

Abstract
Background:
Online video-sharing platforms such as YouTube have become popular sources of medical information for patients. However, concern exists regarding the quality of such non–peer reviewed content. In fact, a previous investigation found the majority of YouTube information related to femoroacetabular impingement (FAI) to be of poor quality.
Purpose:
To provide an updated assessment of the quality of FAI-related videos available on YouTube.
Study Design:
Cross-sectional study.
Methods:
The terms FAI, femoroacetabular impingement, and hip impingement were searched on YouTube, and exclusion criteria were applied to the first 100 results for each term. The diagnostic and treatment content of each video was graded and assigned a quality assessment rating based on a previously used rubric. Video characteristics (e.g. duration, views, “likes”) were compared using both quality assessment rating and video source.
Results:
A total of 142 videos were included in the final analysis. The most common video source was educational (48.6%), followed by physician-sponsored (30.3%). The majority of videos were graded as “somewhat useful” for both diagnostic and treatment content (59.4% and 61.6%, respectively); however, treatment content was rated “not useful” more often than diagnostic information (20.3% vs. 8.7%, respectively). Videos rated as “somewhat useful” received the most views per day on average, while educational videos were the most viewed by source (views and views per day). Educational videos had more views and likes on average than physician-sponsored videos (P < .05), but all other comparisons of video characteristics by source were not significant. Video duration was the only characteristic found to vary significantly by quality assessment rating (P < .001 for both diagnostic and treatment analyses), with higher-quality videos tending to be longer. Videos rated as “excellent” and “very useful” had mean durations >30 minutes but were viewed the least.
Conclusion:
The overall quality of FAI-related content on YouTube remains low. Clinicians should be familiar with medical information available to patients on the internet, as it can influence patients’ perspectives and shared decision-making processes. This review substantiates the need for more publicly available, high-quality video content regarding the diagnosis and treatment of FAI.
Keywords: femoroacetabular impingement, FAI, hip impingement, YouTube
Femoroacetabular impingement (FAI) has generated growing interest in recent years, with increased diagnoses among young athletes in particular. 23 FAI typically results from repetitive, abnormal contact between the proximal femur and the acetabular rim and has been implicated in the development of a number of hip pathologies. 14 Young athletes with FAI combine an abnormal hip morphology with high levels of physical activity, putting them at increased risk of developing early-onset joint degeneration. 3
Treatment of symptomatic FAI generally begins with conservative management, including activity modification and physical therapy. When conservative management fails to provide adequate relief, surgical intervention is often recommended. Hip arthroscopy has become the treatment of choice for FAI in young athletes because of its minimally invasive nature, good outcomes, and potential for a quick return to sport. 2,12,13,18,21 In the United States, hip arthroscopy is most commonly performed on individuals aged 20 to 39 years. 19 Many of these young patients utilize sources outside the clinical setting to learn about their medical diagnoses and treatment options. 11
As awareness surrounding FAI has increased, the volume of related online content has likewise expanded. While 8 in 10 internet users search for medical information online, 11 there is growing concern among health care providers that the information contained in online materials is of low quality. 20,26 Moreover, as the reading proficiency required of much online orthopaedic content is above that of the recommended sixth-grade level, 8,9,17,24,25,27 many patients may seek out information in video format. YouTube (www.youtube.com) is the most popular non–peer reviewed online video-sharing platform among adults in the United States; reports from 2019 and 2020 indicated that 73% of all U.S. adults and 91% of individuals aged 15 to 29 years visit YouTube regularly. 1,22 In 2013, the first assessment of FAI-related videos on YouTube was performed, and it was determined that the content of the identified videos was of poor quality in terms of both diagnostic and treatment information. 15
It is well-known that patients frequently seek out online sources of medical information to better understand diagnoses, make treatment decisions, and assume a more active role in their health care. 27 While this trend is encouraging and an important component of shared decision making, the manner in which physicians acknowledge and engage patients’ medical knowledge during office visits can have significant implications for the physician-patient relationship. 27 Given the marked increase in the diagnosis of FAI among young individuals, the notable utilization of the internet as a source for medical information, and the widespread use of YouTube as a conduit for medical information in video format, it is imperative for orthopaedic surgeons to be familiar with the overall quality of FAI-related content available on the YouTube platform. To this effect, the purpose of this study was to provide an updated evaluation of the quality of diagnostic and treatment information regarding FAI on YouTube. We hypothesized that the overall quality of FAI-related information on YouTube would be improved since it was previously assessed in 2013.
Methods
Search Strategy
The YouTube platform was independently searched by 2 of the authors (C.R.C. and J.S.F.) between June 8 and June 10, 2020. Search execution followed the methodology established by MacLeod et al 15 using the search terms FAI, femoroacetabular impingement, and hip impingement. Results were prioritized using the “relevance” setting, and the first 100 results for each term were reviewed. Unrelated advertisements were not included in the count of 100 results. Exclusion criteria included duplicate videos, content not related to FAI, videos without audio, videos in any language other than English, and videos uploaded before September 7, 2013 (end search date of the previous study).
