

Abstract
It is critical that academic opinion of pandemic pedagogy is comprehensively quantified in order to inform future practices. Thus, this study examines how anatomists in the United Kingdom (UK) and Republic of Ireland (ROI) perceive the teaching adaptations made in response to COVID‐19, and how these adaptations have impacted their experiences teaching, their online work environment and community. Data was collected via a questionnaire from 24 anatomists across 15 universities in the UK (11) and ROI (4). With regards to teaching, 95.6% of academics have upskilled in new technologies to meet the demands of distance teaching. Academics (95.8%) preferred face‐to‐face delivery of practical sessions. Most universities (80.0%) reported that practical sessions will continue in a new form that ensures social distancing. However, 50.0% of academics are uncertain if these adaptations will improve student learning. Many anatomists believe that the new adaptations may hinder student–student (66.7%) and student–tutor (45.8%) interactions. Regarding assessment, 52.6% of academics preferred traditional methods to online. Remote online assessment was difficult to protect against collusion, but provided time saving opportunities for academics. Finally, in terms of working environment, 83.3% of academics stated that their workload increased; 54.2% preferred working on site rather than remotely and 79.2% think that staff interactions are better when working on site. These results demonstrate a widespread concern amongst anatomists regarding the pandemic‐induced adaptations to teaching, assessment and working environment. However, important opportunities were also identified that could ultimately serve to benefit students and educators alike.
Keywords: assessment, COVID‐19, distance teaching, gross anatomy, medical education, remote working
1. INTRODUCTION
1.1. Impact of COVID‐19 on anatomy departments within medical schools
Due to the coronavirus disease 2019 (COVID‐19) pandemic, face‐to‐face teaching was suspended in every university in the Republic of Ireland (ROI) and the United Kingdom (UK) from March 12 and 16, 2020, respectively, (DES, 2020; GOV.UK, 2020a, 2020b; Mahase, 2020). By April 2020, universities across 188 countries had closed (UNESCO, 2020). Anatomy departments faced unparalleled challenges including the need for clinically trained anatomy tutors to return to clinical practice (Willan et al., 2020). There was pressure for anatomists to create bespoke online teaching resources that were in line with the regulatory bodies that govern the use of cadaveric images, for example, the Human Tissue Authority (HTA) in the UK (HTA, 2016). In the UK and the ROI, cessation of in‐person teaching occurred close to the end of the academic year. Thus, emergency assessment protocols had to be established that upheld standards set by the university and the quality assurance agency (QAA), as well as the primary stakeholders in medical education, the General Medical Council (GMC) in the UK and the Irish Medical Council (IMC) in the ROI. During this uncertain time, educators were tasked with engaging in effective communication with students in an open and informative manner to ensure that they felt supported (Brassett et al., 2020; Hall et al., 2020; Meng et al., 2020). Academics' efforts to engage with students effectively were complicated by their need to work remotely whilst effective internal communication networks were developed (Brassett et al., 2020; Longhurst et al., 2020; Pather et al., 2020). Furthermore, the body donation programmes were suspended by most universities across the UK and ROI (HTA, 2020a). In addition to its educational requirements, many anatomy departments assisted local healthcare services with the provision of equipment and mortuary facilities (Finegan et al., 2020; HTA, 2020b). These additional tasks added further workload to the departmental staff and in particular to designated individuals, the bequeathal team and technical staff.
Many of these issues are ongoing. Academics have been required to continually adapt to changes in regulations within the educational sector to facilitate both socially distanced face‐to‐face teaching as well as online/blended learning. It is essential that the experiences and opinions of anatomy educators are duly considered as the uncertainty continues and the conversations about post‐pandemic delivery of anatomical education start to emerge.
1.2. Adaptations to anatomy teaching during the COVID‐19 lockdown
In lieu of traditional lectures, both synchronous and asynchronous resources were utilized in the initial response to the COVID‐19 pandemic (Brassett et al., 2020; Longhurst et al., 2020; Pather et al., 2020). Live sessions, facilitated by teleconferencing software, were utilized by many universities (Brassett et al., 2020; Longhurst et al., 2020; Pather et al., 2020). Software packages such as “Zoom” (Zoom Voice Communications Inc., San Jose, CA) allow for interaction in several ways, including participant video feed, instant polling, chat functions (written and spoken) and breakout rooms, all of which can help the tutor give student feedback and boost student motivation and engagement (Martin and Bolliger, 2018; Ragusa and Crampton, 2018; Brown and Finn, 2020). Software packages also permit using a flipped‐classroom approach, as well as facilitating clinically relevant problem‐solving activities. Engagement improves if students are able to partake in active learning, for example, solving problems that are relevant to their course (Wimpenny and Savin‐Baden, 2013; Boton and Gregory, 2015; Buelow et al., 2018; Martin and Bolliger, 2018). Synchronous sessions alone were not sufficient to replace traditional lectures as many students were residing in different time zones, had additional caregiving responsibilities, compounded by the personal stresses associated with the COVID‐19 crisis (Longhurst et al., 2020). Thus, lectures were also delivered asynchronously; however, interactive asynchronous methodologies were also utilized. For example, open and anonymous discussion boards and social media (Longhurst et al., 2020). In particular, Twitter enables staff‐student interactions that improves student morale and confidence (Hennessy et al., 2016). Additionally, public and private channels on YouTube enable sharing of bespoke video content that can improve communication (Barry et al., 2016; Mustafa et al., 2020). Using social media to develop an online community (an important component of successful online learning) has been reported to reduce anxiety (Rovai, 2002; Hennessy et al., 2016). Student engagement with asynchronous resources can also improve with audio‐visual presence of the teacher (Martin and Bolliger, 2018).
The resources used to replace anatomy practical classes have been multifaceted (Brassett et al., 2020; Longhurst et al., 2020; Pather et al., 2020). They included digitized cadaveric and virtual 3D resources, as well as updating previous materials to include an increased level of interactivity. Regarding anatomy software programmes (e.g., 3D visualization software), it is important that tutors communicate how to use the software in order to increase student–interface interactions (Attardi et al., 2016). Furthermore, when adapting to online teaching during the COVID‐19 lockdown, academics found that they were limited by time constraints and technological skills (Longhurst et al., 2020). Despite these challenges, Longhurst et al. (2020) reported that one of the biggest opportunities for anatomists was the development of new and bespoke anatomical resources. It has been shown that medical students find online resources useful, but it may be related to “personality preference” and online learning alone may not suit all student groups (McNulty et al., 2006; Smith et al., 2014). A recent report from the Educause Center for Analysis and Research found that faculty preferences skewed heavily in the direction of face‐to‐face interactions with students (Galanek and Gierdowski, 2019).
1.3. Adaptations to anatomy assessment during the COVID‐19 lockdown
Alterations in assessment in response to COVID‐19 within medical education have been reported (Ashokka et al., 2020; Boursicot et al., 2020; Hannon et al., 2020; Mooney et al., 2020; Pather et al., 2020; Sam et al., 2020). This can result in issues surrounding constructive alignment, which requires learning outcomes, to be matched to assessment and teaching activity (Biggs and Tang, 2011; Franchi, 2020). During the COVID‐19 lockdown, written examinations that normally took place in central proctored locations were changed to “online decentralized” assessments (Ashokka et al., 2020). Other institutions utilized different strategies such as simulations, teleconferencing or phone conversations as substitutes to traditional examination formats (Patil and Chan Ho Yan, 2003; Hannon et al., 2020; Mooney et al., 2020). Specific to anatomical assessment, Pather et al. (2020) reported that practical anatomy assessments were moved online. Randomized, higher order questions were used to minimize the potential for student collusion (Pather et al., 2020). In other institutions, summative examinations were changed to formative, or changed from closed to open book tests (Brassett et al., 2020). However, anatomy practical examinations were suspended or canceled in certain medical schools and their reinstatement will be a huge focus in the subsequent academic year (Brassett et al., 2020). It is clear from the literature that assessment formats have changed due to the COVID‐19 lockdown, however, it is not known if these changes are sustainable or if academics agree with them.
