

Abstract
Background:
Deloyers procedure enables anastomosis of the ascending colon to the rectum following extended resections that prevent usual fashion anastomosis. During the procedure, the right colon is completely mobilized and counterclockwise rotated to allow tension free and well-vascularized anastomosis while preserving the ileocecal valve. The purpose of this manuscript is to report our experience with laparoscopic Deloyers procedure in a hostile abdomen due to adhesions from previous surgeries.
Methods:
We report the outcomes and our technique of laparoscopic Deloyers procedure in three patients. All patients had a surgical complication necessitating the creation of end colostomy with a short colonic remnant. The bowel status prevented restoration of continuity by the common colorectal anastomosis and laparoscopic Deloyers was elected.
Results:
The procedure was successful in all patients, with no intra-operative complication and average surgery duration of three hours. Patients had uneventful postoperative recovery with only one case of minor complication and an adequate functional outcome.
Conclusion:
Laparoscopic Deloyers is safe and allows the restoration of bowel continuity with preservation of ileocecal valve and good functional outcome even in hostile abdomen.
Keywords: Deloyers procedure, Right colon transposition, Flip flop procedure, Laparoscopic surgery
INTRODUCTION
Deloyers procedure was developed as an alternative to ileorectal anastomosis when only a short colonic segment is available for restoration of bowel continuity. It involves the creation of anastomosis between the right or transverse colon and the rectum. It requires complete mobilization of the right colon with counterclockwise rotation while preserving the ileocolic pedicle. This operation enables a safe, tension-free, colorectal anastomosis in circumstances where the remnant colonic length does not allow for a regular fashion anastomosis.
Deloyers operation may be indicated during the primary operation of an extended left hemicolectomy or as a restoring procedure following an urgent colostomy with a short segment of the remaining colon.
Previous publications, depicting the laparoscopic technique, focused on Deloyers operation performed at the primary operation in a nonhostile abdomen. In our paper, we report 3 cases of a restoring laparoscopic Deloyers operation following complications of previous surgeries.
PATIENTS AND METHODS
Between 2014 and 2020, the senior author (D.H.), a minimally invasive colorectal surgeon (50 cases per year), performed three restoring laparoscopic Deloyers operations following complications of previous surgeries. Patient demographics are reported in Table 1.
Table 1.
Patients Demographics at the Time of Deloyers Operation
| Gender | Age | Comorbidities | BMI | Asa | Duration of Surgery (minutes) | |
|---|---|---|---|---|---|---|
| Patient 1 | Male | 67 | Hypertension, gout, heavy smoker | 29 | 3 | 187 |
| Patient 2 | Female | 71 | Hypertension, diabetes mellitus, chronic renal failure | 24 | 3 | 205 |
| Patient 3 | Male | 76 | Hypertension, osteoporosis, hyperlipidemia, gastroesophageal reflux disease | 23 | 3 | 169 |
Patient 1, a 67-year-old male, underwent laparoscopic Hartmann’s procedure following perforated diverticulitis on 7/2014. Laparoscopic reversal of Hatrman was carried out on 11/2014. On post-operative day (POD) 5 the patient was diagnosed with anastomotic leak and taken to the operating room (OR) for laparoscopic take down of the anastomosis and end colostomy. The remaining colon segment was too short for regular fashion reanastomosis. The restoring laparoscopic Deloyers procedure with intraperitoneal anastomosis took place on 4/2015, duration of the surgery was 187 minutes and was uneventful. The return of bowel function was reported on POD#2 and the patient was discharged on POD#5. On the post-operative period, surgical site infection at the colostomy closure site was diagnosed and treated with drainage and PO antibiotics. At 6 months after surgery the patient reported an average of 5 bowel movements per day.
Patient 2, a 71-year-old female, underwent an open extended left hemicolectomy with colorectal anastomosis on 2/2016 due to synchronous tumors at the height of 25 cm and 45 cm from the anus. On POD#5 she was diagnosed with anastomotic leak and taken to the OR for take down of the anastomosis and end colostomy. The remaining colon segment was too short for regular fashion reanastomosis. The restoring laparoscopic Deloyers procedure with intraperitoneal anastomosis took place on 7/2016, duration of surgery was 205 minutes and was uneventful. The return of bowel function was reported on POD#3 and the patient was discharged on POD#6 with no early post-operative complications. At 6 months after surgery the patient reported an average of 5 bowel movements per day.
