

Abstract
Background
Child marriage is a major public health problem globally, and the prevalence remains high in sub-Saharan African countries, including Mali. There is a dearth of evidence about factors associated with child marriage in Mali. Hence, this studyaimed at investigating the individual/household and community-level factors associated with child marriage among women in Mali.
Methods
Using data from the 2018 Mali Demographic and Health Survey, analysis was done on 8,350 women aged 18-49 years. A Chi-square test was used to select candidate variables for the multilevel multivariable logistic regression models. Fixed effects results weree xpressed as adjusted odds ratios (aOR) at 95% confidence intervals (CI). Stata version 14 software was used for the analysis.
Results
The results showed that 58.2% (95% CI; 56.3%-60.0%) and 20.3% (95%; 19.0%-21.6%) of women aged 18-49 years were married before their 18th and 15th birthday, respectively. Educational status of women (higher education: aOR = 0.25, 95% CI; 0.14-0.44), their partner's/husband's educational status (higher education: aOR = 0.64, 95% CI; 0.47-0.87), women's occupation (professional, technical, or managerial: aOR = 0.50, 95% CI; 0.33-0.77), family size (five and above: aOR = 1.16, 95% CI; 1.03-1.30), and ethnicity (Senoufo/Minianka: aOR = 0.73, 95% CI; 0.58-0.92) were the identified individual/household level factors associated with child marriage, whereas region (Mopti: aOR = 0.27, 95% CI; 0.19-0.39) was the community level factor associated with child marriage.
Conclusions
This study has revealed a high prevalence of child marriage in Mali. To reduce the magnitude of child marriage in Mali, enhancing policies and programs that promote education for both girls and boys, creating employment opportunities, improving the utilization of family planning services, and sensitizing girls and parents who live in regions such as Kayes on the negative effects of child marriage is essential. Moreover, working with community leaders so as to reduce child marriage in the Bambara ethnic communities would also be beneficial.
1. Background
Child marriage, i.e., marriage before the age of 18 is a violation of human rights and a major public health problem globally [1–3]. Worldwide, nearly 21% of young women are married before their 18th birthday, and 650 million girls and women alive today were married as children [4]. Each year, 12 million girls younger than 18 years are married [5]. Low- and middle-income countries (LMICs) particularly in South Asia and sub-Saharan Africa (SSA) account for the highest proportion of child marriage [6]. SSA alone accounts for 37% of the global burden of child marriage [2, 7]. The problem is compounded by pervasive social norms [8]. One in three girls and one in nine girls are married before the age of 18 and 15, respectively, in LMICs [9, 10].
Child marriage has several adverse consequences for girls' physical, mental, and social health and wellbeing [10–12]. It endangers girls' physical and emotional welfare by prematurely pressurizing them into sexual activity, which is a form of systematic sexual violence [13]. The victims of child marriage lack the power or autonomy to negotiate safer sex practices with their spouses [14]. For instance, they may not be able to ask their husband to have an HIV test, use condom, abstain from intercourse, and cannot demand that their husbands be faithful [15, 16]. As a result, they are at increased risk of HIV infection [17]. Although ending child marriage is one of the targets of the Sustainable Development Goals (SDGs), so far, the investments toward this target remain inadequate [18].
Mali is one of the countries in the world with the highest prevalence of early marriage and the most severe child marriage crises [10, 19, 20]. The country has been implementing child marriage prevention interventions as one of the national development agenda strategies [21]. According to the 2010 Mali Multiple Indicator Cluster Survey (MICS) report [22], the prevalence of early marriage was 55%, which was higher than the 37% regional average for SSA in the same year [10]. Previous reports in Mali indicate that 54% of girls are married before they turn 18 years and 16% are married before their 15th birthday [23]. The legal age for marriage in Mali is 18 and 21 years for girls and boys, respectively [10, 19, 20].
Several studies in LMICs suggest that girls and their parents' educational status, household economic status, religion, place of residence, family size, ethnicity, and region are determinants of child marriage [24–26]. Although a few studies in Mali showed that child marriage vary based on education and economic status, place of residence, and across regions [10, 23], comprehensive assessments of factors that affect child marriage in the country are scarce. Hence, this study is aimed at investigating individual/household and community-level factors associated with child marriage using data from the most recent Mali demographic and health survey (DHS). The findings from this study would have practical contribution for the country for the reduction of child marriage. This includes policy makers and programmers can target or consider those clearly identified recent and different level factors during designing and implementing interventions so as to achieve a significant reduction of child marriage in Mali.
2. Methods
2.1. Data Source
For the analysis of this study, we extracted data from the 2018 Mali DHS, which is the sixth DHS since 1987. It is a nationally representative survey designed to provide reliable data for monitoring of demographic and health indicators, including child marriage in the country. It was implemented by l'Institut National de la Statistique (INSTAT) with the financial and technical support of United States Aid for Internal Development (USAID) and Inner-city Fund (ICF) International [27]. The 2018 Mali DHS applied a two-stage stratified cluster sampling technique, which provides reliable estimates of population indicators at national and subnational levels. However, in the Kidal region, only the urban region was surveyed due to security concerns [27]. In the first stage, Enumeration Areas (EA) were selected systematically with Probability Proportional to Size (PPS) in the 2009 Mali population census, and in the second stage, a fixed number of households, usually 25-30 households, are selected from selected EA using a systematic random sampling technique. The survey included 10,519 women in the reproductive age groups (15-49 years) and 4,618 men aged between 15 and 59 years, with a 98% and 96% response rate, respectively. For this study, we included 8,350 women aged 18-49 years.
2.2. Study Variables
2.2.1. Outcome Variable
The outcome variable for this study was child marriage, defined as young girls married before their 18th birthday [1–5]. The outcome variable was dichotomized and coded as “yes” if the age at first marriage among the women occurred before their 18th birthday and “no” if the first marriage was at 18 years and above.
2.2.2. Explanatory Variables
Based on the findings of previous studies on child marriage [10, 24, 26, 28–34], the following individual/household and community level explanatory variables were included in the analysis.
