

Abstract
The COVID‐19 outbreak strongly restricted daily activities, creating a risk factor for negative affect and depression. This study assessed the immediate effects of a behavioural activation (BA) intervention on positive (PA) and negative (NA) state affect. We expected depression and anxiety to function as moderators reducing the intervention effects. In a quasi‐experimental online study, 3624 German‐speaking participants evaluated a list of rewarding activities between 9 April and 26 April 2020. A subsample of 2561 (71%) additionally engaged in an imagination task. Depression, anxiety, socioeconomic variables and COVID‐19 related burdens were assessed as moderators. There was an increase in PA (total sample d = .13; subsample: d = .27) and a decrease in NA (total sample d = −0.68; subsample: d = −0.71; all p < .001). The effects rose with higher levels of depression and anxiety (all p < .001). Furthermore, living with family enhanced the effects on NA, while additionally having to take care of children reduced them. An easy‐to‐use intervention prompting BA could improve state mood during lockdown. Participants with higher depression and anxiety benefit more. Implications for the prevention of mental health problems during a pandemic are discussed.
Keywords: Behavioural activation, COVID‐19, Imagination, Mental health, Negative affect, Prevention
The coronavirus disease 2019 (COVID‐19) pandemic has direct and indirect health, social and economic effects, which are predicted to also negatively impact mental health. As a central characteristic of the crisis, regulations intending to minimise social contacts, thus, the risk of infection, more or less restrict the range of daily activities. From a psychological perspective, this represents a tremendous risk for the individual to lose opportunities for positive reward. The regulations during the COVID‐19 lockdown imply, in other words, a lack of reinforcement as they restrict the range of possible activities dramatically.
A drop in positive reward is one of the most important anteceding and maintaining factors for depression according to Lewinsohn's influential social reinforcement theory (Lewinsohn, 1974). In brief, social reinforcement theory assumes that individuals react with a reduction of their rewarding activities when experiencing depressed mood after initial negative events (such as job loss, divorce, loss of a loved one, etc.). This reduction is, at least temporarily, reinforced by the social environment, which leads to further extinction of instrumental behaviour and excesses of avoidant coping. A behaviour pattern of reduced activities, reduced reinforcement rates and continued depressed mood can then take on the form of a vicious cycle. A treatment approach that directly builds upon the theoretical rationale of social reinforcement theory is behavioural activation (BA).
Although several variants exist, the main focus of BA is on activity monitoring and activity planning, which both aim at counteracting depressogenic factors by provoking more rewarding activities. It is important to note that more recent versions of this method broadened the focus of the activity planning component as they do not only include “pleasant” activities but also those being meaningful in terms of personal values (Hoyer, Čolić, et al., 2020; Hoyer, Hoefler, & Wuellhorst, 2020). The National Institute for Health and Care Excellence designated the method as an empirically validated treatment, which is easy to administer and efficacious for many diverse patient populations and age groups in individual and in group treatment formats (Ekers et al., 2014). Due to its parsimonious and straightforward rationale, BA is considered highly suitable for large‐scale dissemination.
Astonishingly, only little attention has been paid to the preventive potential of BA. In the coronavirus lockdown situation, we consider the BA approach to be ideal for developing a minimal intervention that could counteract the potentially depressogenic and anxiety‐provoking effects of the lockdown. As the effects of BA as a tool for psychological prevention are not yet well‐documented, we planned the present study as a proof‐of‐concept project to demonstrate and analyse the preventive benefits of a short BA intervention on mental well‐being, namely positive and negative state mood.
While the lockdown situation restricted direct social contacts, people spent much more time than usual on the Internet. Applying mental health interventions through the Internet (E‐Mental‐Health) makes it possible to reach very many people who are affected and/or in need of health in a short period of time. The Internet seems thus generally highly suitable for psychological prevention efforts. On the other hand, using the Internet can be associated with informational overflow. Users often only dwell shortly on a specific content and there is intense competition between diverse providers and formats. Hence, we intended to develop an extremely brief intervention, focusing only on the activity planning component of BA.
This was guided by the idea that despite the restrictions during the lockdown, many possible rewarding activities remain. We planned to present a list of potentially rewarding activities via the Internet, giving respondents the chance to choose from this list and to broaden the range of positive and/or meaningful activities that could enhance reinforcement rates even during a typical lockdown day. As a template for a list of positive activities, we referred to the Positive Events Schedule (PES; MacPhillamy & Lewinsohn, 1982). This list, developed in the 1970s, is very long (containing 320 items) and had to be carefully revised and shortened (to no more than 99 items, see the following text). In addition, we intended to enhance the rate of meaningful activities within that list to reflect the recent development in the theoretical rationale of BA.
As it was unclear whether simply dwelling upon and making selections among a list of positive and/or meaningful activities would provoke actual efforts in action planning (and changes in mood, accordingly), we decided to also include a brief imagination exercise to prompt a clearer idea of the planned action. A recent study suggests that simulating mental images, which include potentially rewarding activities and their emotional consequences, could act as a motivational enhancer. This could result in increased behavioural engagement (Renner et al., 2016, 2019). In sum, our intervention included (a) the selection of positive and/or meaningful activities that can be performed even during an acute lockdown scenario and (b) imagining at least one of those activities intensely.
