

Abstract
Background:
Anterior cruciate ligament (ACL) reconstruction with suture tape reinforcement has been shown to biomechanically reduce elongation and increase ultimate strength. However, the amount and consistency of the achieved tension after primary fixation using knotless suture anchors remains unclear.
Purpose:
To determine whether initial tensioning of suture tape before fixation with a knotless suture anchor significantly affects final tension of the suture tape.
Study Design:
Controlled laboratory study.
Methods:
We secured 15 pairs of Sawbones blocks with predrilled tunnels to a tensile testing machine. Suture tape was inserted through a suspensory fixation button on the representative femoral block and threaded top-down through the base of the tibial block over an attachable button system. The suture tape was attached with a knotless suture anchor in a predrilled and tapped hole on the tibial block under the following pretensioning conditions: (1) slight tension of 5 N, (2) no tension, and (3) initial slack. The suture anchor was inserted as the load-time data were recorded. After initial block testing, a porcine model of 24 tibias was used to test the same pretensioning conditions. The initial loads during anchor insertion and screw-in were measured, as well as final tension.
Results:
During block testing, no difference in final tensioning was found when comparing the slight-tension, no-tension, and slack groups (42.3 ± 5.3, 37.7 ± 6.4, and 40.2 ± 7.0 N, respectively; P = .528). Similar to block testing, no difference in final tensioning was found when comparing the slight-tension, no-tension, and slack groups using the porcine model (43.64 ± 6.69, 48.09 ± 13.93, and 44.52 ± 6.84 N, respectively; P = .633).
Conclusion:
The final tension of the suture tape construct appears to be reproducible and consistent, independent of the initial tension introduced with suture anchor placement within the tested parameters.
Clinical Relevance:
The results of the current study can help optimize the placement technique of independent suture tape reinforcement for ACL reconstruction, which is a promising strategy to help prevent ACL rerupture, particularly in the early phases of postoperative rehabilitation.
Keywords: ACL reconstruction, internal bracing, knotless fixation, self-tensioning
Among the most common knee injuries are tears of the anterior cruciate ligament (ACL), with roughly 150,000 ACL reconstructions performed annually in the United States. 13,16 Rerupture after ACL reconstruction continues to be problematic, especially in young, active patients with a high rate of return to high-risk sports. 18 With the goal of preventing rerupture, internal bracing using independent suture tape reinforcement is increasingly being used in soft tissue knee ligament surgery, including ACL reconstruction. 2,5,8 –10 First described by Mackay et al, 12 the goal of the suture tape reinforcement is to act as a “safety belt” in a synergistic load-sharing manner, while avoiding stress shielding of the soft tissue graft. 14 This is particularly relevant to patients undergoing an accelerated postoperative rehabilitation program, in which the internal bracing of the ACL graft during the revascularization process is a potential benefit. 15 It has previously been shown that ACL reconstruction utilizing suture tape augmentation leads to significantly reduced elongation and increased ultimate strength of the construct. 1 In the majority of cases, the fixation of the suture tape is achieved by a knotless suture anchor (PEEK [polyetheretherketone] SwiveLock; Arthrex Inc). 1,2,5,7 –10 In the current literature, knotless fixation with this particular anchor has been shown to have less variable tension compared with knotted constructs; however, the amount and consistency of the achieved tension after primary fixation remain unclear. 3 The purpose of the current study was to determine whether initial tensioning of suture tape before fixation with a knotless suture anchor significantly affects the final tension of the suture tape reinforcement in a biomechanical model. Our hypothesis was that the introduction of slight tension to the suture tape before suture anchor fixation would result in an increased final tension of the construct relative to zero tension or introduction of slack.
Methods
The effect of initial tensioning on the final tension of a knotless suture anchor fixation was tested with a Sawbones model (n = 5) and a porcine bone model (n = 8), per group. Testing was performed using both a synthetic host material (Sawbones model), enabling better comparability among the test groups, and a biological host material (porcine model), representing a more clinically relevant situation.
Sawbones Pretest Model
Initial testing was conducted using 15 pairs of 20 pound-force per cubic foot (pcf) Sawbones (Sawbones SE) blocks with a 3 mm–thick 40 pcf layer on the top and bottom to represent the tibia and femur, including cortices. The blocks were mounted to a tensile testing machine (E10000; Instron), along with a 1-kN load cell. The distance between the Sawbones block surfaces was set to 105 mm, as this constitutes the common total distance between the external apertures of the femoral and tibial tunnels traditionally used for ACL reconstruction. 6 Each block was clamped within the testing machine and aligned straight with the eventual load axis of the suture tape (Figure 1A). The suture tape (FiberTape 2mm; Arthrex Inc) was inserted into a titanium cortical button so that both suture strands had an equal length. Subsequently, the suture ends were threaded top-down through both blocks (Figure 1B). On the tibial side, the 2 ends of the suture tape were passed separately through 2 holes in a 14-mm round accessory button system (ABS) and then secured with the tested knotless suture anchor (PEEK SwiveLock C; 4.75 × 19.1 mm) in a predrilled and tapped hole 1 cm from the tibial exit point (Figure 1C).
