

Abstract
Aims and objectives
To examine what was known about disaster preparedness in residential care and to consider this in the light of the current COVID‐19 pandemic.
Background
Care homes provide long‐term care to vulnerable, frail older people, as well as to young people with profound disabilities. The COVID‐19 pandemic has shown that the residential care sector has been seriously affected in many parts of the world and has exposed major flaws and vulnerabilities in infection control and other processes that have resulted in considerable loss of life of residents of these facilities.
Design
Discursive paper informed by a systematic literature. Review was carried out in line with PRISMA reporting guidelines. The review protocol was registered with PROSPERO on 2020 [CRD42020211847].
Results
The review identified six papers meeting inclusion criteria across care residential facilities in different countries. Several prevention and mitigation strategies were identified to manage and reduce the spread and severity of viral respiratory infection pandemics. These strategies include isolation, restriction of movement, personal protective and hygienic measures, health education and information sharing, monitoring and coordination, and screening and treatment. Preparedness strategies identified were contingency planning such as reporting/communication, leadership, human resource, insurance, occupational health and resource availability. The prevention/mitigation and preparedness strategies helped to achieve decline in disease severity, reduced prevalence, reduced spread of the disease, improved readiness criteria, resource usefulness and increased intervention acceptability. This paper presents a conceptual framework exploring the interconnectedness of preparedness and prevention/ mitigation strategies and associated outcomes. We discuss areas of concern in the context of workforce employment patterns in the sector. Concerns related to the unintended consequences of strategies placed on aged care facilities, which may worsen mental health outcomes for residents, are discussed.
Conclusions
Persons in residential care settings are at greater risk of infection during a pandemic, and therefore, strict measures to protect their safety are warranted. However, they are also a group who already experience social isolation and so any measures involving restrictions to visiting and social interaction, particularly over the longer term, must be accompanied by strategies to mitigate potential loneliness and mental health sequelae arising from long‐term pandemic restrictions.
Relevance to clinical practice
Though there was evidence of activity in preparedness for disasters within the residential care sector, various contextual factors affecting the sector were clearly not adequately considered or addressed in pre‐pandemic disaster planning, particularly in the areas of staff movements between care homes and the length of time that social isolation and restriction measures would need to be in place.
Future pandemic planning should consider the nature of the workforce model in the care home sector, and factor in strategies to better support the mobile and highly casualised workforce.
Keywords: aged care facilities, infection control, literature review, nursing homes, nursing home care, pandemics, residential care, review disaster nursing
What does this paper contribute to the wider clinical community?
In the current pandemic, persons in care homes were subjected to greatly restricted visiting causing potential exacerbation of social isolation in an already isolated population. Future planning should address the social and emotional needs of residents.
Many jurisdictions implemented centralised rapid response teams to support the care home workforce and residents when outbreaks occurred. The effects of these should be evaluated and considered in future planning.
1. INTRODUCTION
Care homes provide long‐term care to vulnerable, frail older people, as well as to young people with profound disabilities. Concerns about the nature and quality of care provided within these care homes have long caused concern for a range of reasons. These reasons include the complex care needs of residents, the nature of the workforce caring for them and the profit model that is used to frame the care home sector in many parts of the world (Davidson & Szanton, 2020; Report of the Aged Care Royal Commission 2021).
The nature of the populations in these care homes means that effective disaster preparation is essential. Writing a decade ago, Usher (2010) posed questions as to the disaster readiness of nurses and highlighted the importance of the readiness in a range of contexts. We argue that care homes are an important setting for pandemic readiness and preparation. The COVID‐19 pandemic has shown that despite great efforts by many, the care home sector has been seriously affected in many parts of the world and has exposed major flaws and vulnerabilities in infection control and other processes (Davidson & Szanton, 2020) that have resulted in considerable loss of life of residents of these facilities. In Victoria, Australia, for example, the majority of deaths from COVID‐19 were in care homes (Cousins, 2020).
In the light of the exposed vulnerability of care home residents, we undertook a review of the literature to examine what was known about disaster preparedness in care homes and to consider this in the light of the current COVID‐19 pandemic. From this, we aim to produce recommendations to inform policy and practice in this crucial area.
2. BACKGROUND
COVID‐19 has rapidly spread across the globe affecting large numbers of people (Centers for Disease Control & Prevention, 2021). At the time of writing, there have been 30 million recorded cases of COVID‐19 globally and approximately 1,000,000 deaths (Dong et al., 2020). In the early months of COVID‐19, there were reports that a proportion of deaths were centred on residents in care homes, and this was noted in several countries (Thompson et al., 2020). This pattern of loss of life continued with deaths disproportionately affecting vulnerable residents (Comas‐Herrera et al., 2020). In April 2020, reports suggest that half the residents of a care home in Canada died due to COVID‐19 (Cecco, 2020). The following month, a care home in New York reported the death of 98 residents due to COVID‐19 (Mustian, 2020). At the same time, Spain, Italy, Sweden and Belgium reported the disproportionate deaths of older people in care homes (The Guardian, 2020). In the same month, early international evidence from the Centre for Disease Control and Prevention found staff mobility across multiple facilities, and staff working whilst symptomatic, lack of training and limited availability of testing all contributed to higher infection and mortality rates in care homes (Comas‐Herrera et al., 2020). The disaster facing care homes was clear when the pandemic was declared by the World Health Organisation (Cousins, 2020).
Strategies to prevent the spread of pandemic influenza such as compliance with social distancing and adherence to stringent infection control practices are important measures in limiting community transmission of COVID‐19. The World Health Organisation (WHO) further outlined its strategic objectives, which were for infected patients (residents) to be identified early, isolated and provided with optimised care (World Health Organization, 2020).
This review will systematically examine and synthesise the evidence on prevention, mitigation, preparedness, response and recovery plans of care homes. A comprehensive search for the published articles was conducted in the following databases: PsycINFO (ProQuest), CINAHL Complete; PubMed; Informit and Google Scholar. This review is reported in line with the PRISMA reporting guidelines (Moher et al., 2009) The PRISMA reporting checklist is provided in File S1.
2.1. Aims and objectives of the review
The following research questions were established for the review:
What are the most commonly applied prevention and mitigation strategies for viral respiratory infection pandemics within long‐term care facilities, nursing homes and aged care facilities?
What are the most commonly applied preparedness strategies for viral respiratory infection pandemics within long‐term care facilities, care homes and aged care facilities?
