

Summary
This paper reports how we applied systems dynamics methods to gain insight into the complexity of obesity‐related behaviors in youth, including diet, physical activity, sedentary behavior, and sleep, by integrating a literature review into causal loop diagrams (CLDs). Results showed that the CLDs consisted of multiple subsystems and three types of dynamics appeared, including (1) feedback loops, (2) connections between feedback loops and subsystems, and (3) mechanisms. We observed clear similarities in the dynamics for the four behaviors in that they relate to “traditional” subsystems, such as home and school environments, as well as to newly added subsystems, including macroeconomics, social welfare, and urban systems. The CLDs provided insights that can support the development of intervention strategies, including (1) the confirmation that a range of mechanisms cover and connect multiple levels and settings, meaning that there is no silver bullet to address obesity; (2) understanding of how interventions in one particular setting, such as school, might be influenced by the interactions with other settings, such as urban systems; and (3) a comprehensive view of (un)intended consequences. This way of framing the problem will assist moving towards public health interventions that respond to and operate in the complexity of the real world.
Keywords: adolescents, causal loop diagrams, obesity, systems dynamics
1. INTRODUCTION
Despite continuous and growing efforts to reduce the burden of childhood overweight and obesity, we see disappointing results, where not a single country has successfully halted the obesity epidemic in the general population to date. 1 , 2 One explanation for this lack of progress is that most existing approaches, although multicomponent, focus on causes of obesity directly related to unhealthy behaviors, such as (lack of) health knowledge, attitudes towards health behavior, or unhealthy school environments. 3 Most programs do not take into account the complexity of the problem, including underlying mechanisms (causes of the causes) that drive these unhealthy behaviors such as stress, peer pressure, or the political environment nor do they take into account dynamic properties, including feedback and adaptation in response to changes (i.e., interventions) in the system. 4
A recent overview of reviews covering 13 systematic reviews of interventions aimed at preventing overweight and obesity in adolescents concludes that the evidence base for the effectiveness of current interventions is weak, in particular because the vast majority of included interventions target the individual and are set in schools with a lack of structural and environmental interventions applied in the wider society. 5 For example, a cluster randomized controlled trial evaluating a school‐based obesity prevention intervention showed no significant intervention effects, despite a theoretically informed and extensively piloted intervention that achieved high levels of engagement, follow‐up, and fidelity of delivery. The authors conclude that school‐based interventions alone might not be sufficiently powerful to affect all relevant environments of an adolescent's life and that therefore future programs should address the full complexity of the problem by using whole‐of‐systems approaches. 6
The lack of a detectable and/or sustainable impact of many public health interventions aligns with the conceptualization of overweight and obesity as a complex problem: the drivers are multiple, diverse, and dynamic, ranging from biological factors and personal behaviors to aspects of the physical, economic, sociocultural, and political environments that shape those drivers. Systems thinking is acknowledged as a promising approach to understanding and responding to the complexity of the obesity epidemic. 7 , 8 , 9 Although there is a growing body of literature on applying systems thinking in public health research, 10 there is still relatively little guidance on how to create an understanding of systems dynamics and design and evaluate public health interventions in complex systems. 11 , 12 , 13 It is therefore important to expand the evidence base on how systems methodologies can be applied and on what the practical value of systems thinking can be in public health research. 14 Within systems approaches, systems dynamics has shown itself particularly useful in understanding the complexity of public health problems. 1 , 15 , 16 One specific tool within systems dynamics is the use of causal loop diagrams (CLDs) to explore the multiple, interacting feedback loops operating in a system of interest. 14 , 17 CLDs provide a visual image of an issue and are appropriate for use in explorative studies, because they are easier to build and understand and have fewer data and resource requirements than quantitative simulation models. 18
The aim of this study is to apply systems dynamics methods to gain insights into the complexity of obesity‐related behaviors. We report on how we applied systems dynamics methods and on the extent to which this led to new understandings of the problem and its underlying dynamics.
2. METHODS
2.1. LIKE project
The results presented in this paper are part of a larger program entitled Lifestyle Innovations Based on Youth Knowledge and Experience (LIKE). LIKE combines systems dynamics and participatory action research to develop, implement, and evaluate a dynamic action program focused on promoting healthy lifestyle habits in young adolescents in the transition from tween to teen (aged 10 to 14). LIKE is embedded in the Amsterdam Healthy Weight Programme (AHWP) and is situated in three lower socioeconomic neighborhoods in Amsterdam (Netherlands). 19
The first part of the LIKE program seeks an understanding of preexisting systems that shape unhealthy lifestyle behaviors by conducting an in‐depth needs assessment. Here, we aim to gain insight into the system from two different perspectives: the stakeholders' perspective that provides an inside view of the system and the researchers' perspective that provides a more outside view of the system, by building on existing evidence and interpreting the inside perspective. The different methods employed to gain insight into these perspectives are explained elsewhere. 19 The current paper presents the results already achieved in terms of understanding the system from the outside perspective through the use of CLDs developed by academic experts within the LIKE program.
2.2. Literature review from a complexity perspective
The general aim of this study was to gain insight into the complexity of obesity‐related behaviors. Petticrew et al. describe methodological implications of such a complexity perspective for the conduct of systematic reviews, 20 which we applied in our study design. For this purpose, we combined conventional approaches to systematic database searching to retrieve all relevant determinants with guidance around developing systems‐based reviews to gain insight into system dynamic properties. In particular, our systems approach meant formulating an explanatory research question around deepening an understanding of relevant system dynamics (i.e., the mechanistic relationship between determinants through interaction and feedback), adopting a pluralist approach to study selection by study design and evidence type, and creating data extraction and presentation processes (i.e., CLDs) that allowed us to elucidate system properties. The exact procedures are detailed below.
2.3. Procedures
We set up a six‐step approach for developing the CLDs. The central aim was to identify factors that could explain the increase in childhood obesity rates in the Netherlands in the past two decades. We further operationalized the research aim by focusing on four types of behaviors that are particularly relevant to childhood obesity and are the focus of the AHWP including dietary behavior, physical activity (PA), sedentary behavior, and sleep, although the evidence on the direct link between the latter two behaviors and obesity is less consistent. 21 , 22 Hence, the primary question for a CLD was: “What factors explain the dynamics in dietary behaviors, physical activity, sedentary behavior, and sleep, in the Netherlands in the past two decades?” We followed the six steps described below for each of the four behavior types; however, it should be noted that—by nature of principles of complexity—this was not always a linear process but rather iterative, in particular in Step 3 (see details below).
-
Step 1:
Establishing CLD working groups
We established four working groups to lead the CLD development, one group for each behavior. Each group consisted of at least three academic researchers with expertise on that specific behavior. Representatives from each working groups met regularly to monitor progress and to coordinate the methods across groups. Where needed, working groups reached out for additional support from academic colleagues during various phases of the CLD building process, including the literature selection as specified in the next step.
-
Step 2:
Extracting determinants from the literature
Prior to the first meeting, two to three members of each working group conducted a pragmatic literature search using conventional methods of database searching (in PubMed) with a focus on systematic reviews supplemented with empirical studies (both qualitative and quantitative) on determinants of the specified behaviors. In addition, academic colleagues were asked to share systematic reviews they considered most relevant. The aim of this literature search was not to identify all possible determinants but rather to confirm the most important ones (see also Step 3). From this literature selection, one or two members of the group extracted all named determinants and grouped these into six broad categories to facilitate checking for completeness: behavioral, psychological, sociocultural, socioeconomic, policy, and physical environment. At the first meeting, each group reviewed the identified determinants and critically discussed the relevance for our target group (early adolescents) and our setting (urban setting in Amsterdam). For example, determinants relating to food deserts or lack of public transport were excluded, because those were not relevant to our setting as Amsterdam has a very dense availability of supermarkets with no profound inequalities in access between neighborhoods 23 as well as a high‐quality public transport system (trams, metro, and busses). This resulted in a longlist of determinants for each behavior (see Appendix A).
