

Abstract
The Pharmaceuticals and Medical Devices Agency (PMDA) has approved hundreds of new drugs in recent years. We retrospectively analyzed the new drugs approved in Japan from 2008 to 2019, and identify the first‐in‐world approvals and clarify the current drug lag. The new drug and the drug lag were defined as a drug with a new active substance and a difference between the approval date in Japan and the international birth date, respectively. Among 400 new drugs approved in Japan during the last 12 years, 80 (20.0%) were first approved in Japan, and 320 were outside Japan (the United States: 202, 50.5%; Europe: 82, 20.5%; other regions: 36, 9.0%). Of these, 45 new drugs have not yet been approved outside Japan, and the remaining 355 have been globally approved in Japan and overseas. The number of new drug approvals were the largest in oncology followed by metabolic/endocrine and infectious diseases. The median drug lags (year) among all 400 new drugs and 355 new drugs with global approvals were 4.3 and 4.7 in the first tertile (2008–2011), 1.5 and 2.6 in the second tertile (2012–2015), and reduced to 1.3 and 2.2 in the third tertile (2016–2019), respectively. Substantial drug lag remains in neurology, psychiatry, and therapeutic areas where the number of new drug approvals was relatively small. Collectively, one‐fifth of the new drugs approved in Japan are first‐in‐world approvals. Drug lag has been greatly decreased, although it still exists.
Study Highlights.
WHAT IS THE CURRENT KNOWLEDGE ON THE TOPIC?
☑ Although new drug approvals in Japan have significantly lagged behind those in United States and Europe for decades, the Pharmaceuticals and Medical Devices Agency (PMDA) recently achieved marked reduction in the review period for new drug applications.
WHAT QUESTION DID THIS STUDY ADDRESS?
☑ Whether PMDA approvals are always behind the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA). How has the Japanese regulatory handled drug lag issues?
WHAT DOES THIS STUDY ADD TO OUR KNOWLEDGE?
☑ Japan has approved 400 drugs with new active substances between 2008 and 2019, and 20.0% of those approvals in Japan were first‐in‐world. Drug lag is greatly decreasing to date, and yet still exists, especially in neurology, psychiatry, and therapeutic areas where the number of new drug approvals was relatively small.
HOW MIGHT THIS CHANGE CLINICAL PHARMACOLOGY OR TRANSLATIONAL SCIENCE?
☑ There are significant disparities in accessibility to new drugs among therapeutic areas in Japan. Future collaboration with patients, academia, industries, and governments will be necessary to resolve the drug lag; that should be more focused on the therapeutic areas with a larger drug lag.
The Pharmaceuticals and Medical Devices Agency (PMDA) is the Japanese regulatory authority that protects the public health by securing safety, efficacy, and quality of drugs and medical devices. For a new drug approval, the PMDA conducts a scientific review on the product application according to the legislations in Japan, and after PMDA approval, Ministry of Health, Labor, and Welfare (MHLW) administratively grants the marketing authorization for the product based on the review report from the PMDA.
Acquiring the first‐in‐world approval for marketing authorization of new drugs yields several benefits in their own country, although such application often depends on the drug development strategy of manufactures. Early access to the latest treatment may improve the morbidity and mortality in patients with significant illness. Advancement of new drug development will bring social and economic profits. The medical review for new drug applications requires human resources, review quality, and trust of organization, and continuous improvement of those factors would increase in the activities and values of regulatory authority. However, there were even few reports reviewing new drug approvals in Japan and much less on those first approved in Japan ahead of the other countries.
Drug lag, the delay in time required for the drug approval, has been a critical issue of public health in Japan for many years. 1 , 2 Drug lag may not be always evil, 3 , 4 and the delay in approval may result in less frequent cautions after granting marketing authorization. 5 , 6 However, drug lag would preclude the chance of patients to use new drugs and the early access to effective treatment. Drug lag is consisted of the delay in development by manufacturers and that in review period by regulatory authority. 7 In this decade, the PMDA achieved marked reduction in the review period for new drug applications. In 2019, the median approval time for the new drugs in the PMDA, the US Food and Drug Administration (FDA), and the European Medicines Agency (EMA) were 304, 243, and 423 days, respectively. 8 Although the delay in regulatory review in Japan has almost been resolved, the persistence of drug lag in several specific therapeutic areas was recently pointed out, 9 , 10 and it has not been well examined on the status quo of drug lag in Japan.
The aim of this study was to conduct a high‐level overview on the new drugs approved in Japan, with a focus on the first‐in‐world approval, and address the changes and current issues of drug lag in Japan.