What are the most effective responses to viral respiratory infection pandemics within long‐term care facilities, care homes and aged care facilities?
2.2. Design
The review protocol was registered with PROSPERO on 29 September 2020 [CRD42020211847] and was carried out in line with the PRISMA reporting guidelines (Moher et al., 2009). The systematic review method provides a way to identify relevant studies, summarise and critically analyse the results and recommend improvements and areas for further research. Upon review of the results of this review, the authors discussed the absence of consideration for the mental health outcomes of residents in aged care facilities as a result of presentation and mitigation strategies, nor discussion or investigation as to the implications of the workforce models. These issues, which are relevant in the context of the COVID‐19 pandemic, are highlighted in this paper.
2.3. Inclusion and exclusion criteria
Inclusion criteria were as follows: primary studies reported in English focusing on the population (i.e. nurses or care home residents) (condition) who have been exposed to/or at risk of viral respiratory infection pandemic or have researched their pandemic preparedness response. Exclusion criteria were as follows: seasonal influenza/flu (non‐pandemic); other pandemics, for example Ebola; and discussion or opinion pieces with no primary data (Table 1).
TABLE 1.
Inclusion and exclusion criteria for selecting articles
| Inclusion criteria | Exclusion criteria |
|---|---|
|
|
2.4. Search strategy
A comprehensive search for the published articles was conducted in the following databases: PsycINFO (ProQuest), CINAHL Complete; PubMed; Informit and Google Scholar. The search terms used in all databases were as follows: (("care home" OR "nursing homes") OR ("care home" OR "care homes") OR "long term care" OR "residential care" OR "aged care") AND (pandemic* OR epidemic* OR outbreak* OR "public health emergen*" OR covid‐19 OR coronavirus) AND (mitigation OR respons* OR recovery OR prepared* OR readiness OR effective* OR education OR training). The limiters applied were as follows: Date; 2000–2020 Peer Reviewed; Scholarly Journals.
2.5. Study selection and outcome
A total of 203 studies were identified from the database searches with an additional two studies identified through hand searching. Following the search, all identified citations were collated and uploaded into EndNote X9 (2020) version and duplicates were removed. All authors participated in the title screening of 203 studies. Full‐text screening of 27 studies was also completed by all authors. A total of 20 studies were excluded at full‐text screening as they did not meet the inclusion criteria. A total of 6 studies are included in this review, and the process undertaken is outlined in Prisma flow chart (Figure 1). Data extraction was undertaken for 7 included studies and is presented in Table 2: table of included studies with characteristics. These papers were published over the period 2003–2020.
FIGURE 1.
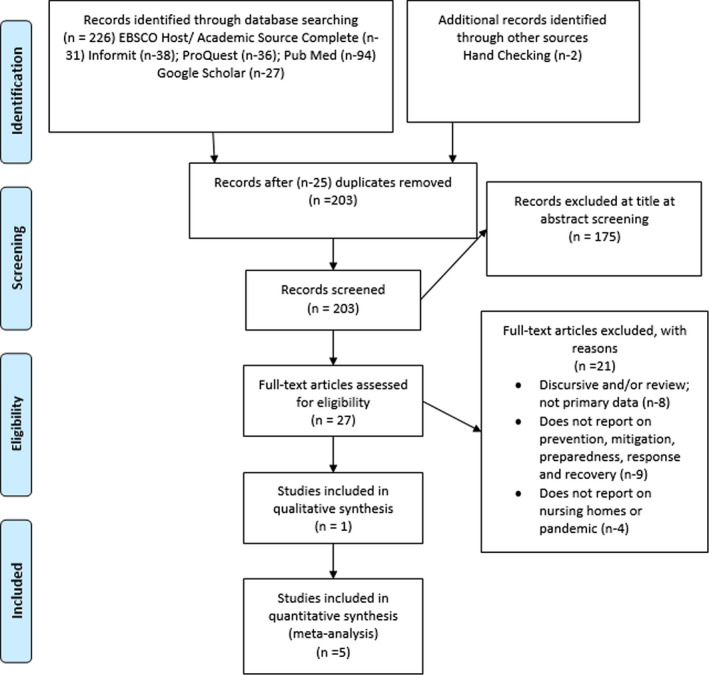
Prisma flow chart
TABLE 2.
Table of included studies with key characteristics
| Author, Year and Country | Aim | Design | Methods | Participants | Pandemic | Results |
|---|---|---|---|---|---|---|
| Affifi et al. (2012), Saudi Arabia | To describe and evaluate the epidemiological characteristics of a confined influenza A (H1N1) outbreak that involved a cluster of LTCF residents in PMMH during the 2010 influenza season, and to show the prevention and control measures taken | Not reported | Quantitative | Twenty‐one residents of a long‐term care facility (LTCF) (13 males, 8 females; male: female ratio 1.6:1). | H1N1 | Several prevention/mitigations strategies such as isolation, movement restrictions, wearing protective materials, observing hygienic measures, monitoring and coordination were implemented. This led to a decline in prevalence and disease severity. |
| Eastwood et al. (2008), Australia | To improve the capacity of residential aged care facilities (RACFs) to respond to communicable disease outbreaks and to determine changes in outbreak response preparation against 19 readiness criteria. | An interventional computer‐assisted telephone interview approach | Quantitative | Of 124 RACFs managers invited to participate in the study, 111 (90%) completed i‐CATI 1, and 108 (87% of all RACFs) completed i‐CATI 2 and i‐CATI 3. | Preparedness for pandemic influenza | Preparedness strategies such as reporting detected respiratory or gastroenteritis outbreak and keeping communicable disease surveillance registers were undertaken improving readiness to respond to pandemic influenza |
| Fell (2008), UK | To inform relevant agencies and ensure appropriate support and advice is given to the sector locally; especially in the context of the DH guidance on pandemic flu for this sector | Rapid assessment | Qualitative | n = 15 managers of aged care and nursing homes | Preparedness for pandemic influenza | Some health education and information sharing programmes were undertaken, and also, preparedness strategies regarding staff shortages, leadership, clinical support and insurance were considered. |
| Mills et al. (2020), USA | To describe the methods the organisation has developed to mitigate the spread of COVID−19 in ALFs, and we present an initial evaluation of this innovation. | Interventional study | Quantitative | n = 1794 residents of 101 assistant living facilities | COVID−19 | The facilities employed prevention/mitigation strategies such as isolation, health education and information sharing, screening, and treatment leading to the reduction in prevalence and disease severity. Also, some preparedness strategies such as leadership and resources were undertaken. |
| Mimi et al. (2003), Hong Kong | To explore the knowledge and understanding of SARS in the older people and to elicit the prevention and precautionary measures taken by the older people and by nursing homes to keep the disease under control and lessen the death toll of the older people in particular. | Descriptive qualitative study | Qualitative | 27 healthcare workers (3 men and 24 women) and 40 older people (33 female and 7 male) residents of nursing homes | SARS | The prevention/mitigation strategies taken to keep the disease under control were movement restrictions, isolation, wearing protective materials, observing hygienic measures, health education and information sharing. |
| Siu et al. (2020), Canada | To examine the LTC clinician perspective on the preparedness and engagement of the LTC sector during the COVID−19 pandemic. | Cross‐sectional survey | Quantitative | 294 long‐term care clinicians. | COVID−19 | The prevention/mitigation measures implemented in the LTC homes were isolation, wearing protective materials, observing hygienic measures, health education and information sharing, screening and treatment, monitoring, and coordination. Also, the homes sought advice and guidance from the local public outbreak preparedness and action committee for future spread. |
2.6. Data extraction
Data from each of the articles were documented using a data extraction form developed in consultation with all authors. The form consisted of sections related to the study particulars, objective, methodology, findings, recommendation and any additional, relevant, information. Findings were extracted based on the questions posed by the review. One author (NG) extracted data from all the included studies using the form, and this was checked independently by another author (SW). The resultant extraction was shared with the first author (KU) for verification and discussion.