2.2.3. Individual/Household Level Factors
Individual/household level factors included women's educational status (no formal education, primary school, secondary school, and higher), partner/husband's educational status (no formal education, primary school, secondary school, and higher), women's occupation (not working, professional/technical or managerial, sales, agricultural self-employed, services, and others), partner/husband occupation (not working, professional/technical or managerial, sales, agricultural self-employed, services, and others), religion (Muslim and others), family size (<5 and 5+), and ethnicity (Bambara, Malinke, Peulh, Sarakole/Soninke/Marka, Sonrae, Dogon, Touareg/Bella, Senoufo/Minianka, Other Malian, and others). Economic status was proxied through a wealth index in the DHS computed using household assets and ownerships using principal component analysis (PCA). Detailed explanation can be found elsewhere [35] and was classified to poorest, poorer, middle, richer, and richest. Media exposure was coded as “yes” if the married woman has exposure for either of the three media sources (newspaper, radio, and television) for at least less than once a week and “no” if otherwise.
2.2.4. Community Level Factors
Community-level factors included place of residence (urban and rural), distance to health facility (big problem and not a big problem), region (Kayes, Koulikoro, Sikasso, Segou, Mopti, Toumbouctou, Gao, Kidal, and Bamako), community literacy level (low, medium, and high), and community socioeconomic status (low, moderate, and high). Community socioeconomic status was computed from occupation, wealth, and education of women who resided in a given community. We applied principal component analysis to calculate women who were unemployed, uneducated, and poor. A standardized score was derived with a mean score (0) and standard deviation [1]. The scores were then segregated into tertile 1 (least disadvantaged), tertile 2, and tertile 3 (most disadvantaged) where the least score (tertile 1) denoted greater socioeconomic status with the highest score (tertile 3) denoting lower socioeconomic status. Community literacy level was derived from women who could read and write (or not read and write) at all.
2.2.5. Statistical Analyses
Descriptive analysis including frequency distribution of respondents and prevalence of child marriage was done. Then, bivariate analysis (chi-square test) was conducted to select candidate explanatory variables using P value less than 0.05 as a cut point. Multicolliniarity test was done among all explanatory variables that had a significant association with child marriage using variance inflation factor (VIF), and the result confirmed that there was no evidence of collinearity among the explanatory variables (Mean VIF = 1.81, Min VIF = 1.01, and Max VIF = 4.13). Evidence shows VIF less than 10 are tolerable [36].
Finally, multilevel multivariable logistic regression was conducted, and four models were constructed to assess the association between individual/household and community level factors and child marriage. The first model was Model 0 which is also called an empty model that ascertained whether or not the outcome variable (child marriage) varied across enumeration areas, also known as primary sampling unit (PSU). The second model (Model I) was constructed to examine the association between child marriage and individual/household level factors. The third model (Model II) was constructed to examine the relationships between community-level factors and child marriage. The final model (Model III) was the complete model that combined both individual/household and community level factors.
The multilevel logistic regression analysis included both fixed and random effects [37–39]. The fixed effects (measures of association) examined associations between explanatory variables and child marriage and were reported using adjusted odds ratio at 95% confidence interval, whereas the random effect assessed variation of child marriage across clusters and was expressed using intraclass-correlation (ICC) [40]. Model adequacy was checked using Likelihood Ratio (LR), and Akaike information criterion (AIC) was used to measure how well the model was fitted [41]. The analysis was carried out using Stata version-14 (Stata Corporation, College Station, TX, USA) software. Sampling weight and “svy” command were applied to correct under- and oversampling and to account for the complex survey design of DHS, respectively.
2.2.6. Ethical Consideration
The analysis was based on publicly available DHS data. Since the ethical clearance was the responsibility of the institution that commissioned, funded, and managed the survey, and further ethical clearance was not required for this study. ICF international and Mali l'Institut National de la Statistique (INSTAT) ensured that the 2018 Mali DHS was conducted in compliance with the national ethical guidelines and U.S. Department of Health and Human Services regulations for the protection of the right of human subjects. More details about data and ethical standards are available at: http://goo.gl/ny8T6X.
3. Results
3.1. Prevalence of Child Marriage
As illustrated in Figure 1, about 58.2% (95% CI; 56.3%-60.0%) of women were first married before they were 18 years old, and nearly 20.3% (95%; 19.0%-21.6%) of the women married before their 15th birthday.
Figure 1.
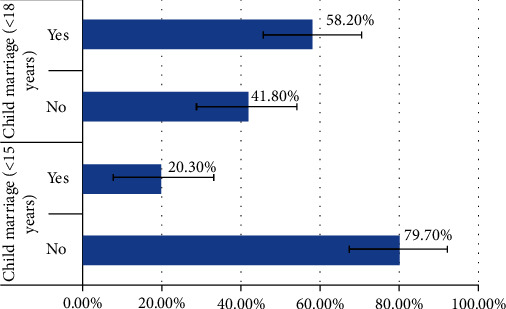
Prevalence of child marriage among women aged 18-49 years: evidence from 2018 Mali demographic and health survey.
Table 1 shows the differences in the prevalence of child marriage across various population sub-groups. In this study, a total of 8,350 women aged 18-49 years were included. Among them, about 68.4% of the participants and nearly three-fourths (73.8%) of their husbands had no formal education. Nearly three-fourths (74%) of the respondents were rural residents, and majority (81.2%) were exposed to either newspaper, radio, or television for at least less than once a week. Nearly two-fifths (39.4%) and one-fourth (25.4%) of the women were either not working or were self-employed in agricultural work, respectively. We found about 49.3% difference in the prevalence of child marriage across educational subgroups, ranging from 62.0% among women who had no formal education to 12.7% among women who had had higher education. The prevalence also varied based on women's occupation types, from 69.1% among women self-employed in agriculture, 55.9% in women who were not working, to 19.7% among women in professional, technical, or managerial occupational groups. About 61.9% of rural women had experienced child marriage, while the proportion was 45.9% among their urban counterparts. There were regional disparities in the prevalence of early marriage. This study shows the lowest prevalence of child marriage (41.3%) in Bamako region, and higher proportions of child marriage were observed in Kayes (76.7%), Toumbouctou (65.1%), and Koulikoro (63.7%) regions, respectively (Table 1).
Table 1.
