

Abstract
The coronavirus disease 2019 (COVID‐19) caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS‐CoV‐2) has led to an unprecedented international health crisis. COVID‐19 clinical presentations cover a wide range from asymptomatic to severe illness and death. Given the limited therapeutic resources and unexpected clinical features of the disease, readily accessible predictive biomarkers are urgently needed to improve patient care and management. We asked the degree to which anemia may influence the outcome of patients with COVID‐19. To this end, we identified 3777 patients who were positively diagnosed with COVID‐19 between March 1 and April 1 2020 in New York City. We evaluated 2,562 patients with available red blood cell, hemoglobin, and related laboratory values. Multivariable cox proportional hazards regression showed that anemia was a significant independent predictor of mortality (hazard ratio (HR): 1.26, 95% Confidence Interval [CI]: 1.06‐1.51), independent of age, sex, and comorbidities. There was a direct correlation between the degree of anemia and the risk of mortality when hemoglobin was treated as a continuous variable (HRadj 1.05; [CI]: 1.01‐1.09). The hemoglobin level that was maximally predictive of mortality, was 11.5 g/dL in males and 11.8 g/dL in females. These findings identify a routinely measured biomarker that is predictive of disease outcomes and will aid in refining clinical care algorithms and optimize resource allocation. Mechanisms of impacts of anemia on COVID‐19 outcome are likely to be multiple in nature and require further investigation.
Keywords: anemia, COVID‐19, haemoglobin, mortality, prognosis, RBC
1. INTRODUCTION
The global coronavirus disease 2019 (COVID‐19) is caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS‐CoV‐2) and was initially observed in late 2019 in Wuhan (Hubei Province), China and has led to an extraordinary global health crisis. Worldwide efforts have rapidly pinpointed biomarkers of disease severity and mortality that are currently guiding patient management [1, 2]. SARS‐CoV‐2 primarily employs angiotensin‐converting enzyme‐2 (ACE‐2) [3, 4] expressed on a variety of cell types [5], to alter cellular homeostasis [6]. However, not all cells involved in the pathogenesis of the disease are directly infected by the virus. For instance, despite the lack of viral invasion, monocytes and macrophages are critical in influencing COVID‐19 disease severity by regulating cytokine production and stimulating adaptive immune response. Although many blood biomarkers including lymphopenia, inflammatory indices such as high levels of circulating pro‐inflammatory cytokines specifically inerleukin‐6 (IL‐6) and TNF‐α, ferritin and coagulation factors have been reported to be associated with severe COVID‐19 [1], their predictive value for the disease course and severity is not yet fully established [7, 8].
While our understanding of the pathophysiology of the disease is rapidly evolving, additional indices that might identify patients who are most at risk of severe outcome in order to inform and improve the standard of care are urgently warranted. One of the debated features of COVID‐19 that puzzled clinicians [9, 10] was that acute respiratory syndrome seen in this disease may not be solely explained by lung alterations, raising the possibility that defective oxygen delivery/perfusion might also be implicated.
Anemia, or reduced blood capacity to carry oxygen, may be acute due to blood loss, or associated with a wide range of chronic conditions including inherited and acquired blood disorders, cancer, inflammation, chronic kidney disease, malnutrition, and aging [11, 12]. COVID‐19 severity was found by some [13] but not others [1, 14, 15] to be associated with anemia. Reports from Wuhan suggest a prevalence of anemia in COVID‐19 patients was 15–51% [16], but robust data on the impact of anemia on COVID‐19 disease progression and mortality remains unreported.
Emerging data raise the possibility that red blood cells (RBCs) might be also directly involved in the pathogenesis of the disease. An early report suggested that a protein expressed on RBCs (CD147 or Basigin) that serves as a receptor for plasmodium falciparum [17], might be an additional receptor for SARS‐CoV‐2 [18] [and reviewed in [19]]. These findings led some clinicians to ask whether anemia has an impact on COVID‐19 patient outcome [20, 21, 22, 23].
Here, we asked whether anemia influences COVID‐19 prognosis and patient outcome. The hypothesis tested is that COVID‐19 patients with anemia experience worse clinical course and higher mortality in comparison to COVID‐19 patients with normal RBC parameters.
2. METHODS
2.1. Patients and outcomes
All patients ≥18 years with an encounter at the Mount Sinai Health System between March 1 and April 1, 2020 who had a COVID‐19 diagnosis that was confirmed by a positive result on a reverse‐transcriptase–polymerase‐chain‐reaction (RT‐PCR) SARS‐CoV‐2 assay of a nasopharyngeal swab specimen were selected (n = 3777) for analysis of patient demographics and comorbidities. Patients from any care setting (ambulatory, emergency department, or hospitalized) were included. Patients who had a complete blood count (CBC, at presentation, n = 2562) were further examined to assess the associations between the primary predictors of interest, (hemoglobin, mean corpuscular volume (MCV), and hematocrit (HCT)) with primary and secondary outcomes (all‐cause mortality and mechanical ventilation). Patient demographics, comorbidity information, laboratory values, mechanical ventilation, and mortality were extracted by physician review of the electronic medical record. Comorbidities were assessed individually, and using the Charlson Comorbidity Index [24, 25], which provides a weighted score of comorbidities, based on the associated increased risk of mortality for each condition. This study was approved by the Program for Protection of Human Subjects (PPHS) of the Icahn School of Medicine at Mount Sinai (IRB # 20–03409).
