

Abstract
Purpose
This study investigated the effect of anxiety on nicotine dependence among university students during the COVID‐19 pandemic.
Design and Methods
This was a descriptive and correlational study. The sample consisted of 503 university students in Turkey. Data were collected online using a demographic characteristics form, the State‐Trait Anxiety Inventory (STAI), and the Fagerström Test for Nicotine Dependence (FTND).
Findings
FTND scores differed by gender, family type, and grade level, while STAI scores differed by gender, income, and region of residence (p < 0.05). Fifty‐one percent of the participants had moderate anxiety, while 65.2% had low nicotine dependence. FTND and STAI mean scores were strongly correlated (p < 0.05).
Practical Implications
The higher the anxiety, the higher the nicotine dependence among university students during the COVID‐19 pandemic.
Keywords: anxiety, COVID‐19, nicotine dependence, pandemic, student
1. INTRODUCTION
Coronavirus disease (COVID‐19) broke out in Wuhan, the capital of Central China's Hubei province, at the end of 2019 and spread across the world rapidly and turned into a pandemic.1, 2 In about 120 million people in the world and Turkey 3 million people have been affected due to COVID‐19. 3
Countries have taken several preventive measures to prevent the spread of COVID‐19, such as social distancing, hygiene measures, quarantine, curfew, travel restrictions, and closures (institutions and workplaces). Face‐to‐face education has also been largely suspended and shifted to distance education due to school closures in response to the pandemic. However, online education increases academic stress in students. 4 Isolation and school closures due to the spread of COVID‐19 change students' daily lives drastically and make them less motivated to study, 5 resulting in anxiety and depression.6, 7 Such multiple stressors also put university students at risk of anxiety and depression. 7 Kaparounakia et al. 8 reported an increase in anxiety symptoms (42.5%) and anxiety levels (73%) in Greek university students due to the COVID‐19 pandemic. Wang and Zhao 7 also found that university students experienced high levels of anxiety during the COVID‐19 pandemic.
Anxiety and boredom are known emotional triggers for smoking. Increasing anxiety at unexpected and unusual times can be an important risk factor for smoking. Especially the psychological effects of social isolation, increasing anxiety levels and its effects on smoking can explain the increase in the rate of use. 9 It has been stated that individuals started to smoke more as a form of defense during difficult processes such as epidemics, due to the feeling of relief that occurs during smoking, emphasized by most cigarette addicts. 10 Social isolation applied during the epidemic process is a risk factor, stressful situations can exacerbate the desire to smoke and create a greater risk of relapse. 11 Studies on smoking after the COVID‐19 outbreak appear to increase smoking rates.9, 12, 13
It is estimated that lifestyle changes, disruption of education, quarantine, and isolation due to the COVID‐19 pandemic lead to mental disorders and nicotine dependence among young people. However, there is no sufficient empirical evidence to support the correlation between anxiety and nicotine dependence. Therefore, the aim of this study is to examine the effect of anxiety on nicotine dependence among university students during the COVID‐19 pandemic.
What characteristics of university students affect their anxiety levels?
What characteristics of university students affect their nicotine addiction levels?
Does the level of anxiety experienced during the pandemic process affect the nicotine addiction rate of university students?
2. METHODS
2.1. Type of the study
This was a descriptive and correlational study.
2.2. Time and place of the study
The study was conducted between May and June 2020.
2.3. Population and sample of the study
The study population consisted of all private and public university students (seven regions of Turkey) who had been smoking for at least 6 months. The inclusion criteria were (1) having been receiving online education during the study, (2) having Internet access, and (3) agreeing to participate. The exclusion criteria were (1) withdrawal from courses due to the COVID‐19 pandemic, (2) having received treatment for nicotine dependence before, and (3) having a mental disorder. A power analysis was performed using GPower (version 3.1.9.2) to determine the appropriate sample size for significant differences. Both male and female participants' mean State‐Trait Anxiety Inventory (STAI) scores were used for the analysis. The post hoc power analysis revealed a power of 95% with an effect size of 0.33 (α = 0.05), indicating that the sample (n = 501) was large enough to detect significant differences (Figure 1). Since the study was collected online, only the participants who completely filled out the questionnaires were included in the study. The study was terminated when a sufficient sample size was reached (n = 503).
Figure 1.
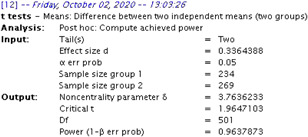
Power analysis [Color figure can be viewed at wileyonlinelibrary.com]
2.4. Data collection tools
Data were collected online using a demographic characteristics form (DCF), the STAI, and the Fagerström Test for Nicotine Dependence (FTND).
2.4.1. Demographic characteristics
The DCF was based on a literature review conducted by the researcher.14, 15, 16 The form consisted of 26 items and three sections. The first section consisted of items on participants' demographic characteristics and health status (gender, family type, perceived income, place of residence, region of residence, housing type, grade level, and chronic disease in themselves and/or in family members). The second section consisted of items on participants' experiences with the COVID‐19 pandemic (having tested or having any family members tested positive for COVID‐19, adaptation to social isolation, and home activities during the pandemic). The third section consisted of items on nicotine dependence and changes in it during the pandemic. Data were collected online (5 min for each participant). Three experts were consulted for the items of the second and third sections.
2.4.2. State‐Trait Anxiety Inventory
The STAI was developed by Spielberger et al. 17 to evaluate how one feels at a particular moment and situation. The STAI was adapted to Turkish by Öner and Le Comte. 18 The STAI consists of 20 items scored on a 4‐point Likert‐type scale of 1 (almost never) to 4 (almost always). The total score ranges from 20 to 80. Higher scores indicate greater anxiety. Ten items (1, 2, 5, 8, 10, 11, 15, 16, 19, and 20) are reverse scored. The Turkish version of the STAI has a Kuder–Richardson reliability coefficient (Cronbach's alpha) of 0.94 to 0.96, 18 which was 0.96 in this study.
