

Abstract
During anterior cervical discectomy and fusion (ACDF), endotracheal tube difficulties are anticipated at the operative level but are unexpected elsewhere in the airway. We report the case of a 66-year-old woman who underwent C4/C5 ACDF to treat adjacent segment disease following a previous anterior cervical fixation surgery. Shortly after her lower jaw was elevated and the fusion cage was inserted, a rise in airway pressure was observed, indicating impaired breathing. Subsequent examination revealed a bent endotracheal tube in the oral cavity as the cause of the respiratory impairment. During anterior cervical surgery, elevating the lower jaw can cause the tongue root to press against the endotracheal tube. Reinforced endotracheal tubes, with a spiral-wound wire in the inner wall, would effectively prevent this issue. In the unlikely event of impaired breathing during such an operation, the oral cavity should be inspected for confirmation of an open airway.
Keywords: Anterior cervical discectomy and fusion, endotracheal tube, reinforced endotracheal tube
Introduction
Anterior cervical discectomy and fusion (ACDF) is a basic procedure commonly performed in anterior cervical surgery.[1] Single-level ACDF can be completed quickly and is not highly invasive. However, collaborative patient management between spine surgeons and anesthesiologists is crucial for the procedure considering the possibility of intraoperative airway difficulties and postoperative complications.[2,3,4] We recently observed ventilatory impairment during an ACDF operation caused by bending of the endotracheal tube in the oral cavity. Therefore, we explored the potential causes of intubation tube obstruction in cervical anterior surgery and present our findings here.
Case Report
The patient was a 66-year-old woman who had undergone anterior decompression and fusion at C5–C7 for cervical ossification of the posterior longitudinal ligament 20 years before admission at a different hospital. At our hospital, ACDF was performed to treat the adjacent segment disease at the C4/C5 level. The patient was placed under anesthesia and intubated using a 7.0-mm tracheal tube (TaperGuard®, Covidien, Tokyo, Japan), assisted by McGrath® video laryngoscopy (Aircraft Medical, Edinburgh, UK). The patient's head was immobilized using a collar, with the head facing straight up and the neck tilted slightly back. ACDF was performed using the right cervical approach following the Smith–Robinson method.[5] The operative level was ascertained by lateral X-ray fluoroscopy [Figure 1a]. The C4/C5 space was opened using a Casper-type spreader, and the disc was removed. The posterior bone spurs and joints of Luschka were partially removed. Next, the posterior longitudinal ligament was cut, the dural sac and nerve root was decompressed, and a fusion cage was inserted. Subsequently, the patient's lower jaw was elevated slightly toward the head [Figure 1b]. Shortly thereafter, the patient's airway pressure, which was monitored by the anesthetic machine, rose to 34.8 cm H2O [Table 1]. Inspection of the operative field revealed no hematomas or other sources of airway compression. The tracheal retraction was discontinued, yet the airway pressure remained elevated. Since the patient's vital signs were still stable, the surgeons decided to quickly close the surgical wound. Fluoroscopy images from the cage insertion were checked again and showed a bent tracheal tube in the oral cavity. After surgery, the surgical drape was removed and the tube was reset by hand under direct visual observation by laryngoscope. The patient's ventilation returned to satisfactory levels, she was taken off anesthesia, and the endotracheal tube was removed. The total surgery time was 97 min, and the over 25 cm H2O high airway pressure duration was approximately 9 min.
Figure 1.
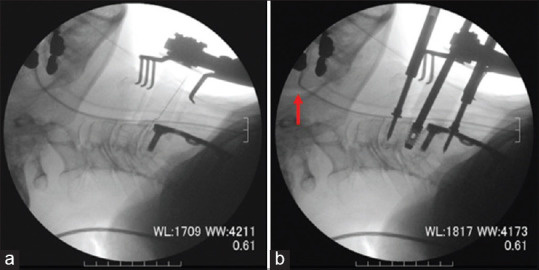
(a) Fluoroscopic X-ray image during the operation to confirm the disc level (side view). A Cathelin needle is inserted at the C4/C5 level, and the tracheal tube is gently curved. (b) Fluoroscopic X-ray image taken after fusion cage insertion (side view). Compared with Figure 1a, the lower jaw is slightly elevated toward the head. The tracheal tube is visibly bent at the root of the tongue (red arrows)
Table 1.
Maximum airway pressure profile
| Max airway pressure (cm H20) 14.3 14.7 14.9 14.5 21.4 34.8 30 |
Her postoperative course was not remarkable, and she was discharged following rehabilitation.