Data Review
Each video that met the inclusion criteria was reviewed independently by 2 authors (C.R.C. and J.S.F.). Video characteristics including duration, date uploaded, number of views, number of “likes,” and number of “dislikes” were recorded. Based on these data, the number of days online, views per day (total views per days online), likes per view (total likes per total views), likes per day (total likes per days online), and likes-dislikes difference were calculated for each video. Videos were stratified by source (physician-sponsored, educational, technique, patient testimonial, news) and evaluated in terms of diagnostic and treatment content using the scoring system previously described by MacLeod et al 15 (Appendix Table A1). For a video to be physician-sponsored, content had to be presented by a physician and/or endorsed by a medical institution. Educational videos involved a didactic explanation of FAI from a nonphysician source, inclusive of other health-related fields such as physical therapy. Technique videos were, specifically, recordings of hip arthroscopy procedures in the setting of FAI and were often paired with audio of the operating surgeon, similar to those presented in an orthopaedic curriculum. Testimonials consisted of patients with FAI describing their experiences (treatments and/or diagnoses) with the pathology. Finally, news videos were uploaded by an official news broadcast agency and did not include a physician interview.
For diagnostic content, a single point was awarded for addressing each item on the diagnostic scoring checklist for a maximum possible score of 16. The diagnostic scoring checklist contained items related to a description of FAI, patient history, physical examination, radiographic findings, advanced imaging, and diagnostic hip injection. 15 For treatment content, a single point was awarded for addressing each item on the treatment scoring checklist except for complications, for which 0.5 points were given for each complication listed up to 2 points, for a maximum possible score of 16. The treatment scoring checklist contained items related to nonoperative management, operative management, rehabilitation, and surgical complications. Each video received separate scores for diagnostic and treatment information.
Based on these numerical scores, videos were divided into 5 quality assessment ratings (QARs): “excellent” (13-16 points), “very useful” (9-12 points), “moderately useful” (5-8 points), “somewhat useful” (1-4 points), and “not useful” (0 points). Videos determined to be part of a series by title (eg part 1, part 2) and/or continuous audio/video were assessed together as a single video entity. Reviewer disagreement on QAR classification was reconciled via discussion.
Data Analysis
Categorical variables were reported as frequencies, and continuous variables were presented as means. One-way analyses of variance were used to compare continuous variables, with Bonferroni-adjusted pairwise t tests performed for any significant differences found. The Pearson correlation coefficient was calculated to assess for associations between video length and other video characteristics (number of likes, number of dislikes, and likes-dislikes difference), stratified by source and QAR. Overall statistical significance was defined as P < .05. Statistical analyses were performed using Microsoft Excel Version 16.16.20 (Microsoft Corp) and R software Version 3.6.2 (R Foundation for Statistical Computing).
Results
Pooled Results
Of the 600 videos produced by the initial search, 458 were excluded, resulting in 142 videos eligible for final analysis (Figure 1). After combining videos determined to be part of a series, 138 videos underwent quality assessment for diagnostic and treatment content. Upload dates ranged from December 20, 2013, to June 6, 2020. The mean duration of all 142 videos was 9 minutes (range, 0:11-53:41 minutes). Videos had a mean of 18,438.8 ± 43,213.5 views, 21.8 ± 52.1 views/day, 343.2 ± 995.7 likes, 0.02 ± 0.02 likes/view, 11.3 ± 33.6 dislikes, and a likes-dislikes difference of 331.9 ± 975.6. As demonstrated in Figure 2, the main source of FAI-related content was educational (48.6%; n = 69), followed by physician-sponsored (30.3%; n = 43), patient testimonial (14.8%; n = 21), technique (4.2%; n = 6), and news (2.1%; n = 3).
Figure 1.
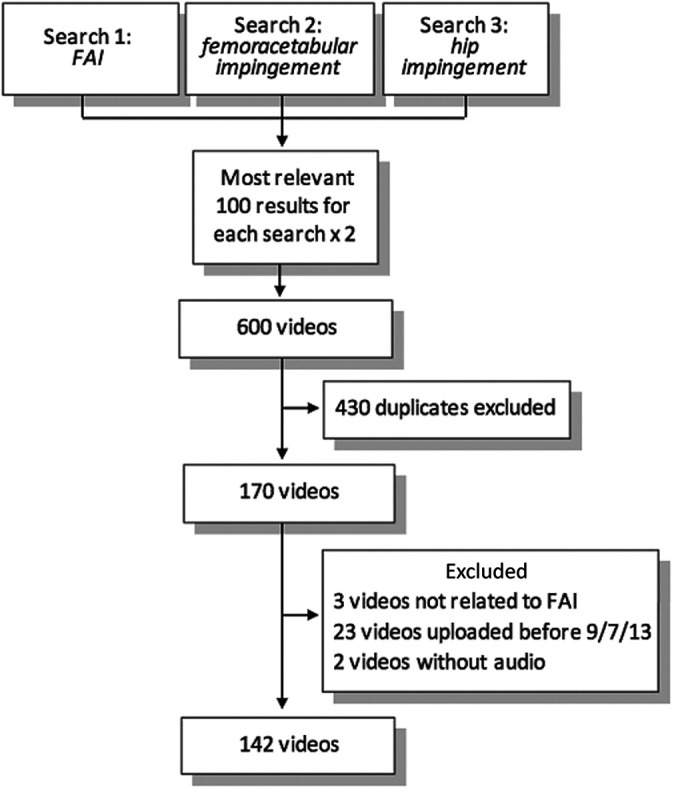
Summary of YouTube search methodology and results. Of the 600 initial search results, 458 videos were excluded. FAI, femoroacetabular impingement.