-
Step 3:
From variables to connections
Once we had all longlists of variables, we had a joint meeting with all working groups to start drawing connections between the variables (see Step 4 for details about drawing these connections). The initial maps that resulted from this exercise were reviewed by authors WW, AS, TA, CD, ALP, and KS and an external expert with long‐standing expertise in systems dynamics methods. During this review process, it became apparent that groups struggled to draw connections between variables based on system dynamic principles, including considering nonlinear relationships, accumulation, feedback loops, effects of time delay, and unintended consequences. 24 This struggle particularly related to the fact that most studies in our literature selection (Step 2) examined the association between a (sub‐)behavior and a single factor, with the association being unidirectional (from determinant to behavior). Therefore, when drawing connections, this resulted in all factors pointing at these sub‐behaviors, with minimal interconnections between factors (in systems dynamics terms known as a “dead buffalo”). To solve this result, we specified five requirements to aid in creating an understanding in relevant system dynamic properties rather than creating a mind map with many connections.
The first, and arguably the most important, requirement related to excluding the main sub‐behaviors from the CLDs, because undoubtedly, all factors would relate to that behavior, and instead, we tailored each CLD to the most relevant sub‐behavior for our target group and setting. This tailoring was not only needed to avoid all determinants pointing to these sub‐behaviors but also because the initial four behaviors were too broad and could be associated with too many determinants. For example, dietary behavior is relatively complex in itself, and the working group identified five sub‐behaviors, including consuming a healthy breakfast, healthy lunch, healthy dinner, unhealthy snacks, and sugar‐sweetened beverages (SSBs). From these sub‐behaviors, we selected the one that we considered of greatest relevance to obesity prevention in our target group, being “frequent unhealthy snacking (including fast food, snacks, and SSBs)” and focused the CLD on that specific sub‐behavior. A similar approach was taken for the other behaviors. They were framed as
dietary behavior: unhealthy snacking (as specified above);
PA: active transportation and outdoor active play (specified from four identified sub‐behaviors based on the contribution to energy expenditure, including active transport, PA at/around school, organized PA, and unorganized PA);
sedentary behavior: leisure time screen use (we considered this behavior more relevant for overweight prevention than, e.g., sitting while reading or using a screen for academic activities. We further specified four time frames: [1] during recess; [2] after school; [3] during the night; and [4] during weekend days); and
sleep: sleep duration, sleep quality, and sleep routine (we defined healthy sleep behavior as the combination of adequate sleep duration, good sleep quality, and regular sleep timing). This meant that we included “sleeping sufficiently” (sleep duration), “sleep onset latency” and “sleeping through the night (sleep quality),” and “having a regular sleep routine and timing” in the CLD.
Following the specification of the sub‐behaviors, we applied the following four requirements to identify factors from the longlists to be initially included in every CLD:
Dynamic properties: An important concept in systems dynamics is change over time, rather than a static situation, which is also reflected in our central question, that is, “What factors explain the dynamics in dietary behaviors, physical activity, sedentary behavior, and sleep, in the Netherlands in the past two decades?” Therefore, we focused on factors that had changed significantly over the last two decades.
Causal relationship: Causal thinking is a key construct in developing CLDs, which includes direct causation but also influence or affect (a influences b); however, it doesn't include association.
Importance or relevance: When building a CLD, it helps to focus on the most important determinants, rather than all possible determinants. While including all variables might be more precise, it doesn't aid in gaining insights into underlying dynamics because there is a risk of including many determinants that mean more or less the same (e.g., accessibility or visibility of unhealthy food) and therefore ending up with many (irrelevant) connections between those variables. Therefore, we initially set a rough guide of including the approximately 20 most relevant factors. This selection was done during a meeting within each working group, where there is little much discussion between group members about the inclusion or exclusion of determinants, partly because sometimes different determinants could be grouped together (e.g., recess exercise and extracurricular PA during weekend were joined into alternatives for sedentary behavior) and also because it was still possible to re‐add determinants in the final step (see (d) below) and/or in the following stages of the CLD building process (e.g., Step 4).
Check for completeness: Once all factors were selected, we verified whether additional factors were needed to complete the CLD in a joint meeting with (representatives from) each CLD working group. This resulted in a shortlist of factors for each behavior.
-
Step 4:
Drawing the connection circle
The shortlisted factors were included in a connection circle, using STICK‐E software (STICK‐E Version 2, © Deakin University). The connection circle was used to examine all possible connections between factors and their polarity. A positive polarity indicated positive causation (as a cause increases, the effect increases; as a cause decreases, the effect decreases). A negative polarity indicated inverse causation (as a cause increases, the effect decreases; as a cause decreases, the effect increases). At this stage, we also checked variable names because the exact formulation had to align with the properties of systems dynamics maps. For example, variables should be formulated neutral (e.g., knowledge) rather than in a specific direction (increased knowledge) because a “decrease in increased knowledge” is confusing. Also, variables should represent a factor that is quantifiable and can change over time, for example, “happiness” rather than “state of mind.” 25 We also specifically avoided drawing too many connections, which would have made the CLD unreadable, by removing duplicate connections running via direct and indirect pathways. For example, increased marketing of unhealthy food leads to increased availability of unhealthy food (i.e., more marketing = more sales = more availability), which leads to increased accessibility of unhealthy food. However, increased marketing might also show a direct link to accessibility (e.g., being able to order fast food by clicking on an advertisement in a social media feed). The latter connection was removed, because it is more likely that this association would be mediated via availability rather than existing via direct causation.
-
Step 5:
Developing the CLDs
Once all connections were identified, we moved the connection circle to the diagram view in STICK‐E, revealing the CLD (see Figure 1A–D). We again reviewed all connections to make sure they were correct. We also checked whether additional factors needed to be included in the CLDs, in particular because certain causations operate through mediating factors that could not be identified from the literature. For example, the factor “use of social media by youth” has an impact on “screen use in peers,” but there is likely an addictive effect of social media involved, a factor that was not identified via the literature search. The missing factor was then added to the CLD after discussion within the working group, including a check on the set requirements (i.e., dynamic properties, causal relationship, importance, or relevance) and where needed also checked again in the literature. Once the CLDs were completed, they were sent to academic experts linked to the LIKE project who were not directly involved in the CLD building process to critically review and comment on the completeness, missing links between factors and sub‐behaviors, missing links between determinants, correctness of links between factors and sub‐behaviors, and fit to the target group and setting, that is, 10–14‐year‐olds from a disadvantaged neighborhood in Amsterdam.
-
Step 6:
Interpreting the CLDs
FIGURE 1.