2.4.3. Fagerström Test for Nicotine Dependence
The FTND was developed by Fagerström (1978) and revised by Heatherton et al. 19 It was adapted to Turkish by Uysal et al. 20 It consists of six items scored on a 2‐ and 4‐point Likert type scale. An FTND total score of ≤3 indicates low dependence, 4 < FTND score < 6 moderate dependence, and an FTND total score of ≥7 high dependence. The scale has a Cronbach's alpha of 0.61, which was 0.72 in this study.
2.5. Ethical considerations
The study was approved by the Human Research Ethics Committee (Date: April 30, 2020; No: 04/23). Written permission was obtained from the Ministry of Health of the Republic of Turkey. Students were informed about the study, and online informed consent was obtained from those who agreed to participate.
2.6. Data collection
After the researchers obtained the necessary permission, they created online versions of the DCF, STAI, and FTND and shared the link to the questionnaires on WhatsApp groups. They asked participants to complete the questionnaires accurately and send the link to other university students (snowballing sampling). Data collection lasted 10–15 min (Figure 2).
Figure 2.
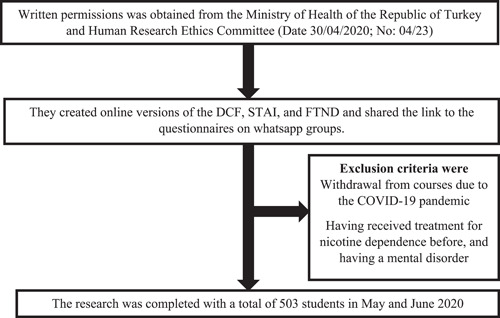
A flow chart of subjects' enrollment. DCF, demographic characteristics form; FTND, Fagerström Test for Nicotine Dependence; STAI, State‐Trait Anxiety Inventory
2.7. Data analysis and evaluation
Data were analyzed using the Statistical Package for Social Sciences (SPSS; version 22.0) at a significance level of 0.05. Percentages, means, the independent‐samples t‐test, analysis of variance test, and Pearson correlation coefficient were used for analysis. The Bonferroni test was used for post hoc comparisons.
2.8. Limitations
The study had two limitations. First, the survey relied on participants' self‐reports, and therefore, data accuracy was not verified. Second, levels of anxiety and nicotine dependence were measured only using the STAI and FTND.
3. RESULTS
The mean age of participants was 21.57 ± 2.46. The mean number of people they had lived with during the pandemic was 4.88 ± 1.81. Of participants, 53.5% were men, 78.5% had a nuclear family, 45.3% had a neutral income, 58.4% were living in the city center, 28.4% were from Eastern Anatolia, 62.4% were living in apartments, and 33% were freshmen. Participants' FTND scores differed by gender, family type, and grade level, while their STAI scores differed by gender, income, and region of residence (p < 0.05). The post hoc test result showed that participants from the Marmara region had higher STAI scores than those from the Black Sea region (Table 1).
Table 1.
Mean FTND and STAI scores by demographic characteristics (n = 503)
| Characteristics | n | % | FTND | STAI | ||
|---|---|---|---|---|---|---|
| X ± SD | Test p | X ± SD | Test p | |||
| Gender | ||||||
| Woman | 234 | 46.5 | 2.13 ± 2.25 | t: −5.57 | 45.28 ± 12.52 | t: 3.74 |
| Man | 269 | 53.5 | 3.35 ± 3.35 | p: 0.000 | 41.29 ± 11.16 | p: 0.000 |
| Family‐type | ||||||
| Nuclear familya | 395 | 78.5 | 2.63 ± 2.53 | F: 3.50 | 43.26 ± 12.00 | F: 1.53 |
| Extended familyb | 86 | 17.1 | 2.67 ± 2.36 | p: 0.031 | 43.05 ± 11.74 | p: 0.216 |
| Broken familyc | 22 | 4.4 | 4.09 ± 2.65 | c > a | 47.81 ± 13.93 | |
| Perceived income | ||||||
| Negative income (income < expenses)a | 149 | 29.6 | 2.73 ± 2.53 | 46.34 ± 11.89 | F: 7.38 | |
| Positive income (income > expenses)b | 126 | 25.0 | 2.75 ± 2.51 | F: 0.076 | 40.96 ± 12.28 | p: 0.001 |
| Neutral income (income = expenses)c | 228 | 45.3 | 2.65 ± 2.53 | p: 0.927 | 42.88 ± 11.71 | a > c > b |
| Place of residence | ||||||
| City | 294 | 58.4 | 2.75 ± 2.55 | F: 1.70 | 44.21 ± 12.30 | F: 2.54 |
| District | 137 | 27.2 | 2.41 ± 2.43 | p: 0.183 | 43.19 ± 12.07 | p: 0.079 |
| Village | 72 | 14.3 | 3.06 ± 2.53 | 40.66 ± 10.69 | ||
| Region of residence | ||||||
| Eastern Anatolia | 143 | 28.4 | 2.69 ± 2.47 | 42.74 ± 12.59 | ||
| Southeastern Anatolia | 73 | 14.5 | 3.09 ± 2.86 | F: 1.63 | 42.09 ± 10.74 | F: 2.51 |
| Central Anatolia | 105 | 20.9 | 2.97 ± 2.58 | p: 0.136 | 43.33 ± 11.83 | p: 0.021 |
| Aegean | 25 | 5.0 | 2.04 ± 2.16 | 45.92 ± 10.59 | ||
| Marmara | 58 | 11.5 | 2.70 ± 2.37 | 47.43 ± 12.14 | ||
| Mediterranean | 69 | 13.7 | 2.04 ± 2.20 | 44.39 ± 12.82 | ||
| Black Sea | 30 | 6.0 | 2.96 ± 2.70 | 38.23 ± 10.48 | ||
| Housing type | ||||||
| Apartment | 314 | 62.4 | 2.60 ± 2.47 | t: 0.48 | 44.52 ± 12.40 | t: 3.50 |
| House | 189 | 37.6 | 2.86 ± 2.60 | p: 0.485 | 41.59 ± 11.26 | p: 0.062 |
| Grade level (year) | ||||||
| Freshman | 166 | 33.0 | 2.68 ± 2.53 | 43.80 ± 12.30 | F: 1.969 | |
| Sophomore | 139 | 27.6 | 2.66 ± 2.34 | F: 1.059 | 43.96 ± 11.74 | p: 0.118 |
| Junior | 105 | 20.9 | 2.45 ± 2.52 | p: 0.366 | 44.49 ± 11.66 | |
| Senior | 93 | 18.5 | 3.08 ± 2.74 | 40.42 ± 12.35 | ||
Abbreviations: FTND, Fagerström Test for Nicotine Dependence; STAI, State‐Trait Anxiety Inventory.
