

Abstract
In 2001, the German Multiple Sclerosis Society, facing lack of data, founded the German MS Registry (GMSR) as a long-term data repository for MS healthcare research. By the establishment of a network of participating neurological centres of different healthcare sectors across Germany, GMSR provides observational real-world data on long-term disease progression, sociodemographic factors, treatment and the healthcare status of people with MS. This paper aims to illustrate the framework of the GMSR. Structure, design and data quality processes as well as collaborations of the GMSR are presented. The registry’s dataset, status and results are discussed. As of 08 January 2021, 187 centres from different healthcare sectors participate in the GMSR. Following its infrastructure and dataset specification upgrades in 2014, more than 196,000 visits have been recorded relating to more than 33,000 persons with MS (PwMS). The GMSR enables monitoring of PwMS in Germany, supports scientific research projects, and collaborates with national and international MS data repositories and initiatives. With its recent pharmacovigilance extension, it aligns with EMA recommendations and helps to ensure early detection of therapy-related safety signals.
Subject terms: Health care, Multiple sclerosis
Introduction
Multiple sclerosis (MS) is the most frequent immune mediated disease of the central nervous system and the most common cause of non-traumatic disability among young adults1,2. In 2015, the cumulative incidence of MS in Germany was estimated at 18 new cases per 100,000 persons per year using public healthcare insurance data2. The yearly prevalence of MS diagnoses has steadily increased but there are still uncertainties concerning its aetiology3. The lack of legal reporting requirements for diagnosed MS cases and difficulties involved in accessing routine medical data impede access to reliable information on MS prevalence and incidence, as well as healthcare standards for persons with MS (PwMS) in Germany. Insufficient interoperability of different electronic healthcare record systems is another reason for the lack of a population-based database. A nationwide MS registry with representative coverage of PwMS would offer the opportunity to monitor long-term disease epidemiology and the health of PwMS. Furthermore, a national MS registry can contribute to data on disease costs, cost–benefit-ratios, quality of healthcare, and patient-reported outcomes (PRO), which is important to the evaluation of PwMS’s quality of life and to regulatory decisions4.
Treatment guidelines for chronic diseases like MS are often established based upon limited evidence regarding the real-world efficacy and safety of disease modifying treatments (DMT)5,6. Additionally, long-term therapeutic effects beyond the duration of phase III clinical trials, and treatment strategy studies are frequently unavailable7. Considering the rapid development of DMT and the significant role of the diverse disease characteristics and patient responses to and preferences in treatment, the documentation of complex individual treatment profiles is becoming increasingly important for personalised treatment decisions that take into account individual disease courses and patient preferences7–9.
Considering several observational studies indicating that early initiation and continuous use of highly effective DMT may reduce risks of long-term disability progression, there is a need for predictive tools to identify the most beneficial treatment strategies9,10. Regarding these needs, registries can provide real-world data to support physicians and PwMS in treatment decisions. Recent incidents of serious adverse events, like endocarditis11, or multifocal leukoencephalopathy12 in PwMS on DMT highlighted the importance of standardised safety data collection under real-world conditions13. In 2017, the European Medicines Agency initiated a workshop bringing together regulatory bodies, market authorisation holders, academics, and registry custodians to discuss the extended use of MS registries for post-authorisation safety monitoring14.
This article aims to show the framework and current setup of the German MS registry (GMSR), including its methodology, technological infrastructure, and network as a reliable nationwide long-term data repository and resource for registry-based trials.
Materials and methods
This article describes the governance, funding, and design of the GMSR. Its history, data collection processes, description of datasets and data quality control mechanisms are outlined, and its research projects presented. Descriptive analysis outlining the status of the GMSR was carried out using R Stat 4.0 (R Foundation, Vienna, Austria). Data for descriptive analyses was extracted 8 January 2021. Data records that were locked due to e.g. documentation errors and records with pending queries were excluded from analysis. Graphical representations include histograms for expanded disability status scale (EDSS) distributions, scatterplots of patient demographics, and clinical characteristics at entry of the GMSR, including two-dimensional density estimates, shown as contour plots (heat maps), and line charts of patients and visit frequency.
Results
The GMSR’s objectives
The GMSR aims to provide a reliable long-term data repository for transparency in epidemiology, demographics, disease characteristics, healthcare access and quality of care of PwMS in Germany, and may be used to monitor improvements of healthcare15. It also implements and supports scientific research projects such as registry-based (randomised) controlled trials and collaborations with other (inter-)national repositories in a modular fashion16. One of its emerging objectives is the collection and reporting of real-world safety data on disease modifying drugs.