Prevalence of child marriage across explanatory variables: evidence from 2018 Mali demographic and health survey.
| Variable | Number (weighted %) | Child marriage (weighted %) | Chi-square, P value | |
|---|---|---|---|---|
| No | Yes | |||
| Overall prevalence | 8,350 (58.18) | NA | NA | |
| Women's educational level | χ 2 = 296.68, P < 0.001 | |||
| No formal education | 6,375 (68.41) | 38.0 | 62.0 | |
| Primary school | 1,108 (12.07) | 38.9 | 61.1 | |
| Secondary school | 1,559 (17.17) | 58.8 | 41.2 | |
| Higher | 203 (2.35) | 87.3 | 12.7 | |
| Husband educational level | χ 2 = 212.24, P < 0.001 | |||
| No formal education | 5,711 (73.81) | 37.5 | 62.5 | |
| Primary school | 700 (9.16) | 42.7 | 57.3 | |
| Secondary school | 954 (12.39) | 52.7 | 47.3 | |
| Higher | 344 (4.65) | 70.6 | 29.4 | |
| Women occupation | χ 2 = 266.71, P < 0.001 | |||
| Not working | 4,305 (39.38) | 44.1 | 55.9 | |
| Professional or technical or managerial | 219 (2.45) | 80.3 | 19.7 | |
| Sales | 2,207 (25.42) | 46.3 | 53.7 | |
| Agricultural self-employed | 1,763 (25.35) | 30.9 | 69.1 | |
| Services | 544 (5.23) | 38.4 | 61.6 | |
| Others | 207 (2.17) | 59.0 | 41.0 | |
| Husband occupation | χ 2 = 129.79, P < 0.001 | |||
| Not working | 732 (8.57) | 40.2 | 59.8 | |
| Professional or technical or managerial | 742 (9.20) | 56.8 | 43.2 | |
| Sales | 1,631 (20.25) | 43.0 | 57.0 | |
| Agricultural self-employed | 2,981 (39.50) | 35.5 | 64.5 | |
| Services | 1,225 (16.22) | 46.4 | 53.6 | |
| Others | 523 (6.26) | 42.0 | 58.0 | |
| Economic status | χ 2 = 244.20, P < 0.001 | |||
| Poorest | 1,653 (17.75) | 39.4 | 60.6 | |
| Poorer | 1,607 (18.66) | 35.2 | 64.8 | |
| Middle | 1,744 (19.27) | 36.5 | 63.5 | |
| Richer | 2,059 (21.14) | 39.5 | 60.5 | |
| Richest | 2,182 (23.18) | 58.1 | 41.9 | |
| Religion | χ 2 = 5.7137, P = 0.1420 | |||
| Muslim | 8,813 (94.02) | 42.2 | 57.8 | |
| Others | 432 (5.98) | 36.7 | 63.3 | |
| Ethnicity | χ 2 = 85.74, P < 0.001 | |||
| Bambara | 2,543 (33.28) | 40.5 | 59.5 | |
| Malinke | 713 (8.91) | 37.2 | 62.8 | |
| Peulh | 1,150 (13.52) | 41.9 | 58.1 | |
| Sarakole/soninke/marka | 747 (10.15) | 33.8 | 66.2 | |
| Sonrae | 1,143 (6.01) | 45.2 | 54.8 | |
| Dogon | 583 (8.77) | 52.3 | 47.7 | |
| Touareg/Bella | 849 (1.78) | 36.8 | 63.2 | |
| Senoufo/minianka | 826 (9.44) | 43.6 | 56.4 | |
| Other Malian | 481 (5.47) | 44.6 | 55.4 | |
| Others | 210 (2.66) | 54.8 | 45.2 | |
| Media exposure | χ 2 = 12.5672, P < 0.01 | |||
| No | 1,869 (18.8) | 38.0 | 62.0 | |
| Yes | 7,376 (81.2) | 42.8 | 57.2 | |
| Family size | χ 2 = 10.8820, P < 0.05 | |||
| <5 | 2,475 (25.62) | 44.8 | 55.2 | |
| 5+ | 6,770 (74.38) | 40.7 | 59.3 | |
| Residence | χ 2 = 158.60, P < 0.001 | |||
| Urban | 3,045 (26.01) | 54.1 | 45.9 | |
| Rural | 6,200 (73.99) | 38.1 | 61.9 | |
| Distance to health facility | χ 2 = 17.1518, P < 0.01 | |||
| Big problem | 2,885 (28.83) | 38.4 | 61.6 | |
| Not a big problem | 6,360 (71.17) | 43.3 | 56.7 | |
| Region | χ 2 = 442.64, P < 0.001 | |||
| Kayes (ref) | 1,149 (14.80) | 23.3 | 76.7 | |
| Koulikoro | 1,250 (19.39) | 36.3 | 63.7 | |
| Sikasso | 1,410 (16.69) | 38.1 | 61.9 | |
| Segou | 1,156 (15.27) | 46.8 | 53.2 | |
| Mopti | 681 (10.29) | 54.6 | 45.4 | |
| Toumbouctou | 886 (3.56) | 34.9 | 65.1 | |
| Gao | 642 (2.78) | 48.1 | 51.9 | |
| Kidal | 580 (0.0009) | 58.1 | 41.9 | |
| Bamako | 1,491 (17.12) | 58.7 | 41.3 | |
| Community literacy level | χ 2 = 244.75, P < 0.001 | |||
| Low (ref) | 3,221 (36.28) | 34.9 | 65.1 | |
| Medium | 2,991 (30.43) | 38.2 | 61.8 | |
| High | 3,033 (33.30) | 54.5 | 45.5 | |
| Community socioeconomic status | χ 2 = 245.11, P < 0.001 | |||
| Low (ref) | 5,134 (57.73) | 36.9 | 63.1 | |
| Medium | 1,069 (11.13) | 35.0 | 65.0 | |
| High | 3,042 (31.14) | 55.4 | 44.6 | |
3.2. Fixed Effects (Measures of Association)
3.3. Individual/Household Level Factors
The results in Table 2 show lower odds of child marriage among women who had secondary education (aOR = 0.71, 95% CI; 0.60-0.85) and higher education (aOR = 0.25, 95% CI; 0.14-0.44) compared to women who had no formal education. Similarly, we found lower odds of child marriage among women whose husbands had higher education compared to women whose husbands had no formal education (aOR = 0.64, 95% CI; 0.47-0.87). In addition, this study shows higher odds of child marriage among women living in households with large family size compared to women living in households with small family size (aOR = 1.16, 95% CI; 1.03-1.30). The findings indicate that the likelihood of child marriage among women with professional, technical, or managerial occupations (aOR = 0.50, 95% CI; 0.33-0.77) was lower compared to women who were not working. Our findings show that compared to women of Bambara ethnicity, the odds of child marriage were lower among women from Senoufo/Minianka (aOR = 0.73, 95% CI; 0.58-0.92) (Table 2).