Figure 2.
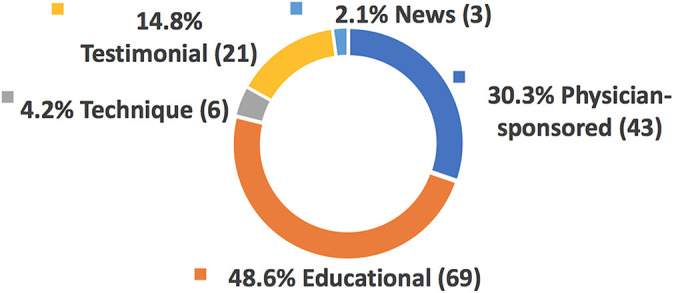
Breakdown of femoroacetabular impingement–related content on YouTube by video source.
Analysis by Content Group
In terms of diagnostic content, the majority of videos were found to be somewhat useful (59.4%; n = 82) (Table 1). Only 2 videos (1.5%) received a score in the excellent range, 9 (6.5%) were very useful, 33 (23.9%) were moderately useful, and 12 (8.7%) were not useful. Videos that contained moderately useful diagnostic information had the most views (mean, 32,668.7 views), but very useful videos had the most views per day (mean, 34.6 views/day); neither difference was statistically significant. Regarding the treatment of FAI, the majority of videos were also graded as somewhat useful (61.6%; n = 85) (Table 2). No video was rated as excellent, 4.3% were very useful (n = 6), 13.8% were moderately useful (n = 19), and 20.3% (n = 28) were not useful. Videos with somewhat useful treatment information had the most total views (mean, 26,676.6 views) and likes (mean, 541.1 likes), most views per day (mean, 28.1 views/day), and largest likes-dislikes difference (mean difference, 523.9), although the differences were not statistically significant.
Table 1.
Video Characteristics and Source by QAR for Diagnostic Content a
| QAR b | |||||||
|---|---|---|---|---|---|---|---|
| Total | Excellent | Very Useful | Moderately Useful | Somewhat Useful | Not Useful | P | |
| Video characteristic | |||||||
| No. of videos (%) | 138 (100) | 2 (1.5) | 9 (6.5) | 33 (23.9) | 82 (59.4) | 12 (8.7) | |
| Mean duration, min:s | 9:16 | 33:41 | 32:36 | 12:04 | 5:38 | 4:47 | <.001 |
| Mean days online | 947 | 465 | 850 | 1158 | 908 | 788 | .128 |
| Mean views | 18,973 | 54 | 5398 | 32,669 | 16,585 | 10,967 | .283 |
| Mean views per day | 22.4 | 0.1 | 34.6 | 27.5 | 19.7 | 20.9 | .859 |
| Mean likes | 353.6 | 2.0 | 99.6 | 560.2 | 337.0 | 138.0 | .626 |
| Mean likes per day | 0.543 | 0.003 | 1.798 | 0.538 | 0.479 | 0.229 | .352 |
| Mean likes per view | 0.016 | 0.002 | 0.023 | 0.015 | 0.017 | 0.012 | .524 |
| Mean dislikes | 11.6 | 0.0 | 1.9 | 23.7 | 9.0 | 3.0 | .196 |
| Mean likes-dislikes | 342.0 | 2.0 | 97.8 | 536.5 | 327.8 | 135.0 | .653 |
| Video source | |||||||
| Physician-sponsored | 42 | 2 | 5 | 12 | 19 | 4 | |
| Educational | 66 | 0 | 4 | 14 | 44 | 4 | |
| Technique | 6 | 0 | 0 | 0 | 4 | 2 | |
| Patient testimonial | 21 | 0 | 0 | 7 | 13 | 1 | |
| News | 3 | 0 | 0 | 0 | 2 | 1 | |
a Bolded P value indicates statistically significant difference by QAR. QAR, quality assessment rating.
b QAR score: 13-16 points = excellent; 9-12 points = very useful; 5-8 points = moderately useful; 1-4 points = somewhat useful; and 0 points = not useful.
Table 2.