The GMSR’s design
The GMSR established a network of participating centres across different healthcare sectors in Germany (see Fig. 1). Centres that were accredited ‘MS Centre’, ‘Specialised MS Centre’, or ‘MS Rehabilitation Centre’ by the German MS Society participate in the GMSR documentation. Certificates are awarded to university clinics, acute care clinics, rehabilitation clinics, MS outpatient clinics and resident neurologists complying with specific criteria. Compliance is re-evaluated every 2 years17. With this certificate, each centre commits itself to recruiting PwMS and collecting data for the GMSR. Physicians and other medical staff carry out patient enrolment and data collection for the registry during routine examinations. After the provision of written informed consent by adult PwMS (see Table 1), previous medical data can be collected, and prospective data collection starts and is carried out until the patient’s death or withdrawal of informed consent.
Figure 1.
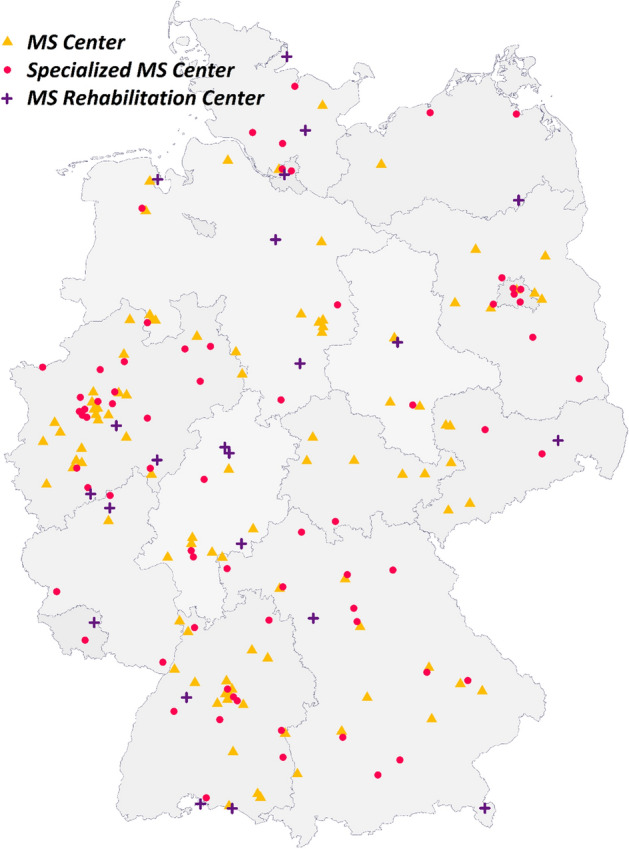
Distribution of 187 MS centres participating in the GMSR across Germany. These include 70 specialised MS centres (red circle), 95 MS centres (orange triangle), and 22 MS rehabilitation centres (purple cross). GMSR German Multiple Sclerosis registry. The map was created with R 4.0 based on data from gadm.org.
Table 1.
Inclusion and exclusion criteria of the GMSR.
| Inclusion criteria | Exclusion criteria |
|---|---|
| Age ≥ 18 years | Indefinable MS disease type (according to McDonald or Poser criteria) at date of inclusion |
| Written informed consent provided | Inability to give informed consent |
| Diagnosed MS (according to the applicable McDonald or Poser criteria) with definable disease type or clinically isolated syndrome (CIS) | |
| Primary residence in Germany |
CIS clinically isolated syndrome, MS multiple sclerosis.
Members of the medical staff enter data into a web-based electronic data capture (EDC) system. This system allows a single patient’s data to be reported by multiple centres. To avoid duplicate patient entries, patient-identifying data (first name, last name, sex, date of birth) is entered into the registry at enrolment and used to generate a unique pseudonym. A trusted third party stores these pseudonyms and the corresponding identifying data separated from the registry data. To guarantee patient privacy, only de-identified medical data is stored in the registry’s database and used for analysis.
Data collection
In 2005, the registry started regular operations and has been continuously improved since then. At first, data was collected through the ‘MSDS Klinik/Praxis’ software, which had been locally installed in centres. Encoded datasets stored digitally were transmitted quarterly to the MSFP-gGmbH (MSFP) for quality checks and analysis. Since 2016, it is mandatory to document via the standardised web-based platform and device-independent EDC-system ‘secuTrial’ and documentation through MSDS has been discontinued. The web-based EDC-system is compliant with established tools and concepts of the Technology and Methods Platform for Networked Medical Research e.V. (TMF) and is certified for conducting clinical trials (GCP, GAMP5, FDA 21 CFR Part 11). PRO can be integrated to the system through patients uploading information themselves through an app or web browser. Data entry happens directly through interfaces of the EDC system.
Governance of the GMSR
The GMSR is operated by the MSFP, a non-profit organisation founded in 2001 as a subsidiary of the German Multiple Sclerosis Foundation to develop and manage the registry on behalf of the German Multiple Sclerosis Society. The governance of the GMSR includes a scientific advisory group of clinicians and representatives of MS centres as well as methodology experts (of medical statistics, epidemiology and medical informatics), that approves and oversees scientific projects and research activities18.
