

Abstract
Purpose:
The aim of this report was to report 2 patients who presented with acute corneal graft rejection 2 weeks after receiving the BNT162b2 messenger RNA (mRNA) vaccine for severe acute respiratory syndrome coronavirus 2.
Methods:
Case report.
Results:
Two men, aged 73 and 56 years, with a history of penetrating keratoplasty due to keratoconus were noted to have acute corneal graft rejection 2 weeks after receiving a first dose of the BNT162b2 mRNA vaccine. Both patients were treated with hourly dexamethasone 0.1% and oral prednisone 60 mg per day with prompt resolution of keratoplasty rejection.
Conclusions:
The BNT162b2 mRNA vaccine may be have been associated with a low-risk corneal graft rejection that responded well to topical and systemic steroids. Treating physicians should be aware of this potential complication and patients should be advised to report any visual changes after vaccination.
Key Words: COVID-19, corneal graft rejection, coronavirus vaccine
Corneal transplantation is the most prevalent solid-organ transplant (SOT) surgery performed worldwide.1 Vaccination-associated corneal graft rejection is a rare event.2 Only 12 individuals reported this complication, most of whom recovered with topical corticosteroid therapy.2 A recent detailed analysis, however, fails to prove direct causation.2
Severe acute respiratory syndrome coronavirus 2 and its pandemic coronavirus disease 2019 (COVID-19) has accelerated vaccine development. The BNT162b2 messenger RNA vaccine has been administered in Israel as of December 19, 2020.3 At the present time, 3.7 million individuals of a population of 9.2 million have been vaccinated. We report 2 individuals who presented to the cornea clinic with acute corneal graft rejection after administration of the BNT162b2 vaccine. The Shaare Zedek Medical Center Institutional Review Board approved this study, and patient consent was obtained.
CASE SUMMARY
Patient 1
A 73-year-old man presented with discomfort in his left eye 13 days after receiving a first dose of BNT162b2 vaccine. Ocular history included penetrating keratoplasty (PKP) in this eye due to keratoconus (1977) and regraft (2019) due to late endothelial failure. Medical history was unremarkable. The patient was maintained on 1 drop of dexamethasone 0.1% daily. A clear corneal graft was documented 2 months before admission. On presentation, corrected distance visual acuity decreased from 20/80 to 20/200. On biomicroscopy, ciliary injection, corneal edema, Descemet folds, and keratic precipitates (KPs) were noted (Fig. 1A). A diagnosis of corneal graft rejection was made. Treatment with hourly drops of dexamethasone 0.1% and oral prednisone 60 mg per day was initiated. The following week, visual acuity returned to baseline, and the corneal graft was clear (Fig. 1B). Oral and topical steroid treatment was slowly tapered, and 3 weeks after initial presentation, the patient was on 10 mg of oral prednisone and topical dexamethasone 0.1% 3 times per day.
FIGURE 1.
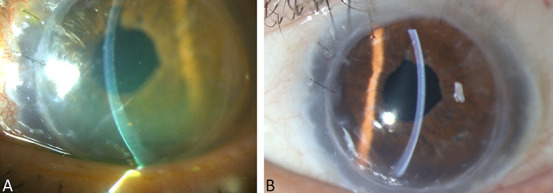
Anterior segment findings for patient 1. A, Slit lamp photograph demonstrating ciliary injection and an edematous corneal graft with Descemet folds and KPs. B, The same eye after receiving 1 week of therapy, demonstrating a clear corneal graft.
Patient 2
A 56-year-old man presented with a 2-day history of blurred vision and redness of the right eye, 14 days after receiving a first dose of the BNT162b2 vaccine. Medical history was unremarkable. Ocular history included keratoconus, with bilateral PKP performed 25 and 7 years before in the right and left eyes, respectively. Repeat right eye PKP due to late endothelial failure was performed 10 months before presentation. Topical steroid treatment had been discontinued 4 months earlier in the right eye and several years before in the left eye. On admission, corrected distance visual acuity decreased to counting fingers at 10 cm from 20/25 recorded 3 months before. Diffuse corneal edema, KPs, and anterior chamber (AC) cells were noted on slit lamp biomicroscopy, indicating corneal graft rejection. The contralateral PKP graft did not demonstrate any signs of rejection, and no AC reaction was noted. Treatment with hourly drops of dexamethasone 0.1% and oral prednisone 60 mg per day was initiated. At 1 week follow-up, marked improvement was noted with only mild corneal edema, KPs, and AC cells (Fig. 2). Two weeks later, further resolution of the corneal edema was noted, and visual acuity returned to baseline. Four weeks after the initial presentation the corneal graft was clear, oral prednisone was tapered to a dose of 10 mg per day and topical dexamethasone 0.1% was lowered to 4 times per day.
FIGURE 2.
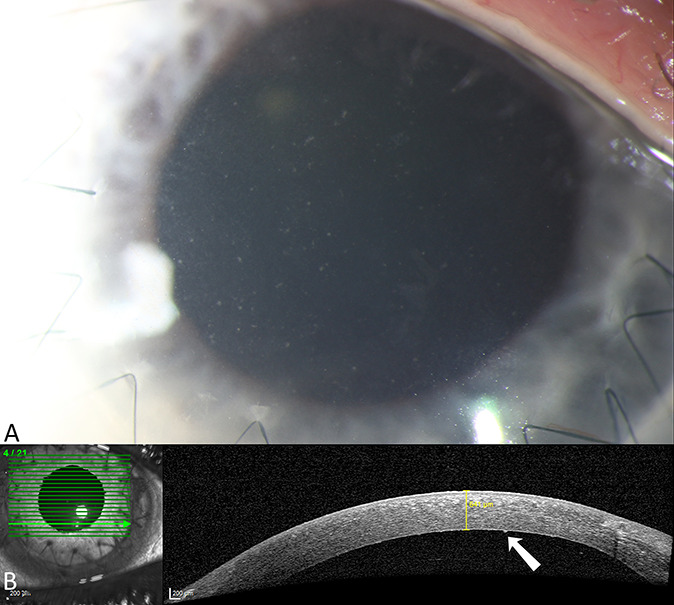
Anterior segment findings for patient 2. A, Slit lamp photograph of the corneal graft with mild diffuse KPs demonstrated (white arrow). B, Anterior segment optical coherence tomography and mild corneal edema (641 μm).