*p < 0.05.
Of participants, 12.1% had a chronic disease, 44.5% had a family member with a chronic disease, 1.8% had tested positive for COVID‐19, 2% had a family member who had tested positive for COVID‐19, and 76.9% was able to adapt to social isolation. Participants' mean FTND and STAI scores were compared by chronic disease, having been tested positive for COVID‐19, and adaptation to social isolation. Chronic disease and adaptation to social isolation affected their mean FTND scores (p < 0.05, Table 2). During social isolation, participants mostly spent time on social media (77.1%), followed by sleeping (71.4%), watching TV (64.2), and listening to music (65.6%). Participants who did nothing during social isolation had a significantly higher mean STAI score than those who read books during social isolation (Table 2).
Table 2.
Distribution of mean FTND and STAI scores by chronic disease, testing positive for COVID‐19, and adaptation to social isolation (n = 503)
| n | % | FTND | STAI | |||
|---|---|---|---|---|---|---|
| X ± SD | Test p | X ± SD | Test p | |||
| Chronic disease in family members | ||||||
| Yes | 224 | 44.5 | 2.70 ± 2.65 | t: −0.039 | 43.93 ± 11.34 | t: 0.849 |
| No | 279 | 55.5 | 2.70 ± 2.42 | p: 0.969 | 43.01 ± 12.61 | p: 0.396 |
| Chronic disease in the participant | ||||||
| Yes | 61 | 12.1 | 3.40 ± 2.75 | t: 2.33 | 46.24 ± 14.47 | t: 1.95 |
| No | 442 | 87.9 | 2.60 ± 2.47 | p: 0.020 | 43.03 ± 11.65 | p: 0.051 |
| Having been tested positive for COVID‐19 | ||||||
| Yes | 9 | 1.8 | 3.22 ± 3.34 | t: 0.61 | 47.22 ± 10.49 | t: 0.95 |
| No | 494 | 98.2 | 2.69 ± 2.51 | p: 0.536 | 43.35 ± 12.08 | p: 0.341 |
| Anyone tested positive for COVID‐19 in the family | ||||||
| Yes | 10 | 2.0 | 3.00 ± 3.36 | t: 0.37 | 50.80 ± 11.90 | t: 1.95 |
| No | 493 | 98.0 | 2.69 ± 2.50 | p: 0.710 | 43.27 ± 12.03 | p: 0.051 |
| Adaptation to social isolation | ||||||
| Yes | 387 | 76.9 | 2.43 ± 2.41 | t: 4.403 | 43.39 ± 12.37 | t: 0.126 |
| No | 116 | 23.1 | 3.59 ± 2.68 | p: 0.000 | 43.55 ± 11.01 | p: 0.899 |
| Home activities during the pandemic | ||||||
| Watching TV | 323 | 64.2 | 2.70 ± 2.53 | 0.038/0.970 | 42.71 ± 12.10 | 1.778/0.076 |
| Reading books | 249 | 49.5 | 2.60 ± 2.61 | 0.874/0.383 | 41.66 ± 11.78 | 3.272/0.001 |
| Listen to music | 330 | 65.6 | 2.60 ± 2.43 | 1.187/0.236 | 42.96 ± 12.30 | 1.176/0.240 |
| Doing housework | 308 | 61.2 | 2.60 ± 2.47 | 1.174/0.241 | 43.49 ± 11.91 | 1.154/0.877 |
| Doing nothing | 166 | 33.0 | 2.96 ± 2.55 | 1.650/0.100 | 47.50 ± 13.19 | 5.473/0.000 |
| Spending time on social media | 388 | 77.1 | 2.64 ± 2.54 | 0.918/0.359 | 43.35 ± 11.95 | 0.254/0.800 |
| Exercising | 166 | 33.0 | 2.37 ± 2.36 | 2.079/0.038 | 41.98 ± 12.40 | 1.891/0.059 |
| Oversleeping | 359 | 71.4 | 2.67 ± 2.50 | 0.405/0.686 | 43.58 ± 12.30 | 0.462/0.644 |
| Studying | 65 | 12.9 | 2.46 ± 2.38 | 0.836/0.404 | 43.20 ± 12.69 | 0.163/0.871 |
| Playing video games | 25 | 5.0 | 2.40 ± 2.50 | 0.621/0.535 | 41.60 ± 12.90 | 0.777/0.438 |
Note: More than one option marked. “Yes” responses were taken into account. An independent sample t‐test was used.
Abbreviations: FTND, Fagerström Test for Nicotine Dependence; STAI, State‐Trait Anxiety Inventory.
*p < 0.05.
Of participants, 60% had smokers in the family, and 52.7% perceived their relationships with family members as “normal.” Less than half of the participants (32.4%) smoked more cigarettes, 57.7% stockpiled packs of cigarettes, 41.7% experienced anxiety/stress about not being able to buy cigarettes, 64.8% did not regret smoking, and 58.1% made no effort to reduce smoking during social isolation (Table 3). Participants' mean FTND and STAI scores differed by “other smokers in the family,” “perceived relationship with family members,” “increased smoking during social isolation,” “stockpiling cigarettes during curfews,” and “anxiety and stress caused by not being able to buy cigarettes during social isolation” (p < 0.05, Table 3).
Table 3.
