

Abstract
Background
During the height of the coronavirus disease 2019 (COVID-19) pandemic, elective surgeries, including oncologic surgeries, were delayed. Little prospective data existed to guide practice, and professional surgical societies issued recommendations grounded mainly in common sense and expert consensus, such as medical therapy for early-stage breast and prostate cancer patients. To understand the patient experience of delay in cancer surgery during the pandemic, we interviewed breast and prostate cancer patients whose surgeries were delayed due to the pandemic.
Patients and Methods
Patients with early-stage breast or prostate cancer who suffered surgical postponement at Brigham and Women’s Hospital (BWH) were invited to participate. Semi-structured telephone interviews were conducted with 21 breast and prostate cancer patients. Interviews were transcribed, and qualitative analysis using ground-theory approach was performed.
Results
Most patients reported significant distress due to cancer and COVID. Key themes that emerged included the lack of surprise and acceptance of the surgical delays but endorsed persistent cancer- and delay-related worries. Satisfaction with patient–physician communication and the availability of a delay strategy were key factors in patients’ acceptance of the situation; perceived lack of communication prompted a few patients to seek care elsewhere.
Discussion
The clinical effect of delay in cancer surgery will take years to fully understand, but there are immediate steps that can be taken to improve the patient experience of delays in care, including elicitation of individual patient perspectives and ongoing communication. More work is needed to understand the wider experiences of patients, especially minority, socioeconomically disadvantaged, and uninsured patients, who encounter delays in oncologic care.
Graphical Abstract

Supplementary Information
The online version contains supplementary material available at 10.1245/s10434-021-10319-0.
In March 2020, the American College of Surgeons recommended that any nonessential surgeries be postponed to preserve personal protective equipment (PPE) and personnel as the US healthcare system grappled to accommodate increased needs within the healthcare system due to the COVID-19 pandemic.1 Triaging cancer surgeries presented a unique challenge to healthcare systems as oncologic surgery, while not truly “elective,” also rarely qualified as urgent or emergent. In addition, oncologic treatment is multidisciplinary, meaning that surgical delays not only have ramifications for locoregional control, but also for systemic treatment planning.2 Little, if any, prospective data existed to guide cancer care in such a situation, and professional societies were tasked with developing alternative treatment plans grounded in common sense and expert consensus. Among those cancers for which surgical delay was considered to be reasonable included ductal carcinoma in situ (DCIS), early-stage, hormone-receptor-positive (HR+) breast cancer and early-stage prostate cancer.3–5
The first surge of COVID-19 presented unprecedented barriers to oncologic care, but it also represented an extreme example of a competing health-related stressor that our patients must contend with on a regular basis. Although society recommendations advocated that clear, consistent messaging and reassurance be provided when discussing treatment delays or alternative treatment strategies with patients, there was limited practical guidance available regarding alleviating patient anxieties2 Our objective was to explore the lived experience of cancer patients who experienced surgical delays during the first wave of the pandemic, to understand how a significant competing health-related stressor changed their relationship to their cancer-related worry, and to identify opportunities to improve care.
Patients and Methods
Overview
This study was approved by the Mass General Brigham Institutional Review Board.
Participants/Recruitment
We recruited adults ≥ 18 years who were scheduled to undergo breast or prostate surgery for malignant cancer conditions at Brigham and Women’s Hospital whose surgery was delayed owing to COVID-19 at the onset of the pandemic. Eligible patients were identified by clinicians’ referrals using the following criteria: having DCIS, early-stage HR+ breast cancer, or low-, intermediate-, or high-risk prostate cancer, for whom surgery had been previously scheduled but was postponed owing to change in hospital policy; date range for previously scheduled surgeries was 18 March 2020 to 1 June 2020. Study authors (C.M., Q.C.) identified patients within their respective departments (breast, urology) who met inclusion criteria via chart review; following identification, patients were contacted by phone by study staff (M.K., J.S., C.Sh.) and provided information about the study. The discussion was supplemented by an information sheet and letter from the investigator by either mail or email (patient preference). After the study was explained, patients were asked if they would like to enroll and choose a time to complete the phone interview. No incentives were offered for participation; at the beginning of the phone call, patients were informed that their participation was completely voluntary and that, while no direct benefit could be expected from their participation, their perspective would inform improvements in the delivery of surgical care.