2.2. Classification of laboratory values
Anemia was defined by WHO criteria (hemoglobin levels < 13 g/dL for males and < 12 g/dL for females) [26]. A secondary analysis classified severe, moderate, and mild anemia as hemoglobin < 7 g/dL, 7–9.9 g/dL, and 10–11.9 g/dL (females) or 10–12.9 g/dL (males), respectively. An additional secondary analysis evaluated hemoglobin as a continuous predictor. The normal range for MCV was defined as 80–100 fL.
2.3. Statistical analysis
Chi‐squared tests and Wilcoxon rank sum were performed to assess differences in anemia, demographics, and other laboratory values according to mortality. As uniform follow‐up time was not available for each patient, outcomes were modeled using time‐to‐event analysis. A multivariable Cox proportional hazards regression model was performed to assess the independent predictors of mortality utilizing a stepwise selection of patient (age, sex, race, Charlson Comorbidity Index) and clinical (anemia, lymphocyte count, and platelet count) characteristics. An additional stepwise multivariable Cox proportional hazards model was performed to assess the independent predictors of mechanical ventilation status utilizing the same predictors. D‐dimer was intentionally omitted from the regression model given the lack of biologic rationale for inclusion (thereby making confounding unlikely) and to avoid over‐fitting.
A secondary analysis was conducted to explore the sex‐specific optimal hemoglobin levels that best predict mortality. These hemoglobin cut points may help inform the point at which lower hemoglobin levels are of clinical concern. Optimal cutpoints were calculated using the X‐Tile software [27], separately for males and females. The X‐tile software tests each level of hemoglobin as the predictor in a Cox‐proportional hazards model, and calculates the associated log‐rank statistics. The optimal cut‐point is defined at the point with the maximum χ2 value, which indicates the greatest difference between the survival distributions of those with and without low hemoglobin levels. The significance of this split was assessed by applying the Miller‐Siegmund P‐value correction. A multivariable analysis was rerun with anemia defined according to the optimal cutpoints.
3. RESULTS
3.1. Patients characteristics
There were 3777 adult patients with an RT‐PCR confirmed diagnosis of COVID‐19 who presented between March 1 and April 1, 2020 at hospitals within the Mount Sinai Health System in New York City, which was the epicenter of the pandemic at the time; 2562 of whom had laboratory data available with a median follow up of 21 (interquartile range [IQR] 11–37) days, censoring patients at time of death. Of patients with laboratory data available, 1,973 (77.0%) were hospitalized. The median age of patients was 59 (IQR 42–71) years and the sample was mostly non‐white or Hispanic (72.6%) (Table 1). Forty‐five percent were female. Fifty‐four percent of patients had no reported comorbidities. Mechanical ventilation was required for 14.1% (n = 531) of the patients and 16.7% (n = 629) of the patients died at time of last follow up (Table 1).
TABLE 1.
Description of the study sample by availability of laboratory data (n = 3777)
| Variable | Labs (n = 2563, 67.9%) N (%) | No Labs (n = 1214, 32.1%) N (%) | P‐value |
|---|---|---|---|
| Sex | |||
| Male | 1459 (56.9) | 610 (50.3) | .0001 |
| Female | 1104 (43.1) | 604 (49.8) | |
| Race ‡ | |||
| Non‐Hispanic white | 632 (24.7) | 381 (33.4) | <.0001 |
| Non‐white, Hispanic | 1931 (75.3) | 760 (66.6) | |
| Age (years) ‡ | |||
| < 52 | 628 (24.5) | 735 (64.4) | <.0001 |
| 52 ‐ 64 | 605 (23.6) | 253 (22.2) | |
| 64 ‐ 75 | 707 (27.6) | 124 (10.9) | |
| > 75 | 622 (24.3) | 29 (2.5) | |
| Comorbidities | |||
| Myocardial Infarction | 134 (5.2) | 17 (1.4) | <.0001 |
| Congestive Heart Failure | 275 (10.7) | 21 (1.7) | <.0001 |
| Peripheral Vascular Disease | 135 (5.3) | 5 (0.4) | <.0001 |
| Stroke or TIA* | 205 (8.0) | 8 (0.7) | <.0001 |
| Dementia | 196 (7.7) | 7 (0.6) | <.0001 |
| COPD † | 160 (6.2) | 8 (0.7) | <.0001 |
| Connective Tissue Disease | 59 (2.3) | 13 (1.1) | .0098 |
| Peptic Ulcer Disease | 23 (0.9) | 9 (0.7) | .6251 |
| Liver Disease | 57 (2.2) | 5 (0.4) | <.0001 |
| Diabetes | 516 (20.1) | 103 (8.5) | <.0001 |
| Diabetes with end organ damage | 417 (16.3) | 22 (1.8) | <.0001 |
| Chronic Kidney Disease Stage III | 331 (12.9) | 22 (1.8) | <.0001 |
| Solid Cancers | 216 (8.4) | 23 (2.7) | <.0001 |
| Leukemia/Lymphoma | 66 (2.6) | 9 (0.7) | .0002 |
| AIDS | 11 (0.4) | 4 (0.3) | .6491 |
| Hemiplagia | 24 (0.9) | 2 (0.2) | .0074 |
| Charlson Comorbidity Score | |||
| Mean (SD) | 1.7 (2.1) | 0.4 (1.0) | <.0001 |
| BMI (kg/m2) # | |||
| ≤ 30 | 1523 (59.4) | 665 (54.8) | <.0001 |
| > 30 | 879 (34.3) | 221 (18.2) | |
| Mechanical Ventilation | |||
| No | 2045 (80.0) | 1201 (98.9) | <.0001 |
| Yes | 518 (20.2) | 13 (1.1) | |
| Anemia § (< 12 g/dL Hemoglobin, females; < 13 g/dL, males) | |||
| Yes | 793 (30.9) | ||
| No | 1770 (69.1) | ||
| Absolute Lymphocyte Count$ (# x 109 / L) | |||
| < 1 | 848 (44.4) | ||
| ≥1 | 1066 (55.7) | ||
| Platelet count ¶ (# x 109 / L) | |||
| < 150 | 438 (22.5) | ||
| ≥150 | 1510 (77.5) | ||
Transient Ischemic Attack.