2.7. Quality appraisal
The quality of the studies included in this review was assessed using the Mixed Method Appraisal Tool [MMAT]. Two of the authors independently appraised the quality of the studies using five quality criteria on the MMAT. The assessment procedure involves the following: (1) SW independently assessed the quality of all the studies. (2) The studies were assessed independently by NG. Any discrepancies between the authors were resolved through discussion with the involvement of a third author (DJ). The scores of the studies were calculated by counting and expressing as a percentage the total number obtained by each study. All the studies obtained 86 and above scores and were awarded high quality (Appendix 1).
2.8. Data analysis
The review aimed to identify the prevention/mitigation strategies, preparedness strategies and the effective response employed by care homes to manage viral respiratory infection pandemics. The data were not suitable for statistical analysis; therefore, the data were analysed manually using thematic analysis adapted from Braun and Clarke (2013). The analysis involved reviewing and familiarising with the extracted data, generating initial codes, searching for themes, reviewing and grouping themes, and rigorous interpretation of data to form a conceptual framework. Specifically, an initial coding frame using the research objectives was developed. The data were reviewed extensively for themes related to the research objectives. The identified themes were then grouped and regrouped into a revised set of inter‐related themes and subthemes to form a synthesised conceptual framework.
3. RESULTS
3.1. Study characteristics
Table 2 presents the summary of key characteristics of the 6 studies included in the review. The studies were conducted in six countries: Saudi Arabia, Australia, the UK, the USA, Hong Kong and Canada. More than half of the studies (4/6; 67%) used quantitative methods. The remaining two adopted qualitative methods. The research designs employed were interventional (2/6; 33%), cross‐sectional (1/6; 17%), rapid assessment (1/6; 17%) and descriptive (1/6; 17%). One study did not report on the design. Some of the viral respiratory infection pandemics identified were H1NI influenza (1/6; 17%), COVID‐19 (2/6; 33%) and SARS (1/6; 17%). Two studies were conducted on the general pandemic influenza virus. Half (3/6; 50%) of the studies were conducted with clinicians/managers. Also, two of the studies were conducted with residents. One study was on both residents and professionals.
The prevention and mitigation strategies presented in this section are as follows: isolation, restriction of movement, personal protective and hygienic measures, health education and information sharing, monitoring and coordination, and screening and treatment. The preparedness strategies identified are examined in terms of as contingency planning. This review highlights that prevention/mitigation strategies and preparedness strategies do not have a linear relationship with each other. The two strategies overlap, coexist and support each other.
3.2. Viral respiratory infection/disease outbreaks
The review identified several viral respiratory infection pandemics across care homes in different countries. The included studies addressed influenza A (H1N1) outbreak in Saudi Arabia (Affifi et al., 2012), response to communicable disease outbreaks in Australia (Eastwood et al., 2008), preparedness towards pandemic flu in the UK (Fell, 2008), mitigating the spread of COVID‐19 in the USA (Mills et al., 2020), prevention and precautionary measures to respond to SARS in a Hong Kong Nursing Home (Mimi et al., 2003) and preparedness and engagement of long‐term care (LTC) to COVID‐19 pandemic in Ontario, Canada (Siu et al., 2020).
Different proportions of viral respiratory infection pandemics were recorded in three of the care homes studied. For example, Affifi et al. (2012) reported that 47.7% (21/44) of patients staying in the care facility had suspected influenza A (H1N1) within five days during the outbreak in Saudi Arabia. However, laboratory results indicated that 12 of the 21 (57.1%) patients tested H1N1 PCR‐positive, and 9 (42.9%) tested negative. Similarly, Mills et al. (2020) reported that seven individuals in some selected care homes (0.4% of census) tested positive for SARS‐CoV‐2 by nucleic acid test, during the COVID‐19 outbreak in the USA. Finally, Eastwood et al. (2008) reported that 17 (15%) facilities reported a total of 61 outbreaks of respiratory infection in 2004 as part of a response to communicable disease outbreaks in Australia. Similarly, 44 (40%) of the facilities reported a total of 111 outbreaks of gastroenteritis. Moreover, between July–September 2005, 18 (17%) of the facilities reported a total of 23 respiratory outbreaks (Eastwood et al., 2008).