Distribution of mean FTND and STAI scores by smoking during the COVID‐19 pandemic (n = 503)
| n | % | FTND | STAI | |||
|---|---|---|---|---|---|---|
| X ± SD | Test p | X ± SD | Test p | |||
| Other smokers in the family | ||||||
| Yes | 302 | 60.0 | 3.05 ± 2.54 | t: 3.90 | 44.45 ± 12.75 | t: 2.35 |
| No | 201 | 40.0 | 2.17 ± 2.40 | p: 0.000 | 41.88 ± 10.78 | p: 0.019 |
| Perceived relationship with family members | ||||||
| Supportivea | 164 | 32.6 | 2.57 ± 2.62 | F: 17.58 | 39.68 ± 11.18 | F: 4.35 |
| Normalb | 265 | 52.7 | 2.56 ± 2.37 | p: 0.000 | 44.16 ± 11.44 | p: 0.013 |
| Conflictingc | 74 | 14.7 | 3.50 ± 2.71 | c > a = b | 49.08 ± 13.49 | c > b > c |
| Increased smoking during social isolation | ||||||
| Yes | 163 | 32.4 | 4.31 ± 2.59 | t: 11.05 | 46.94 ± 12.74 | t: 4.61 |
| No | 340 | 67.6 | 1.93 ± 2.08 | p: 0.000 | 41.74 ± 11.35 | p: 0.000 |
| Stockpiling cigarettes during curfews | ||||||
| Yes | 290 | 57.7 | 4.09 ± 2.52 | t: 12.02 | 45.17 ± 12.79 | t: 2.80 |
| No | 213 | 42.3 | 1.68 ± 1.98 | p: 0.000 | 42.14 ± 11.34 | p: 0.005 |
| Anxiety and stress caused by not being able to buy cigarettes during social isolation | ||||||
| Yes | 210 | 41.7 | 3.90 ± 2.53 | t: 9.79 | 46.82 ± 12.60 | t: 5.49 |
| No | 293 | 58.3 | 1.84 ± 2.14 | p: 0.000 | 40.99 ± 11.05 | p: 0.000 |
| Regretting smoking during social isolation | ||||||
| Yes | 177 | 35.2 | 2.72 ± 2.47 | t: 0.15 | 44.27 ± 11.20 | t: 1.15 |
| No | 326 | 64.8 | 2.69 ± 2.55 | p: 0.880 | 42.96 ± 12.49 | p: 0.248 |
| Making efforts to reduce smoking during the pandemic | ||||||
| Yes | 211 | 41.9 | 2.50 ± 2.46 | t: −1.50 | 43.89 ± 11.53 | t: 0.73 |
| No | 292 | 58.1 | 2.84 ± 2.55 | p: 0.134 | 43.09 ± 12.43 | p: 0.464 |
Abbreviations: FTND, Fagerström Test for Nicotine Dependence; STAI, State‐Trait Anxiety Inventory.
*p < 0.05.
Participants had a mean STAI of 43.42 ± 12.06. Slightly more than half of the participants (51%) had moderate anxiety. Participants had a mean FTND score of 2.7 ± 2.5. More than half of them (65.2%) had low nicotine dependence (Table 4).
Table 4.
Mean FTND and STAI scores (n = 503)
| Scale | n | % | Min–max | X ± SD |
|---|---|---|---|---|
| STAI | ||||
| Mild anxiety (20–39.9) | 197 | 39.1 | 20–79 | 43.42 ± 12.06 |
| Moderate anxiety (40–59.9) | 257 | 51.0 | ||
| Severe anxiety (60–80) | 49 | 9.7 | ||
| FTND | ||||
| Low dependence (≤3) | 328 | 65.2 | 0–10 | 2.7 ± 2.5 |
| Moderate dependence (4–6) | 124 | 24.7 | ||
| High dependence (≥7) | 51 | 10.1 | ||
Abbreviations: FTND, Fagerström Test for Nicotine Dependence; STAI, State‐Trait Anxiety Inventory.
In Table 5, whether there is a relationship between the nicotine addiction and state level of the students was examined; a statistically positive and very strong significant correlation was found between FNBT and DAÖ mean scores (r = 0.106, p = 0.017).
Table 5.
Correlation evaluation of students' FNBT and STAI scores (n = 503)
| STAI | ||
|---|---|---|
| FNBT | Pearson correlation | 0.106 |
| Sig. (two‐tailed) | 0.017 | |
| n | 503 |
Abbreviations: FTND, Fagerström Test for Nicotine Dependence; STAI, State‐Trait Anxiety Inventory.
*p < 0.05.
A multi‐logit model was established to determine the factors affecting nicotine addiction. When the likelihood ratio in the model was examined, it was found that the model was statistically significant. It is also calculated as 0.119 for R 2 Cox–Snell and 0.145 for Nagelkerke, which shows the explanation power for the model. When the individual estimation results for the levels of the dependent variable were examined, two models were estimated for nicotine levels as medium and high. For those with moderate nicotine levels, the anxiety level of the individual, having a broken family and gender are influencing factors. In addition, those with a fragmented family structure are more likely to have moderate nicotine addiction than those who do not, and men are more likely than women. For those with high nicotine levels, the age and gender of the individual are influencing factors. As the age of the person increases, the possibility of having a high level of nicotine addiction increases. In addition, men are the categories that are more likely to have moderate nicotine addiction than women. The variables that are significant in both models are the person's gender. Men are more likely to have a moderate to high nicotine addiction than women are more likely to have both moderate and high nicotine addiction (Table 6).
Table 6.