Chart review was subsequently performed to collect demographic information including age, race, gender, marital status, primary insurer, grade/stage of cancer, and planned surgery.
Interview Guide and Data Collection
A semi-structured interview guide was developed, based on literature review and clinical experience, by a surgical oncologist (C.M.) with input from an interdisciplinary team of those experienced with cancer care, including subspecialists in breast, urology, otolaryngology, and internal medicine (Supplementary). The goal of the guide was to understand the experience of cancer patients whose surgeries were delayed due to the pandemic. Using the National Comprehensive Cancer Network’s Distress Thermometer as a guide, we also asked patients to rate their cancer- and COVID-related worries on a scale of 0–10, with 0 being no worry and 10 being extreme worry. Experts suggest a cutoff score of 3 to identify distress.6 Semi-structured interviews were conducted between 1 and 7 May 2020 by phone by three trained research assistants (M.K., J.S., C.Sh.) who have prior experience in conducting patient interviews. Interviews were approximately 20 min long. Verbal informed consent was obtained at the beginning of each interview. Interviews were audio-recorded and transcribed verbatim.
Analysis
Content analysis guided by grounded theory was performed using NVIVO qualitative software (Version 12). Open-line coding by two coders was performed for five randomly selected transcripts, and a preliminary codebook was developed by a team trained in qualitative methods (C.M., C.S., M.K., J.S.). The constant comparative method of grounded theory guided coding.7,8 Following development of the codebook, the multidisciplinary team met to assess its credibility.9 All other transcripts were double-coded, with frequent meetings to review coding discrepancies and refine the codebook. Using an inductive and iterative approach, final themes were determined by the study team, taking into account alternative interpretations, researcher biases, latent themes, and clinical implications of the findings. Sampling continued alongside refining of the codebook until consensus was achieved and thematic saturation was reached, and at this time all interview activities were halted.10,11
Results
Participant demographics are presented in Table 1. Of 43 patients identified to meet inclusion criteria, 21 patients were interviewed: 8 female patients with breast cancer and 13 male patients with prostate cancer; 3 declined, 2 did not speak English, and the remaining 17 were not contacted as thematic saturation had been achieved. The median age was 63 years (IQR 47–79 years), and 18 patients identified as non-Hispanic White, 2 as Hispanic White, and 1 as Asian American. The most common insurance was employer-sponsored/private plan (47.6%), followed by Medicare (38.1%). All but one breast cancer patient had stage I ER+ cancer (the eighth had DCIS), and the majority of prostate cancer patients had intermediate-grade cancer (G3+4). Delayed surgeries included double mastectomy (2 patients), lumpectomy (6 patients), and prostatectomy (13 patients). Nineteen of 21 patients were married.
Table 1.
Cohort demographics (N = 21)
| Breast cancer (N = 8) | Prostate cancer (N = 13) | |
|---|---|---|
| Age, median (IQR) | 66 years (58–68.5 years) | 61 years (58–65 years) |
| Gender | ||
| Male | 8 (100%) | 13 (100%) |
| Female | ||
| Race/ethnicity | ||
| White, non-Hispanic | 8 (100%) | 10 (76.9%) |
| White, Hispanic | 2 (15.4%) | |
| Asian American | 1 (7.7%) | |
| Married | 6 (75%) | 13 (100%) |
| Primary insurance provider | ||
| Employer-sponsored Insurance | 4 (50%) | 6 (30.8%) |
| Medicare | 4 (50%) | 4 (46.2%) |
| Tricare | 1 (7.7%) | |
| Medicaid | 2 (15.4%) | |
| Breast cancer stage | ||
| Ductal carcinoma in situ (DCIS) | 1 (12.5%) | |
| Stage I, estrogen-receptor+ (ER+) | 7 (87.5%) | |
| Prostate cancer grade | ||
| High grade | 1 (7.7%) | |
| Intermediate grade | 10 (76.9%) | |
| Low grade | 2 (15.4%) | |
| Surgery | ||
| Lumpectomy | 6 (75%) | |
| Double mastectomy | 2 (25%) | |
| Prostatectomy | 13 (100%) |
When asked to rate their worry about cancer and COVID on a scale of 0–10, patients reported a median score of 4/10 for cancer-related worries (IQR 2.5–7) and 5/10 for COVID-related worries (IQR 2–7). Seven patients rated their worries about cancer to be more significant that COVID, and eight patients rated their worries about COVID to be more significant than cancer (Fig. 1).
