

Abstract
Background:
Exposure to fatal police violence may play a role in population-level inequities in risk for preterm delivery.
Objective:
To evaluate whether exposure to fatal police violence during pregnancy affects the hazard of preterm delivery and whether associations differ by race/ethnicity and fetal sex.
Methods:
We leveraged temporal variation in incidents of fatal police violence within census tracts to assess whether occurrence of fatal police violence in a person’s tract during pregnancy was associated with increased hazard of extremely (20–27 weeks), early (28–31 weeks), moderate (32–33 weeks), and late (32–36 weeks) preterm delivery in California from 2007–2015. We used both death records and the Fatal Encounters database to identify incidents of fatal police violence. We estimated hazard ratios (HR) using time-varying Cox proportional hazard models stratified by census tract, controlling for age, race/ethnicity, educational attainment, health insurance type, parity, and the year and season of conception. We further stratified by race/ethnicity and infant sex to evaluate whether there were differential effects by these characteristics.
Results:
Exposure to an incident of fatal police violence was associated with a small increase in the hazard of late preterm birth using both the death records (N=376,029; HR 1.05, 95% CI 1.00, 1.10) and the Fatal Encounters data (N=938,814; HR 1.03, 95% CI 1.00, 1.06). We also observed an association for moderate preterm birth in the Fatal Encounters data (HR 1.06, 95% CI 0.98, 1.15). We did not observe associations for early or extremely preterm birth in either data source. Larger relative hazards of moderate (HR 1.25, 95% CI 0.93, 1.68) and late preterm delivery (HR 1.18, 95% CI 1.05, 1.33) were observed among Black birth parents with female births in the Fatal Encounters data.
Conclusions:
Preventing police use of lethal force may reduce preterm delivery in communities where such violence occurs.
Keywords: police, violence, premature birth, pregnancy, health inequity
Social media quote
In California from 2007–2015, occurrence of fatal police violence against Black people in the community was associated with an increased hazard of moderate preterm delivery (32–33 weeks) among Black people who were pregnant when the incident occurred.
Background
Police violence is recognized as a critical problem in public health and a barrier to health equity.1–4 In neighborhoods with predominantly Black or Brown residents, people are exposed to greater police surveillance and greater use-of-force, independent of situational factors (e.g., resisting), officer characteristics (e.g., training), and contextual factors (e.g., neighborhood crime rate).5–7 In particular, Black residents are more likely to be victims of fatal police violence compared to people of other races or ethnicities.8,9 This has been facilitated in part by racial residential segregation, in which Black families were restricted to living in certain neighborhoods that subsequently suffered disinvestment and criminalization.10,11 Given that police violence disproportionately affects communities of color and is rooted in the institutional authority of the state, it is a form of structural racism that may contribute to health inequities,10,12 through either direct physical victimization13,14 or witnessing or hearing about police violence.15,16
Given evidence that experiences of mental distress and stressful life events during pregnancy can increase risk of preterm delivery,17–19 exposure to fatal police violence during pregnancy may have similar implications for the health of the fetus and gestating parent, henceforth “birth parent”. Other forms of community violence have been associated with adverse pregnancy outcomes,20–24 and evidence suggests residents exposed to community violence can experience post-traumatic stress disorder or elevations in anxiety and depression.25–27 Acute exacerbation of these mental health issues during pregnancy has been tied to adverse pregnancy outcomes.28–31
Black parents have the highest levels of preterm birth,32 which has not been explained by individual-level risk factors.33 Therefore, structural determinants should be examined as drivers of inequities in neonatal health.34,35 Given the disproportionate victimization of Black people by police violence, pregnant Black people may worry that their child’s life is devalued and that their family is at risk of harm.36–38 Thus, Black birth parents may be more likely to internalize fatal police violence as an explicit threat to themselves and their families. Evidence suggests that the physiologic impacts of acute stressors may vary based on chronic stress levels;39 therefore, given the potential for both greater potency of fatal police violence as a stressor and higher chronic stress levels for Black people,25,40,41 there may be differential impacts of police violence by race/ethnicity. Furthermore, evidence suggests there may be important interactions between exposure to stress, the immune system, and fetal sex hormones that may influence risk for adverse outcomes by fetal sex.42,43 Accordingly, we hypothesized the relationship between fatal police violence and preterm birth may differ by fetal sex.
Research on the relationship between exposure to police violence and reproductive health outcomes is limited.44 This may be due in part to the fact that communities where police violence occurs have unique characteristics—like underinvestment in infrastructure, education, health care services, and sources of economic mobility—that make them difficult to compare to other communities.11 Because these characteristics are so highly correlated, it is difficult to disentangle them by statistical adjustment.45 Therefore, to isolate the association between exposure to fatal police violence and preterm birth, we leveraged temporal variability in fatal police violence within communities to examine the acute impact of fatal police violence on the hazard of preterm delivery among those who are pregnant at the time of its occurrence.
Methods
Cohort selection
This study utilized birth records from 2007–2015 and death records from 2006–2015 from the California Department of Public Health, Center for Health Statistics and Informatics. We also used the Fatal Encounters database from 2006–2015. Each of these data sources are described in more detail below. We included all singleton live births for which conception is estimated to have occurred after January 1, 2007 and before March 1, 2015 to ensure conceptions of all gestational ages were observed.46 We used birth parent address at delivery to determine census tract of residence. There were 4,028,133 live singleton births in California with estimated conception dates between January 1, 2007 and March 1, 2015. After removing 4.4% of births that were missing information on the outcome or covariates, our sample size was 3,850,390 (Table 1).
Table 1.
