

Abstract
Many healthcare organizations are now routinely screening patients for social needs such as food and housing. It is largely unknown whether the needs they identify would have been expressed by the patient in the absence of screening. To better understand expressed and unexpressed social needs, we administered a social needs screener to 1,397 low-income adults who called a 2-1-1 helpline in Missouri seeking assistance with social needs between June 2017 and October 2019. Merging data from the screener and 2-1-1, we found that the screener identified all of the social needs expressed to 2-1-1 for about half the participants, and on average identified at least one social need not expressed to 2-1-1 (i.e., unexpressed needs). Certain social needs (utility payment assistance, housing) were much more likely to be expressed than unexpressed, while others (childcare, employment, personal safety) were almost universally unexpressed. In regression analyses, having certain expressed needs significantly increased the odds of having certain unexpressed needs. For example, those seeking transportation assistance from 2-1-1 had greater odds of unexpressed needs for food (OR=3.19; 95% CI = 1.45-7.02) and healthcare (OR=2.18; 95% CI = 1.06-4.48) than those not expressing transportation needs. Those seeking employment assistance from 2-1-1 had greater odds of unexpressed needs for personal safety (OR=3.04; 95% CI = 1.20-7.68) and healthcare (OR=2.58; 95% CI = 1.15-5.77) than those not expressing employment needs. Implications for healthcare (screening detects expressed and unexpressed needs) and social service organizations (certain requests may be markers for other needs) are discussed.
Keywords: Social determinants, social needs, basic needs, low-income populations, healthcare, social services
Introduction
The healthcare sector’s increasing investment in addressing social needs such as food insecurity and housing instability (Horwitz et al., 2020) requires quality data on individual and community social needs (Thomas-Henkel & Schulman, 2017). At the individual level, many low-income patients are now routinely screened for social needs (Andermann, 2018; Artiga and Hinton, 2018). At the community level, social service agencies are increasingly adept at tracking requests for assistance with social needs and service utilization (Artiga & Hinton, 2018; Kreuter, Garg, Thompson, et al., 2020). Both types of data provide a valuable, although incomplete, profile of social needs. This first-of-its-kind study combines the two approaches to estimate the total social needs experienced in a low-income population, and quantifies the size and nature of the gap between them.
In Bradshaw’s classic taxonomy of social needs, expressed needs are those that are sufficiently important to an individual that the person will act upon them by seeking assistance or services (Bradshaw & Jonathan, 1972). Unexpressed needs are those that a person feels but does not articulate (Shoham & Strauss, 2008). A need may be unexpressed because the person views it as sensitive in nature and doesn’t want to talk about it with others (Billings & Cowley, 1995), lacks the time or resources to address multiple and equally important needs simultaneously (Alio, 2017), believes the need cannot be addressed and accepts it as unchangeable (Heinemann et al., 2002), or perceives the need to be less urgent or a lower priority than other needs that are expressed (Heflin & Scott, 2011; Polit et al., 2000; Tach & Greene, 2014).
Many expressed social needs are likely to be captured by social service agency records and at least some unexpressed social needs will be identified by proactive screening such as that now being conducted in many healthcare settings. Combining the two sources of information will provide a fuller accounting of the social needs burden affecting low-income Americans, help identify which types of social needs tend to be expressed vs. unexpressed, and determine whether certain expressed social needs might be useful markers for other, unexpressed social needs. Better understanding of the relationships between expressed and unexpressed social needs will inform cross-sector collaboration between social services and healthcare organizations and enhance the social needs screening and intervention efforts of both.
Methods
Study context
This study analyzed data from an ongoing randomized intervention trial testing two interventions to help low-income smokers quit (McQueen et al., 2019). Participants were recruited after calling the 2-1-1 telephone helpline in Missouri. 2-1-1 is a federally-designated 3-digit information and referral number that receives 12-13 million requests per year across the U.S., (211.Org, n.d.) mostly from low-income Americans seeking help with social needs such as food, rent, and utility payments (Thompson et al., 2015). Live operators answer each call, document callers’ requests (up to three per call) using an extensive taxonomy of needs (described below), and provide referrals to local agencies that can help address each of the caller’s needs.