Multinomial logit model analysis for nicotine addiction (n = 503)
| FTND = Moderate | |||||
|---|---|---|---|---|---|
| Variables | Coefficients | Std Error | RRR+ | Test p | |
| Constant | −3.627763 | 1.053442 | 0.0265756 | 0.001* | |
| Anxiety | 0.0371145 | 0.0094081 | 1.037812 | 0.000* | |
| Age | 0.0273256 | 0.043647 | 1.027702 | 0.531 | |
| Family‐type | |||||
| Extended family | −0.5115012 | 0.3172461 | 0.5995948 | 0.107 | |
| Broken family | 1.41797 | 0.5040674 | 4.128731 | 0.005* | |
| Gender | |||||
| Male | 0.8926936 | 0.2329911 | 2.441698 | 0.000* | |
| FTND = High | |||||
| Constant | −6.691293 | 1.205853 | 0.0012417 | 0.000* | |
| Anxiety | 0.023993 | 0.013582 | 1.024283 | 0.077 | |
| Age | 0.1449237 | 0.043366 | 1.155951 | 0.001* | |
| Family‐type | |||||
| Extended family | −0.6538456 | 0.458691 | 0.5200421 | 0.154 | |
| Broken family | 1.072888 | 0.7263694 | 2.923811 | 0.140 | |
| Gender | |||||
| Male | 1.199679 | 0.3420909 | 3.319051 | 0.000* | |
| LR(10): 63.532, p = 0.000 | AIC: 1.634 | BIC: −2256.621 | |||
| Cox–Snell R 2: 0.119 | Nagelkerke R 2: 0.145 | ||||
Abbreviations: AIC, Akaike information criterion; BIC, Bayesian information criteria; FTND, Fagerström Test for Nicotine Dependence; LR, likelihood ratio.
4. DISCUSSION
University students are a group at high risk for symptoms of depression and anxiety. 7 The mental health of university students is adversely affected due to the spread of the epidemic throughout the country, strict isolation measures and the closure of schools, colleges and universities, decrease in students' motivation to study, increasing pressures for independent learning, and abandonment of daily routines. 5 Increasing anxiety at unexpected and unusual times can be an important risk factor for smoking. 9 For this reason, in this study, the effect of anxiety experienced by university students during the COVID‐19 process on nicotine addiction was discussed, and the findings were discussed in line with the literature.
Most of our participants had been smoking during the COVID‐19 pandemic. Male participants had significantly higher nicotine dependence than females (Table 1). Research on Turkish university students shows in general that male students have significantly higher nicotine dependence than females.21, 22, 23 Provenzano et al. 16 reported that male nursing students had significantly higher nicotine dependence than females. Mallet and Dubertret 24 found that men had significantly higher nicotine dependence than women during the COVID‐19 pandemic. Male and female behaviors are shaped according to certain stereotypes within the structure of the society they are in. For this reason, men more independent. Starting from a young age, raising men in a more liberal nature, putting a cigarette in the mouth of a boy gives rise to the idea of “I am strong, I am free” in boys and triggers nicotine addiction in men. 25 As a result of the regression analysis performed in our study, it was found that our variable, which was significant in the model in which nicotine addiction was moderate and high, was the gender of the person (Table 6). The probability of nicotine addiction was found to be higher in men than in women, and this finding is consistent with the literature and analysis. Our female participants experienced more anxiety than males (Table 1), which was consistent with the literature. Yakar et al. 14 reported that female medical students suffered from anxiety more than males during the COVID‐19 pandemic. Wu et al. 26 and Zhao et al. 27 also found that Chinese female university students experienced more anxiety than males during the COVID‐19 pandemic. Women are more emotional than men due to physiological differences between men and women, such as genetic sensitivity, hormone, and cortisol levels. Because of these differences, women were more vulnerable to stress and pain than men, so they may experience more sadness and anxiety. 28
Participants from broken families had higher nicotine dependence than those from nuclear families (Table 1). Research, in general, shows that people from broken families have higher nicotine dependence than others.21, 29 A study from Italy has found a correlation between nicotine dependence and nonconventional family types (single‐parent, broken families, etc.). 30 Young people from broken families are more likely to develop nicotine dependence and criminal behavior due to socioeconomic problems and limited parental control. 31 As a result of the regression analysis performed in our study, our variable, which was significant in the model with moderate nicotine addiction, was found to be the family type of the person (Table 6). The probability of nicotine addiction was found to be higher in the fragmented family‐type compared to other family types, and this finding is consistent with the literature and analysis. It is noteworthy that participants from broken families had higher nicotine dependence during the pandemic. Therefore, more research is warranted on factors affecting nicotine dependence in people from broken families.
Participants with a negative income had higher anxiety than those with a positive income (Table 1). Low socioeconomic status is associated with both increased nicotine dependence and anxiety. 32 The loss of job and income makes the COVID‐19 curfews more challenging and stressful for all family members. 33 The pandemic has adverse financial impacts on thousands of people. 32 Negative income may have put the participants in a vicious cycle; not being able to afford to buy cigarettes caused more anxiety, which resulted in increased nicotine dependence.
Participants from the Marmara region experienced higher levels of anxiety than those from the other regions (Table 1). The World Health Organization (WHO) 34 conducted an epidemiological study involving people of all age groups from Turkey and found that respondents from Eastern Anatolia (50%), Aegean (49%), and Marmara regions had the highest pandemic‐related anxiety. 34 Participants from the Marmara region reported the highest levels of anxiety, probably because it is the region with the highest number of COVID‐19 cases. It is also because Marmara has coastal cities with good climatic conditions, social opportunities, and a large young university‐educated population, which we believe has been severely affected by social isolation during the pandemic.
Participants with chronic diseases had higher nicotine dependence than others (Table 2). WHO states that people with chronic diseases are more likely to develop severe or critical COVID‐19. 35 Those participants may have developed more nicotine dependence because they were unable to access health services, buy their prescription drugs, and socialize due to quarantine constraints during the COVID‐19 pandemic while at the same time having to cope with their chronic diseases.
Participants who had difficulty adapting to social isolation had higher FTND scores (Table 2). Günay 36 found that children quarantined during the COVID‐19 pandemic had posttraumatic stress scores four times as high as those who were not. Moreover, changes in lifestyle and psychosocial stress caused by quarantine may lead to a vicious cycle, exacerbating the already existing physical and mental health issues. 37 This may have resulted in increased nicotine dependence among our participants.
Participants mostly spent time on social media, slept, watched TV, or listened to music. Participants who read books or did nothing at home during the COVID‐19 pandemic had significantly high anxiety (Table 2). People play video games, watch TV shows, use social media, or browse the internet to reduce the symptoms of epidemic‐related stress, anxiety, and depression. 38 An international study on media consumption at home during the COVID‐19 pandemic have reported that people watch news broadcasts more (67%) and spend more time on messaging apps (45%) and social media (44%), with the highest increases observed in Generation Z. 39 Loss of interest in activities is a sign of anxiety among adolescents. Therefore, it is not surprising that participants who did nothing at home during the pandemic had significantly high anxiety.
