

Abstract
BACKGROUND:
Hyperoxia (HO) causes kidney injury in preterm infants; however, whether these effects are modifiable is unknown. We hypothesized that administration of exogenous soluble Klotho, a kidney-derived antioxidant, would attenuate HO-induced kidney injury during postnatal nephrogenesis in rats.
METHODS:
Sprague Dawley neonatal rats assigned to normoxia (21% O2) or HO (85% O2) groups from postnatal day (P) 1 to 21 were randomly assigned to receive alternate day intraperitoneal injections of recombinant Klotho or placebo for 3 weeks. They were recovered in normoxia for an additional 3 weeks and sacrificed at 6 weeks. Renal artery resistance and pulsatility indices, tubular injury scores, glomerular area, and renal antioxidant capacity were assessed.
RESULTS:
Rodents exposed to HO during postnatal nephrogenesis had reduced kidney Klotho expression, glomerulomegaly, and higher tubular injury scores. Exogenous Klotho administration improved renal perfusion as indicated by decreases in both resistance and pulsatility indices and increased antioxidant enzyme expression.
CONCLUSIONS:
HO exposure during postnatal nephrogenesis in rodents results in a decline in kidney Klotho expression, decreased renal perfusion, enlarged glomerular size, and tubular injury. The exogenous administration of Klotho attenuated HO-induced kidney injury and augmented antioxidant capacity.
INTRODUCTION
Preterm infants are born during active nephrogenesis resulting in a reduced complement of nephrons, clinically encompassed under the diagnosis of “oligonephropathy of prematurity.”1,2 This nephron deficit, coupled with a hostile extrauterine environment and nephrotoxic insults, plays a role in the programming of chronic kidney disease (CKD) and ultimately reduced longevity for preterm born individuals.3–6 In addition, preterm infants are often treated with supplemental oxygen and high oxygen levels relative to the hypoxic intrauterine environment,7 which results in oxidative stress during the neonatal period.8,9 Owing to the low levels of antioxidants inherent to neonates,10,11 preterm infants are particularly susceptible to cellular injury and cell death via free radicals when the antioxidant capacity of the neonate is overwhelmed. In humans, kidney development is normally completed by 34–36 weeks’ gestation.12,13 The exposure to high oxygen levels, while nephrogenesis is still ongoing, has been proposed as one factor that may impair development and/or injure the immature kidneys of preterm neonates.13
Few studies have focused on the short- and long-term impact of hyperoxia (HO) exposure on the developing kidney. Some have reported that increased oxidative stress adversely affects glomerular and tubular maturity.14 While studies have tried to understand the effects and mechanisms by which HO induces kidney injury, none have used antioxidant therapies to determine whether these renal effects are reversible or preventable. This is in contrast to the many animal studies published that have demonstrated positive results using various antioxidant agents and mesenchymal stem cell therapies to ameliorate HO-related lung injury of prematurity.15–17
Klotho is a single-pass transmembrane protein that is highly expressed in the kidney. It was originally identified incidentally when disruption of the protein resulted in premature multiorgan failure resembling aging.18 Membrane Klotho is proteolytically cleaved, and its transcript undergoes alternative splicing to generate a soluble form, which has endocrine and antioxidant properties. In physiologic conditions, the kidney is the primary source of circulating soluble Klotho.19 Soluble Klotho exerts multiple actions, including antioxidation, anti-senescence, pro-autophagy, anti-apoptosis, anti-fibrosis, and anti-insulin actions.20,21 Klotho has been extensively studied in the context of CKD, which is considered a state of “pan-Klotho” deficiency.22 It has also been studied as a novel therapeutic agent in the prevention or attenuation of kidney injury in animal models of acute kidney injury (AKI).23 Supplementation of exogenous Klotho and/or upregulation of endogenous Klotho production may confer renoprotection due to its putative antioxidation properties.24 This effect, however, has not been tested in injury models during active nephrogenesis.
We hypothesized that the administration of exogenous Klotho would attenuate HO-induced glomerular and tubular injury via improved antioxidant capacity in a rodent model of postnatal nephrogenesis. The aims of our study were (1) to study the effects of HO at the time of nephrogenesis on glomerular and tubular integrity, (2) to investigate the effects of HO on kidney Klotho expression, (3) to evaluate whether the administration of exogenous Klotho would modify HO-induced kidney injury, and (4) to assess whether Klotho administration enhances kidney antioxidant capacity.
MATERIALS AND METHODS
Animals
Pregnant Sprague Dawley rats were purchased from Charles River Laboratories (Wilmington, MA). Animals were treated according to the National Institute of Health (NIH) guidelines for the use and care of laboratory animals following approval of the study protocol by the University of Miami Animal Care and Use Committee, protocol approval number: 15-168.