Patient 3, a 76-year old male, underwent laparoscopic extended left hemicolectomy with colorectal anastomosis for splenic flexure adenocarcinoma on 10/2019. On POD#10 he was diagnosed with delayed anastomotic leak and taken to the OR for laparoscopic take down of anastomosis and end colostomy. The restoring laparoscopic Deloyers procedure with intraperitoneal anastomosis took place on 2/2020, duration of surgery was 169 minutes and was uneventful. The return of bowel function was reported on POD#3 and the patient was discharged on POD#5 with no early post-operative complications. At 6 months after surgery the patient reported an average of 5 bowel movements per day. Gastrografin enema 6 months following surgery is shown in Figure 1.
Figure 1.

A gastrografin enema of patient #3 at six months after surgery. The anastomosis is marked with red arrow. Transition of contrast to the small bowel can be seen in the right upper quadrant.
SURGICAL TECHNIQUE
Prior to surgery, careful review of previous operative notes and all available imaging studies along with meticulous physical examination is necessary for optimal surgical planning.
Patients were positioned in a low lithotomy position. In cases of anticipated adhesions from previous laparotomies, a Veress needle in Palmer's point was used to insufflate the abdomen. Then, a 5 mm camera was inserted with a 5 mm optical trocar. Additional 5 mm trocars were inserted and adhesiolysis was performed. In cases where less adhesions were anticipated, following laparoscopic surgeries, the colostomy site was used for access. The colostomy was sewed with a running suture and dissected off the abdominal wall in the usual fashion. A 15 mm trocar was inserted and secured through the ostomy opening and the abdomen insufflated to 15 mmHg. Additional three 5 mm trocars were placed in LUQ, LLQ, and RUQ.
The gastro-colic ligament was incised near the transverse colon and complete mobilization of the transverse colon including the hepatic flexure was carried out. The midcolic artery was identified, dissected out, and sealed at its origin with a bipolar energy device (LigaSure™, Medtronic) (Figure 2). A lateral to medial mobilization of the cecum and ascending colon with preservation of the ileocolic pedicle was done. On the lateral side, careful attention to working in the avascular plane along the Toldt line between the mesocolon and retroperitoneum was given. Following the complete mobilization of the right colon, an appendectomy was performed in the standard fashion, controlling the mesoappendix with an energy device and removing the appendix with a stapling device (Endo GIA™, Medtronic, 45 mm, purple load) (Figure 3).
Figure 2.

Following transverse colon mobilization and midcolic ligation. The midcolic stump is marked with red arrow.
Figure 3.

The appendiceal stump (blue asterisk) at the base of the cecum is seen at the right upper quadrant next to the gallbladder (green asterisk).
A colotomy of the transverse colon was made and the anvil of a circular stapler (EEA™ Circular Stapler, Medtronic 28 mm) was introduced. The distal transverse colon was resected using a stapling device (Endo GIA™, Medtronic, 80 mm, purple load) at the demarcation line. The shaft of the anvil was projected through the staple line. Afterwards, the colon was rotated counterclockwise (sagittal plane), directing the cecum cranially and the ascending colon caudally. Thorough examination of the bowel and colon position was performed to avoid twists and confirmation of the desired counterclockwise orientation. The bowel continuity was achieved by forming an end to end colorectal anastomosis with the circular stapler (Figure 4). Illustration of the procedure is shown in Figure 5.
Figure 4.