Figure 1.
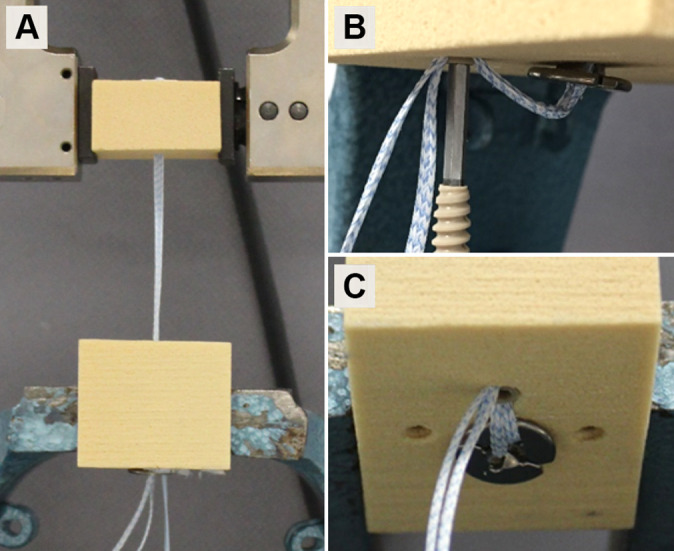
(A) Final Sawbones block testing setup. (B) Suture anchor insertion with introduced slack with prior mosquito forceps clamping. (C) Final suture anchor seating.
The free suture tape ends were pretensioned under the following conditions: (1) under slight tension with a preload of 5 N produced by a hanging weight, which was defined during pretests and represents a slight manually applied load; (2) under no tension, defined as having the suture anchor eyelet aligned with the anchor aperture with no initial preload; and (3) with initial slack introduced by having the suture tape go over a clamped mosquito forceps. Five pairs of blocks were tested for each experimental condition. The suture anchor was inserted until the anchor was flush with the cortical surface of the Sawbones as load-time data were recorded by the load cell at a sampling rate of 500 Hz, and initial and final tensions were recorded. A one-way analysis of variance was used to identify statistically significant differences. For differences that were significant, a Tukey post hoc test was carried out for pairwise analysis. An alpha of .05 was set as statistically significant.
Porcine Model
The second portion of this biomechanical study involved porcine tibias. For this purpose, 24 porcine knees were obtained from a local slaughterhouse. All soft tissue was carefully removed, and the tibia was embedded in a 2-component polyurethane system (RenCast; Huntsman Advanced Materials). The embedded porcine tibias were clamped to the same tensile testing machine (E10000) and load cells that were utilized in preliminary block testing. A tunnel was drilled through the tibia to simulate the tibial tunnel of an ACL reconstruction using a 4.0-mm drill bit (Figure 2A). A hole was drilled for suture anchor fixation 1 cm from the tibial exit using a drill bit–and-tap system specific to the suture anchor (SwiveLock drill bit and 4.75-mm tap) (Figure 2A). A custom-made acrylic block represented the fixed femural end. Similar to initial block testing, the suture tape (FiberTape, 2 mm) ends were passed through the cortical button so that both suture strands had an equal length and were fixed to the load cell located superior to the tibia. Subsequently, the suture ends were threaded top-down through the tibial tunnel and through an ABS button and secured with a SwiveLock C 4.75 × 19.1–mm anchor in the 3 different conditions. The total distance measured from the origin of the suture tape in the acrylic block superiorly to its exit out the tibial tunnel was set to 105 mm, as this constitutes the common total distance between the external apertures of the femoral and tibial tunnels 6 (Figure 2B).
Figure 2.