METHODS
Data sources, definitions, and analyses
We retrospectively investigated new drugs, which were defined as drugs containing new active substances (NASs), approved in Japan between 2008 and 2019. Data of the new drugs was obtained from our database. The definition of the NASs was described elsewhere. 8 Briefly, NAS included a new chemical, biological, biotechnology, or radiopharmaceutical substance that has not been previously available for therapeutic or diagnostic use in humans. The products with a small difference in molecular structure of the existing compound, such as isomers and salt modification, were included when their efficacy and safety properties differed from that substance previously being available. Vaccines, biosimilars, generic medicines, plant and insect extracts, re‐approved products, and new names, indications, doses, or combinations for existing compounds were all excluded in this study.
The first‐in‐world approval was determined by the international birth date (IBD), the date of first marketing authorization for a new drug in any country in the world, and the regions of the first‐in‐world approval were collected using the reports from manufacturers and literatures. We named the new drugs that Japan has granted first‐in‐world approvals were “Japan‐first” products, and those first approved outside Japan were “global‐first” products. The new drugs approved in Japan were classified into those with “global approval,” which have been approved in Japan and overseas, and those with “local approval,” which have not yet been approved outside Japan, and thus, the new drug with local approval was always a Japan‐first product in this study.
The number of the new drugs by year, the therapeutic areas, the nationality of the manufacturers, and the issuance of safety letters were analyzed between the new drugs with “global approval” and “local approval” and between “Japan‐first” and “global‐first” products. Therapeutic areas of the new drugs were determined based on the indication and pharmacological action. The frequency of postmarketing drug safety alerts, named “Yellow Letter (emergent communication)” and “Blue Letter (rapid communication),” and discontinuation from any cause were compared to evaluate one aspect of review quality by the PMDA.
The median drug lag (year), as the difference between the approval date in Japan and the IBD, was calculated among the all new drugs approved in Japan and the new drugs with global approvals. The drug lag of Japan‐first products is “zero.” To analyze the change of the median drug lag, an observation period of 12 years was divided into the first tertile (2008–2011), the second tertile (2012–2015), and the third tertile (2016–2019), and those in the second and third tertiles were compared with that in the first tertile as a reference. The changes of drug lag in each therapeutic area were also analyzed.
Statistical analyses
Student t‐test or Wilcoxon rank sum test was used as appropriate, and a P value of 5% was considered as significant. Analyses were performed using JMP 13.0.0 (SAS Institute, Cary, NC).
Ethical approval
Not required.
RESULTS
Between 2008 and 2019, a total of 400 drugs with NASs have been approved in Japan, in which 20.0% were first‐in‐world (Table 1 ). Among 400 new drugs, 202 (50.5%) were first approved in the United States, 82 (20.5%) were in Europe, 80 (20.0%) were in Japan, and 36 (9.0%) were in the other regions (Figure 1 ). The vast majority were the new drugs with global approvals, and 45 (11.3%) were those with local approvals as not yet approved outside Japan. Among 355 new drugs with global approvals, 9.9% were first approved in Japan. There was a difference in nationality of the manufacturers between the new drugs with global approvals and local approvals. The local approvals were mostly by the Japanese manufacturers, although 134 of 173 (77.5%) products by Japanese manufacturers achieved global approvals. The proportion of the Japanese manufacturers was high for the Japan‐first products (80.0%), and that of the non‐Japanese manufacturers were also high for the global‐first products (93.6%). For postmarketing alert for drug safety, the Blue Letters were provided for 9 (2.5%) products with global approvals and 1 (2.2%) with local approvals, and 2 (2.5%) of Japan‐first and 8 (2.5%) of global‐first products. No Yellow Letter has been published during the past 12 years. Discontinuation from any cause, including significant concern in efficacy or safety, expiration of approval, or manufacturer’s decision, were seen in 4 (1.1%) products with global approvals and 1 (2.2%) with a local approval, and 2 (2.5%) in Japan‐first and 3 (0.9%) of global‐first products. There was no specific trend in the number of new drugs by year for both new drugs with global approvals and local approvals (Figure 2 a,b).
Table 1.
Regions of the first regulatory approval in the world, nationality of the manufacturers, and issuance of safety letters among new drugs approved in Japan between 2008 and 2019
| All (n = 400) | Global approval (n = 355) | Local approval (n = 45) | |
|---|---|---|---|
| First‐in‐world approvals | |||
| Japan (Japan‐first) | 80 (20.0) | 35 (9.9) | 45 (100.0) |
| United States | 202 (50.5) | 202 (56.9) | ‐ |
| Europe | 82 (20.5) | 82 (23.1) | ‐ |
| Others | 36 (9.0) | 36 (10.1) | ‐ |
| Nationality of manufacturers | |||
| Japanese | 173 (43.3) | 134 (37.7) | 39 (86.7) |
| Non‐Japanese | 218 (54.5) | 213 (60.0) | 5 (11.1) |
| Mixed a | 9 (2.3) | 8 (2.3) | 1 (2.2) |
| Issuance of safety letters | |||
| Japan‐first | 2/80 (2.5) | 1/35 (2.9) | 1/45 (2.2) |
| Global‐first | 8/320 (2.5) | 8/320 (2.5) | ‐ |
| Discontinuations | |||
| Japan‐first | 2/80 (2.5) | 1/35 (2.9) | 1/45 (2.2) |
| Global‐first | 3/320 (0.9) | 3/320 (0.9) | ‐ |
Data are shown as the number of items or manufacturers (%). The percentage for first‐in‐world approvals and nationality of the manufacturers are calculated for each column. The percentage for issuance of safety letters and discontinuations are calculated for each line.