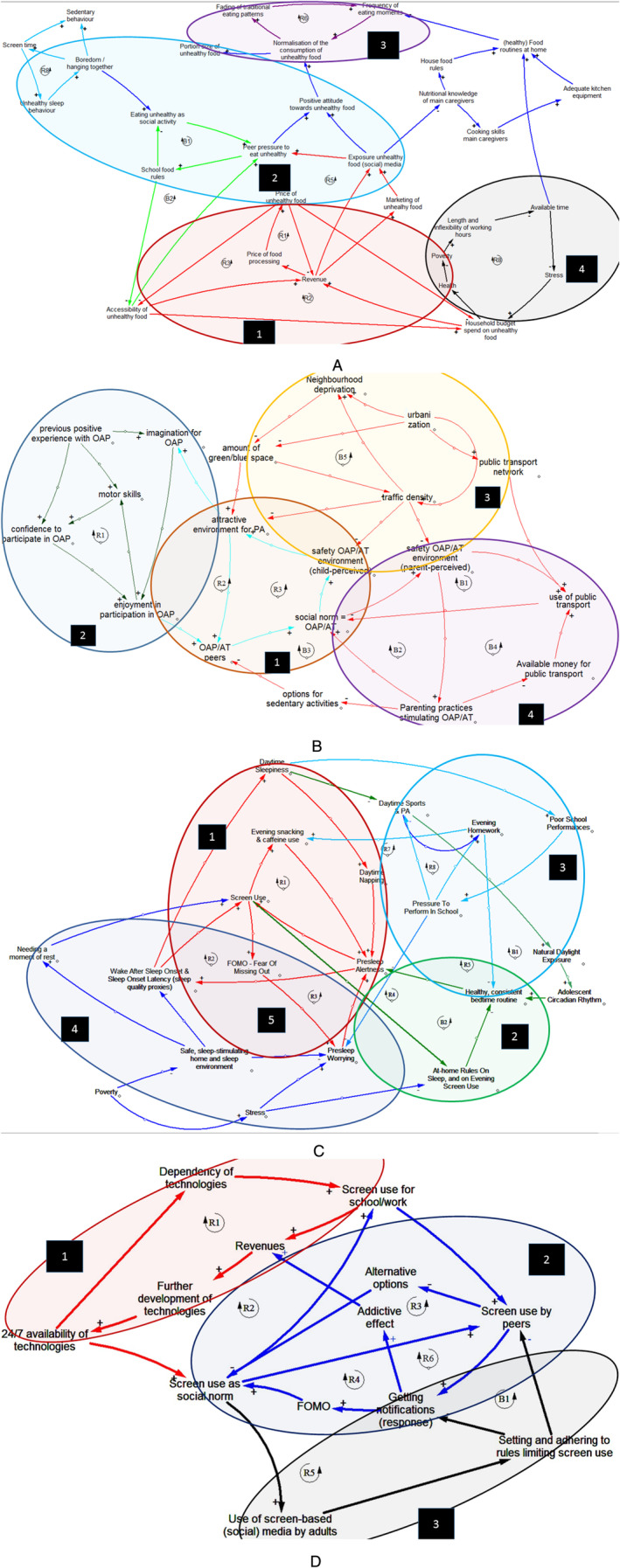
(A) Unhealthy snacking CLD. (B) Physical activity CLD. AT, active transport. OAP, outdoor active play; (C) Sleep CLD. PA, physical activity. (D) Screen use CLD. Alternative options, alternative options to screen use; FOMO, fear of missing out. CLD, causal loop diagram
At this stage, the CLDs read like a map of factors with connecting arrows rather than a systems dynamics map. The next step therefore involved interpreting the CLD, including an unraveling of the underlying systems dynamics. For that purpose, we exported the CLDs to Vensim (PLE 8.0.9) and used the feedback loops function to identify reinforcing and balancing feedback loops. The resulting loops were used to understand mechanisms, subsystems, and connections between subsystems.
3. RESULTS
The longlists of factors identified from the literature, the selected factors for each CLD, and the factors that were added during the CLD building process are displayed in Appendix A. The longlists and the final CLDs consisted of 55 and 28 factors for dietary behavior, 58 and 19 for screen use, 47 and 20 for PA, and 30 and 13 for sleep, respectively.
Figure 1A–D shows the final CLDs that were developed in the process, and Table 1 describes the observed dynamics within those CLDs. The numbered squares in the CLD indicate the subsystems involved (see Table 1 for labels). A first observation is that the resulting CLDs for each behavior consisted of multiple subsystems, whereby clear similarities emerged in subsystem types between the four CLDs. For all behaviors, we found subsystems relating to determinants that are typically included in empirical research, such as home environment, school environment, and social factors. However, we also found determinants relating to subsystems generally not included in empirical research, including macroeconomics, social welfare, technology, and urban systems. A second observation is that three types of dynamics appeared within and between these subsystems, including (1) feedback loops (i.e., a chain of connected variables that continue to re‐affect themselves, which can be reinforcing or balancing) and (2) connections between feedback loops and between subsystems (i.e., through variables that are included in multiple feedback loops). These could subsequently be used to describe (3) mechanisms in the system (i.e., using subsystems and feedback loops to organize ideas in the system).
TABLE 1.
Dynamics within the CLDs: Subsystems, mechanisms, and feedback loops
| CLD | Subsystems | Feedback loops | Mechanisms |
|---|---|---|---|
| Diet | 1. Food prices | R1/R2: Price of unhealthy food – household budget spent on unhealthy food – revenue – price of food processing – price of unhealthy food | Higher availability of unhealthy snacks decreases the price of unhealthy snacks, which increases accessibility of unhealthy snacks. This leads to more revenue, which leads to more marketing, and then to a higher availability. A lower price of unhealthy snacks increases the amount of the household budget spent on unhealthy snacks and drinks. |
| R3/R4: Price of unhealthy food – accessibility of unhealthy food – household budget spent on unhealthy food – revenue – price of food processing – price of unhealthy food | |||
| 2. Peer pressure | R5: Exposure to unhealthy food marketing (on social media) – peer pressure to eat unhealthy – accessibility of unhealthy food – revenue – exposure to unhealthy food marketing (on social media) | Accessibility to unhealthy snacks and exposure to unhealthy snack marketing lead to peer pressure to eat unhealthy snacks, which lead to a positive attitude and normalization of unhealthy snacks. School food rules can balance the accessibility of unhealthy snacks and in turn also limit peer pressure. | |
| R7: Boredom/hanging together – screen time – unhealthy sleep behavior – boredom/hanging together | Boredom and hanging out together increases sedentary behavior and increases screen time. Increased screen time leads to an increase in unhealthy sleep behavior, which will lead to more boredom/hanging together because the adolescents are tired. Hanging together also leads to an increase in eating unhealthy snacks as a social activity (LINK to screen use/sleep). | ||
| B1: School food rules – eating as a social activity – peer pressure to eat unhealthy – school food rules | |||
| B2: School food rules – accessibility of unhealthy food – peer pressure to eat unhealthy – school food rules | |||
| 3. Traditional eating patterns | R6: Normalization of the consumption of unhealthy food – fading of traditional eating patterns – frequency of eating moments | Normalization of unhealthy snacking leads to the fading of traditional eating patterns and to an increase of eating moments during a day; this again will lead to a normalization of unhealthy eating and so forth. | |
| 4. Poverty | R8: Length work hours – available time – stress – household food budget spent on unhealthy food – health – poverty – length work hours | Length and inflexibility of work hours leads to stress and less available time, which leads to increased household budget spent on unhealthy snacks, which leads to less health and more poverty (i.e., less income) and again leads to more length and inflexibility of work hours and so forth. | |
| Physical activity | 1. Physical capabilities | R1: Motor skills – confidence to participate in outdoor active play – enjoyment in participating in outdoor active play – motor skills | More outdoor active play leads to better motor skills and fitness, which makes youth more confident and increases the enjoyment in outdoor active play. This in turn increases chances of children to participate in outdoor active play, partly through better developed imagination (youth learn to know more games they can play). |
| 2. Social norm | R2: Attractive environment for PA – imagination for outdoor active play – enjoyment in participating in outdoor active play – outdoor active play/active transport peers – social norm – safety outdoor active play/active transport environment (child perceived) – attractive environment for PA | Having more PA equipment and materials available—which can be stimulated by local government policies and parents—leads to an attractive PA environment and through that more active transport/outdoor active play. Parents will stimulate youths' outdoor active play/active transport, when they perceive the environment as safe and attractive and if it is regarded as “normal” (social norm). | |
| R3: Attractive environment for PA – outdoor active play/active transport peers – social norm – safety outdoor active play/active transport environment (child perceived) – attractive environment for PA | If there are more options to spend time sedentary, the social norm related to outdoor active play/active transport changes, resulting in less children playing and being outside. For parents, it has also become easier to let children participate in sedentary activities (LINK to screen use). | ||
| B3: Options for sedentary activities – outdoor active play/active transport peers – social norm – safety outdoor active play/active transport environment (parent perceived) – parenting practices stimulating outdoor active play/active transport – options for sedentary activities | |||
| 3. Public transport | B1/B2: Safety outdoor active play/active transport environment (parent perceived) – parenting practices stimulating outdoor active play/active transport – social norm – safety outdoor active play/active transport environment (parent perceived) | A perceived (more) unsafe environment leads to more parents choosing for their kids to use public transport rather than cycling/walking. This changes the social norm regarding cycling/walking and again influences perceived safety of the environment. This is also influenced by the availability of money for public transport in youth. | |
| B4: Available money for public transport – use of public transport – social norm outdoor active play/active transport – safety outdoor active play/active transport environment (parent perceived) – parenting practices stimulating outdoor active play/active transport – available money for public transport | |||
| 4. Urbanization | B5: Traffic density – neighborhood deprivation – amount of green/blue space – traffic density | More urbanization leads to increased traffic density, which results in children and parents experiencing the environment as less safe. An attractive PA environment (e.g., amount of blue/green space, safe environment, and attractive opportunities to play outside) can positively influence outdoor active play and inhibit youths' use of alternative sedentary options. | |