Chronic Obstructive Pulmonary Disease.
Race was missing for 73 patients and age was missing for 74 patients.
$ BMI information missing for 489 patients.
Laboratory measurements reported on 2,563 patients, 1 patient dropped in subsequent analyses due to missing age.
2,558 patients with valid platelet measures.
2,507 patients with valid lymphocyte measures.
Mortality was significantly associated with increasing age (P < .0001), male sex (P < .0001), a higher Charlson comorbidity score (P < .0001), and mechanical ventilation (P < .0001) (Table 2). In this cohort, there was no statistically significant difference in mortality by race (Table 2, P = .45).
TABLE 2.
Description of study sample according to mortality status (n = 3777)
| Variable | Alive (n = 3148, 83.3%) N (%) | Deceased (n = 629, 16.7%) N (%) | P‐value |
|---|---|---|---|
| Sex | |||
| Male | 1680 (53.4) | 389 (61.8) | <.0001 |
| Female | 1468 (46.6) | 240 (38.2) | |
| Race ‡ | |||
| Non‐Hispanic white | 835 (27.1) | 178 (28.6) | .4529 |
| Non‐white, Hispanic | 2246 (72.9) | 445 (71.4) | |
| Age (years) ‡ | |||
| < 52 | 1325 (43.0) | 38 (6.1) | <.0001 |
| 52 ‐ 64 | 751 (24.4) | 107 (17.2) | |
| 64 ‐ 75 | 628 (20.4) | 203 (32.6) | |
| > 75 | 377 (12.2) | 274 (44.1) | |
| Comorbidities | |||
| Myocardial Infarction | 99 (3.1) | 52 (8.3) | <.0001 |
| Congestive Heart Failure | 178 (5.7) | 118 (18.8) | <.0001 |
| Peripheral Vascular Disease | 92 (2.9) | 48 (7.6) | <.0001 |
| Stroke or TIA* | 135 (4.3) | 78 (12.4) | <.0001 |
| Dementia | 102 (3.2) | 101 (16.1) | <.0001 |
| COPD † | 108 (3.4) | 60 (9.5) | <.0001 |
| Connective Tissue Disease | 61 (1.9) | 11 (1.8) | .7517 |
| Diabetes | 492 (15.6) | 127 (20.2) | .0048 |
| Diabetes with end organ damage | 264 (8.4) | 175 (27.8) | <.0001 |
| Chronic Kidney Disease Stage III | 232 (7.4) | 121 (19.2) | <.0001 |
| Localized Solid Tumor | 151 (4.8) | 46 (7.3) | .0096 |
| BMI (kg/m2) # | |||
| BMI ≤ 30 | 1795 (63.0) | 393 (64.6) | .4796 |
| BMI > 30 | 888 (37.0) | 212 (35.4) | |
| Charlson Comorbidity Score | |||
| Mean (SD) | 1.01 (1.7) | 2.58 (2.3) | <.0001 |
| Anemia § (< 12 g/dL Hemoglobin, females; < 13 g/dL, males) | |||
| Yes | 534 (27.4) | 258 (42.4) | <.0001 |
| No | 1418 (72.6) | 352 (57.6) | |
| Absolute Lymphocyte Count # (# x 109 / L) | |||
| < 1 | 848 (44.4) | 312 (52.6) | .0004 |
| ≥1 | 1066 (55.7) | 281 (47.4) | |
| Platelet count ¶ (# x 109 / L) | |||
| < 150 | 438 (22.5) | 167 (27.4) | .01 |
| ≥150 | 1510 (77.5) | 443 (72.6) | |
| Mechanical Ventilation | |||
| No | 2999 (95.3) | 247 (39.3) | <.0001 |
| Yes | 149 (4.7) | 382 (30.7) | |
Transient Ischemic Attack.
Chronic Obstructive Pulmonary Disease.
Race and age was missing for 73 patients and age was missing for 74 patients.
Laboratory measurements reported on 2,562 patients.
2,558 patients with valid platelet measures.
2,507 patients with valid lymphocyte measures. .
3.2. Anemia in patients with COVID‐19
Further analyses were performed on 2562 (67.9%) of the patients with laboratory measurements of hemoglobin, RDW, and MCV. The median time from COVID‐19 diagnosis to the collection of laboratory parameters was 0 (IQR 0–1) days. Seven hundred ninety‐two (30.9%) patients met the clinical criteria for anemia; 311 (12.1%) patients had MCV values outside a normal range, while 502 (19.6%) patients had RDW values above normal (Table 3). In addition, 605 (23.6%) patients had thrombocytopenia and 1,159 (46.3%) had lymphopenia.