In case of drug development by a manufacture co‐funded by Japanese and non‐Japanese companies or by multiple manufactures including Japanese and non‐Japanese companies.
Figure 1.
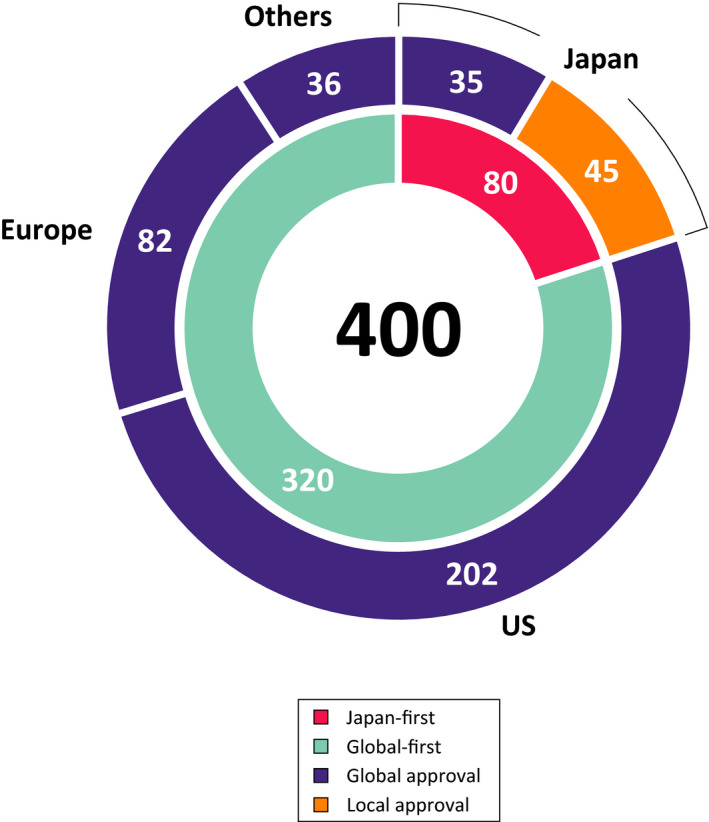
Regions of the first approval among new drugs approved in Japan between 2008 and 2019. Among 400 new drugs approved in Japan, 80 (20.0%) were first approved in Japan (Japan‐first, red), and 320 (80.0%) were outside Japan (global‐first, green). The number of first‐in‐world approvals were the largest in United States (202 items, 50.5%), followed by Europe (82 items, 20.5%), Japan, and the others regions (36 items, 9.0%). The Japan‐first drugs included 45 drugs that have not yet been approved in the other regions (local approval, orange). The remaining 355 drugs have been approved in Japan and overseas (global approval, purple).
Figure 2.
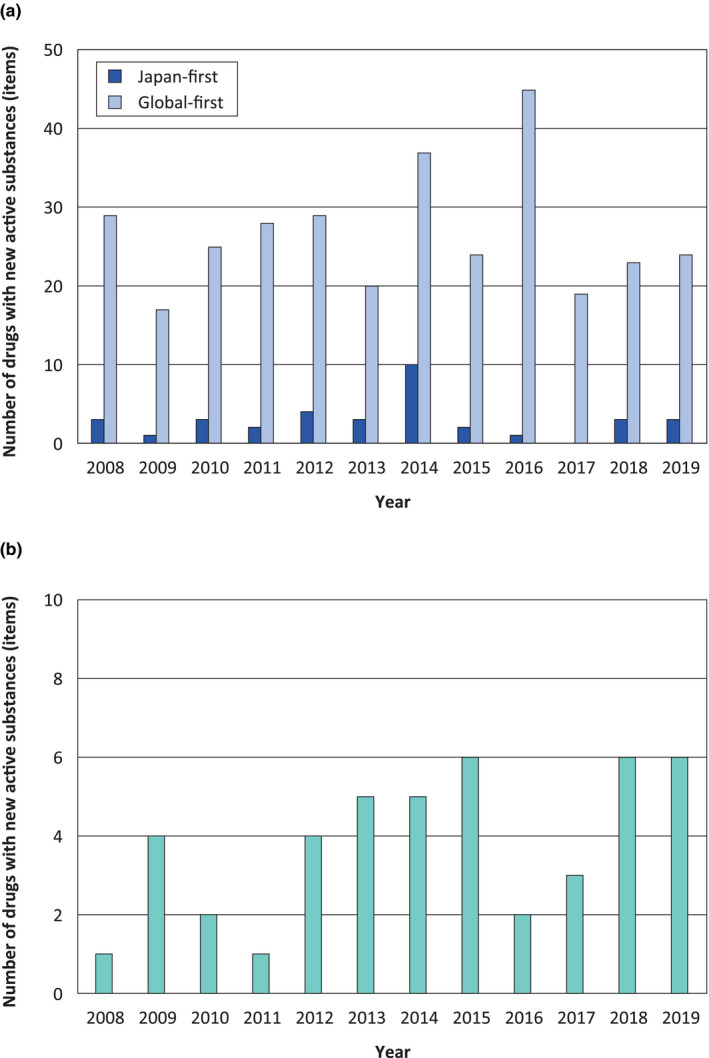
Change of the number of new drugs approved in Japan between 2008 and 2019. There was no specific trend in the number of new drugs with (a) global approvals and (b) local approvals. Dark and light blue bars indicate the number of Japan‐first and global‐first products with global approvals, respectively. Green bars indicate the number of new drugs with local approvals that is Japan‐first products.