We expected that this combined intervention would lead to improved state mood (more positive and less negative affect; Hypothesis 1) and could, thus, prove to be an easily accessible, effective tool for emotion regulation during lockdown periods. Furthermore, we expected that those suffering from more depression and anxiety symptoms would have more problems adapting to the short intervention (Hypothesis 2). This was grounded on the assumption that the symptoms of depression and anxiety would interfere with an adequate adoption of our task: Depression is characterised inter alia by sadness, a loss of interest, concentration problems and so on. Anxiety is correlated with depression and both are correlated with inhibition. Against this backdrop, we argued that depression and anxiety function as moderating variables that reduce the intervention's effect.
METHODS
Study design and sample
The web‐based study was cross‐sectional and had a quasi‐experimental design (Kazdin, 2013). There was no randomised group assignment. The groups were formed according to the information on whether the participants carried out the partial interventions. It was conducted with SoSci Survey (Leiner, 2019). Recruitment and data collection occurred between 9 April 2020 and 26 April 2020. The participants were recruited through social media, online and newspaper articles. All individuals had to be at least 16 years old and had to have sufficient knowledge of the German language to participate in the study. To encourage the recruitment, all participants had the opportunity to download the list with 99 rewarding activities at the end of the survey. The participation was anonymous, voluntary and non‐commercial. All participants gave their consent on the first survey page, and the study was conducted in accordance with the declaration of Helsinki. Based on the fact that data were completely anonymous and the IP addresses of the respondents were not stored, the ethics committee of the Dresden University of Technology deemed further formal evaluation of the study not necessary.
A total of 3625 German‐speaking subjects participated. One participant was excluded subsequently because of unserious answers. The final sample consisted of 3624 participants. A subsample of 2561 (71%) engaged in an imagined BA exercise (IBA, see the following text). Table 1 shows the sociodemographic and clinical characteristics of the sample.
TABLE 1.
Sociodemographic and clinical characteristics of the samples and group differences
| Descriptions | ||||
|---|---|---|---|---|
| Total | ALO a | AL + IBA b | Group differences c | |
| Characteristics | (N = 3624) | (n = 1063) | (n = 2561) | p |
| Age, M (SD) | 36.84 (11.74) | 36.70 (11.06) | 36.89 (12.01) | .716 |
| Sex, % | ||||
| Female | 83.3 | 83.0 | 83.4 | .951 |
| Male | 16.3 | 16.6 | 16.2 | |
| Diverse | 0.4 | 0.5 | 0.4 | |
| Years of education, % | ||||
| <8 | 0.4 | 0.4 | 0.4 | .015 |
| 8–10 | 18.4 | 19.9 | 17.7 | |
| 11–13 | 29.4 | 40.0 | 28.8 | |
| 14+ | 51.8 | 48.7 | 53.2 | |
| Employment status, % | ||||
| Still in school/university | 18.2 | 15.3 | 19.3 | .002 |
| Full‐time employed | 39.3 | 42.4 | 38.0 | |
| Part‐time employed | 21.2 | 22.3 | 20.7 | |
| Unemployed | 2.9 | 2.6 | 3.0 | |
| Retired | 2.9 | 1.9 | 3.4 | |
| On parental leave/other exemptions | 7.1 | 7.4 | 6.9 | |
| Other | 8.5 | 8.1 | 8.6 | |
| Living arrangements, % | ||||
| Living alone | 19.8 | 15.9 | 21.5 | <.001 |
| Shared apartment | 8.7 | 7.1 | 9.4 | |
| Living with spouse | 29.7 | 30.7 | 29.3 | |
| Living with family | 41.7 | 46.4 | 39.8 | |
| Number of children, % | ||||
| 0 | 60.3 | 55.1 | 62.7 | .113 |
| 1 | 16.8 | 18.1 | 16.4 | |
| 2 | 17.0 | 20.7 | 15.7 | |
| 3+ | 5.2 | 6.0 | 4.7 | |
| More time at home in %, M (SD) | 58.26 (29.13) | 56.93 (29.85) | 58.82 (28.81) | .077 |
| Change of work situation, % | ||||
| Loss of employment | 4.4 | 4.0 | 4.5 | .107 |
| Reduced working hours | 9.4 | 9.8 | 9.3 | |
| Increased working hours | 5.0 | 5.7 | 4.8 | |
| Change to home‐office | 48.5 | 45.4 | 49.7 | |
| No change at all | 32.7 | 35.1 | 31.7 | |
| Double burden (work and childcare), % | 21.9 | 26.1 | 20.2 | <.001 |
| Risk of severe course of COVID‐19, % | 20.0 | 20.4 | 19.8 | .692 |
| Personally infected by COVID‐19, % | 0.4 | 0.4 | 0.4 | .909 |
| Flat mate infected by COVID‐19, % | 0.3 | 0.1 | 0.4 | .179 |
| PANAS pre, M (SD) | ||||
| PA | 2.61 (0.69) | 2.58 (0.66) | 2.62 (0.69) | .131 |
| NA | 1.89 (0.67) | 1.91 (0.68) | 1.89 (0.66) | .402 |
| Activity list | ||||
| Came up with new ideas, yes % | 51.7 | 40.5 | 56.3 | <.001 |
| Motivation, M (SD) | 7.66 (2.04) | 7.16 (2.06) | 7.87 (1.98) | <.001 |
| PHQ‐9, M (SD) | 7.58 (5.31) | 7.32 (5.36) | 7.68 (5.28) | .061 |
| GAD‐7, M (SD) | 6.26 (4.79) | 6.21 (4.91) | 6.28 (4.74) | .649 |
| IBA | ||||