TABLE 3.
Description of patients according to hemoglobin levels (n = 2562)
| Anemia | P‐value | ||
|---|---|---|---|
| No (n = 1770, 69.3%) N(%) | Yes (n = 792, 30.9%) N(%) | ||
| Sex | |||
| Male | 1007 (56.9) | 451 (57.0) | .9600 |
| Female | 763 (43.1) | 341 (43.0) | |
| Race | |||
| Non‐Hispanic white | 443 (25.0) | 189 (23.9) | .5166 |
| Non‐white, Hispanic | 1327 (75.0) | 603 (76.1) | |
| Age (years)⋀ | |||
| < 52 | 482 (27.3) | 146 (1845) | <.0001 |
| 52 ‐64 | 449 (25.4) | 156 (19.7) | |
| 64 – 75 | 483 (27.3) | 224 (28.3) | |
| > 75 | 356 (20.1) | 266 (33.6) | |
| Charlson Comorbidity Score | |||
| Mean (SD) | 1.17 (1.7) | 2.92 (2.4) | <.0001 |
| Hematocrit (%) mean (SD) | |||
| Males | 44.4 (3.6) | 33.8 (4.9) | <.0001 |
| Females | 41.0 (3.4) | 32.2 (4.2) | <.0001 |
| Red blood cell distribution width (%) | |||
| > 15 | 151 (8.5) | 350 (44.3) | <.0001 |
| ≤ 15 | 1619 (91.5) | 442 (55.7) | |
| Mean corpuscular volume (fL) | |||
| < 80 | 74 (4.2) | 114 (14.4) | <.0001 |
| 80–100 | 1640 (92.7) | 611 (77.2) | |
| > 100 | 56 (3.2) | 67 (8.5) | |
| Absolute Lymphocyte Count"/> (# x 109 / L) | |||
| < 1 | 778 (44.5) | 381 (50.4) | .007 |
| ≥1 | 970 (55.5) | 375 (49.6) | |
| Platelet count*(# x 109 / L) | |||
| < 150 | 394 (22.3) | 211 (26.7) | .01 |
| ≥150 | 1374 (77.7) | 578 (73.3) | |
| Mechanical Ventilation | |||
| No | 1430 (80.8) | 615 (77.6) | .067 |
| Yes | 340 (19.2) | 177 (22.4) | |
2557 patients with valid platelet and hemoglobin measures.
2504 patients with valid lymphocyte and hemoglobin measures. .
As anticipated, anemia was statistically significantly associated with increasing age (P < .0001), and higher Charlson comorbid index scores (P < .0001). Also as expected, patients with anemia were more likely to have a lower HCT in both males and females (P < .0001), RDW > 15% (P < .0001), and MCV outside the range of 80–100 fL (P < .0001; Table 3). As expected, anemia was also significantly associated with thrombocytopenia (P = .01) and lymphopenia (P = .007)
The relationship between anemia and outcomes was further evaluated by applying a multivariable model. After stepwise selection, the model for mortality included age, sex, and Charlson comorbidity index. We found anemia to be independently significantly associated with a higher risk of mortality (HRadj: 1.26, 95% Confidence Interval [CI]: 1.06–1.51; Table 4). However, anemia was not significantly independently associated with mechanical ventilation after adjustment for age, sex, race, and lymphocyte count (HRadj: 1.11, 95% CI: 0.92‐1.34; Table 5).
TABLE 4.
Independent predictors of mortality among COVID‐19 positive patients
| n = 2497"/> | |
|---|---|
| HR ‡ adj (95% CI) | |
| Anemia Yes vs No* | 1.26 (1.06 ‐ 1.51) |
| Female vs Male | 0.67 (0.60 ‐ 0.84) |
| Age (years) < 52 | 1.0 (ref) |
| 52 ‐ 63 | 2.39 (1.65 – 3.48) |
| 64–75 | 3.85 (2.71 – 5.47) |
| > 75 | 6.66 (4.70 – 9.44) |
| Charlson Comorbidity Index (continuous) | 1.06 (1.02 ‐ 1.10) |
(< 12 g/dL Hemoglobin, females; < 13 g/dL, males).
65 patients excluded from analysis for missing data.
Adjusted for all variables listed.
TABLE 5.
Predictors of mechanical ventilation among COVID‐19 positive patients
| n = 2,485"/> | |
|---|---|
| HR ‡ adj (95% CI) | |
| Anemia: Yes vs No* | 1.11 (0.92‐1.34) |
| Female vs Male | 0.79 (0.65 ‐ 0.94) |
| Non‐Hispanic white vs Non‐white, Hispanic | 0.81 (0.65 – 1.00) |
| Age (years) < 52 | |
| 52 ‐63 | 1.69 (1.27 – 2.62) |
| 64–75 | 2.28 (1.74 – 2.99) |
| > 75 | 1.59 (1.18 ‐ 2.15) |
| Absolute Lymphocyte Count (# x 109 / L) | |
| ≥1 | 1.0 (ref) |
| < 1 | 1.24 (1.03‐1.48) |
(< 12 g/dL Hemoglobin, females; < 13 g/dL, males).
77 patients excluded from analysis for missing data.
Adjusted for all variables listed.