1.4. Adaptations to working environment during the COVID‐19 lockdown
Remote working was identified as both an opportunity and a challenge during the initial phase of the COVID‐19 pandemic (Longhurst et al., 2020). This is likely to reflect personal home‐life circumstances such as home office set‐up, technical literacy and childcare and caring responsibilities (Longhurst et al., 2020). Anatomists also highlighted concerns around support for online teaching, technical failures and network sustainability (Pather et al., 2020), all of which are heightened in the context of remote working. Academic collaborations are a source of support and were identified as an important opportunity presented by the COVID‐19 pandemic (Longhurst et al., 2020). Creating a collaborative online community is critical as the pandemic continues to alter the academic landscape and the long‐term effects on university life are uncertain. Online anatomical conferences were held to share information around best practices for online teaching. For example, The British Association of Clinical Anatomists (BACA) are hosting a virtual series throughout the year called “BACA Beats” (BACA, 2020) to celebrate anatomy and continue the conversation in adapting anatomy teaching methods. In addition, the Anatomical Society held its first ever virtual winter meeting completely online in January 2021, in which a number of speakers discussed digital learning in Anatomy (Anatomical Society, 2021).
Online anatomy communities are also sharing resources and best practice methods on social media and anatomy‐related forums (Evans et al. 2020). There is huge potential to share expertise in sub‐specialties across satellite campuses and institutions around the world. Furthermore, online communities can improve student–staff relationships as the use of social media has been shown to foster a sense of community between academics and students (Hennessy et al., 2016). It is necessary to investigate if academic perception of remote working and their working environment has changed as the pandemic has progressed. It is critical that academic support networks continually adapt to help anatomists navigate new pedagogical terrains.
1.5. Teacher's perception of pandemic pedagogy
There is a paucity of quantitative data in the literature regarding the perceptions of educators to pandemic induced changes in teaching. Two papers have provided qualitative descriptions of the issues faced by academic staff. Patra et al. (2021) described staff concerns in an Indian University regarding the mental toll on staff, pay cuts and the fact that the switch to online learning disproportionately affected senior staff. A thematic analysis on the effect of the disruption to education in Australia and New Zealand focusing on the initial responses in March 2020 highlighted similar issues with regards to workload, job security and university budget deficits. In addition, they highlighted lack of computer skills and reduced interaction with students. Cheng et al. (2021), surveyed 358 educators in China and is the only study to present quantitative data pertaining to educators' opinion to date. Of those surveyed over half were satisfied with the effectiveness of their online teaching but only approximately one‐third wished to continue with online teaching (primarily theory sessions only). However, it is apparent that the pandemic and ensuing lockdowns have varied extensively between countries and has impacted universities at different timepoints in their semesters.
1.6. Aims and objectives
To‐date, there is paucity of literature on perceptions of educators in the UK and ROI. The opinions of anatomy educators must be captured as the uncertainty continues and the conversations about postpandemic delivery of anatomical education begin to emerge. This type of analysis is essential to ensure that the views and wellbeing of anatomy educators are considered as academics continue to teach during a pandemic, whilst moving towards the development of a robust anatomical curriculum in the postpandemic era. The current study examines how anatomists in the UK and ROI perceive the teaching adaptations made in response to COVID‐19 and how these adaptations have impacted their delivery of anatomy, their work environment and online teaching community. Specifically, this study aims to address the following objectives.
1) To quantify academic opinions of adaptations to teaching, (in particular practical classes) and assessment strategies.
2) To quantify academic perception of remote working and the online community.
3) To identify challenges and opportunities related to these adaptations.
2. MATERIALS AND METHODS
Ethical approval for this study was granted by the School of Medicine Research Ethics Committee at Trinity College Dublin, the University of Dublin (application number: 20200604). A questionnaire was designed to request information on departmental adaptations and individual opinions on the ongoing responses to the COVID‐19 pandemic. The questionnaire was created by the authors of this study. Questions were designed using results from previous research on initial adaptations to the COVID‐19 lockdown (Longhurst et al., 2020). This ensured that questions reflected the adaptations being made by universities in the UK and ROI. Draft questions were selected for review and outsourced to colleagues in the researchers' respective universities by way of a pilot study. Suggested post‐pilot amendments were agreed by all researchers before inclusion. Five multipart questions were selected based on: teaching (institutional information and role of academic; adaptations to anatomical teaching during the COVID‐19 lockdown); assessments (adaptations to assessment in anatomy during the COVID‐19 lockdown); teaching and assessment for the upcoming academic year and finally remote working and online community. Student–student interactions were defined as the interactions between one learner and other learners alone or in group settings, with or without the real‐time presence of an instructor. Student–tutor interactions referred to the interactions between the learner and the expert of the subject material (Moore, 1989). The questionnaire was created using Qualtrics (Provo, Utah, United States) and distributed to heads of anatomy departments or personal professional contacts within anatomy departments across the UK and ROI (Data S1). The questionnaire was then circulated within departments. A total of 24 responses were received from 15 of the 34 medical schools in the UK and ROI. Feedback was given by responding to Likert‐style agreeable scales, multiple choice questions and through free‐text responses. Depending on the question, if there was an inconsistency between individual responses from the same university with regards to overall departmental approaches (e.g., cessation of the body donor programme) all responses from that university were removed. Data were recorded in and analyzed using Microsoft Excel (Redmond, Washington, United States) software. Descriptive statistics were calculated for Likert items. A chi‐square test for independence was used to test for dependency between academic experience/workload and academic perspective of distance teaching/working environment (ɑ = 0.05). Thematic analysis of the free‐text responses was completed following the six‐step, reflexive approach to thematic analysis, as described by Braun et al., 2019. Thematic analysis was approached using an inductive, semantic and (critical) realist framework. This framework was chosen so that theme generation was based on explicit content within the data, in line with the objectives for this research. All responses were analyzed using thematic analysis by two researchers (DS and KD) as per Braun et al. (2019). The dataset was analyzed, and initial codes were manually generated by both authors by highlighting relevant responses. Any discrepancies were put to all members of the research team. Codes were then assigned a theme which were again reviewed by all authors.
3. RESULTS
3.1. Demographics
There were 24 respondents from 15 different universities (11 from England, four from Ireland). This represented a response rate of 44.1%. Reported job titles included clinical anatomists 4.1% (n = 1), teaching fellows 8.3% (n = 2), lecturers 41.7% (n = 10), senior lecturers 16.7% (n = 4) and professors/directors/subject leaders 29.2% (n = 7). Teaching experience was mixed with 41.7% having 0–5 years (n = 10), 16.7% having 5–10 years (n = 4) and 41.7% having over 10 years lecturing experience (n = 10).
3.2. Suspension of body donor program
Nine universities were identified of which four did not operate a body donor program. Of the remaining five universities, four were facing a reduction in the number of cadaveric specimens available for teaching and one expected to operate normally.
3.3. Academic opinion of online anatomy teaching
Academics (78.3%; n = 18) did not prefer online lecturing to face‐to‐face lecturing (total n = 23; Figure 1A and Table 1). Similarly, academics (95.8%; n = 23) did not prefer online practical classes to face‐to‐face practical classes (total n = 24; Figure 1A and Table 1). Academic preference of lecture and practical delivery was independent from teaching experience (p = 0.80 and p = 0.44, respectively, Chi‐Square test for independence). In order to adapt to distance teaching, 95.6% (n = 22) of academics upskilled in new technologies (total n = 23; Figure 1A and Table 1). When asked if their workload increased to adapt to distance teaching, 83.3% (n = 20) of academics agreed (total n = 24; Figure 1A and Table 1). However, workload was independent from academic preference of lecture and practical delivery (p = 0.37 and p = 0.98, respectively, Chi‐Square test for independence).
FIGURE 1.