4. CONCEPTUAL FRAMEWORK EXPLAINING THE INTERCONNECTEDNESS OF PREPAREDNESS AND PREVENTION/MITIGATION STRATEGIES
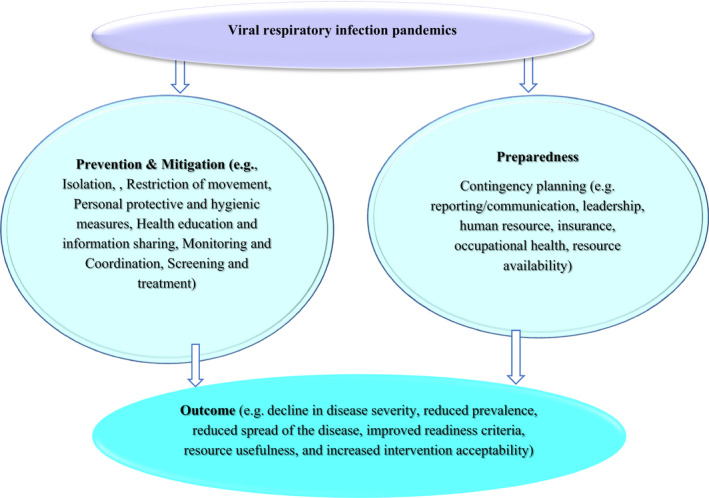
Figure 2 illustrates a conceptual framework explaining the interconnectedness of prevention/mitigation and preparedness strategies (independent variables) and their relationship with the outcome (dependant variables). The proposed framework suggests that the prevention/mitigation, as well as preparedness strategies for viral respiratory infection pandemics, could have a significant impact on the management outcomes or response. For example, the prevention/mitigation strategies could yield an outcome such as a decline in disease severity, reduced prevalence and reduced spread of the disease. Similarly, preparedness strategies could result in an impact on the management outcome of viral respiratory infection pandemics (e.g. improved readiness criteria, resource usefulness). However, the independent variables (prevention/mitigation and preparedness) do not have a linear relationship with each other. The two strategies overlap, coexist and support each other. As shown in Figure 1, prevention and mitigation activities (e.g. isolation, restriction of movement, personal protective and hygienic measures, health education and information sharing) during viral respiratory infection pandemics are likely to be considered during the preparedness activities. The strategies are interconnected and could be implemented simultaneously.
FIGURE 2.
Conceptual framework explaining the interconnectedness of preparedness and prevention/ mitigation strategies
5. PREVENTION/MITIGATION
The synthesis identified several preventive and mitigation strategies to manage and reduce the spread and severity of viral respiratory infection pandemics. The preventive and mitigation strategies were categorised into isolation (Affifi et al., 2012; Mills et al., 2020; Mimi et al., 2003; Siu et al., 2020), restriction of movement (Affifi et al., 2012; Mimi et al.), personal protective and hygienic measures (Affifi et al., 2012; Mimi et al., 2003; Siu et al., 2020), health education and information sharing (Fell, 2008; Mills et al., 2020; Mimi et al., 2003; Siu et al., 2020), monitoring and coordination (Affifi et al., 2012; Mills et al., 2020; Siu et al., 2020), and screening and treatment (Affifi et al., 2012; Eastwood et al., 2008; Mills et al., 2020; Siu et al., 2020).
5.1. Isolation
The reviewed studies identified isolation as a prevention and mitigation strategy for viral respiratory infection pandemics. Isolation was conceptualised as a measure used to maintain physical distance in the care homes in a quest to preventing the spread of infection. Four studies identified residents and professionals been isolated during respiratory viral pandemics explained this measure. For example, whilst symptomatic individuals during influenza A (H1N1) in Saudi Arabia were isolated from other patients (Affifi et al., 2012), symptomatic employees during COVID‐19 in Ohio were isolated at home, tested for COVID‐19 and waited until they met the Center for Disease Control and Prevention return to work criteria for healthcare workers (Mills et al., 2020).
Also, Mimi et al. (2003) indicated that during the SARS outbreak in Hong Kong, residents who returned from the hospital after a follow‐up appointment or on discharge from the hospital following medical treatment stayed in an isolated room in the nursing home for 14 days. Also, Siu et al. (2020) reported that established isolation protocols were instituted for respiratory conditions, whilst the sick staff was encouraged to take time off work for LTC homes in Ontario Canada during COVID‐19.
5.2. Restriction of movement
The findings revealed strategies used to guard visitors during influenza A (H1N1) in Saudi Arabia and the SARS outbreak in Hong Kong to stop the spread of viral respiratory infection pandemics. These measures involved temporary closure of facilities to visitors and restricting visiting hours per day. For example, Affifi et al. (2012), reporting on a single facility, noted there was temporal closure of the facility to new admissions and visitors for some specified period and a gradual release of the ban on visitors guided by a daily assessment of outbreak progress (Affifi et al., 2012), whereas during the SARS outbreak in Hong Kong, visiting hours were shortened to 6 hours per day. Again, letters were sent to all visitors urging them to refrain from visiting nursing homes if they experienced any of the signs and symptoms of the SARS (Mimi et al., 2003).
5.3. Personal protective and hygienic measures
Personal protective and hygienic measures were operationalised as practices that meet public health rules to stop the spread of viral respiratory infection pandemics. Two of the studies highlighted that the personal protective equipment used to stop the spreading of illness was wearing a protective gown/clothing, gloves, facemask and surgical masks (Mimi et al., 2003; Siu et al., 2020). For example, Mimi et al. (2003) reported that staff had to use strict personal protective equipment (e.g. wearing a protective gown, gloves and facemask, surgical mask in handling isolated residents) whilst all visitors were required to wear surgical masks, during the SARS outbreak in Hong Kong. In particular, escorted staff wore protective clothing and changed their clothing before returning to work at the nursing home (Mimi et al., 2003). Similarly, Siu et al. (2020) reported that there was increased availability of personal protective equipment (PPE) 127 (79.4%) during the COVID‐19 outbreak in Ohio, USA.
Also, personal hygienic practices identified from the reviewed studies were the use of disinfectants to clean hands (Mimi et al., 2003), hand sanitising (Siu et al., 2020), and cough etiquette or droplet precautions (Affifi et al., 2012). Specifically, Mimi et al. (2003) indicated that disinfection agents for handwashing and cleaning were provided and that all visitors were required to use disinfectants to clean their hands when they arrived at the nursing home during the SARS outbreak in Hong Kong. The hygienic procedures in the nursing home environment were satisfactory, and the environment was perceived to be less risky compared with the general hospital (Mimi et al., 2003). In a related finding, Siu et al. (2020) suggested increased availability of hand sanitiser 132 (82.5%) during COVID‐19 in Ohio, USA. Also, Affifi et al. (2012) concluded that appropriate hand hygiene, cough etiquette standard and droplet precautions were reinforced and intensified during influenza A (H1N1) in Saudi Arabia.