| Sleep | 1. Screen use | R1: Screen use – evening snacking and caffeine use – presleep alertness – screen use | Screen use in the evening creates more presleep arousal and mental alertness due to interaction with others via (social) media. This in turn leads to more worrying, for example, via fear of missing out and wanting to fit in, which leads to later bed times and staying up late when finally lying in bed. In bed, the screen (mobile, tablet) often tags along, where it keeps providing cues to check and keep using the screen until late hours. |
| R2: Screen use – evening snacking and caffeine use – presleep alertness – wake up after sleep onset – screen use | Caffeine use creates more presleep arousal and mental alertness, which causes youth to go to bed later as well as impairs their quality of sleep. In turn, this leads to more daytime sleepiness, again more caffeine use, and daytime napping. This mechanism is strengthened by the dominant peer norms that it is cool to drink caffeinated energy drinks and go to bed very late. | ||
| R3: Screen use – FOMO – presleep worrying – presleep alertness – screen use | |||
| 2. Rules at home | B2: At‐home rules on sleep and evening screen use – healthy bedtime routine – presleep alertness – screen use – at‐home rules on sleep and evening screen use | Clear rules at home can help reduce evening screen use, which leads to a healthier bedtime routine and less presleep alertness, and these positive effects can help reinforce clear rules at home. | |
| 3. Academic pressure | R4: Pressure to perform in school – presleep worries – presleep alertness – wake up after sleep onset – daytime sleepiness – poor school performances – pressure to perform in school | During adolescence, youth (because of their brain development) generally have difficulties to efficiently plan their homework and get it done during the day/not too late. However, the pressure to perform at school leads to more evening homework activities, presleep worries, mental alertness, and, as a consequence, later bedtimes and staying up late. This creates more tiredness during the day, which hampers their school performances, adding to the problem and strengthening this vicious circle. | |
| R5: Pressure to perform in school – evening homework – healthy consistent bedtime routine – presleep alertness – wake up after sleep onset – daytime sleepiness – poor school performances – pressure to perform in school | |||
| R6: Pressure to perform in school – evening homework – evening snacking and caffeine use – presleep alertness – wake up after sleep onset – daytime sleepiness – poor school performances – pressure to perform in school | |||
| R7: Pressure to perform in school – daytime PA – natural daylight exposure – circadian rhythm – healthy bedtime routine – presleep alertness – wake up after sleep onset – daytime sleepiness – poor school performances – pressure to perform in school | |||
| B1: Daytime PA – natural daylight exposure – circadian rhythm – healthy bedtime routine – presleep alertness – wake up after sleep onset – daytime sleepiness – daytime PA | |||
| 4. Sleep environment | No feedback loops identified | Poverty‐related issues cause adolescents to worry more, yet also affect their sleep because of co‐sleeping and due to their home environment more often being crowded, noisy, and unsafe compared with peers with a higher socioeconomic position. | |
| 5. Reinforcing sleep factors | Presleep worrying – presleep alertness – wake up after sleep – screen use | Different factors relating to sleep quality reinforce each other in a vicious circle, which in turn is often reinforced by screen use. For example, screen use leads to more presleep worrying and presleep alertness and also to more waking up after falling asleep, which again triggers screen use (checking phone after waking up). | |
| Screen use | 1. Revenue | R1: 24/7 availability of technologies – dependency on technologies – screen use for school/work – revenue – further development of technologies – 24/7 availability of technologies | The 24/7 availability of technologies—for example, smartphones, apps, and Wi‐Fi—has resulted in an increase in dependency of technologies of both adolescents and adults, for communication but also practical reasons (e.g., alarm clock). The frequent use of these technologies generates income (revenue) for the developers of the technologies (of smartphones, apps, etc.), which subsequently provides the opportunity for technology developers to develop more/improved technologies that further increase the dependency of technologies. |
| R2: 24/7 availability of technologies – dependency on technologies – screen use for school/work – screen use peers – getting notifications – addictive effect – revenues | |||
| 2. Social norm | R3: Screen use as social norm – screen use peers – alternative options – screen use as social norm | The 24/7 availability of technologies has resulted in an increased use of social media, (online) games, and passive media (e.g., Netflix) by youth. The use of these media/games has an addictive/attractive effect on itself, thereby further increasing the screen use of youth. Additionally, the addictive/attractive effect results in youth being anxious to miss out on something (i.e., fear of missing out): They want to know the latest news/posts on social media of friends or significant others, and they want to finish all levels of a certain game and have seen the series/movies that their friends (or significant others) talk about. This fear of missing out further increases screen use. | |
| R4: Screen use as social norm – screen use peers – getting notifications – fear of missing out – screen use as social norm | |||
| R5: Screen use as social norm – screen use by adults – setting and adhering to rules around screen time – getting notifications (response) – fear of missing out – screen use as social norm | |||
| R6: Screen use as social norm – screen use peers – getting notifications – addictive effect – revenues – further development of technologies – 24/7 availability of technologies – screen use as social norm | |||
| 3. Rules for screen use | B1: Setting and adhering to rules around screen time – screen use by peers – getting notifications (response) – fear of missing out – screen use as social norm – setting and adhering to rules around screen time | Setting rules around screen use can limit screen use by adolescents and their peers and in turn notifications, fear of missing out, and screen use as social norm, which can further strengthen the effects of rules around screen use. However, setting of rules is also influenced by the social norm and use of screens by adults. |
Abbreviations: CLD, causal loop diagram; FOMO, fear of missing out; PA, physical activity.
First of all, with regard to feedback loops, we found 11 loops in the unhealthy snacking CLD, eight in the PA, nine in the sleep, and seven in the screen use CLD. Important to note is that we mostly found reinforcing feedback loops that would strengthen the unhealthy behavior dynamics, as opposed to balancing loops that would counteract those dynamics, except for the PA CLD where it was the other way around. This latter effect is most likely because the sub‐behaviors in this CLD (i.e., active transportation and outdoor active play) were framed the other way around (positive for health) as opposed to the sub‐behaviors in the other CLDs (framed as negative for health). Looking at the feedback loops in more detail, in the unhealthy snacking CLD, we found reinforcing feedback loops relating to revenue and marketing of unhealthy food, household food budgets, and social norms towards unhealthy food. The balancing feedback loops in this CLD related to a decrease in peer pressure to eat unhealthy snacks, which resulted from school food policies that limit availability and exposure to unhealthy food. In the sleep CLD, we observed many interrelating feedback loops in particular with regard to the various determinants of sleep quality including presleep worries, presleep alertness, and wake up after sleep onset. Because these variables interrelate with each other and all can be individually linked to factors such as stress and screen use, we observed many feedback loops that also interrelated with each other; for example, screen use leads to more presleep alertness that leads to more waking up after sleep, which leads to more screen use. In the PA and screen use CLDs, we observed in particular many feedback relating to social norms, where, for example, social norm towards walking/cycling affects perceived safety that affects walking/cycling, which in turn affects social norm (fewer cyclists on the street). With regard to screen use, we found that all feedback loops operated through either social norm or the 24/7 availability of technology and related revenues and peer pressure.