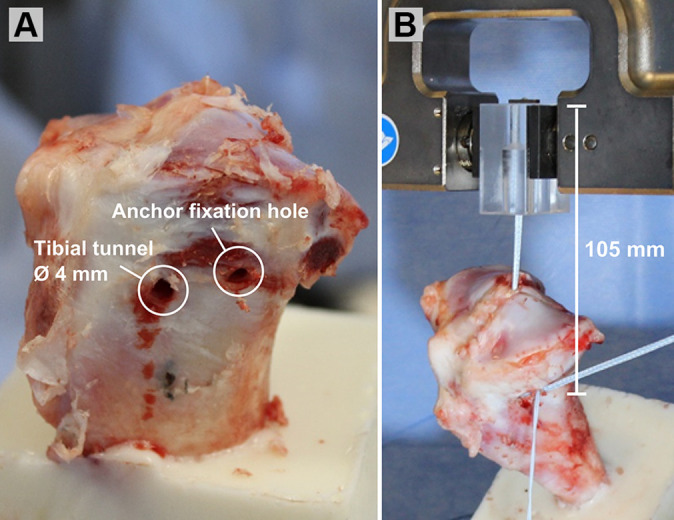
Porcine model experimental setup. (A) The tibial tunnel was drilled using a 4.0-mm drill bit, and a hole was drilled for suture anchor fixation using a drill bit and-tap system specific to the suture anchor. (B) Final experimental setup.
Each group was tested under 1 of the 3 same conditions used in the preliminary block testing: (1) under slight tension with a preload of 5 N, (2) under no tension, or (3) with initial slack (Figure 3, A-C). Eight specimens underwent testing for each condition. Load-cell data were recorded starting from the time of the pretensioning condition and were continuously collected during anchor insertion, anchor screw-in, and a ramp to a final force of 50 N, for which displacement of the model was also recorded. The initial load, final load, and displacement were statistically compared using a one-way analysis of variance. For differences that were significant, a Tukey post hoc test was carried out for pairwise analysis. An alpha of .05 was set as statistically significant.
Figure 3.

Illustration of the 3 pretensioning conditions utilized in the porcine model before suture anchor fixation. (A) Suture anchor insertion under slight tension using 5 N of preload during the entire process. (B) Suture anchor insertion with no initial tension on the suture—the suture is just slightly in contact with the bone at the aperture. (C) Suture anchor insertion with slack in the suture tape (constant slack ensured by use of the clamp).
Results
Sawbones Pretest Model
After each pretensioning condition, the initial load experienced by the suture tape was significantly greater for the slight-tension group (5.09 ± 0.44 N) when compared with the no-tension group (0.98 ± 0.56 N; P < .001) and slack group (1.17 ± 0.48 N; P < .001) after pairwise analysis (Table 1). No difference was found in initial loads between the no-tension and slack groups (P = .820). After suture anchor fixation, there was no difference in final loads experienced by the suture tape among the pretensioned conditions slight tension, no-tension, and slack groups (42.3 ± 5.3, 37.7 ± 6.4, and 40.2 ± 7.0 N, respectively; P = .528) (Figure 4).
Table 1.
Initial and Final Suture Tape Tension Values During Sawbones Block Testing (n = 5) a
| Pretension Condition | Initial Tension (N) | Final Tension (N) | ||
|---|---|---|---|---|
| Slight tension | 5.09 ± 0.44 b | 42.30 ± 5.30 | ||
| No tension | 0.98 ± 0.56 | P < .001 | 37.70 ± 6.40 | P = .528 |
| Slack | 1.17 ± 0.48 | 40.20 ± 7.00 | ||
a Data are expressed as mean ± SD.
b The slight-tension condition was significantly greater than both the no-tension (P < .001) and slack (P < .001) conditions on Tukey post hoc analysis for pairwise comparisons. There was no significant difference in initial tension between the no-tension and slack conditions (P = .820).
Figure 4.
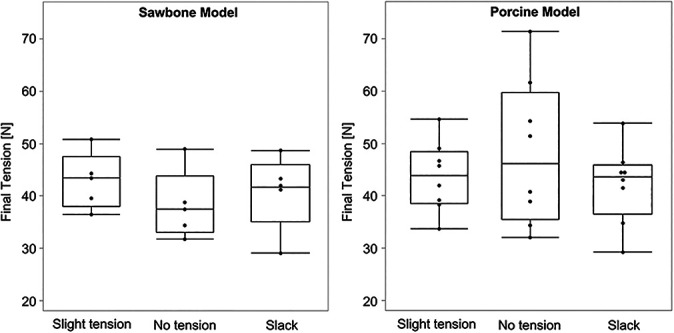
Box plots depicted the final tension for each pretensioning condition for the (left) Sawbones model and the (right) porcine model. Black points indicate raw data values. Values are presented as median (line), interquartile range (box), and minimum and maximum (whiskers).