5.4. Health education and information sharing
The reviewed studies identified health education and information sharing practices used to prevent and/mitigate the spread of viral respiratory infection pandemics in nursing homes. Health education and information sharing in this context were defined as the process of receiving or imparting knowledge, skills, attitudes and beliefs of the respiratory viral infection to stakeholders. Four studies identified some measures such as increasing formal and informal education on the viral respiratory infection pandemics (Siu et al., 2020) and systematic communication of information on outbreak advice/mitigation guidance to stakeholders such as staff, residents and visitors (Fell, 2008; Mills et al., 2020; Mimi et al., 2003). For example, Mills et al. (2020) highlighted that both formal and informal education and mitigation guidance were provided during COVID‐19 in Ohio, USA. In particular, all home‐based primary care (HBPC) practitioners and support staff participated in educational sessions, which were developed by the outbreak committee and practice medical director (Mills et al., 2020). In a related finding, Siu et al. (2020) reported an increased staff education about infection control processes (83.1%, 133/160) in Ontario, Canada. Similarly, Mimi et al. (2003) indicated that more in‐service training, such as tailored education for the residents of elderly care homes, was important during the SARS outbreak in Hong Kong. For example, nurses from the Hong Kong Hospital Authority and outreach nurses were invited to give a health talk to residents and staff on SARS prevention (Mimi et al., 2003).
Furthermore, three studies reported that systematic sharing or communication of information (e.g. through letters and advice sources) to stakeholders was used to prevent and mitigate the spread of viral respiratory infection. Specifically, Fell (2008) recommended that systematically communicating information about flu pandemic (clinical, public health and business continuity) with nursing homes was seen as critical—both pre‐ and during the pandemic flu in the UK. Also, staff and LTC stakeholders (68.8%) working at LTC homes in Canada were increasingly updated about COVID‐19 (Siu et al., 2020). Conversely, Mills et al. (2020) concluded that infection control procedures/ mitigation guidance such as sharing COVID‐19 materials to all ALF partners recognised as an enabler to suppress infection rates in assisted living facility (ALF) residents.
5.5. Monitoring and coordination
Several studies identified monitoring and coordinating as a strategy to prevent and mitigate the spread of viral respiratory infection pandemics. The monitoring and coordinating were explained as any means by which stakeholders keep track of and facilitate the prevention/mitigation of respiratory viral infection pandemics. Specifically, four studies demonstrated that measures such as continuous liaison/coordination with stakeholders(Affifi et al., 2012; Siu et al., 2020), notification of local/regional public health authority or health department (Eastwood et al., 2008; Mills et al., 2020) and established surveillance plan (Affifi et al., 2012) were used to prevent and mitigate the viral respiratory infection pandemics. For example, whilst the ALF notified the health department for each positive case during COVID‐19 in the USA (Mills et al., 2020), only three residential aged care facilities (RACFs) voluntarily notified the public health unit of a respiratory outbreak in response to communicable disease outbreaks in Australia (Eastwood et al., 2008). Similarly, Siu et al. (2020) indicated that whilst there was active coordination with public health officials (133, 83.1%) and with acute care (5.3%, 2/38) during COVID‐19 in Ontario, Canada, Mills et al. (2020) revealed that assisted living facilities in Ohio implemented any COVID‐19 guidance in collaboration with the health department. Also, Affifi et al. (2012) concluded that there was a continuous liaison with the local public health authority regarding new case notification, laboratory results and daily case progress reporting during influenza A (H1N1) outbreak in Saudi Arabia. Finally, Affifi et al. (2012) reported that coordinated efforts such as a surveillance plan was established to monitor active daily surveillance for all suspected H1N1 patients, including clinical evaluation, vital signs and O2 saturation. The surveillance plan aimed at preventing and mitigating the spread of the viral respiratory infection pandemics.
5.6. Screening and treatment
The reviewed studies identified screening and treatment as a potential strategy to prevent and mitigate the spread of viral respiratory infection pandemics. In particular, four studies indicated that examples of these strategies were active screening or regular diagnostic testing (staff, visitors, new admission and residents) (Mills et al., 2020; Siu et al., 2020), vaccination and immunisation of staff and visitors if there is an available vaccine (Affifi et al., 2012; Eastwood et al., 2008) and considering laboratory‐confirmed cases for full treatment (Affifi et al., 2012). Specifically, Siu et al. (2020) demonstrated that whilst active screening of new LTC admissions (90.0%, 144/160) and passive screening of visitors and staff (Siu et al., 2020) were instituted during COVID‐19 in Ontario, Canada, Mills et al. (2020) indicated a cloud‐based, mobile‐enabled, symptom‐screening application was developed to promote self‐screening of all employees to record their temperature daily and answer simple screening questions. This was implemented to prevent employees from coming to work sick. Also, regular diagnostic testing of all visiting practitioners was instituted using a ‘2‐pronged’ approach that includes nasopharyngeal swab for SARS‐CoV‐2 nucleic acid to diagnose acute infection for those who are acutely symptomatic (Mills et al., 2020). Again, rapid POC test was performed for asymptomatic employees for IgM and IgG antibodies against SARS‐CoV‐2 to determine recent or past infection (Mills et al., 2020). Eastwood et al. (2008) reported that whilst the proportion of RACFs actively promoting staff vaccination increased from 81–91% between i‐CATI 1 and i‐CATI 2 in response to communicable disease outbreaks in Australia, Affifi et al. (2012) recommended reviewing seasonal and H1N1 influenza immunisation status of LTCF patients and staff, as well as immunising those not protected with specific available vaccine during influenza A (H1N1) outbreak in Saudi Arabia.
6. PREPAREDNESS
Preparedness strategies were conceptualised as actions or intended actions that ensure the availability of resources necessary to carry out an effective response that aimed at stopping the spread of viral respiratory infection in the future. The preparedness strategies were centred on contingency planning in response to viral respiratory infection (Eastwood et al., 2008; Fell, 2008; Mills et al., 2020; Siu et al., 2020).
6.1. Contingency planning
Contingency planning as a preparedness strategy is an action plan designed to assist care homes to respond effectively to a future outbreak of respiratory viral infection pandemics. Several studies highlighted that contingency planning was carried out in areas such as reporting/communication needs (e.g. communicable disease surveillance registers, communicable disease outbreak plan) (Eastwood et al., 2008; Mills et al., 2020; Siu et al., 2020), human resource (e.g. responding to staff shortage), increased clinical needs, occupational health, leadership (e.g. outbreak preparedness and action Committee) and insurance (Fell, 2008; Siu et al., 2020).