Video Characteristics and Source by QAR for Treatment Content a
| QARb | |||||||
|---|---|---|---|---|---|---|---|
| Total | Excellent | Very Useful | Moderately Useful | Somewhat Useful | Not Useful | P | |
| Video characteristic | |||||||
| No. of videos (%) | 138 (100) | 0 (0) | 6 (4.3) | 19 (13.8) | 85 (61.6) | 28 (20.3) | |
| Mean duration (min:s) | 9:16 | N/A | 31:06 | 14:45 | 8:35 | 2:58 | <.001 |
| Mean days online | 947 | N/A | 452 | 1,095 | 950 | 934 | .137 |
| Mean views | 18,973 | N/A | 5496 | 9917 | 26,677 | 4787 | .072 |
| Mean views per day | 22.4 | N/A | 5.7 | 24.8 | 28.1 | 7.1 | .264 |
| Mean likes | 353.6 | N/A | 78.8 | 82.2 | 541.1 | 33.2 | .064 |
| Mean likes per day | 0.543 | N/A | 0.103 | 0.797 | 0.683 | 0.054 | .263 |
| Mean likes per view | 0.016 | N/A | 0.023 | 0.013 | 0.017 | 0.014 | .407 |
| Mean dislikes | 11.6 | N/A | 2.0 | 3.6 | 17.1 | 2.6 | .138 |
| Mean likes-dislikes | 342.0 | N/A | 76.8 | 78.6 | 523.9 | 30.6 | .075 |
| Video source | |||||||
| Physician-sponsored | 42 | 0 | 5 | 10 | 16 | 11 | |
| Educational | 66 | 0 | 1 | 2 | 48 | 15 | |
| Technique | 6 | 0 | 0 | 3 | 3 | 0 | |
| Patient testimonial | 21 | 0 | 0 | 3 | 17 | 1 | |
| News | 3 | 0 | 0 | 1 | 1 | 1 | |
a Bolded P value indicates statistically significant difference by QAR. N/A, not applicable; QAR, quality assessment rating.
b QAR score: 13-16 points = excellent; 9-12 points = very useful; 5-8 points = moderately useful; 1-4 points = somewhat useful; and 0 points = not useful.
Analysis by Source
Mean QAR did not vary significantly by video source, with the majority of videos graded as somewhat useful for all sources. In the analysis of video characteristics by source, educational videos had the most total views (mean, 33,999.8 views), views per day (mean, 35.9 views/day), total likes (mean, 667.4 likes), and likes per day (mean, 0.8 likes/day) and had the largest likes-dislikes difference (mean difference, 646.4). The popularity of educational videos is further illustrated in Table 3, which demonstrates that the 10 most viewed FAI videos were all sourced from this category. Bonferroni-adjusted pairwise t tests revealed that educational videos had significantly more views, likes, and dislikes and a greater likes-dislikes difference compared with physician-sponsored videos (P < .05). There were no significant differences in any of the other comparisons of video characteristics.
Table 3.
Overview of the Most Viewed Videos a
| No. of Views | No. of “Likes” | Video Title | URL | Source | QAR b | |
|---|---|---|---|---|---|---|
| Diagnostic | Treatment | |||||
| 236,733 | 1600 | What is FAI? Learn the truth about femoroacetabular impingement. | https://www.youtube.com/watch?v=x1d9-JcMBoU | Educational | Moderately useful | Somewhat useful |
| 218,492 | 5800 | Hip pain relief: top 3 mistakes (labral tears, arthritis, FAI) | https://www.youtube.com/watch?v=7IEy8vd6wjc | Educational | Moderately useful | Somewhat useful |
| 192,101 | 5600 | The Ultimate Guide To Hip Impingement For Powerlifters & Weightlifters ft. Shane Dowd | https://www.youtube.com/watch?v=RU8K3UAF_JA | Educational | Moderately useful | Somewhat useful |
| 171,063 | 2700 | How To FIX Frontal Hip Pain | Femoral Acetabular Impingement | https://www.youtube.com/watch?v=xx6SzL-S8SY | Educational | Somewhat useful | Somewhat useful |
| 166,259 | 5500 | Hip Flexor Strain VS Hip Impingement | #AskSquatU Show Ep. 46| | https://www.youtube.com/watch?v=ueeGt9ESkNE | Educational | Somewhat useful | Somewhat useful |
| 156,486 | 4700 | Fix For Hip Pain When Squatting (Impingement) |#AskSquatU Show Ep. 9| | https://www.youtube.com/watch?v=xVUzxzVDPyI | Educational | Somewhat useful | Somewhat useful |
| 150,782 | 1800 | Hip Impingement? Causes, Treatment, & Test for Femoral Acetabular Syndrome | https://www.youtube.com/watch?v=S0b_I6liRLg | Educational | Moderately useful | Somewhat useful |
| 138,771 | 3000 | Hip Impingement and How to Clear it Freakishly Fast | Trevor Bachmeyer | SmashweRx | https://www.youtube.com/watch?v=f3b9Nz-G0Kw | Educational | Somewhat useful | Somewhat useful |
| 116,354 | 788 | BEST EXERCISES for FAI Hip Impingement | https://www.youtube.com/watch?v=vRwCHfS_Dt0 | Educational | Somewhat useful | Somewhat useful |
| 97,643 | 1500 | Hip Impingement (FAI) Pain Stretches & Exercises - Ask Doctor Jo | https://www.youtube.com/watch?v=ATQcSDuumL8 | Educational | Somewhat useful | Somewhat useful |
a QAR, quality assessment rating
b QAR score: 13-16 points = excellent; 9-12 points = very useful; 5-8 points = moderately useful; 1-4 points = somewhat useful; and 0 points = not useful.