Ethical considerations/registration
The GMSR was first approved by the ethics committee of the Julius-Maximilians-University of Würzburg (number of vote 142/12). After switching to a web-based documentation system, it received further ratification from ethical committees such as the Thuringia state chamber of physicians and other universities.
Before inclusion to the MS registry, patients are informed about its conduct by medical staff and must provide written informed consent before data collection can commence. Within this consent, patients can allow their data to be used for further research activities. Data collection, storage and analysis are conducted according to current European and national legislations for data protection.
The GMSR is registered at the German registry of clinical trials with registration number DRKS00011257, and at the European Network of Centres for Pharmacoepidemiology and Pharmacovigilance with reference number ENCEPP/DSPP/21378.
History of GMSR
The history of the GMSR is described in Supplementary Document 1.
Dataset
In 2014, the GMSR’s dataset was revised to fulfil the increased requirement for harmonization and comparability of data of different data sources. As a result, the dataset is a combination of datasets of the German Multiple Sclerosis Society and the German Competence Network Multiple Sclerosis. The current minimal dataset (see Supplementary Table 1) contains information on disease onsets, diagnoses, MS disease courses19,20, disabilities (as measured in EDSS and MS Functional Composite as well by MS Symptoms), disease activity, MS therapy and socio-economic statuses21. In 2019, the GMSR dataset was extended by a pharmacovigilance module to include documentation on medical history, body mass index, adverse events and pregnancies (see Table 2). This documentation has been rolled out to eligible centres. The GMSR dataset is expandable regarding new research questions and adapts to the specific requests of documenting parties using its dynamic web-based EDC system and modular structure. Physicians schedule frequency of visits according to patients’ needs for medical care and routine follow-ups, which the registry recommends to be carried out at least on an annual basis. Relapses, adverse events, and pregnancies are documented as separate events.
Table 2.
GMSR dataset.
| Dataset description | |
|---|---|
| Informed consent | Inclusion and exclusion criteria |
| Scope of consent | |
| Patient profile | Sex |
| Date of birth | |
| Diagnostic criteria (McDonald, Poser) | |
| Disease onset | |
| Date of diagnosis | |
| Initial symptoms | |
| Retrospective medical history data | |
| Sociodemographic data | Education |
| Occupation | |
| Family status | |
| Residence | |
| Disease status | Disease course (lublin categories) |
| Expanded disability status scale | |
| MRI reports | |
| Multiple sclerosis functional composite-index (Nine-hole peg test, PASAT3, 25-foot walk test) | |
| Symptomatic therapy | Symptoms |
| Therapy | |
| Medicationa | Prior and current disease-modifying treatment |
| Treatment duration | |
| Reasons for treatment discontinuations/switches | |
| (In)dependence | Type of care |
| Medical aides | |
| Relapses | Relapse date |
| Therapy | |
| Pharmacovigilance-Module* | Comorbidities |
| Adverse events | |
| Pregnanciesa |
GMSR German multiple sclerosis registry, PASAT3 paced auditory serial addition test (3 s-interstimulus interval).
*Voluntary extended documentation, not collected by default.
aThe GMSR cooperates with the German MS and child wish registry to allow follow up in more detail.
Data quality
To constantly ensure high data quality, the GMSR established a wide range of quality control measures. The web-based data entry system ensures that centres have the latest versions of questionnaires. Each questionnaire is checked for consistency of dates, of value ranges and for plausibility. Branching logic (asking only relevant questions based on previous answers) ensures that data is only entered for applicable fields. Furthermore, cross-reference-checks compare data between different questions and forms. Longitudinal checks aim at preventing implausible data changes over time. Additionally, the registry uses R-Syntax for automated quality control to find discrepancies and implausibilities. Participating centres receive findings through query management system within the EDC-System. All data changes are recorded in audit trails. The database only accepts records with the completed minimal dataset. Participating centres are provided with training materials and tutorials. Yearly benchmarking reports include visualised comparative data, based on the centre’s population versus other centres’ populations of the same type and individual feedback on data quality. Centres and MSFP can execute ad-hoc statistics and reports as well as customised database searches at any time.
Data analysis
The GMSR conducts retrospective analysis for a variety of MS-related research questions. These include demographic studies, measurements of care availability, causal inferences but also pharmacovigilance studies and epidemiological assessments6,22–25. Most analyses are performed using R26. Before data is analysed, it is checked for duplicates, completeness, plausibility and consistency. The GMSR’s data is accessible at reasonable request by any qualified investigator under terms and conditions of the registry’s use-of-access policies and subject to informed consent of patients. Requests for research projects can be proposed via an application form on GMSR’s website18.