Sociodemographic characteristics of people who gave birth in California with conception dates between January 1, 2007 and March 30, 2015, compared to those living in a neighborhood with any incident of fatal police violence during the study period, by exposure status and across data sources.
| All California births N (%) |
Death records | Fatal encounters | |||||
|---|---|---|---|---|---|---|---|
| Total N (%) |
Not exposed to fatal police violence N (%) |
Exposed to fatal police violence N (%) |
Total N (%) |
Not exposed to fatal police violence N (%) |
Exposed to fatal police violence N (%) |
||
| N | 3,850,390 | 376,029 | 341,936 | 34,093 | 938,814 | 841,314 | 97,500 |
| Preterm | |||||||
| 20–27 weeks | 15,698 (0.4) | 1,664 (0.4) | 1,575 (0.5) | 89 (0.3) | 4,258 (0.5) | 3,972 (0.5) | 286 (0.3) |
| 28–31 weeks | 22,128 (0.6) | 2,267 (0.6) | 2,121 (0.6) | 146 (0.4) | 5,868 (0.6) | 5,388 (0.6) | 480 (0.5) |
| 32–33 weeks | 28,270 (0.7) | 2,920 (0.8) | 2,694 (0.8) | 226 (0.7) | 7,415 (0.8) | 6,735 (0.8) | 680 (0.7) |
| 34–36 weeks | 200,022 (5.2) | 20,402 (5.4) | 18,660 (5.5) | 1,742 (5.1) | 50,690 (5.4) | 45,853 (5.5) | 4,837 (5.0) |
| Race/ethnicity | |||||||
| White, non-Latinx | 1,060,741 (27.6) | 78,079 (20.8) | 71,245 (20.8) | 6,834 (20.1) | 206,091 (22.0) | 185,246 (22.0) | 20,845 (21.4) |
| Black, non-Latinx | 202,477 (5.3) | 21,403 (5.7) | 19,444 (5.7) | 1,959 (5.8) | 64,843 (6.9) | 57,821(6.9) | 7,022 (7.2) |
| Asian or Pacific Islander, non-Latinx | 524,797 (13.6) | 35,578 (9.5) | 32,649 (9.6) | 2,929 (8.6) | 99,986 (10.7) | 90,597 (10.8) | 9,389 (9.6) |
| Other, non-Latinx | 97,796 (2.5) | 8,385 (2.2) | 7,672 (2.2) | 713 (2.1) | 22,930 (2.4) | 20,557 (2.4) | 2,373 (2.4) |
| Latinx | 1,964,579 (51.0) | 232,584 (61.9) | 210,926 (61.7) | 21,658 (63.5) | 544,964 (58.1) | 487,093 (57.9) | 57,871 (59.4) |
| Educational attainment | |||||||
| Less than high school | 839,244 (21.8) | 107,703 (28.6) | 97,469 (28.5) | 10,234 (30.0) | 253,272 (27.0) | 226,101 (26.9) | 27,171 (27.9) |
| High school graduate | 1,006,821 (26.2) | 111,352 (29.6) | 101,227 (29.6) | 10,125 (29.7) | 273,834 (29.2) | 244,896 (29.1) | 28,938 (29.7) |
| Some college | 973,788 (25.3) | 91,125 (24.2) | 82,997 (24.3) | 8,128 (23.8) | 234,979 (25.0) | 210,613 (25.0) | 24,366 (25.0) |
| College graduate | 1,030,537 (26.8) | 65,849 (17.5) | 60,243 (17.6) | 5,606 (16.4) | 176,729 (18.8) | 159,704 (19.0) | 17,025 (17.5) |
| Age (mean) | 28.6 | 27.6 | 27.6 | 27.5 | 27.8 | 27.8 | 27.6 |
| Insurance type | |||||||
| Public | 1,902,580 (49.4) | 224,316 (59.7) | 203,650 (59.6) | 20,666 (60.6) | 547,608 (58.3) | 489,110 (58.1) | 58,498 (60.0) |
| Private | 1,799,930 (46.8) | 140,079 (37.3) | 127,672 (37.3) | 12,407 (36.4) | 358,955 (38.2) | 323,291 (38.4) | 35,664 (36.6) |
| Self-pay or other | 147,880 (3.8) | 11,634 (3.1) | 10,614 (3.1) | 1,020 (3.0) | 32,251 (3.4) | 28,913 (3.4) | 3,338 (3.4) |
| Parity | |||||||
| 1 | 1,526,031 (39.6) | 139,482 (37.1) | 126,857 (37.1) | 12,625 (37.0) | 357,517 (38.1) | 320,533 (38.1) | 36,984 (37.9) |
| 2 | 1,220,576 (31.7) | 113,628 (30.2) | 103,407 (30.2) | 10,221 (30.0) | 285,248 (30.4) | 256,002 (30.4) | 29,246 (30.0) |
| 3 or more | 1,103,783 (28.7) | 122,919 (32.7) | 111,672 (32.7) | 11,247 (33.0) | 296,049 (31.5) | 264,779 (31.5) | 31,270 (32.1) |
Note: The Other, non-Latinx group included American Indian, non-Latinx; Alaska Native, non-Latinx; multi-race, non-Latinx; or other race, non-Latinx people.
Exposure
We evaluated birth parent exposure to fatal police violence within the census tract of residence during pregnancy using two sources of data. First, we used death records from California and identified cases of fatal police violence via the ICD-10 legal intervention cause of death codes (further description is available in the eAppendix). However, since prior literature suggests these records may undercount deaths due to legal intervention,47 we also used the Fatal Encounters database of incidents of fatal police violence. This database is publicly available and compiled by paid researchers and crowd-sourced contributions using media coverage and public records to identify instances of police action that result in a fatality. Each entry is validated against other existing media databases and data from government agencies, and recent studies have suggested these data are more complete than death records.48
The death records were geocoded to the decedent’s address at the time of death, and the Fatal Encounters records were geocoded to the location of the fatal interaction between the decedent and the police. Therefore, our analyses using the death records evaluate the impact on preterm birth of having a neighbor killed by police during pregnancy, whereas the analyses using the Fatal Encounters database assess the impact of a police killing occurring in a person’s neighborhood during pregnancy.
To ensure variation in the exposure within neighborhoods, we restricted our analyses to neighborhoods in which there was at least one incident of fatal police violence over the study period. For the analysis using death records, restriction to exposed census tracts resulted in a sample size of 376,029. Of these, 34,093 birth parents (9.1%) were exposed to fatal police violence during their pregnancy. Using the Fatal Encounters data, there were 938,814 birth parents who lived in a census tract in which there was a police-related fatality over the study period, and 97,500 birth parents (10.4%) were exposed during pregnancy. There were no census tracts in which all birth parents were exposed, and therefore no exposed birth parents were excluded from the analysis. In general, census tracts in which there was at least one incident of fatal police violence tended to have a greater proportion of birth parents who were Black or Latinx, had less than high school education, and had public insurance compared to all births in California (Table 1).
