

We describe evolution of persistent immune thrombocytopaenic purpura (ITP) from acute ITP in a young woman with clinically otherwise inapparent severe acute respiratory syndrome ‐ coronavirus 2 (SARS‐CoV‐2) infection (COVID‐19); her development of ITP was matter for an earlier report.[1] ITP is an acquired disease in which thrombocytopaenia results from autoantibodies against platelet antigens. Approximately 10% of patients with acute ITP develop persistent (lasting 3–12 months) or chronic (>12 months) ITP.[2] Infections with viruses like Epstein‐Barr virus and cytomegalovirus can trigger acute ITP.[3] Many instances of acute ITP associated with COVID‐19 are described [1, 4, 5, 6]. Instances of persistent or chronic ITP associated with COVID‐19 have not been reported.
A previously well 30‐year‐old woman sought dental care for new‐onset gingival bleeding in August 2020. A markedly decreased platelet count (3 × 109/L) was found. She was referred to our hospital.
On admission, her gums bore coagulated blood and her extremities prominent purpural and petechial lesions (Figure 1A). She denied medication. A platelet count was very low (4 × 109/L; 2018, 164 × 109/L) with a high increase in reticulated platelet count (28.6%, expected < 2.0%). Platelet‐associated IgG was elevated at 559 ng/107 platelets (expected < 46 ng/107). No other haematologic abnormality was found in peripheral blood. Current infection with Epstein‐Barr virus, cytomegalovirus, hepatitis B virus, hepatitis C virus, or human immunodeficiency virus ‐1 and ‐2, autoantibodies (Table 1), and Helicobacter pylori antigen (tested in stool) were not detectable. Bone‐marrow examination showed markedly increased numbers of megakaryocytes (264 × 106/L), without dysplasia (Figure 1B). Computed tomography identified no splenomegaly and unexpectedly found bilateral ground‐glass lower‐lobe lung opacity; the patient was afebrile, and chest roentgenograms had been assessed as without abnormality. Real‐time polymerase chain reaction (RT‐PCR) testing for SARS‐CoV‐2, using saliva, accordingly was performed 2 days in a row, in both without detecting evidence of infection.
FIGURE 1.
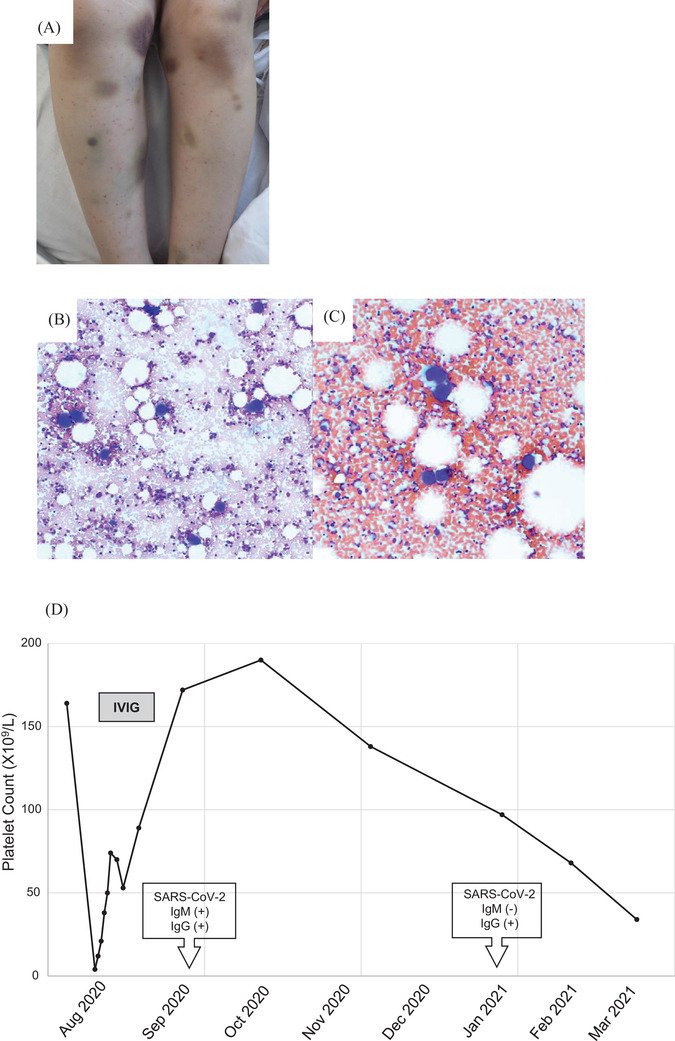
(A) Purpuric lesions and petechiae, both legs, at presentation. (B and C) Normocellular bone‐marrow aspirate with increase in megakaryocyte numbers (May‐Grünwald‐Giemsa, original magnifications, 100 x); (B) August 2020 and (C) March 2021. (D) Course, platelet count
Abbreviations: IVIG, intravenous immunoglobulin therapy; SARS‐CoV‐2, severe acute respiratory syndrome ‐ coronavirus 2; SARS‐CoV‐2 IgG, anti‐SARS‐CoV‐2 IgG‐class antibody; SARS‐CoV‐2 IgM, anti‐SARS‐CoV‐2 IgM‐class antibody
TABLE 1.