Oncology, metabolic/endocrine, and infectious diseases were the top three active therapeutic areas for new drugs with global approvals (Figure 3a ). For new drugs with local approvals, infection, metabolic/endocrine, and oncology were the top three active therapeutic areas for drug development (Figure 3b ). Among the major therapeutic areas for new drugs (≥ 20 items in total), the proportion of Japan‐first was the largest in infectious diseases (17 items, 34.7%) followed by metabolic/endocrine (17 items, 27.9%), whereas those were very small in neurology (1 item, 3.4%) and psychiatry (1 item, 5.0%). The indication for new drugs in oncology varied widely, but many of those in metabolic/endocrine diseases were for diabetes (23 items) and osteoporosis (6 items), and those in infectious diseases were for infection with hepatitis virus C (13 items), bacteria (13 items), and human immunodeficiency virus (8 items).
Figure 3.
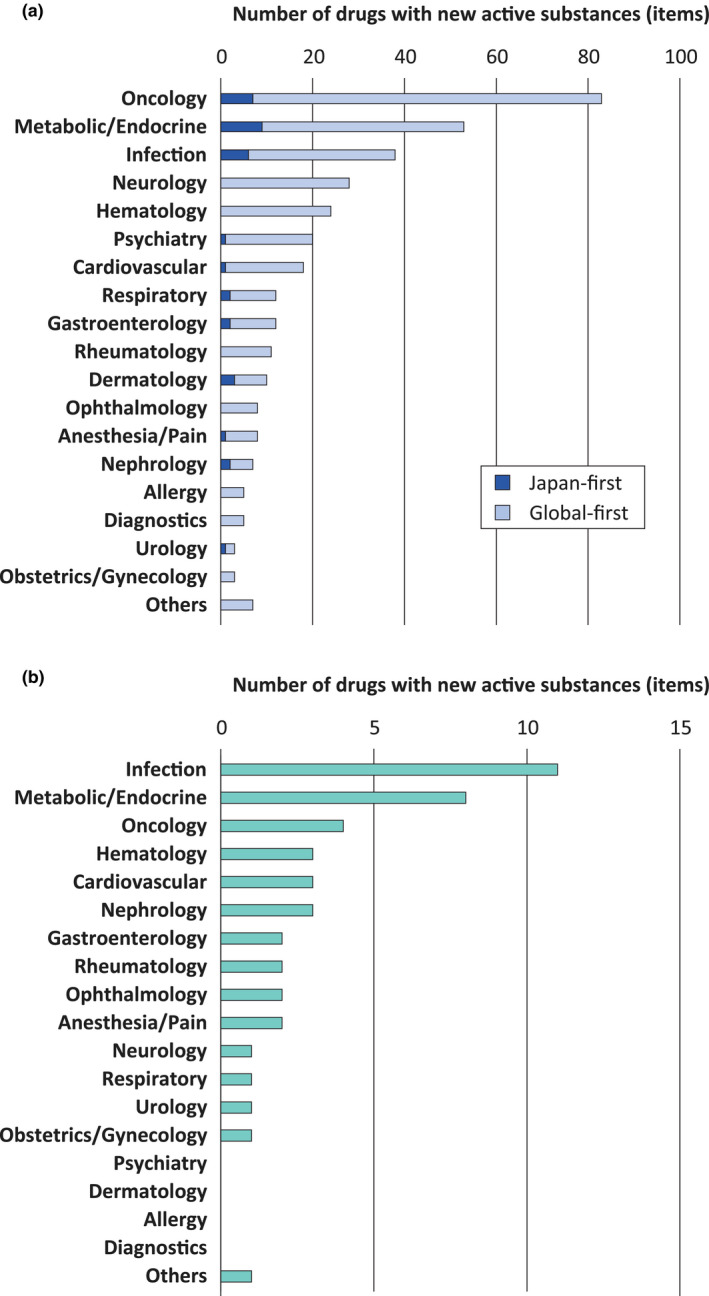
Therapeutic areas among new drugs approved in Japan between 2008 and 2019. Top three active therapeutic areas for new drugs with (a) global approvals and (b) local approvals were oncology, metabolic/endocrine, and infectious diseases, and infection, metabolic/endocrine, and oncology, respectively. Among those three major therapeutic areas, the number of Japan‐first products were relatively large. Among therapeutic areas with ≥ 20 items in total, the number of new drugs with local approvals was low in neurology and psychiatry. Dark and light blue bars indicate the number of Japan‐first and global‐first products with global approvals, respectively. Green bars indicate the number of new drugs with local approvals that is Japan‐first products.