Second, with regard to connections, we found multiple connections between subsystems. An example of this multiplicity was found in the influence of macroeconomic factors such as poverty or the price of unhealthy food upon factors relating to the home setting. Also, we found dynamic connections between the four behavior types. Notably, screen use was included in all CLDs, as it linked to sleep, unhealthy snacking, and PA. For example, in the PA CLD, the various options for sedentary behavior (including screen use) lead to less outdoor play.
Third, from the feedback loops, subsystems, and connections that came to light in the CLDs, we were able to identify several mechanisms—where “mechanism” is defined as a segment of a larger process in the system. We found three to five such mechanisms in each CLD. Mechanisms generally included a combination of different feedback loops, and they provided a qualitative description of what we observed in the CLD. In the sleep CLD, for instance, we identified a mechanism relating to adolescents' brain development and sleep; it showed that adolescents are still in the developmental phase, which involves learning to plan and foresee medium‐ or long‐term consequences of choices. They therefore have difficulties in efficiently planning their homework and getting their homework done during the day. The pressure to perform at school leads to more evening homework activities, presleep worries, mental alertness, and hence, later bedtimes. This creates more tiredness during the day, hampering school performance and strengthening the vicious circle. In the screen use CLD, we found that the 24/7 availability of technologies resulted in an increased use of social media, online and other digital games, and passive media such as Netflix. The use of such media also has an addictive effect that further fuels screen use. Additionally, social pressure among adolescents fosters anxiety of being left out (fear of missing out [FOMO]), and FOMO further intensifies screen use. Clear connections also emerged between screen use and sleep, further revealing how the different mechanisms interrelate.
4. DISCUSSION
4.1. Principal findings
By highlighting the system dynamics underlying the obesity‐related behaviors in question, the CLDs presented in this paper bring new insights to existing conceptual models on determinants of dietary behavior, PA, sedentary behavior, and sleep in adolescents. Most of the current literature focuses on single determinants directly related to the behaviors studied, possibly implying that associations or relationships between determinants and behaviors are linear and form an important explanation for the presence or absence of that behavior. 16 By integrating the existing literature and expert views into CLDs, we were able to generate a holistic and dynamic perspective on the lifestyle behaviors in question. We did so by drawing connections between factors and subsystems and by qualitatively interpreting the mechanisms that arose from the observed dynamics in the CLDs. The CLDs confirm that there are many interrelating factors explaining obesity‐related health behaviors and that there are powerful dynamics underlying these determinants that are generally not emerging from observational or intervention studies. Although those dynamics vary slightly between the four studied behaviors, we observed clear similarities in that they relate both to “traditional” subsystems, such as the home and school environment, and to newly added subsystems, including macroeconomic and microeconomic systems, social welfare, technology, and urban systems.
4.2. Reflections on the most important findings
The Foresight Obesity Systems Map was the first conceptual model to show obesity as a consequence of complex adaptive systems 26 ; however, this map still has a structure centered on the individual rather than focusing on underlying systems dynamics. 1 An important observation from the CLDs is the appearance of numerous reinforcing feedback loops that could strengthen the unhealthy behaviors and only a few balancing loops that could support the healthier alternative. Moreover, the reinforcing feedback loops were generally linked to higher level subsystems (such as macroeconomic or urban systems), in contrast to the balancing feedback loops, which were observed in home settings or school systems. An explanation for this finding could be that the main question in our study was framed in terms of factors that could explain the recent increase in childhood obesity rates—a question that logically leads to causal relationships that strengthen the outcome as opposed to balancing it. Indeed, in the PA CLD, where the sub‐behaviors were framed the other way around, we found more balancing as opposed to reinforcing feedback loops. In future studies, it will therefore be important to deliberately specify the question in all relevant directions by focusing on factors that form a risk factor as well as factors that protect from obesity‐related behaviors.
We observed that the balancing feedback loops found in our CLDs generally related to some kind of intervention (e.g., school food rules and rules around screen use) but also that these balancing loops were linked to counteracting subsystems such as social pressure to use screens or food prices of unhealthy food. This finding illustrates that using CLDs and searching for balancing feedback loops could be a promising approach to develop intervention strategies because it aids looking beyond specific settings and behaviors, thus providing a more holistic view of potential consequences, intended or unintended. For example, from the CLDs, it became clear that although interventions in home or school settings might be effective in changing behaviors in one particular setting, the interactions with macroeconomic and urban systems make those effects hard to maintain in the “real” world. This was also observed in a recent study by Ram and colleagues who conducted a natural experiment examining the effect on mental health outcomes when people relocated to a new, more favorable neighborhood. 27 Although participants, in comparison with controls, now lived closer to parks and in more walkable areas, had better access to public transport, and showed marked improvements in their neighborhood perceptions, there was no overall effect on mental health and well‐being outcomes. The authors conclude that changes in the built environment alone are unlikely to produce detectable improvements in mental health and well‐being. 27 The CLDs that we developed within the current study support this view that a focus on a single mechanism has insufficient power to achieve substantial and sustainable change in the system. A range of mechanisms cover and connect multiple levels and settings. For example, unhealthy sleep hygiene at home may be a result of societal pressure to perform at school, leading to tiredness at school. Therefore, addressing a part of that chain, such as exclusively focusing on the home setting, is unlikely to effectively tackle unhealthy sleeping behavior in adolescents. There is no silver bullet to address obesity, and multiple actions will likely be needed to effect sustainable changes where it is crucial to move beyond promoting the narrow public health benefits of prevention interventions and show that a more paradigmatic shift would have a multiplicity of sustained benefits across sectors including the economy and environment. 15 , 28 A key observation reflecting this observation in our study is the central position of screen use in the CLDs. It revealed the ways in which screen use connects dietary behavior, PA, and sleep—with more screen use leading to more unhealthy snacking, less PA, and lower sleep quality, whereas the latter again led to more snacking and less PA. This finding underlines the importance of addressing multiple behaviors simultaneously when promoting obesity‐related behaviors in adolescents. 29
However, developing intervention strategies that target different levels of the system is not easy. 28 , 30 An important dynamic for such strategies relates to group‐level processes, including social norms. Social norms, such as norms about PA, dietary behavior, or screen use, shape individual behavior. 31 , 32 Adolescents' individual behavior, in turn, also affects what is perceived as normal by other adolescents, thus impacting such behaviors of their peers. Our CLDs on screen use and PA in particular suggest that feedback via social norm can be very powerful as it explained the majority of the identified feedback loops. It thereby underlines the importance of actions focusing on group‐level determinants, such as social norms with respect to “normative physical activity,” in order to effectively promote healthy energy‐related behaviors. Of course, social norm is a complex construct itself, heavily influenced by, for example, social media, marketing, and policy that emerged out of a paradigm that values free market principles (e.g., weak industry self‐regulation rather than strict policies 33 ), which again all should (and can) be considered when using systems models to understand health‐related behaviors. 28 Crielaard et al. show how systems dynamics modeling can be used to further unpack the influence of social norm on obesity by simulating the system's emergent behavior. 34
