikely in the short term.
Following primary open-globe repair, the main concerns regarding visual and functional outcomes are post-traumatic endophthalmitis, retinal detachment and PVR [2, 9]. A previous study from our department reported post-traumatic culture-positive endophthalmitis rates as 9.5% following deadly weapon-related open-globe injuries [10]. In that study, lens disruption and grade 4 injuries (presenting visual acuity worse than 5/200 to light perception) were reported to be clinical features associated with an increased risk of infection. In our study, 11% of the patients underwent evisceration due to irreparable damage. We excluded these patients because we could not be certain whether they would develop endophthalmitis, and thus our rate of endophthalmitis was zero. Delayed timing of primary globe repair has been previously associated with an increased risk of infection [11]. Colyer et al. [12] reported that PPV and IOFB removal could be delayed if primary closure was undertaken within hours of injury, and topical/systemic antibiotics were initiated. In that review, there were no cases of endophthalmitis among 79 patients who underwent early closure and received topical and oral antibiotics. In another previous study conducted in our clinic, Staphylococcus epidermidis was identified as the most common isolate, suggesting contamination. These informative results indicate the importance of combat medics in the field applying certain preventive measures. A wide range of systemic and topical antibiotic prophylaxis and proper first intervention within hours of injury are good examples of preventive medicine practices. In addition, a previous case series of ocular injuries related to explosive materials reported no endophthalmitis [12–15]. All these reports suggest that hot, metallic, projectile particles may be associated with endophthalmitis less frequently. An endophthalmitis vitrectomy study suggests that routine immediate PPV is not necessary for patients with better than light perception vision at presentation [16]; however, we know that PVR is more common in cases with endophthalmitis. Furthermore, multiple breaks, large retinal tears and vitreous haemorrhage are usually reported in seriously injured eyes. These factors are known to create a high risk in terms of PVR development. Essex et al. [17] showed that the infection frequency steadily increased with each hour’s delay of surgery. Blanch et al. reported that every 24 h of delay between the injury and primary open-globe repair was associated with a reduction in the predicted visual acuity of 0.37 (95% CI: 0.14–0.60) logMAR [18]. On the other hand, early PPV causes a higher risk of haemorrhage, and the induction of posterior vitreous detachment may be challenging in the absence of spontaneous resolution within that timeframe. Complete core vitrectomy followed by peripheral vitreous removal and endotamponade use is also challenging. It has been suggested that more than 24 h delay in primary open-globe repair causes a fourfold increase in the risk of endophthalmitis [19].
The second major factor determining visual prognosis following an open-globe injury is PVR development. Retinal lesions, lens disruption and vitreous haemorrhage are factors providing a medium for migrating cells to stimulate PVR [9]. IOFB and its dimensions are the main risk factors because the larger foreign body has higher penetrating energy. This increases the possibility of reaching and injuring the retina, and higher amounts of proteinaceous lens material mixing with a higher amount of blood in the vitreous. It is also known that PVR development occurs as a result of fibrous and RPE proliferation linked to posterior segment lesions [20]. In a study by Ozdek et al. [21], PCR with PPV was reported to be effective in perforating eye injuries and IOFB-related retinal lesions. The authors performed the removal of the underlying necrotic choroid and all other tissues using a vitrectomy cutter followed by endodiathermy. In our study, 64% of the patients had IOFBs, and 43% of these patients also had retinal lesions related to IOFB. The remaining IOFBs were steady in the vitreous gel. The patients with retinal lesions (retained in the choroid/sclera or exit wounds due to perforation) underwent PPV with chorioretinectomy (Fig. 5). None of the patients in Group-1 (2–4 days) developed PVR. In Group-2 (5–7 days), the PVR rate was 7%, and all of these patients had IOFBs retained in the choroid located nasally to the optic disc. The highest PVR rate (15%) was found in Group-3 (8–14 days). Chorioretinectomy for retinal wounds located at the posterior pole remains controversial since a pigmentary reaction is often seen surrounding the PCR site. The distance of the lesion to the fovea or a major vessel is a major challenge in deciding whether to apply laser treatment or diathermy. On the other hand, the outcomes of patients who undergo late chorioretinectomy are known to be superior to those who do not undergo this procedure, but far inferior to those who undergo PCR [3]. In our cases, we performed PCR; however, tissue debridement and laser/endodiathermy use were limited in cases with IOFBs located at the posterior pole. These cases developed PVR with subretinal fibrous bands probably due to the limited removal of the inflammatory components. In Group-4 (>14 days), the PVR rate was 7%, which was lower compared to the late surgery group and could be misleading. However, the very late surgery group mostly comprised of patients with stable ocular conditions but more critical general health status related to IED injuries. In addition, these PVR rates belonged not only to patients that underwent PCR, but also those that did not undergo this procedure. In a subgroup analysis, we evaluated the PVR rates among the patients that underwent PCR and determined these rates to be 0% for Group-1, 9% for Group-2, 20% for Group-3 and 25% for Group-4. Exit wounds located more posteriorly are prone to developing PVR, but in our study, nasally located IOFBs were also prone to this complication even after PCR.