Fig. 1.
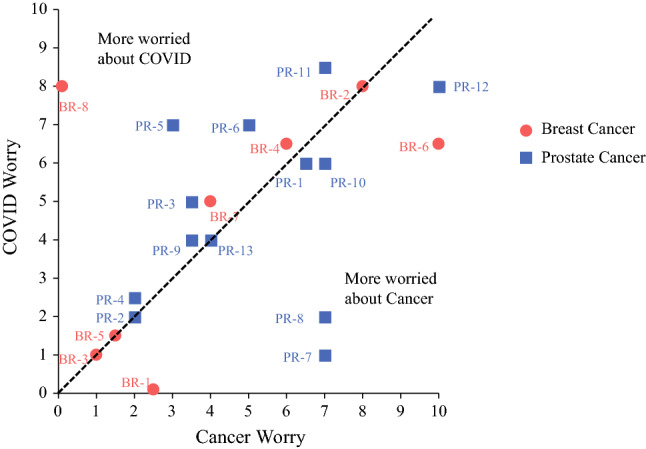
Comparison of Cancer and COVID-related worries among patients with surgical delays
At time of interviews, first-wave pandemic hospital policy remained in effect, and surgeries had been delayed but not rescheduled. Four major themes were identified in the interview:
Distress associated with diagnosis and pandemic: (Table 2, Fig. 2): participants reported coping with a diagnosis of cancer during a pandemic came with complex, competing emotions and concerns. Patients reflected on the experience of dealing with two life-changing events, cancer and COVID, simultaneously. They worried about their personal health and that of their family. They described finding control through new routines to maintain personal safety and social distancing.
Table 2.
Themes and quotes from interviews of breast and prostate cancer patients undergoing surgical delays at Brigham and Women’s Hospital
| Distress associated with diagnosis and pandemic | |
| Cancer-related worry | “I mean, the disease ‘cancer’ is something that immediately triggers fear in you…you know what I mean?” (PR) |
| Change in cancer narrative |
“Usually, you get cancer and that’s the biggest story in lives of everyone you know…now it’s not.” (BR) “It’s really strange, because you have this script in your mind…if I get cancer, this is what it will look like…I did a GoFundMe to try to raise money for this surgery, and I feel ridiculous asking people for money at this time, but we could use help. So it’s just this surrealness of this whole experience happening in the shadow of this other really huge thing in the world.” (BR) |
| Worry for self |
“I’m acutely aware how susceptible I am because of the lung situation [previous lung cancer].” (BR) “I’m 65, I’m in the category of people that should worry…” (PR) |
| Worry for others |
“…my parents are older and have underlying conditions…and they’re basically living with children not old enough to pick their noses.” (BR) “My mother is 98, she moved into our house because her assisted living facility was going in to lockdown and I thought she would be safer and happier with us.” (BR) |
| COVID compounds cancer worry | “I mean, we went on shelter, and I got my cancer diagnosed at exactly the same time. And my anxiety was really, really high. I was in the house and I had absolutely nothing to distract me.” (BR) |
| Reassurance in new routines | “Indeed this is dangerous, highly contagious, all that. And if I avoid contact with people, stay home – [if] I take walks outside, with full gear, full protection equipment, I feel comfortable.” (PR) |
| Initial reaction | |
| No surprise | “My son’s family lives in Italy, so I was well aware of what was taking place, [the delay] didn’t surprise me.” (BR) |
| Frustration |
“My concern is that if this gets delayed further, it’s not acceptable to me.” (BR) “I, just like everyone else in the world, would like to have a little control over my life.” (PR) |
| Lack of control | “I, like everybody else in the world, would like to have a little bit of control in my life, right?” (PR-) |
| Relief | “Actually, relief, because I was starting to worry about going to any hospital given what was happening with COVID…pleased to hear the hospital’s thinking is in line with mine.” (PR) |
| Avoidance | “I’ve been in denial…this may not happen for a month, month-and-a-half. I’ve blocked it out pretty well.” (PR) |