Participants who had other smokers in the family had higher nicotine dependence and anxiety (Table 3), which is consistent with the literature. Having family members who smoke affects nicotine dependence among students. 40 Oğuz et al. 41 found that students with smoking mothers and sisters had higher nicotine dependence. Birinci and Bulut 33 also reported that students with smoking parents or siblings had higher nicotine dependence. Elbi et al. 42 detected a positive correlation between the nicotine dependence rates of students and their family members.
Participants with conflicting relationships with family members had higher nicotine dependence and anxiety (Table 3). Many people were in constant contact with family members during the quarantine. Having to spend more time at home with family during the COVID‐19 pandemic is frustrating and inhibiting for young people who are used to socializing and connecting with their friends, which inevitably resulted in increased anger and anxiety.37, 43, 44 Therefore, young people with conflicting relationships with family members may turn to smoke, which is frowned upon by parents.
Participants who smoked more cigarettes, stockpiled packs of cigarettes, and were worried about the possibility of not being able to go out and get cigarettes during the COVID‐19 pandemic had higher nicotine dependence and anxiety (Table 3). Social isolation is as serious a risk factor as nicotine dependence, obesity, and a sedentary lifestyle. 45 Social isolation, voluntary social distancing, and lockdowns make smoking and exposure to secondhand smoke more likely. 46 Health and social measures for COVID‐19 may have caused participants to experience more anxiety, making them smoke more and stockpile more packs of cigarettes to cope with stress and anxiety.
Participants had a mean STAI of 43.42 ± 12.06. Slightly more than half of the participants (51%) had moderate anxiety (Table 4). Söğüt et al. 46 investigated midwifery students' pandemic‐related knowledge and anxiety and found that most students experienced mild anxiety. 46 Yakar et al. 14 looked into medical students' pandemic‐related knowledge and anxiety and reported that they had a mean STAI of 43.54, which was similar to our result. Rakhmanov and Dane 15 also examined the knowledge and anxiety levels of African university students regarding the COVID‐19 pandemic and determined that they experienced severe (24%), moderate (22%), or mild anxiety (30%). Zhao et al. 27 also found that 37.4% of Chinese university students experienced anxiety during the COVID‐19 pandemic. The differences in results may be due to differences in regions of residence, infection and death rates and measures by country, and social and familial factors. As a result of the regression analysis performed in our study, our variable, which was significant in the model with moderate nicotine addiction, was found to be the person's anxiety level (Table 5). The possibility of nicotine addiction was found to be higher in those with high anxiety levels than those with low levels, and this finding is consistent with the literature and analysis.
Many adolescents smoke less than adults. However, adolescents who smoke, especially those who regularly smoke, experience nicotine dependence and withdrawal. 47 Participants had a mean FTND score of 2.7. More than half of them (65.2%) had low nicotine dependence (Table 4). Elbi et al. 42 and Provenzano et al. 16 also reported low nicotine dependence among more than half of university students. Chinwong et al. 47 looked into the prevalence of nicotine dependence in Thai university students and found that 71.7% of the male students (mean FTND = 2.3) and 88.4% of the female students (mean FTND = 1.8) had low nicotine dependence. 48
There is a correlation between anxiety and nicotine dependence.46, 49 In this study, it was found that as the anxiety levels of the students increased, the rate of nicotine addiction also increased (Table 5). Izadpanah et al. 49 found that young people with nicotine dependence had high anxiety. Zvolensky et al. 50 reported a moderate correlation between anxiety sensitivity and nicotine dependence among Latin smokers. Many smokers argue that smoking helps them cope with stress. Therefore, people who wanted to cope with stress during the pandemic turned to smoking. 10 The results showed that the participants were trapped in a vicious circle. On the one hand, they smoked more to reduce anxiety, but on the other hand, they experienced more anxiety as they feared that they would not be able to find or afford to buy cigarettes during the pandemic. Therefore, students should be informed about strategies to cope with stress and anxiety during pandemics.
5. CONCLUSION
There was a positive correlation between anxiety and nicotine dependence among smoking participants. The severity of nicotine dependence depended on the gender, family type, chronic disease, adaptation to social isolation, other smokers in the family, quality of relationship with family members, stockpiling packs of cigarettes, and anxiety about not being able to find or afford to buy cigarettes during the pandemic. The severity of anxiety depended on the gender, income, region of residence, activities at home during social isolation, other smokers in the family, quality of relationship with family members, increase in nicotine dependence, stockpiling packs of cigarettes, and anxiety about not being able to find or afford to buy cigarettes during the pandemic.
6. IMPLICATIONS FOR NURSING PRACTICE
Experts and parents should pay attention to young people concerning pandemic‐related physical and mental issues. Young people going through difficult times are more prone to substance and tobacco use. Therefore, online courses should address not only the subjects in the curriculum but also physical and mental issues and provide content to raise students' awareness of the dangers of substance and tobacco use. Telehealth services should be provided to university students. COVID‐19 pandemic has taken hold of the whole world rapidly and continues to change our lives drastically. Therefore, we need more studies with larger samples to examine its effects on substance and tobacco use among adolescents.
CONFLICT OF INTERESTS
The authors declare that there are no conflict of interests.
ACKNOWLEDGMENT
The authors would like to thank the university students who participated in the study.
Ayran G, Köse S, Küçükoğlu S, Aytekin Özdemir A. The effect of anxiety on nicotine dependence among university students during the COVID‐19 pandemic. Perspect Psychiatr Care. 2022;58:114‐123. 10.1111/ppc.12825
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- 1. Hussain A, Bhowmik B, do Vale Moreira NC. COVID‐19 and diabetes: knowledge in progress. Diabetes Res Clin Pract. 2020;162:108142. 10.1016/j.diabres.2020.108142 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Varvadas C, Nikitara K. COVID‐19 and smoking: a systematic review of the evidence. Tob Induc Dis. 2020;18:20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. COVİD 19 Data Portal Turkey . https://covid19.tubitak.gov.tr/dunyada-durumm. Accessed March 17, 2021.