Fig. 5. Preoperative and postoperative retinal images of a patient with IOFB.

a The baseline fundus images of a patient with IOFB and retinal laceration. *The retina and choroid are damaged, and fibroblastic activity is seen. b The fundus image of the same patient following PPV, IOFB removal, and PCR with three rows of endolaser surrounding the zone.
Ghoraba et al. [22] reported a prophylactic scleral encircling band combined with PPV for the management of perforating ocular injury. They positioned the band to support the vitreous base. In our study, eight patients underwent additional scleral buckling surgery. Fifty per cent of all patients had reattached retinas, and these cases were all in Group-1 (n = 2) and Group-2 (n = 2) with no development of PVR in the scleral buckling session. The remaining 50% of these patients were in the late group that developed PVR, and for these cases, neither PPV nor scleral buckling was successful.
Post-traumatic PVR is one of the major prognostic factors mostly related to the level of initial ocular injury and timing of surgery. Surgical timing based on the nature of initial injury in each patient is highly recommended. Han et al. [5] described the individualised timing of PPV for ocular trauma. Zone 3 retinal laceration and perforation are major risk factors. In our study, all patients who developed PVR were above the cut-off value reported by Han et al. (0.589). In addition, in Group-1, 16% of the cases were above the cut-off value but these patients did not develop PVR, which similarly underlines the importance of the timing and quality of the surgery. We observe a wide spectrum of both anterior and posterior segment injuries, which lead to visual loss in a variety of circumstances. Therefore, the determination of the extent of the injury for formulating an individual treatment plan is crucial. There is also a need for standardised terminology to predict FVA while deciding on a treatment plan. In our study, we presented the negative impact of OTS category 1 (p = 0.018; OR: 3.89) and zone 3 injuries (p = 0.006; OR: 3.82) on predicting FVA. Guven et al. [23] also described OTS category 1 and zone 3 injury as having a negative effect on FVA in open-globe injuries.
Prevention is the best course of management for combat ocular trauma [24]. Soldiers complain that the current protective eyewear equipment becomes foggy and obstruct their ability while fighting in urban conflict. Our study revealed that none of the patients had been wearing their eye protection. This may be related to amnesia from traumatic injury but the lack of documentation by primary responders is a limitation. Military personnel are equipped with protective eyewear but it is crucial if this equipment was on their face rather than on their helmet. Breeze et al. [25] stated that the essential cover of the brain and eyes reduced the incidence of combat ocular injuries, and this can be achieved in all directions using a combination of a helmet and a visor.
The main limitation of our study was a deficit in recording significant information, including foreign body dimensions and the distance between retinal lesions and the posterior pole in cases where multiple PCR procedures were performed for more than one retinal lesion. This was related to the retrospective nature of the study and the difficulty in examining cases where treatment for life-threatening injuries was ongoing.