Specifically, three studies reported that the care homes expressed their preparedness to communicate/report/notify new viral respiratory infection, as well as recording into communicable disease surveillance registers (Eastwood et al., 2008; Mills et al., 2020; Siu et al., 2020). For example, Eastwood et al. (2008) reported that care homes (74%) were prepared to notify the public health unit (PHU) if they detected a respiratory or gastroenteritis outbreak in response to communicable disease outbreaks in Australia. Also, communicable disease surveillance registers were in place as readiness criteria for outbreak management (Eastwood et al., 2008). The surveillance register contained information such as personal identification details, date of disease onset, resident symptoms and location of resident in the facility. Other practices were making available outbreak preparedness plans. In a related finding, Mills et al. (2020) indicated that the care homes built a secure, cloud‐based Web application to capture confirmed cases and potential exposures, during COVID‐19 in Ohio. The Web application auto‐notified entry of new patient cases to help the clinical team and administrative teams to plan and train staff on necessary isolation and infection control procedures (Mills et al., 2020). Also, over 120 COVID‐19 action resource materials were deployed during COVID‐19 in Ohio. Such resource library was posted to the organisational intranet, and updates were also communicated by email to the organisation 3 times per week (Mills et al., 2020).
Three studies demonstrated that there were proactive planning and assumptions/expectations in areas such as leadership, workforce shortage, increased clinical needs, occupational health issues and insurance. For example, Fell (2008) concluded that it was unclear about who is in charge concerning flu pandemic; however, it was recommended that either the Director of Public Health or Director of Adult Social Services was responsible for contingency planning in preparedness towards pandemic flu in the UK. Similarly, Mills et al. (2020) reported that during the COVID‐19 outbreak in Ohio, a cross‐functional team of leaders was assembled to form an Outbreak Preparedness and Action Committee. Such leadership planning was implemented to develop a comprehensive preparedness plan and served as a means of consolidating internal and external communications regarding COVID‐19 questions, planning and response.
Furthermore, Fell (2008) identified several planning assumptions in preparedness towards pandemic flu in the UK. These assumptions were anticipated staff shortages during a pandemic (e.g. reliant on bank or agency staff to cover workforce shortfalls), occupational health (staff coming to work whilst symptomatic) and high‐quality continuity planning as possible insurance to limit loss in the event of a pandemic. Finally, Fell (2008) highlighted the need to provide additional clinical support in care homes for symptomatic residents who were unable to be admitted to the hospital.
7. OUTCOME/EFFECTIVE RESPONSES
The synthesis identified several outcomes of the prevention/mitigation and preparedness strategies used to manage and reduce the spread and severity of viral respiratory infection pandemics. Several of the reviewed studies highlighted that the strategies yielded outcomes such as a decline in disease severity(Affifi et al., 2012; Mills et al., 2020), perceived reduced prevalence(Affifi et al., 2012; Mills et al., 2020), reduced spread of the disease (Affifi et al., 2012), improved readiness criteria (Eastwood et al., 2008), resource usefulness (Eastwood et al., 2008), increased intervention acceptability (Eastwood et al., 2008; Mills et al., 2020; Siu et al., 2020), perceived feasibility and enabler of intervention to reduce the spread of viral respiratory infection.
Two studies suggested a decline in disease severity after implementing viral respiratory infection prevention and mitigation strategies. In particular, Affifi et al. (2012) reported that prevention and mitigation practices during the influenza A (H1N1) outbreak in Saudi Arabia yielded several positive outcomes such as a steady decline in the disease severity, shortened primary attack rate, absence of secondary attacks and no spread of the disease from the isolation areas to the other facility wards throughout the outbreak. Similarly, Mills et al. (2020) concluded that COVID‐19‐positive ALF residents who did not require hospitalisation were able to isolate in their room and recover with symptomatic support. Herein, a highly coordinated and frequently communicated approach to infection control, employee screening and visitor management was perceived to enable suppression of COVID‐19 in ALFs.
Furthermore, Eastwood et al. (2008) concluded that RACFs reported a marked improvement against the 19 readiness criteria (e.g. surveillance register components, outbreak plan components) in response to communicable disease outbreaks in Australia. Again, Eastwood et al. (2008) reported that whilst interventions aimed at responding to communicable disease outbreaks were considered this ‘very acceptable’ (54%, 58 of 108), Siu et al. (2020) concluded that 54.4% (87/160) agreed that the recommendations were feasible for LTC, though 76.3% (122/ 160) agreed with such recommendations. Finally, Mills et al. (2020) demonstrated that in the first 100 days of the COVID‐19 outbreak in the USA, HBPC‐led outbreak mitigation was perceived as an enabler to suppress COVID‐19 infection rates in ALF residents.
8. DISCUSSION
Though there was evidence of activity in preparedness for disasters within the care home sector, various contextual factors affecting the sector were clearly not adequately considered or addressed in pre‐pandemic disaster planning. Care homes internationally have been affected by the COVID‐19 pandemic (Thompson et al., 2020), and this is in line with issues around infection control in the sector generally (Davidson & Szanton, 2020). Barnett and Grabowski (2020) reported that in the USA, of 2590 nonfoodborne outbreaks of norovirus during 2009–2012, 80% occurred within the long‐term care sector, highlighting the vulnerability of care home residents to the rapid spread of infection with serious results to residents. These same authors highlight that issues unique to the care home sector make residents not only more susceptible to contracting infection but also more vulnerable to serious complications including death. These unique issues include high levels of chronicity and functional impairment, the proximity between residents and structural issues including lack of facilities for effective quarantine (Barnett & Grabowski, 2020; Davidson & Szanton, 2020).
Findings of this review highlight some areas of concern that should be considered in future pandemic preparation. One of the major factors to be considered concerns the workforce employment patterns in the sector. The nursing home sector in many countries features high levels of casualisation of non‐nursing personnel, factors influencing staff behaviour and levels of risk associated with pandemic.
Whilst some authors (Siu et al., 2020) suggested that sick staff be encouraged to take time off work during the COVID‐19 pandemic, many staff may not have access to paid sick leave entitlements (Barnett & Grabowski, 2020), meaning they may be pressured to continue to work whilst unwell (Comas‐Herrera et al., 2020). Furthermore, the sector often does experience recruitment issues, and this is likely acutely exacerbated if numbers of staff are absent due to quarantine (Barnett & Grabowski, 2020).