Discussion
This case presents an important procedural issue: the endotracheal tube can bend inside the oral cavity at a location far from the operative field during anterior cervical surgery. It also presents the importance of selecting a reinforced (spiral) tube during such a procedure.
When we first observed impaired ventilation in the patient, our first conjecture was that the tube had been obstructed when retracting the trachea to expand the surgical field. However, the airway pressure did not subside even after the retraction was stopped. We next suspected that the elevation of the lower jaw was the cause; specifically, the bending of the tube was thought to be the result of compression by the root of the tongue [Figure 2]. To confirm, we performed postoperative tests using the same model of endotracheal tube as that used in the operation. When the tube was set in a straight line [Figure 3a], it only deformed slightly in response to applied anterior pressure [Figure 3b]. By contrast, when it was pulled to the side to simulate the contralateral trachea retraction to the incision site in the anterior cervical approach [Figure 3c], it easily bent under the same anterior pressure [Figure 3d]. These simulations led us to conclude that, in this case, anterior pressure from the tongue root caused the tracheal tube to bend and become obstructed due to the patient's elevated lower jaw while the trachea was retracted (i.e., when her tube was shifted to the side). When a patient's breathing becomes impaired during an operation, the first suspected cause is usually airway difficulties at the operative level. The present case illustrates the importance of checking other sources of the problem, foremost among them, the inside of the oral cavity.
Figure 2.
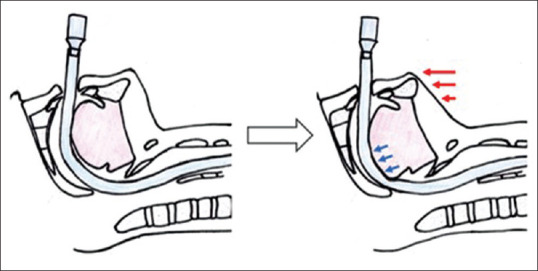
Schematic of orotracheal intubation during the surgery (sagittal cross-section). Slight elevation of the lower jaw toward the head (red arrows) results in anterior pressure on the tube by the tongue root (blue arrows)
Figure 3.
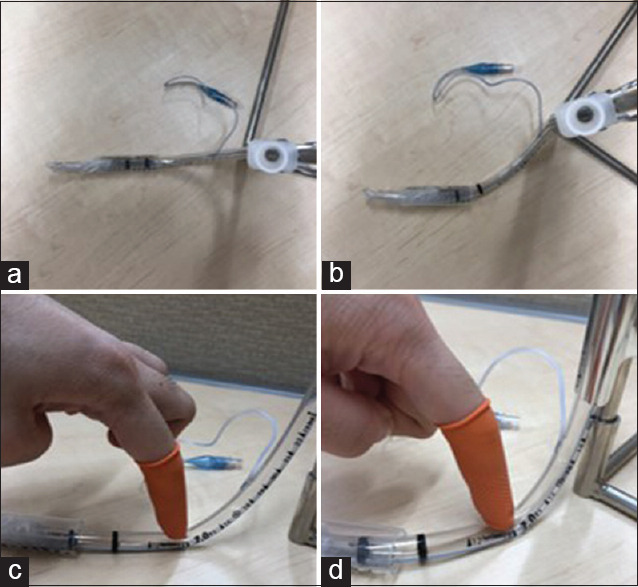
A 7.0-mm endotracheal tube (TaperGuard®, Covidien, Dublin, Ireland) is tested after the procedure. The trachea is modeled by the syringe and the tongue root by the finger. (a) Front view. (b) Lateral view. The tube deforms only slightly when anterior pressure is applied. (c) Front view. The trachea is retracted laterally, simulating the present case. (d) Side view. The tube is deformed in response to anterior pressure
The selection of a reinforced tracheal tube, with a spiral-wound wire in the inner wall, is often recommended for anterior cervical surgery. However, in clinical practice, surgeons might not choose to use one due to the relative ease of airway management when the patient lays supine (anterior approach) rather than prone or when the operation length is short, especially for single-level procedures, as was the case here. We performed similar tests on a reinforced endotracheal tube for comparison (TaperGuard® Reinforced, Covidien). When the simulated airway was retracted [Figure 4a], the tube did not bend even when considerable anterior pressure was applied [Figure 4b]. Therefore, we believe that the ventilation difficulties we observed in this case would not have occurred if we had used a reinforced tube. We, therefore, recommend proactively selecting a reinforced tracheal tube for cervical spine operations for posterior approaches in prone positions, as well as for anterior approaches in supine positions.