The median drug lags, as the difference between the approval date in Japan and the IBD significantly decreased in the observation period (Figure 4 ). A 3‐year moving average of the median drug lag showed the decrease more clearly. The median drug lags among all new drugs and the new drugs with global approvals were 4.3 and 4.7 years in the first tertile (2008–2011), 1.5 and 2.6 years in the second tertile (2012–2015; P = 0.12 and 0.19, vs. first tertile), and reduced to 1.3 and 2.2 years in the third tertile (2016–2019; P < 0.01 and < 0.01, vs. first tertile), respectively.
Figure 4.
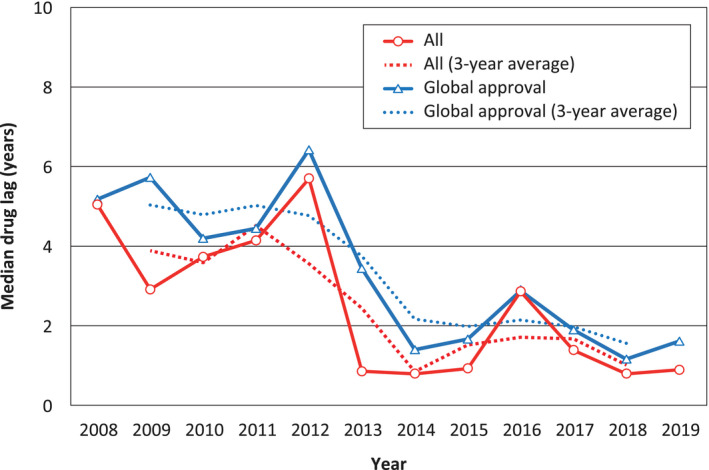
Drug lag among new drugs approved in Japan between 2008 and 2019. Shown are the median drug lag (year) for new drugs approved in Japan calculated on all new drugs (399 items, circles with a red line) and on the new drugs with global approvals (354 items, triangles with a blue line). The analysis of all new drugs is a sum of the new drugs with global approvals and local approvals, in which drug lag is zero for local approvals. A 3‐year moving average of the median drug lag (year) are shown as a dot line for each color. The median drug lag peaked in around 2011–2012, and continuously decreased since 2013. Benzoyl peroxide (Bepio) is excluded from the analysis due to no data are available on the international birth date.
The drug lags in several therapeutic areas were also likely decreasing in recent years (Figure 5 ). Among all new drugs, the therapeutic area where the lag was < 1 year was only infectious diseases in the first tertile, but those number increased in the second and third tertiles. The drug lag improved or maintained well in the therapeutic areas where the new drug development is active, such as oncology, metabolic/endocrine, and infectious diseases. On the contrary, the drug lag was the largest in neurology followed by psychiatry among the therapeutic areas with ≥ 20 items in 12 years. In addition, the drug lag seemed large in the therapeutic areas where the number of new drug approvals was relatively small.
Figure 5.
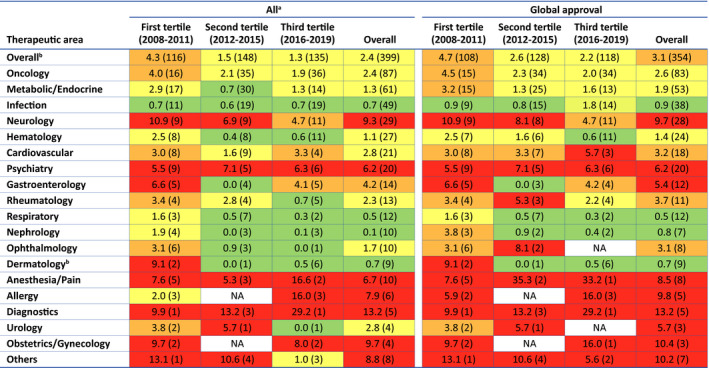
Change of drug lag in each therapeutic area among new drugs approved in Japan. Data are described as median years (number of items). Red, orange, yellow, and green cells indicate ≥ 5 years of drug lag, 3 years ≤ drug lag < 5 years, 1 year ≤ drug lag < 3 years, and < 1 year of drug lag, respectively. NA, not available. aSum of the new drugs with global approvals and local approvals, in which drug lag is zero for local approvals. bBenzoyl peroxide (Bepio) is excluded due to no data are a vailable on the international birth date.