Analysis by Quality Assessment Rating
The majority of videos were rated as somewhat useful for both diagnostic and treatment information (Figure 3). However, videos were much more likely to be scored as not useful for treatment content than for diagnostic content (20.3% vs 8.7%). The highest rated videos overall for both diagnostic and treatment content are listed in Table 4.
Figure 3.

Quality assessment rating (QAR) of femoroacetabular impingement-related videos on YouTube. Videos were evaluated for diagnostic and treatment content separately and scored on a scale from 0 (worst) to 16 (best). The majority of videos were found to be somewhat useful (QAR 1-4) for both diagnostic (59.4%; n = 82) and treatment (61.6%; n = 85) content.
Table 4.
Overview of the Most Useful Videos in Terms of Composite QAR a
| Composite QAR b | Video Title | Video URL | Source |
|---|---|---|---|
| Very useful | An Overview of Femoroacetabular Impingement and How to Treat It | https://www.youtube.com/watch?v=UR7-bSzwrkU | Physician-sponsored |
| Very useful | Dr. Gatt Discusses Femoroacetabular Impingement | https://www.youtube.com/watch?v=Hn6AF_9qojA | Physician-sponsored |
| Very useful | Hip Femoral Acetabular Impingement Pts. 1 & 2 c | https://www.youtube.com/watch?v=zcX_m1I3DsQ | Physician-sponsored |
| Very useful | Hip Arthroscopy for Femoroacetabular Impingement | https://www.youtube.com/watch?v=D8zlHVsMofo | Physician-sponsored |
| Very useful | Femoroacetabular Impingement (FAI) - The Young Orthopod | https://www.youtube.com/watch?v=ENjq5Is94PE | Educational |
| Moderately useful | Femoroacetabular Impingement (FAI) | https://www.youtube.com/watch?v=shKtRUgdnys | Physician-sponsored |
| Moderately useful | Femoroacetabular Impingement (FAI) Causes & Treatment to Avoid Surgery | https://www.youtube.com/watch?v=4YJYDcyyCw0 | Physician-sponsored |
| Moderately useful | Marcus Bankes Introduction to Hip Impingement (FAI) | https://www.youtube.com/watch?v=z1kit_01WT4 | Physician-sponsored |
| Moderately useful | Femoroacetabular Impingement | https://www.youtube.com/watch?v=SaMFvI_3j4g | Physician-sponsored |
| Moderately useful | Femoral Acetabular Impingement | https://www.youtube.com/watch?v=LdDhRVewKCU | Educational |
| Moderately useful | Hip Impingement FAI What is it and how do we treat it |
https://www.youtube.com/watch?v=Xv_bO2uqbno
|
Physician-sponsored |
a QAR, quality assessment rating.
b QAR calculated by averaging diagnostic and treatment QAR scores, where 13-16 points = excellent, 9-12 points = very useful, 5-8 points = moderately useful, 1-4 points = somewhat useful, and 0 points = not useful.
c Videos scored as a series.
The only video characteristic found to vary significantly by QAR was duration (P < .001 for both diagnostic and treatment content). Videos rated as excellent and very useful for diagnostic content were significantly longer than were moderately useful, somewhat useful, and not useful videos (P < .05 for all). Moderately useful videos were also longer than were somewhat useful videos (P < .05). Interestingly, excellent and very useful videos had mean durations >30 minutes but were viewed the least and excellent videos had the fewest views per day. For treatment content, very useful videos were significantly longer than were moderate, somewhat, and not useful videos (P < .05 for all). Moderately useful videos tended to be longer than were not useful videos, but the difference was not significant. Upon further analysis, video length was not significantly correlated with views, likes, dislikes, likes-dislikes difference, or views per day. Likes per day was the only metric found to be significantly associated with video length (P < .001). Video quality, as defined by QAR, also was not correlated with views, likes, dislikes, likes-dislikes difference, likes per day, views per day, or likes per view.