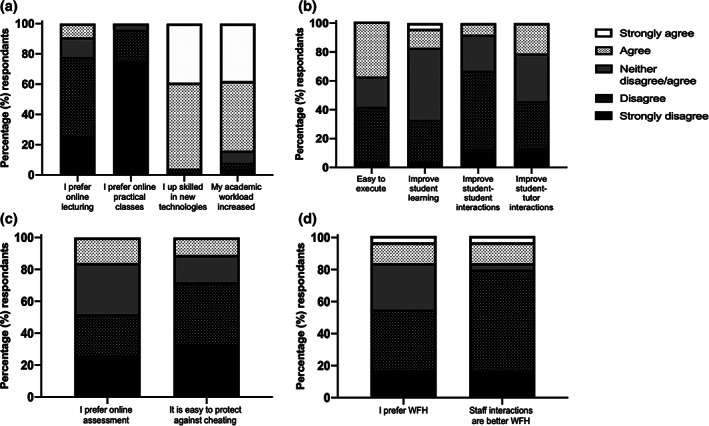
Academic preferences and adaptations to distance teaching (A), practical classes (B), assessment (C) and remote working (D). (A) The majority of academics did not prefer online lecturing/practical classes to face‐to‐face teaching. The majority of academics upskilled in new technologies and experienced increased workload due to distance teaching. (B) Academic opinion was divided about the ease at which practical class adaptations could be executed. 50% of academics were uncertain if adaptations would improve student learning. The majority of academics did not think that adaptations to practical classes would improve student–student interactions but 33% were uncertain if adaptations would improve student–tutor interactions. (C) 52% of academics did not prefer delivering assessments online and 72% of academics found it difficult to protect assessments against collaborative answering. (D) 54.2% of academics did not prefer working from home (WFH) and 79.2% thought that staff interactions suffered as a result
TABLE 1.
Academic opinion of adaptations to distance teaching
| I prefer delivering anatomy lecture content through distance teaching rather than in person face‐to‐face % (n) | I prefer delivering practical anatomy content through distance teaching rather than in person face‐to‐face (%) | I up skilled in new technologies to adapt to distance teaching (%) | My academic workload increased to adapt to distance teaching (%) | |
|---|---|---|---|---|
| Strongly disagree | 26.1 (6) | 75.0 (18) | 0.0 (0) | 4.2 (1) |
| Disagree | 52.2 (12) | 20.8 (5) | 4.3 (1) | 4.2 (1) |
| Neither disagree/agree | 13 (3) | 4.2 (1) | 0.0 (0) | 8.3 (2) |
| Agree | 8.7 (2) | 0.0 (0) | 56.5 (13) | 45.8 (11) |
| Strongly agree | 0.0 (0) | 0.0 (0) | 39.1 (9) | 37.5 (9) |
| n. no | 23 | 24 | 23 | 24 |
3.4. Academic opinion of changes in the delivery of anatomy teaching
Of the 15 universities, 80.0% (n = 12) are proceeding with online or in‐person anatomy practical sessions; 13.3% (n = 2) are canceling practical sessions and 6.7% (n = 1) are postponing practicals (total n = 15). Seventy‐five percent (n = 18) of respondents stated that they will have some form of in‐person, face‐to‐face teaching within their practical sessions (total n = 24). Of those that are proceeding with in‐person face‐to‐face practical sessions, 41.7% (n = 10) stated that adaptations to practical sessions will not be easy to execute. Furthermore, 50.0% (n = 12) are uncertain if these adaptations will improve student learning; 66.7% (n = 16) and 45.8% (n = 11) disagree that these adaptations will improve student–student and student–tutor interactions, respectively (total n = 24; Figure 1B and Table 2). Thematic analysis revealed that the biggest challenges facing universities in implementing adaptations to anatomy practical sessions was the management of logistics (33.0%; n = 7) and increased workload (33.3%; n = 7). Academics were also concerned about how to authentically replicate the dissection room experience online (19%; n = 4); decreases in staff numbers/capabilities (9.5%; n = 2) and financial pressures to purchase personal protective equipment (PPE; 4.8%; n = 1; total n = 21). The biggest opportunities presented to universities included the addition of online resources (66.7%; n = 12) and smaller group teaching size (33.3%; n = 6; total n = 18).
TABLE 2.
Academic opinion of adaptations to practical classes
| I think that adapting dissection activities/practical classes will be easily executed % (n) | I think that adaptations to dissection activities/practical classes will improve student learning (%) | I think that adaptations to dissection activities/practical classes will improve student–student interactions (%) | I think adaptations to dissection activities/practical classes will improve student–tutor interactions (%) | |
|---|---|---|---|---|
| Strongly disagree | 4.2 (1) | 4.2 (1) | 12.5 (3) | 12.5 (3) |
| Disagree | 37.5 (9) | 29.2 (7) | 54.2 (13) | 33.3 (8) |
| Neither disagree/agree | 20.8 (5) | 50.0 (12) | 25 (6) | 33.3 (8) |
| Agree | 37.5 (9) | 12.5 (3) | 8.3 (2) | 20.8 (5) |
| Strongly agree | 0.0 (0) | 4.2 (1) | 0.0 (0) | 0.0 (0) |
| n. no | 24 | 24 | 24 | 24 |
Of the respondents that already provided access to cadaveric material, 73.3% (n = 11) plan to provide students with the opportunity to perform dissection (total n = 15) and 90.5% (n = 19) plan to provide access to cadaveric material (total n = 21, Table 3). In order for practical sessions to adhere to government guidelines, universities that are providing face‐to‐face practical sessions are using PPE (90.9%; n = 10), reducing class sizes (90.9%; n = 10), implementing social distancing measures (90.9%; n = 10) and restricting the number of students per donor/specimen (63.3%; n = 7; total n = 11). Regarding licenses for anatomical education software, 46.7% (n = 7) of universities have purchased or are planning to purchase licenses and 33.3% (n = 5) would like to but are restricted by budget (total n = 15).
TABLE 3.
Student access to practical class activities
| Will medical students have the opportunity to perform anatomy dissection in the next academic semester? % (n) | Will medical students have physical access to cadaveric material in the next academic semester? (%) | |
|---|---|---|
| Yes | 73.3 (11) | 90.5 (19) |
| No | 6.7 (1) | 4.8 (1) |
| Undecided | 20.0 (3) | 4.8 (1) |
| n. no | 15 | 21 |
| n. no that did not provide access pre‐lockdown | 8 | 2 |
3.5. Academic opinion of changes in the delivery of anatomy assessment
Over half (52.6%; n = 10) of academics preferred the delivery of assessments by paper format as compared to remote online (total n = 19; Figure 1C and Table 4). Assessments were not easy to protect against collaborative answering/cheating according to 72.2% (n = 13) of academics (total n = 18; Figure 1C and Table 4). Over half (52.6%; n = 10) of written examinations were closed book (total n = 19), compared to 77.8% (n = 7) of practical examinations (n = 9). Only 16.6% (n = 3) of respondents stated that students were monitored during written assessments (total n = 18) and no invigilation measures were taken for practical assessments (total n = 8). Regarding summative assessment, 61.9% (n = 13) and 70.0% (n = 7) of academics stated that the format for written and practical examinations changed from the previous semester (total n = 21 and n = 10, respectively). The most commonly used question formats for both formative and summative assessments were multiple choice / single best answer questions (Table 5). Furthermore, 9.1% (n = 2) and 38.5% (n = 5) of summative written and practical examinations were canceled due to the COVID‐19 lockdown (total n = 22 and n = 13, respectively, Table 5).
TABLE 4.
Academic opinion of adaptations to assessments
| I prefer the delivery of assessment online rather than standard assessment procedures % (n) | I found it easy to protect assessments against collaborative answering/cheating % (n) | |
|---|---|---|
| Strongly disagree | 26.3 (5) | 33.3 (6) |
| Disagree | 26.3 (5) | 38.9 (7) |
| Neither disagree/agree | 31.6 (6) | 16.7 (3) |
| Agree | 15.8 (3) | 11.1 (2) |
| Strongly agree | 0.0 (0) | 0.0 (0) |
| n. no | 19 | 18 |
TABLE 5.
Format of assessment
| Assessment type | Multiple choice/single best answer % (n) | Short answer % (n) | Long answer/essay % (n) | None/canceled % (n) | n. no | |
|---|---|---|---|---|---|---|
| Written | Formative | 92.3 (12) | 53.9 (7) | 0.0 (0) | 7.7 (1) | 13 |
| Summative | 86.4 (19) | 36.4 (8) | 4.6 (1) | 9.1 (2) | 22 | |
| Practical | Formative | 58.3 (7) | 8.3 (1) | 0.0 (0) | 33.3 (4) | 12 |
| Summative | 46.2 (6) | 23.1 (3) | 0.0 (0) | 38.5 (5) | 13 | |
Thematic analysis revealed that the most common challenge faced by academics in delivering assessments online was cheating/collusion (40.9%; n = 9). Changes to assessment format was another challenge encountered (27.3%; n = 6), with academics citing “loss of constructive alignment” and “inflated results” as some of their concerns. Technical issues (18.2%; n = 4), increased workload (9.1%; n = 2) and management of logistics (4.5%; n = 1) were also identified as concerns among academics (total n = 22).