Table 2.
Multilevel multivariable results for magnitude and its individual/household and community level factors of child marriage among women aged 18-49 years: evidence from 2018 Mali DHS.
| Variable | Model 0 | Model I | Model II | Model III |
|---|---|---|---|---|
| Women's educational level | ||||
| No formal education (ref) | ||||
| Primary school | 1.05 (0.89-1.23) | 1.02 (0.87-1.20) | ||
| Secondary school | 0.71 (0.60-0.85)∗∗∗ | 0.71 (0.60-0.85)∗∗∗ | ||
| Higher | 0.24 (0.13-0.43)∗∗∗ | 0.25 (0.14-0.44)∗∗∗ | ||
| Husband educational level | ||||
| No formal education (ref) | ||||
| Primary school | 0.93 (0.78-1.11) | 0.94 (0.78-1.12) | ||
| Secondary school | 0.86 (0.72-1.02) | 0.87 (0.73-1.03) | ||
| Higher | 0.63 (0.46-0.86)∗∗ | 0.64 (0.47-0.87)∗∗ | ||
| Women occupation | ||||
| Not working (ref) | ||||
| Professional or technical or managerial | 0.50 (0.33-0.77)∗∗ | 0.50 (0.33-0.77)∗∗ | ||
| Sales | 1.00 (0.87-1.14) | 1.02 (0.90-1.17) | ||
| Agricultural self-employed | 1.33 (1.13-1.56)∗∗ | 1.17 (1.00-1.38) | ||
| Services | 1.14 (0.91-1.44) | 1.10 (0.88-1.38) | ||
| Others | 0.81 (0.53-1.22) | 0.84 (0.55-1.27) | ||
| Husband occupation | ||||
| Not working (ref) | ||||
| Professional or technical or managerial | 1.06 (0.82-1.36) | 1.06 (0.82-1.37) | ||
| Sales | 1.19 (0.97-1.45) | 1.22 (0.99-1.50) | ||
| Agricultural self-employed | 1.11 (0.91-1.34) | 1.12 (0.92-1.35) | ||
| Services | 0.95 (0.77-1.18) | 0.99 (0.80-1.23) | ||
| Others | 1.19 (0.92-1.55) | 1.18 (0.91-1.53) | ||
| Economic status | ||||
| Poorest (ref) | ||||
| Poorer | 1.03 (0.87-1.22) | 1.00 (0.85-1.19) | ||
| Middle | 0.94 (0.79-1.12) | 0.90 (0.76-1.07) | ||
| Richer | 0.94 (0.77-1.14) | 0.98 (0.78-1.22) | ||
| Richest | 0.61 (0.49-0.77)∗∗∗ | 0.80 (0.59-1.08) | ||
| Ethnicity | ||||
| Bambara (ref) | ||||
| Malinke | 1.16 (0.93-1.46) | 0.97 (0.77-1.22) | ||
| Peulh | 1.02 (0.85-1.23) | 1.02 (0.85-1.22) | ||
| Sarakole/soninke/marka | 1.16 (0.92-1.44) | 1.01 (0.80-1.26) | ||
| Sonrae | 0.90 (0.73-1.12) | 1.10 (0.83-1.47) | ||
| Dogon | 0.69 (0.53-0.90)∗∗ | 0.96 (0.72-1.29) | ||
| Touareg/Bella | 0.77 (0.59-0.99)∗ | 1.01 (0.71-1.43) | ||
| Senoufo/minianka | 0.73 (0.59-0.92)∗∗ | 0.73 (0.58-0.92)∗∗ | ||
| Other Malian | 0.88 (0.68-1.13) | 0.90 (0.70-1.15) | ||
| Others | 0.61 (0.41-0.91)∗ | 0.72 (0.50-1.06) | ||
| Media exposure | ||||
| No (ref) | ||||
| Yes | 1.11 (0.97-1.26) | 1.13 (1.00-1.29) | ||
| Family size | ||||
| <5 (ref) | ||||
| 5+ | 1.14 (1.02 − 1.28)∗ | 1.16 (1.03-1.30)∗∗ | ||
| Residence | ||||
| Urban (ref) | ||||
| Rural | 0.91 (0.70-1.17) | 0.95 (0.72-1.25) | ||
| Distance to health facility | ||||
| Big problem (ref) | ||||
| Not a big problem | 0.90 (0.81-1.01) | 0.93 (0.83-1.05) | ||
| Region | ||||
| Kayes (ref) | ||||
| Koulikoro | 0.65 (0.50-0.83)∗∗ | 0.68 (0.52-0.90)∗∗ | ||
| Sikasso | 0.51 (0.40-0.66)∗∗∗ | 0.59 (0.44-0.78)∗∗∗ | ||
| Segou | 0.37 (0.29-0.48)∗∗∗ | 0.39 (0.29-0.51)∗∗∗ | ||
| Mopti | 0.28 (0.21-0.37)∗∗∗ | 0.27 (0.19-0.39)∗∗∗ | ||
| Toumbouctou | 0.53 (0.40-0.71)∗∗∗ | 0.50 (0.35-0.72)∗∗∗ | ||
| Gao | 0.35 (0.25-0.47)∗∗∗ | 0.33 (0.22-0.50)∗∗∗ | ||
| Kidal | 0.24 (0.16-0.35)∗∗∗ | 0.30 (0.17-0.50)∗∗∗ | ||
| Bamako | 0.36 (0.26-0.49)∗∗∗ | 0.41 (0.29-0.58)∗∗∗ | ||
| Community literacy level | ||||
| Low (ref) | ||||
| Medium | 0.95 (0.81-1.11) | 0.96 (0.81-1.14) | ||
| High | 0.68 (0.52-0.88)∗∗ | 0.78 (0.59-1.03) | ||
| Community socioeconomic status | ||||
| Low (ref) | ||||
| Medium | 0.89 (0.72-1.12) | 0.97 (0.76-1.24) | ||
| High | 0.69 (0.52-0.90)∗∗ | 0.88 (0.64-1.21) | ||
| Random effect result | ||||
| PSU variance (95% CI) | 0.43 (0.34-0.54) | 0.23 (0.16-0.32) | 0.14 (0.10-0.21) | 0.14 (0.09-0.21) |
| ICC | 0.11 | 0.06 | 0.04 | 0.04 |
| LR test | 357.81 | 100.98 | 64.42 | 47.61 |
| Wald chi-square and P value | Ref | χ 2 = 255.73, P < 0.001 | χ 2 = 268.89, P < 0.001 | χ 2 = 385.69, P < 0.001 |
| Model fitness | ||||
| Log-likelihood | -5534.34 | -4868.39 | -5430.90 | -4818.24 |
| AIC | 11072.68 | 9802.79 | 10893.82 | 9730.49 |
| PSU | 345 | 345 | 345 | 345 |
Notes: ref reference, ∗significant at P < 0.05, ∗∗significant at P < 0.01, ∗∗∗significant at P < 0.001. ICC: intraclass correlation; AIC: Akaike information criterion; PSU: primary sampling unit.