Discussion
The purpose of this review was to provide an updated assessment of the quality of videos related to FAI on YouTube. Based on the results of this study, individuals who search YouTube for information on FAI will mostly encounter low-quality content, both in terms of diagnostic and treatment information. Of the 142 videos assessed, only 2 (1.5%) achieved a score of excellent for diagnostic information, and no videos were graded as excellent for treatment information. The majority of videos were scored as somewhat useful for both diagnostic (59.4%) and treatment information (61.6%). Interestingly, video quality was not correlated with views, likes, views per day, likes per day, likes per view, or likes-dislikes difference.
YouTube is one of the most popular online video-sharing platforms in the world, with a digital library numbering in the billions that attracts >30 million visitors per day. 1 For this reason, uploading content to such a popular online repository offers multiple benefits to health care providers including practice-promotion, personal notoriety, patient education, and even direct financial reimbursement if videos achieve sufficient popularity. However, with so much non–peer reviewed content available for public consumption, it is imperative that content uploaded by the medical community provides a reliable and accurate source of information for patients. This is only the second study to analyze the quality of FAI-related videos on YouTube. Compared with the previous study by MacLeod et al, 15 the overall quality of FAI-related content has not improved significantly. In fact, that investigation also found the majority of videos to be somewhat useful for both diagnostic and treatment information (53.8% and 60.3%, respectively). The primary source of FAI-related videos on YouTube has changed from physician-sponsored (44%) in the previous study to educational (48.6%) in the current study.
Possibly because of a smaller sample size (n = 52), MacLeod et al 15 did not find any significant differences in video characteristics (duration, views, likes, views per day, likes per day, likes per view, or likes-dislikes difference) between QAR groupings. The current study assessed nearly 3 times the number of videos and found that duration varied significantly by QAR, with the highest-quality videos (excellent and very useful) having longer mean durations. However, these videos also had fewer views and views per day on average, suggesting a possible viewer preference for brevity over thoroughness. Other recent analyses of viewer engagement with internet videos have also revealed a preference for brevity. 4,5,10 A 2016 study, for instance, found that >60% of viewers lost interest around the 4-minute mark, adding that viewership decayed exponentially after a video exceeded 6 minutes. 10 Interestingly, however, the mean duration of YouTube videos in 2018 was 11 minutes 42 seconds. 4 Although further research on this topic is warranted, our findings suggest that the optimal FAI video ranges from 5 to 15 minutes. Based on observed viewing patterns, it seems prudent to address the most vital patient-relevant content first—potential causes of hip pain, pertinent patient history, required imaging, treatment options, postoperative protocol—before addressing more physician-oriented information, such as radiographic interpretation and surgical technique.
Regarding diagnostic content, videos assessed in this study generally provided a good description of FAI including common symptoms, such as pain in the anterior groin that is exacerbated by repetitive movements. On the other hand, the differential diagnosis for FAI and risk-factors associated with FAI were rarely addressed. The differential diagnosis for FAI is broad and includes diverse musculoskeletal pathologies, such as psoas tendinitis, trochanteric bursitis, snapping hip syndrome, athletic pubalgia, and femoral neck stress fractures. Although the videos assessed in this study focused on FAI by definition, failing to at least mention some of the more common causes of hip pain in the adolescent and adult populations may lead to improper self-diagnosis and self-treatment, which can delay care and lead to further injury.
In terms of treatment content, most videos provided adequate information related to nonoperative and operative options. However, videos seldom mentioned postoperative restrictions, rehabilitation protocols, or surgical complications. While advances in hip arthroscopy have certainly allowed for reduced recovery time and lower complication rates compared with open procedures, rehabilitation after arthroscopic management of FAI still involves multiple weeks of protected weightbearing, and return to sports is often delayed for several months. 16 As such, ensuring that patients are aware of the typical postoperative protocol after surgical treatment of FAI is of the utmost importance in terms of managing patient expectations, promoting patient adherence, and ensuring optimal outcomes.
This study has several limitations that merit further discussion. First, the content available on YouTube is constantly changing. Consequently, the findings of this study only reflect a snapshot in time, as defined by the study period. Second, the YouTube search algorithm takes into account numerous variables including a user’s geographic location and search history. 6,7 Accordingly, the videos assessed in this study may differ slightly from the video results produced from a search of the same terms by another user. However, by including the first 100 results produced by each search term, the videos assessed in this study are likely representative of the FAI-related information that most users would encounter. Third, the quality assessment checklist used to evaluate videos emphasized thoroughness over other measures of quality. Carrying forward the methodology devised by MacLeod et al 15 allowed for a longitudinal assessment of FAI-related content on YouTube but precluded the assessment of quality based on other variables such as inclusion of illustrations/graphics/animations and required reading level. Fourth, the extracted data for viewer engagement did not specify how long a user watched a particular video, how many views came from independent users, or the degree of viewer comprehension. Therefore, caution should be taken when interpreting metrics such as views, likes, and dislikes. Fifth, it is important to note that this study’s findings are specific to YouTube and should not be extrapolated to other online video platforms. Future studies should perform similar assessments of other popular online video repositories such as Vimeo.