Outcome
Time to birth was measured using the best obstetric estimate of gestational age in weeks from the birth records. We excluded implausible gestational ages below 20 or above 44 weeks. We defined four categories of preterm birth: extremely preterm (delivery during 20–27 weeks gestation), early preterm (delivery during 28–31 weeks), moderate preterm (delivery during 32–33 weeks), and late preterm (delivery during 34–36 weeks).
Covariates
We adjusted for birth parent age, age-squared (to account for possible non-linearities in the effect of age), race/ethnicity, educational attainment, health insurance type, parity, and the year and season of conception. These confounders came from the birth record. In California birth records, race and Latino origin are recorded separately. Birth record race categories included White, Black or African American, Asian, Pacific Islander, Native American, and Alaska Native. For the analyses that compare associations between Black versus non-Black people, participants were categorized as Black if their reported race was Black or African American alone or in combination with other races or ethnicities. For the race-concordant analyses and analyses with more detailed racial categories, we used the more common approach of classifying any person of Latino origin, including Mexican, Mexican-American, Puerto Rican, Cuban, Spanish, or other Latino origin, as Latinx regardless of their recorded race (Table 1). We calculated the year and season of conception from the conception date, which we estimated by subtracting the obstetric estimate of gestational age at birth from the date of birth. Additional information about covariates is available in the eAppendix.
Statistical Analysis
We analyzed the hazard of preterm delivery among people who lived in the same census tract and either did or did not have incidents of fatal police violence occur in that tract during the length of their pregnancies, which we defined as the period between the estimated conception date and the date of birth. Evaluating the relationship between exposures that occur during pregnancy and preterm birth can be problematic because infants born preterm by definition have less time in-utero to accrue exposure. When the outcome is a function of time at risk, and time-varying exposures are assessed as though they occurred at the start of follow up (or in this case, at conception), immortal time bias can result.49 To address this, we analyzed time to birth as a survival outcome, first conducting descriptive analyses using Kaplan Meier survival plots and then estimating time-varying Cox proportional hazard models stratified by census tract.50 This approach allows the person-time in exposed and unexposed states to be accurately represented in the estimation, and permits each census tract to have its own baseline hazard, analogous to including a fixed effect on each census tract. We estimated separate models for each category of preterm birth, and used robust standard errors to address clustering at the census tract-level. We evaluated the proportional hazards assumption and covariates in violation were interacted with time.
To evaluate the extent to which fetal sex modified the overall results, we included an interaction term in the main analyses and calculated the relative excess risk due to interaction (RERI) using the following equation for evaluating additive interaction in proportional hazard models:51 , where is the estimated hazard ratio for exposure to fatal police violence, is the estimated hazard ratio for a female birth, and is the estimated hazard ratio for exposure to fatal police violence, having a female birth, and their interaction.
We also estimated race-concordant analyses; that is, whether incidents of fatal police violence involving a victim of the birth parent’s own racial/ethnic group increased hazard of preterm delivery. For these analyses, we matched the race/ethnicity of the victim on the death records or the Fatal Encounters database to that of the birth parent on the birth records.
We examined overall associations and stratified by infant sex, parental race/ethnicity, and infant sex by parental race/ethnicity. Because our hypothesis was that associations may be stronger for Black people, our main comparison was Black versus non-Black people.
Sensitivity analyses
To assess the robustness of our results, we conducted two sensitivity analyses. First, we stratified by detailed racial/ethnic groups. Second, we included fetal deaths (after 20 weeks gestation) as events to account for their occurrence as a possible competing risk for preterm birth. Due to the unavailability of fetal death records after 2011, we conducted these analyses from 2007–2011.
All analyses were conducted using Stata version 13.1; code is available in the appendix.
Ethics approval
This study was approved by the Committees for the Protection of Human Subjects for the California Health and Human Services Agency and the University of California, Berkeley.
Results
Those who were exposed to fatal police violence during pregnancy had slightly higher likelihood of birth before 37 weeks (eFigures 1 and 2). In adjusted models, we observed a small, but precise increased hazard of late preterm birth (34–36 weeks) associated with exposure to fatal police violence during pregnancy using both the death records (HR 1.05, 95% CI 1.00, 1.10) and the Fatal Encounters data (HR 1.03, 95% CI 1.00, 1.06) (Figure 1). There was suggestive evidence of effect modification by fetal sex, as the associations were slightly stronger for female compared to male fetuses in both the death records and Fatal Encounters data. We also observed a similar association for moderate preterm birth (32–33 weeks) in the Fatal Encounters data. Associations for earlier subtypes of preterm birth were smaller overall and much less precise. To evaluate the extent to which fetal sex affected the overall results, we included an interaction term between the exposure and fetal sex in the model for late preterm birth and calculated the RERI.51 We observed a positive estimate of the RERI for both the death records (0.03, 95% CI −0.07, 0.13) and Fatal Encounters data (0.05, 95% CI −0.01, 0.10).
Figure 1.