The nature of the care home sector means that staff may work in several facilities on a casual basis. In Australia during the current pandemic, entrenched and extensive casualisation of the workforce meant that some workers carried COVID‐19 in and between facilities (Crotty et al., 2020; Pollock et al., 2020). Initially, there was a lack of screening of all persons entering facilities and no data gathered about staff movements and other work they were doing, meaning that vulnerable residents, as well as co‐workers, were put at risk (Crotty et al., 2020). Issues around staff mix with very few registered nurses also meant that care home staff may have inadequate familiarity and literacy with infection control measures including handwashing and use of personal protective equipment (Barnett & Grabowski, 2020). During the current pandemic, some jurisdictions tried to mitigate the lack of staff (due to quarantine) and lack of knowledge of infection control through the formation of rapid response teams, dispatched to care home settings with active COVID‐19 cases, to support staff in meeting resident care and safety needs (Chang, 2020; Cornwall, 2020; Washington State Department of Health & Social Services, 2020). During the current pandemic, access to care home settings has been greatly reduced in many jurisdictions (Australian Government, 2020), compromising the social and emotional welfare of residents (Barnett & Grabowski, 2020) and the guidelines for infection prevention and control do not adequately address the movement of staff between long‐term or aged care facilities (Rios et al., 2020).
This review identified that restriction or cessation of visitors to aged care facilities was an effective strategy to suppress the virus (for examples, see Affifi et al. (2012) & Mimi et al. 2003); however, the impact of the isolation these restrictions cause was not addressed and needs further examination. Lockdowns and other social distancing measures placed on already isolated individuals in aged care facilities may worsen mental health outcomes, increasing anxiety and causing major depressive disorders (Domènech‐Abella et al., 2019).
9. RECOMMENDATIONS AND RELEVANCE TO CLINICAL PRACTICE
Though there was evidence of activity in preparedness for disasters within the care home sector, various contextual factors affecting the sector were clearly not adequately considered or addressed in pre‐pandemic disaster planning. Future pandemic planning should consider the nature of the workforce model in the care home sector, and factor in strategies to better support the mobile and highly casualised workforce.
Many jurisdictions implemented centralised rapid response teams to support the care home workforce and residents when outbreaks occurred. The effects of these should be evaluated and considered in future planning. Finally, we recommend registered nurses be present in all care home settings to support adequate pandemic planning and preparation, and ensure that all staff has an adequate working knowledge of infection control measures including handwashing and use of personal protective equipment.
10. LIMITATIONS OF THE REVIEW
The COVID‐19 pandemic has highlighted new issues not reflected in the extant literature. The pandemic meant persons in care homes had greatly restricted visiting causing potential exacerbation of social isolation in an already isolated population. Future planning and research should address the social and emotional needs of residents.
Due to the timeline imposed on this review, we were unable to provide a comprehensive search of grey literature that may have yielded further information on preventative and preparedness strategies employed by care homes. However, whilst these documents may have provided guidance, the efficacy of these measures in the context of a pandemic was the focus of this review, and grey literature may not have addressed reported outcomes in this way.
11. CONCLUSION
Persons in care homes are at greater risk of infection during a pandemic and therefore warrant strict measures to protect their safety. Findings from this review highlight many effective strategies considered in preparation for pandemic, and it is likely that these were effective and valuable. However, the current pandemic has shown that over time, these protective measures may themselves have caused hardship. Older people in care homes already experience social isolation and so any measures involving restrictions to visiting and social interaction, particularly over the longer term, must be accompanied by strategies to mitigate potential loneliness and mental health sequelae arising from the long‐term pandemic restrictions.
Supporting information
Supplementary Material
APPENDIX 1. Quality appraisal
| Quantitative | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study | Clear research objectives | Data addressing research objectives | Participants’ representativeness | Measurement appropriateness | Complete outcome data | Confounders accounted in design and analysis | Participant exposed to pandemic | Total | Percentage (%) | Ratings (5–7 = high; 3–4 = medium; <3 = low) |
| Affifi et al. (2012) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | 100 | High |
| Eastwood et al. (2008) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | 100 | High |
| Mills et al. (2020) | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 6 | 86 | High |
| Siu et al. (2020) | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 6 | 86 | High |
| Qualitative | ||||||||||
| Study | Clear research objectives | Data addressing research objectives | Qualitative approach appropriate to answer the question | Methods of qualitative data collection adequate to address research question | Adequacy findings derived from the data | Interpretation of results | Coherency between qualitative data sources, collection, analysis and interpretation | Total | ||
| Fell (2008) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | 100 | High |
| Mimi et al. (2003) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | 100 | High |
DATA AVAILABILITY STATEMENT
The data that support this study are available from the corresponding author upon reasonable request.