Status quo
As of January 2021, 187 centres of all healthcare sectors throughout Germany participate in the GMSR, and the new registry database includes documentation of more than 196,000 consultations of more than 33,000 PwMS. Figure 1 shows the geographic distribution of participating centres across Germany. 5% of registered patients were reported by multiple centres. Recent estimations based on the claims data of participating centres put the number of PwMS treated annually by the participating centres at approximately 90,000. Thus, covering about one-third of the German MS-population (estimated at 240,000–250,000).
At time of data extraction, the yearly documentation for 2020 included 26,491 visits of more than 13,000 patients, with an average of two consultations per patient per year (see Fig. 2). 3530 patients joined the registry in 2020. Table 3 shows the number of visits in which specific (sets of) variables are present.
Figure 2.

Number of recorded visits per years (by January 2021). Total (cumulative) number of patients included in the GMSR by the end of each year is shown by the black solid line, while the number of patients with actual baseline or follow-up visits during the resp. year is shown by the dashed line. The number of visits per year is show as bars, distinguishing baseline and follow-up visits. GMSR German Multiple Sclerosis registry.
Table 3.
Number of patients and visits by scale/category of information.
| Number of visits | Number of patients | |
|---|---|---|
| Total | 196,632 | 33,174 |
| History of onset and diagnosis (dates) | – | 29,019 |
| Education | 121,155 | 27,172 |
| Employment | 154,394 | 28,677 |
| Family | 178,794 | 31,096 |
| Nine-hole peg test | 30,019 | 8194 |
| 25-foot walk test | 17,829 | 7808 |
| EDSS | 201,712 | 33,059 |
| MRI | 35,427 | 18,318 |
| DMD (y/n) | 164,660 | 31,734 |
| Current MS-symptoms* | 172,032 | 32,277 |
| (In-)dependence** | 165,204 | 31,597 |
DMD disease modifying drugs, EDSS expanded disability status scale, MRI magnetic resonance imaging.
*Fatigue, paresis, bowel and bladder disturbances etc.
**Care settings and the prescription/use of aids.
In total, more than 33,000 PwMS were included in the MS Registry since 2014. Baseline data separated by disease course as well as the current distribution of EDSS scores of patients are presented in Supplementary Table S2 and in Fig. 3. In 2020, 4% of visits were documented by rehabilitation centres, 43% by MS centres and 53% by specialised MS centres. By January 2021, 75% of queries on visits data of 2020 were answered and closed. The average time for a final response to a query was 4 (± 7) months (median 1 month) and 81% of all queries were answered.
Figure 3.

Current EDSS distribution among patients (n = 33,059) in the GMSR. EDSS expanded disability status scale, GMSR German Multiple Sclerosis registry.
The GMSR baseline demographic data is comparable to recent publications based on German statutory health claims data regarding female to male ratios, most affected age groups and geographical distribution. The age and disease duration of PwMS at registry entry are presented in Supplementary Figure 1. Compared to European MS registries, there are differences in reported percentages of secondary progressive MS (SPMS) within the registry’s population, whereas the differences in EDSS are narrower. Wider DMT options for patients with relapsing–remitting MS (RRMS) may be the reason for a bias in classification by the treating neurologist27. Table 4 compares baseline GMSR patient data with data from the registries of Italy, Denmark, France, and Sweden28–32.
Table 4.
Comparison of patient characteristics.
| German MS registry | Italian MS registry22 | Danish MS registry23,24 | OFSEP25 | Swedish MS registry26 | |
|---|---|---|---|---|---|
| Female | 71% | 67% | 69% | 71% | 70.3% |
| Age at onset (years) | 33.1 ± 10.7 | 30.5 ± 10.5 | 32.6 ± 10.8 | ||
| CIS | 1.8% | 5.6% | 2.4% | 12.1% | |
| RRMS | 75.8% | 75.3% | 80% | 55.2% | 67.5% |
| SPMS | 15.7% | 12.9% | 12.7% | 21.4% | 24.6% |
| PPMS | 6.7% | 6.1% | 4.8% | 11.2% | 7.9% |
Patients with unknown disease course are excluded.
CIS clinically isolated syndrome, MS multiple sclerosis, OFSEP observatoire français de la sclérose en plaques, PPMS primary progressive MS, RRMS relapsing–remitting MS, SPMS secondary progressive MS.
Funding
The establishment and maintenance of the GMSR is funded by the German Multiple Sclerosis Foundation and the German Multiple Sclerosis Society. Additionally, the MSFP has received financial support from Biogen, Bristol Myers Squibb, Merck Serono, Novartis, Roche and Sanofi for the specific purposes of operating the GMSR. Principles of the cooperation between MSFP and pharmaceutical companies are: (1) Transparency: each stakeholder gets the same information at the same time and the type and scope of sponsorship is made public, (2) Financing: to avoid an increased influence of a single stakeholder or a financial dependence on one funder, stakeholders contribute equal amounts, regardless of the company’s market share, (3) Information exchange: stakeholders meet at least once a year to discuss results, ideas for scientific evaluations and further joint activities, (4) Scientific independence: the MSFP has the right to publish registry results independently.