Conclusion
Patients, particularly those who are younger, frequently utilize online video platforms such as YouTube to learn about medical conditions. Therefore, it is essential for clinicians to be aware of the quality of online content, as such information has the potential to affect the physician-patient relationship and ultimately influence patient care. In this study, the FAI-related content on YouTube was found to be low quality overall, both in terms of diagnostic and treatment information. In addition, video quality was not correlated with popularity, as measured by views and likes. The findings of this review indicate that, in general, YouTube is not a reliable source of high-quality information related to the diagnosis and treatment of FAI.
APPENDIX
Table A1.
Quality Assessment Checklist Used to Evaluate the Diagnostic and Treatment Content of FAI-related YouTube Videos a .
| Diagnostic Content |
| Explanation (2 points) · Discussion of what FAI is (cam lesion, pincer lesions) · Discussion of a differential diagnosis of hip pain History (6 points) · Hip pain (groin, lateral, buttock, anterior thigh, knee) · “C sign” · Mechanical symptoms (catching, clicking, locking, instability) · Provoking factors (pain with activity, repetitive hip flexion, prolonged sitting) · High-risk activities (athletic activity, repetitive hip flexion and rotation) · Preexisting pathologic hip conditions (DDH, SCFE, Legg-Calve-Perthes disease, coxa vara, malunited femoral neck space, femoral osteotomy, acetabular osteotomy) Physical Examination (5 points) · Limited range of motion (decreased flexion, adduction, internal rotation) · Log roll · Resisted straight-leg raise · Impingement test · Posterior impingement test (flexion, abduction, external rotation) Other (3 points) · Radiographic findings · Advanced imaging (CT, CTA, MRI, MRA) · Diagnostic hip injection with local anesthetic |
| Treatment Content |
| Presurgical (3 points) · Nonoperative treatment (activity modification, physical therapy, core strengthening) · Surgical indications (intra-articular pathologic conditions of the hip amenable to treatment) · FAI surgical contraindications (osteoarthritis, degenerative changes, asymptomatic radiographic findings) Surgical Procedures (7 points) · Surgical setup (supine or lateral decubitus with traction table) · Hip arthroscopy · Open or mini-open procedures · Labral debridement or repair · Femoroplasty (femoral head-neck reshaping) · Acetabuloplasty · Articular cartilage procedures (chondroplasty, microfracture) Rehabilitation (4 points) · Period of protected weightbearing and ROM · Physical therapy · No twisting or impact activity for 12 weeks · Unrestricted activity at approximately 6 months Complications (2 points) · Minimum of 4 (nerve injury, vascular injury, chondral damage, fluid extravasation, infection, venous thromboembolism, iatrogenic fracture, osteonecrosis, heterotopic ossification, hip instability, adhesions); 0.5 points each for maximum of 2 points |
a Developed by MacLeod et al. 15 CT, computed tomography; CTA, computed tomography arthrography; DDH, developmental dysplasia of the hip; FAI, femoroacetabular impingement; MRA, magnetic resonance arthrography; MRI, magnetic resonance imaging; ROM, range of motion; SCFE, slipped capital femoral epiphysis.
Footnotes
Final revision submitted December 22, 2020; accepted February 9, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.P.T. has received a grant from Arthrex and education payments from Smith & Nephew, Peerless Surgical, Arthrex, and Gotham Surgical. T.S.L. has received speaking fees from Linvatec, education fees from Arthrex and Gotham Surgical, nonconsulting fees from Arthrex and Smith & Nephew, and consulting fees from KCI USA, Smith & Nephew, and Linvatec. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
- 1. Aslam S. YouTube by the numbers: stats, demographics & fun facts. Omnicore. Updated October 28, 2020. Accessed December 18, 2020. https://www.omnicoreagency.com/youtube-statistics/
- 2. Botser IB, Smith TW, Jr, Nasser R, Domb BG. Open surgical dislocation versus arthroscopy for femoroacetabular impingement: a comparison of clinical outcomes. Arthroscopy. 2011;27(2):270–278. [DOI] [PubMed] [Google Scholar]
- 3. Byrd JW. Femoroacetabular impingement in athletes, part 1: cause and assessment. Sports Health. 2010;2(4):321–333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Clement J. Average YouTube video length as of December 2018, by category. Statista. Updated July 17, 2018. Accessed December 14, 2020. https://www.statista.com/statistics/1026923/youtube-video-category-average-length/