DISCUSSION
Principal findings
The present study showed that Japan has granted first‐in‐world approvals in 20.0% of all new drugs approved in Japan during the last 12 years. Drug lag for the new drugs approved in Japan has decreased significantly in recent years, although there remains substantial delay in new drug approvals in Japan, especially in neurology, psychiatry, and therapeutic areas with low activities in drug development.
Findings of this study and comparison with other studies
There has been a criticism that the number of NASs that first‐in‐world approval by the PMDA is small, even though the review period was greatly reduced. 11 In fact, a previous report showed that < 10% of the new drugs were submitted to the PMDA before submission to the FDA and EMA between 2008 and 2014. 7 However, the present study revealed there were substantial new drugs that have not yet been approved outside Japan, and the proportion of first‐in‐world approvals in Japan was not exceedingly small in recent years. In addition, we have shown that Japan has approved 400 drugs with NASs between 2008 and 2019, and this number was comparable with those approved by the FDA (447 items) and EMA (335 items) in the same period (personal communication with the Centre for Innovation in Regulatory Science).
This study clarified that oncology, metabolic/endocrine, and infectious diseases are the most active areas for new drug development in Japan. This trend may be consistent with the recent new drug approvals in the FDA and EMA and other regulatory authorities. 8 The number of Japan‐first products were also the largest in these three therapeutic areas. They may commonly have a large number of patients with unmet needs for cure and significant discoveries of therapeutic targets and NASs in recent years, such as programmed cell death 1 or programmed cell death‐ligand 1 inhibitors in oncology, sodium glucose co‐transporter 2 inhibitors, glucagon‐like peptide‐1 receptor agonists, and dipeptidyl peptidase 4 inhibitors in diabetes, and anti‐hepatitis C virus drugs in infectious diseases. In addition, appropriate endpoints in clinical trials that are necessary for conducting the confirmatory clinical trials for the evaluation of efficacy and safety of drugs have been well‐established in these areas (e.g., overall survival, hemoglobin A1c, and time to improvement of infection).
Evaluation of the review quality may be a challenge for regulatory authorities. In this study, the frequency of postmarketing cautions for drug safety in the Japan‐first products were similar to that in the global‐first products. The cautions are provided when there are significant concerns for drug safety based on the postmarketing clinical trials, surveys, or real‐world evidence. The frequency of discontinued products for any cause also did not differ obviously between the groups. Although we did not collect all the revisions of drug labels in this study, the presented findings suggested that the medical review quality by the PMDA for new drugs first approved in Japan was as appropriate as those that have already been available other than in Japan.
This study showed that drug lag has been reduced but is persisting some in Japan. The median drug lag peaked in around 2011–2012 and has markedly decreased since 2013. The transient peak of drug lag should be the effect of the installation of the promotion program and committee for the development of unapproved or off‐label drugs that was launched in 2009 to address the issue of unapproved drugs or off‐label uses of drugs, which are approved in the other developed countries but not in Japan. Although this committee is still working, the drug lag is continuously decreasing to date, and this may be associated with the decrease in the review period by the infrastructural improvement of drug approval system, including huge increase in the reviewers in the PMDA (data not shown).
However, we found that the drug lag remains critical in neurology, psychiatry, and the therapeutic areas with a small number of new drug approvals. A previous study showed that drugs developed by domestic manufacturers have a significantly shorter delay in development than that by foreign manufacturers. 12 In this study, the number of new drugs with local approvals and the Japan‐first products was generally low in those therapeutic areas, which seemed to be consistent with the previous report. These findings suggested that Japanese industries have not been eager to develop new drugs in such areas, and those might be due to relatively weak research or academic activity, lack of strong financial support, and uncertainness of the development scenario in Japan. Furthermore, some specific causes may underlie the difficulties in the new drug development in neurology, psychiatry, and the therapeutic areas with a small number of new drug approvals. There are significant differences in the prevalence of diseases between Japan and Western countries; for example, the number of patients with multiple sclerosis, a major therapeutic target in the United States and Europe, in Japan has been reported only 10% of that in the United States. 13 The Dialysis Outcomes and Practice Patterns Study (DOPPS), a worldwide cohort study, revealed that the physician‐reported prevalence and the percentage of treated patients for depression was much lower in Japan than in 11 other DOPPS countries, 14 despite that the patient‐reported mental summary scores were similar among Japan, the United States, and Europe. 15 These findings suggested that there are stubborn ignorance, prejudice, and discrimination against patients with mental illness to be resolved in Japan, and those may result in an unattractive pharmaceutical market in psychiatry.