| Listened to audio, % | 70.7 | 0.00 | 100 | – |
| Female voice, % | 54.8 | – | 77.3 | – |
| Quality of implementation, M (SD) | 7.72 (2.58) | – | 7.73 (2.57) | – |
| Increase of implementation, yes % | – | 63.7 | – | |
| PANAS post, M (SD) | ||||
| PA | 2.69 (0.84) | 2.41 (0.79) | 2.80 (0.82) | <.001 |
| NA | 1.44 (0.61) | 1.51 (0.68) | 1.41 (0.57) | <.001 |
Notes: Significant results are bold. AL = Activity list; COVID‐19 = Corona virus disease 2019; GAD‐7 = Generalised Anxiety Disorder‐7; IBA = Imaginary behavioural activation; NA = Negative affect; PA = Positive affect; PANAS = Positive and Negative Affect Schedule; PHQ‐9 = Patient Health Questionnaire‐9.
Participants finished only the activity list.
Participants finished the activity list and additionally the IBA.
Between‐group differences of categorical variables were calculated with the chi‐square test. For differences between continuous variables, a t‐test was used.
Measures
Participants completed questions about demographics, COVID‐19 related burdens, affect, depression and anxiety. Table S1 (in Appendix S1) shows the full variable list. The German versions of the instruments were used.
Positive and negative affect
We measured the subjects' state affect with the Positive and Negative Affect Schedule (PANAS; Watson et al., 1988; German version: Krohne et al., 1996). It consists of two 10‐item‐scales to measure positive affect (PA; e.g. active, enthusiastic) and negative affect (NA; e.g. afraid, distressed). Participants were asked how they felt in the exact moment using a Likert scale ranging from 1 (not at all) to 5 (very much). A total score for PA and NA (mean across all PA items and all NA items) can be derived. The German version of the PANAS showed high reliability (Cronbach's α = .86 to .93) for positive and negative affect (Breyer & Bluemke, 2016). Positive and negative affect (PANAS) were assessed before and after completing a list of rewarding activities and engaging in the IBA.
Depression
Symptoms of depression were measured with the Patient Health Questionnaire‐9 (PHQ‐9; Kroenke et al., 2001; German version: Löwe et al., 2002). It is based on the Diagnostic and Statistical Manual of Mental Disorders (DSM‐IV; APA, 1994) and consists of nine items depicting diagnostic criteria of depression over the past 2 weeks (e.g. a loss of interest, feelings of depression or hopelessness). The participants could indicate their answers on a 4‐point Likert scale ranging from 0 (= not at all) to 3 (= nearly every day). The total score ranges from 0 to 27, with higher scores indicating more severity of depressive symptoms (Kroenke et al., 2001). The German version of the PHQ‐9 showed high reliability (Cronbach's α = .88; Gräfe et al., 2004).
Anxiety
Symptoms of anxiety were measured with the Generalised Anxiety Disorder‐7 (GAD‐7; Spitzer et al., 2006; German version: Löwe et al., 2002). It is based on the DSM‐IV (APA, 1994) and consists of seven items depicting diagnostic criteria of generalised anxiety disorder over the past 2 weeks (e.g. feelings of anxiety or nervousness, worrying about different things). The participants could indicate their answers on a 4‐point Likert scale ranging from 0 (not at all) to 3 (nearly every day). The score ranges from 0 to 21 with higher scores indicating a more severe course of anxiety symptoms (Löwe et al., 2008). The German version of the GAD‐7 showed high reliability (Cronbach's α = .89; Löwe et al., 2008). The PHQ‐9 and the GAD‐7 are two modules of the Patient Health Questionnaire.
Activity list
The PES (MacPhillamy & Lewinsohn, 1982) with 320 positive activities was modified by Hoyer and Krämer (2021) to 301 items. Since many activities were not viable due to the COVID‐19 related restrictions in everyday life, four independent raters indicated on a scale from 0 to 2 how suitable each activity from the list was (0 = unsuitable, 1 = only suitable to a limited extent, 2 = suitable). One‐hundred thirty‐seven items reached the criterion of a sum score of seven points (across all four raters). We sorted out 21 items because of unspecific, unsuitable or too specific content (e.g. “having leisure time,” “using virtual reality glasses”). Because of doublings and similarities, we combined 45 items to 11 items (e.g. “listening to an audiobook” and “listening to a podcast” combined to “listening to an audiobook or podcast”). We also modified 35 existing items (e.g. “going shopping” to “online shopping”) to suit the COVID‐19 related restrictions. We discussed 23 additional self‐provided COVID‐19 suitable items and included 17 of them (e.g. “streaming an online lecture,” “watching a movie in a foreign language”). In the end, the list was shortened and supplemented to 99 implementable activities. For the complete list, see the electronic supplemental material (Table S2).