3.3.1. Community Level Factors
Region of residence was found to have a significant association with child marriage. Compared to women residing in the Kayes region, the odds of child marriage among women living in all other eight regions were lower. For instance, the odds of child marriage among women living in Mopti, Kidal, and Gao regions were lower by approximately by 73% (aOR = 0.27, 95% CI; 0.19-0.39), 70% (aOR = 0.30, 95% CI; 0.17-0.50), and 67% (aOR = 0.33, 95% CI; 0.22-0.50), respectively, compared to women living in Kayes region (Table 2).
3.3.2. Random Effects (Measures of Variations) Results
As shown in Table 2, the values of AIC indicate that there was a substantial decrease in the individual/household only model and the model with only community-level factors compared to the final model, and this supports the goodness of fit of the final model developed in the analysis. Thus, the complete model, that included the individual/household and community level factors, was selected for predicting child marriage. The null model (Table 2) demonstrates that there was significant variation in the likelihood of child marriage across the clusters (σ2 = 0.43, 0.34-0.54). The null model showed that 11% of the total variance in early marriage was attributed to between-cluster variations (ICC = 0.11). The between-cluster variations decreased from 11% in the null model to 6% in the individual/household-level only model (Model I). In Model II (individual/household-level), the ICC declined to 4% and then remained as 4% in the complete model (Model III, ICC = 0.04), which had both the individual/household and community level factors. This indicates that the variations in the likelihood of child marriage could be attributed to the variances in the clustering at the primary sampling units.
4. Discussion
In this study, we investigated the individual/household and community-level factors associated with child marriage among women aged 18-49 years using the 2018 Mali demographic and health survey. The study shows that 58.2% (95% CI; 56.3%-60.0%) and 20.3% (95%; 19.0%-21.6%) of women aged 18-49 years were married before their 18th and 15th birthday, respectively. The finding from the current study was lower as compared to a study in SSA [28] that showed that the prevalence of child marriage in Niger, Chad, Guinea, and Mali were 81.7%, 77.9%, 72.8%, and 69.0%, respectively. This variation might be due to variation in methodology used [28] including target population (20-24 years versus 18-49 years) and time when the data was collected (2012/13 and 2018 DHS). Our finding is also lower as compared to a study in Ethiopia that reported that the prevalence of child marriage was 62.8% [42], however, higher than studies in Ghana (29.9%) [43] and Zambia (31.4%) [43]. This might be partly explained by socioeconomic and cultural variations across studied countries [28, 42–44].
Women's educational status, partner/husband educational status, women's occupation, economic status, family size, and ethnicity were the individual/household level factors, whereas region was the community level factor associated with child marriage. More specifically, we found lower odds of child marriage among women who had secondary school and higher education compared to women who had no formal education. This finding is in agreement with some studies from Mali [10], Democratic Republic of Congo [30], Serbia [26], Sudan [45], Ethiopia [29], and several sub-Saharan African countries [28]. For instance, according to the Mali MICS report, among women aged 20-24 years old, the prevalence of child marriage varied from 77% among those with no education, to 64% and 38% among women who had attended primary and secondary school, respectively [10, 22].
Educational attainment increases knowledge and awareness about reproductive health including recommended age for marriage and the negative consequences of child marriage, whereas there may be poor information and knowledge about child marriage and its related problems among girls with no formal education [29]. Several previous studies reported that educated girls who gain skills are less likely to be married at a young age compared to noneducated girls [31, 32]. On the contrary, in places where poor educational opportunities prevail, either related to poverty or geographic location, higher rates of child marriage are reported [46, 47]. This is supported by other findings that show associations between higher child marriage rates and lack of infrastructure and educational services, more commonly seen when schools are too far to reach [34, 48, 49].
Children who drop out of school have higher chances of being married off early. However, children who are in school and acquiring knowledge have a tendency to delay marriage, childbearing and to have small numbers of healthier children [13]. Child marriage also constrains schooling opportunities [50]. Child marriage certainly refutes the right of children to education that helps them to develop personal skills, prepare for adulthood, and to effectively contribute to their family and society. Undeniably, it is too difficult for married girls to continue their schooling since they may be practically excluded from attending school [51].
In this study, lower odds of child marriage among women whose husbands attended higher education were observed. Similar findings were reported in Ethiopia [52]. Similar to economic status, having no formal education and lower educational levels are risks for child marriage, whereas attaining a higher educational level is a protective factor [53]. Education is a known factor for changing attitudes, behaviors, and negative sociocultural norms. Not only for girls, the benefit of education for boys is also crucial because educated boys can easily recognize the negative socioeconomic consequences of child marriage that can help them to delay themselves and their promised girls from child marriage [52].
Moreover, we found lower odds of child marriage among women with professional, technical, or managerial occupations compared to women who were not working. A study conducted in Gambia demonstrated comparable findings [33]. Similarly, a previous study by Singh and Vennam [31] reported that girls who were not employed or working in their family were more likely to be married at a younger age, compared to girls who were employed, specifically those working in the service sector or garment industry.
Additionally, in families where unemployed girls are living together or dependent on their families, some parents are induced to marry off their daughters early for the sake of reducing the financial burden within the family; this practice is more common among communities in rural settings [33]. We found that higher odds of child marriage were reported among women whose occupation was agricultural self-employed, compared to women who were not working. Because of the lack of adequate income generation opportunities for the girls especially in the rural communities, child marriage is commonly viewed as an employment option in some African countries [33].