| Anxiety | “It’s just a lot of anxiety because its like, “Okay. This thing is growing inside of me. How long is it going to take?” … your mind keeps reeling. I think if the COVID wasn’t here I’d already be in recovery, you know?” (PR) |
| Acceptance of surgical delay | |
| Trust in physician |
“I feel really good about my doctor. He’s looking out for me, trying to make the best plan for me he can.” (PR) “…I didn’t really panic about it, because I figured I was in good hands – you guys are the experts, not me.” (PR) |
| Unchanged outcomes | “…the surgeon telling me, listen, this isn’t a clinical setback, you’re going to be fine. Your outcomes are going to be the same.” (BR) |
| Education on condition | “[my doctors] were like teachers…they were reassuring. She drew pictures. She’s great and reassuring.” (BR) |
| Hearing of delay directly from surgeon | “[the surgeon] called me herself and explained that they were going to schedule me for [this date]. She explained why, and I just accepted it…” (BR) |
| Comforted by alternative strategy | “It was easier to take the news knowing that the option to take the estrogen therapy as a preventative prior to surgery actually made me feel better.” (BR) |
| Asymptomatic | “I feel really healthy. Perhaps if I did have symptoms, that worry would escalate.” (PR) |
| Community need over individual | “…people are dying and sick, so I just have to accept the fact that I have to wait because there are people who need hospitalization more than I do at this time.” (BR) |
| Anxiety alongside acceptance | “I’d like to have a plan, a date, to know it was going to happen…they say they haven’t forgotten about me…it’s just the uncertainty of not knowing when.” (BR) |
| Lack of acceptance of surgical delay | |
| Delay not communicated by surgeon | “I got no support. I would think in the future, people wouldn’t want to leave a message like that about my cancer surgery being cancelled on someone’s message machine.” (BR) |
| Unclear next steps |
“I would have liked to have heard maybe sometime, “Hey, we haven’t forgotten you. It’s still pretty bad. We are looking at such-and-such date.” (PR) “Now we’ve had the biopsy, and I go home and sit until the end of June. And what happens at the end of June? Is my surgery going to happen on that day, or is the date going to change? I don’t know.” (BR) |
| Sought care elsewhere | “I got a referral to [alternate hospital] and they were very responsive…they called me and said ‘would you like to come in next week?’ And I had my surgery on Wednesday.” (BR) |
BR breast cancer patient, PR prostate cancer patient
Fig. 2.

Diagram of the patient experience of surgical delay
Initial reactions to surgical delay: with respect to receiving news about their surgical delay, the majority of patients were not surprised but reported various emotional reactions to the news—frustrations, worries, and feelings of relief. Many felt frustrated, and that the surgical delay was a tangible example of individual loss of control due to the pandemic. Some worried that the delay in surgery would result in worse outcomes. Some patients felt relief at being able to avoid the hospital during the pandemic, and others reported the delay allowed them to avoid thinking about their diagnosis. After their initial emotional reaction, patients described their coping mechanisms as well as facilitators and barriers to coping with the surgical delay. The majority of patients expressed acceptance and understanding of the delay, but a few were unable to reach such a point.