IBA
Participants had the possibility to additionally engage in an imaginary behavioural activation task. To encourage their participation, we highlighted that participating in the mental imagery task could increase the motivation and likelihood of carrying out an activity (Renner et al., 2019). For the auditory imaginary behavioural activation exercise, the participants were instructed to select one activity from the list and imagine themselves in detail in the scenario using a self‐provided audio file. They could choose between a female and a male voice with a time span of 2:40 minutes versus 3:10 minutes for the audio instruction. This procedure was based on the study of Renner and colleagues (Renner et al., 2016).
Statistical analysis
The statistical analyses were conducted using Stata Statistical Software Version 15 (StataCorp, 2017). Group differences in the baseline characteristics were calculated using t tests and chi‐square tests. Changes between pre and post were calculated using linear regression analysis with time as the predictor and the PA and NA total scores as outcomes. Time was dummy coded and modelled as discrete (0 = pre, 1 = post). This approach is equivalent to a paired samples t test (Field, 2017). The p‐value was set to .05 and two‐sided testing was conducted, while listwise deletion was applied. The effect sizes (ES) were derived as differences in means divided by the standard deviation at pre. In accordance with Cohen (1988), ES above 0.2 were interpreted as small, ES above 0.5 as medium and ES above 0.8 as large. Based on Hayes's recommendations (Hayes, 2013), the moderation analyses consisted of separate linear regression analyses (i.e. simple moderation analyses). In each analysis, the unstandardised moderator was included as an interaction term with the time‐variable (Hayes, 2013). When NA and PA are outcomes, this approach takes associations with pre‐scores and the moderator into account (Rabe‐Hesketh & Skrondal, 2012). This procedure was also carried out for participants that engaged in the IBA. Because of multiple tests, we applied the Holm‐Bonferroni correction for the significance level (Holm, 1979).
RESULTS
Descriptive statistics
The sample is composed of much more women than men and of more young than old participants. Furthermore, there is an over‐proportionate rate of highly educated participants. There were slight differences between the “Activity list only” group (ALO) and the group completing the activity list and the imagination exercise (AL + IBA) in years of education, employment status and living arrangements. Also, participants partaking in the IBA exercise were more motivated and came up with more new ideas for activities. In addition, significantly less people with a double burden of work and childcare completed the imagination exercise (see Table 1).
The scoring on the PHQ‐9 and the GAD‐7 (see Table 1) indicates slightly higher means than seen in normative samples. With reference to common cut‐off scores published for the PHQ‐9 (Manea et al., 2012), 36% of the sample can be characterised to be at least mildly impaired by depressive symptoms if the lowest cut‐off of 8 is chosen, and 21% of the sample if the highest cut‐off of 11 is chosen. Regarding standard cut‐off scores published for the GAD‐7 (Plummer et al., 2016), 33% of the sample can be characterised to be at least mildly impaired by anxiety symptoms if the lowest cut‐off of 7 is chosen, and 18% of the sample if the highest cut‐off of 10 is chosen.
Activity list
On average, M = 26.63 (SD = 14.87) activities were chosen as relevant by the participants. The number of activities correlated negatively with age (r = −.22, p < .001). Its correlations with depression (r = −.10, p < .001) and anxiety (r = −.10, p < .001) were low and not of practical significance.
All activities on the list were selected at least once. The five activities that were selected most often were: watching a movie/a TV series (70%); doing chores (67%); going for a walk (67%); cleaning the apartment thoroughly (65%); chatting with friends and family in‐person or over phone/Skype (65%); while the five activities selected least often were: writing/reciting a poem (1%); conducting a fashion show at home (2%); confess something to somebody (2%); participating in internet‐corona‐challenges, e.g. #oldphotochallenge (3%); and learning a magic trick (3%). The complete list and the relative frequencies for each activity can be inspected in the electronic supplemental material (Table S2).
Changes in positive and negative affect
We did a complete‐case analysis, i.e. for affect changes we analysed data only in individuals who answered all PA or NA items.
Activity list only
When considering all participants, there was an increase in positive affect, M pre = 2.61 (SD = 0.69), M post = 2.69 (SD = 0.84), t (3517) = 4.74, p < .001, d = 0.13; and a decrease in negative affect, M pre = 1.89 (SD = 0.68), M post = 1.44 (SD = 0.61), t (3514) = −30.31, p < .001, d = −0.68.