Comparable to previous studies [26, 28, 54–56], the present study demonstrated lower odds of child marriage among women of higher socioeconomic status as compared to women of lower socioeconomic status. This could be due to the fact that, unlike the poorest families, the richest households are not economically vulnerable and attracted by the wealth of other families; thus, they are able to provide for and educate their children [11, 32].
In this study, we found higher odds of child marriage among women living in large-sized families compared to women living in small-sized families. Consistent findings are reported in previous studies in Sudan [45] and Ethiopia [29]. This could be because parents with large family sizes may use child marriage to decrease their family size for the sake of reducing the use of parental resources and improving their economic resources through getting bride prices [29]. Evidence in West and Central Africa showed that in some rural parts of the region, girls are considered not only as a source of wealth but they are also given out in marriage to increase their family's prestige and social class since they are given in exchange for livestock like cattle, sheep, and goats [11, 57].
In line with studies in Gambia [33], Nigeria [34], and Indonesia [56], our study indicates that child marriage was influenced by women's ethnicity. This could be due to the fact that ethnicity is representative of local practices/values and sociological markers of cultural diversity [58, 59]. Evidence shows child marriages are highly linked with local sociocultural situations [60, 61], and cultural beliefs and practices are seen across different ethnic groups [34]. Even though higher socioeconomic status and urban residence are top considerations for the reduction of child marriage [62–64], it is documented that variations also exist based on ethnicity [65].
In this study, we found that region was significantly associated with child marriage. This is similar to previous evidence in Mali [10, 23] and Nigeria [62]. For instance, a prior report in Mali documented huge differences in child marriage across regions with higher concentrations in Southwestern regions which are more rural and have higher poverty rates [23]. In 2018, United Nations (UN) Women identified hotspots for child marriage in Kayes (70.9%), Sikasso (63.7%), and Mopti (64.5%) [23]. Differences in the prevalence of child marriage could partly be due to differences in the proportion of girls who are out of school or girls whose education is stalled [10]. Additionally, differences in ethnicity, socioeconomic status, norms, and cultures across regions may create regional variations in the prevalence of child marriage [62].
4.1. Strengths and Limitations
Using the recent nationally representative data and multiple modelling approach and examining a broad array of factors, we extend the literature on child marriage by identifying predictors of child marriage at the individual/household and community-levels in Mali. However, the study has some limitations. First, the cross-sectional nature of the study design may not allow for inferring cause-effect relationships in the associations observed. Second, the study might be affected by recall bias and social desirability since the data are self-reported and surveys are interviewer-administered. Finally, even though we attempted to incorporate most factors available in the dataset, cultural factors that need qualitative study designs were not covered and we recommend future studies to fill this gap.
5. Conclusion
The study highlights that more than half of the women were first married before their 18th birthday. Women's educational status, partner's/husband's educational status, women's occupation, family size, and ethnicity were the identified individual/household level factors associated with child marriage. Region was the community-level factor associated with child marriage. Hence, in order to reduce the prevalence of child marriage in the country, enhancing girls' and boy's educational level and empowering girls or women through creating employment opportunities, especially professional or technical and managerial occupations, may be required. Improving the utilization of family planning services, working with community leaders to enhance community awareness about child marriage, giving special attention to regions like Kayes, and experience sharing from subgroups with lower child marriage rates such as from Senoufo/Minianka ethnic groups may reduce the social vulnerabilities associated with child marriage.
Acknowledgments
The authors thank the MEASURE DHS project for their support and for free access to the original data.
Abbreviations
- AHR:
Adjusted hazard ratio
- CI:
Confidence interval
- DHS:
Demographic and Health Survey
- EA:
Enumeration area
- ICF:
Inner-city fund
- INSTAT:
l'Institut National de la Statistique
- LMIC:
Low- and middle-income countries
- PSU:
Primary sampling unit
- SDGs:
Sustainable development goals
- SSA:
Sub-Saharan Africa
- UNDP:
United Nations Development Program
- UNICEF:
United Nations Children's Fund
- USAID:
United States Aid for Internal Development
- WHO:
World Health Organization.
Data Availability
Data for this study were sourced from Demographic and Health surveys (DHS) and available here: https://dhsprogram.com/methodology/survey/survey-display-517.cfm.
Ethical Approval
Ethics approval was not required for this study since the data is secondary and is available in the public domain. More details regarding DHS data and ethical standards are available at: http://goo.gl/ny8T6X.
Consent
No consent to publish was needed for this study as we did not use any details, images, or videos related to individual participants. In addition, data used are available in the public domain.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Authors' Contributions
SY and BZ contributed to the study design and conceptualization. They reviewed the literature and performed the analysis. CZO, BOA, EKA, EB, and AS provided technical support and critically reviewed the manuscript for its intellectual content. SY had final responsibility to submit for publication. All authors read and amended drafts of the paper and approved the final version.
References
- 1.UNICEF. Child marriage is a violation of human rights, but is all too common. https://data.unicef.org/topic/child-protection/child-marriage/
- 2.UNICEF. Child marriage around the world. 2020. https://www.unicef.org/stories/child-marriage-around-world/
- 3.UNICEF. Ending child marriage: progress and prospects. https://data.unicef.org/resources/ending-child-marriage-progress-and-prospects/
- 4.Efevbera Y., Bhabha J. Defining and deconstructing girl child marriage and applications to global public health. BMC Public Health. 2020;20(1):p. 1547. doi: 10.1186/s12889-020-09545-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.GIRLS NOT BRIDES. About child marriage. https://www.girlsnotbrides.org/about-child-marriage/
- 6.Efevbera Y., Bhabha J., Farmer P., Fink G. Girl child marriage, socioeconomic status, and undernutrition: evidence from 35 countries in sub-Saharan Africa. BMC Medicine. 2019;17(1):p. 55. doi: 10.1186/s12916-019-1279-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.UNFPA-UNICEF: Global Programme to End Child Marriage. Evolution in the evidence base on child marriage 2000–2019. UNICEF/UN0324156/Biju Boro. https://www.unfpa.org/sites/default/files/resource-pdf/Child-marriage-evidence-report-2021.pdf.