Before ending each call, 2-1-1 operators offered a random sample of callers a chance to participate in the study. Consented study participants then completed a baseline telephone survey administered by the research team soon after they had called 2-1-1. Those enrolled between June 2017 and October 2019 (n=1,397) were included in analyses. Research procedures and materials for the study were approved by Human Research Protection Office at Washington University in St. Louis and are reported elsewhere (McQueen et al., 2019).
Participants
All participants were adult daily smokers living in Missouri. They had to be comfortable speaking English and could not be pregnant. Operators at 2-1-1 delivered standard service, then screened callers for smoking status and interest in participation. Callers in crisis or calling 2-1-1 on behalf of another person were ineligible. Detailed eligibility and enrollment procedures for the trial are reported elsewhere (McQueen et al., 2019).
Measures
Data for the study came from two sources: requests for assistance made by participants when they called 2-1-1 (expressed needs), and responses to a telephone survey screening for social needs (baseline survey screener).
Expressed needs.
When an individual calls 2-1-1 and seeks assistance with one or more social need, we consider those to be “expressed needs.” Operators at 2-1-1 treat each expressed need as a separate service request and classify the type of request using a taxonomy of over 10,000 categories and sub-categories (2-1-1 LA County, n.d.). In our sample, participants made 2,447 requests that were classified into 281 unique codes in the taxonomy. We grouped the 281 codes into 12 social needs categories and an “other” category. Eight of these categories overlapped with social needs assessed in the baseline survey: housing, utilities, healthcare, food, transportation, childcare, employment, and personal safety (n=1,924 combined requests). Four did not: adult/disabled care, legal services, financial assistance (e.g., tax services), and household goods (e.g., furniture vouchers) (n=365 combined requests). The remaining requests were categorized as “other” because they did not fall within a social need category (e.g., directory assistance) (n=158 requests).
We created a dichotomous variable for each of the 12 social needs categories, and participants received a “1” if they expressed to 2-1-1 having any need in that category or a “0” if they did not. Some participants had multiple service requests in the same category (e.g., shelters and homeless motel vouchers, both classified within housing); these were also coded as a “1”. The total number of expressed social needs for each participant was determined by summing across the 12 social need categories. Because 2-1-1 Operators can only document up to three service requests per call, a participant could have up to three expressed needs if each of their service requests fell within a different category.
Baseline survey screener.
Administered by the research team via telephone, the baseline survey assessed social needs using a brief screener including items based on Segal’s Personal Empowerment Scale and studies by Blazer and colleagues (Blazer et al., 2005; Segal et al., 1993). Eight items assessed the likelihood that in the next month the respondent would: (1) have a place to stay (housing); (2) be able to pay their current electric, gas or water bill in full (utilities); (3) have enough food to feed themselves and others in their home (food); (4) have reliable transportation to get to appointments, meetings, work, and getting the things they need for daily living (transportation); (5) have trouble finding or paying for childcare (childcare); and (6) be threatened physically by another person (personal safety). Response options were very likely/likely/unlikely/very unlikely. Responses of “very unlikely” and “unlikely” for items 1-4 were coded as “unmet”, as were responses of “very likely” and “likely” for items 5 and 6. Responses of “unlikely” or “very unlikely” for items 1-4, and “likely” or “very likely” for items 5-6 were classified as “unmet” needs.
Also assessed were: (7) the amount of space in the home (housing) with response options of too much/about the right amount/not enough; and (8) rating the safety of their neighborhood (neighborhood safety) with response options of very unsafe/unsafe/safe/very safe. Responses of “not enough” for item 7, and “very unsafe” or “unsafe” for item 8 were classified as “unmet”.
Other social needs items evaluated whether participants (9) had health insurance (healthcare); (10) had one person they think of as a personal doctor (healthcare); and (11) had trouble finding or keeping a job in the past 12 months (employment). Responses of “uninsured/do not have health insurance”, “no”, and “yes” were classified as “unmet” needs for items 9, 10 and 11, respectively.
Among the 11 items, two were related to housing (Item 1: unstable housing, Item 7: not enough space in the home) and healthcare (Item 9: no health insurance, Item 10: no personal doctor). Participants were classified as having housing needs if either of the two housing items were unmet, and classified as having healthcare needs if both healthcare items were unmet. Thus, we created 9 categories of social needs from the 11 items on the baseline screener, and participants could have 0-9 needs.
Unexpressed needs.