Experimental design
Sprague Dawley neonatal rats assigned to normoxia (21% O2) or HO (85% O2) groups from postnatal day (P) 1 to 21 were randomly assigned to receive alternate day intraperitoneal injections of recombinant mouse Klotho prepared by dissolving in phosphate-buffered solution (PBS) (30 mcg/kg; R&D Systems, Minneapolis, MN) or placebo (PL; PBS) from P1. Rats were recovered in normoxic conditions for an additional 3 weeks. Oxygen exposure was achieved in a Plexiglas chamber by a flow-through system and the oxygen level inside the Plexiglas chamber was monitored continuously with Maxtec oxygen analyzers (model OM25-RME, Salt Lake City, UT). Mothers were switched every 48 h between the HO and normoxia chambers to prevent lung damage. Litter size was adjusted to ten pups to control for the effect of litter size on nutrition and growth.
Histological examination
Kidneys were weighed at 6 weeks, fixed in formaldehyde, and paraffin-embedded. Serial 5 pm sections from the kidney (in the coronal plane) were stained with hematoxylin and eosin and examined by light microscopy. For each section, multiple digital microphotographs10–15 were taken at ×2.5 and ×40 magnification to assess the glomerular area and tubular injury scoring.
Renal function
Serum creatinine was measured at the time of sacrifice in all pups at 6 weeks.
Glomerular measures
Under ×40 magnification, 10 mature glomeruli were selected randomly for histomorphometry. Using the Image J analysis software, the boundary of the Bowman’s capsule of each glomerulus (10 per kidney) and the average glomerular crosssectional area were determined by a nephrologist trained on use of the software program.25
Tubular injury score
A pathologist blinded to the treatment group examined at least 40 cortical fields at ×100 magnification. Tubular injury was defined by any of the following features: tubular dilatation, tubular atrophy, vacuolization, degeneration and sloughing of tubular epithelial cells, or thickening of tubular basement membrane. The scoring system used was as follows: 0 = no tubular injury; 1 = <10% of tubules injured; 2 = 10–25% of tubules injured; 3 = 26–50% of tubules injured; 4 = 51–75% of tubules injured; and 5 = >75% of tubules injured.20
Renal Doppler measurements
Pulse-wave Doppler measurement was performed in the right renal artery (RRA) of rats under anesthesia (1% isoflurane) using the Vevo2100 imaging system (VisualSonics, Toronto, Canada) at 6 weeks of life. The data were analyzed with the VevoLab 1.7.1 software (VisualSonics). Peak systolic velocity (PSV), peak diastolic velocity (PDV), and velocity-time integral (VTI) measurements were used to calculate the RRA resistive index (RRA RI = (PSV – PDV)/PSV) and RRA pulsatility index (RRA PI = (PSV – PDV)/ VTI, mean velocity). All measurements were performed excluding the respiration peaks and obtained in triplicate and the mean values were used for data analysis.
Quantitative real-time polymerase chain reaction (RT-PCR)
Total RNA was isolated from kidney tissue stabilized in RNAlater using the RNeasy Midi Kit (Qiagen, Valencia, CA) as per the manufacturer’s instructions. Tissues were disrupted and homogenized using a rotor-stator homogenizer (Ultra-Turrax T8, IKA Works, Wilmington, NC). Samples were centrifuged for 15 min at 12,000 × g at 4°C. The upper aqueous phase was transferred to a new collection tube, and an equal volume of 70% ethanol was added and vortexed. Following step centrifugation at 10,000 × g, RNA was eluted using 30–50 μl RNase-free water. RNA purity and concentration were determined by NanoDrop 1000 Spectrophotometer (Thermo Fisher Scientific, Waltham, MA). Total RNA (2 μg) was reverse transcribed using a first-strand cDNA synthesis kit according to the manufacturer’s protocol (Superscript VI VILO Master Mix with ezDNase Ensyme, Thermo Fisher Scientific). This kit contains ezDNase enzyme, which is a double-strand-specific thermolabile DNase that is used to remove gDNA contamination from template RNA prior to the RT reaction. Real-time RT-PCR using TaqMan™ Fast Advanced Master Mix (Applied Biosystems, Foster City, CA) was performed on an ABI Fast 7500 system (Applied Biosystems) using a standard cycling protocol. Primers for Klotho, catalase, and glyceraldehyde-3-phosphate-dehydrogenase (GAPDH), as an internal control, were pre-developed by Applied Biosystems. The relative mRNA expression of Klotho was normalized to GAPDH expression.