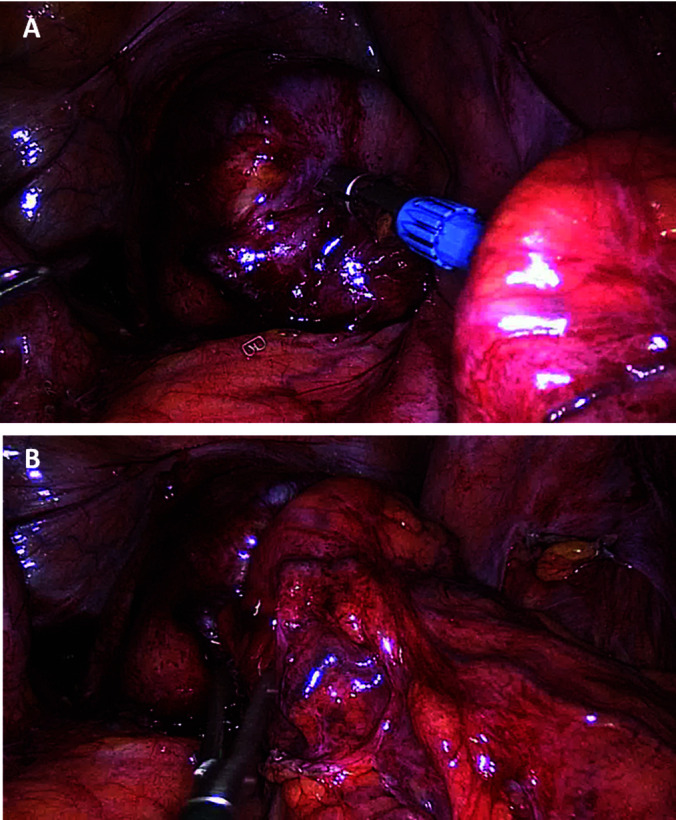
Preparation (A) and completion (B) of colorectal anastomosis.
Figure 5.

Schematic illustration of the Deloyers procedure following previous surgeries. The preoperative state with the mid-transverse colon supplied by the mid-colic vessels is shown in A. Ligation of the mid-colic vessels, subsequently, resection of the ischemic transverse colon and appendectomy is shown in B. The ascending colon facing down after counterclockwise rotation (sagittal plane) prior to stapled colo-rectal anastomosis is shown in C.
DISCUSSION
Our case series shows the safety and feasibility of laparoscopic Deloyers procedure despite a hostile abdomen with adhesions following complications of previous surgeries.
Deloyers procedure was developed to achieve better functional outcome after more extensive resections. Potential benefits include preservation of the ileocecal valve, longer segments of functioning large bowel, and possible lower rate of anastomotic leak compared to ileo-rectal anastomosis.1 Preserving the terminal ileum and the ileocecal valve has a physiological benefit of preventing small bowel bacterial overgrowth,2 better water and sodium absorption, altogether allowing better stool consistency.3
Since the original report by Deloyers4 several groups reported their experience and outcomes of this procedure. The largest, by Manceau et al.5 reported the outcomes of 48 patients who underwent open Deloyers procedure mainly during Hartmann reversal and following complications of previous colorectal anastomosis. They reported early complications rate of 23% with no anastomotic leaks and good functional outcome on long-term follow up with an average of 4 bowel movements per day. The first laparoscopic Deloyers procedure was published in 2016.6 Sciuto et al.7 shared their experience of laparoscopic Deloyers performed in 10 patients, mostly during elective primary extended left hemicolectomy. They had 10% leak rate with no postoperative mortality. Functional outcome was similar to those previously reported.8 A recent study9 described single port laparoscopic Deloyers in 6 patients with an average operating time of nearly six hours. Their technique differed by using only a short segment of ascending colon for reconstruction. The complication rate was 50% with no anastomotic leak. The final outcome was encouraging with good functional outcome and solid stool consistency.
Our report focuses on laparoscopic Deloyers as a salvage procedure following previous surgical complications. Despite being technically demanding, particularly in a hostile abdomen following complications of previous operations, we were able to reproduce previous results of other groups with no anastomotic leak and only one minor complication, the average duration of surgery was three hours only.
Deloyers procedure is rarely indicated, nevertheless, it must be in the armamentarium of minimally invasive colorectal surgeons. It allows the restoration of bowel continuity with low tension anastomosis while preserving the ileocecal valve in cases otherwise calling for ileorectal anastomosis. While performing this uncommon procedure it is important to avoid the potential pitfalls mentioned above and specifically, preservation of the ileocolic pedicle, confirming the viability of the distal colonic segment after ligation of the midcolic vessels, attention while performing the bowel rotation at the counterclockwise direction, avoiding excessive tension on the anastomosis and blood vessels. The importance of preventive appendectomy should not be overlooked.