- 5. Comscore. Comscore Releases January 2014 U.S. Online Video Rankings. Comscore. Updated February 21, 2014. Accessed December 14, 2020. https://www.comscore.com/Insights/Press-Releases/2014/2/comScore-Releases-January-2014-US-Online-Video-Rankings
- 6. Cooper P. How does the YouTube algorithm work? A guide to getting more views. Hootsuite. Accessed July 9, 2020. https://blog.hootsuite.com/how-the-youtube-algorithm-works/
- 7. Covington P, Adams J, Sargin E. Deep neural networks for YouTube recommendations. RecSys '16: Procedings of the 10th ACM Conference on Recommender Systems. Association of Computing Machinery; 2016:191–198. [Google Scholar]
- 8. Crozier-Shaw G, Queally JM, Quinlan JF. Metal-on-metal total hip arthroplasty: quality of online patient information. Orthopedics. 2017;40(2):e262–e268. [DOI] [PubMed] [Google Scholar]
- 9. Dalton DM, Kelly EG, Molony DC. Availability of accessible and high-quality information on the Internet for patients regarding the diagnosis and management of rotator cuff tears. J Shoulder Elbow Surg. 2015;24(5):e135–e140. [DOI] [PubMed] [Google Scholar]
- 10. Fishman E. How long should your next video be? Wistia. Updated July 5, 2016. Accessed December 14, 2020. https://wistia.com/learn/marketing/optimal-video-length#2-there-is-significant-drop-off-between-2-and-3-minutes
- 11. Fox S. Health Topics. Pew Research Center Information and Technology. Updated February 1, 2011. Accessed June 13, 2020. https://www.pewresearch.org/internet/2011/02/01/health-topics-2/
- 12. Levy DM, Kuhns BD, Frank RM, et al. High rate of return to running for athletes after hip arthroscopy for the treatment of femoroacetabular impingement and capsular plication. Am J Sports Med. 2017;45(1):127–134. [DOI] [PubMed] [Google Scholar]
- 13. Litrenta J, Mu BH, Ortiz-Declet V, et al. Hip arthroscopy successfully treats femoroacetabular impingement in adolescent athletes. J Pediatr Orthop. 2020;40(3):e156–e160. [DOI] [PubMed] [Google Scholar]
- 14. Lynch TS, Bedi A, Larson CM. Athletic hip injuries. J Am Acad Orthop Surg. 2017;25(4):269–279. [DOI] [PubMed] [Google Scholar]
- 15. MacLeod MG, Hoppe DJ, Simunovic N, et al. YouTube as an information source for femoroacetabular impingement: a systematic review of video content. Arthroscopy. 2015;31(1):136–142. [DOI] [PubMed] [Google Scholar]
- 16. Matsuda DK, Carlisle JC, Arthurs SC, Wierks CH, Philippon MJ. Comparative systematic review of the open dislocation, mini-open, and arthroscopic surgeries for femoroacetabular impingement. Arthroscopy. 2011;27(2):252–269. [DOI] [PubMed] [Google Scholar]
- 17. Mehta MP, Swindell HW, Westermann RW, Rosneck JT, Lynch TS. Assessing the readability of online information about hip arthroscopy. Arthroscopy. 2018;34(7):2142–2149. [DOI] [PubMed] [Google Scholar]
- 18. Minkara AA, Westermann RW, Rosneck J, Lynch TS. Systematic review and meta-analysis of outcomes after hip arthroscopy in femoroacetabular impingement. Am J Sports Med. 2019;47(2):488–500. [DOI] [PubMed] [Google Scholar]
- 19. Montgomery SR, Ngo SS, Hobson T, et al. Trends and demographics in hip arthroscopy in the United States. Arthroscopy. 2013;29(4):661–665. [DOI] [PubMed] [Google Scholar]
- 20. Murray E, Lo B, Pollack L, et al. The impact of health information on the Internet on health care and the physician-patient relationship: national U.S. survey among 1.050 U.S. physicians. J Med Internet Res. 2003;5(3):e17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. O’Connor M, Minkara AA, Westermann RW, Rosneck J, Lynch TS. Return to play after hip arthroscopy: a systematic review and meta-analysis. Am J Sports Med. 2018;46(11):2780–2788. [DOI] [PubMed] [Google Scholar]
- 22. Pew RC. Social media fact sheet. Pew Research Center Information and Technology. Updated June 12, 2019. Accessed Accessed June 13, 2020. https://www.pewresearch.org/internet/fact-sheet/social-media/
- 23. Philippon MJ, Patterson DC, Briggs KK. Hip arthroscopy and femoroacetabular impingement in the pediatric patient. J Pediatr Orthop. 2013;33(suppl 1):S126–S130. [DOI] [PubMed] [Google Scholar]
- 24. Roberts H, Zhang D, Dyer GS. The readability of AAOS patient education materials: evaluating the progress since 2008. J Bone Joint Surg Am. 2016;98(17):e70. [DOI] [PubMed] [Google Scholar]
- 25. Sheppard ED, Hyde Z, Florence MN, et al. Improving the readability of online foot and ankle patient education materials. Foot Ankle Int. 2014;35(12):1282–1286. [DOI] [PubMed] [Google Scholar]
- 26. Tan SS, Goonawardene N. Internet health information seeking and the patient-physician relationship: a systematic review. J Med Internet Res. 2017;19(1):e9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Wiess BD. Health Literacy and Patient Safety: Help Patients Understand. Manual for Clinicians. 2nd ed. American Medical Association Foundation; 2007.