Registry-based studies and sub-cohorts
Besides the operation of the MS registry, the MSFP develops and provides the EDC system for MS research projects that can (partly) be linked to registry data (see Supplementary Table 2)33.
Discussion
The GMSR is a unique and reliable long-term data repository for real-world data on epidemiology and health of PwMS in Germany. It allows long-term monitoring of the disease course, analysis of different treatments and evaluation of the comparative efficacy, effectiveness and safety of an increasing number of DMT, which cannot be addressed as much by randomised clinical trials (RCT)10,24,34. The GMSR holds data on all approved DMT instead of focusing on specific drugs24. In RCT, inclusion criteria often do not fit the effect mechanism of the active substance, for instance, patients with low disease activity or long disease duration are included in studies on high anti-inflammatory effect substances7. Their high costs and intensity result in their rather short duration and insufficiency concerning real-world effectiveness in the long-term1,7. Therefore, registry data is important for patients, physicians, industry, regulatory authorities and health insurance system to provide support to treatment decisions and the development of health promotion measures5,10.
The increasing number of DMTs leads to individual treatment decisions, which consider disease related variables like symptoms or clinical findings, but also patient preferences. The evaluation of the severity and significance of specific patient symptoms and their consequences for disease management are often different from that of physicians35. Consequently, PRO will become more important3,7. The technical infrastructure of the GMSR allows implementation of PRO measurement via eCRFs that can be completed directly by patients and is directly linked to medical data36.
The creation of an added value within the GMSR for health professionals to document disease progression and treatment history directly through the EDC system, like automatically generated discharge letters and medical reports, could encourage them to participate in the MS registry and is constantly pursued by the GMSR. A technical interface to the centre’s primary information system could have a similar effect due to the reduced documentation effort. It could furthermore establish a documentation system for several different prospective studies and reduce time and costs expenditure in the future. Despite its positive effects, the reuse and integration of electronic healthcare records for research purposes is still in its early stages37.
To increase follow-up rates, it is necessary to provide an incentive for participating centres to document visits regularly. Possible incentives which are offered by the GMSR to achieve this goal are financial compensation, requirements analysis at annual user meetings and guidance documents for follow-up processes.
Over the years, the GMSR’s findings have benefited MS science. The monitoring of PwMS through the registry allowed for the first-time estimates concerning its prevalence, disease types, symptoms and degree of symptomatic treatment. Furthermore, the registry enables register based RCTs and General Data Protection Regulation compliant patient recruitment.
Recently, evaluations of registry data on symptom frequency and symptomatic treatment patterns showed that fatigue is one of the most common symptoms. This has only been analysed in smaller cohorts38 but is of high importance as fatigue impacts patients well-being and employment30. Through GMSR’s participation in international projects, insights and comparison of data of PwMS from other countries and healthcare systems, such as employment statuses23, time until the initiation of a DMT22 and validation of secondary progressive MS classification methods39 were gained.
However, the GMSR suffers from certain biases and limitations. The registry is not population-based. To date, there is no legal obligation to report MS cases in Germany. The introduction of an obligation would contribute to completeness of the registry’s data and nationwide coverage. PwMS are treated in all areas of care (e.g. general practioners, urologist etc.) and are therefore not always seen regularly in a specialised neurologic unit, thus a legal obligation like in cancer would ensure the completeness. As the registry focuses on neurological care providers of special experience in the treatment of PwMS, the proportion of clinically diagnosed RRMS cases is higher than presented in the German statutory claims data. Our estimations show that since its revision in 2014, the registry has captured more than 33,000 PwMS resulting in about one-third of the PwMS seen in the participating centres. If data from the prior registry data collection, commenced at the turn of the century, is included, the coverage of the GMSR reaches more than 73,000 PwMS. On annual basis the participating specialised centres treat roundabout one-third of the prevalent German MS-population. Especially PwMS suffering from progressive disease courses tend to seek neurological expertise less often, possibly explaining their underrepresentation in the GMSR. However, by including PwMS from specialised rehabilitation centres, the GMSR still captures a higher percentage of the progressive patients than if it would just recruit from outpatient facilities40.
Recent research on the conversion of RRMS into SPMS within the GMSR and other registries showed that significant amounts of patients might be clinically labelled as RRMS while still receiving DMTs although objective algorithms would judge the disease course differently27.
With legal barriers in place that make the inclusion of under-age PwMS quite challenging and specific paediatric data collections already in place it was decided in the conception phase of the GMSR to allow registry entry only to adult PwMS. Paediatric MS patients are often treated in different settings than adult MS-patients. However, the informed consent allows the collection of retrospective data from patients and paediatric onset MS patients are included after their 18th birthday in the GMSR41,42.