Thematic analysis revealed that the most common opportunity identified by academics was time saving. Academics (36.8%; n = 7) stated that time was saved due to reduced marking, not having to set up traditional spotters, the ability to monitor all students at once and the ease of delivering scripts. There was also an opportunity to host more frequent assessments (21.1%; n = 4), make use of software features (21.1%; n = 4), identify new resources (15.8%; n = 3) and create a higher standard of examination (5.3%; n = 1; total n = 19).
Furthermore, 20.8% (n = 5) of academics think that assessments will continue to be delivered online and remotely (total n = 24), but there is uncertainty (63.2%; n = 12) if additional measures will be implemented to protect against collaborative answering / cheating (total n = 19).
3.6. Academic opinion of remote working and online community
Over half (54.2%; n = 13) of academics did not prefer working remotely as compared to on site (total n = 24; Figure 1D and Table 6). Academic preference for remote working was not related to teaching experience or workload (p = 0.40 and p = 0.37, respectively, Chi Square test for independence). Staff interactions were not better when working remotely as compared to on site according to 79.2% (n = 19) of academics (total n = 24; Figure 1D and Table 6). Academics' opinion of staff interactions was not related to teaching experience or workload (p = 0.21 and p = 0.98, respectively, Chi Square test for independence).
TABLE 6.
Academic opinion of remote working and online community
| I prefer working from home than on site % (n) | I think staff interactions are better from working from home rather than on site % (n) | |
|---|---|---|
| Strongly disagree | 16.7 (4) | 16.7 (4) |
| Disagree | 37.5 (9) | 62.5 (15) |
| Neither disagree/agree | 29.2 (7) | 4.2 (1) |
| Agree | 12.5 (3) | 12.5 (3) |
| Strongly agree | 4.2 (1) | 4.2 (1) |
| n. no | 24 | 24 |
The COVID‐19 lockdown led to new personal academic collaborations according to 41.7% (n = 10) of academics (total n = 24). Six participants expanded on this and stated that the lockdown led to increased research collaborations (n = 4) and / or attendance of sharing of best practice meetings (n = 3). Academic collaboration was not related to teaching experience or workload (p = 0.12 and p = 0.68, respectively, Chi Square test for independence). Additionally, 54.2% (n = 13) of academics were encouraged to attend more online conferences (total n = 24). Online conference attendance was not related to teaching experience or workload (p = 0.13 and p = 0.57, respectively, Chi‐Square test for independence).
4. DISCUSSION
The aim of this study was to inform the wider medical education community about academic perspectives in relation to the changes in anatomical education due to the COVID‐19 pandemic. The literature in this area has largely focused on what resources and strategies were implemented to deliver anatomy lectures and practical sessions, due to the lockdown and cessation of face‐to‐face teaching (Brassett et al., 2020, Evans et al., 2020; Gupta and Pandey, 2020; Herr and Nelson, 2020, Longhurst et al., 2020; Naidoo et al., 2020; Tucker and Anderson, 2020; Pather et al., 2020; Cheng et al., 2021, Flynn et al., 2021 Harmon et al., 2021). However, there is limited literature describing anatomist's opinions on the changes and how their working life has been impacted (Pather et al. 2020; Cheng et al., 2021; Patra et al. 2021). The following discussion is divided into three parts which reflects the three discrete sections of the distributed survey: teaching, assessment and working environment.
4.1. Teaching
With regards to the move to online teaching, 78.3% of academics still prefer face‐to‐face lectures over lectures delivered online. Furthermore, 95.8% of academics preferred face‐to‐face practical sessions over sessions delivered online. This is in line with a Chinese study that found only 2 (0.6%) wanted to continue with online practical sessions (Cheng et al., 2021). Practical sessions are a significant part of the delivery of anatomical education within the medical curriculum (Drake et al., 2002, 2009; Estai and Bunt, 2016). Not only do practical sessions allow students to develop a deep comprehension of 3D anatomical relations, variations and pathologies (Aziz et al., 2002; Azer et al., 2007; Smith and Mathias, 2009; Estai and Bunt, 2016; Macdonald 2020), they also facilitate the development of communication and teamwork skills and provide a valuable opportunity for peer‐tutor interactions (Korf et al., 2008; Kumar and Kumar, 2019; Franchi, 2020). Students can also access osteology specimens, radiographic images and models in a laboratory setting (Franchi, 2020). Practical sessions that utilize cadaveric material allow students to develop skills in manual dexterity, empathy, encountering death and elements of professionalism (Aziz et al., 2002; Korf et al., 2008; Estai and Bunt, 2016; Kumar and Kumar, 2019; Brassett et al., 2020; Jones, 2020; Souza et al., 2020). Thus, it is unsurprising that nearly all academics were dissatisfied with recreating these elements for delivering practical sessions online. Furthermore, 95.6% of academics stated that they have upskilled in technological capabilities. This indicates that academics may have learnt how to utilize online teaching resources but still find it more difficult to deliver content online compared to face‐to‐face. It must also be stated that senior faculty members experienced disproportionate levels of stress and anxiety, compared to younger faculty, as they switched to online learning platforms (discussed in Patra, 2020).
In light of academic preference for in person teaching, 80.0% of universities are planning to reinstate some form of face‐to‐face anatomy practical sessions as soon as local restrictions allow. Mathiowetz et al. (2016) reported that participation in anatomy practical sessions was favorable to online courses in terms of examination marks, perceived learning and satisfaction (Mathiowetz et al., 2016). However, 41.7% of respondents are facing challenges in the execution of these sessions, with logistics and workload being the largest concerns. Also, 50.0% of the respondents are uncertain if these adaptations will improve student learning. This mixed opinion was also stated by Chen et al. (2021) as only 29% of teachers they survey believed students would achieve 80–100% of the intended learning outcomes.
Many anatomists believe that the new adaptations may hinder student–student (66.7%) and student–tutor (45.8%) interactions. Prior to the pandemic, the hours dedicated to anatomy have faced reduction over the years. Thus, the anatomy practical sessions provide an important point of contact between the students and their tutors. Academics must consider how best to minimize the broader implications resulting from losing elements of these sessions. This may include increased discussions outside of the practical session be it through synchronous or asynchronous methodologies. In the UK and ROI, many of the anatomy practical sessions were already completed before the COVID‐19 lockdown, and hence, the impact of long‐term reduced tutor contact remains to be seen. Therefore, it is imperative that anatomists provide adequate online substitutes and that medical schools prioritize in person face‐to‐face anatomy practical sessions where possible. In addition, faculty should provide logistical support to the anatomy departments that are concerned with implementing new and ever‐changing guidelines on social distancing within educational settings.
As the body donor programme was largely suspended in universities across the UK and ROI, four out of five of the surveyed universities are facing a reduction in the number of cadaver specimens available for teaching. This is similar globally; in China 53.3% of anatomy departments received fewer donated bodies or temporarily suspended donor programs (Cheng et al., 2021). Disruptions to body donations have also been reported in India (Ravi, 2020), Nigeria (Okafor and Chia, 2020) and Australia and New Zealand (Pather et al., 2020). The potential for a repeated suspension of body donor programs over the next year cannot be ruled out. Not only does this have ethical implications as discussed by Jones (2020), but it also means that departmental teams may need to consider which resources can serve as substitutes for the foreseeable future. The resources that have been utilized to date include digitized cadaveric resources and/or virtual 3D resources. Dissection videos can boost student satisfaction (Mahmud et al. 2011). However, their impact on learner gain is mixed with some studies showing an improvement (DiLullo et al., 2006; Walker et al., 2008) while others have not revealed improved grades (Granger and Calleson, 2007; Saxena et al., 2008; Mahmud et al., 2011). As these videos only provide passive learning opportunities, adding in activities and clear links to clinically relevant anatomy may aid in this regard (Langfield et al., 2018; Grosser et al., 2019). Bespoke resources may increase student satisfaction but are very time consuming for academics to produce and may not increase learner gain (Mandernach 2009; Gewin 2020). There are highly regarded online resources already in existence with Acland's Video Atlas of Human Anatomy (Acland, 2013) being one of the most notable. Therefore, educators should weigh up the cost–benefit implications of making in‐house resources. Data pertaining to the effectiveness of virtual 3D resources is mixed (Triepels et al., 2020). Reviews on students' perceived learning may be, at least in part, attributed to staff and student's ability to use these platforms (Doubleday et al., 2011; Attardi et al., 2016). Importantly, when used in addition to cadaveric material they have had positive results (Yammine and Violato, 2015; Darras et al., 2019). Thus, supplementing the practical sessions with virtual 3D resources may be a useful avenue to pursue given the potential long‐term implications of COVID‐19 on access to cadaveric material in the future. At the start of the pandemic, anatomical software companies frequently permitted free access to a multitude of their services. However, permanent access may rely on institutional ability to purchase licenses anatomical software programmes (Franchi, 2020). This is reflected in our results as 33.3% of universities were restricted from accessing additional educational resources due to budgetary constraints. In the longer‐term, departments need to consider how these resources should be embedded within the curriculum both as the uncertainty continues and in the preceding years.