- 8.UNICEF. State of the World’s Children 2013: Children with Disabilities. New York: United Nation’s Children’s Fund; 2013. [Google Scholar]
- 9.United Nations Children’s Fund. Ending Child Marriage: Progress and Prospects. New York: UNICEF; 2014. [Google Scholar]
- 10.UNFPA. Marrying too young: end child marriage. New York, NY: UNFPA; 2012. [Google Scholar]
- 11.UNICEF. Child marriage, adolescent pregnancy and family formation in West and Central Africa. UNICEF; 2015. [Google Scholar]
- 12.Walker J. A. Early marriage in Africa – trends, harmful effects, and interventions. African Journal of Reproductive Health. 2012;16(2):231–240. [PubMed] [Google Scholar]
- 13.Chaudhuri E. R. Unrecognized sexual abuse and exploitation of children in child, early and forced marriage. Plan International; 2015. [Google Scholar]
- 14.UNFPA. Child marriage and other harmful practices. A desk review of evidence from South Asia. UNFPA Asia-Pacific Regional Office; 2020. [Google Scholar]
- 15.Clark S. Early marriage and HIV risks in sub-Saharan Africa. Studies in Family Planning. 2004;35(3):149–160. doi: 10.1111/j.1728-4465.2004.00019.x. [DOI] [PubMed] [Google Scholar]
- 16.Nour N. M. Health consequences of child marriage in Africa. Emerging Infectious Diseases. 2006;12(11):1644–1649. doi: 10.3201/eid1211.060510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Petroni S., Yates R., Siddiqi M., et al. Understanding the relationships between HIV and child marriage: conclusions from an expert consultation. Journal of Adolescent Health. 2019;64(6):694–696. doi: 10.1016/j.jadohealth.2019.02.001. [DOI] [PubMed] [Google Scholar]
- 18.Anjorin S., Yaya S. Anaemia among under-five children: Is maternal marriage at 18th birthday and above protective? Evidence from 15 countries in Sub-Saharan Africa. Maternal & Child Nutrition. 2021;(article e13226) doi: 10.1111/mcn.13226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.International Planned Parenthood Federation (IPPF) and the International Women’s Rights Action Watch. Options and opportunities for adolescents: Mali. London: IPPF; 2000. Reproductive Rights 2000, wall chart. [Google Scholar]
- 20.Population Council. Child Marriage Briefing: Mali. New York: Population Council; 2004. [Google Scholar]
- 21.Engebretsen S., Gueye M., Melnikas A. J., Fofana S., Fané B., Amin S. Adolescent girls’ migration and its impact on early marriage: qualitative findings in Mali. PLoS ONE. 2020;15(3, article e0230370) doi: 10.1371/journal.pone.0230370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Programme National de contre le Paludisme-PNLP/Mali INFO-STAT/Mali and ICF Macro. Enquete sur la prevalence de I’Anemie et de la Parasitemie palustre chez les enfants (EA & P) au Mali 2010. Calverton, Maryland, USA: CPS/DNSI and ICF Macro; 2010. [Google Scholar]
- 23.Girls Not Brides. Child marriage around the world: Mali. https://www.girlsnitbrides.org/child-marriage/mali/
- 24.Mensch B. S., Singh S., Casterline J. B. Trends in the timing of first marriage among men and women in the developing world. In: Lloyd C. B., Behrman J. R., Stromquist N. P., Cohen B., editors. The Changing Transitions to Adulthood in Developing Countries: Selected Studies. Washington, D.C.: The National Academies Press; 2006. pp. 118–171. [Google Scholar]
- 25.Mathur S., Greene M., Malhotra A. Too Young to Wed: The Lives, Rights and Health of Young Married Girls. International Center for Research on Women: Washington, D.C; 2003. [Google Scholar]
- 26.Hotchkiss D. R., Godha D., Gage A. J., Cappa C. Risk factors associated with the practice of child marriage among Roma girls in Serbia. BMC International Health and Human Rights. 2016;16(1):p. 6. doi: 10.1186/s12914-016-0081-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Institut National de la Statistique - INSTAT. Enquête Démographique et de Santé au Mali 2018. Bamako, Mali et Rockville, Maryland, USA: INSTAT, CPS/SS-DS-PF et ICF; 2019. Cellule de Planification et de Statistique Secteur Santé-Développement Social et Promotion de la Famille CPS/SS-DS-PF et ICF. [Google Scholar]
- 28.Yaya S., Odusina E. K., Bishwajit G. Prevalence of child marriage and its impact on fertility outcomes in 34 sub-Saharan African countries. BMC International Health and Human Rights. 2019;19(1):p. 33. doi: 10.1186/s12914-019-0219-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Bezie M., Addisu D. Determinants of early marriage among married women in Injibara town, north West Ethiopia: community-based crosssectional study. BMC Women's Health. 2019;19(1):p. 134. doi: 10.1186/s12905-019-0832-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Mpilambo J. E., Appunni S. S., Kanayo O., Stiegler N. Determinants of early marriage among young women in Democratic Republic of Congo. Journal of Social Sciences. 2017;52(1–3):82–91. doi: 10.1080/09718923.2017.1322393. [DOI] [Google Scholar]
- 31.Singh R., Vennam U. Factors shaping trajectories to early marriage. Vol. 149. Young Lives Working Paper; 2016. [Google Scholar]
- 32.UNICEF/UNFPA. Key drivers of the changing prevalence of child marriage in three countries in three countries in South Asia. Working paper; 2018. [Google Scholar]
- 33.Lowe M., Joof M., Rojas B. M. Social and cultural factors perpetuating early marriage in rural Gambia: an exploratory mixed methods study. F1000Research. 2019;8(8):p. 1949. doi: 10.12688/f1000research.21076.3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Mobolaji J. W., Fatusi A. O., Adedini S. A. Ethnicity, religious affiliation and girl-child marriage: a cross-sectional study of nationally representative sample of female adolescents in Nigeria. BMC Public Health. 2020;20(1):p. 583. doi: 10.1186/s12889-020-08714-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Rutstein S. O., Johnson K. DHS Comparative Reports No. 6. Calverton, Maryland: ORC Macro; 2004. The DHS Wealth Index. [Google Scholar]
- 36.O’brien R. M. A caution regarding rules of thumb for variance inflation factors. Quality & quantity. 2007;41(5, article 9018):673–690. doi: 10.1007/s11135-006-9018-6. [DOI] [Google Scholar]