Activity list + IBA
When considering only participants that engaged in both the activity list and the IBA, there was a slightly larger increase in positive affect, M pre = 2.62 (SD = 0.70), M post = 2.80 (SD = 0.82), t (2544) = 8.59, p < .001, d = 0.27, as well as a minimally larger decrease in negative affect, M pre = 1.89 (SD = 0.65), M post = 1.41 (SD = 0.57), t (2544) = −27.71, p < .001, d = −0.71.
When comparing the two groups (activity list vs. activity list + IBA), there was a main effect of time for both PA (d = 0.25, p < .001) and NA (d = −0.59, p < .001), while there was no main effect of group: for PA (d = 0.05, p = .153); for NA (d = −0.03, p = .400). There was an interaction effect for both PA (d = 0.51, p < .001) and NA (d = −0.12, p = .018), that is, partaking in the IBA, in addition to the completion of the activity list alone, significantly increased PA and reduced NA (see Figure 1).
Figure 1.
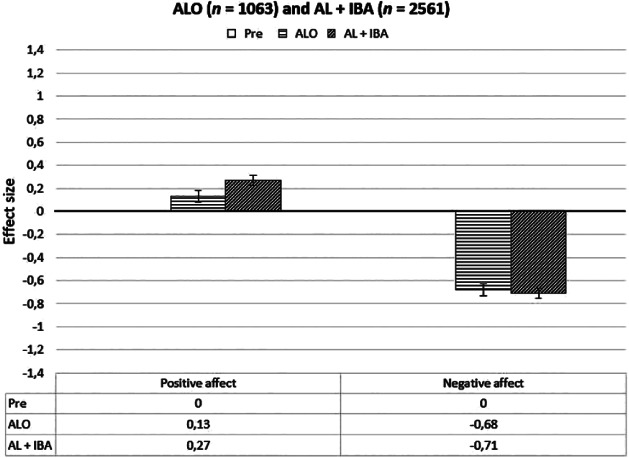
Effect sizes of positive and negative affect.Note: ALO = Activity list only; AL + IBA = Activity list and imagined behavioural activation.
Moderators of change
Depression and anxiety showed significant interaction effects with time (pre and post) for both PA and NA in the complete sample and the subsample, indicating a higher increase in PA and a higher decrease in NA with the rise in depression and anxiety (see Tables 2 & 3).
TABLE 2.
Moderators of effect size change in positive affect from pre to post in the complete sample and in the subsample
| Interaction effects with time (pre‐post) | |||||||
|---|---|---|---|---|---|---|---|
| Complete sample | Subsample | ||||||
| Moderators, reference categories | β | p | 95% CI | β | p | 95% CI | |
| PHQ‐9 a | 0.02 | <.001 | [0.01, 0.03] | 0.02 | =.001 | [0.01, 0.03] | |
| GAD‐7 a | 0.01 | =.009 | [0.00, 0.02] | 0.02 | =.009 | [0.00, 0.03] | |
| Age a | −0.00 | =.197 | [−0.00, 0.00] | −0.00 | =.520 | [−0.01, 0.00] | |
| Sex, Female b | Male | −0.07 | =.333 | [−0.21, 0.07] | −0.10 | =.226 | [−0.27, 0.06] |
| Diverse | −0.16 | =.678 | [−0.91, 0.59] | −0.19 | =.686 | [−1.12, 0.74] | |
| Living arrangements, Alone b | With non‐family members | 0.12 | =.281 | [−0.09, 0.32] | 0.12 | =.339 | [−0.12, 0.35] |
| With spouse | −0.01 | =.869 | [−0.16, 0.13] | 0.03 | =.775 | [−0.15, 0.20] | |
| With family | −0.06 | =.426 | [−0.20, 0.08] | −0.02 | =.784 | [−0.19, 0.14] | |
| Work situation, Loss of employment b | Reduced working hours | −0.09 | =.545 | [−0.39, 0.21] | −0.12 | =.493 | [−0.47, 0.23] |
| Increased working hours | −0.12 | =.474 | [−0.46, 0.21] | −0.18 | =.357 | [−0.59, 0.21] | |
| Change to home‐office | −0.03 | =.797 | [−0.29, 0.22] | −0.08 | =.603 | [−0.38, 0.22] | |
| No change at all | −0.11 | =.406 | [−0.37, 0.15] | −0.16 | =.297 | [−0.47, 0.14] | |
| Double burden (work and childcare), yes b | No | 0.04 | =.540 | [−0.09, 0.16] | 0.01 | =.835 | [−0.14, 0.17] |
| Risk of severe course of COVID‐19, yes b | No | 0.07 | =.320 | [−0.06, 0.19] | 0.06 | =.420 | [−0.09, 0.21] |
| Personally infected by COVID‐19, yes b | No | −0.18 | =.684 | [−1.04, 0.68] | −0.51 | =.329 | [−1.54, 0.52] |
| Flat mate infected by COVID‐19, yes b | No | −0.28 | =.569 | [−1.26, 0.69] | −0.17 | =.745 | [−1.20, 0.86] |
Note: Significant results are bold. COVID‐19 = Coronavirus disease 2019; GAD‐7 = Generalised Anxiety Disorder‐7; PHQ‐9 = Patient Health Questionnaire‐9.