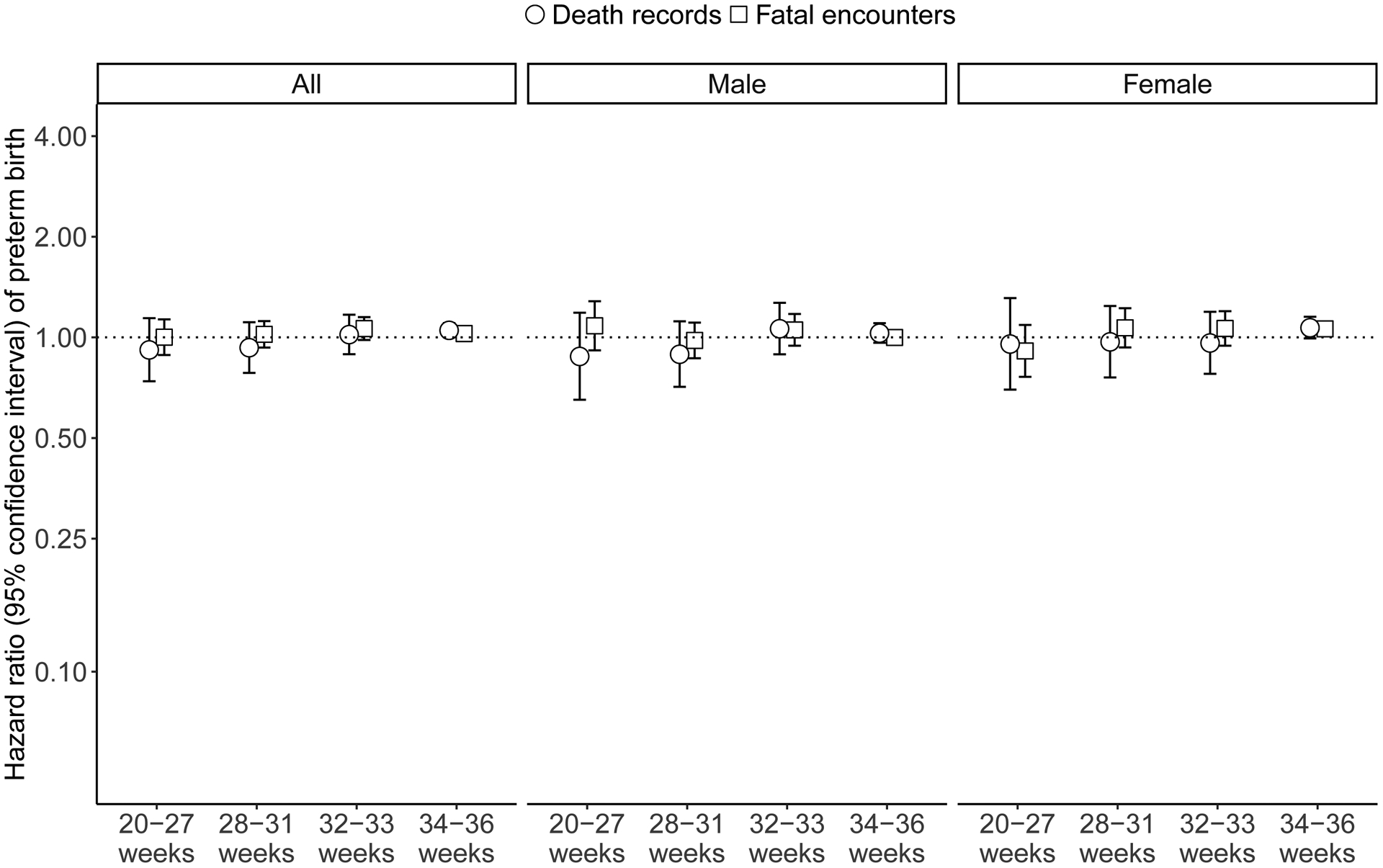
Hazard ratios of preterm birth categories, overall and by fetal sex, by exposure to fatal police violence in a person’s census tract during pregnancy among California residents with live singleton births from 2007–2015 who lived in census tracts with at least one incident of fatal police violence during the study period.
Note: These analyses controlled for birth parent age, age-squared, race/ethnicity, educational attainment, health insurance type, parity, and the year and season of conception.
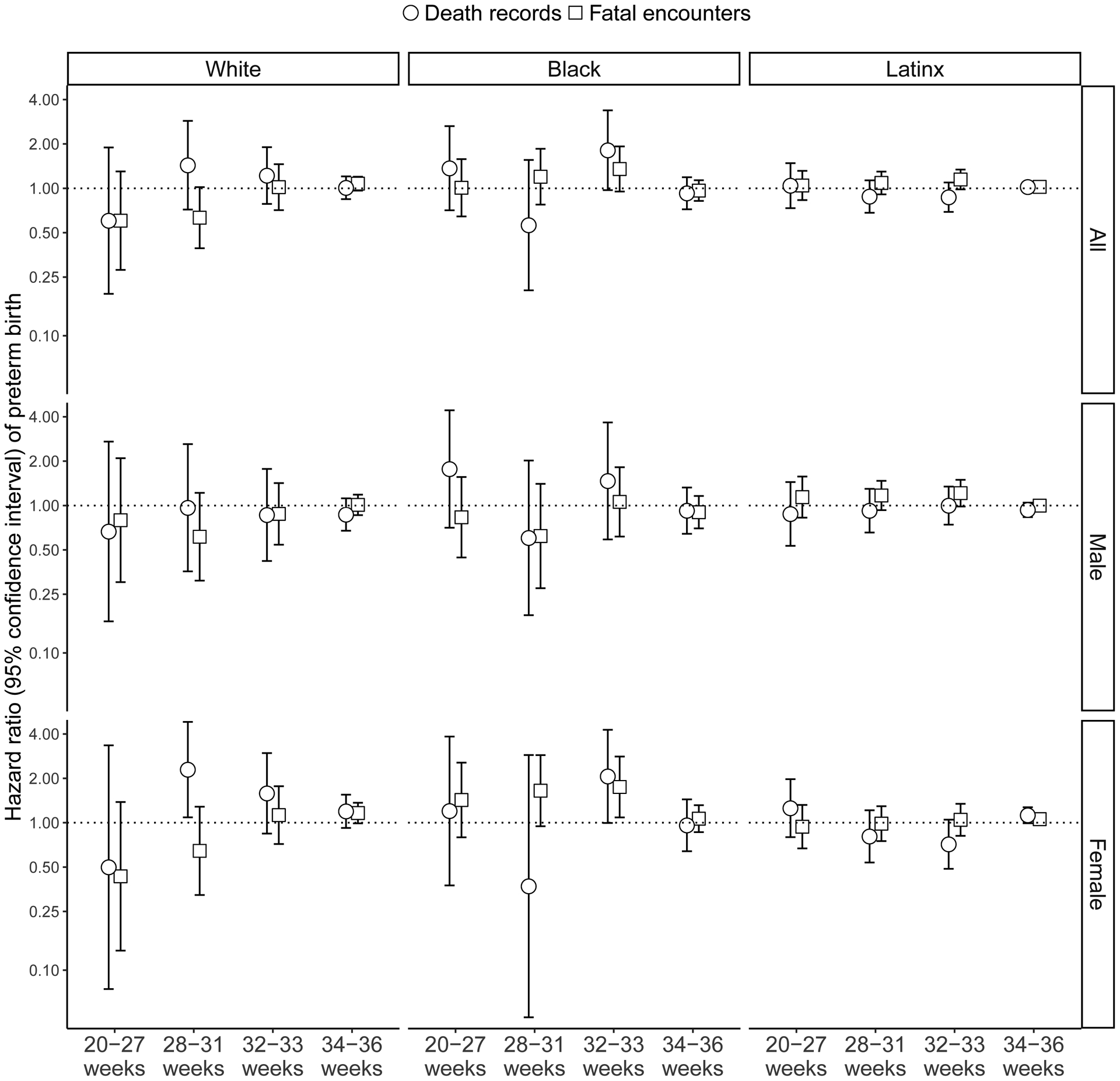
Analyses stratified by race showed stronger associations among Black birth parents overall for moderate preterm birth (32–33 weeks), but not late preterm birth (34–36 weeks), although estimates were imprecise (Figure 2). Stratification by additional race/ethnic groups showed no consistent patterning, and confidence intervals were wide (eFigure 3). We observed elevated associations for both moderate and late preterm birth among Black birth parents with female infants, especially in the Fatal Encounters data (Figure 2). In the race-concordant analyses, in which we evaluated the association between preterm birth and an incident of fatal police violence in which the victim’s race/ethnicity matched that of the birth parent, we observed stronger associations among Black birth parents for moderate preterm birth (32–33 weeks), particularly among those with female infants in the death records (HR 2.06, 95% CI 1.00, 4.27) and Fatal Encounters (HR 1.75, 95% CI 1.09, 2.81) (Figure 3). We also observed elevated associations among Latinx birth parents with female infants for late preterm birth (34–36 weeks) in the death records (HR 1.06, 95% CI 0.97, 1.15) and Fatal Encounters (HR 1.12, 95% CI 0.99, 1.27) (Figure 3).