REFERENCES
- Affifi, R. M. , Omar, S. R. , & El Raggal, A. A. (2012). A novel influenza A (H1N1) outbreak experience among residents of a long term‐care facility in Saudi Arabia during 2010 seasonal flu circulation. Infectious Disease Reports, 4(1), 23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Australian Government . (2020). Visitor restrictions for residential aged care services. Online: Australian Government Retrieved from https://www.agedcarequality.gov.au/providers/visitor‐restrictions‐residential‐aged‐care‐services [Google Scholar]
- Barnett, M. L. , & Grabowski, D. C. (2020). Nursing homes are ground zero for COVID‐19 pandemic. Paper presented at the JAMA Health Forum. [DOI] [PubMed] [Google Scholar]
- Braun, V. , & Clarke, V. (2013). Successful qualitative research: A practical guide for beginners. Sage. [Google Scholar]
- Cecco, L. (2020, 8 April 2020). Canada nursing home reels from death of almost half its residents. The Guardian p. 1. Retrieved from https://www.theguardian.com/world/2020/apr/08/canadian‐nursing‐home‐reels‐from‐death‐of‐half‐its‐residents‐bobcaygeon [Google Scholar]
- Centers for Disease Control and Prevention (2021). Global COVID‐19. Retrieved from https://www.cdc.gov/coronavirus/2019‐ncov/global‐covid‐19/index.html [Google Scholar]
- Chang, R. (2020). Govt To Send ‘Rapid Response Teams’ To COVID‐Hit Nursing Homes. TBSeFM News. Retrieved from http://tbs.seoul.kr/eFm/newsView.do?typ_800=P&idx_800=3417110&seq_800= [Google Scholar]
- Comas‐Herrera, A. , Zalakaín, J. , Litwin, C. , Hsu, A. T. , Lane, N. , & Fernández, J.‐L. (2020). Mortality associated with COVID‐19 outbreaks in care homes: early international evidence. Ltccovid. Org. International Long‐Term Care Policy Network, 1–6. https://ltccovid.org/wp‐content/uploads/2020/06/Mortality‐associated‐with‐COVID‐21‐May‐3.pdf [Google Scholar]
- Cornwall, P. (2020). ‘Rapid response teams’ being sent to short‐staffed nursing homes in Washington state as COVID‐19 surges again. Retrieved from https://www.seattletimes.com/seattle‐news/health/rapid‐response‐teams‐being‐sent‐to‐short‐staffed‐nursing‐homes‐in‐washington‐state‐as‐covid‐19‐surges‐again/ [Google Scholar]
- Cousins, S. (2020). Experts criticise Australia's aged care failings over COVID‐19. The Lancet, 396(10259), 1322–1323. 10.1016/S0140-6736(20)32206-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crotty, F. , Watson, R. , & Lim, W. K. (2020). Nursing homes: the titanic of cruise ships–will residential aged care facilities survive the COVID‐19 pandemic? Internal Medicine Journal, 50, 1033–1036. 10.1111/imj.14966 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davidson, P. M. , & Szanton, S. L. (2020). Nursing homes and COVID‐19: We can and should do better. Journal of Clinical Nursing, 29, 2758–2759. 10.1111/jocn.15297 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Domènech‐Abella, J. , Mundó, J. , Haro, J. M. , & Rubio‐Valera, M. (2019). Anxiety, depression, loneliness and social network in the elderly: Longitudinal associations from The Irish Longitudinal Study on Ageing (TILDA). Journal of Affective Disorders, 246, 82–88. 10.1016/j.jad.2018.12.043 [DOI] [PubMed] [Google Scholar]
- Dong, E. , Du, H. , & Gardner, L. (2020). An interactive web‐based dashboard to track COVID‐19 in real time. The Lancet Infectious Diseases, 20(5), 533–534. 10.1016/S1473-3099(20)30120-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eastwood, K. , Osbourn, M. , Francis, L. , Merritt, T. , Nicholas, C. , Cashman, P. , Durrheim, D. Wiggers, J. (2008). Improving communicable disease outbreak preparedness in residential aged care facilities using an interventional interview strategy. Australasian Journal on Ageing, 27(3), 143–149.Retrieved from https://onlinelibrary.wiley.com/doi/abs/ 10.1111/j.1741-6612.2008.00299.x [DOI] [PubMed] [Google Scholar]
- Fell, G. (2008). Preparedness of residential and nursing homes for pandemic flu. Journal of Public Health, 30(1), 99–102.Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7313825/pdf/fdm086.pdf [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mills, W. R. , Buccola, J. M. , Sender, S. , Lichtefeld, J. , Romano, N. , Reynolds, K. , Price, M. , Phipps, J. , & White, L. , & Howard, S. (2020). Home‐based primary care led‐outbreak mitigation in assisted living facilities in the first 100 days of coronavirus disease 2019. Journal of the American Medical Directors Association, 21(7), 951–953.Retrieved from https://www.jamda.com/article/S1525‐8610(20)30519‐3/pdf [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mimi, M. , Pun, S. P. , & Benzie, I. F. (2003). Experiencing SARS: perspectives of the elderly residents and health care professionals in a Hong Kong nursing home. Geriatric Nursing, 24(5), 266–269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moher, D. , Liberati, A. , Tetzlaff, J. , Altman, D. G. , & Group, P. (2009). Preferred reporting items for systematic reviews and meta‐analyses: the PRISMA statement. PLoS Med, 6(7), e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mustian, J. (2020, 2 May 2020). NY nursing home reports 98 deaths linked to coronavirus. ABC News. Retrieved from https://abcnews.go.com/US/wireStory/ny‐nursing‐home‐reports‐98‐deaths‐linked‐coronavirus‐70465506 [Google Scholar]
- Pollock, A. M. , Clements, L. , & Harding‐Edgar, L. (2020). Covid‐19: why we need a national health and social care service. British Medical Journal, 369, 1–2. 10.1136/bmj.m1465 [DOI] [PubMed] [Google Scholar]
- Rios, P. , Radhakrishnan, A. , Williams, C. , Ramkissoon, N. , Cormack, G. V. , Grossman, M. R. , Muller, M. P. , Straus, S. E. , & Tricco, A. C. (2020). Preventing the transmission of COVID‐19 and other coronaviruses in older adults aged 60 years and above living in long‐term care: a rapid review. Systematic Reviews, 9(1), 1–8. 10.1186/s13643-020-01486-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Siu, H.‐ Y.‐H. , Kristof, L. , Elston, D. , Hafid, A. , & Mather, F. (2020). A cross‐sectional survey assessing the preparedness of the long‐term care sector to respond to the COVID‐19 pandemic in Ontario, Canada. [DOI] [PMC free article] [PubMed] [Google Scholar]
- The Guardian (2020). Across the world, figures reveal horrific toll of care home deaths. The Guardian. Retrieved from. https://www.theguardian.com/world/2020/may/16/across‐the‐world‐figures‐reveal‐horrific‐covid‐19‐toll‐of‐care‐home‐deaths [Google Scholar]
- Thompson, D.‐C. , Barbu, M.‐G. , Beiu, C. , Popa, L. G. , Mihai, M. M. , Berteanu, M. , & Popescu, M. N. (2020). The impact of COVID‐19 pandemic on long‐term care facilities worldwide: An overview on international issues. BioMed Research International, 2020, 1–7. 10.1155/2020/8870249 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Usher, K. (2010). Are we ready? Preparing nurses to respond to disasters and emerging infectious diseases. Journal of Clinical Nursing, 19, 1483–1484. 10.1111/j.1365-2702.2009.02979.x [DOI] [PubMed] [Google Scholar]
- Washington State Department of Health and Social Services (2020). DSHS to provide Rapid Response Nursing Teams to long‐term care facilities heavily impacted by COVID‐19 [Press release]. Retrieved from https://www.dshs.wa.gov/os/office‐communications/media‐release/dshs‐provide‐rapid‐response‐nursing‐teams‐long‐term‐care‐facilities‐heavily‐impacted‐covid‐19 [Google Scholar]
- World Health Organization (2020). Guidance on COVID‐19 for the care of older people and people living in long‐term care facilities, other nonacute care facilities and home care. Retrieved from Online: https://apps.who.int/iris/handle/10665/331913 [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Material
Data Availability Statement
The data that support this study are available from the corresponding author upon reasonable request.