Secondary analyses of hemoglobin as a continuous variable, or categorized according to severity showed similar results. In a multivariable model adjusted for age, sex, race, and Charlson comorbidity index, there was a statistically significant increase in mortality (HRadj 1.05; [CI]: 1.01‐1.09) with decreasing hemoglobin levels. However, decreasing hemoglobin levels were not significantly independently associated with mechanical ventilation (HRadj 1.02; [CI]: 0.98–1.07). Similar results were obtained across severity categories of anemia, although the highest category contained very few cases.
3.3. Optimal hemoglobin cutpoints to predict outcomes
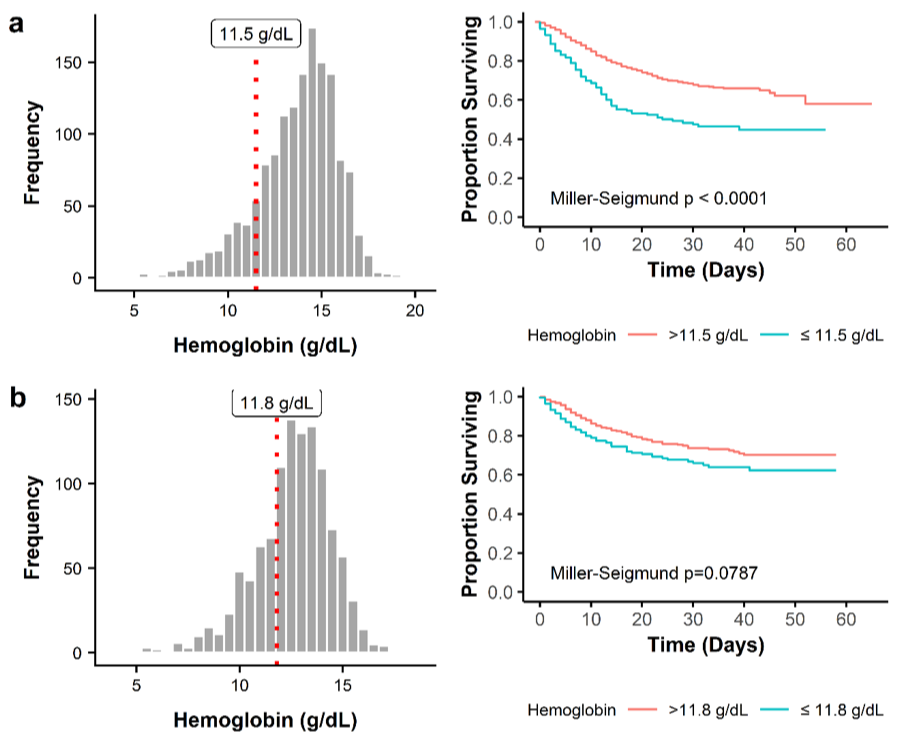
Next, we aimed to determine the hemoglobin level that is maximally predictive of mortality, using the X‐Tile software. For males, the optimal hemoglobin cutpoint was defined at 11.5 g/dL (Miller‐Seigmund P < .0001) (Figure S1a). In females, the optimal cutpoint was defined at 11.8 g/dL (Miller‐Seigmund P = .0787) (Figure S1b). When the optimal hemoglobin cut points were applied to the model instead of the WHO definition of anemia, a stronger association (HRadj 1.40, 95% CI: 1.17‐1.69), was observed between hemoglobin and mortality after adjustment for confounders.
4. DISCUSSION
The results of this study indicate previously unrecognized association between decreasing hemoglobin levels and increased risk of mortality in COVID‐19 patients, independent of age, sex, comorbidities, and other hematologic parameters including lymphocyte and platelet count. While considered among other known risk factors, anemia may serve as an early indicator of poor outcomes in patients with COVID‐19. These results may provide a rationale for including anemia in algorithms assessing risk prediction in COVID‐19 mortality and severity.
Although modulations of red cell distribution width (RDW) are thought to predict disease severity and worse outcomes [28], RBC indices are often underappreciated especially in patients with only mild anemia. We originally hypothesized that severe anemia would be predictive of COVID‐19 severity and mortality. Surprisingly, our analysis found that the ideal hemoglobin cutoffs for considering anemia as a significant contributor to mortality was 11.5 g/dL in males and 11.8 g/dL in females. The maximally predictive hemoglobin for mortality in male patients was only just below the WHO criteria for anemia, interestingly, suggesting that even mild compromises in hemoglobin reserve can be prognostically detrimental in COVID‐19. Recently published evidence has also suggested than an elevation in RDW may be prognostic in hospitalized COVID‐19 patients [29]. Interestingly, in our cohort we observed an association between RDW and mortality only in non‐anemic patients (manuscript under review).
The impact of anemia observed in COVID‐19 in this study has precedent. Anemia is known to be a poor prognostic marker in several other respiratory diseases. In chronic obstructive pulmonary disease (COPD), anemia is a well validated independent predictor of mortality [30, 31]. Similarly, in congestive heart failure, a hemoglobin < 13 g/dL is independently associated with an increased risk of hospitalization and death [32]. In intubated patients in the intensive care unit, hemoglobin < 10 g/dL is associated with a five‐fold increase in the risk of unsuccessful extubation [33]. The impact of anemia on COVID‐19 outcomes may in part be a consequence of the highly inflammatory state associated with COVID‐19. Anemia may be an independent risk factor for poor outcome for reasons that are not yet evident and require further investigations. In this context, the relationship between erythroid cell production, iron metabolism, and inflammatory signaling may be relevant [34, 35, 36, 37, 38, 39]. However, it is important to note that acute anemia in the critically ill is almost always caused by acute bleeding and hemolysis [40]. However, elevation of circulating IL‐6 levels on hepcidin and its modulation of iron availability and red blood cell production may limit the compensatory erythropoietic response in COVID‐19 patients [41, 42, 43, 44].