Western blot analysis
The protein expression of Klotho and manganese superoxide dismutase (MnSOD) in kidney homogenates was determined by western blot analysis. The polyclonal antibodies for Klotho (1:1000) and MnSOD (1:50) were obtained from Abcam (Cambridge, MA) and Cell Signaling Technology (Danvers, MA). Kidney homogenates were separated by 10% sodium dodecyl sulfate-polyacrylamide gel electrophoresis, transferred to nitrocellulose membranes, and blocked overnight at 4°C in 5% bovine serum albumin. Immunodetection was performed by incubating the membranes with the primary antibodies diluted in blocking buffer for 1 h at room temperature. After washing, a chemiluminescent horseradish peroxidase substrate was diluted in blocking buffer and applied for 60 min. Band intensity was quantified with the Quantity One software (Bio-Rad, Hercules, CA), with β-Actin acting as the normalization protein (1:10,000; Sigma-Aldrich, St. Louis, MO).
Statistical analysis
Data are presented as mean ± SD. Unpaired t test and two-way analysis of variance were used to analyze the data. All data were analyzed using Graph Pad Prism v6.0 for Windows (GraphPad Software, San Diego, CA). Two-tailed P values <0.05 were considered statistically significant.
RESULTS
HO affects the renal expression of Klotho
We first sought to determine whether neonatal HO exposure altered kidney Klotho expression. The mRNA and protein expression of Klotho in kidney homogenates of neonatal rats exposed to 21 days of HO or normoxia are depicted in Fig. 1. Exposure to neonatal HO for 21 days resulted in significantly decreased kidney Klotho gene and protein expression (Fig. 1a, b).
Fig. 1. Kidney Klotho expression decreases with hyperoxia (HO) exposure.
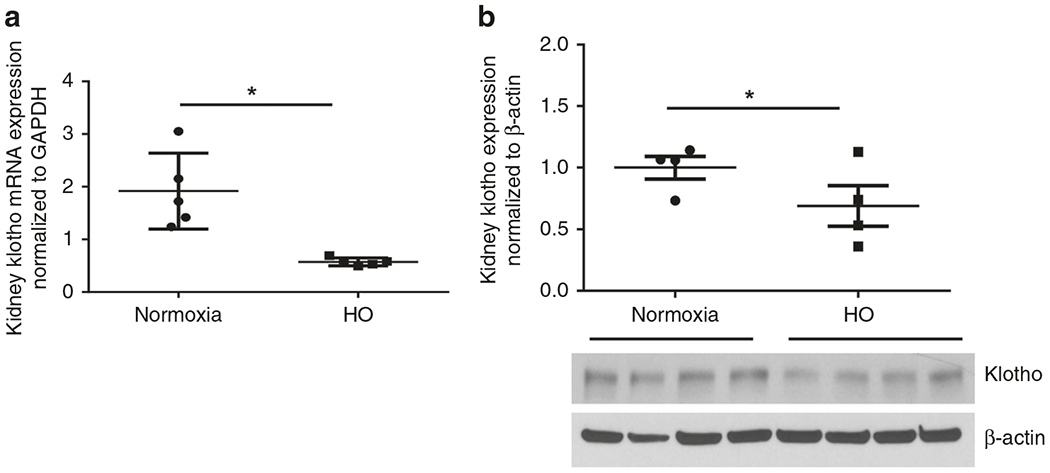
Significantly, decreased Klotho mRNA (a) and protein (b) expression in the kidneys of rats exposed to HO for 21 days. (P <0.05; *Normoxia vs HO, n = 4–5/group).
Klotho administration increases kidney antioxidant capacity
HO exposure increases oxidative stress, and both MnSOD and catalase are key regulators of oxidative injury.26,27 Given that Klotho has antioxidant effects,24 we next questioned whether early Klotho administration would preserve kidney MnSOD and catalase levels in rats exposed to neonatal HO. Western blot analysis demonstrated reduced MnSOD protein expression in the kidneys of 6-week-old rats raised in either normoxia or HO (Fig. 2a, b). Administration of exogenous Klotho for 21 days resulted in a twofold increase in kidney MnSOD expression in both normoxia and HO conditions (Fig. 2a, b). The increase in MnSOD was similarly augmented in both animal groups following Klotho administration, suggesting that Klotho effectively normalized kidney MnSOD expression despite HO exposure (Fig. 2a, b). Moreover, in HO-exposed animals, Klotho supplementation also significantly increased kidney catalase mRNA expression (Fig. 2c).
Fig. 2. Klotho increases renal antioxidant capacity in neonatal HO-exposed rats.

a Increased renal manganese superoxide dismutase (MnSOD) protein expression in 6-week-old rats treated with recombinant Klotho. b A representative western blot is shown in the lower panel with MnSOD expression normalized to β-Actin. c Increased catalase mRNA expression in 6-week-old rats treated with recombinant Klotho. PL is placebo. (P < 0.05; *Normoxia-PL vs normoxia-Klotho or HO-PL vs HO-Klotho; n = 3–5/group).