Regulatory perspectives and future challenges
Although drug lag has been discussed in Western countries since around 1980, 3 , 4 it was not a major public issue in Japan until the 2000s. 1 , 2 As described above, there is a view that drug lag is not always bad, however, we, as a regulatory review team, aim to minimize drug lag. The shortening of the review period for new drug applications, which the PMDA has set as a major goal in the last two decades, was to achieve a reduction in drug lag. The presented findings are of importance that overall drug lag has significantly decreased in the last 12 years. In the coming era, we believe that a therapeutic area‐focused support will be needed.
To improve the delay in development is still a critical issue in Japan. A recent report showed that Japan has the greatest submission gap in the six major regulatory authorities, including the PMDA, FDA, EMA, Health Canada, Swissmedic, and the Australian Therapeutic Goods Administration. 8 Japan has the third largest pharmaceutical market at the national level in the world that should be an attractive market for manufacturers. However, several factors may lead to the difficulty of conducting clinical trials in Japan, such as the difference in disease prevalence, language barrier, and the high cost of clinical trials in Japan. 1 , 2 , 16 The Japanese medical insurance system for the whole nation may also be a hurdle in patient recruitment to clinical trials. As this national health insurance allows people to access easily to approved drugs, many available treatments are already in use. Patients and physicians might be reluctant to participate in clinical trials and compare with placebo going so far as to discontinue the familiar ongoing treatments. Given the challenge of study participant recruitment, the public awareness on drug lag issue seems to be currently insufficient in Japan. This is a cliché, but education to public, patients, and physicians, cultivation of clinical trialists, and advancement of infrastructure are the keys to increase clinical trials in Japan.
As the Japanese regulatory authority, the PMDA generally requests to submit efficacy and safety data on Japanese populations for new drug applications. Requirement of additional clinical trials in Japan inevitably increase the delay in development for new drug applications in which the efficacy and safety data have been available in foreign countries. 17 In this point, multiregional clinical trials yielding Japanese participants may be useful for simultaneous global drug development and reducing the delay in development in Japan. 18 A previous report suggested that recent success for drug lag reduction may be associated with the increase in multiregional clinical trials in Japan. 17 In addition, in certain areas, a master protocol may also be useful to reduce the delay in development for new drugs, because it enables evaluation of multiple drugs from multiple companies. 19 The master protocol use indeed saved the time and costs in the development of new cancer drugs. 20 On the other hand, several differences in intrinsic and extrinsic ethnic factors, such as drug‐metabolizing enzymes and transporters and dietary habits, between Japanese and Western people are needed to be considered before planning multiregional clinical trials and determining the appropriate doses. 17 , 21 Collaboration among regulatory authorities and an increase in the affinity for drug applications would also be important to accelerate simultaneous global drug development and reducing the delay in development in Japan. 22 , 23 We believe that making a consensus with regulatory authorities on the appropriateness of clinical trial designs would be a solid path to new drug applications.
During the last two decades, several initiatives by collaboration with government, industry, and academia emerged to reduce the delay in development in Japan. To stimulate drug development further, the Japan Agency for Medical Research and Development (AMED) was established in 2015, aiming to concentrate funds and improving the clinical trial infrastructures. In addition, the SAKIGAKE system has been developed to enable the rapid drug application for serious diseases without effective treatment or for markedly effective drugs relative to the existing drugs. The effects of AMED and SAKIGAKE enterprises should be evaluated in the near future.
Patient and public involvement would also be essential for advancement of new drug development. The FDA is working on “patient‐focused drug development” to better incorporation of the patient’s voice in drug development and evaluation. 24 The EMA also respects patient’s involvements into regulatory decisions. 25 We, the PMDA, has launched the program for implementing patient‐focused and putting patient satisfaction as the highest priority. We found the drug lag is a continuing issue in specific therapeutic areas, and it can be considered that not only the systematic revision but also individual programs centered on patients, related academic societies, industries, and governments are necessary to improve such situations.
Regulatory science is often focusing on the estimation and prediction of safety and efficacy for the patient‐centered development drugs and medical devices. 26 , 27 Nevertheless, evaluation of the performance and review quality may be an approach of regulatory science in a broad sense. In this study, we listed the drugs with NASs approved in Japan in the last 12 years, revealed the proportion of the new drugs first approved in Japan prior to the other countries, compared the global developments with domestic developments, and found the change of the drug lag with certain improvement and some still need help. We hope this paper shall expedite to understand the current situation of the new drug approval in Japan and encourage future advancement and harmonization of regulatory science.
Strengths and limitations of this study
The study has following important strengths. First, the study was conducted based on the PMDA database for 12 years. Second, we focused on the IBD and analyzed the drug lag between Japan and overseas among the new drugs approved in Japan. Many drug lag studies have focused on its magnitude among two or three major regulatory authorities, including Japan, the United States, and Europe by comparing the approval date with each other. 1 , 2 , 12 , 16 , 28 , 29 , 30 This method seems suitable to detect the whole lag between specific regions but disregards the fact that there are many products first approved by the regulatory authorities other than those three. Finally, the methodology in this study to address the issues of drug lag in each therapeutic area may be generalizable in other regions and shall provide important findings for improving public health disparities and concerted collaboration with patients, academia, industries, and governments.