Figure 2.

Hazard ratios of preterm birth categories, by birth parent race/ethnicity and fetal sex, by exposure to fatal police violence in a person’s census tract during pregnancy among California residents with live singleton births from 2007–2015 who lived in census tracts with at least one incident of fatal police violence during the study period.
Note: These analyses controlled for birth parent age, age-squared, educational attainment, health insurance type, parity, and the year and season of conception.
Figure 3.
Hazard ratios of preterm birth categories, by birth parent race/ethnicity and fetal sex, by exposure to fatal police violence against a victim of the same race as the birth parent in their census tract during pregnancy among California residents with live singleton births from 2007–2015 who lived in census tracts with at least one incident of fatal police violence during the study period.
Note: These analyses controlled for birth parent age, age-squared, race/ethnicity, educational attainment, health insurance type, parity, and the year and season of conception.
In sensitivity analyses, the findings were largely consistent. The analyses that included fetal deaths found a similar overall association for late preterm birth using the Fatal Encounters data, but the results using the death records were attenuated (eFigure 4). There was also less clear patterning by fetal sex overall. However, when stratifying by birth parent race/ethnicity, we observed stronger associations for Black birth parents with female infants, especially for moderate preterm birth (32–33 weeks) (eFigure 5). The race-concordant results that included fetal deaths resulted in similar findings (eFigure 6).
Comment
Principal findings
In this study we found that exposure to fatal police violence during pregnancy was associated with small increased hazard of late preterm birth. We also found suggestive patterns of effect modification for Black birth parents with female infants. Our results were similar in models utilizing two different measures of exposure to fatal police violence, suggesting that both living in a census tract in which fatal police violence occurred and having a neighbor who was killed by the police may be detrimental for birth outcomes. Race-concordant analyses, in which we matched the race of the victim and the birth parent, also indicated elevated hazard of moderate preterm delivery (32–33 weeks) associated with fatal police violence exposure among Black birth parents in both data sources. This suggests exposure to fatal police violence during pregnancy, especially when the victim is Black, may play a role in population-level inequities in preterm delivery.
Strengths of the study
We evaluated nine years of data on births and incidents of fatal police violence in California, a large and diverse state. We compared people within the same census tracts to reduce issues of structural confounding, and utilized two different sources of data on fatal police violence, which minimizes the chance that our findings were due to irregularities in one data source. We estimated hazards of preterm birth using time-varying Cox proportional hazard models in order to address issues of immortal time bias, and stratified by race and sex to assess the possibility of heterogeneous effects of exposure. We also evaluated four different categories of preterm birth, which are thought to have different etiologies and have distinct implications for future child development.
Limitations of the data
This study had several limitations. In particular, we used administrative data that has several potential sources of measurement error. We only had access to birth parent addresses at the time of delivery. Therefore, exposure status for people who moved during pregnancy may be misclassified. We used the best obstetrical estimate of gestational age to determine preterm birth categories; however, previous work has shown it may underestimate preterm births compared to early ultrasound.55 We were unable to separate spontaneous versus indicated preterm delivery as there is insufficient information on the birth records. In addition, data on fatal police violence have not been reliably collected in California or the United States generally. In particular, Black victims of fatal police violence may be more likely to have their cause of death misclassified in vital statistics data.48 To address this, we used two sources of data that capture different measures of fatal police violence. Increased media attention in recent years around deaths from police violence may have resulted in more incidents being captured in later years for both the Fatal Encounters and death records; however, by including fixed effects for the year of conception in our analysis, we aimed to reduce the possibility that these time trends in reporting biased our results. In line with existing research on neighborhood violence and health, we used census tracts to characterize parental exposure; however, they are an imperfect proxy for communities, and our approach may have resulted in some exposure misclassification if people were exposed to deaths in nearby tracts. Finally, our study population comprised all singleton live births that occurred among birth parents living in California during the study period, and included fetal deaths for the years in which those data were available. However, these data exclude any spontaneous and induced abortions, resulting in left-truncation of the cohort. Risk of spontaneous abortion that is differential by exposure can induce selection bias into the analysis, although the bias is expected to be toward the null for harmful exposures.56
We did not examine differences in associations by whether the victim of fatal police violence was armed or unarmed during the confrontation with police. While this distinction may be relevant for studies of police use of force, it not relevant per se for those living in communities in which people are killed by the police. We expect living in a neighborhood in which a violent death occurs at the hands of police—whether or not that death was considered “justifiable” by the authorities—is still likely to be traumatic from the perspective of people who knew the victim or lived nearby. Further, narratives that distinguish between armed and unarmed status have been linked to racialized stereotypes of Black criminality, thus precipitating the use of this language by the media almost exclusively to describe Black men.57 Finally, from a measurement perspective, we note that distinctions between “armed” and “unarmed” status may be inherently flawed given the notable range in what constitutes armed status.58
This study examined exposure to acute incidents of fatal police violence during pregnancy, and thus our analysis was restricted to areas in which there was at least one incident of fatal police violence during the study period. The focus on acute exposure helped address issues of structural confounding but did not incorporate what we know about the roles of residential segregation and neighborhood stratification in shaping both exposure to fatal police violence and adverse parental and infant health outcomes.59,60 Furthermore, previous evidence suggests that living in a neighborhood with chronically high police surveillance and aggressive policing is linked to worse health.14 Therefore, our focus on acute incidents likely captures only a small portion of the relationship between police and community interactions and parental and infant health. Future research should find innovative ways to study long-term exposure to police violence, as it may be more relevant for understanding inequities in reproductive health. Future research could also investigate how additional characteristics of the decedent, like age, may affect the relationship with birth outcomes, assess whether nonfatal police violence is associated with adverse birth outcomes, or evaluate the mechanisms underlying the differences between the two forms of exposure we consider here.