Klotho administration improves HO-induced renal vascular changes
RRA Doppler flow measurements done at 6 weeks of life prior to sacrifice are depicted in Fig. 3. HO significantly increased both the RRA RI and RRA PI, suggesting restricted renal perfusion and increased vascular stiffness. The administration of Klotho improved the restricted renal perfusion profile in the animals exposed to HO as evidenced by a significant decrease in their RRA PI and RRA RI reflecting attenuation of the renal vascular stiffness (Fig. 3).
Fig. 3. Klotho attenuates HO-induced elevated renal vascular changes.
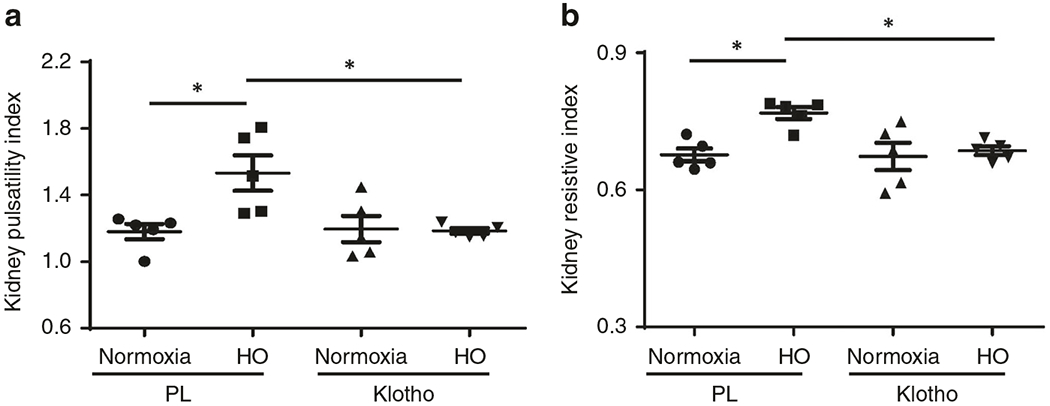
Significantly improved right renal artery (RRA) a pulsatility index (PI) and b resistive index (RI) in Klotho-treated HO-exposed 6-week-old rats. (P <0.05; *Normoxia-PL vs HO-PL; n = 4–5/group).
Effect of Klotho on creatinine levels
Final serum creatinine concentrations were virtually similar in the untreated animals after normoxia or HO (0.20 ± 0.00 vs 0.20 ± 0.00 mg/dl; normoxia-PL vs HO-PL, n = 8/group) and the corresponding Klotho-treated (0.20 ±0.00 vs 0.18 ± 0.04 mg/dl; normoxia-Klotho vs HO Klotho, n = 5–6/group) experimental groups after 6 weeks.
Klotho prevents HO-induced glomerulomegaly
Compared to the animals raised in normoxia, those exposed to HO developed glomerulomegaly as indicated by a significantly increased glomerular area (8454 ±594 vs 6410 ±302 μm2; normoxia-PL vs HO-PL, P < 0.05; n = 5–6/group; Fig. 4). Administration of Klotho demonstrated effective protection from the development of glomerulomegaly, as indicated by the lack of significant differences between the Klotho-treated groups in their glomerular area measurements (7027 ±318 vs 7520 ± 182.2 μm2; normoxia-Klotho vs HO-Klotho).
Fig. 4. Klotho and HO-induced glomerular changes.
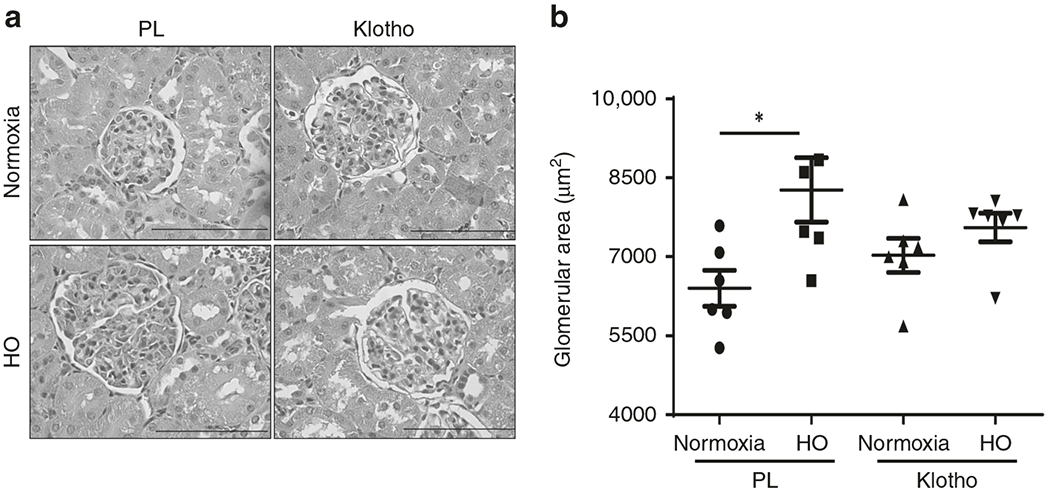
a Hematoxylin and eosin-stained kidney sections demonstrating decreased glomerulomegaly in Klotho-treated HO-exposed 6-week-old rats. Magnification is ×40. Scale bar is 100 μm. b Neonatal HO increased glomerular area, but there was no difference in glomerular area between the normoxic and HO-treated Klotho groups. (P < 0.05; *Normoxia-PL vs HO-PL, n = 5–6/group).