CONCLUSION
In our modest experience, laparoscopic Deloyers is safe and feasible. When performed by a experienced minimally invasive colorectal surgeon. Low morbidity and good functional outcome can be anticipated, even in challenging circumstances following complications of previous surgeries.
Footnotes
Conflicts of Interest: The authors declare no conflict of interest regarding the publication of this article.
Disclosure: none.
Informed consent: Dr. Dux declares that written informed consent was obtained from the patient’s for publication of this study/report and any accompanying images.
Contributor Information
Joseph Dux, Department of General and Oncological Surgery—Surgery C, Sheba Medical Center, Tel Hashomer, Israel..
Ephraim Katz, Department of General and Oncological Surgery—Surgery C, Sheba Medical Center, Tel Hashomer, Israel..
Mohammad Adileh, Department of General and Oncological Surgery—Surgery C, Sheba Medical Center, Tel Hashomer, Israel..
Lior Segev, Department of General and Oncological Surgery—Surgery C, Sheba Medical Center, Tel Hashomer, Israel..
David Hazzan, Department of General and Oncological Surgery—Surgery C, Sheba Medical Center, Tel Hashomer, Israel..
References:
- 1.Jouvin I, Pocard M, Najah H. Deloyers procedure. J Visc Surg. 2018;155(6):493–501. [DOI] [PubMed] [Google Scholar]
- 2.Bertelsen CA, Larsen HM, Neuenschwander AU, Laurberg S, Kristensen B, Emmertsen KJ. Long-term functional outcome after right-sided complete mesocolic excision compared with conventional colon cancer surgery: a population-based questionnaire study. Dis Colon Rectum. 2018;61(9):1063–1072. [DOI] [PubMed] [Google Scholar]
- 3.Costalat G, Garrigues JM, Didelot JM, Yousfi A, Boccasanta P. Subtotal colectomy with ceco-rectal anastomosis (Deloyers) for severe idiopathic constipation: an alternative to total colectomy reducing risks of digestive sequelae. Ann Chir. 1997;51(3):248–255. [PubMed] [Google Scholar]
- 4.Deloyers L. Suspension of the right colon permits without exception preservation of the anal sphincter after extensive colectomy of the transverse and left colon (including rectum): technic indications immediate and late results. Lyon Chir. 1964;60:404–413. [PubMed] [Google Scholar]
- 5.Manceau G, Karoui M, Breton S, Blanchet AS, Rousseau G, Savier E, Siksik JM, Vaillant JC, Hannoun L. Right colon to rectal anastomosis (Deloyers procedure) as a salvage technique for low colorectal or coloanal anastomosis: postoperative and long-term outcomes. Dis Colon Rectum. 2012;55(3):363–368. [DOI] [PubMed] [Google Scholar]
- 6.Antona AD, Reggio S, Pirozzi F, Corcione F. Laparoscopic 3D high-definition Deloyers procedure: when, how, why? Updates Surg. 2016;68(1):111–113. [DOI] [PubMed] [Google Scholar]
- 7.Sciuto A, Grifasi C, Pirozzi F, Leon P, Pirozzi REM, Corcione F. Laparoscopic Deloyers procedure for tension-free anastomosis after extended left colectomy: technique and results. Tech Coloproctol. 2016;20(12):865–869. [DOI] [PubMed] [Google Scholar]
- 8.Kontovounisios C, Baloyiannis Y, Kinross J, Tan E, Rasheed S, Tekkis P. Modified right colon inversion technique as a salvage procedure for colorectal or coloanal anastomosis. Colorectal Dis. 2014;16(12):971–975. [DOI] [PubMed] [Google Scholar]
- 9.Choi BJ, Kwon W, Baek SH, Jeong WJ, Lee SC. Single-port laparoscopic Deloyers procedure for tension-free anastomosis after extended left colectomy or subtotal colectomy: A 6-patient case series. Medicine (Baltimore). 2020;99(31):e21421. [DOI] [PMC free article] [PubMed] [Google Scholar]