Conclusion
This is the first study concerning the effect of PPV timing on IED-related open-globe injuries in the literature. We believe that a proper first intervention in terms of sterility with systemic antibiotic prophylaxis is the first step to prevent endophthalmitis. Early or delayed surgery (within 1 week) with PCR is the best choice but injury-related intraoperative complications should be handled by an experienced eye trauma surgeon in an experienced clinic with the support of a team of experienced healthcare professionals. Another important finding of our study is that there is an increased possibility of corneal donor failure if PKP is combined with other ocular surgery. It is better to wait for a sufficient length of time to reduce inflammation generated by trauma and other surgical procedures. All patients that undergo IOFB removal should be carefully followed up for at least 6 months for the early detection and treatment of PVR.
Summary
What was known before
Chorioretinectomy is a surgical method performed at limited centres.
Recurrent retinal detachment, endophthalmitis and traumatic PVR are the most common reasons for surgical failure in open-globe injuries.
Endophthalmitis is rare for eyes with explosive material-related ocular injuries.
What this study adds
Vitrectomy should not be postponed for more than 1 week for open-globe injuries.
Prophylactic chorioretinectomy should be performed during the 1st week if needed especially for posterior and nasal retinal lacerations.
Improvised explosive devices cause ocular injuries with metallic and non-metallic particles. Endophthalmitis is rare even though with non-metallic IOFBs after explosion-related ocular injuries.
Data availability
The data sets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
Compliance with ethical standards
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Sobaci G, Mehmet Mutlu F, Bayer A, Karagul S, Yildirim E. Deadly weapon-related open-globe injuries outcome assessment by the ocular trauma classification system. Am J Ophthalmol. 2000;129:47–53. doi: 10.1016/S0002-9394(99)00254-8.. [DOI] [PubMed] [Google Scholar]
- 2.Erdurman FC, Hurmeric V, Gokce G, Durukan AH, Sobaci G, Altinsoy HI. Ocular injuries from improvised explosive devices. Eye. 2011;25:1491–8. doi: 10.1038/eye.2011.212.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kuhn F, Schrader W. Prophylactic chorioretinectomy for eye injuries with high proliferative-vitreoretinopathy risk. Clin Anat. 2018;31:28–38. doi: 10.1002/ca.22906.. [DOI] [PubMed] [Google Scholar]
- 4.Ghoraba HH, Ellakwa AF, Ghali AA, Abdel Fattah HM. Long-term results of 360˚A scleral buckling and vitrectomy with silicone oil tamponade for management of gunshot perforating ocular injury. Eye. 2012;26:1318–23. doi: 10.1038/eye.2012.150.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Han L, Jia J, Fan Y, Yang L, Yue Z, Zhang W, et al. The Vitrectomy timing individualization system for ocular trauma (VtiSot) Sci Rep. 2019;9:12612. doi: 10.1038/s41598-019-48862-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Yu H, Li J, Yu Y, Li G, Li D, Guan M, et al. Optimal timing of vitrectomy for severe mechanical ocular trauma: a retrospective observational study. Sci Rep. 2019;9:18016. doi: 10.1038/s41598-019-54472-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kuhn F, Maisiak R, Mann L, Mester V, Morris R, Witherspoon CD. The ocular trauma score (OTS) Ophthalmol Clin North Am. 2002;15:163–5. doi: 10.1016/S0896-1549(02)00007-X.. [DOI] [PubMed] [Google Scholar]
- 8.Kuhn F. The timing of reconstruction in severe mechanical trauma. Ophthalmic Res. 2014;51:67–72. doi: 10.1159/000351635.. [DOI] [PubMed] [Google Scholar]
- 9.Jonas JB, Knorr HL, Budde WM. Prognostic factors in ocular injuries caused by intraocular or retrobulbar foreign bodies. 2000;107:823–8. 10.1016/S0161-6420(00)00079-8. [DOI] [PubMed]