Interestingly, the association between anemia and mechanical ventilation on multivariable analysis was not significant. The decision to intubate is clinically made, with variation in practice among clinicians. Therefore, mechanical ventilation is subject to a degree of bias. As an example, patients who are greater than 75 had a lower OR of intubation as compared with patients 64–75 (Table 5).
The current study has limitations that are important to recognize. This study was unable to robustly explore prior history of anemia in our patient cohort, nor was it able to investigate baseline hematological indices in the patient population specifically in patients with hemoglobinopathies. Our study also lacked information about symptom onset timing, therefore we were unable to determine whether a patient's anemia was pre‐existing or a result of a worsening COVID‐19 infection. Our study was also limited by inability to assess the degree to which hemolysis may be contributing to baseline anemia. LDH was universally elevated in our patient cohort and haptoglobin levels were rarely obtained in this retrospective dataset. Patients with available lab data represent those with a higher risk burden, and likely a more serious infection in need of clinical care and intervention, while those without lab data may have been tested in outpatient environments, including rapid testing centers, or may not have reported clinical manifestation of symptoms for COVID‐19. In addition, patients presenting to care had variable severity of acute disease and inflammation, which we were unable to evaluate and might be an important confounder as the impact of acute inflammation on anemia remains unclear. We were also unable to assess a broad set of socio‐economic predictors of disease outcomes such as patient income or living conditions, which have been increasingly underlined as highly important in determining outcomes in the New York City outbreak.
Strengths of our study include a large population of COVID‐19 patients with common hematological parameters collected at multiple sites in New York City. Our study was also able to measure a complete Charlson comorbidity index, which is a powerful and well‐validated measure of overall mortality outcomes in the general population [24, 25].
These results have potential clinical implications in terms of risk stratification and early implementation of treatment strategies. These may include reducing the inflammatory consequences of COVID‐19 respiratory borne viral infection. The heightened inflammatory state drives pulmonary compromise and multi‐organ failure and likely intersects with the clotting cascade [45, 46]. Agents that are currently in clinical evaluation in targeting the pathological inflammatory cytokine production include inhibitors of Janus kinase (JAK) 2 and Bruton tyrosine kinase (BTK) as well as selective cytokine antagonists [47, 48]. In addition, dexamethasone, a potent anti‐inflammatory, has been shown to decrease mortality in COVID‐19 patients who are hospitalized and requiring respiratory support [49].
Identification of a patient at higher risk for complications of COVID‐19 would allow for a risk‐adapted approach with early intervention employing such therapeutics that may mitigate the inflammation‐mediated organ damage and thrombo‐inflammation and coagulopathy that significantly contributes to mortality. As prospective studies evaluate various rational therapies for COVID‐19 often re‐purposed from other approved indications, it will be important to stratify for baseline clinical variables such as anemia, as shown in this study, in order to determine whether the intervention has specific benefit in high‐risk subsets. Steroids have been shown to have a positive effect on COVID‐19 outcome and are now increasingly incorporated into institutional treatment guidelines [49].
In summary, anemia is a critical previously unrecognized independent predictor of poor outcomes in patients with COVID‐19. These readily available biomarkers should be considered by clinicians when risk‐stratifying a patient with COVID‐19 and may eventually identify a subset of patients that require early specific therapeutic intervention. The underlying pathological relationship of mild anemia with poor outcomes may at least in a subset of patients be linked to inflammation, thereby, informing a targeted treatment approach, however, further investigation is required.
AUTHOR CONTRIBUTIONS
DT, JR, JM, ET, and SG conceived and designed the study. JR, NA, and WLC performed the statistical analyses, DT, JR, NA, and ET analyzed the data. All authors participated in writing and editing the manuscript.
CONFLICT OF INTEREST
The authors declare no relevant conflict of interest
Supporting information
Supplementary Figure 1‐ Distribution of haemoglobin levels and Kaplan‐Meier survival estimates of mortality for those with and without low haemoglobin for (a) males and (b) females. For males, the optimal cutpoint was 11.5 g/dL; for females the optimal cutpoint was 11.8 g/dL.
{kind=link}
ACKNOWLEDGMENTS
The authors thank Members of the Hematology and Medical Oncology Fellowship and Institute for Translational Epidemiology at Mount Sinai Health System especially Drs. Leonard Naymagon, Maaike van Gerwen, Mathilda Alsen, Santiago Thibaud, Alaina Kessler, Sangeetha Venugopal, Iman Makki, Qian Qin, Sirish Dharmapuri, Tomi Jun, Sheena Bhalla, Shana Berwick, and Jonathan Feld for their work and assistance in creating the clinical database; the authors also thank Drs Jane Little (University of North Carolina) and Miguel Abboud (American University of Beirut Medical Center) for critically reviewing the manuscript. This work was in part supported by 5P30CA196521‐05 to EM and funds from R01HL136255 and NYSTEM IIRP C32602GG to SG.