- 37.Gelman A., Hill J. Data Analysis Using Regression and Multilevelhierarchical Models. New York, NY, USA: Cambridge University Press; 2007. [Google Scholar]
- 38.Merlo J., Wagner P., Ghith N., Leckie G. An original stepwise multilevel logistic regression analysis of discriminatory accuracy: the case of neighbourhoods and health. PloS one. 2016;11(4, article e0153778) doi: 10.1371/journal.pone.0153778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Zegeye B., el-Khatib Z., Ameyaw E. K., et al. Breaking barriers to healthcare access: a multilevel analysis of individual- and community-level factors affecting women’s access to healthcare services in Benin. International Journal of Environmental Research and Public Health. 2021;18(2):p. 750. doi: 10.3390/ijerph18020750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Perinetti G. StaTips part IV: selection, interpretation and reporting of the intraclass correlation coefficient. South European journal of orthodontics and dentofacial research. 2018;5(1):3–5. doi: 10.5937/sejodr5-17434. [DOI] [Google Scholar]
- 41.Acquah H. G. Comparison of Akaike information criterion (AIC) and Bayesian information criterion (BIC) in selection of an asymmetric price relationship. Journal of Development and Agricultural Economics. 2010;2(1):1–6. [Google Scholar]
- 42.Tessema Z. T. Spatial distribution and associated factors’ of early marriage among reproductive age women in Ethiopia: a secondary data analysis of Ethiopian Demographic and Health Survey 2016. BMC Women's Health. 2020;20(1):p. 268. doi: 10.1186/s12905-020-01103-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.on behalf of the Ghana LEAP 1000 evaluation team, de Groot R., Kuunyem M. Y., Palermo T. Child marriage and associated outcomes in northern Ghana: a cross-sectional study. BMC Public Health. 2018;18(1, article 5166):p. 285. doi: 10.1186/s12889-018-5166-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Chitempa N. Girl Empowerment and Child Marriage: Empowering Girls to Prevent and End Child Marriage in Zambia. 2018.
- 45.Ali A., Ibrahim I., Abdelgbar S., Elgessim M. Socio-demographic factors affecting child marriage in Sudan. Journal of Women's Health Care. 2014;3(4):p. 163. doi: 10.4172/2167-0420.1000163. [DOI] [Google Scholar]
- 46.Karim N., Greene M., Picard M. The cultural context of child marriage in Nepal and Bangladesh. CARE research report; 2016. [Google Scholar]
- 47.Roest J. Child marriage and early childbearing in India: risk factors and policy implications. Young Lives; 2016. [Google Scholar]
- 48.UNICEF. Adolescents in India: a desk review of existing evidence and behaviours, programmes and policies. 22. Vol. 40. New Delhi: Population Council and UNICEF; 2013. [Google Scholar]
- 49.UNICEF. Desk Review of Child Marriage. New Delhi: UNICEF; 2011. [Google Scholar]
- 50.Field E., Ambrus A. Early marriage, age of menarche, and female schooling attainment in Bangladesh. Journal of Political Economy. 2008;116(5):881–930. doi: 10.1086/593333. [DOI] [Google Scholar]
- 51.UNICEF. Early Marriage Child Spouses. Florence, Italy: UNICEF Innocenti Research Centre; 2001. [Google Scholar]
- 52.Jones N., Tefera B., Stephenson J., et al. Early marriage and education: the complex role of social norms in shaping Ethiopian adolescent girls’ lives. Country Report. Overseas Development Institute; 2014. [Google Scholar]
- 53.USIAD and ICRW. New insights on preventing child marriage: a global analysis of factors and programs. United States Agency for International Development (USAID) and International Center for Research on Women (ICRW); 2007. [Google Scholar]
- 54.Cader A. A. Ending child, early, and forced marriage: SRHR as central to the solution. Vol. 40. Asian-Pacific Resource & Research Centre for Women (ARROW); 2017. [Google Scholar]
- 55.Sayi T. S., Sibanda A. Correlates of child marriage in Zimbabwe. Journal of Family Issues. 2018;39(8):2366–2388. doi: 10.1177/0192513X18755198. [DOI] [Google Scholar]
- 56.Rumble L., Peterman A., Irdiana N., Triyana M., Minnick E. An empirical exploration of female child marriage determinants in Indonesia. BMC Public Health. 2018;18(1):p. 407. doi: 10.1186/s12889-018-5313-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Birech J. Child marriage: a cultural health phenomenon. International Journal of Humanities and Social Science. 2013;3(17):97–103. [Google Scholar]
- 58.Sociology of ethnicity and health: this Is not a sociology blog. https://thisisnotasociology.blog/2015/03/23/sociology-of-ethnicity-and-health/
- 59.SciELO-Public Health. Persisting problems related to race and ethnicity in public health and epidemiology research. https://scielosp.org/scielo.php?pid=S0034-89102013000100014&script=sci_arttext/ [DOI] [PubMed]
- 60.Bicchieri C., Jiang T., Lindemans J. W. A social norms perspective on child marriage: the general framework. 2014.
- 61.Wahhaj Z. A theory of child marriage. School of Economics. University of Kent; 2015. [Google Scholar]
- 62.Adebowale S. A., Fagbamigbe F. A., Okareh TO, Lawal G. O. Survival analysis of timing of first marriage among women of reproductive age in Nigeria: regional differences. African Journal of Reproductive Health. 2012;16(4):95–107. [PubMed] [Google Scholar]
- 63.Kamal S. M. M., Hassan C. H., Alam G. M., Ying Y. Child marriage in Bangladesh: trends and determinants. Journal of Biosocial Science. 2015;47(1):120–139. doi: 10.1017/S0021932013000746. [DOI] [PubMed] [Google Scholar]
- 64.Ayiga N., Rampagane V. Determinants of age at first marriage in sub-Saharan Africa: a comparative study of Uganda and South Africa. Journal of Social Development in Africa. 2013;28(1):9–34. [Google Scholar]
- 65.Sisters in Islam [SIS] National Report: Malaysia. Malaysia: Asian-Pacific Resource and Research Centre for Women [ARROW]; 2018. Child marriage: its relationship with religion, culture and patriarchy. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data for this study were sourced from Demographic and Health surveys (DHS) and available here: https://dhsprogram.com/methodology/survey/survey-display-517.cfm.