

Abstract
Patient: Female, 60-year-old
Final Diagnosis: Subarachnoid hemorrhage
Symptoms: Coma
Medication: —
Clinical Procedure: —
Specialty: Neurosurgery
Objective:
Rare disease
Background:
Retroesophageal right subclavian artery, aberrant right subclavian artery, or lusoria artery constitutes an anatomical variation with a very low prevalence in the general population. Its presence in a patient does not add difficulty for cerebral arteries catheterization when a femoral approach is used, but may make the catheterization of cerebral vessels difficult when a right transradial approach is used. Unfortunately, this type of configuration of the artery is discovered after the decision to use the type of approach.
Case Report:
A 60-year-old woman with a diagnosed subarachnoid hemorrhage was studied with angiography through a transradial approach. A left carotid bifurcation aneurysm was diagnosed after three-vessel angiography was performed with a Simmons type 2 catheter, making a complete loop between the right subclavian artery, aortic arc, and left carotid artery. The ruptured cerebral aneurysm was completely occluded with 8 coils. The microcatheter used for the procedure emerged from the tip of an intermediate catheter located at the union of the vertical and horizontal segment of the petrous segment of the left carotid artery.
Conclusions:
The presence of an aberrant right subclavian artery during cerebral angiography performed through a right transradial approach renders the treatment of a left carotid cerebral aneurysms more difficult but not impossible. Utilizing an appropriate intermediate catheter allows for stable navigation of the microcatheter and complete treatment of the aneurysm. This is the first report of cerebral aneurysm embolization through a right transra-dial approach in a patient with an aberrant right subclavian artery.
Keywords: Aberrant Subclavian Artery, Intracranial Aneurysm, Subarachnoid Hemorrhage
Background
A retroesophageal right subclavian artery, or arteria lusoria, is an anatomical variant in which the right subclavian artery arises distal to the left subclavian artery as a fourth branch of the aorta. It courses towards the right arm behind the trachea and esophagus. This anatomic variant has just a 1% prevalence in the general population, but is present in almost 1 in 4 individuals who have 1 or more chromosomal defects [1,2]. It remains clinically silent in the majority of cases, usually only discovered during angiographic procedures.
In a study in which a transradial approach was used during coronary interventions, among the 0.45% of patients with a lusoria arteria, the procedural success rate was just 60%, versus 97.5% in patients without this anatomical variant [3]. To date, there have been no reports published on the treatment of cerebral aneurysms in patients with this aberrancy of the right subclavian artery.
Case Report
A 60-year-old woman presented to our unit with a subarachnoid hemorrhage: Hunt Hess 4, Fisher 4 (Figure 1). The patient was intubated, then a right radial approach was used to occlude the aneurism using a technique described in previous publications [4,5].
Figure 1.
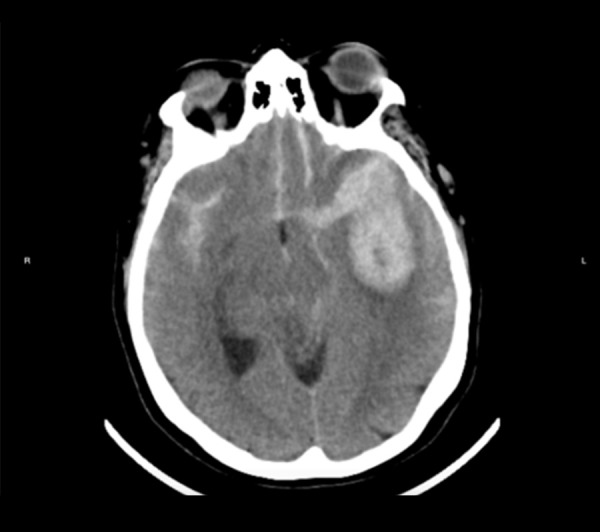
Computed tomography (CT) shows a subarachnoid hemorrhage and left temporal hematoma.
A Simmons type 2 catheter (Merit Medical Systems, Utah, USA) was slid over a 260 mm 0.035”glide-wire (Terumo Interventional Systems, Somerset, NJ) at the aortic valve. A 90° angle was observed between the ascending aorta and right subclavian artery (Figure 2). Three-vessel angiography was performed with the Simmons catheter. Left carotid injection was performed with a completely curved Simmons catheter (Figure 3). Over the glide-wire, we ascended an intermediate 072” Navien catheter (Medtronic, Minneapolis, Minnesota, USA) up to the carotid petrous segment. Then, over a 0.014”guide-wire, we advanced a microcatheter into the aneurysm (Figure 4), where we released 8 coils to successfully occlude it (Figures 5, 6).