4.3. Methodological considerations
At the start of the study, we envisaged that developing CLDs based on the relevant literature would aid in understanding the complexity of obesity‐related behaviors. In the process of building the CLDs, especially in Step 4, we indeed uncovered important underlying dynamics that have generally not been reported in the literature to date. When unhealthy behaviors emerged from those dynamics, it also became evident that achieving significant reductions in overweight and obesity will require change in macroeconomic, social welfare, technology, and urban systems, rather than a focus on the desired health behavior alone. Although we are confident that the observed dynamics exist, our methods relied on extensive expert interpretation and not exclusively on data from the scientific literature. We should therefore point out that the reported CLDs do not provide evidence for the exact working of the dynamics and have not yet been empirically tested. Nonetheless, by using the CLD technique, we uncovered dynamics that are generally underreported. It is now important to augment our evidence base regarding those types of dynamics and to broaden our use of interdisciplinary and transdisciplinary research methods. 28
The fact that the dynamics found in our study are currently underreported in the literature raises the question of whether they should be included in the CLDs as described in this paper. Indeed, during the CLD development process, several factors were added by the academic experts, which were not extracted from the literature (although some were extracted from additional qualitative studies). We do not consider this a particular weakness of our study. Those macrolevel factors are, in fact, discussed in the literature but generally not in systematic reviews, so that such factors did not always come up in our original search. The CLDs therefore expose a gap between what is currently covered by the main body of literature (which focuses mostly on determinants directly related to health behaviors and/or that are well defined and easy to measure) and the existing body of expert opinion on important factors to be addressed in obesity prevention (macrolevel factors more indirectly related to health behaviors). Examples of literature where macrolevel factors are discussed are numerous. They include reports by the Lancet Commission on Obesity 1 and the 2018 World Health Organization (WHO) Independent High‐Level Commission on Noncommunicable Diseases, both of which recommend political leadership, changes in governance, health and finance systems, and accountability in order to deliver change in noncommunicable disease prevalence. 35 In line with this, a recent viewpoint by Berwick has argued that mostly circumstances outside the health domain nurture or impair health and that the power of societal forces (conditions of birth and early childhood, education, work, the social circumstances of children's elders, and community resilience) is enormous compared with the power of public health to counteract negative forces. 36 A next step would therefore be to delve deeper into the exact workings of these macrolevel subsystems, in order to provide insight for potential intervention strategies. Here, it seems particularly worthwhile to invest in strategies that can improve these societal circumstances, so that individuals will require a lower level of agency to derive benefit. Such strategies are likely to be the most effective and most equitable. 37
Another methodological consideration relates to the generalizability of our findings. As noted above, we did not aim to develop a full conceptual model but rather to understand the systems dynamics underlying four obesity‐related behaviors in adolescents in urban neighborhoods with a lower socioeconomic status. We expect that the types of dynamics observed in this study (mechanisms, feedback loops, and connections between subsystems) are more or less universal to other settings and that our findings can aid other studies in uncovering similar dynamics. However, understanding the exact working of such mechanisms will likely require repeating the process for another specific setting, including country, target population, and target behaviors. Moreover, the exact outcome of a CLD depends on the boundaries set, as in our exclusion of factors relating to adolescent biology such as genetic factors or hormonal influences. Such factors might need to be included to gain a more comprehensive understanding of a system. Here, it is also important to include the viewpoint of the target group itself (as well as important stakeholders), which we will do in the next stages of the LIKE program to build a more complete understanding of the system. 19
Finally, an important next step is to look at the temporal dimensions in our CLDs. We have included mechanisms that work in different time frames—some with a relatively short time span (such as caffeine use) and some with a long‐term nature (for instance, participation in outdoor active play leads to increased motor fitness or change of social norm). When it comes to the development of interventions, it is important to specify the time frame that applies to specific mechanisms, because that will also guide the type of intervention that is required and the ways that effectiveness should be determined.
5. CONCLUSION
Our findings demonstrate that there are many interrelating factors explaining obesity‐related behaviors and that there are powerful dynamics underlying these determinants, which are generally not included in observational or intervention studies. We observed clear similarities in the highlighted dynamics in the four studied behaviors: the causal loops include traditional themes, such as home and school environment, as well as less explored themes relating to macroeconomic systems, social welfare, technology, and urban systems. The use of CLDs can support developing intervention strategies, because they create a more dynamic, holistic view of intended and unintended potential consequences, and of the ways in which interventions in one particular setting, such as home or school, might be influenced by the interactions with other settings, such as macroeconomic and urban systems.
CONFLICT OF INTEREST
None declared.
ACKNOWLEDGEMENTS
We'd like to thank all experts who critically reviewed the causal loop diagrams: Prof Jaap Seidell, Dr Maartje van Stralen, Dr Carry Renders, Dr Roel Hermans, and Emma van den Eynde. This work was supported by a grant from the Netherlands Cardiovascular Research Initiative: an initiative with support of the Dutch Heart Foundation, ZonMw, CVON2016‐07 LIKE.
APPENDIX A. LONGLIST AND SHORTLIST OF FACTORS RELATED TO OBESITY‐RELATED BEHAVIOR EXTRACTED FROM THE LITERATURE THAT WERE INCLUDED IN THE CAUSAL LOOP DIAGRAMS
| Dietary behavior | Physical activity | Sedentary behavior | Sleep |
|---|---|---|---|
|
‐ Unhealthy snacking and consumption of sugar‐sweetened beverages ‐ Dieting ‐ Skipping meals ‐ Nutrition education obtained from parents ‐ Healthy (parental) role model behavior ‐ House food rules ‐ Pressure to finish eating/plate ‐ Involving child in nutrition‐related practices ‐ Healthy food routines parents ‐ Healthy body image ‐ Disordered eating behavior ‐ Peer pressure to eat unhealthy ‐ Social support healthy eating towards child and parents ‐ Parental support healthy eating ‐ Nutrition knowledge child and parents (nutritional knowledge of main caregiver) ‐ Availability of unhealthy and healthy foods and drinks (availability of unhealthy food) ‐ Accessibility of unhealthy and healthy food and drinks (accessibility of unhealthy food) ‐ Visibility healthy foods and drinks ‐ Income parents ‐ Highest attained education parents ‐ Level of education child ‐ Risk perception child ‐ Attitudes towards healthy/unhealthy eating child and parents (positive attitude towards unhealthy food) ‐ Self‐efficacy towards healthy eating child and parents ‐ Sleep deprivation child (unhealthy sleep behavior) ‐ Mental health child ‐ (Un)healthy food drink preferences child ‐ Price of healthy and unhealthy food and drinks (Price of unhealthy food) ‐ Marketing of healthy and unhealthy foods and drinks (marketing of unhealthy food) ‐ Social media exposure related to body image ‐ Social norm healthy eating Impulsive behavior child ‐ Nutrition education at school ‐ Cooking skills child and parents (cooking skills main caregivers) ‐ Availability of parents around eating times/moments (available time) ‐ Length and inflexibility of working hours ‐ Fading of traditional eating patterns ‐ Frequency of eating moments ‐ Household budget spent on unhealthy food ‐ (healthy) Food routines at home ‐ Adequate kitchen equipment ‐ Physical activity child ‐ Sedentary behavior ‐ Smoking ‐ Stress levels of child and parents (stress) ‐ Screen time ‐ Portion size (portion size of unhealthy food) ‐ Unconscious overeating ‐ Emotional eating ‐ Eating together at the table ‐ School food rules ‐ Availability of healthy school canteen ‐ Availability of healthy sport canteen ‐ Attractive presentation of unhealthy food and drinks ‐ Duration of lunch breaks ‐ Opening hours of school canteen ‐ Meal duration ‐ Bringing own lunch to school ‐ Availability of vending machines with unhealthy food at school ‐ Parents have a paid job ‐ Authoritative parenting style ‐ Authoritarian parenting style ‐ Permissive parenting style ‐ Using food as a reward ‐ Boredom/hanging together ‐ Eating unhealthy as social activity ‐ Normalization of the consumption of unhealthy food ‐ Exposure of unhealthy food (social) media ‐ Price of food processing ‐ Revenue ‐ Poverty ‐ Health |