Klotho attenuates HO-induced tubular injury
HO-exposed rats displayed higher tubular injury scores compared to normoxia-exposed rats (2.9 ± 0.34 vs 4.2 ± 0.36; normoxia-PL vs HO-PL, P = 0.014; n = 6/group; Fig. 5). The most common abnormality noted was tubular cell vacuolization. Klotho administration decreased the tubular injury score (4.20 ±0.35 vs. 2.90 ± 0.31; HO-PL vs HO-Klotho, P = 0.015; n = 6/group; Fig. 5).
Fig. 5. Klotho prevents HO-induced tubular injury.
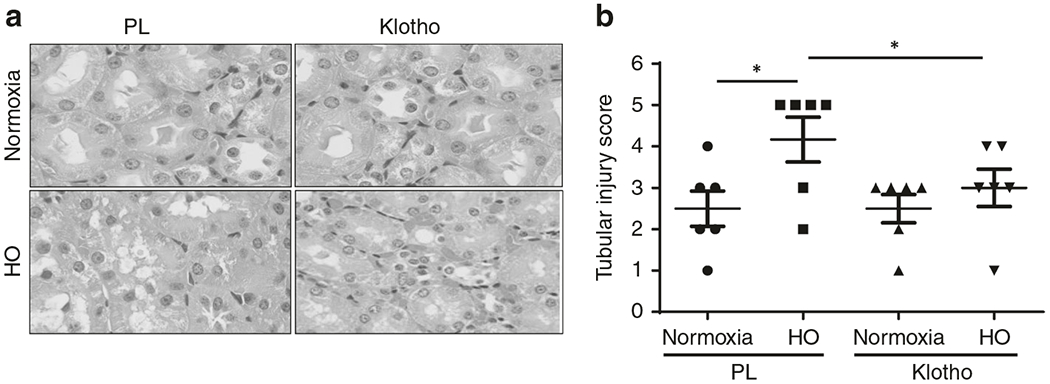
a Hematoxylin and eosin-stained kidney sections demonstrating decreased tubular injury in Klotho-treated HO-exposed 6-week-old rats. Magnification is ×100. Scale bar is 100 μm. b Neonatal HO increased tubular injury score in 6-week-old rats, but this was markedly decreased in the HO-treated Klotho groups. (P < 0.05; *Normoxia-PL vs HO-PL; n = 5–6/group).
Effect of Klotho on body weight
Body weights at the time of sacrifice were similar in the untreated animals after normoxia or HO: (normoxia-PL = 171.1 ±25.4 g, HO-PL = 179.5 ± 26.6 g, n = 10/group) as well as in the corresponding Klotho-treated groups (normoxia-Klotho = 191.1 ± 15.1 g, HO-Klotho = 172.6 ± 25.7 g, n = 6–9/group). There was also no difference with HO or Klotho exposure in the kidney weight or the kidney-to-body weight ratio.
DISCUSSION
Klotho is highly expressed in the kidney, and CKD is a state of Klotho deficiency that exerts multiple systemic adverse effects on numerous organs, including the kidneys and the vascular system.19–22 In the present study, we demonstrate in a rodent model of HO-induced kidney injury that HO exposure during early postnatal nephrogenesis was accompanied by a marked reduction of renal Klotho expression, in addition to restricted renal perfusion, glomerulomegaly, and higher tubular injury scores. Administration of exogenous Klotho improved renal vascular perfusion, abrogated both glomerulomegaly and tubular injury, and restored kidney antioxidant capacity.