Acceptance of surgical delay: patients reported a number of factors influencing their willingness to accept the surgical delay. Communication with their surgeon facilitated trust and acceptance. Patients looked to their surgeons for guidance on the implications of delaying surgery. Some trusted their surgeon implicitly. Others gained confidence from their surgeon’s ability to explain their treatment plan in patient-friendly language. News of the surgical delay directly from their surgeon was particularly important. The offer of an alternative treatment strategy, such as hormonal therapy, was also reassuring. Patients who were asymptomatic had an easier time accepting the delay, while others viewed care of COVID patients as a higher priority overall than their individual needs. However, even with open communication, the uncertainty of the timeline for next steps in cancer care left patients with persistent anxiety.
Lack of acceptance of surgical delay: patients who perceived poor communication had difficulty in accepting delays. Patients who received news of the cancellation indirectly, such as in a voicemail, reported significant distress. Some patients felt lost after receiving the news and wished their surgical teams would be more proactive in checking in with updates. A few patients, unsatisfied with their treatment plan, sought treatment elsewhere, in the form of second opinions or earlier surgery dates.
Discussion
Cancer and surgery are separately recognized to be stressful life events, and the ongoing pandemic has added a new stressor into the lives of these vulnerable patients12,13 The median scores for cancer-related and COVID-related worry were 4 and 5, respectively; if we were to use the cut-off of 3 to denote clinically significant stress, as past studies have done,6,14 the majority of our patient population may be considered to be suffering from significant health-related distress. We found that surgical delays triggered a variety of reactions within cancer patients, and that their ability to cope with this change in treatment plan was influenced by communication with their surgeon. These findings highlight the role of the surgeon in managing patient distress due to both cancer and COVID, as well as opportunities to improve communication in trying and uncertain times.
Our findings contribute to a small, but growing, body of research offering insight into the lived experience of cancer patients whose care has been affected by the pandemic. Across all oncologic subspecialties, patients who require ongoing cancer treatment have expressed concern about disease progression based on altered treatment plans due to the pandemic.15–18 Although newer studies, including those in early-stage breast and prostate cancers, provide data to suggest that treatment delays will not be associated with worse outcomes,19,20 the consequences of surgical delays will not be fully understood for years to come. However, the distress due to cancer and COVID is already present, and screening and treatment should occur in real time. There are a variety of distress screening tools that can be utilized in clinical practice, including telemedicine, such as the NCCN Distress Thermometer we utilized in this study.21 Referral pathways should be in place so that patients with distress can be immediately referred to providers such as chaplains, psychologists, and social workers. Additionally, distress screening should be an iterative process; although best practice guidelines, such as the American College of Surgeons Commission on Cancer, recommend distress screening at least one time, the impact of unforeseen circumstances, such as a global pandemic, highlights the need to repeat distress screening throughout cancer care, as both individual and global factors might contribute to changing levels of distress.22
The pandemic has presented obstacles to optimal, patient-centered communication, at a time when the uncertainty of new treatment protocols places patients at a disadvantage to accessing and interpreting available information. Surgeons are routinely tasked with the responsibility of addressing the known psychological distress of a patient facing cancer surgery while also providing reassurance regarding alternative treatment plans or delays due to the uncertainty of the pandemic. High-quality communication is that which facilitates breaking bad news and discussing prognosis and treatment plans alongside responding to emotion and showing empathy.23 We found that perceived quality of communication was associated with patient coping. In our cohort, patients found reassurance and were more accepting of their altered treatment plan when they trusted that their surgeons were making the most informed decision on their behalf and felt that conversations with their surgeons mitigated negative emotions. Trust was built through simple acts, such as the surgeon being the direct contact in the delivery of bad news (i.e., delay of surgery) and discussion of risks due to deviation from standard protocol. Conversely, patients who were dissatisfied with the quality of communication about the delay, those who did not feel they were in a partnership with their surgeon, reported impaired coping. Building trust is essential, as patient trust in their physician is associated with adherence to medical advice and participation in decision making.24,25 Previous research examining patient response to prolonged wait times for surgery has demonstrated that patients who perceive communication issues about the delay report increased anxiety, anger, and frustration.13 Cancer care delays have been widespread because of COVID: a survey by the American Cancer Society’s Cancer Action Network, conducted in April 2020 found that almost 80% of cancer patients had experienced a delay in accessing care because of COVID-19, such as follow-up appointments with their oncologists, and 17% reported delay in receipt of therapy (chemotherapy, radiation, surgery). It is not surprising that during a period of such uncertainty patients seek increased connection with their healthcare providers, and speaks to the need for uniform, consistent messaging by multidisciplinary oncology teams to support patients.