Two conditions had to be met in order for a social need that was identified in the baseline survey to be considered an “unexpressed need” for a participant. First, the social need had to be in one of the eight categories that were common to both 2-1-1 service requests and the baseline survey: housing, utilities, healthcare, food, transportation, childcare, employment, and personal safety. Neighborhood safety, the ninth baseline survey need category, was excluded because few individuals call 2-1-1 for this type of request. Second, the participant could have no expressed needs in the same category as an unexpressed need. For example, if a participant indicated in the baseline survey that they were unlikely to be able to pay their current electric, gas or water bill in full, but had already requested utility payment assistance when they called 2-1-1, “utilities” would not be an unexpressed need. But if the same participant had not requested help with utility payment assistance when calling 2-1-1, then “utilities” would be an unexpressed need.
Applying these conditions to each participant’s 2-1-1 requests and baseline survey responses, we coded each of the eight overlapping social need categories as a “1” if it was an unexpressed need or “0” if it was not. Missing data were coded as a “0.” The total number of unexpressed social needs for each participant was determined by summing across the eight social need categories (range: 0-8).
Demographics.
The baseline survey assessed participants’ gender, age, race/ethnicity, level of education, and annual pre-tax household income.
Analyses
Two datasets (one with 2-1-1 service requests and another with social needs baseline survey data) were merged and re-coded to create the unexpressed needs variables. Data were managed using R (R Core Team, 2019) and analyzed using SPSS (Version 25.0; Armonk, NY: IBM Corp.) and Stata (Stata Statistical Software: Release 16. College Station, TX, USA: StataCorp, 2019).
How many social needs?
Frequencies and mean number of social needs are reported for expressed needs, needs identified by the baseline survey, and unexpressed needs.
Which needs are more likely to be expressed versus unexpressed?
In each of the eight social need categories for which 2-1-1 requests and baseline survey responses are both available, we report the proportion of participants for whom the need was expressed versus unexpressed.
Are certain expressed needs associated with having certain unexpressed needs?
We estimated eight binary logistic regression models to predict each of the unexpressed needs (dependent variables) based on the eight overlapping expressed needs (independent variables). Each model included as predictors the expressed needs variables for all categories of social needs except the one being predicted. For example, because no participants could have both an expressed and unexpressed need for utility payment assistance, the model predicting unexpressed utility needs omitted expressed utility needs as a predictor, and all participants with expressed utility needs. We report odds ratios and 95% confidence intervals for each independent variable and chi-squares for each to assess overall model fit.
Findings
Participants’ mean age was 48.1 years. Most were female (72%) and Black (59%). Nearly one third (31%) had not completed high school, and half (51%) reported annual pre-tax household income less than $10,000 (see Table 1).
Table 1:
Sociodemographic characteristics and expressed and unexpressed needs (n= 1,397)
| Sample Characteristics | N (%) | Mean (SD) | |
|---|---|---|---|
| Gender | Female | 1,007 (72.2) | |
| Age (years) | < 25 | 34 (2.4) | 48.11 (12.25) |
| 25 – 40 | 397 (28.4) | ||
| 41 – 55 | 508 (36.4) | ||
| 56 – 65 | 378 (27.1) | ||
| > 65 | 80 (5.7) | ||
| Race | Black | 830 (59.4) | |
| White | 462 (33.1) | ||
| Other | 105 (7.6) | ||
| Ethnicity | Non-Hispanic | 1,358 (97.2) | |
| Hispanic | 28 (2.0) | ||
| Don’t know/Refused | 11 (0.7) | ||
| Education | < High school | 430 (30.8) | |
| High school/GED | 415 (29.1) | ||
| Some college | 314 (22.5) | ||
| College degree | 136 (9.7) | ||
| Don’t know/refused | 102 (7.3) | ||
| Annual income (USD$) | < 10,000 | 714 (51.1) | |
| 10,000 to < 15,000 | 250 (17.9) | ||
| 15,000 to < 20,000 | 146 (10.5) | ||
| 20,000 to < 25,000 | 113(8.1) | ||
| 25,000 to < 35,000 | 84 (6.0) | ||
| ≥ 35,000 | 42 (2.9) | ||
| Don’t know/refused | 48 (5.0) | ||
| Expressed needs (#) | 0 | 56 (4.0) | 1.23 (0.55) |
| 1 | 1,003 (71.8) | ||
| 2 | 302 (21.6) | ||
| 3 | 36 (2.6) | ||
| Baseline screener needs (#) | 0 | 285 (20.4) | 1.81 (1.46) |
| 1 | 376 (26.9) | ||
| 2 | 352 (25.2) | ||
| ≥3 | 384 (27.5) | ||
| Unexpressed needs (#) | 0 | 499 (35.7) | 1.13 (1.14) |
| 1 | 471 (33.7) | ||
| 2 | 253 (18.1) | ||
| ≥3 | 174 (12.5) | ||
Expressed and Unexpressed Social Needs
Table 1 also shows that on average, participants expressed 1.23 (SD= 0.55) social needs when calling 2-1-1, and reported 1.81 (SD= 1.46) needs when completing the brief 11-item (9 category) baseline survey. Of the social needs identified by the baseline survey, 1.13 (SD= 1.14) were classified as unexpressed needs because they were in one of the eight overlapping social need categories and were not requested by the participant when they called 2-1-1. Most participants (64.3%) had at least one unexpressed need; 30.6% had two or more unexpressed needs, and 12.5% had three or more unexpressed needs.