Interpretation
The larger magnitudes of association for Black birth parents with female infants may point to unmeasured male fetal loss in this population as a result of exposure to fatal police violence. The male-to-female live birth ratio (i.e., the sex ratio) has been used to assess fetal loss because male fetuses are more vulnerable to in-utero stressors. For example, evidence shows the sex ratio decreased after the September 11, 2001 terrorist attacks52 and after the collapse of the East German economy.53 Furthermore, analysis of the sex ratio among California births from 1960–1996 has shown that Black birth parents had consistently lower sex ratios compared to white birth parents,54 suggesting that Black people may experience higher male fetal loss compared to white people. Given our findings of stronger associations of fatal police violence with preterm birth among Black birth parents with female infants together with this prior evidence of elevated male fetal loss following stressful community events, it is possible that Black birth parents carrying male fetuses who were exposed to fatal police violence during early pregnancy may have experienced elevated fetal loss. This question should be explored in future research.
To our knowledge, no previous study has examined the association between exposure to police violence in the community during pregnancy and preterm birth. However, while not focusing specifically on fatal police violence, several prior studies have looked at homicide exposure within communities and risk of preterm birth. A previous study in California did not find a relationship between exposure to homicide in a census tract during early pregnancy and risk of preterm birth,20 though living in a neighborhood with high firearm violence in California was associated with increased risk of spontaneous preterm birth24 and a study of mothers in Brazil found an increased risk of preterm birth associated with increased homicide rates.22 These studies did not stratify by infant sex, which may have masked important heterogeneity, as our findings suggest stronger effects on female infants.
Conclusions
Our results suggest that exposure to fatal police violence during pregnancy is associated with a small increased hazard of late preterm delivery among all births, and larger increased hazard of moderate preterm delivery among births to Black people. Therefore, despite the small magnitude of associations, mitigating this violence could improve birth outcomes and reduce inequities in adverse birth outcomes by race or ethnicity in California. In 2018, the American Public Health Association released a policy statement regarding law enforcement violence as a public health issue with suggested steps for reducing incidents of fatal police violence.1 These include improving methods of data collection by implementing mandatory reporting to local public health departments, and shifting government priorities and resources away from criminalizing the symptoms of social inequity to investing in primary prevention (e.g., education, economic opportunity, housing). In the near term, other community and/or clinical interventions could serve as harm reduction mechanisms, mitigating the potential impacts of exposure to fatal police violence and other forms of stress on pregnant people.61–63
Supplementary Material
Synopsis.
Study Question:
Does exposure to fatal police violence in a person’s Census tract during pregnancy increase the hazard of preterm delivery, and do associations differ by race/ethnicity and fetal sex?
What’s already known:
No prior studies that we are aware of have examined this question, although exposure to other forms of violence in a woman’s community during pregnancy has been associated with adverse birth outcomes.
What this study adds:
This study provides evidence that fatal police violence affects the health of pregnant people living in communities where it occurs, and that it may play a role in inequities in preterm birth by race/ethnicity.
Sources of Funding:
This study was supported by NIH grant DP2HD080350, the UC Firearm Violence Research Center, the UC Berkeley Committee on Research, and the Cheri Pies Dissertation Award.
Footnotes
The authors declare no conflicts of interest.
References
- 1.American Public Health Association. Addressing Law Enforcement Violence as a Public Health Issue. 2018.