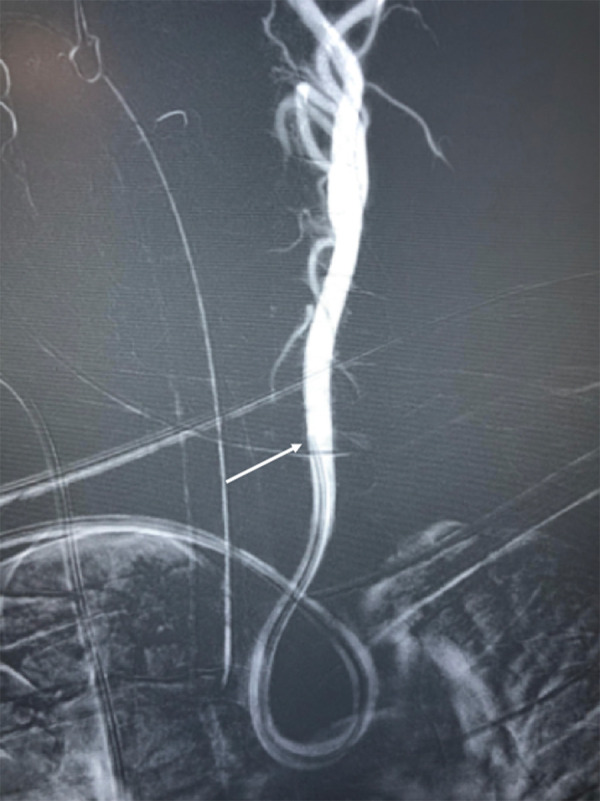
Figure 2.

Later aortogram. Dotted lines mark a 90° angle between the right subclavian artery and aortic arc. Arrowheads indicate subclavian artery direction and black arrows show aortic arc direction.
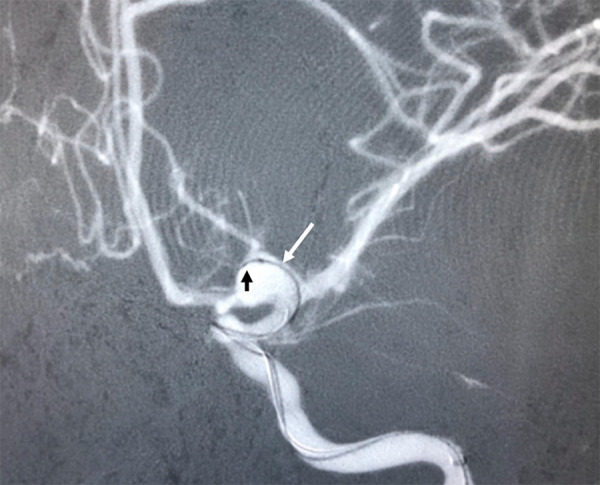
Figure 3.
A complete curved Simmons catheter is located in the left carotid artery during angiography. White arrow shows distal tip of Simmons catheter in common left carotid artery.
Figure 4.
Oblique anteroposterior angiography shows the microcatheter inside the aneurysm (white arrow) and the first coil entering it (black arrow).
Figure 5.
Oblique anteroposterior angiography shows the aneurysm occluded. Black arrow indicates the tip of the intracranial support catheter within the carotid artery’s petrous segment.
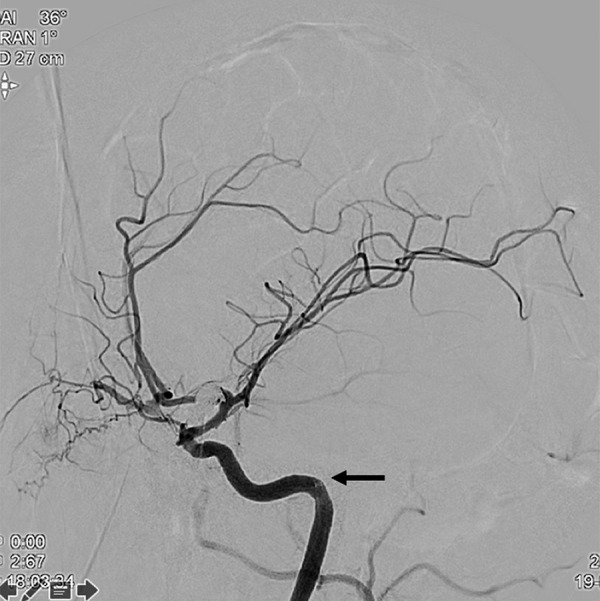
Figure 6.