With no public funding for maintaining a long-term operation of a data source like the GMSR, funding remains a challenge that cannot be solely covered by the patient society. The GMSR has therefore started to involve the industry for funding. The extension of the dataset by the pharmacovigilance module was an important step for the use of registry data in non-interventional PASS, which was promoted by the EMA43. This may reduce costs, increase transparency, and create confidence in the value of pharmacotherapy of MS.
Supplementary Information
Acknowledgements
We would like to thank all the patients who gave their informed consent. Furthermore, this study would not have been possible without the efforts of the centres participating in the registries. The centres are listed in the Supplement.
Author contributions
L.M.O. substantially contributed to the conception, to the study design and to the data interpretation. She drafted the manuscript and critically revised the completed final draft for important intellectual content. D.E. substantially contributed to the conception, to the study design and to the data interpretation. He conducted the statistical analysis and critically revised the completed final draft for important intellectual content. P.F., T.F., J.H., K.H., T.P., C.W., F.P. and U.K.Z. critically revised the completed final draft for important intellectual content and contributed to the revision. A.S. substantially contributed to the conception, to the study design and to the data interpretation. He supervised this study and critically revised the completed final draft for important intellectual content.
Funding
The German MS Registry of the German MS Society was initiated and funded by the German MS Foundation and the German MS Society in 2001. It is operated by a not-for-profit company, the MSFP. In 2021, Biogen, Celgene (BMS), Merck, Novartis Roche and Sanofi are participating in the multi-stakeholder funding approach to support the registry’s operation and to allow the collection and reporting of data required as part of the EMA-minimal data set. Industry funding does not result in restrictions to publishing data, nor do the funders have access to the raw data or have any influence over the scientific conduct of the registry.
Competing interests
Lisa-Marie Ohle reports no disclosure relevant to the content of the submitted manuscript, her work on the project was funded by a grant from the innovation fund of the German Federal Joint Committee (01VSF18038). David Ellenberger reports no disclosure relevant to the content of the submitted manuscript. Peter Flachenecker has received speaker’s fees and honoraria for advisory boards from Almirall, Bayer, Biogen Idec, Celgene, Genzyme, Novartis, Merck-Serono, Roche and Teva. He has participated in pharmaceutical company sponsored trials by Roche. None resulted in a conflict of interest. Tim Friede has received personal fees for consultancies (including data monitoring committees) in the past three years from Bayer, Biosense Webster, Boehringer Ingelheim, Cardialysis, CSL Behring, Daiichi Sankyo, Enanta, Fresenius Kabi, Galapagos, Janssen, Liva Nova, Novartis, Parexel, Penumbra, Roche, SGS, Vifor; all outside the submitted work. Judith Haas reports no disclosure relevant to the content of the submitted manuscript. Kerstin Hellwig reports no disclosure relevant to the content of the submitted manuscript. Tina Parciak reports no disclosure relevant to the content of the submitted manuscript. Friedemann Paul has received speaking fees, travel support, honoraria from advisory boards, and/or financial support for research activities from Bayer, Novartis, Biogen, Teva, Sanofi-Aventis/Genzyme, Merck Serono, Alexion, Chugai, MedImmune, Shire, German Research Council, Werth Stiftung of the City of Cologne, German Ministry of Education and Research, EU FP7 Framework Program, Arthur Arnstein Foundation Berlin, Guthy Jackson Charitable Foundation, and National Multiple Sclerosis of the USA. He serves as academic editor for PLoS ONE and associate editor for Neurology, Neuroimmunology and Neuroinflammation. None resulted in a conflict of interest. Clemens Warnke has received institutional support from Novartis, Alexion, Sanofi-Genzyme, Biogen, Janssen, and Roche. Uwe K. Zettl has received speaking fees, travel support and /or financial support for research activities from Alexion, Almirall, Bayer, Biogen, Bristol-Myers-Squibb, Janssen, Merck Serono, Novartis, Octapharm, Roche, Sanofi Genzyme, Teva as well as EU, BMBF, BMWi and DFG. None resulted in a conflict of interest. Alexander Stahmann has no personal pecuniary interests to disclose, other than being the lead of the German MS Registry, which receives funding from a range of public and corporate sponsors, recently including The German Innovation Fund (G-BA), The German MS Trust, German MS Society, Biogen, Celgene (Bristol Myers Squibb), Merck Serono, Novartis, Roche and Sanofi. None resulted in a conflict of interest.
Footnotes
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
The online version contains supplementary material available at 10.1038/s41598-021-92722-x.