- 2.Jee-Lyn García J, Sharif MZ. Black Lives Matter: A Commentary on Racism and Public Health. American Journal of Public Health 2015;105:e27–e30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Alang S, McAlpine D, McCreedy E, Hardeman R. Police Brutality and Black Health: Setting the Agenda for Public Health Scholars. American Journal of Public Health 2017;107:662–665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cooper HLF, Fullilove M. Editorial: Excessive Police Violence as a Public Health Issue. Journal of Urban Health : Bulletin of the New York Academy of Medicine 2016;93:1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Terrill W, Reisig MD. Neighborhood Context and Police Use of Force. Journal of Research in Crime and Delinquency 2003;40:291–321. [Google Scholar]
- 6.Gelman A, Fagan J, Kiss A. An Analysis of the New York City Police Department’s “Stop-and-Frisk” Policy in the Context of Claims of Racial Bias. Journal of the American Statistical Association 2007;102:813–823. [Google Scholar]
- 7.Lautenschlager R, Omori M. Racial Threat, Social (Dis)organization, and the Ecology of Police: Towards a Macro-level Understanding of Police Use-of-force in Communities of Color. Justice Quarterly 2019;36:1050–1071. [Google Scholar]
- 8.Mooney AC, McConville S, Rappaport AJ, Hsia RY. Association of Legal Intervention Injuries With Race and Ethnicity Among Patients Treated in Emergency Departments in California. JAMA Network Open 2018;1:e182150–e182150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Buehler JW. Racial/Ethnic Disparities in the Use of Lethal Force by US Police, 2010–2014. American Journal of Public Health 2016;107:295–297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Feldman JM, Gruskin S, Coull BA, Krieger N. Police-Related Deaths and Neighborhood Economic and Racial/Ethnic Polarization, United States, 2015–2016. American Journal of Public Health 2019;109:458–464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Williams DR, Collins C. Racial Residential Segregation: A Fundamental Cause of Racial Disparities in Health. Public Health Reports 2001;116:404–416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bailey ZD, Krieger N, Agénor M, Graves J, Linos N, Bassett MT. Structural racism and health inequities in the USA: evidence and interventions. The Lancet 2017;389:1453–1463. [DOI] [PubMed] [Google Scholar]
- 13.Edwards F, Esposito MH, Lee H. Risk of Police-Involved Death by Race/Ethnicity and Place, United States, 2012–2018. American Journal of Public Health 2018;108:1241–1248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sewell AA. The Illness Associations of Police Violence: Differential Relationships by Ethnoracial Composition. Sociological Forum 2017;32:975–997. [Google Scholar]
- 15.Bor J, Venkataramani AS, Williams DR, Tsai AC. Police killings and their spillover effects on the mental health of black Americans: a population-based, quasi-experimental study. The Lancet 2018;392:302–310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Boyd RW, Ellison AM, Horn IB. Police, Equity, and Child Health. Pediatrics 2016;137:e20152711. [DOI] [PubMed] [Google Scholar]
- 17.HOFFMAN MC, MAZZONI SE, WAGNER BD, LAUDENSLAGER ML, ROSS RG. Measures of Maternal Stress and Mood in Relation to Preterm Birth. Obstetrics and gynecology 2016;127:545–552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kramer MR, Hogue CJ, Dunlop AL, Menon R. Preconceptional stress and racial disparities in preterm birth: an overview. Acta Obstetricia et Gynecologica Scandinavica 2011;90:1307–1316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kramer MS, Lydon J, Séguin L, Goulet L, Kahn SR, McNamara H, et al. Stress Pathways to Spontaneous Preterm Birth: The Role of Stressors, Psychological Distress, and Stress Hormones. American Journal of Epidemiology 2009;169:1319–1326. [DOI] [PubMed] [Google Scholar]
- 20.Goin DE, M. Gomez A, Farkas K, Zimmerman SC, Matthay EC, Ahern J Exposure to Community Homicide During Pregnancy and Adverse Birth Outcomes: A Within-Community Matched Design. Epidemiology 2019;30:713–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Torche F, Villarreal A. Prenatal Exposure to Violence and Birth Weight in Mexico: Selectivity, Exposure, and Behavioral Responses. American Sociological Review 2014;79:966–992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Foureaux Koppensteiner M, Manacorda M. Violence and birth outcomes: Evidence from homicides in Brazil. Journal of Development Economics 2016;119:16–33. [Google Scholar]
- 23.Mayne SL, Pool LR, Grobman WA, Kershaw KN. Associations of neighbourhood crime with adverse pregnancy outcomes among women in Chicago: analysis of electronic health records from 2009 to 2013. J Epidemiol Community Health 2018;72:230–236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Goin DE, Rudolph KE, Gomez AM, Ahern J. Mediation of Firearm Violence and Preterm Birth by Pregnancy Complications and Health Behaviors: Addressing Structural and Postexposure Confounding. American Journal of Epidemiology 2020;189:820–831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Goldmann E, Aiello A, Uddin M, Delva J, Koenen K, Gant LM, et al. Pervasive exposure to violence and posttraumatic stress disorder in a predominantly African American Urban Community: The Detroit neighborhood health study. Journal of Traumatic Stress 2011;24:747–751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Cecil CAM, Viding E, Barker ED, Guiney J, McCrory EJ. Double disadvantage: the influence of childhood maltreatment and community violence exposure on adolescent mental health. Journal of Child Psychology and Psychiatry 2014;55:839–848. [DOI] [PubMed] [Google Scholar]
- 27.Brown JR, Hill HM, Lambert SF. Traumatic stress symptoms in women exposed to community and partner violence. Journal of Interpersonal Violence 2005;20:1478–1494. [DOI] [PubMed] [Google Scholar]
- 28.Graignic-Philippe R, Dayan J, Chokron S, Jacquet A-Y, Tordjman S. Effects of prenatal stress on fetal and child development: A critical literature review. Neuroscience & Biobehavioral Reviews 2014;43:137–162. [DOI] [PubMed] [Google Scholar]
- 29.Seng JS, Oakley DJ, Sampselle CM, Killion C, Graham-Bermann S, Liberzon I. Posttraumatic stress disorder and pregnancy complications. Obstetrics & Gynecology 2001;97:17–22. [DOI] [PubMed] [Google Scholar]
- 30.Dunkel Schetter C, Tanner L. Anxiety, depression and stress in pregnancy: implications for mothers, children, research, and practice. Current opinion in psychiatry 2012;25:141–148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Weinstock M The potential influence of maternal stress hormones on development and mental health of the offspring. Brain, Behavior, and Immunity 2005;19:296–308. [DOI] [PubMed] [Google Scholar]
- 32.Ratnasiri AWG, Parry SS, Arief VN, DeLacy IH, Lakshminrusimha S, Halliday LA, et al. Temporal trends, patterns, and predictors of preterm birth in California from 2007 to 2016, based on the obstetric estimate of gestational age. Maternal Health, Neonatology and Perinatology 2018;4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Culhane JF, Goldenberg RL. Racial Disparities in Preterm Birth. Seminars in Perinatology 2011;35:234–239. [DOI] [PubMed] [Google Scholar]
- 34.Mendez DD, Hogan VK, Culhane JF. Institutional racism, neighborhood factors, stress, and preterm birth. Ethnicity & Health 2014;19:479–499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Chambers BD, Erausquin JT, Tanner AE, Nichols TR, Brown-Jeffy S. Testing the Association Between Traditional and Novel Indicators of County-Level Structural Racism and Birth Outcomes among Black and White Women. Journal of Racial and Ethnic Health Disparities 2018;5:966–977. [DOI] [PubMed] [Google Scholar]
- 36.McSpadden L Mother’s fear for her black son. Courier Journal https://www.courier-journal.com/story/opinion/contributors/2014/08/11/mothers-fear-black-son/13905957/. Published August 11, 2014. Last accessed March 1, 2020.