Continuous moderators.
Reference category for categorical moderators.
TABLE 3.
Moderators of effect size change in negative affect from pre to post in the complete sample and in the subsample
| Interaction effects with time (pre‐post) | |||||||
|---|---|---|---|---|---|---|---|
| Complete sample | Subsample | ||||||
| Moderators, reference categories | β | p | 95% CI | β | p | 95% CI | |
| PHQ‐9 a | −0.03 | <.001 | [−0.03, −0.02] | −0.04 | < .001 | [−0.04, −0.03] | |
| GAD‐7 a | −0.04 | <.001 | [−0.04, −0.03] | −0.05 | < .001 | [−0.06, −0.04] | |
| Age a | 0.00 | =.414 | [−0.00, 0.01] | 0.00 | =.448 | [−0.00, 0.00] | |
| Sex, Female b | Male | 0.17 | =.006 | [0.05, 0.29] | 0.15 | =.032 | [0.01, 0.29] |
| Diverse | 0.43 | =.193 | [−0.22, 1.07] | 0.24 | =.545 | [−0.53, 1.01] | |
| Living arrangements, Alone b | With non‐family members | −0.02 | =.805 | [−0.20, 0.16] | −0.02 | =.813 | [−0.22, 0.17] |
| With spouse | −0.03 | =.683 | [−0.15, 0.10] | −0.03 | =.701 | [−0.17, 0.11] | |
| With family | −0.12 | = .042 | [−0.24, −0.01] | −0.13 | = .051 | [−0.27, 0.00] | |
| Work situation, Loss of employment b | Reduced working hours | −0.03 | =.806 | [−0.29, 0.22] | −0.06 | =.684 | [−0.35, 0.23] |
| Increased working hours | 0.12 | =.393 | [−0.16, 0.41] | 0.15 | =.363 | [−0.18, 0.48] | |
| Change to home‐office | 0.05 | =.661 | [−0.17, 0.27] | 0.06 | =.657 | [−0.19, 0.30] | |
| No change at all | 0.06 | =.628 | [−0.17, 0.28] | 0.05 | =.696 | [−0.20, 0.30] | |
| Double burden (work and childcare), yes b | No | 0.11 | =.037 | [0.01, 0.22] | 0.15 | =.019 | [0.02, 0.28] |
| Risk of severe course of COVID‐19, yes b | No | −0.01 | =.815 | [−0.12, 0.10] | 0.02 | =.719 | [−0.10, 0.15] |
| Personally infected by COVID‐19, yes b | No | 0.40 | =.287 | [−0.34, 1.13] | 0.37 | =.402 | [−0.49, 1.22] |
| Flat mate infected by COVID‐19, yes b | No | 0.35 | =.415 | [−0.49, 1.18] | 0.26 | =.544 | [−0.59, 1.12] |
Note: Significant results are bold. COVID‐19 = Coronavirus disease 2019; GAD‐7 = Generalised Anxiety Disorder‐7; PHQ‐9 = Patient Health Questionnaire‐9.
Continuous moderators.
Reference category for categorical moderators.
Changes in positive and negative affect were also calculated for participants above the cut‐offs for PHQ‐9 and GAD‐7. As Figure 2 shows, participants with clinically relevant anxiety and depression symptoms benefitted most, reaching the largest effect size for their mood change after the intervention.
Figure 2.
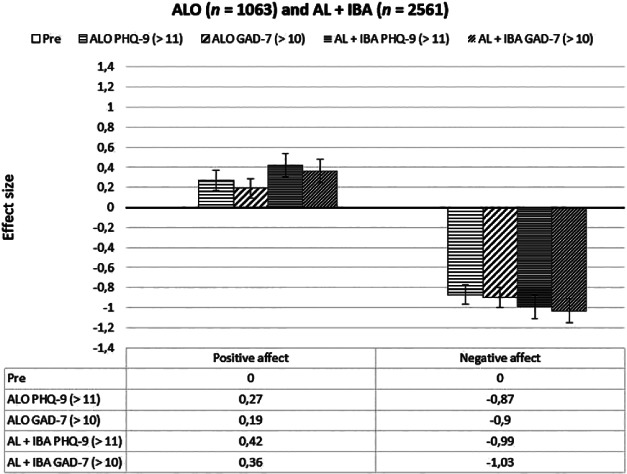
Effect sizes of positive and negative affect in subgroups above the highest cut‐offs for PHQ‐9 (>11) and GAD‐7 (>10).Note: ALO = Activity list only; AL + IBA = Acvtivity list + imagined behavioural activation.
Some of the other variables were significant moderators only for NA, but not for PA. Regarding NA, sex proved to be significant, indicating a lower decrease in males compared to females in both the complete sample and the subsample; living arrangements, indicating a greater decrease in individuals living with family members in the complete sample; and having to take care of children and having to work at the same time (double burden) lowered the decrease in NA significantly in the complete sample, as well as the subsample. Detailed statistics are shown in Tables 2 (PA) and 3 (NA).