‐ Access/availability of family transport ‐ Access/provision of school facilities/resources ‐ Availability of PA equipment (PA materials) ‐ Active means of transport to school ‐ Access/distance to destinations ‐ Traffic‐related hazards (safety OAP/AT environment [parent perceived]) ‐ Traffic density ‐ Availability/access/proximity of public transport system (public transport network) ‐ Use of public transport ‐ Priority spending money on public transport ‐ Availability/access/proximity of recreational facilities (attractive environment for PA) ‐ Availability/access PA infrastructure/equipment (attractive environment for PA) ‐ Environment aesthetics (attractive environment for PA) ‐ Amount of green/blue space ‐ Urbanization ‐ Pedestrian and cyclist safety structure (safety OAP/AT environment [parent perceived]) ‐ Walkability ‐ Time spent outdoors ‐ PA‐related policies by local government ‐ PA school policy ‐ PA‐related school policies (time allowed for free play, field trips) ‐ Organized activities ‐ Recess (proportion class time vs. recess) ‐ School type (high school vs. vocational) ‐ Encouragement from significant others (parenting practices stimulating OAP/AT) ‐ Having a companion for PA (OAP/ACT peers) ‐ Parental modeling ‐ Parental watching ‐ Awareness of PA ‐ Parental concern about environment (safety OAP/AT environment [parent perceived]) ‐ Safety OAP/AT environment (child perceived) ‐ Involvement of social contact ‐ Encouragement at school ‐ Teacher management (organization of activities) ‐ PA level at school (teacher PA level) ‐ Seeing people exercise (neighborhood) (OAP/AT peers) ‐ Affective judgement (enjoyment in participation in OAP) ‐ Imagination for OAP ‐ Previous positive experience with OAP ‐ Interest ‐ Perceived behavioral control ‐ Perceived physical appearance ‐ Perceived fitness (motor fitness) ‐ Perceived competence (motor skills) ‐ Physical self‐concept (confidence to participate in OAP) ‐ Self‐efficacy (confidence to participate in OAP) ‐ Self‐worth (confidence to participate in OAP) ‐ Autonomous motivation/regulation ‐ Motivation (motivation to participate in OAP) ‐ Social norm OAP/AT ‐ Goal setting/planning ‐ Intention ‐ Knowledge of PA benefits ‐ Parental occupation ‐ Payment of fees ‐ Income individual or household ‐ Education level ‐ More options to spend free time sedentary |
‐ Sedentary behavior at baseline ‐ Eating in front of TV ‐ Food intake ‐ Between meal snacking ‐ Depressive symptoms ‐ Sometimes eating breakfast ‐ Child independent mobility ‐ Deprivation ‐ After school MVPA (alternative options for screen use)* ‐ Attendance after school program (alternative options for screen use)* ‐ SES/parental education ‐ Octracism (social support) ‐ Playground density (number of children at playground) ‐ TV set in bedroom ‐ Existence of safe places to cross roads (school neighborhood) ‐ Time (year of measurement) ‐ Time (SB at school vs. out of school) ‐ Neighborhood SES ‐ Weekend days ‐ Activity setting (type/location) ‐ Campus area per student ‐ School's facilities (lack of/poor quality) (alternative options for screen use)* ‐ Changing facilities ‐ Bike storage facilities ‐ Safe play (= boring) ‐ Spacious environment ‐ School's building design (e.g., more stairs) ‐ Outdated/poor equipment ‐ Rainfall ‐ After school program collects feedback on activities children want ‐ After school staff provided with 1–4 h of PA training ‐ Duration after school PA program session (alternative options for screen use)* ‐ After school program conducted outside (alternative options for screen use)* ‐ At least 25% of after school programs allocated to PA ‐ TV environment ‐ Time in public place; after school ‐ Time outside at home; after school ‐ Time outside at other home; after school ‐ Perceived school climate/support (teacher) ‐ School social capital (e.g. connectedness) ‐ Hours of PE ‐ Extracurricular PA weekend (alternative options for screen use)* ‐ Duration morning breaks (>15 min) ‐ Duration of lunch break ‐ Provision of pedestrian training ‐ PA infrastructure (lack of, e.g., limited physical environment) (alternative options for screen use)* ‐ Existence of lollypop person (crossing guard) ‐ Number of PA policies ‐ School offers intramural sport (alternative options for screen use)* ‐ Recess exercise (alternative options for screen use)* ‐ Quality of sports management ‐ Maternal TV viewing ‐ Watching TV as a family ‐ Number of parent in the house ‐ Parental TV habits ‐ With mom/dad; after school ‐ With unrelated adult; after school ‐ 24/7 availability of technologies ‐ Use of technologies by schools/companies ‐ Dependency of technologies ‐ Screen use for school/work ‐ Revenues (frequent use of screens generates income for technology developers) ‐ Further development of technologies ‐ Use of screen‐based (social) media by adults ‐ Getting response ‐ Attractive/addictive effect ‐ Use of screen‐based (social) media and (online) games by youths ‐ Social contact ‐ FOMO ‐ Screen use as social norm ‐ Setting and adhering to rules limiting screen use *Several factors from the longlist have been collapsed into the factor “alternative options for screen use.” |
‐ Accessibility to media device(s) in the bedroom: (1) TV, (2) game console, (3) computer, (4) tablet, and (5) mobile phone ‐ Late‐night (multi)passive* media use via (1) TV, (2) computer, (3) tablet, and (4) mobile phone ‐ Late‐night (multi)active* media use via (1) game console, (2) computer, (3) tablet, and (4) mobile phone ‐ Total time per day spent watching TV (screen use) ‐ Total daily time spent per day playing videogames (screen use) ‐ Alcohol use ‐ Evening light exposure (nonmedia device) ‐ Proper timing and intensity of daylight exposure (natural daylight exposure) ‐ Caffeine use (coffee, energy drinks, etc.) (evening snacking and caffeine use) ‐ Doing homework in the evening (evening homework) ‐ Parent‐set bedtimes and other sleep hygiene practices (at‐home rules on sleep and on evening screen use) ‐ Parental personal determinants towards healthy sleeping (knowledge, attitude, skills) ‐ Parental modeling ‐ Lacking a healthy, consistent bedtime routine ‐ Bedroom characteristics (cool, dark, quiet, clean) (safe, sleep‐stimulating home and sleep environment) ‐ Being and/or feeling unsafe at home (stress; presleep worrying) ‐ Presleep alertness ‐ Relaxing presleep activities ‐ Overcrowding at home (safe, sleep‐stimulating home and sleep environment) ‐ Noise hindering at home ‐ Needing a moment of rest ‐ Side job ‐ Biorhythm‐adapted school start times ‐ Extracurricular and social activities ‐ Sports and other after school activities during the day (daytime sports and PA) ‐ Sports and other after school activities during the evening (evening sports and PA) ‐ Pressure to perform in school (pressure to perform in school) ‐ Poor school performance ‐ Stressful school environment and/or being bullied ‐ Sleep disturbances (wake up after sleep onset and sleep onset latency [sleep quality]) ‐ Mental health issues ‐ Medicine use ‐ Obesity ‐ Obstructive sleep apnea ‐ Clinical sleep disturbances ‐ Seasonal effects on duration of days ‐ Biological morningness or eveningness preference ‐ Adolescent circadian rhythm ‐ Daytime napping ‐ Daytime sleepiness ‐ FOMO *Passive media use = watching movies, series, Netflix, YouTube, and so forth without the goal of social interaction. *Active media use = media use with an activity and/or social interaction component. |
Waterlander WE, Singh A, Altenburg T, et al. Understanding obesity‐related behaviors in youth from a systems dynamics perspective: The use of causal loop diagrams. Obesity Reviews. 2021;22:e13185. 10.1111/obr.13185
Wilma E. Waterlander and Amika Singh shared first author.