- 10.Sabaci G, Bayer A, Mutlu FM, Karagül S, Yildirim E. Endophthalmitis after deadly-weapon-related open-globe injuries: risk factors, value of prophylactic antibiotics, and visual outcomes. Am J Ophthalmol. 2002;133:62–9. doi: 10.1016/S0002-9394(01)01320-4.. [DOI] [PubMed] [Google Scholar]
- 11.Thompson WS, Rubsamen PE, Flynn HW, Jr, Schiffman J, Cousins SW. Endopthalmitis after penetrating trauma. Risk factors and visual acuity outcomes. Ophthalmology. 1995;102:1696–701. doi: 10.1016/S0161-6420(95)30807-X. [DOI] [PubMed] [Google Scholar]
- 12.Colyer MH, Weber ED, Weichel ED, Dick JS, Bower KS, Ward TP, et al. Delayed intraocular foreign body removal without endophthalmitis during Operations Iraqi Freedom and Enduring Freedom. Ophthalmology. 2007;114:1439–47. doi: 10.1016/j.ophtha.2006.10.052.. [DOI] [PubMed] [Google Scholar]
- 13.Blanch RJ, Bindra MS, Jacks AS, Scott RA. Ophthalmic injuries in British Armed Forces in Iraq and Afghanistan. Eye. 2011;25:218–23. doi: 10.1038/eye.2010.190.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Thach AB, Ward TP, Dick JS, 2nd, Bauman WC, Madigan WP, Jr, Goff MJ, et al. Intraocular foreign body injuries during Operation Iraqi Freedom. Ophthalmology. 2005;112:1829–33. doi: 10.1016/j.ophtha.2005.04.024. [DOI] [PubMed] [Google Scholar]
- 15.Weichel ED, Colyer MH. Combat ocular trauma and systemic injury. Curr Opin Ophthalmol. 2008;19:519–25. doi: 10.1097/ICU.0b013e3283140e98.. [DOI] [PubMed] [Google Scholar]
- 16.Endophthalmitis Vitrectomy Study Group. Results of the endophthalmitis vitrectomy study. A randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Arch Ophthalmol. 1995;113:1479–94. doi: 10.1001/archopht.1995.01100120085015.. [DOI] [PubMed] [Google Scholar]
- 17.Essex RW, YI Q, Charles PG, Allen PJ. Post-traumatic endophthalmitis. Ophthalmology. 2004;111:2015–22. doi: 10.1016/j.ophtha.2003.09.041.. [DOI] [PubMed] [Google Scholar]
- 18.Blanch RJ, Bishop J, Javidi H, Murray PI. Effect of time to primary repair on final visual outcome after open globe injury. Br J Ophthalmol. 2019;103:1491–4. doi: 10.1136/bjophthalmol-2017-311559. [DOI] [PubMed] [Google Scholar]
- 19.Thompson JT, Parver LM, Enger CL, Mieler WF, Liggett PE. Infectious endophthalmitis after penetrating injuries with retained intraocular foreign bodies, National Eye Trauma System. Ophthalmology. 1993;100:1468–74. doi: 10.1016/S0161-6420(93)31454-5.. [DOI] [PubMed] [Google Scholar]
- 20.Kruger EF, Nguyen QD, Ramos-Lopez M, Lashkari K. Proliferative vitreoretinopathy after trauma. Int Ophthalmol Clin. 2002;42:129–43. doi: 10.1097/00004397-200207000-00015.. [DOI] [PubMed] [Google Scholar]
- 21.Ozdek S, Hasanreisoglu M, Yuksel E. Chorioretinectomy for perforating eye injuries. Eye. 2013;27:722–7. doi: 10.1038/eye.2013.18.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ghoraba HH, Zaky AG, Ellakwa AF. Long-term follow-up of vitrectomy with or without 360° encircling buckle, for rhegmatogenous retinal detachment due to inferior retinal breaks. Clin Ophthalmol. 2016;10:1145–51. doi: 10.2147/OPTH.S102082.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Guven S, Durukan AH, Erdurman C, Kucukevcilioglu M. Prognostic factors for open-globe injuries: variables for poor visual outcome. Eye. 2019;33:392–7. doi: 10.1038/s41433-018-0218-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Robert S. The injured eye. Philos Trans R Soc. 2011;366:251–60. [DOI] [PMC free article] [PubMed]
- 25.Breeze J, Tong DC, Powers D, Martin NA, Monaghan AM, Evriviades D, et al. Optimising ballistic facial coverage from military fragmenting munitions: a consensus statement. Br J Oral Maxillofac Surg. 2017;55:173–8. doi: 10.1016/j.bjoms.2016.10.018. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data sets generated and/or analysed during the current study are available from the corresponding author on reasonable request.