Figure 4.
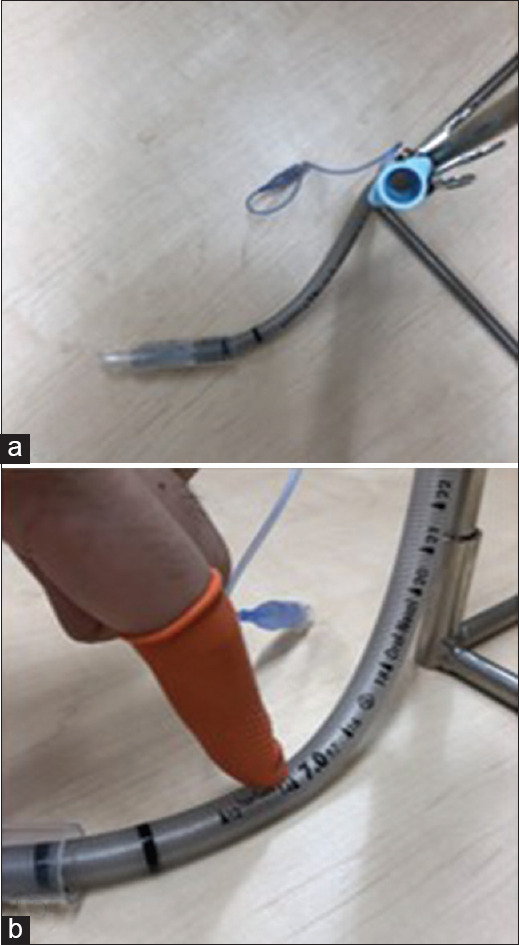
Similar testing is performed on a 7.0-mm reinforced endotracheal tube (TaperGuard® Reinforced, Covidien, Dublin, Ireland). (a) Front view. The trachea is retracted laterally, simulating the present case. (b) Side view. The reinforced tube does not bend, even in response to strong anterior pressure
There is one limitation to this report to consider. We surmised that the endotracheal tube bending during retraction was most likely induced by three-dimensional stresses on the tube; however, our tests did not constitute a scientific validation of this proposed mechanism.
Conclusion
This report documents the case of a patient whose breathing was impaired during ACDF when her endotracheal tube bent in her oral cavity. Based on our experience, we recommend the use of reinforced tracheal tubes with a spiral-wound wire in the inner wall for cervical surgery, even when an anterior approach is used. Importantly, in the event of impaired breathing during such an operation, the oral cavity should be inspected for confirmation of an open airway.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has provided her consent for her images and other clinical information to be reported in the journal. The patient understands that her name and initials will not be published, and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Saifi C, Fein AW, Cazzulino A, Lehman RA, Phillips FM, An HS, et al. Trends in resource utilization and rate of cervical disc arthroplasty and anterior cervical discectomy and fusion throughout the United States from 2006 to 2013. Spine J. 2018;18:1022–9. doi: 10.1016/j.spinee.2017.10.072. [DOI] [PubMed] [Google Scholar]
- 2.Epstein NE. A review of complication rates for Anterior Cervical Diskectomy and Fusion (ACDF) Surg Neurol Int. 2019;10:100. doi: 10.25259/SNI-191-2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Fountas KN, Kapsalaki EZ, Nikolakakos LG, Smisson HF, Johnston KW, Grigorian AA, et al. Anterior cervical discectomy and fusion associated complications. Spine (Phila Pa 1976) 2007;32:2310–7. doi: 10.1097/BRS.0b013e318154c57e. [DOI] [PubMed] [Google Scholar]
- 4.Chaudhary SK, Yu B, Pan F, Li X, Wang S, Shaikh II, et al. Manual preoperative tracheal retraction exercise decreases the occurrence of postoperative oropharyngeal dysphagia after anterior cervical discectomy and fusion. J Orthop Surg (Hong Kong) 2017;25:2309499017731446. doi: 10.1177/2309499017731446. [DOI] [PubMed] [Google Scholar]
- 5.Smith GW, Robinson RA. The treatment of certain cervical-spine disorders by anterior removal of the intervertebral disc and interbody fusion. J Bone Joint Surg Am. 1958;40-A:607–24. [PubMed] [Google Scholar]