- 37.Boyd-Franklin N Black Families in Therapy: Understanding the African American Experience. Guilford Press; 2006. [Google Scholar]
- 38.Dottolo AL, Stewart AJ. “Don’t Ever Forget Now, You’re a Black Man in America”: Intersections of Race, Class and Gender In Encounters with the Police. Sex Roles 2008;59:350–364. [Google Scholar]
- 39.Padgett DA, Glaser R. How stress influences the immune response. Trends in Immunology 2003;24:444–448. [DOI] [PubMed] [Google Scholar]
- 40.Suglia SF, Staudenmayer J, Cohen S, Enlow MB, Rich-Edwards JW, Wright RJ. Cumulative Stress and Cortisol Disruption among Black and Hispanic Pregnant Women in an Urban Cohort. Psychological Trauma: Theory, Research, Practice and Policy 2010;2:326–334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Black MC, Basile KC, Breiding MJ, Smith SG, Walters ML, Merrick MT, et al. The national intimate partner and sexual violence survey: 2010 summary report. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention; 2011;19:39–40. [Google Scholar]
- 42.Wainstock T, Shoham-Vardi I, Glasser S, Anteby E, Lerner-Geva L. Fetal sex modifies effects of prenatal stress exposure and adverse birth outcomes. Stress 2015;18:49–56. [DOI] [PubMed] [Google Scholar]
- 43.Clifton VL. Review: Sex and the human placenta: mediating differential strategies of fetal growth and survival. Placenta 2010;31 Suppl:S33–39. [DOI] [PubMed] [Google Scholar]
- 44.Premkumar A, Nseyo O, Jackson AV. Connecting Police Violence With Reproductive Health. Obstetrics & Gynecology 2017;129:153. [DOI] [PubMed] [Google Scholar]
- 45.Messer LC, Oakes JM, Mason S. Effects of Socioeconomic and Racial Residential Segregation on Preterm Birth: A Cautionary Tale of Structural Confounding. American Journal of Epidemiology 2010;171:664–673. [DOI] [PubMed] [Google Scholar]
- 46.Barnett AG. Time-Dependent Exposures and the Fixed-Cohort Bias. Environmental Health Perspectives 2011;119:a422–a423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Barber C, Azrael D, Cohen A, Miller M, Thymes D, Wang DE, et al. Homicides by Police: Comparing Counts From the National Violent Death Reporting System, Vital Statistics, and Supplementary Homicide Reports. American Journal of Public Health 2016;106:922–927. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Feldman JM, Gruskin S, Coull BA, Krieger N. Quantifying underreporting of law-enforcement-related deaths in United States vital statistics and news-media-based data sources: A capture–recapture analysis. PLOS Medicine 2017;14:e1002399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Platt RW, Hutcheon JA, Suissa S. Immortal Time Bias in Epidemiology. Current Epidemiology Reports 2019;6:23–27. [Google Scholar]
- 50.Therneau TM, Grambsch PM. Modeling Survival Data: Extending the Cox Model. New York: Springer-Verlag; 2000. [Google Scholar]
- 51.Li R, Chambless L. Test for Additive Interaction in Proportional Hazards Models. Annals of Epidemiology 2007;17:227–236. [DOI] [PubMed] [Google Scholar]
- 52.Catalano R, Bruckner T, Marks AR, Eskenazi B. Exogenous shocks to the human sex ratio: the case of September 11, 2001 in New York City. Human Reproduction 2006;21:3127–3131. [DOI] [PubMed] [Google Scholar]
- 53.Catalano RA. Sex ratios in the two Germanies: a test of the economic stress hypothesis. Human Reproduction 2003;18:1972–1975. [DOI] [PubMed] [Google Scholar]
- 54.Smith D, Behren JV. Trends in the sex ratio of California births, 1960–1996. Journal of Epidemiology & Community Health 2005;59:1047–1053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Barradas DT, Dietz PM, Pearl M, England LJ, Callaghan WM, Kharrazi M. Validation of Obstetric Estimate Using Early Ultrasound: 2007 California Birth Certificates. Paediatric and Perinatal Epidemiology 28:3–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Goin DE, Casey JA, Kioumourtzoglou M-A, Cushing LJ, Morello-Frosch R Environmental hazards, social inequality, and fetal loss: Implications of live-birth bias for estimation of disparities in birth outcomes. Environmental Epidemiology 2021;In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Dukes KN, Gaither SE. Black Racial Stereotypes and Victim Blaming: Implications for Media Coverage and Criminal Proceedings in Cases of Police Violence against Racial and Ethnic Minorities. Journal of Social Issues 2017;73:789–807. [Google Scholar]
- 58.Nix J, Campbell BA, Byers EH, Alpert GP. A Bird’s Eye View of Civilians Killed by Police in 2015. Criminology & Public Policy 2017;16:309–340. [Google Scholar]
- 59.Chambers BD, Baer RJ, McLemore MR, Jelliffe-Pawlowski LL. Using Index of Concentration at the Extremes as Indicators of Structural Racism to Evaluate the Association with Preterm Birth and Infant Mortality—California, 2011–2012. Journal of Urban Health 2019;96:159–170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Mehra R, Boyd LM, Ickovics JR. Racial residential segregation and adverse birth outcomes: A systematic review and meta-analysis. Social Science & Medicine 2017;191:237–250. [DOI] [PubMed] [Google Scholar]
- 61.Picklesimer AH, Billings D, Hale N, Blackhurst D, Covington-Kolb S. The effect of CenteringPregnancy group prenatal care on preterm birth in a low-income population. American Journal of Obstetrics and Gynecology 2012;206:415.e1–415.e7. [DOI] [PubMed] [Google Scholar]
- 62.Mazzoni SE, Carter EB. Group prenatal care. American Journal of Obstetrics and Gynecology 2017;216:552–556. [DOI] [PubMed] [Google Scholar]
- 63.Kozhimannil KB, Hardeman RR, Attanasio LB, Blauer-Peterson C, O’Brien M. Doula Care, Birth Outcomes, and Costs Among Medicaid Beneficiaries. American Journal of Public Health 2013;103:e113–e121. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.