Funding information ZonMw, Grant/Award Number: CVON2016‐07; Dutch Heart Foundation
REFERENCES
- 1. Swinburn BA, Kraak VI, Allender S, et al. The global syndemic of obesity, undernutrition, and climate change: the Lancet Commission report. Lancet. 2019;393(10173):791‐846. [DOI] [PubMed] [Google Scholar]
- 2. World Health Organization (WHO) . Taking Action on Childhood Obesity. Geneva: World Health Organization; 2018. [Google Scholar]
- 3. Hammond RA. Complex systems modeling for obesity research. Prev. Chronic Dis. 2009;6(3):A97. [PMC free article] [PubMed] [Google Scholar]
- 4. Waterlander WE, Mhurchu CN, Eyles H, et al. Food futures: developing effective food systems interventions to improve public health nutrition. Agr. Syst. 2018;160:124‐131. [Google Scholar]
- 5. Flodgren GM, Helleve A, Lobstein T, Rutter H, Klepp KI. Primary prevention of overweight and obesity in adolescents: an overview of systematic reviews. Obes. Rev. 2020;21(11):e13102. 10.1111/obr.13102 [DOI] [PubMed] [Google Scholar]
- 6. Lloyd J, Creanor S, Logan S, et al. Effectiveness of the Healthy Lifestyles Programme (HeLP) to prevent obesity in UK primary‐school children: a cluster randomised controlled trial. Lancet Child Adolesc Health. 2018;2(1):35‐45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Meadows D. Living in a world of systems. In: Thinking in Systems. London: Earthscan; 2008. [Google Scholar]
- 8. Minary L, Alla F, Cambon L, Kivits J, Potvin L. Addressing complexity in population health intervention research: the context/intervention interface. J Epidemiol Community Health. 2018;72(4):319‐323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Rutter H, Savona N, Glonti K, et al. The need for a complex systems model of evidence for public health. Lancet. 2017;390(10112):2602‐2604. [DOI] [PubMed] [Google Scholar]
- 10. El‐Sayed AM, Galea S. Systems Science and Population Health. Oxford Scholarship Online: Oxford University Press; 2017. [Google Scholar]
- 11. Moore GF, Evans RE, Hawkins J, et al. From complex social interventions to interventions in complex social systems: future directions and unresolved questions for intervention development and evaluation. Evaluation‐us. 2019;25(1):23‐45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Allender S, Brown AD, Bolton KA, Fraser P, Lowe J, Hovmand P. Translating systems thinking into practice for community action on childhood obesity. Obes Rev. 2019;20(52):179‐184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Carey G, Malbon E, Carey N, Joyce A, Crammond B, Carey A. Systems science and systems thinking for public health: a systematic review of the field. BMJ Open. 2015;5(12):e009002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Baugh Littlejohns L, Baum F, Lawless A, Freeman T. The value of a causal loop diagram in exploring the complex interplay of factors that influence health promotion in a multisectoral health system in Australia. Health Res Policy Syst. 2018;16(1):126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Hawe P, Shiell A, Riley T. Theorising interventions as events in systems. Am J Commun Psychol. 2009;43(3–4):267‐276. [DOI] [PubMed] [Google Scholar]
- 16. Wittenborn AK, Rahmandad H, Rick J, Hosseinichimeh N. Depression as a systemic syndrome: mapping the feedback loops of major depressive disorder. Psychol Med. 2016;46(3):551‐562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Hovmand PS, Andersen DF, Rouwette E, Richardson GP, Rux K, Calhoun A. Group model‐building ‘scripts’ as a collaborative planning tool. Syst Res Behav Sci. 2012;29(2):179‐193. [Google Scholar]
- 18. Gerritsen S, Harre S, Rees D, et al. Community group model building as a method for engaging participants and mobilising action in public health. Int J Environ Res Public Health. 2020;17(10). 10.3390/ijerph17103457 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Waterlander WE, Luna Pinzon A, Verhoeff A, et al. A system dynamics and participatory action research approach to promote healthy living and a healthy weight among 10–14‐year‐old adolescents in Amsterdam: the LIKE programme. Int J Environ Res Public Health. 2020;17(14). 10.3390/ijerph17144928 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Petticrew M, Knai C, Thomas J, et al. Implications of a complexity perspective for systematic reviews and guideline development in health decision making. BMJ Glob Health. 2019;4(Suppl 1):e000899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. van Ekris E, Altenburg TM, Singh AS, Proper KI, Heymans MW, Chinapaw MJM. An evidence‐update on the prospective relationship between childhood sedentary behaviour and biomedical health indicators: a systematic review and meta‐analysis. Obes Rev. 2016;17(9):833‐849. [DOI] [PubMed] [Google Scholar]
- 22. Morrissey B, Taveras E, Allender S, Strugnell C. Sleep and obesity among children: a systematic review of multiple sleep dimensions. Pediatr Obes. 2020;15(4):e12619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Helbich M, Schadenberg B, Hagenauer J, Poelman M. Food deserts? Healthy food access in Amsterdam. Appl Geogr. 2017;83:1‐12. [Google Scholar]
- 24. Allender S, Owen B, Kuhlberg J, et al. A community based systems diagram of obesity causes. Plos One. 2015;10(7):e0129683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. The Systems Thinker . Guidelines for drawing causal loop diagrams. In. Vol 222011.
- 26. Government Office for Science . Foresight: tackling obesities: future choices‐project report; 2007. [DOI] [PubMed]
- 27. Ram B, Limb ES, Shankar A, et al. Evaluating the effect of change in the built environment on mental health and subjective well‐being: a natural experiment. J Epidemiol Community Health. 2020;74(8):631‐638. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Milsom P, Smith R, Walls HA. Systems thinking approach to inform coherent policy action for NCD prevention: comment on “How neoliberalism is shaping the supply of unhealthy commodities and what this means for NCD prevention”. Int J Health Policy Manag. 2020;9(5):212‐214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Brown T, Moore TH, Hooper L, et al. Interventions for preventing obesity in children. Cochrane Database Syst Rev. 2019;7:CD001871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Gerritsen S, Harre S, Swinburn B, et al. Systemic barriers and equitable interventions to improve vegetable and fruit intake in children: interviews with national food system actors. Int J Environ Res Public Health. 2019;16(8). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Ball K, Jeffery RW, Abbott G, McNaughton SA, Crawford D. Is healthy behavior contagious: associations of social norms with physical activity and healthy eating. Int J Behav Nutr Phy. 2010;7(1):86. 10.1186/1479-5868-7-86 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Wally CM, Cameron LD. A randomized‐controlled trial of social norm interventions to increase physical activity. Ann Behav Med 2017;51(5):642‐651. [DOI] [PubMed] [Google Scholar]
- 33. Kunkel DL, Castonguay JS, Filer CR. Evaluating industry self‐regulation of food marketing to children. Am J Prev Med. 2015;49(2):181‐187. [DOI] [PubMed] [Google Scholar]
- 34. Crielaard L, Dutta P, Quax R, et al. Social norms and obesity prevalence: from cohort to system dynamics models. Obes Rev. 2020;21(9):e13044. 10.1111/obr.13044 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. World Health Organization (WHO) . Time to Deliver. Report of the WHO Independent High‐Level Commission on Noncommunicable Diseases. Geneva; 2018. [Google Scholar]
- 36. Berwick DM. The moral determinants of health. JAMA. 2020;324(3):225‐226. [DOI] [PubMed] [Google Scholar]
- 37. Adams J, Mytton O, White M, Monsivais P. Why are some population interventions for diet and obesity more equitable and effective than others? The Role of Individual Agency. Plos Med. 2016;13(4). [DOI] [PMC free article] [PubMed] [Google Scholar]