Porcine Model
After each pretensioning condition, the initial load experienced by the suture tape was significantly greater for the slight-tension group (4.78 ± 0.72 N) when compared with the no-tension group (1.07 ± 0.84 N; P < .001) and slack group (0.61 ± 0.27 N; P < .001) after pairwise analysis (Table 2). No difference was found in initial load between the no-tension and slack groups (P = .359). After suture anchor fixation, there was no difference in final load experienced by the suture tape among the pretensioned conditions slight tension, no-tension, and slack groups (43.64 ± 6.69, 48.09 ± 13.93, and 44.52 ± 6.84 N, respectively; P = .633) (Figure 4). There was no significant difference in the displacement experienced during a force ramp to 50 N among the pretensioned groups slight tension, no-tension, and slack groups (0.08 ± 0.06, 0.06 ± 0.05, and 0.06 ± 0.05 mm, respectively; P = .694).
Table 2.
Initial and Final Suture Tape Tension and Displacement Values During Porcine Model Testing (n = 8) a
| Pretension Condition | Initial Tension (N) | Final Tension (N) | Displacement (mm) | |||
|---|---|---|---|---|---|---|
| Slight tension | 4.78 ± 0.72 b | 43.64 ± 6.69 | 0.08 ± 0.06 | |||
| No tension | 1.07 ± 0.84 | P < .001 | 48.09 ± 13.93 | P = .633 | 0.06 ± 0.05 | P = .694 |
| Slack | 0.61 ± 0.27 | 44.52 ± 6.84 | 0.06 ± 0.05 | |||
a Data are expressed as mean ± SD.
b The slight-tension condition was significantly greater than both the no-tension (P < .001) and slack (P < .001) conditions on Tukey post hoc analysis for pairwise comparisons. There was no significant difference in initial tension between the no-tension and slack conditions (P = .359).
Discussion
This biomechanical study shows that fixation of a suture tape with a knotless anchor resulted in a reproducible and consistent final tension, independent of the initial tension introduced with suture anchor placement.
There is significant interest in suture tape augmentation in the setting of soft tissue knee ligament surgery. Clinical studies have shown that suture tape augmentation in the setting of ACL repair increases the success rate of the repair. 14,17 Biomechanical studies have demonstrated that independent suture tape reinforcement of small-diameter ACL grafts reduces graft elongation and has a higher ultimate load to failure. 1 However, excessive pretensioning of the suture tape augmentation should be avoided to prevent stress shielding and late fatigue failure of the graft. 4
The knee flexion angle at the time of fixation for the tape, if used as an internal brace for ACL reconstruction, may play an important role in preventing excessive tension on the joint during range of motion. The length of the ACL has been shown to be at its maximum at a knee flexion angle of 0°. 11 If the suture tape is fixed at a decreased ACL ligament length, for example at 30° of knee flexion, the tension of the suture tape will increase when the knee is extended to 0°, which could put too much constraint on the joint. One option to potentially prevent this complication would be a second-look arthroscopy to cut the suture tape reinforcement at a specified time point. 14 Alternatively, the suture tape may be placed with some slack such that it acts more as a “safety belt”, allowing the graft to experience a physiologic amount of load. 1 Similarly, in rotator cuff surgery, where a linked double-row repair construct with similar fixation is commonly used, the results from this study would seem to indicate that there is no need to excessively pretension the suture tape when inserting the lateral row knotless anchors.
The purpose of this biomechanical study was to investigate whether the amount of suture tape pretensioning had a significant effect on the final tension of the construct. Contrary to our initial hypothesis, the current study demonstrated no significant difference in final tension of the suture tape reinforcement, regardless of the pretensioning scenario in the Sawbones and porcine models. A final tension in the range of 40 to 50 N was reached in all 3 groups, suggesting that the final tension of the suture tape construct was created by the friction drag of the suture anchor eyelet while it was inserted into the predrilled hole. In other words, the suture anchor appeared to provide a self-tensioning feature as it secured the suture tape independent of the initial pretension, leading to reproducible and consistent knotless fixation. The initial tension on the suture tape was therefore only dependent on the surgeon’s preference.
Limitations
Weaknesses of the current study include the nonclinical, time-zero nature of the data. In addition, Sawbones blocks and porcine knees were used instead of cadaveric specimens. However, we believe that this model better allowed us to isolate the tension of the suture and minimize other confounding variables. Although the study of the properties of a specific anchor and suture construct may limit the generalizability of this result to other forms of fixation, we believe this is a strength, as the majority of the published literature has reported using the studied suture anchor for fixation of knotless suture tape augmentation constructs. 1,2,5,7 –10
Conclusion
The final tension of the suture tape construct appears to be reproducible and consistent, independent of the initial tension introduced with suture anchor placement within the tested parameters.