DISCUSSION
Our first hypothesis that selecting and imagining rewarding activities would lead to improved state mood was clearly supported for both positive and negative affect. Importantly, the effect was much higher for negative affect, the aspect of mood which might be more critical in terms of the prevention of mental health problems (Mayne, 1999). When comparing the subsamples of those having partaken in the imagination exercise and those who had not, it was found that the improvement in PA was larger in those who also underwent the imagination exercise. It is of note that this cannot be attributed to a causal effect of the imagination exercise as there was no randomisation. Nevertheless, the finding demonstrates that a brief imagination has the potential to lift state mood even on the population scale when it is delivered online. Summarised, there are (good) indications, that a very brief intervention, performed as the selection of rewarding (pleasant or meaningful) activities with or without a subsequent imagination task, can contribute to reducing state mood problems. Furthermore, our results support previous findings that the simple act of engaging in an activity is directly associated with (rather than followed by) a reduction of negative mood (or depressed feelings; Hoyer, Hoefler, & Wuellhorst, 2020).
In our second hypothesis, we had predicted that depression and anxiety function as moderating variables that reduce the effect of the intervention as their symptoms may corrupt the adequate performance of the intervention. This hypothesis is to be clearly rejected. On the contrary, the higher depression and anxiety were, the higher the effects of the intervention (see Figure 1), which indicates that those experiencing mood problems might have been especially motivated to seriously engage in the task.
Interestingly, data exploration pointed towards further moderators, especially regarding the immediate effects on negative state mood. There was a lower decrease in males than females in both the complete sample and the subsample; furthermore, male persons did not benefit as much as females from the intervention in terms of positive state mood. There is room for speculating about the explanation of this effect. One is that the list contained a several activities that were applicable for women but rather not for men, at least if typical sex roles are concerned (such as “conducting a private fashion show,” etc.). Another possible explanation is that women are typically higher in psychological mindedness (Shill & Lumley, 2002) and, accordingly, might have been more open to the overall psychological approach of the study and the intervention. The same reason applies to explaining the fact that more than 80% of the participants were female.
Some clear limitations of our study have to be discussed. Most prominently, it was no randomised controlled trial and there was no control treatment. Accordingly, no causal interpretation of the results is possible and it is not clear whether alternative interventions would yield worse, similar or even better results. Second, the examined community sample is not representative of the entire German population. It rather represents those who find it valuable to take part in a psychological study, who are well‐educated and female. However, the sample might be representative for those who can potentially be reached by preventative measures for mental health delivered via the Internet. Third, the study was not conducted as a cross‐national one, and not all items of the activity list might be relevant for communities in other parts of the world. Finally, we have no information as to whether the intervention would or would not unfold lasting effects, a question going beyond the scope of this cross‐sectional study.
Based on a proof‐of‐concept study, we can now provide relatively robust indications (given the large sample) that the selecting of positive and meaningful activities can be a helpful tool for limiting state negative mood and that it can be adequately performed even in a lockdown situation. Replicating this approach in a controlled study with alternative treatments and in different countries across the world should further substantiate the findings. As the ultra‐brief‐BA‐based intervention used can easily be applied via the Internet, we consider our study as a good starting point for this future research.
Supporting information
Appendix S1. Supporting Information
All authors contributed substantially and equally to the study conceptualisation, data collection, analysis and interpretation of data and to the drafting and critical revision of the manuscript.
Open Access funding enabled and organized by Projekt DEAL.
References
- APA . (1994). Diagnostic and statistical manual of mental disorders: DSM‐IV. American Psychiatric Association. [Google Scholar]
- Breyer, B. , & Bluemke, M. (2016). Deutsche Version der positive and negative affect schedule PANAS (GESIS panel). Zusammenstellung sozialwissenschaftlicher Items und Skalen (ZIS). 10.6102/ZIS242 [DOI] [Google Scholar]
- Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Erlbaum. [Google Scholar]