Previous studies in rat metanephric organ culture studies have demonstrated that both vasculogenesis and tubulogenesis are enhanced when kept in low rather than 21% oxygen concentrations.28 Nephrogenesis in utero occurs at very low oxygen tension; after birth, blood oxygen levels quickly rise,29,30 which can result in oxidative stress even in conditions of “normoxia” and particularly with the use of supplemental oxygen therapy or HO.31–33
Nephrogenesis is complete by the 36th week of gestation in humans, but it continues until approximately P10 in rats.34 Hence, the exposure to HO in rats shortly after birth could have comparable consequences to those caused by O2 exposure in extremely premature infants born at ~24–25 weeks of gestation, during the critical period of postnatal nephrogenesis.1,2 In this regard, a few studies have investigated the short- and long-term impacts of HO on the developing kidneys in rodent models.14,18,26,33,34
Glomerulomegaly is a surrogate marker of kidney injury in preterm infants since it precedes reduced nephron number that leads to secondary glomerular hyperfiltration, a pathophysiological hallmark of CKD.2,4,35 Glomerular injury has been demonstrated in rodent studies wherein HO during the postnatal period led to an increase in the renal corpuscle size.14,18 Our study not only differs from the prior studies by the relatively longer duration of HO (3 weeks) and the higher oxygen concentration (85%) but also demonstrates the association between oxidative injury and glomerulomegaly. These results suggest that exposure to HO during the period of active nephrogenesis may contribute to hyperfiltration and compensatory hypertrophy as an adaptation to injury. This has been shown to parallel hyperfiltration related to low nephron number as seen in preterm born infants.35
The present study confirms the deleterious effects of HO on renal tubular integrity,18 as evidenced by the higher renal tubular injury scores in the neonatal rats reared in oxygen-enriched environments. Several mechanisms may contribute to these tubular changes, including vascular derangements and oxidative stress.18
While antioxidant agents have successfully prevented oxidative stress-induced lung injury in rats,15–17 the effects of an antioxidant agent on kidney histomorphometry in a rodent model of postnatal nephrogenesis have not been evaluated. α-Klotho is a transmembrane protein highly expressed in the kidney and its cleaved product in the circulation (soluble Klotho) functions as an endocrine substance with far-reaching effects including potent antioxidation properties.20 We found that the exogenous administration of Klotho prevented the glomerulomegaly and attenuated tubular injury to levels similar to those seen in the placebo animals kept under normoxia conditions. Furthermore, HO resulted in a marked reduction of kidney Klotho mRNA expression levels coinciding with the increased renal oxidative stress, and notably antioxidant capacity was restored by exogenous Klotho administration. These findings in the kidney are similar to previous studies showing resistance to oxidative stress16 and protection against oxidative damage in pulmonary epithelia.17 Following Klotho administration, a recent study in adult rats with experimental renal insufficiency showed that early administration of α-Klotho prevented the progression of AKI to CKD and also protected the heart from cardiac remodeling.36 The supplementation of exogenous Klotho and/or upregulation of endogenous renal Klotho production may confer both renal and lung protection, which is proposed to be associated with, but not restricted to, its antioxidative properties.37,38 Our group has preliminary and unpublished data corroborating the findings that Klotho administration has a systemic and not only kidney-specific effects given that we have found improvement in pulmonary hypertension, left ventricular hypertrophy, and cardiac dysfunction in the same rat model. In addition, improved renal perfusion after Klotho administration could be part of the mechanism by which oxidative injury was diminished in the treated group.
Our experimental studies have potential clinical implications. Given that glomerular hypertrophy and tubular injury are known antecedents to progressive CKD, the present results suggest that exposure to HO during active nephrogenesis may have an additive negative impact on the inherent glomerular and tubular alterations in preterm born individuals.2 While the mRNA expression of Klotho was clearly identified in the kidney tissue of the animals kept in normoxia with normal renal histopathology, Klotho expression fell significantly in those kept in HO and those that displayed glomerular and tubular abnormalities. Moreover, this occurred without an overt reduction in kidney function as evidenced by the similar serum creatinine measurements in all the groups at the time of sacrifice. Similar declines in Klotho expression have been observed in the kidney biopsy samples of patients with advancing CKD and reduced glomerular filtration rate (GFR) when compared to patients with preserved GFR.38 Notably, administration of Klotho to the hyperoxic animals attenuated significantly the structural abnormalities reflecting renal injury via restoring the kidney’s antioxidant capacity and could in turn decrease the risk of progression toward CKD, as demonstrated in animals with experimentally induced AKI.34 This further supports the notion that exogenous Klotho administration can provide effective renoprotection during exposure to an injurious environment such as hyperoxemia in the neonatal period.
The potential downstream pathways of Klotho were also explored in this model, specifically the impact on renal cell apoptosis. Whereas HO-PL animals had an increase in cleaved caspase 3 expression, Klotho treatment dampened this expression, although it did not reach statistical significance, hence data are not shown. In addition, NRF2, nuclear factor erythroid 2-related factor 2, which is a transcription factor that regulates the expression of antioxidant proteins,39 was tested in our model (data not shown), and we found no significant difference between Klotho-treated and PL groups, which may be related to the relatively short exposure period to Klotho.
Some of the limitations of our study include the lack of renal functional biomarkers and that no rodents were sacrificed during the period of nephrogenesis (i.e., within the first 10 postnatal days) and hence limited our ability to compare the early from the later effects of HO and Klotho supplementation during this critical period of nephrogenesis. In addition, we did not assess for systemic hypertension or the role of the renin-angiotensin system (RAS) or nitrous oxide in altering the rats’ renal perfusion profiles during oxidative stress, although other studies have reported RAS dysregulation in oxidative stress animal models.40 Future studies should assess for the impact of Klotho on the RAS and early markers of injury such as proteinuria or urinary biomarkers.