Delivering compassionate cancer care remotely using patient-centered communication should be the goal for all providers, and further research should be focused on adapting communication skills for telemedicine. Telemedicine was previously viewed as impractical for oncology, particularly due to concerns about building trust and breaking bad news via telemedicine.26 However, cancer patients who have participated in telehealth interventions respond favorably, noting that virtual technology improves efficiency while facilitating an experience of personalized care and providing reassurance.27–30 Since the beginning of the pandemic, the use of telemedicine has increased dramatically out of necessity, and components of telehealth will likely become a routine part of cancer care. In particular, oncology teams may need resources and training to break bad news and convey empathy when using a virtual platform.23 In our cohort, patients identified predominantly emotional problems, and we did not capture social issues such as financial stress or change in employment, both known obstacles for cancer patients. As the limiting factor in utilizing psychosocial services is referral, surgeons have an opportunity to help engage patients in appropriate supports early; patients who are screened for distress and provided with referrals for psychosocial services have extremely high rates of utilization.31,32
Finally, delays in cancer care are not limited to the COVID-19 pandemic. While the pandemic represents a unique situation and cause of surgical delays, it remains a difficult truth that there is a wide range in time from diagnosis to surgery for patients on a regular basis. Multiple reasons underlie these delays; they may be due to patients seeking multiple opinions, difficulties in coordinating reconstruction, necessary further workup, insurance/financial problems, lack of surgeon availability, and many others.33 While time to surgery has been suggested as a quality metric, it is a difficult one to embrace given the multitude of factors that may contribute to it. All patients deserve timely cancer care, but the underlying complexities of time to surgery require more qualitative work to fully understand the barriers and facilitators of care delays in different locales. While it will take time to develop effective interventions to curtail surgical delays in a non-pandemic-stricken world, we believe our study underscores the importance of high-quality physician–patient communication in instances in which surgical intervention may be delayed.
There are a few limitations to acknowledge. First, the sample of patients interviewed all received their care at a single tertiary care center in Boston and had one of two lower-risk cancers; they may not represent the experience of all patients undergoing active treatment. Second, the population served at our institution is predominantly White and of a higher socioeconomic status, and their experiences may not be generalizable to the cancer community at large. Given the uncertain nature of many things in the early days of the pandemic, we felt that a convenience sample of patients whose experiences occurred within the same time period was an appropriate first step to give voice to a vulnerable group that had not been interviewed during this pandemic; however, patient participation was voluntary, and we cannot comment on the experience of those who opted not to participate and may have had a different experience, particularly at a different time point. Further study of patients to examine length of delay and different types of surgery and cancer is warranted.
Conclusion
Our study is the first to use semi-structured interviews and qualitative analysis to assess treatment delays among early-stage surgery patients due to COVID. These interviews shed light on the essential role surgeons have in communicating treatment delays in an uncertain time. Best practices for cancer care should be adapted to assist providers in breaking bad news and conveying empathy when addressing difficult topics fraught with uncertainty, to promote strong patient–physician partnerships, even in a remote environment. These findings also underscore the importance of anticipating distress and screening cancer patients for distress early and frequently throughout care, particularly during the ongoing pandemic.
Supplementary Information
Below is the link to the electronic supplementary material.
Disclosure
The authors have no conflicts of interest related to this work. Dr. Trinh has general disclosures: honorarium (Bayer, Astellas, Janssen) and grant (Intuitive Surgical, Pfizer).
Footnotes
Christina Minami and Quoc-Dien Trinh are co-senior authors.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.American College of Surgeons. ACS guidelines for triage and management of elective cancer surgery cases during the acute and recovery phases of coronavirus disease 2019 (COVID-19) Pandemic. 2020. https://www.facs.org/-/media/files/covid19/acs_triage_and_management_elective_cancer_surgery_during_acute_and_recovery_phases.ashx. Accessed 17 Feb 2021.