- Ekers, D. , Webster, L. , Van Straten, A. , Cuijpers, P. , Richards, D. , & Gilbody, S. (2014). Behavioural activation for depression: An update of meta‐analysis of effectiveness and sub group analysis. PLoS One, 9(6), e100100. 10.1371/journal.pone.0100100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Field, A. P. (2017). Discovering statistics using IBM SPSS (5th ed.). Sage. [Google Scholar]
- Gräfe, K. , Zipfel, S. , Herzog, W. , & Löwe, B. (2004). Screening psychischer Störungen mit dem “Gesundheitsfragebogen für Patienten (PHQ‐D)”. Diagnostica, 50(4), 171–181. 10.1026/0012-1924.50.4.171 [DOI] [Google Scholar]
- Hayes, A. F. (2013). Introduction to mediation, moderation, and conditional process analysis: A regression‐based approach. Guilford Press. [Google Scholar]
- Holm, S. (1979). A simple sequentially rejective multiple test procedure. Scandinavian Journal of Statistics, 6(2), 65–70. [Google Scholar]
- Hoyer, J. , & Krämer, L. (2021). Verhaltensaktivierung. Standards der Psychotherapie. Hogrefe. [Google Scholar]
- Hoyer, J. , Čolić, J. , Grübler, G. , & Gloster, A. T. (2020). Valued Living before and after CBT. Journal of Contemporary Psychotherapy, 50(1), 37–45. 10.1007/s10879-019-09430-x [DOI] [Google Scholar]
- Hoyer, J. , Hoefler, M. , & Wuellhorst, V. (2020). Activity and subsequent depression levels: A causal analysis of behavioural activation group treatment with weekly assessments over 8 weeks. Clinical Psychology & Psychotherapy, 27, 330–336. 10.1002/cpp.2430 [DOI] [PubMed] [Google Scholar]
- Kazdin, A. E. (2013). Research design in clinical psychology (fourth ed.). Pearson. [Google Scholar]
- Kroenke, K. , Spitzer, R. L. , & Williams, J. B. (2001). The PHQ‐9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. 10.1046/j.1525-1497.2001.016009606.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krohne, H. W. , Egloff, B. , Kohlmann, C.‐W. , & Tausch, A. (1996). [). Investigations with a German version of the positive and negative affect schedule (PANAS)]. Diagnostica, 42(2), 139–156. [Google Scholar]
- Leiner, D. J. (2019). SoSci survey (3.1.06) . https://www.soscisurvey.de
- Lewinsohn, P. M. (1974). Clinical and theoretical aspects of depression. In Calhoun K. S., Adams H. E., & Mitchel K. M. (Eds.), Innovative treatment methods in psychopathology (pp. 63–120). Wiley. [Google Scholar]
- Löwe, B. , Decker, O. , Müller, S. , Brähler, E. , Schellberg, D. , Herzog, W. , & Herzberg, P. Y. (2008). Validation and standardization of the generalized anxiety disorder screener (GAD‐7) in the general population. Medical Care, 46(3), 266–274. 10.1097/MLR.0b013e318160d093 [DOI] [PubMed] [Google Scholar]
- Löwe, B. , Spitzer, R. L. , Zipfel, S. , & Herzog, W. (2002). PHQ‐D: Gesundheitsfragebogen für Patienten. Manual Komplettversion und Kurzform. Pfizer. [Google Scholar]
- MacPhillamy, D. , & Lewinsohn, P. (1982). The pleasant events schedule: Studies on reliability, validity, and scale intercorrelation. Journal of Consulting and Clinical Psychology, 50(3), 363–380. 10.1037/0022-006x.50.3.363 [DOI] [PubMed] [Google Scholar]
- Manea, L. , Gilbody, S. , & McMillan, D. (2012). Optimal cut‐off score for diagnosing depression with the patient health questionnaire (PHQ‐9): A meta‐analysis. CMAJ, 184(3), E191–E196. 10.1503/cmaj.110829 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mayne, T. J. (1999). Negative affect and health: The importance of being earnest. Cognition and Emotion, 13(5), 601–635. 10.1080/026999399379203 [DOI] [Google Scholar]
- Plummer, F. , Manea, L. , Trepel, D. , & McMillan, D. (2016). Screening for anxiety disorders with the GAD‐7 and GAD‐2: A systematic review and diagnostic metaanalysis. General Hospital Psychiatry, 39, 24–31. 10.1016/j.genhosppsych.2015.11.005 [DOI] [PubMed] [Google Scholar]
- Rabe‐Hesketh, S. , & Skrondal, A. (2012). Multilevel and longitudinal modeling using Stata. Volume I: Continuous responses (Third ed.). Stata Press. [Google Scholar]
- Renner, F. , Ji, J. L. , Pictet, A. , Holmes, E. A. , & Blackwell, S. E. (2016). Effects of engaging in repeated mental imagery of future positive events on behavioural activation in individuals with major depressive disorder. Cognitive Therapy and Research, 41(3), 369–380. 10.1007/s10608-016-9776-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Renner, F. , Murphy, F. C. , Ji, J. L. , Manly, T. , & Holmes, E. A. (2019). Mental imagery as a “motivational amplifier” to promote activities. Behaviour Research and Therapy, 114, 51–59. 10.1016/j.brat.2019.02.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shill, M. A. , & Lumley, M. A. (2002). The psychological mindedness scale: Factor structure, convergent validity and gender in a non‐psychiatric sample. Psychology and Psychotherapy: Theory, Research and Practice, 75(2), 131–150. 10.1348/147608302169607 [DOI] [PubMed] [Google Scholar]
- Spitzer, R. L. , Kroenke, K. , Williams, J. B. W. , & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD‐7. Archives of Internal Medicine, 166(10), 1092–1097. 10.1001/archinte.166.10.1092 [DOI] [PubMed] [Google Scholar]
- StataCorp . (2017). Stata statistical software: Release 15. StataCorp LLC. [Google Scholar]
- Watson, D. , Clark, L. , & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54(6), 1063–1070. 10.1037/0022-3514.54.6.1063 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1. Supporting Information