In conclusion, the findings of this study demonstrate that HO exposure in a model of postnatal nephrogenesis results in reduced kidney Klotho expression and restricted renal perfusion associated with glomerular and tubular injury and that the exogenous administration of Klotho attenuates HO-induced tubular injury and prevents glomerulomegaly at 6 weeks as well as improvement in kidney antioxidant capacity and restoration of renal perfusion. Future studies should be directed toward understanding the molecular pathways driving oxidative stress and injury as well as looking at the comparison between early and late outcomes of HO on the developing kidney. Therapeutic strategies to prevent neonatal AKI and progression to CKD are lacking. Our findings call for future translational studies to explore the clinical applications of exogenous Klotho administration in premature infants with oxidative stress-related renal insufficiency.
ACKNOWLEDGEMENTS
This work was supported by grant funding from the Batchelor Children’s Research Awards to C.L.A. and K.C.Y. L.A.S. is funded by grants from the NIH (1R01HL140468) and the Miami Heart Research Institute. K.Y. is a recipient of AHA predoctoral fellowship (18PRE33960070).
Footnotes
Competing interests: The authors declare no competing interests.
REFERENCES
- 1.Rodriguez MM et al. Histomorphometric analysis of postnatal glomerulogenesis in extremely preterm infants. Pediatr. Dev. Pathol 7, 17–25 (2004). [DOI] [PubMed] [Google Scholar]
- 2.Abitbol CL & Rodriguez MM The long-term renal and cardiovascular consequences of prematurity. Nat. Rev. Nephrol 8, 265–274 (2012). [DOI] [PubMed] [Google Scholar]
- 3.Crump C et al. Gestational age at birth and mortality in young adulthood. JAMA 306, 1233–1240 (2011). [DOI] [PubMed] [Google Scholar]
- 4.Luyckx VA et al. A developmental approach to the prevention of hypertension and kidney disease: a report from the Low Birth Weight and Nephron Number Working Group. Lancet 390, 424–428 (2017). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Abitbol CL, DeFreitas MJ & Strauss J Assessment of kidney function in preterm infants: lifelong implications. Pediatr. Nephrol 31, 2213–2222 (2016). [DOI] [PubMed] [Google Scholar]
- 6.Abitbol CL & Moxey-Mims M Chronic kidney disease: low birth weight and the global burden of kidney disease. Nat. Rev. Nephrol 12, 199–200 (2016). [DOI] [PubMed] [Google Scholar]
- 7.Davis JM & Auten RL Maturation of the antioxidant system and the effects on preterm birth. Semin. Fetal Neonatal Med 15, 191–195 (2010). [DOI] [PubMed] [Google Scholar]
- 8.Vento M et al. Oxidative stress in asphyxiated term infants resuscitated with 100% oxygen. J. Pediatr 142, 240–246 (2003). [DOI] [PubMed] [Google Scholar]
- 9.Vento M et al. Resuscitation with room air instead of 100% oxygen prevents oxidative stress in moderately asphyxiated term neonates. Pediatrics 107, 642–647 (2001). [DOI] [PubMed] [Google Scholar]
- 10.Georgeson GD et al. Antioxidant enzyme activities are decreased in preterm infants and in neonates born via caesarean section. Eur. J. Obstet. Gynecol. Reprod. Biol 103, 136–139 (2002). [DOI] [PubMed] [Google Scholar]
- 11.Lee YS & Chou YH Antioxidant profiles in full term and preterm neonates. Chang Gung Med. J 28, 846–851 (2005). [PubMed] [Google Scholar]
- 12.Hinchliffe SA, Sargent PH, Howard CV, Chan YF & van Velzen D Human intrauterine renal growth expressed in absolute number of glomeruli assessed by the disector method and Cavalieri principle. Lab. Invest 64, 777–784 (1991). [PubMed] [Google Scholar]
- 13.Sutherland MR et al. Accelerated maturation and abnormal morphology in the preterm neonatal kidney. J. Am. Soc. Nephrol 22, 1365–1374 (2011). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sutherland MR et al. Neonatal hyperoxia: effects on nephrogenesis and long-term glomerular structure. Am. J. Physiol. Ren. Physiol 304, F1308–F1316 (2013). [DOI] [PubMed] [Google Scholar]
- 15.Bryan C et al. TNFalpha-stimulated protein 6 (TSG-6) reduces lung inflammation in an experimental model of bronchopulmonary dysplasia. Pediatr. Res 85, 390–397 (2019). [DOI] [PubMed] [Google Scholar]
- 16.Vaidya R et al. Recombinant CCN1 prevents hyperoxia induced lung injury in neonatal rats. Pediatr. Res 82, 863–871 (2017). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Reiter J et al. Stromal derived factor-1 mediates the lung regenerative effects of mesenchymal stem cells in a rodent model of bronchopulmonary dysplasia. Respir. Res 18,137 (2017). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Jiang JS, Chou HC, Yeh TF & Chen CM Neonatal hyperoxia exposure induces kidney fibrosis in rats. Pediatr. Neonatol 56, 235–241 (2015). [DOI] [PubMed] [Google Scholar]