References
- 1.Flachenecker P, Stuke K. National MS registries. J. Neurol. 2008;255:102–108. doi: 10.1007/s00415-008-6019-5. [DOI] [PubMed] [Google Scholar]
- 2.Holstiege J, Steffen A, Goffrier B, Bätzing J. Epidemiology of multiple sclerosis—A population-based, Germany-wide study. Versorgungsatlas. 2017;17(09):1–16. [Google Scholar]
- 3.Committee for Medicinal Products for Human Use (CHMP). Guideline on Clinical Investigation of Medicinal Products for the Treatment of Multiple Sclerosis. https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-investigation-medicinal-products-treatment-multiple-sclerosis_en-0.pdf (2015).
- 4.Flachenecker P, et al. Multiple sclerosis registries in Europe—Results of a systematic survey. Mult. Scler. 2014;20:1523–1532. doi: 10.1177/1352458514528760. [DOI] [PubMed] [Google Scholar]
- 5.Jalusic KO, et al. Effect of applying inclusion and exclusion criteria of phase III clinical trials to multiple sclerosis patients in routine clinical care. Mult. Scler. 2021 doi: 10.1177/1352458520985118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ellenberger D, et al. Decreasing longitudinal use of glucocorticosteroids in multiple sclerosis. Mult. Scler. Relat. Disord. 2018;25:173–174. doi: 10.1016/j.msard.2018.07.040. [DOI] [PubMed] [Google Scholar]
- 7.Gehr S, Kaiser T, Kreutz R, Ludwig WD, Paul F. Suggestions for improving the design of clinical trials in multiple sclerosis—Results of a systematic analysis of completed phase III trials. EPMA J. 2019;10:425–436. doi: 10.1007/s13167-019-00192-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Steinemann N, et al. The Swiss Multiple Sclerosis registry (SMSR): Study protocol of a participatory, nationwide registry to promote epidemiological and patient-centered MS research. BMC Neurol. 2018;18:111. doi: 10.1186/s12883-018-1118-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Laakso SM, et al. Multiple sclerosis in Finland 2018—Data from the national register. Acta Neurol. Scand. 2019;140:303–311. doi: 10.1111/ane.13145. [DOI] [PubMed] [Google Scholar]
- 10.Trojano M, et al. Treatment decisions in multiple sclerosis—Insights from real-world observational studies. Nat. Rev. Neurol. 2017;13:105–118. doi: 10.1038/nrneurol.2016.188. [DOI] [PubMed] [Google Scholar]
- 11.Faissner S, et al. Endocarditis following ocrelizumab in relapsing-remitting MS. Neurol. Neuroimmunol. Neuroinflamm. 2020;7:e680. doi: 10.1212/NXI.0000000000000680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Toorop AA, et al. Mild progressive multifocal leukoencephalopathy after switching from natalizumab to ocrelizumab. Neurol. Neuroimmunol. Neuroinflamm. 2021;8:e904. doi: 10.1212/NXI.0000000000000904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rommer PS, et al. Management of MS patients treated with daclizumab—A case series of 267 patients. Front. Neurol. 2020;11:996. doi: 10.3389/fneur.2020.00996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.European Medicines Agency. Report on Multiple Sclerosis Registries—Workshop 7 July 2017. https://www.ema.europa.eu/en/documents/report/report-multiple-sclerosis-registries_en.pdf (2017).
- 15.Zettl UK, et al. MS in Deutschland: Symptome und behandlungsdefizite—aktuelle daten aus dem MS-register der DMSG für die MS-forschung. Neurotransmitter. 2018;29:36–39. doi: 10.1007/s15016-018-6423-8. [DOI] [Google Scholar]
- 16.Rahn AC, et al. Development and evaluation of an interactive web-based decision-making programme on relapse management for people with multiple sclerosis (POWER@MS2)—Study protocol for a randomised controlled trial. Trials. 2021;22:139. doi: 10.1186/s13063-021-05059-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.German Multiple Sclerosis Society, Federal Association e.V (DMSG). [DMSG-awarded centres]. https://www.dmsg.de/service/kliniken-praxen/dmsg-ausgezeichnete-zentren/ (2021).
- 18.MS Research and Project Development gGmbH (MSFP). Website of the GMSR. https://www.msregister.de/en.