- 2.Hwang ES, Balch CM, Balch GC, et al. Surgical oncologists and the COVID-19 pandemic: guiding cancer patients effectively through turbulence and change. Ann Surg Oncol. 2020 doi: 10.1245/s10434-020-08673-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Society for Surgical Oncology. Resource for management options of breast cancer during COVID-19; 2020.
- 4.National Comprehensive Cancer Network. Management of prostate cancer during the COVID-19 pandemic - Google Scholar. https://www.nccn.org/covid-19/pdf/NCCN_PCa_COVID_guidelines.pdf. Accessed 17 Feb 2021.
- 5.Dietz JR, Moran MS, Isakoff SJ, et al. Recommendations for prioritization, treatment, and triage of breast cancer patients during the COVID-19 pandemic. The COVID-19 pandemic breast cancer consortium. Breast Cancer Res Treat. 2020;181(3):487–497. doi: 10.1007/s10549-020-05644-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cutillo A, O’Hea E, Person SD, Lessard D, Harralson TL, Boudreaux E. The distress thermometer: cutoff points and clinical use. Oncol Nurs Forum. 2017;44(3):329–336. doi: 10.1188/17.ONF.329-336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chun Tie Y, Birks M, Francis K. Grounded theory research: a design framework for novice researchers. SAGE Open Med. 2019;7:2050312118822927. doi: 10.1177/2050312118822927. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sbaraini A, Carter SM, Evans R, Blinkhorn A. How to do a grounded theory study: a worked example of a study of dental practices. BMC Med Res Methodol. 2011;11(1):128. doi: 10.1186/1471-2288-11-128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Guest G, MacQueen K, Namey E. Validity and reliability (credibility and dependability) in qualitative research and data analysis. In: Applied Thematic Analysis. SAGE Publications, Inc.; 2014:79–106. 10.4135/9781483384436.n4.
- 10.Schwarze ML, Kaji AH, Ghaferi AA. Practical guide to qualitative analysis. JAMA Surg. 2020;155(3):252–253. doi: 10.1001/jamasurg.2019.4385. [DOI] [PubMed] [Google Scholar]
- 11.Morse JM. Data were saturated …. Qual Health Res. 2015;25(5):587–588. doi: 10.1177/1049732315576699. [DOI] [PubMed] [Google Scholar]
- 12.Smith SK, Loscalzo M, Mayer C, Rosenstein DL. Best practices in oncology distress management: beyond the screen. Am Soc Clin Oncol Educ B. 2018;38:813–821. doi: 10.1200/edbk_201307. [DOI] [PubMed] [Google Scholar]
- 13.Carr T, Teucher U, Mann J, Casson AG. Waiting for surgery from the patient perspective. Psychol Res Behav Manag. 2009;2:107–119. doi: 10.2147/PRBM.S7652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Arastu A, Patel A, Mohile SG, et al. Assessment of financial toxicity among older adults with advanced cancer. JAMA Netw Open. 2020;3(12):e2025810. doi: 10.1001/jamanetworkopen.2020.25810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chen G, Wu Q, Jiang H, et al. Fear of disease progression and psychological stress in cancer patients under the outbreak of COVID-19. Psychooncology. 2020;29(9):1395–1398. doi: 10.1002/pon.5451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Frey MK, Chapman-Davis E, Glynn SM, et al. Adapting and avoiding coping strategies for women with ovarian cancer during the COVID-19 pandemic. Gynecol Oncol. 2021;160(2):492–498. doi: 10.1016/j.ygyno.2020.11.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kennard K, Williams AD, Goldblatt LG, et al. COVID-19 Pandemic: changes in care for a community academic breast center and patient perception of those changes. Ann Surg Oncol. 2021 doi: 10.1245/s10434-020-09583-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Moran H, Brooks JV, Spoozak L. Undergoing active treatment for gynecologic cancer during COVID-19: a qualitative study of the impact on healthcare and social support. Gynecol Oncol Rep. 2020;34:100659. doi: 10.1016/j.gore.2020.100659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Minami CA, Kantor O, Weiss A, Nakhlis F, King TA, Mittendorf EA. Association between time to operation and pathologic stage in ductal carcinoma in situ and early-stage hormone receptor-positive breast cancer. J Am Coll Surg. 2020;231(4):434–447.e2. doi: 10.1016/j.jamcollsurg.2020.06.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Nguyen D-D, Haeuser L, Paciotti M, et al. Systematic review of time to definitive treatment for intermediate-risk and high-risk prostate cancer: are delays associated with worse outcomes? J Urol. 2021 doi: 10.1097/ju.0000000000001601. [DOI] [PubMed] [Google Scholar]
- 21.National Comprehensive Cancer Network. NCCN guidelines for patients distress during cancer care.; 2020. https://www.nccn.org/patients/guidelines/content/PDF/distress-patient.pdf. Accessed April 15, 2021.