DISCUSSION
Vaccination in SOT recipients has been demonstrated as efficacious and safe because meta-analyses showed no evidence of SOT rejection after vaccination.4 It has been demonstrated that SOT recipients benefit from routine immunization practices.5 Only a few cases of corneal graft rejection after vaccination have been described after influenza, hepatitis B, tetanus toxoid, and yellow fever immunizations.2,6,7 The mechanism for vaccination-induced corneal graft rejection is not well understood. Although the eye is a site of immune privilege, active ocular inflammation can be a cause of corneal graft rejection. Vaccinations may be the trigger for a cascade of inflammatory responses either through the development of cross-reactivity with cellular antigens or because of a nonspecific immune activation.2 The BNT162b2 messenger RNA vaccine introduces genetic material into cells, which in turn generates a systemic antibody response.8 This vaccine has demonstrated high levels of neutralizing antibody titers and antigen-specific CD8+ and TH1-type CD4+ T-cell responses.9
In this report, 2 individuals presented with corneal graft rejection 2 weeks after the BNT162b2 vaccination. Neither patient had reported previous infection with severe acute respiratory syndrome coronavirus 2 nor had a history of autoimmune disease, uveitis, or herpes infection. In addition, there were no previous episodes of corneal graft rejection in either patients. Both individuals responded well to timely treatment with topical and systemic corticosteroids. To our knowledge, these are the first reported patients with acute corneal graft rejections in the setting of the COVID-19 vaccine. Although the association between vaccination and corneal graft rejections is presumptive, the proximity of the BNT162b2 vaccine to the corneal graft rejection in both individuals suggests that the immunizations may have contributed to these events.
As the worldwide COVID-19 vaccination campaign proceeds, more reports are necessary to draw a direct connection between the BNT162b2 vaccine and corneal graft rejection. Corneal graft recipients should be encouraged to receive the BNT162b2 vaccine, especially considering a recent report associating COVID-19 infection itself with acute corneal graft rejection in a patient after PKP.10 Ophthalmologists and primary care physicians should be aware of this treatable yet potentially vision-threatening possible complication. Individuals who have received the BNT162b2 vaccination should be counseled to promptly report any ocular pain or change in vision after immunization. Topical steroid treatment before and after the COVID-19 vaccination should be considered for high-risk patients.
Footnotes
The authors have no funding or conflicts of interest to disclose.
Contributor Information
Eduardo Roditi, Email: eduardoroditi@hotmail.com.
David Zadok, Email: davzadok@gmail.com.
Liron Berkowitz, Email: lironberkovitz@gmail.com.
Yishay Weill, Email: yishayweill@gmail.com.
REFERENCES
- 1.Hori J, Yamaguchi T, Keino H, et al. Immune privilege in corneal transplantation. Prog Retin Eye Res. 2019;72:100758. [DOI] [PubMed] [Google Scholar]
- 2.Lockington D, Lee B, Jeng BH, et al. Survey of corneal surgeons' attitudes regarding keratoplasty rejection risk associated with vaccinations. Cornea. 2021. [epub ahead of print]. doi: 10.1097/ICO.0000000000002662. [DOI] [PubMed] [Google Scholar]
- 3.Polack FP, Thomas SJ, Kitchin N, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med. 2020;383:2603–2615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mulley WR, Dendle C, Ling JE, et al. Does vaccination in solid-organ transplant recipients result in adverse immunologic sequelae? A systematic review and meta-analysis. J Heart Lung Transpl. 2018;37:844–852. [DOI] [PubMed] [Google Scholar]
- 5.Chong PP, Avery RK. A comprehensive review of immunization practices in solid organ transplant and hematopoietic stem cell transplant recipients. Clin Ther. 2017;39:1581–1598. [DOI] [PubMed] [Google Scholar]
- 6.Solomon A, Frucht-Pery J. Bilateral simultaneous corneal graft rejection after influenza vaccination. Am J Ophthalmol. 1996;121:708–709. [DOI] [PubMed] [Google Scholar]
- 7.Vignapiano R, Vicchio L, Favuzza E, et al. Corneal graft rejection after yellow fever vaccine: a case report. Ocul Immunol Inflamm. 2021:1–4. [DOI] [PubMed] [Google Scholar]
- 8.Jhaveri R. The COVID-19 mRNA vaccines and the pandemic: do they represent the beginning of the end or the end of the beginning? Clin Ther. 2021;43:549–556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sahin U, Muik A, Vogler I, et al. BNT162b2 induces SARS-CoV-2-neutralising antibodies and T cells in humans. medRxiv. 2020. doi: 10.1101/2020.12.09.20245175. [DOI] [Google Scholar]
- 10.Jin SX, Juthani V. Acute corneal endothelial graft rejection with coinciding COVID-19 infection. Cornea. 2020;40:123–124. [DOI] [PMC free article] [PubMed] [Google Scholar]