4.2. Assessment
Regarding assessment, 52.6% of academics preferred the delivery of assessments via standard printed exams as compared to online assessment procedures. Multiple choice/single best answer examinations were the most common assessment modality utilized in both written and practical examinations. A large proportion of academics reported that summative assessment format changed due to online delivery, which is in‐line with previous reports (Pather et al., 2020; Brassett et al., 2020; Cheng et al., 2021). However, there remained very little difference between formative and summative assessment modalities. This may indicate that academics adapted to the changes in assessment type by providing students with aligned formative assessment questions. This is one of the guiding principles of assessment by the Quality Assurance Agency (QAA) that ensures students are prepared for examinations (QAA, 2018). In light of the pandemic, students have reported that including formative quizzes in online teaching sessions will improve quality and learning (Srinivasan, 2020).
Although the majority of written (52.6%) and practical (77.8%) examinations were closed book, only 16.6% of respondents stated that they monitored students during assessments. Overall, 72.2% of academics reported that they did not think assessments were easy to protect against collaborative answering/cheating. This is not a new phenomenon and has been a concern of educators since the digital revolution of higher education (Parker et al. 2011). For future online assessments, technology such as text matching software, analytics software and remote invigilation (using webcams or facial recognition software) can be used to reduce cheating and collusion (QAA, 2020; Reid and Sam 2020). Approximately one‐third of academics reported that one of the opportunities of online assessment was timesaving. Cantillon et al. (2004) reported that changing to online assessments in the long‐term may reduce overall departmental workload. However, it requires significant institutional buy‐in, in addition to departmental upskilling and an increase in workload in the short‐term. Setting up traditional spotter examinations in the anatomy laboratory is time consuming and therefore the move to online assessment by universities may be favorable in the long‐term (Dennick et al., 2009; Schubert et al., 2009; Reid and Sam, 2020). Furthermore, online assessment of anatomy practical sessions does not affect student performance compared to traditional methodologies (Dennick et al., 2009; Inuwa et al., 2012). However, online images may not be able to provide further context and retrieval cues that were established during the practical session and issues surrounding constructive alignment must be considered going forward (Ali et al., 2015). Thus, online assessment can be seen as a challenge or an opportunity relative to the support provided to set it up. If examinations continue to be facilitated through online platforms, then a combined approach between faculty and university may be crucial to ensure adequate examination integrity.
4.3. Remote working environment
Government restrictions and public health advice suddenly mandated that academics work from home and this change in work practice occurred without any time for departmental teams to implement internal communication strategies to mitigate against the loss of face‐to‐face communication. This study demonstrated that anatomists have mixed opinions in regard to remote working; approximately, 54.2% of academics do not prefer working remotely with 83.3% of academics stating that their workload increased. Working from home (WFH) can provide benefits such as improved work‐life balance, productivity and creativity (Hunter, 2019). It has the added benefit of allowing workers to save money, as there is no longer the need to commute. Furthermore, a previous study reported that WFH reduces depression in women with children (Shepherd‐Banigan et al., 2015). Academics have reported that WFH has enhanced social connectivity and inclusivity, whilst adopting new technologies (Watermeyer et al., 2020). However, WFH may contribute to employees experiencing burnout, a mental health syndrome characterized by “feelings of energy depletion or exhaustion, increased mental distance from one's job or feelings of cynicism or negativism about one's job, and reduced professional efficacy” (World Health Organization, 2019). Furthermore, as the transition to remote working was immediate and full‐time for all staff, mechanisms may not have been in place to support staff working remotely. This is supported by the fact that 79.2% did not think that staff interactions were better when working remotely as compared to on site. Additionally, unfavorable working conditions have been reported since the lockdown. Academics have reported that working from home intensified work and eroded the work‐life balance, in addition to affecting their pedagogical roles (Watermeyer et al., 2020). Workers with children and/or other caring responsibilities, in addition to those who lack confidence/experience in technology, are disproportionately affected (Hoffman et al., 2020). In India, it has been reported that some academics faced salary cuts and a reduction in staff numbers, causing emotional turmoil for faculty (Patram 2021) whilst academics in Australia and New Zealand experienced stress related to job security (Pather et al., 2020). The current study found that academic opinion on remote working and internal communications was not related to differences in teaching experience, the amount of technological upskilling that was undertaken or an individual's workload. This indicates that preferences to working remotely may be due to personal circumstances and that it is imperative that department heads and line managers provide as much flexibility as possible. Additionally, internal communications within departments need to be under continued review to ensure that they are adequate for the continuous changes and increased workloads for staff. Furthermore, 41.7% stated that the COVID‐19 lockdown led to new personal academic collaboration. The nature of the collaborations varied and 54.2% stated that the national lockdown encouraged them to attend more virtual conferences. The results of this survey suggest that communication within and between departments may have been hindered by the sudden switch to remote working. To further increase collaboration within departments, academics should regularly highlight any opportunity to share resources or information regarding upcoming events such as virtual conferences.
4.4. Limitations
The limitations of the study are related to the subset of samples obtained which included universities from England and the ROI but not Scotland, Wales or Northern Ireland. Regional adaptations and governmental guidance may yield differences in approaches to re‐establishing on campus, face‐to‐face teaching. Second, we exclusively collected data regarding the anatomical education of medical students and not any other discipline. Thus, it should be acknowledged that this survey would not have captured any unique challenges encountered by nonmedical disciplines or their respective solutions. Third, the COVID‐19 pandemic is ongoing and continues to be unpredictable. Between regional and national changes in public health policies, universities may be affected in different ways during the upcoming academic year. Thus, it is important to acknowledge that this survey is a temporal snapshot and as such, follow‐up studies are required to ascertain any long‐term effects that this crisis has had on the delivery of anatomy education to medical students.
5. CONCLUSIONS
This study has highlighted that anatomists have concerns about the adaptations required for the delivery of teaching and assessment in response to the COVID‐19 pandemic. As we continue with this model of teaching, anatomists are worried that staff–staff, staff–student and student–student interactions will suffer as a consequence. Despite these concerns, this study has identified a number of opportunities that have arisen due to the massive shift to online teaching. Anatomists have upskilled considerably, and bespoke learning resources have been created and new online assessment strategies identified. This can lead to time saving and decreased academic workload. Finally, long‐term consequences of the COVID‐19 pandemic may make it more difficult for medical schools to operate body donor programmes and dissection facilities. However, full evaluation of these resources in conjunction with consideration on availability of cadaveric resources are required prior to embedding them into the curriculum going forward. There may be disparities in the disruptions to face‐to‐face teaching and assessment between medical schools and this may affect students in different ways. Thus, the effect of these changes on anatomical comprehension and competency will need to be evaluated. Anatomists must now redouble their efforts to engage meaningfully on these issues with both the national and international community such that they may capitalize on any arising opportunity and form long‐lasting collaborations for the betterment of our students and discipline.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
Supporting information
DATA S1: Supporting Information
ACKNOWLEDGMENTS
The authors would like to express their sincerest gratitude to the fellow anatomists who contributed to this study, to Dr Mark Pickering (University College Dublin) for his helpful advice regarding statistics and to Dr Claire Smith for her valuable guidance regarding manuscript preparation. Open access funding provided by IReL.