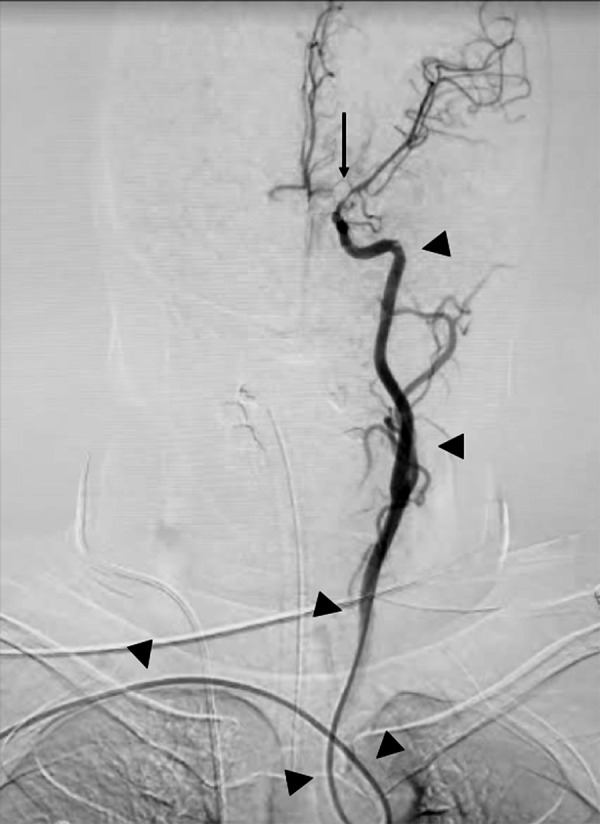
Final anteroposterior angiography shows the trajectory of the intracranial support catheter (arrowheads) and the aneurysm occluded (arrow).
Discussion
Usually, an aberrant right subclavian artery is discovered after the decision has been made to use the radial approach for an intervention; consequently, it is important to have a tool on hand that can be used to overcome this aberrancy. In such patients, using the right radial artery approach, instead of the Simmons catheter going straight into the ascending aorta, as usual, it ends up in the descending aorta, where a straight-angle curve to the ascending aorta must be navigated to reach the aortic valve.
This variation in anatomy adds a new curve before catheterization of the supra-aortic vessels (Figure 3). This anatomical variant does not preclude further advancement of a Simmons catheter, since a glide-wire can be employed to facilitate navigation of the curve. Nonetheless, the new curvature increases the difficulty of catheterization and makes holding the micro-catheter inside cerebral vessels more difficult during therapeutic procedures. In this scenario, where the pathology is more distant, a long-sheath system cannot be used, since its rigid component does not reach far enough to help navigate the vessel’s aberrant curvature. Similarly, using classic guide catheters alone is useless, because they are too short to provide the stability needed for the procedure.
Intracranial support catheters have both adequate flexibility to conform to such curves and enough length to reach the carotid artery’s petrous segment and provide stability to the microcatheter. We believe these 2 characteristics are the basis for the therapeutic success we achieved in our patient. The key moment in our procedure was negotiating the intracranial support catheter with the glide-wire at the first loop between the right subclavian and left carotid artery. This step required a very distal wire position as the intracranial support catheter was advanced. Once the tip of the catheter reached the carotid artery’s petrous segment, however, the remainder of the procedure was relatively straight-forward.
This is the first report of cerebral aneurysm embolization in a patient with an aberrant right subclavian artery. Based on our experience, we believe that using an intermediate catheter is key to approaching the carotid vessel and, once there, holding the microcatheter inside the aneurysm so it can be treated.
Conclusions
The discovery of an aberrant right subclavian artery during cerebral angiography performed through a right transradial approach renders the treatment of cerebral aneurysms more difficult. Utilizing an intracranial support catheter can facilitate the embolization of cerebral aneurysms in patients with this anatomical variant.
References:
- 1.Polednak AP. Prevalence of the aberrant right subclavian artery reported in a published systematic review of cadaveric studies: The impact of an outlier. Clin Anat. 2017;30(8):1024–28. doi: 10.1002/ca.22905. [DOI] [PubMed] [Google Scholar]
- 2.Scala C, Leone Roberti Maggiore U, Candiani M, et al. Aberrant right subclavian artery in fetuses with Down syndrome: A systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2015;46(3):266–76. doi: 10.1002/uog.14774. [DOI] [PubMed] [Google Scholar]
- 3.Valsecchi O, Vassileva A, Musumeci G, et al. Failure of transradial approach during coronary interventions: anatomic considerations. Catheter Cardiovasc Interv. 2006;67(6):870–78. doi: 10.1002/ccd.20732. [DOI] [PubMed] [Google Scholar]
- 4.Goland J, Doroszuk G. Transradial approach for endovascular diagnosis and treatment of ruptured cerebral aneurysms: A descriptive study. Surg Neurol Int. 2019;10:87. doi: 10.25259/SNI-44-2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Goland J, Doroszuk GF, Garbugino SL, Ypa MP. Transradial approach to treating endovascular cerebral aneurysms: Case series and technical note. Surg Neurol Int. 2017;8:73. doi: 10.4103/sni.sni_393_16. [DOI] [PMC free article] [PubMed] [Google Scholar]