Results, assays for infection and autoantibodies
| August 2020 | March 2021 | |
|---|---|---|
| Agent | ||
| HIV | (‐) | (‐) |
| Hepatitis B virus | (‐) | (‐) |
| Hepatitis C virus | (‐) | (‐) |
| Epstein‐Barr virus | IgG: 160x, IgM < 10x, EBNA 160x | IgG: 80x, IgM < 10x, EBNA 20x |
| Cytomegalovirus | (‐) | (‐) |
| Helicobacter pylori | (‐) | Not assayed |
| Autoantibodies | ||
| Anti‐nuclear | (‐) | (‐) |
| Anti‐SS‐A | (‐) | (‐) |
| Anti‐SS‐B | (‐) | (‐) |
| Anti‐DNA (IU/ml) | <2.0 | <2.0 |
| Anti‐platelet | (‐) | (‐) |
| Anti‐β2‐glycoprotein I (U/ml) | <1.2 | <1.2 |
Abbreviations: Anti SS‐A, anti‐Sjögren's‐syndrome‐related antigen A autoantibodies; Anti‐SS‐B, anti‐Sjögren's‐syndrome‐related antigen B autoantibodies; HIV, human immunodeficiency virus ‐1 and ‐2; EBNA, Epstein‐Barr virus nuclear antigen.
Acute ITP was diagnosed, and intravenous immunoglobulin therapy (IVIG), 400 mg/kg, was initiated. Corticosteroids were not used because of possible pneumonia. On the fourth day of IVIG, her platelet count had increased to 38 × 109/L. Nasopharyngeal RT‐PCR testing detected SARS‐CoV‐2 sequences. Haemorrhagic disease responded to IVIG. The patient was discharged home on hospital day 10 [1].
She attended clinic monthly in follow‐up. In October 2020, her platelet count had recovered (190 × 109/L); however, it gradually fell again (97 × 109, 68 × 109, 30 × 109/L: January, February, March 2021, respectively). Anti‐SARS‐CoV‐2 immunoassays of serum detected anti‐SARS‐CoV‐2 IgG‐ but not IgM‐class antibody. Autoantibodies and evidence of infection again were absent (Table 1), and bone‐marrow examination findings were like those before (increase in megakaryocyte numbers at 51 × 106/L without dysplasia [Figure 1C]). Persistent ITP following acute ITP associated with COVID‐19 was diagnosed. As her platelet count is steady at >30 × 109/L (Figure 1D) without evident bleeding, corticosteroid therapy has been withheld in favour of close observation.
Mild thrombocytopaenia has been observed in approximately 5%–10% of patients with COVID‐19 infection [7]. Implicated factors and mechanisms include cytokine storm, direct infection of haematopoietic and bone‐marrow stromal cells, antibody‐mediated platelet destruction, reduced effect of thrombopoietin, increased circulating‐platelet consumption via lung injury or multiple‐organ failure, and immune complexes [8, 9]. Recent guidelines recommend steroids as first‐line therapy for ITP associated with COVID‐19. IVIG is recommended when an immediate rise in platelet count is required [10]. Administration of thrombopoietin‐receptor agonists may be associated with increased risk of thrombosis and hepatobiliary biomarker abnormalities; that these agents be avoided in COVID‐19 is recommended at present [5, 10]. As noted above, we refrained from administering corticosteroids for fear of potentiating infection via immunosuppression. Platelet counts promptly rose with IVIG treatment.
Failure to develop anti‐SARS‐CoV‐2 antibodies associated with immunochemotherapy (e.g., rituximab, corticosteroids) is described [11, 12]. Our patient, by contrast, had been well, receiving no such treatment. Anti‐SARS‐CoV‐2 antibodies of both IgM‐ and IgG‐class were present on initial presentation, and on repeat evaluation prompted by recurrence of thrombocytopaenia only IgG‐class anti‐SARS‐CoV‐2 antibody was demonstrable, consonant with remote COVID‐19 and persistent thrombocytopaenia. Bennett et al describe relapse of COVID‐19‐associated thrombocytopaenia 28 days after response to IVIG therapy and propose pre‐existent and undiagnosed ITP [13]. In our patient, a previously normal platelet count may argue against that hypothesis.