- 19.Kuro-o M et al. Mutation of the mouse klotho gene leads to a syndrome resembling ageing. Nature 390, 45–51 (1997). [DOI] [PubMed] [Google Scholar]
- 20.Hu MC, Matsumura Y, Aizawa H & Moe OW Fibroblast growth factor 23 and Klotho: physiology and pathophysiology of an endocrine network of mineral metabolism. Annu. Rev. Physiol 75, 503–533 (2013). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kuro-o M A potential link between phosphate and aging-lessons from Klotho-deficient mice. Mech. Ageing Dev 131, 270–275 (2010). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Barker SL et al. The demonstration of alphaKlotho deficiency in human chronic kidney disease with a novel synthetic antibody. Nephrol. Dial. Transpl 30, 223–233 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Christov M, Neyra JA, Gupta S & Leaf DE Fibroblast growth factor 23 and Klotho in AKI. Semin. Nephrol 39, 57–75 (2019). [DOI] [PubMed] [Google Scholar]
- 24.Yamamoto M et al. Regulation of oxidative stress by the anti-aging hormone klotho. J. Biol. Chem 280, 38029–38034 (2005). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Schneider CA, Rasband WS & Eliceiri KW NIH Image to ImageJ: 25 years of image analysis. Nat. Methods 9, 671–675 (2012). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bresciani G, da Cruz IB & Gonzalez-Gallego J Manganese superoxide dismutase and oxidative stress modulation. Adv. Clin. Chem 68, 87–130 (2015). [DOI] [PubMed] [Google Scholar]
- 27.Ahn J et al. Associations between catalase phenotype and genotype: modification by epidemiologic factors. Cancer Epidemiol. Biomark. Prev 15, 1217–1222 (2006). [DOI] [PubMed] [Google Scholar]
- 28.Popescu CR et al. Hyperoxia exposure impairs nephrogenesis in the neonatal rat: role of HIF-1alpha. PLoS ONE 8, e82421 (2013). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kamlin CO, O’Donnell CP, Davis PG & Morley CJ Oxygen saturation in healthy infants immediately after birth. J. Pediatr 148, 585–589 (2006). [DOI] [PubMed] [Google Scholar]
- 30.Rabi Y, Yee W, Chen SY & Singhal N Oxygen saturation trends immediately after birth. J. Pediatr 148, 590–594 (2006). [DOI] [PubMed] [Google Scholar]
- 31.Saugstad OD Update on oxygen radical disease in neonatology. Curr. Opin. Obstet. Gynecol 13, 147–153 (2001). [DOI] [PubMed] [Google Scholar]
- 32.Marquez MG, Cabrera I, Serrano DJ & Sterin-Speziale N Cell proliferation and morphometric changes in the rat kidney during postnatal development. Anat. Embryol. (Berl.) 205, 431–440 (2002). [DOI] [PubMed] [Google Scholar]
- 33.Yzydorczyk C et al. Neonatal oxygen exposure in rats leads to cardiovascular and renal alterations in adulthood. Hypertension 52, 889–895 (2008). [DOI] [PubMed] [Google Scholar]
- 34.Sutherland MR et al. Age- and sex-related changes in rat renal function and pathology following neonatal hyperoxia exposure. Physiol. Rep 4, e12887 (2016). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Puelles VG et al. Estimating individual glomerular volume in the human kidney: clinical perspectives. Nephrol. Dial. Transpl 27, 1880–1888 (2012). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Hu MC et al. Recombinant alpha-Klotho may be prophylactic and therapeutic for acute to chronic kidney disease progression and uremic cardiomyopathy. Kidney Int. 91, 1104–1114 (2017). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ravikumar P et al. alpha-Klotho protects against oxidative damage in pulmonary epithelia. Am. J. Physiol. Lung Cell. Mol. Physiol 307, L566–L575 (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Sakan H et al. Reduced renal α-Klotho expression in CKD patients and its effect on renal phosphate handline and vitamin D metabolism. PLoS ONE 23, e86301 (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Wang R et al. Reduced NRF2 expression suppresses endothelial progenitor cell function and induces senescence during aging. Aging 11, 7021–7035 (2019). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Saleem M, Wang X, Pokkunuri I & Asghar M Superoxide via Sp3 mechanism increases renal renin activity, renal AT1 receptor function, and blood pressure in rats. Am. J. Physiol. Ren. Physiol 315, F1478–F1483 (2018). [DOI] [PMC free article] [PubMed] [Google Scholar]