Biographies
Kate Dulohery, B.Sc., M.Sc., Ph.D., F.H.E.A., is a senior lecturer in anatomy in the School of Medicine at University of Sunderland, Sunderland, UK. She teaches anatomy to medical and allied health students and her research interests include incorporation of technology in anatomical education.
Deidre Scully, B.Sc., M.Sc., Ph.D., is a postdoctoral research fellow in the Department of Molecular Physiology and Biophysics, Baylor College of Medicine, Houston TX, USA. She previously held the position of Anatomy Teaching Fellow in the School of Medicine, Trinity College Dublin where she coordinated all elements of practical classes for medical and allied health students. Her research interests include medical education and reproductive biology.
Georga J. Longhurst, B.Sc. (hons)., M.Sc., P.G.Cert.H.B.E., F.H.E.A., is a lecturer in anatomical sciences at St George's University of London in London, UK. She teaches anatomy to medical and allied health students. She has a research interest in anatomical education.
Danya Stone, B.Sc., M.Sc., F.H.E.A., is a lecturer in anatomy at Brighton and Sussex Medical School (Brighton), Falmer, UK. She teaches anatomy to medical students and contributes to teaching on multiple external courses. Her research interest is in medical education.
Thomas Campbell, B.A., M.B., B.Ch., B.A.O., M.Sc., Ph.D., is a lecturer in human anatomy at the School of Medicine, University College Dublin, Belfield, Dublin, Republic of Ireland. He teaches both allied health and medical students, and his research interests include neuroscience, 3D printing and education.
Dulohery, K. , Scully, D. , Longhurst, G. J. , Stone, D. M. , & Campbell, T. (2021). Emerging from emergency pandemic pedagogy: A survey of anatomical educators in the United Kingdom and Ireland. Clinical Anatomy, 34(6), 948–960. 10.1002/ca.23758
Kate Dulohery and Deirdre Scully have contributed equally to this work.
Contributor Information
Kate Dulohery, Email: kate.dulohery@sunderland.ac.uk.
Deirdre Scully, Email: deirdremaryscully@gmail.com.
REFERENCES
- Acland R. 2013. Acland's video atlas of human anatomy. Wolters Kluwer Health, Inc. Retrieved from https://aclandanatomy.com/. [Google Scholar]
- Ali, A. , Khan, Z. , Konczalik, W. , Coughlin, P. , & El Sayed, S. (2015). The perception of anatomy teaching among UKmedical students. Bulletin of the Royal College Surgeons of England, 97, 397–400. [Google Scholar]
- Ashokka, B. , Ong, S. Y. , Tay, K. H. , Loh, N. H. W. , Gee, C. F. , & Samarasekera, D. D. (2020). Coordinated responses of academic medical centres to pandemics: Sustaining medical education during COVID‐19. Medical Teacher, 11, 1–10. [DOI] [PubMed] [Google Scholar]
- Anatomical Society . 2021. Anatomical Society Meetings. Retrieved from https://www.anatsoc.org.uk/meetings/our-meetings/anatsocmeeting.
- Attardi, S. M. , Choi, S. , Barnett, J. , & Rogers, K. A. (2016). Mixed methods student evaluation of an online systemic human anatomy course with laboratory. Anatomical Sciences Education, 9, 272–285. [DOI] [PubMed] [Google Scholar]
- Azer, S. A. , Eizenberg, N. , Azer, S. A. , & Eizenberg, N. (2007). Do we need dissection in an integrated problem‐based learning medical course? Perceptions of first and second year students. Surgical and Radiologic Anatomy, 29, 173–180. [DOI] [PubMed] [Google Scholar]
- Aziz, M. A. , Mckenzie, J. C. , Wilson, J. S. , Cowie, R. J. , Ayeni, S. A. , & Dunn, B. K. (2002). The human cadaver in the age of biomedical informatics. The Anatomical Record, 269, 20–32. [DOI] [PubMed] [Google Scholar]
- BACA . 2020. Meetings, British Association of Clinical Anatomists Retrieved from https://www.baca-anatomy.co.uk/pages/81-meetings.
- Barry, D. S. , Marzouk, F. , Chulak‐Oglu, K. , Bennett, D. , Tierney, P. , & O'Keeffe, G. W. (2016). Anatomy education for the YouTube generation. Anatomical Sciences Education, 9, 90–96. [DOI] [PubMed] [Google Scholar]
- Biggs, J. B. , & Tang, C. (2011). Teaching for quality learning at university (4th ed., p. 480). Open University Press, Inc. [Google Scholar]
- Boton, E. C. , & Gregory, S. (2015). Minimizing attrition in online degree courses. Journal of Education Online, 12, 62–90. [Google Scholar]
- Boursicot, K. , Kemp, S. , Ong, T. H. , Wijaya, L. , Goh, S. H. , Freeman, K. , & Curran, I. (2020). Conducting a high‐stakes OSCE in a COVID‐19 environment. MedEdPublish, 9, 1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brassett, C. , Cosker, T. , Davies, D. C. , Dockery, P. , Gillingwater, T. H. , Lee, T. C. , Milz, S. , Parson, S. H. , Quondamatteo, F. , & Wilkinson, T. (2020). COVID‐19 and anatomy: Stimulus and initial response. Journal of Anatomy, 237, 393–403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Braun, V. , Clarke, V. , Hayfield, N. , & Terry, G. (2019). Thematic analysis. In Liamputtong P. (Ed.), Handbook of research methods in health social sciences (pp. 843–860). Singapore. [Google Scholar]
- Brown, M. E. , & Finn, G. M. (2020). Intra‐COVID collaboration: Lessons for a post‐COVID world. Medical Education, 55, 122–124. 10.1111/medu.14366. [DOI] [PubMed] [Google Scholar]
- Buelow, J. R. , Barry, T. , & Rich, L. E. (2018). Supporting learning engagement with online students. Online Learning, 22, 313–340. [Google Scholar]
- Cantillon, P. , Irish, B. , & Sales, D. (2004). Using computers for assessment in medicine. British Medical Journal, 329, 606–609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cheng, X. , Chan, L. K. , Pan, S. , Cai, H. , Li, Y. , & Yong, X. (2021). Gross anatomy education in China during the Covid‐19 pandemic: A National Survey. Anatomical Sciences Education, 14, 8–18. [DOI] [PubMed] [Google Scholar]
- Darras, K. E. , Spouge, R. , Hatala, R. , Nicolaou, S. , Hu, J. , Worthington, A. , Krebs, C. , & Forster, B. B. (2019). Integrated virtual and cadaveric dissection laboratories enhance first year medical students' anatomy experience: A pilot study. BMC Medical Education, 19, 1–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dennick, R. , Wilkinson, S. , & Purcell, N. (2009). Online eAssessment. Medical Teacher, 31, 192–206. [DOI] [PubMed] [Google Scholar]
- DES . 2020. Department of Education and Skills. Briefing on Covid‐10 responses in education and training sector. 1st. Government of Ireland. 26. Retrieved from https://www.education.ie/en/The-Department/Announcements/briefing-on-covid-19-responses-in-the-education-and-training-sector.pdf [Google Scholar]
- DiLullo, C. , Coughlin, P. , D'Angelo, M. , McGuinness, M. , Bandle, J. , Slotkin, E. M. , Shainker, S. A. , Wenger, C. , & Berray, S. J. (2006). Anatomy in a new curriculum: Facilitating the learning of gross anatomy using web access streaming dissection videos. Journal of Visual Communication in Medicine, 29, 99–108. [DOI] [PubMed] [Google Scholar]
- Doubleday, E. G. , O'Loughlin, V. D. , & Doubleday, A. F. (2011). The virtual anatomy laboratory: Usability testing to improve an online learning resource for anatomy education. Anatomical Sciences Education, 4, 318–326. [DOI] [PubMed] [Google Scholar]
- Drake, R. L. , Lowrie, D. J. , & Prewitt, C. M. (2002). Survey of gross anatomy, microscopic anatomy, neuroscience, and embryology courses in medical school curricula in the United States. The Anatomical Record, 269, 118–122. [DOI] [PubMed] [Google Scholar]
- Drake, R. L. , McBride, J. M. , Lachman, N. , & Pawlina, W. (2009). Medical education in the anatomical sciences: The winds of change continue to blow. Anatomical Sciences Education, 2, 253–259. [DOI] [PubMed] [Google Scholar]
- Estai, M. , & Bunt, S. (2016). Best teaching practices in anatomy education: A critical review. Annals of Anatomy, 208, 151–157. [DOI] [PubMed] [Google Scholar]
- Evans, D. J. , Bay, B. H. , Wilson, T. D. , Smith, C. F. , Lachman, N. , & Pawlina, W. (2020). Going virtual to support anatomy education: A STOPGAP in the midst of the Covid‐19 pandemic. Anatomical Sciences Education, 13, 279–283. [DOI] [PubMed] [Google Scholar]
- Finegan, O. , Fonseca, S. , Guyomarc'h, P. , Morcillo Mendez, M. D. , Rodriguez Gonzalez, J. , Tidball‐Binz, M. , & Winter, K. A. (2020). International Committee of the red Cross (ICRC): General guidance for the management of the dead related to COVID‐19. Forensic Science International: Synergy, 2, 129–137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flynn, W. P. , Kumar, N. , Donovan, R. , Jones, M. , & Vickerton, P. (2021). Delivering online alternatives to the anatomy laboratory: Early experience during the COVID‐19 pandemic. Clinical Anatomy, 2021, 1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Franchi, T. (2020). The impact of the Covid‐19 pandemic on current anatomy education and future careers: A student's perspective. Anatomical Sciences Education, 13, 312–315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galanek, J. D. , & Gierdowski, D. C. (2019). ECAR study of faculty and information technology, 2019. Research report. ECAR. [Google Scholar]
- Gewin, V. (2020). Five tips for moving teaching online as COVID‐19 takes hold. Nature, 580, 295–296. [DOI] [PubMed] [Google Scholar]
- GOV.UK . 2020a. Staying at home and away from others (social distancing) ‐ GOV.UK. Retrieved from https://www.gov.uk/government/publications/full-guidance-on-staying-at-home-and-away-from-others/full-guidance-on-staying-at-home-and-away-from-others.