Expressed and Unexpressed by Type of Social Need
Figure 1 shows that some social needs were more likely to be expressed while others were more likely to be unexpressed. Among 919 participants with utility payment needs, 73% expressed the need when calling 2-1-1; for the remaining 27%, utility needs were unexpressed, identified only by the baseline survey. Similarly, housing needs (n=621) were more likely to be expressed than unexpressed, 67% to 33%. Social needs that were unexpressed more often than expressed included personal safety (93% to 7%), employment (92% to 8%), childcare (90% to 10%), transportation (86% to 14%), and healthcare (71% to 29%).
Figure 1:
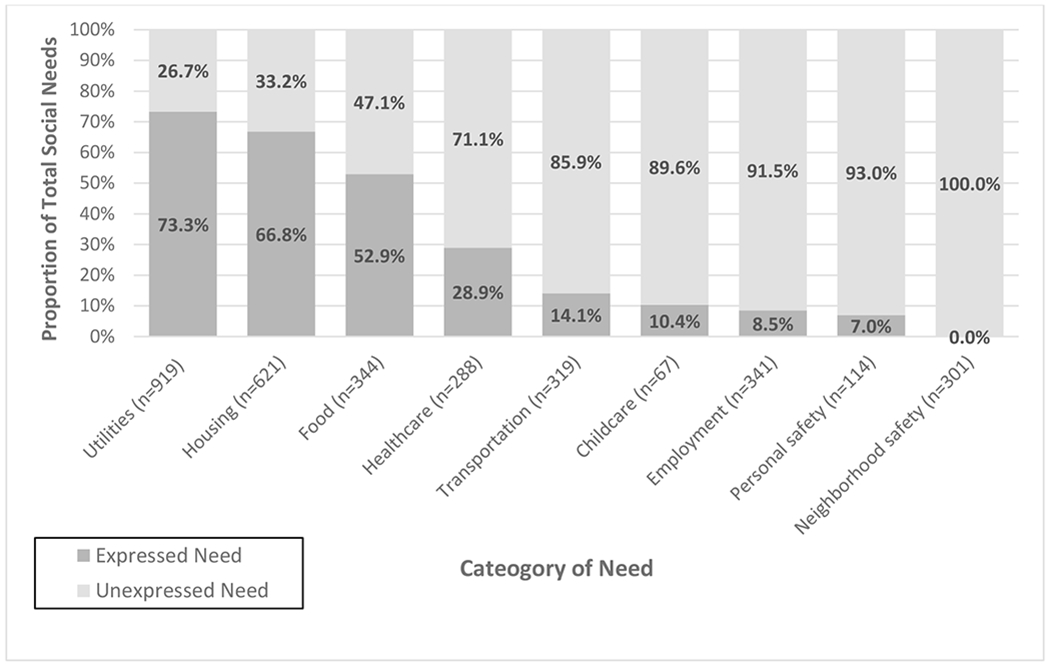
Proportion of social needs that are expressed or unexpressed, by category of need (n=1,397)
Associations between Expressed and Unexpressed Needs
In some instances, when participants expressed certain social needs to 2-1-1, the odds of them having certain other unexpressed social needs were significantly greater than the odds for those who did not express the same need to 2-1-1 (Table 2). In separate models, those who expressed housing as a social need had greater odds of having an unexpressed need related to transportation (Model 5: OR=1.73; 95% CI: 1.26-2.36) or utilities (Model 1: OR=1.44; 95% CI: 1.02-2.04) than those who did not express housing needs. Participants that expressed food needs had 57% greater odds of having unexpressed employment needs than those who did not express food needs (Model 7: OR=1.57; 95% CI: 1.08-2.28). Those who expressed transportation needs to 2-1-1 had greater odds of having unexpressed needs related to food (Model 3: OR=3.19; 95% CI: 1.45-7.02) and healthcare (Model 4: OR=2.18; 95% CI: 1.06-4.47) that those who did not express transportation needs. Similarly, those who expressed employment needs when calling 2-1-1 had greater odds of having unexpressed needs for personal safety (Model 8: OR=3.04; 95% CI: 1.20-7.68) and healthcare (Model 4: OR=2.58; 95% CI: 1.15-5.77) compared to those who did not express employment needs.