Tremblay D, Rapp JL, Alpert N, et al. Mild anemia as a single independent predictor of mortality in patients with COVID‐19. eJHaem. 2021;2:319–326. 10.1002/jha2.167
Douglas Tremblay and Joseph L. Rapp contributed equally
Contributor Information
John Mascarenhas, Email: john.mascarenhas@mssm.edu.
Emanuela Taioli, Email: emanuela.taioli@mountsinai.org.
Saghi Ghaffari, Email: Saghi.Ghaffari@mssm.edu.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- 1. Henry BM, de Oliveira MHS, Benoit S, Plebani M, Lippi G. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID‐19): a meta‐analysis. Clin Chem Lab Med, 2020;58:1021–28. [DOI] [PubMed] [Google Scholar]
- 2. Vabret N, Samstein R, Fernandez N, Merad M, Sinai Immunology Review P, et al. Advancing scientific knowledge in times of pandemics. Nat Rev Immunol. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Lu R, Zhao X, Li J, Niu P, Yang B, Wu H, et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet, 2020;395:565–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Wan Y, Shang J, Graham R, Baric RS, Li F. Receptor Recognition by the Novel Coronavirus from Wuhan: an Analysis Based on Decade‐Long Structural Studies of SARS Coronavirus. J Virol, 2020;94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Hamming I, Timens W, Bulthuis ML, Lely AT, Navis G, van Goor H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J Pathol, 2004;203:631–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Bojkova D, Klann K, Koch B, Widera M, Krause D, Ciesek S, et al. Proteomics of SARS‐CoV‐2‐infected host cells reveals therapy targets. Nature, 2020;583:469–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Liao D, Zhou F, Luo L, Xu M, Wang H, Xia J, et al. Haematological characteristics and risk factors in the classification and prognosis evaluation of COVID‐19: a retrospective cohort study. Lancet Haematol. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Wu C, Chen X, Cai Y, Xia J, Zhou X, Xu S, et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern Med. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Couzin‐Frankel J. The mystery of the pandemic's 'happy hypoxia'. Science, 2020;368:455–6. [DOI] [PubMed] [Google Scholar]
- 10. Gattinoni L, Coppola S, Cressoni M, Busana M, Rossi S, Chiumello D. COVID‐19 Does Not Lead to a "Typical" Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med, 2020;201:1299–300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Chaparro CM, Suchdev PS. Anemia epidemiology, pathophysiology, and etiology in low‐ and middle‐income countries. Ann N Y Acad Sci, 2019;1450:15–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Sankaran VG, Weiss MJ. Anemia: progress in molecular mechanisms and therapies. Nat Med, 2015;21:221–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Zhao J, Gao HY, Feng ZY, Wu QJ. A Retrospective Analysis of the Clinical and Epidemiological Characteristics of COVID‐19 Patients in Henan Provincial People's Hospital, Zhengzhou, China. Front Med (Lausanne), 2020;7:286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Fan BE, Chong VCL, Chan SSW, Lim GH, Lim KGE, Tan GB, et al. Hematologic parameters in patients with COVID‐19 infection. Am J Hematol, 2020;95:E131‐4. [DOI] [PubMed] [Google Scholar]
- 15. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet, 2020;395:497–506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Pourbagheri‐Sigaroodi A, Bashash D, Fateh F, Abolghasemi H. Laboratory findings in COVID‐19 diagnosis and prognosis. Clin Chim Acta, 2020;510:475–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Crosnier C, Bustamante LY, Bartholdson SJ, Bei AK, Theron M, Uchikawa M, et al. Basigin is a receptor essential for erythrocyte invasion by Plasmodium falciparum. Nature, 2011;480:534–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Wang KEA. SARS‐CoV‐2 invades host cells via a novel route: CD147‐spike protein. . Preprint at bioRxiv10.1101/2020.03.14.988345 (2020). 2020.
- 19. Merad M, Martin JC. Pathological inflammation in patients with COVID‐19: a key role for monocytes and macrophages. Nat Rev Immunol, 2020;20:355–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Beerkens F, John M, Puliafito B, Corbett V, Edwards C, Tremblay D, et al. COVID‐19 pneumonia as a cause of acute chest syndrome in an adult sickle cell patient. Am J Hematol, 2020;95:E154‐6. [DOI] [PubMed] [Google Scholar]
- 21. Das A, Das M, Ghosh S, et al. Impact of nutritional status and anemia on COVID‐19: Is it a public health concern? Evidence from National Family Health Survey‐4 (2015‐2016), India. Public Health, 2020;185:93–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Roy NBA, Telfer P, Eleftheriou P, de la Fuente J, Drasar E, Shah F, et al. Protecting vulnerable patients with inherited anaemias from unnecessary death during the COVID‐19 pandemic. Br J Haematol, 2020;189:635–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Sahu KK, Siddiqui AD, Cerny J. Managing sickle cell patients with COVID‐19 infection: the need to pool our collective experience. Br J Haematol, 2020;190:e86‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis, 1987;40:373–83. [DOI] [PubMed] [Google Scholar]
- 25. Quan H, Li B, Couris CM, Fushimi K, Graham P, Hider P, et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol, 2011;173:676–82. [DOI] [PubMed] [Google Scholar]