- 4. Grubic N, Badovinac S, Johri AM. Student mental health in the midst of the COVID‐19 pandemic: A call for further research and immediate solutions. Int J Soc Psychiatry. 2020;66(5):517‐518. 10.1177/0020764020925108 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Cao W, Fang Z, Hou G, et al. The psychological impact of the COVID‐19 epidemic on college students in China. Psychiatry Res. 2020;287:112934. 10.1016/j.psychres.2020.112934 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Van Bortel T, Basnayake A, Wurie F, et al. Psychosocial efects of an Ebola outbreak at individual, community and international levels. Bull World Health Organ. 2016;94(3):210‐214. 10.2471/blt.15.158543 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Wang C, Zhao C. The impact of COVID‐19 on anxiety in Chinese university students. Front Psychol. 2020;11:1168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Kaparounakia CK, Patsalia ME, Mousaa DV, Papadopouloua E, Papadopouloua K, Fountoulakis K. University students' mental health amidst the COVID‐19 quarantine in Greece. Psychiatry Res. 2020;290:113111. 10.1016/j.psychres.2020.113111 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Arpacıoğlu S, Ünibol B. Investigation of changes in alcohol‐smoking usage and related situations in the coronavirus outbreak. Cyprus Turkish J Psychiatry Psychol. 2020;2(3):128‐138. [Google Scholar]
- 10. Tetik B, Tekinemre I, Taş S. The effect of the COVID‐19 pandemic on smoking cessation success. J Community Health. 2020.8 1‐5. 10.1007/s10900-020-00880-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Caponnetto P, Inguscio L, Saitta C, Maglia M, Benfatto F, Polosa R. Smoking behavior and psychological dynamics during COVID‐19 social distancing and stay‐at‐home policies: a survey. Health Psychol Res. 2020;8. 10.4081/hpr.2020.9124 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Fidancı İ, Aksoy H, Yengil Taci D, Ayhan Başer D, Cankurtaran M. Evaluation of the effect of the Covid‐19 pandemic on smoking addiction levels. Int J Clin Pract. 2021;75(5). 10.1111/ijcp.14012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Stanton R, To QG, Khalesi S, et al. Depression, anxiety and stress during covid‐19: associations with changes in physical activity, sleep, tobacco and alcohol use in Australian adults. Int J Environ Res Public Health. 2020;17(11):4065. 10.3390/ijerph17114065 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Yakar B, Öztürk Kaygusuz T, Pirincci E, Onalan E, Ertekin YH. Tıp fakültesi öğrencilerinin Türkiye'deki mevcut COVID‐19 salgını hakkında bilgi, tutum ve kaygıları. Fam Pract Palliat Care. 2020;36‐44. 10.22391/fppc.737469 [DOI] [Google Scholar]
- 15. Rakhmanov O, Dane S. Knowledge and anxiety levels of African University students against COVID‐19 during the pandemic outbreak by an online survey. J Res Med Dent Sci. 2020;8(3):53‐56. [Google Scholar]
- 16. Provenzano S, Santangelo OE, Grigis D, Giordano D, Firenze A. Smoking behaviour among nursing students: attitudes toward smoking cessation. J Prev Med Hyg. 2019;60:E203‐E210. 10.15167/2421-4248/jpmh2019.60.3.1049 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Spielberger CD, Gorsuch RC, Luschene RE. Manual for The State‐Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press; 1970. 10.1007/978-94-007-0753-5_2825 [DOI] [Google Scholar]
- 18. Öner N, Le Compte A. State‐Trait Anxiety Inventory Handbook. İstanbul: Boğaziçi University Publication; 1983. 10.1007/978-0-387-78665-0_6696 [DOI] [Google Scholar]
- 19. Heatherton TL, Kozlovski LT, Frecker RC, Fageström K. The Fagerström Test for Nicotine Dependence: a revision of the Fagerstrom Tolerance Questionnaire. Br J Addict. 1991;86(9):1119‐1127. [DOI] [PubMed] [Google Scholar]
- 20. Uysal MA, Kadakal F, Karşidağ C, Bayram NG, Uysal O, Yilmaz V. Fagerström Test for Nicotine Dependence: reliability in a Turkish sample and factor analysis. Tuberk Toraks. 2004;52:115‐121. [PubMed] [Google Scholar]
- 21. Karadoğan D, Önal Ö, Kanbay Y. Prevalence and determinants of smoking status among university students: Artvin Coruh University sample. PLoS One. 2018;13(12):e0200671. 10.1371/journal.pone.0200671 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Selçuk K, Avcı D, Mercan Y. Smoking addiction among university students and the willingness and self‐efficacy to quit smoking. Clin Exp Health Sci. 2018;8:36‐43. https://dergipark.org.tr/en/pub/aitdergi/issue/45818/578339 [Google Scholar]
- 23. Terzi Ö, Kumcağız H, Terzi M, Dündar C. Cigarette smoking and determination of nicotine dependence levels in university students. Addicta Turk J Addict. 2020;6(Supp4):168‐181. 10.5152/addicta.2020.19134 [DOI] [Google Scholar]
- 24. Mallet J, Dubertret C, Le Strat Y. Addictions in the COVID‐19 era: current evidence, future perspectives a comprehensive review. Prog Neuropsychopharmacol Biol Psychiatry. 2021;106:110070. 10.1016/j.pnpbp.2020.110070 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Tunç Z, Kolburan G. An investigation of the relationship between self‐esteem and smoking addiction in adolescence. Aydın J Hum Soc. 2019;5(1):55‐70. https://dergipark.org.tr/tr/pub/aitdergi/issue/45818/578339 [Google Scholar]
- 26. Wu J‐H, Du J‐K, Lee H‐E, Tsai T‐C. Effects of anxiety on dental students' noncognitive performance in their first objective structured clinical examination. The Kaohsiung J Med Sci. 2020;36(10):850‐856. 10.1002/kjm2.12231 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Zhao S‐J, Zhang L‐G, Wang L‐L, et al. Prevalence and socio‐demographic correlates of psychological health problems in Chinese adolescents during the outbreak of COVID‐19. Eur Child Adolesc Psychiatry. 2020;29:749‐758. 10.1007/s00787-020-01541-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Gao W, Ping S, Liu X. Gender differences in depression, anxiety, and stress among college students: a longitudinal study from China. J Affect Disord. 2020;263:292‐300. 10.1016/j.jad.2019.11.121 [DOI] [PubMed] [Google Scholar]
- 29. Islam K, Datta AK, Seth S, Roy A, DasJiao R. A study on the prevalence and correlates of nicotine dependence among adolescents of Burdwan Town, West Bengal. Indian J Psychiatry. 2019;61(1):89‐93. 10.4103/psychiatry.IndianJPsychiatry_112_18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Banzer R, Haring C, Buchheim A, et al. Factors associated with different smoking status in European adolescents: results of the SEYLE study. Eur Child Adolesc Psychiatry. 2017;26(11):1319‐1329. 10.1007/s00787-017-0980-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Hsu Y‐T, Kawachi I. Timing of family adversity during adolescence and its impact on alcohol and tobacco initiation: a longitudinal study among Taiwanese adolescents. Child Psychiatry Hum Dev. 2019;50(2):257‐267. 10.1007/s10578-018-0838-0 [DOI] [PubMed] [Google Scholar]
- 32. eKoronafobi . https://npistanbul.com/koronavirus/turkiyenin-koronafobi-haritasi. Accessed September 20, 2020.