Table 2:
Estimated odds ratios and 95% confidence intervals from binary logistic regression models predicting unexpressed social needs
| Individual models predicting each unexpressed need | ||||||||
|---|---|---|---|---|---|---|---|---|
| Expressed needs | Utilities (n=725) | Housing (n=981) | Food (n=1,207) | Healthcare (n=1,307) | Transportation (n=1,352) | Childcare (n=1,353) | Employment (n=1,367) | Personal safety (n=1,389) |
| Utilities | - | 0.85 (0.60-1.21) | 0.94 (0.64-1.38) | 1.13 (0.80-1.59) | 0.83 (0.61-1.13) | 0.85 (0.46-1.54) | 1.04 (0.78-1.39) | 0.82 (0.52-1.29) |
| Housing | 1.44 (1.02-2.04) * | - | 1.06 (0.71-1.59) | 1.20 (0.84-1.71) | 1.73 (1.26-2.36) ** | 1.41 (0.77-2.58) | 1.34 (0.99-1.82) | 1.14 (0.72-1.83) |
| Food | 1.25 (0.83-1.89) | 1.18 (0.76-1.82) | - | 0.64 (0.38-1.08) | 1.28 (0.85-1.93) | 0.73 (0.30-1.78) | 1.57 (1.08-2.28) * | 1.40 (0.80-2.44) |
| Healthcare | 0.91 (0.51-1.62) | 0.63 (0.32-1.22) | 0.65 (0.28-1.51) | - | 0.80 (0.42-1.51) | 0.53 (0.12-2.33) | 1.40 (0.82-2.38) | 0.45 (0.14-1.50) |
| Transportation | 1.28 (0.64-2.56) | 1.53 (0.73-3.22) | 3.19 (1.45-7.02) ** | 2.18 (1.06-4.47) * | - | 1.04 (0.24-4.48) | 0.94 (0.45-1.94) | 1.38 (0.52-3.66) |
| Childcare | 2.01 (0.27-14.83) | 0.65 (0.08-5.71) | 4.39 (0.72-26.84) | † | 0.71 (0.08-6.02) | - | 1.64 (0.30-9.11) | 1.59 (0.18-13.91) |
| Employment | 1.77 (0.66-4.73) | 1.43 (0.55-3.72) | 1.06 (0.35-3.17) | 2.58 (1.15-5.77) * | 0.60 (0.21-1.75) | † | - | 3.04 (1.20-7.68) * |
| Personal safety | 1.41 (0.23-8.58) | 0.93 (0.10-8.45) | † | 0.78 (0.09-6.36) | 0.53 (0.06-4.36) | † | 1.21 (0.24-6.03) | - |
|
| ||||||||
| LR χ2 (df) | 7.66 (7) | 6.32 (7) | 11.31 (6) | 12.65 (6) * | 23.70 (7) ** | 4.20 (5) | 9.36 (7) | 11.37 (7) |
p < .05;
p < .01
No participants who expressed the need in this row had an unexpressed need in the intersecting column. The expressed need variable and participants who expressed it were therefore omitted from the model due to absence of variability on the outcome.
Discussion
In our sample of low-income adults, expressed social needs underestimated total social needs by about 1.13 needs per person (i.e., at least one social need was unexpressed). Certain social needs such as transportation, childcare, employment and personal safety that were commonly unexpressed, were identified through screening, but were seldom the focus of help-seeking behavior initiated by the individual.