- GOV.UK . 2020b. Coronavirus (COVID‐19): guidance for educational settings ‐ GOV.UK. Retrieved from https://www.gov.uk/government/publications/guidance-to-educational-settings-about-covid-19/guidance-to-educational-settings-about-covid-19.
- Granger, N. A. , & Calleson, D. (2007). The impact of alternating dissection on student performance in a medical anatomy course: Are dissection videos an effective substitute for actual dissection? Clinical Anatomy, 20, 315–321. [DOI] [PubMed] [Google Scholar]
- Grosser, J. , Bientzle, M. , Shiozawa, T. , Hirt, B. , & Kimmerle, J. (2019). Acquiring clinical knowledge from an online video platform: a randomized controlled experiment on the relevance of integrating anatomical information and clinical practice. Anatomical Sciences Education, 12(5), 478–484. 10.1002/ase.1841 [DOI] [PubMed] [Google Scholar]
- Gupta, N. , & Pandey, S. (2020). Disruption of anatomy dissection practical in COVID‐19 pandemic: Challenges, problems and solutions. J Lumbini med Coll 8:135–137.Egrating anatomical information and clinical practice. Anatomical Sciences Education, 12, 478–484. [Google Scholar]
- Hall, A. K. , Nousiainen, M. T. , Campisi, P. , Dagnone, J. D. , Frank, J. R. , Kroeker, K. I. , Brzezina, S. , Purdy, E. , & Oswald, A. (2020). Training disrupted: Practical tips for supporting competency‐based medical education during the COVID‐19 pandemic. Medical Teacher, 7, 756–761. [DOI] [PubMed] [Google Scholar]
- Hannon, P. , Lappe, K. , Griffin, C. , Roussel, D. , & Colbert‐Getz, J. (2020). An objective structured clinical examination: From examination room to zoom breakout room. Medical Education, 54, 861. [DOI] [PubMed] [Google Scholar]
- Harmon, D. , Attardi, S. M. , Barremkala, M. , Bentley, D. , Brown, K. M. , Dennis, J. K. , Goldman, H. M. , Harrell, K. M. , Klein, B. A. , Ramnanan, C. J. , Richtsmeier, J. T. , & Farkas, G. J. (2021). An analysis of anatomy education before and during covid‐19: May–August 2021. Anatomical Sciences Education, 14, 132–147. [DOI] [PubMed] [Google Scholar]
- Hennessy, C. M. , Kirkpatrick, E. , Smith, C. F. , & Border, S. (2016). Social media and anatomy education: Using twitter to enhance the student learning experience in anatomy. Anatomical Sciences Education, 9, 505–515. [DOI] [PubMed] [Google Scholar]
- Herr, M. J. , & Nelson, R. J. (2020). Administering a stay‐at‐home dental gross anatomy practical during COVID‐19. Journal of Dental Education, 2020, 1–2. [DOI] [PubMed] [Google Scholar]
- Hoffman, K. E. , Garner, D. , Koong, A. C. , & Woodward, W. A. (2020). Understanding the intersection of working from home and burnout to optimize post‐COVID19 work arrangements in radiation oncology. International Journal of Radiation Oncology, Biology, Physics, 108, 370–373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- HTA . 2016. Human tissue authority. HTA guidelines: filming or photographing of bodies or body parts that have been donated to medical schools or surgical training Centres. 1st. Human Tissue Authority. 3. Retrieved from https://www.hta.gov.uk/sites/default/files/HTA%20%20Filming%20Guidelines%20-%20Body%20Donation%20%28v1.1%29.pdf. [Google Scholar]
- HTA . 2020a. Anatomy sector guidance human tissue authority. Retrieved from https://www.hta.gov.uk/anatomy-sector-guidance.
- HTA . 2020b. HTA licensing of emergency mortuary facilities human tissue authority. Retrieved from https://www.hta.gov.uk/policies/hta-licensing-emergency-mortuary-facilities.
- Hunter, P. (2019). Remote working in research. EMBO Reports, 20, e47435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Inuwa, I. M. , Taranikanti, V. , Al‐Rawahy, M. , & Habbal, O. (2012). Anatomy practical examinations: How does student performance on computerized evaluation compare with the traditional format? Anatomical Sciences Education, 5, 27–32. [DOI] [PubMed] [Google Scholar]
- Jones, D. G. (2020). Ethical responses to a pandemic: Implications for the ethos and practice of anatomy as a health science discipline. Anatomical Sciences Education, 13, 549–555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Korf, H. W. , Wicht, H. , Snipes, R. L. , Timmermans, J. P. , Paulsen, F. , Rune, G. , & Baumgart‐Vogt, E. (2008). The dissection course: necessary and indispensable for teaching anatomy to medical students. Annals of Anatomy, 190, 16–22. [DOI] [PubMed] [Google Scholar]
- Kumar, G. S. , & Kumar, A. (2019). Building professionalism in human dissection room as a component of hidden curriculum delivery: A systematic review of good practices. Anatomical Sciences Education, 12, 210–221. [DOI] [PubMed] [Google Scholar]
- Langfield, T. , Colthorpe, K. , & Ainscough, L. (2018). Online instructional anatomy videos: Student usage, self‐efficacy, and performance in upper limb regional anatomy assessment. Anatomical Sciences Education, 11, 461–470. [DOI] [PubMed] [Google Scholar]
- Longhurst, G. J. , Stone, D. M. , Dulohery, K. , Scully, D. , Campbell, T. , & Smith, C. F. (2020). Strength, weakness, opportunity, threat (SWOT) analysis of the adaptations to anatomical education in the United Kingdom and Republic of Ireland in response to the Covid‐19 pandemic. Anatomical Sciences Education, 13, 301–311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Macdonald, J. (2020). What do we lose when we can't go to the anatomy lab? Journal of Anatomy, 237, 601–602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mahase, E. (2020). Covid‐19: UKstarts social distancing after new model points to 260 000 potential deaths. BMJ, 368, 1–2. [DOI] [PubMed] [Google Scholar]
- Mahmud, W. , Hyder, O. , Butt, J. , & Aftab, A. (2011). Dissection videos do not improve anatomy examination scores. Anatomical Sciences Education, 4, 16–21. [DOI] [PubMed] [Google Scholar]
- Mandernach, B. J. (2009). Effect of instructor‐personalized multimedia in the online classroom. International Review of Research in Open and Distance Learning, 10, 605. [Google Scholar]
- Martin, F. , & Bolliger, D. U. (2018). Engagement matters: Student perceptions on the importance of engagement strategies in the online learning environment. Online Learning Journal, 22, 205–222. [Google Scholar]
- Mathiowetz, V. , Yu, C.‐H. , & Quake‐Rapp, C. (2016). Comparison of a gross anatomy laboratory to online anatomy software for teaching anatomy. Anatomical Sciences Education, 9, 52–59. [DOI] [PubMed] [Google Scholar]
- McNulty, J. A. , Espiritu, B. , Halsey, M. , & Mendez, M. (2006). Personality preference influences medical student use of specific computer‐aided instruction (CAI). BMC Medical Education, 6, 1–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meng, L. , Hua, F. , & Bian, Z. (2020). Coronavirus disease 2019 (COVID‐19): emerging and future challenges for dental and Oral medicine. Journal of Dental Research, 99, 481–487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mooney, C. J. , Peyre, S. E. , Clark, N. S. , & Nofziger, A. C. (2020). Rapid transition to online assessment: Practical steps and unanticipated advantages. Medical Education, 54, 857–858. [DOI] [PubMed] [Google Scholar]