- 19.Ellenberger D, et al. Is benign MS really benign? What a meaningful classification beyond the EDSS must take into consideration. Mult. Scler. Relat. Disord. 2020;46:102485. doi: 10.1016/j.msard.2020.102485. [DOI] [PubMed] [Google Scholar]
- 20.Ellenberger D, et al. Aggressive multiple sclerosis—A matter of measurement and timing. Brain. 2020;143:e97. doi: 10.1093/brain/awaa306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Rommer PS, et al. Relapsing and progressive MS: The sex-specific perspective. Ther. Adv. Neurol. Disord. 2020;13:1756286420956495. doi: 10.1177/1756286420956495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Stahmann A, et al. Variation in time to first disease modifying therapy in people with MS in the United States, United Kingdom, and Germany (517) Neurology. 2020;94:517. [Google Scholar]
- 23.Salter A, et al. Data harmonization for collaborative research among MS registries: A case study in employment. Mult. Scler. 2021;27:281–289. doi: 10.1177/1352458520910499. [DOI] [PubMed] [Google Scholar]
- 24.Flachenecker P, et al. Multiple sclerosis in Germany: Updated analysis of the German MS Registry 2014–2018. Fortschr. Neurol. Psychiatr. 2020;88:436–450. doi: 10.1055/a-0985-4124. [DOI] [PubMed] [Google Scholar]
- 25.Rommer PS, et al. Symptomatology and symptomatic treatment in multiple sclerosis: Results from a nationwide MS registry. Mult. Scler. 2019;25:1641–1652. doi: 10.1177/1352458518799580. [DOI] [PubMed] [Google Scholar]
- 26.R Core Team. R: A Language and Environment for Statistical Computing. https://www.R-project.org (2020).
- 27.Hillert, J. et al.Ongoing Disease Modifying Treatment Associated with Mis-classification of Secondary Progressive as Relapsing-Remitting Multiple Sclerosis. https://cslide.ctimeetingtech.com/msdc2020/attendee/confcal/session/calendar?q=hillert&r=pt%7E43 (2020).
- 28.Trojano M, et al. The Italian Multiple Sclerosis register. Neurol. Sci. 2019;40:155–165. doi: 10.1007/s10072-018-3610-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Magyari M, Joensen H, Laursen B, Koch-Henriksen N. The Danish Multiple Sclerosis registry. Brain Behav. 2021;11:e01921. doi: 10.1002/brb3.1921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.The Multiple Sclerosis International Federation (MSIF). Atlas of MS, 3rd edition. www.atlasofms.org (2020).
- 31.Observatoire français de la sclérose en plaques (OFSEP). Description de la cohorte OFSEP au 15 décembre 2019. http://www.ofsep.org/fr/la-cohorte-ofsep/descriptif-de-la-cohorte (2019).
- 32.Swedish MS registry (SMSREG). Web-based platform for live visualization and interactive statistical analysis: Mean EDSS value for patients by county. https://vap.carmona.se/open/msvap/graf/oj_medel_edss_cross/ (2020).
- 33.Spiekerkötter, L.-M. et al.Das MS-Register der DMSG als Plattform für die Forschung: Vorteile einer einheitlichen und verknüpften Datenerfassung. https://www.dgnvirtualmeeting.org/#!resources/das-ms-register-der-dmsg-als-plattform-fur-die-forschung-vorteile-einer-einheitlichen-und-verknupften-datenerfassung (2020).
- 34.McGettigan P, et al. Patient registries: An underused resource for medicines evaluation: Operational proposals for increasing the use of patient registries in regulatory assessments. Drug Saf. 2019;42:1343–1351. doi: 10.1007/s40264-019-00848-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Heesen C, et al. Perceptions on the value of bodily functions in multiple sclerosis. Acta Neurol. Scand. 2018;137:356–362. doi: 10.1111/ane.12881. [DOI] [PubMed] [Google Scholar]
- 36.Stahmann A, Meyer C, Lee M, Buckow K. PRO-dokumentation von lebensqualitätsdaten im MS-register der Deutschen multiplen sklerose gesellschaft (DMSG) Bundesverband e.V. mdi Forum Med. Dok. Med. Inform. 2015;17:18–19. [Google Scholar]
- 37.von Martial S, et al. EMR-integrated minimal core dataset for routine health care and multiple research settings: A case study for neuroinflammatory demyelinating diseases. PLoS ONE. 2019;14:e022886. doi: 10.1371/journal.pone.0219656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Wood B, et al. Prevalence and concurrence of anxiety, depression and fatigue over time in multiple sclerosis. Mult. Scler. 2013;19:217–224. doi: 10.1177/1352458512450351. [DOI] [PubMed] [Google Scholar]
- 39.Forsberg L, Glaser A, Manouchehrinia A, Ramanujam R, Spelman T. Validation of three secondary progressive multiple sclerosis classification methods in five registries within the spms research collaboration network. Mult. Scler. 2020;26:1–42. [Google Scholar]
- 40.Weih M, et al. Data on multiple sclerosis in Germany and their representation in the ambulatory registry NeuroTransData (NTD) network. Fortschr. Neurol. Psychiatr. 2020;88:379–385. doi: 10.1055/a-1130-6222. [DOI] [PubMed] [Google Scholar]
- 41.Haas, J. et al. Verlauf der MS bei Beginn im Kindesalter. DGN Congress (2019).
- 42.Stahmann, A. et al. Employment outcomes in paediatric onset MS. ECTRIMS Congress (2019).
- 43.European Medicines Agency. Patient registries. https://www.ema.europa.eu/en/human-regulatory/post-authorisation/patient-registries.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.