These findings reinforce the importance of systematic screening for social needs as is now being adopted by many healthcare organizations (Andermann, 2018; Artiga & Hinton, 2018). The 11-item (9 category) social needs baseline survey often identified the same social needs that participants reported to 2-1-1, but also detected unexpressed needs for which they had not requested help. For nearly half (48.8%) of participants, the baseline survey identified all of the social needs they expressed to 2-1-1 in the eight overlapping categories.
However, not all low-income individuals will be seen regularly in a healthcare setting and/or screened there for social needs. Our findings are also informative for social service agencies and referral helplines that may encounter these individuals on a more frequent basis. Participants calling 2-1-1 for help with employment needs had 2.5 times greater odds of also having unexpressed healthcare needs and 2.1 times greater odds of having unexpressed transportation needs compared to participants not seeking help for employment. Other findings suggested possible links between housing (expressed) and utilities and transportation (both unexpressed); transportation and food; and, food and employment.
Practically speaking, such evidence could inform a more proactive and integrated approach to addressing social needs for social service agencies. For example, clients needing X also could be systematically screened for Y, and services addressing X and Y could be coordinated. A more anticipatory, data-based approach is one of the main goals of the current movement towards community information exchange (CIE) systems (Haque et al., 2018; Healthierhere.org, n.d.), and could help improve performance and outcomes of an often fragmented social service safety net system. For example, a 2-1-1 caller asking for help paying rent might be proactively screened for transportation needs, as well. If both were needed, the caller could be automatically entered through a CIE into separate queues for assistance from transportation agencies and housing agencies. The same would be true if that person entered the system through a transportation agency, or through a housing agency. 2-1-1 does not provide comprehensive case management, but other organizations do and a CIE database might help them identify eligible clients.
The associations reported here provide an initial proof-of-concept that some expressed social needs could be markers for other unexpressed needs. Because the evidence comes from a single study in a single state, we encourage researchers and practitioners to explore similar associations in other settings and locations to strengthen confidence in acting upon these findings.
It is tempting to infer from these findings that there is an underlying hierarchy of social needs in which addressing uncertainty about one’s housing, food and heat supersede in urgency or priority addressing other social needs. There is some support for this in the literature, with several studies showing that in the face of multiple social needs, low-income families will prioritize food and rent (Polit et al., 2000; Tach & Greene, 2014). In some cases, however, it may be that unexpressed needs are not less important or lower priorities than expressed needs, but rather that other considerations affect a person’s willingness to actively seek assistance to address an unexpressed need. For example, out of 114 participants that were concerned about interpersonal violence or being threatened physically, only 7% expressed that need to 2-1-1. They may have viewed it as sensitive (Billings & Cowley, 1995) or unchangeable, especially by 2-1-1 (Heinemann et al., 2002).
Our data do not explain why some needs are unexpressed. A 2016 report on help-seeking behaviors among low-income individuals identified three primary barriers to help-seeking: insufficient knowledge of resources, survival fatigue from the stress and strain of living with scarcity, and psychological factors such as perceived stigma associated with not being able to care for one’s self or family (Lens et al., n.d.). Additionally, mistrust and fear may act as barriers. For example, many Hispanics are disinclined to engage with services and resources (e.g., housing, medical care) fearing being reported to immigration agencies or affecting their citizenship application (Ro, 2020).
In some cases, individuals may feel they can resolve certain needs outside the social service system (e.g., through their social support network), or they may realize that certain services can only be used once within a specific timeframe (Boyum et al., 2016) and want to save that request for a more dire situation. Still other needs might not be expressed because the caller knows from past interactions that they are not eligible.
There are some limitations that must be considered in our approach and analysis. First, although 2-1-1 data may be the closest we come in the U.S. to a daily surveillance system of social needs (Kreuter, Garg, Javed, et al., 2020), they do not necessarily provide a complete picture of community need. Use of 2-1-1s can be greater in urban than rural settings in some states, and because many individuals will seek help elsewhere (i.e., going directly to a specific service provider) or not at all, 2-1-1s almost certainly underestimate community needs.