- Moore, M. G. (1989). Three types of interactions. American Journal of Distance Education, 3, 1–7. [Google Scholar]
- Mustafa, A. G. , Taha, N. R. , Alshboul, O. A. , Alsalem, M. , & Malki, M. I. (2020). Using YouTube to learn anatomy: Perspectives of Jordanian medical students. BioMed Research International, 2020, 1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Naidoo, N. , Akhras, A. , & Banerjee . (2020). Confronting the challenges of anatomy education in a competency‐based medical curriculum during Normal and unprecedented times (COVID‐19 pandemic): Pedagogical framework development and implementation. JMIR Medical Education, 6, e21701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Okafor, I. A. , & Chia, T. (2020). Covid‐19: Covid‐19: Emerging considerations for body sourcing and Handling.A perspective view from Nigeria. Anatomical Sciences Education, 14, 154–162. [DOI] [PubMed] [Google Scholar]
- Parker K, Lenhart A, Moore K. (2011). The digital revolution and higher education. Pew Internet. Retrieved from http://www.pewinternet.org/2011/08/28/the-digital-revolution-and-higher-education [Google Scholar]
- Pather, N. , Blyth, P. , Chapman, J. A. , Dayal, M. R. , Flack, N. A. M. S. , Fogg, Q. A. , Green, R. A. , Hulme, A. K. , Johnson, I. P. , Meyer, A. J. , Morley, J. W. , Shortland, P. J. , Štrkalj, G. , Štrkalj, M. , Valter, K. , Webb, A. L. , Woodley, S. J. , & Lazarus, M. D. (2020). Forced disruption of anatomy education in Australia and New Zealand: An acute response to the Covid‐19 pandemic. Anatomical Sciences Education, 13, 284–300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patil, N. G. , & Chan Ho Yan, Y. (2003). SARS and its effect on medical education in Hong Kong. Medical Education, 37, 1127–1128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patra, A. , Chaudhary, P. , & Ravi, K. S. (2021). Adverse impact of Covid‐19 on anatomical sciences teachers of India and proposed ways to handle this predicament. Anatomical Sciences Education, 14(2), 163–165. [DOI] [PubMed] [Google Scholar]
- QAA . 2018. UKquality code, advice and guidance: Assessment. UK Standing committee for Higher Education. Retrieved from https://www.qaa.ac.uk/quality-code/advice-and-guidance/assessment.
- QAA . 2020. Covid‐19 supporting resources. Quality Assurance Agency for Higher Education. Retrieved from https://www.qaa.ac.uk/news-events/news/qaa-publishes-guidance-on-assessing-with-integrity-in-digital-delivery.
- Ragusa, A. T. , & Crampton, A. (2018). Sense of connection, identity and academic success in distance education: Sociologically exploring online learning environments. Rural Society, 27, 125–142. [Google Scholar]
- Ravi, K. S. (2020). Dead body Management in Times of Covid‐19 and its potential impact on the availability of cadavers for medical education in India. Anatomical Sciences Education, 13, 313–314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reid, M. D. , & Sam, A. H. (2020). Reflections on assessment in the wake of change from the COVID‐19 pandemic. Medical Education, 55, 128–130. [DOI] [PubMed] [Google Scholar]
- Rovai, A. P. (2002). Development of an instrument to measure classroom community. The Internet and Higher Education, 5, 197–211. [Google Scholar]
- Sam, A. H. , Reid, M. D. , & Amin, A. (2020). High‐stakes remote‐access open‐book examinations. Medical Education, 54, 767–768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saxena, V. , Natarajan, P. , O'Sullivan, P. S. , & Jain, S. (2008). Effect of the use of instructional anatomy videos on student performance. Anatomical Sciences Education, 1, 159–165. [DOI] [PubMed] [Google Scholar]
- Schubert, S. , Schnabel, K. P. , & Winkelmann, A. (2009). Assessment of spatial anatomical knowledge with a 'three‐dimensional multiple choice test' (3D‐MC). Medical Teacher, 31, e13–e17. [DOI] [PubMed] [Google Scholar]
- Shepherd‐Banigan, M. , Bell, J. F. , Basu, A. , Booth‐LaForce, C. , & Harris, J. R. (2015). Workplace stress and working from home influence depressive symptoms among employed women with young children. International Journal of Behavioral Medicine, 23, 102–111. [DOI] [PubMed] [Google Scholar]
- Smith, C. F. , & Mathias, H. S. (2009). Medical students' approaches to learning anatomy: Students' experiences and relations to the learning environment. Clinical Anatomy, 23, 106–114. [DOI] [PubMed] [Google Scholar]
- Smith, C. F. , Martinez‐Álvarez, C. , & McHanwell, S. (2014). The context of learning anatomy: Does it make a difference? Journal of Anatomy, 224, 270–278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Souza, A. D. , Kotian, S. R. , Pandey, A. K. , Rao, P. , & Kalthur, S. G. (2020). Cadaver as a first teacher: A module to learn the ethics and values of cadaveric dissection. Journal of Taibah University Medical Science, 15, 94–101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Srinivasan, D. K. (2020). Medical students' perceptions and an anatomy teacher's personal experience using an e‐learning platform for tutorials during the Covid‐19 crisis. Anatomical Sciences Education, 13, 318–319. [DOI] [PubMed] [Google Scholar]
- Triepels, C. P. , Smeets, C. F. , Notten, K. J. , Kruitwagen, R. , Futterer, J. J. , Vergeldt, T. F. , & Van Kuijk, S. M. (2020). Does three‐dimensional anatomy improve student understanding? Clinical Anatomy, 33, 25–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tucker, R. P. , & Anderson . (2020). Dissection experience and performance on a human gross anatomy written examination: Lessons learned during the Covid‐19 pandemic. Anatomical Sciences Education, 14(2), 169–170. [DOI] [PubMed] [Google Scholar]
- UNESCO . 2020. School closures caused by coronavirus (Covid‐19). Retrieved from https://en.unesco.org/covid19/educationresponse.
- Walker, D. J. , Topping, K. , & Rodrigues, S. (2008). Student reflections on formative e‐assessment: Expectations and perceptions. Learning, Media and Technology, 33, 221–234. [Google Scholar]
- Watermeyer, R. , Crick, T. , & Knight, G. J. (2020). COVID‐19 and digital disruption in UK universities: afflictions and affordances of emergency online migration. Higher Education. 81, 623–641. 10.1007/s10734-020-00561-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Willan, J. , King, A. J. , Jeffery, K. , & Bienz, N. (2020). Challenges for NHS hospitals during covid‐19 epidemic. BMJ, 368, 1–2. [DOI] [PubMed] [Google Scholar]
- Wimpenny, K. , & Savin‐Baden, M. (2013). Alienation, agency and authenticity: A synthesis of the literature on student engagement. Teaching in Higher Education, 18, 311–326. [Google Scholar]
- World Health Organization . 2019. Burn‐out an “occupational phenomenon”: International classification of diseases. Retrieved from https://www.who.int/mental_health/evidence/burn-out/en.
- Yammine, K. , & Violato, C. (2015). A meta‐analysis of the educational effectiveness of three‐dimensional visualization technologies in teaching anatomy. Anatomical Sciences Education, 8, 525–538. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
DATA S1: Supporting Information