- 22.American College of Surgeons. Optimal resources for cancer care 2020 standards. 2020. https://www.facs.org/-/media/files/quality-programs/cancer/coc/optimal_resources_for_cancer_care_2020_standards.ashx. Accessed 15 Apr 2021.
- 23.Kissane DW, Bylund CL, Banerjee SC, et al. Communication skills training for oncology professionals. J Clin Oncol. 2012;30(11):1242–1247. doi: 10.1200/JCO.2011.39.6184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Holwerda N, Sanderman R, Pool G, et al. Do patients trust their physician? The role of attachment style in the patient–physician relationship within one year after a cancer diagnosis. Acta Oncol (Madr) 2013;52(1):110–117. doi: 10.3109/0284186X.2012.689856. [DOI] [PubMed] [Google Scholar]
- 25.Hillen M. Cancer patients’ trust in their physician—a review. Psychooncology. 2010;20(3):227–241. doi: 10.1002/pon.1745. [DOI] [PubMed] [Google Scholar]
- 26.Wolf I, Waissengrin B, Pelles S. Breaking bad news via telemedicine: a new challenge at times of an epidemic. Oncologist. 2020;25(6):e879. doi: 10.1634/theoncologist.2020-0284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Pennell NA, Dicker AP, Tran C, Jim HSL, Schwartz DL, Stepanski EJ. mHealth: mobile technologies to virtually bring the patient into an oncology practice. Am Soc Clin Oncol Educ B. 2017;37:144–154. doi: 10.1200/edbk_176093. [DOI] [PubMed] [Google Scholar]
- 28.Sirintrapun SJ, Lopez AM. Telemedicine in cancer care. Am Soc Clin Oncol Educ B. 2018;38:540–545. doi: 10.1200/edbk_200141. [DOI] [PubMed] [Google Scholar]
- 29.Cox A, Lucas G, Marcu A, et al. Cancer survivors’ experience with telehealth: a systematic review and thematic synthesis. J Med Internet Res. 2017 doi: 10.2196/jmir.6575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Larson JL, Rosen AB, Wilson FA. The effect of telehealth interventions on quality of life of cancer patients: a systematic review and meta-analysis. Telemed e-Health. 2018;24(6):397–405. doi: 10.1089/tmj.2017.0112. [DOI] [PubMed] [Google Scholar]
- 31.Hamilton J, Kroska EB. Distress predicts utilization of psychosocial health services in oncology patients. Psychooncology. 2019;28(1):61–67. doi: 10.1002/pon.4910. [DOI] [PubMed] [Google Scholar]
- 32.Acquati C, Kayser K. Addressing the psychosocial needs of cancer patients: a retrospective analysis of a distress screening and management protocol in clinical care. J Psychosoc Oncol. 2019;37(3):287–300. doi: 10.1080/07347332.2018.1523822. [DOI] [PubMed] [Google Scholar]
- 33.Bleicher RJ. Timing and delays in breast cancer evaluation and treatment. Ann Surg Oncol. 2018;25(10):2829–2838. doi: 10.1245/s10434-018-6615-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.