Additionally, in regression analyses, odds ratios for needs that were expressed by fewer participants, such as childcare, did not reach significance. For non-significant findings there may not have been enough cases to provide the power to detect more subtle relationships between expressed and unexpressed needs. Also, our baseline social needs screener did not measure all possible social needs. For example, within the category of housing we did not assess housing quality, which is included in some other social needs screeners (Cartier et al., 2018).
Additionally, although some 2-1-1 operators document brief call notes along with a maximum of three service requests per participant, these notes were not included in the analysis. It is possible, therefore, that some participants with the maximum of three expressed needs (n= 36 (2.6%) of the sample), might have additional needs documented in the call notes or would have identified other needs if given the opportunity, which could lead to underestimating expressed needs and overestimating unexpressed needs. Finally, our sample is comprised of adult smokers who called 2-1-1, limiting generalizability to other samples and those who do not actively seek assistance with social needs
Future research can help overcome these limitations, using participatory and qualitative methods to provide deeper insights into the reasons some social needs are expressed and others unexpressed, and whether people’s willingness to express certain social needs might vary by setting (e.g., 2-1-1s, healthcare, schools).
Practice-based evidence demonstrating the feasibility of applying conditional “if-then” types of social needs screening in the social service sector also would help evaluate the potential impact of study findings. It would be inefficient and likely unrealistic to expect that every community would have the resources to conduct a social needs survey to estimate community need. However, the findings from this study suggest that by adding a few targeted assessments questions, existing social service resources such as 2-1-1 might be able to capture a fuller picture of community needs.
Ultimately, application of these findings could enhance integration across social service sectors and agencies and help support CIE systems (211 San Diego, n.d.) now being implementing in some communities. We encourage other researchers and practice professionals to join us in exploring these questions and potential applications.
What is known about this topic?
Social needs are disproportionately present among low-income populations.
The healthcare sector has an increasing interest in addressing social needs, but requires quality data on individual and community social needs.
What this paper adds?
Expressed social needs underestimated total social needs among low-income adults.
Certain social needs that were commonly unexpressed, were identified through screening, but were seldom the focus of help-seeking behavior initiated by the individual.
Our findings reinforce the importance of systematic screening for social needs and provide an initial proof-of-concept that some expressed social needs could be markers of other unexpressed needs. For healthcare and social service agencies, such evidence could inform a more proactive and integrated approach to addressing social needs.
Funding sources:
National Cancer Institute R01CA201429 (PI: Kreuter);
NIDDK 1R01DK115916-01 (PI: Kreuter; McQueen)
Footnotes
Conflict of interest statement:
The authors have no conflicts of interest to declare.
Data Availability Statement:
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
References
- 2-1-1 LA County, (n.d.). The Taxonomy Web Site. https://211taxonomy.org/
- 211.org. (n.d.). https://www.211.org/pages/about
- 211 San Diego, (n.d.). https://ciesandiego.org/
- Alio P (2017). Identifying, prioritizing, and addressing client needs: Strategies for home visitors. www.mihcoe.org
- Andermann A (2018). Screening for social determinants of health in clinical care: Moving from the margins to the mainstream. In Public Health Reviews (Vol. 39, Issue 1). BioMed Central Ltd. 10.1186/s40985-018-0094-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Artiga S, & Hinton E (2018). Beyond Health Care: The Role of Social Determinants in Promoting Health and Health Equity / The Henry J. Kaiser Family Foundation. KFF. https://www.kff.org/disparities-policy/issue-brief/beyond-health-care-the-role-of-social-determinants-in-promoting-health-and-health-equity/ [Google Scholar]