Footnotes
Final revision submitted September 11, 2020; accepted November 11, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.A. has received speaking fees from Arthrex and hospitality payments from Stryker. P.A.S. has received educational support from Elite Orthopedics, consulting fees from Arthrex, nonconsulting fees from Alpha Orthopedic Systems and Arthrex, and royalties from Arthrex. M.P., A.P.M., and C.A.W. are employees of Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.
References
- 1. Bachmaier S, Smith PA, Bley J, Wijdicks CA. Independent suture tape reinforcement of small and standard diameter grafts for anterior cruciate ligament reconstruction: a biomechanical full construct model. Arthroscopy. 2018;34(2):490–499. [DOI] [PubMed] [Google Scholar]
- 2. Daggett M, Redler A, Witte K. Anterior cruciate ligament reconstruction with suture tape augmentation. Arthrosc Tech. 2018;7(4):e385–e389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Denard PJ, Adams CR, Fischer NC, Piepenbrink M, Wijdicks CA. Knotless fixation is stronger and less variable than knotted constructs in securing a suture loop. Orthop J Sports Med. 2018;6(5):2325967118774000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Gagliardi AG, Carry PM, Parikh HB, et al. ACL repair with suture ligament augmentation is associated with a high failure rate among adolescent patients. Am J Sports Med. 2019;47(3):560–566. [DOI] [PubMed] [Google Scholar]
- 5. Golden T, Friedman AMB, Jazayeri R, Sanderson B, Levy E. Primary repair of the medial collateral ligament with a double row suture technique and suture tape augmentation for acute tibial-sided injuries. Arthrosc Tech. 2019;8(4):e395–e398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Gomoll AH, Bach BR. Managing tunnel malposition and widening in revision anterior cruciate ligament surgery. Oper Tech Sports Med. 2006;14(1):36–44. [Google Scholar]
- 7. Heusdens CHW, Hopper GP, Dossche L, Roelant E, Mackay GM. Anterior cruciate ligament repair with independent suture tape reinforcement: a case series with 2-year follow-up. Knee Surg Sports Traumatol Arthrosc. 2019;27(1):60–67. [DOI] [PubMed] [Google Scholar]
- 8. Hopper GP, Heusdens CHW, Dossche L, Mackay GM. Medial patellofemoral ligament repair with suture tape augmentation. Arthrosc Tech. 2019;8(1):e1–e5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Hopper GP, Heusdens CHW, Dossche L, Mackay GM. Posterior cruciate ligament repair with suture tape augmentation. Arthrosc Tech. 2019;8(1):e7–e10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Hopper GP, Heusdens CHW, Dossche L, Mackay GM. Posterolateral corner repair with suture tape augmentation. Arthrosc Tech. 2018;7(12):e1299–e1303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Kim YK, Yoo JD, Kim SW, et al. Intraoperative graft isometry in anatomic single-bundle anterior cruciate ligament reconstruction. Knee Surg Relat Res. 2018;30(2):115–120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Mackay GM, Blyth MJ, Anthony I, Hopper GP, Ribbans WJ. A review of ligament augmentation with the InternalBrace™: the surgical principle is described for the lateral ankle ligament and ACL repair in particular, and a comprehensive review of other surgical applications and techniques is presented. Surg Technol Int. 2015;26:239–255. [PubMed] [Google Scholar]
- 13. Mall NA, Chalmers PN, Moric M, et al. Incidence and trends of anterior cruciate ligament reconstruction in the United States. Am J Sports Med. 2014;42(10):2363–2370. [DOI] [PubMed] [Google Scholar]
- 14. Smith JO, Yasen SK, Palmer HC, et al. Paediatric ACL repair reinforced with temporary internal bracing. Knee Surg Sports Traumatol Arthrosc. 2016;24(6):1845–1851. [DOI] [PubMed] [Google Scholar]
- 15. Smith PA, Bley JA. Allograft anterior cruciate ligament reconstruction utilizing internal brace augmentation. Arthrosc Tech. 2016;5(5):e1143–e1147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Spindler KP, Wright RW. Clinical practice. Anterior cruciate ligament tear. N Engl J Med. 2008;359(20):2135–2142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. van Eck CF, Limpisvasti O, ElAttrache NS. Is there a role for internal bracing and repair of the anterior cruciate ligament? A systematic literature review. Am J Sports Med. 2018;46(9):2291–2298. [DOI] [PubMed] [Google Scholar]
- 18. Webster KE, Feller JA, Leigh WB, Richmond AK. Younger patients are at increased risk for graft rupture and contralateral injury after anterior cruciate ligament reconstruction. Am J Sports Med. 2014;42(3):641–647. [DOI] [PubMed] [Google Scholar]