- 33. Birinci M, Bulut T. Impact of COVID‐19 on social‐economically disadvantaged groups: an assessment from social work perspective. Turk J Soc Work. 2020;4(1):62‐68. [Google Scholar]
- 34. World Health Organization (WHO) . Novel coronavirus (2019‐nCoV): situation report. 2020. https://www.who.int/docs/default-source/coronaviruse. Accessed October 1, 2020.
- 35. Brooks SK, Webster RK, Smith LE, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. The Lancet. 2020;395(10227):912‐920. 10.1016/s0140-6736(20)30460-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Günay U. Youth in the epidemic period. In: Aylaz R, Yıldız E, eds. The Public Effects of Novel Coronavirus Disease and Nursing Approaches. Malatya: İnönü University Publishing House; 2020:83‐88. [Google Scholar]
- 37. Blasi MDI, Giardina A, Giordano C, et al. Problematic video game use as an emotional coping strategy: evidence from a sample of MMORPG gamers. J Behav Addict. 2019;8(1):25‐34. 10.1556/2006.8.2019.02 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Statista Coronavirus impact: global in‐home media consumption by country. 2020. https://www.statista.com/statistics/1106498/home-media-consumption-coronavirus-worldwide-by-country/. Accessed September 1, 2020.
- 39. Göker ME, Turan Ş. Covid‐19 Pandemisi Sürecinde Teknoloji Kullanımı Önerileri. Eskişehir Türk Dünyası Uygulama ve Araştırma Merkezi Halk Sağlığı Dergisi. 2020. 10.35232/estudamhsd.767526 [DOI] [Google Scholar]
- 40. Sarioglu N, Cuce C, Erel F, Kose M, Arslan M, Bodur AS. Smoking prevalance and affecting factors among Students of Balıkesir University. Eurasian J Pulmonol. 2016;18(1):29‐34. 10.30565/medalanya.615964 [DOI] [Google Scholar]
- 41. Oğuz S, Çamcı G, Kazan M. The prevalence of cigarette smoking and knowing status for diseases caused by smoking among university students. Van Med J. 2018;25(3):332‐337. 10.5505/vtd.2018.02411 [DOI] [Google Scholar]
- 42. Elbi H, Aktaş A, Rahman S, Altan S, Özyurt BC. Self‐reported prevalence of tobacco uses among university students; Including the Fagerstrom Test, among an University Students, Turkey. J Tepecik Educ Res Hosp. 2018. 10.5505/vtd.2018.02411 [DOI] [Google Scholar]
- 43. Kardeş V. Mental and behavioural evolution of during and after the pandemic. Turk J Diab Obes. 2020;2:160‐169. [Google Scholar]
- 44. Mavruk C, Kıral E. Subjective social isolation risks. Acad Elegance. 2019;6(12):491‐509. [Google Scholar]
- 45. Şen Ş, Sönmez CI, Ayhan Başer D. Anksiyete Sensitivitesinin Nikotin Bağımlılığı Ve Sigara Bırakma Başarısına Etkileri. Acta Med Alanya. 2020;4(1):29‐36. 10.30565/medalanya.615964 [DOI] [Google Scholar]
- 46. Söğüt S, Dolu İ, Cangöl E. The relationship between COVID‐19 knowledge levels and anxiety states of midwifery students during the outbreak: a cross‐sectional web‐based survey. Perspect Psychiatr Care. 2021;57(1):246‐252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Chinwong D, Mookmanee N, Chongpornchai J, Chinwong S. A comparison of gender differences in smoking behaviors, intention to quit, and nicotine dependence among Thai university students. J Addict. 2018;2018:8081670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Rujnan T, Çaykara B, Sağlam Z, Pençe HH. Sigara bağımlılarında depresyon, anksiyete, uykululuk ve uyku kalitesi düzeyleri arasındaki ilişkinin belirlenmesi. Acibadem Universitesi Saglik Bilimleri Dergisi. 2019. 10.31067/0.2019.212 [DOI] [Google Scholar]
- 49. Izadpanah M, Najafi M, Khosravani V. Anxiety in social interactions and nicotine dependence in nicotine‐dependent men: the role of metacognitions about smoking. Addict Behav. 2021;112:106656. [DOI] [PubMed] [Google Scholar]
- 50. Zvolensky M, Bakhshaiea J, Shepherda JM, et al. Anxiety sensitivity and smoking among Spanish‐speaking Latinx smokers. Addict Behav. 2019;90:55‐61. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.