- Billings JR, & Cowley S (1995). Approaches to community needs assessment: a literature review. Journal of Advanced Nursing, 22(4), 721–730. 10.1046/j.1365-2648.1995.22040721.x [DOI] [PubMed] [Google Scholar]
- Blazer DG, Sachs-Ericsson N, & Hybels CF (2005). Perception of unmet basic needs as a predictor of mortality among community-dwelling older adults. American Journal of Public Health, 95(2), 299–304. 10.2105/AJPH.2003.035576 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boyum S, Kreuter MW, McQueen A, Thompson T, & Greer R (2016). Getting Help from 2-1-1: A Statewide Study of Referral Outcomes. Journal of Social Service Research, 42(3), 402–411. 10.1080/01488376.2015.1109576 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bradshaw, & Jonathan. (1972). Taxonomy of social need. In Problems and progress in medical care: essays on current research (7th Series, pp. 71–82). Oxford University Press. http://eprints.whiterose.ac.uk/118357/ [Google Scholar]
- Cartier Y, Fichtenberg C, & Gottlieb L (2018). Social Interventions Research & Evaluation Network (SIREN): Screening Tools Comparison, https://sirenetwork.ucsf.edu/tools-resources/mmi/screening-tools-comparison
- Haque SN, Ebron S, Bailey R, & Blumenthal B (2018). Using Health Information Exchange to Support Community-based Innovations. Perspectives in Health Information Management, https://perspectives.ahima.org/usinghie/ [Google Scholar]
- Healthierhere.org. (n.d.). Community Information Exchange. https://www.healthierhere.org/wp-content/uploads/2019/10/CIE-Opportunity-Onepager-2.0-103019.pdf
- Heflin C, & Scott EK (2011). Mitigating Material Hardship: The Strategies Low-Income Families Employ to Reduce the Consequences of Poverty*. Sociological Inquiry, 81(2), 223–246. 10.1111/j.1475-682X.2011.00369.x [DOI] [Google Scholar]
- Heinemann AW, Sokol K, Garvin L, & Bode RK (2002). Measuring unmet needs and services among persons with traumatic brain injury. Archives of Physical Medicine and Rehabilitation, 83(8), 1052–1059. 10.1053/apmr.2002.34283 [DOI] [PubMed] [Google Scholar]
- Kreuter M, Garg R, Javed I, Golla B, Wolff J, & Charles C (2020). 3.5 Million Social Needs Requests During COVID-19: What Can We Learn From 2-1-1? Health Affairs. https://www.healthaffairs.org/do/10.1377/hblog20200729.432088/full/ [Google Scholar]
- Kreuter M, Garg R, Thompson T, McQueen A, Javed I, Golla B, Caburnay C, & Greer R (2020). Assessing The Capacity Of Local Social Services Agencies To Respond To Referrals From Health Care Providers. Health Affairs (Project Hope), 39(4), 679–688. 10.1377/hlthaff.2019.01256 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lens V, Nugent M, Wimer C, & Pavlenko A (n.d.). Why don’t low-income New Yorkers seek help? https://www.robinhood.org/uploads/2019/12/PovertyTracker_Winter_Final.pdf
- McQueen A, Roberts C, Garg R, Caburnay C, Fu Q, Gordon J, Bush T, Pokojski R, Thompson T, & Kreuter M (2019). Specialized tobacco quitline and basic needs navigation interventions to increase cessation among low income smokers: Study protocol for a randomized controlled trial. Contemporary Clinical Trials, 80, 40–47. 10.1016/j.cct.2019.03.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Polit DF, London AS, Martinez JM, & Mott CS (2000). Food Security and Hunger in Poor, Mother-Headed Families in Four U.S. Cities Funders of the Project on Devolution and Urban Change: A Working Paper, www.mdrc.org.
- Ro C (2020, April 20). Coronavirus: Why some racial groups are more vulnerable. BBC Future. https://www.bbc.com/future/article/20200420-coronavirus-why-some-racial-groups-are-more-vulnerable [Google Scholar]
- Segal SP, Silverman C, & Temkin T (1993). Empowerment and self-help agency practice for people with mental disabilities. Social Work, 38(6), 705–712. http://www.ncbi.nlm.nih.gov/pubmed/8256142 [PMC free article] [PubMed] [Google Scholar]
- Shoham S, & Strauss SK (2008). Immigrants’ information needs: their role in the absorption process. Information Research, 13(4), 359. http://informationr.net/ir/13-4/paper359.html [Google Scholar]
- Tach LM, & Greene SS (2014). “Robbing Peter to pay Paul”: Economic and cultural explanations for how lower-income families manage debt. Social Problems, 61(1), 1–21. [Google Scholar]
- Thomas-Henkel C, & Schulman M (2017). Screening for Social Determinants of Health in Populations with Complex Needs: Implementation Considerations, www.chcs.org/sdoh-screening/.
- Thompson T, Kreuter MW, & Boyum S (2015). Promoting Health by Addressing Basic Needs: Effect of Problem Resolution on Contacting Health Referrals. Health Education and Behavior, 43(2), 201–207. 10.1177/1090198115599396 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.