- 26. Cappellini MD, Motta I. Anemia in Clinical Practice‐Definition and Classification: Does Hemoglobin Change With Aging? Semin Hematol, 2015;52:261–9. [DOI] [PubMed] [Google Scholar]
- 27. Camp RL, Dolled‐Filhart M, Rimm DL. X‐tile: a new bio‐informatics tool for biomarker assessment and outcome‐based cut‐point optimization. Clin Cancer Res, 2004;10:7252–9. [DOI] [PubMed] [Google Scholar]
- 28. Bazick HS, Chang D, Mahadevappa K, Gibbons FK, Christopher KB. Red cell distribution width and all‐cause mortality in critically ill patients. Crit Care Med, 2011;39:1913–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Foy BH, Carlson JCT, Reinertsen E, Padros IVR, Pallares Lopez R, Palanques‐Tost E, et al. Association of Red Blood Cell Distribution Width With Mortality Risk in Hospitalized Adults With SARS‐CoV‐2 Infection. JAMA Netw Open, 2020;3:e2022058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Chambellan A, Chailleux E, Similowski T, Group AO. Prognostic value of the hematocrit in patients with severe COPD receiving long‐term oxygen therapy. Chest, 2005;128:1201–8. [DOI] [PubMed] [Google Scholar]
- 31. Martinez FJ, Foster G, Curtis JL, Criner G, Weinmann G, Fishman A, et al. Predictors of mortality in patients with emphysema and severe airflow obstruction. Am J Respir Crit Care Med, 2006;173:1326–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Go AS, Yang J, Ackerson LM, Lepper K, Robbins S, Massie BM, et al. Hemoglobin level, chronic kidney disease, and the risks of death and hospitalization in adults with chronic heart failure: the Anemia in Chronic Heart Failure: Outcomes and Resource Utilization (ANCHOR) Study. Circulation, 2006;113:2713–23. [DOI] [PubMed] [Google Scholar]
- 33. Khamiees M, Raju P, DeGirolamo A, Amoateng‐Adjepong Y, Manthous CA. Predictors of extubation outcome in patients who have successfully completed a spontaneous breathing trial. Chest, 2001;120:1262–70. [DOI] [PubMed] [Google Scholar]
- 34. Greenfest‐Allen E, Malik J, Palis J, Stoeckert CJ Jr. Stat and interferon genes identified by network analysis differentially regulate primitive and definitive erythropoiesis. BMC Syst Biol, 2013;7:38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Khoramian Tusi B, Socolovsky M. High‐throughput single‐cell fate potential assay of murine hematopoietic progenitors in vitro. Exp Hematol, 2018;60:21–9 e23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Liang R, Camprecios G, Kou Y, McGrath K, Nowak R, Catherman S, et al. A Systems Approach Identifies Essential FOXO3 Functions at Key Steps of Terminal Erythropoiesis. PLoS Genet, 2015;11:e1005526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Morera D, Roher N, Ribas L, Balasch JC, Donate C, Callol A, et al. RNA‐Seq reveals an integrated immune response in nucleated erythrocytes. PLoS One, 2011;6:e26998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Muckenthaler MU, Rivella S, Hentze MW, Galy B. A Red Carpet for Iron Metabolism. Cell, 2017;168:344–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Pradhan P, Vijayan V, Gueler F, Immenschuh S. Interplay of Heme with Macrophages in Homeostasis and Inflammation. Int J Mol Sci, 2020;21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Ganz T. Anemia of Inflammation. N Engl J Med, 2019;381:1148–57. [DOI] [PubMed] [Google Scholar]
- 41. Fraenkel PG. Anemia of Inflammation: A Review. Med Clin North Am, 2017;101:285–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Ganz T, Nemeth E. Iron sequestration and anemia of inflammation. Semin Hematol, 2009;46:387–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Liang R, G S.. Advances in understanding the mechanisms of erythropoiesis in homeostasis and disease. British Journal of Hematology, In press, 2016;0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Nemeth E, Rivera S, Gabayan V, Keller C, Taudorf S, Pedersen BK, et al. IL‐6 mediates hypoferremia of inflammation by inducing the synthesis of the iron regulatory hormone hepcidin. J Clin Invest, 2004;113:1271–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Connors JM, Levy JH. Thromboinflammation and the hypercoagulability of COVID‐19. J Thromb Haemost, 2020;18:1559–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Engelmann B, Massberg S. Thrombosis as an intravascular effector of innate immunity. Nat Rev Immunol, 2013;13:34–45. [DOI] [PubMed] [Google Scholar]
- 47. Roschewski M, Lionakis MS, Sharman JP, Roswarski J, Goy A, Monticelli MA, Roshon M, Wrzesinski SH, Desai JV, Zarakas MA, Collen J, Rose K, Hamdy A, Izumi R, Wright GW, Chung KK, Baselga J, Staudt LM & Wilson WH Inhibition of Bruton tyrosine kinase in patients with severe COVID‐19. Sci Immunol, 2020;5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Zhang S, Li L, Shen A, Chen Y, Qi Z. Rational Use of Tocilizumab in the Treatment of Novel Coronavirus Pneumonia. Clin Drug Investig, 2020;40:511–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Group RC, Horby P, Lim WS, Emberson JR, Mafham M, Bell JL, et al. Dexamethasone in Hospitalized Patients with Covid‐19 ‐ Preliminary Report. N Engl J Med. 2020.. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Figure 1‐ Distribution of haemoglobin levels and Kaplan‐Meier survival estimates of mortality for those with and without low haemoglobin for (a) males and (b) females. For males, the optimal cutpoint was 11.5 g/dL; for females the optimal cutpoint was 11.8 g/dL.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.