Mahevas et al describe 14 patients with COVID‐19‐associated ITP, of whom three relapsed (with recovery) on day 30, day 35, and day 58 during follow‐up [5]. As their follow‐up period was only 50–60 days, whether persistent or chronic ITP developed is unknown. The authors point out, however, that COVID‐19 may trigger a tolerance breakdown that could lead to persistent or chronic ITP.
We believe that our patient is the first instance described of persistent ITP (>7 months follow‐up) evolved from acute ITP associated with COVID‐19. Thrombocytopaenia is a common comorbidity in COVID‐19, likely with several aetiologies, among them ITP. As acute ITP triggered by events other than COVID‐19 may progress to persistent or chronic ITP even after initial recovery in platelet count, we anticipate that more patients like ours will be encountered. Continuous and long‐term monitoring of acute ITP associated with COVID‐19 thus must be considered essential.
CONFLICT OF INTEREST
The authors declare that there was no conflict of interest in carrying out this study.
AUTHOR CONTRIBUTIONS
Yoshiki Furukawa and Yoko Azusawa wrote the manuscript. Miki Ando directed the study and wrote the manuscript. Jun Ando designed the project. Yoko Tabe performed anti‐SARS‐CoV‐2 immunoassays. Shintaro Kinoshita interpreted data. Sakiko Harada, Tomonori Ochiai, Kazuya Sugimoto, Tadahiro Honda and Norio Komatsu reviewed the manuscript and provided scientific discussions. All authors have read and approved the manuscript.
ACKNOWLEDGEMENTS
Written informed consent was obtained from the patient for publication of the case report and accompanying images.
Furukawa Y, Ando M, Azusawa Y, Kinoshita S, Harada S, Ochiai T, et al. Persistent immune thrombocytopaenic purpura associated with SARS‐CoV‐2 infection. eJHaem. 2021;2:530–533. 10.1002/jha2.201
REFERENCES
- 1. Ochiai T, Ando J, Harada S, Hiki M, Ando M, Komatsu N. Immune thrombocytopenia preceded by asymptomatic COVID‐19 infection. Rinsho Ketsueki. 2021;62(1):58–60. [DOI] [PubMed] [Google Scholar]
- 2. Rodeghiero F, Stasi R, Gernsheimer T. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: report from an international working group. Blood. 2009;113(11):2386–93. [DOI] [PubMed] [Google Scholar]
- 3. Cines DB, Bussel JB, Liebman HA, Luning Prak ET. The ITP syndrome: pathogenic and clinical diversity. Blood. 2009;113(26):6511–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Zulfiqar AA, Lorenzo‐Villalba N, Hassler P, Andres E. Immune thrombocytopenic purpura in a patient with Covid‐19. N Engl J Med. 2020;382(18):e43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Mahevas M, Moulis G, Andres E. Clinical characteristics, management and outcome of COVID‐19‐associated immune thrombocytopenia: a French multicentre series. Br J Haematol. 2020;190(4):e224–e9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Tsao HS, Chason HM, Fearon DM. Immune thrombocytopenia (ITP) in a pediatric patient positive for SARS‐CoV‐2. Pediatrics. 2020;146(2):e20201419. [DOI] [PubMed] [Google Scholar]
- 7. Chen N, Zhou M, Dong X. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Yang X, Yang Q, Wang Y. Thrombocytopenia and its association with mortality in patients with COVID‐19. J Thromb Haemost. 2020;18(6):1469–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Deruelle E, Ben Hadj Salem O, Sep Hieng S, Pichereau C, Outin H, Jamme M. Immune thrombocytopenia in a patient with COVID‐19. Int J Hematol. 2020;112(6):883–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Pavord S, Thachil J, Hunt BJ. Practical guidance for the management of adults with immune thrombocytopenia during the COVID‐19 pandemic. Br J Haematol. 2020;189(6):1038–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Yasuda H, Tsukune Y, Watanabe N. Persistent COVID‐19 pneumonia and failure to develop anti‐SARS‐CoV‐2 antibodies during rituximab maintenance therapy for follicular lymphoma. Clin Lymphoma Myeloma Leuk. 2020;20(11):774–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Ormazabal Velez I, Indurain Bermejo J, Espinoza Perez J, Imaz Aguayo L, Delgado Ruiz M, Garcia‐Erce JA. Two patients with rituximab associated low gammaglobulin levels and relapsed covid‐19 infections treated with convalescent plasma. Transfus Apher Sci. 2021:103104. 10.1016/j.transci.2021.103104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Bennett J, Brown C, Rouse M, Hoffmann M, Ye Z. Immune thrombocytopenia purpura secondary to COVID‐19. Cureus. 2020;12(7):e9083. [DOI] [PMC free article] [PubMed] [Google Scholar]