Despite these strengths, there are several limitations to be addressed in this study. First, our analyses were limited to the NASs approved in Japan, and drugs with new indications, doses, or combinations for existing compounds were not investigated. Therefore, our analyses disregarded that there are various diseases where drugs are usually introduced from the other diseases, such as immunosuppressive drugs for inflammatory bowel diseases are often developed as a new indication after approval for rheumatoid arthritis. Second, our analyses were the depictions based on the approval status at the end of 2019 so that some local approvals may change to global approvals in the future. Third, our approach could not identify the whole drug lag, including the drugs that are available in any countries in the world but not in Japan, however, our findings are likely compatible with the previous and recent drug lag studies. 1 , 2 , 8 , 12 , 16 Fourth, we could not calculate the delay in development, because it is difficult to define and measure the date of start of drug development in each manufacturer. 5 Although the submission gap has been used as an alternative measure of the delay in development, it is impossible to distinguish the gap is caused by the delay of the initiation of development or longer development periods. Further consideration is needed on the methodology for evaluating the lag of development.
CONCLUSION
The study showed that Japan‐first products accounted for one‐fifth of new drugs approved in Japan. First‐in‐world approval in Japan did not affect the frequency of the postmarketing safety issues. Although drug lag has been significantly decreased, there is still a substantial delay in accessibility to new drugs. Japan needs to challenge further improvement in drug lag resolution.
Conflict of Interest
The authors declared no competing interests for this work.
Funding
No funding was received for this study.
Author Contributions
M.T. and M. Ikuma wrote the manuscript. M.T. designed the research. M.T., M. Idei, H.S., R.K., D.S., K.S., S.K., T.H., A.Y., M.N., and M. Ikuma. performed the research. M.T. analyzed the data.
Acknowledgment
The authors thank the Centre for Innovation in Regulatory Science for valuable discussion on the definition and providing information on NASs approved by FDA and EMA. The views expressed in this article are those of the authors and do not necessarily reflect the official views of the PMDA.
[The copyright line for this article was changed on 23 December 2020 after original online publication].
References
- 1. Hirai, Y. , Kinoshita, H. , Kusama, M. , Yasuda, K. , Sugiyama, Y. & Ono, S. Delays in new drug applications in Japan and industrial R&D strategies. Clin. Pharmacol. Ther. 87, 212–218 (2010). [DOI] [PubMed] [Google Scholar]
- 2. Tsuji, K. & Tsutani, K. Approval of new drugs 1999–2007: comparison of the US, the EU and Japan situations. J. Clin. Pharm. Ther. 35, 289–301 (2010). [DOI] [PubMed] [Google Scholar]
- 3. Morgan, J.P. The drug lag: good or bad? J. Am. Pharm. Assoc. 17, 553–555 (1977). [DOI] [PubMed] [Google Scholar]
- 4. Drug lag bad: drug lack worse. Br. Med. J. 280, 670 (1980). [PMC free article] [PubMed] [Google Scholar]
- 5. Yamada, T. , Kusama, M. , Hirai, Y. , Arnold, F. , Sugiyama, Y. & Ono, S. Analysis of pharmaceutical safety‐related regulatory actions in Japan: do tradeoffs exist between safer drugs and launch delay? Ann. Pharmacother. 44, 1976–1985 (2010). [DOI] [PubMed] [Google Scholar]
- 6. Kikuchi, C. , Murakami, M. , Shimomura, H. , Shimada, S. & Aoyama, T. Influence of drug lag on new drug label revisions. Ther. Innov. Regul. Sci. 53, 138–145 (2019). [DOI] [PubMed] [Google Scholar]
- 7. Poirier, A.F. Closing the drug lag for new drug submission and review in Japan: An industry perspective. Clin. Pharmacol. Ther. 98, 486–488 (2015). [DOI] [PubMed] [Google Scholar]
- 8. Rodier, C. , Bujar, M. , McAuslane, N. , Liberti, L. & Munro, J. New drug approvals in six major authorities 2010–2019: focus on facilitated regulatory pathways and internationalisation. R&D Briefing 77, 1–24 (2020). [Google Scholar]
- 9. Maeda, H. & Kurokawa, T. Recent trends for drug lag in clinical development of oncology drugs in Japan: does the oncology drug lag still exist in Japan? Int. J. Clin. Oncol. 20, 1072–1080 (2015). [DOI] [PubMed] [Google Scholar]
- 10. Okabayashi, S. , Kobayashi, T. & Hibi, T. Drug lag for inflammatory bowel disease treatments in the east and west. Inflamm. Intest. Dis. 3, 25–31 (2018). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Downing, N.S. , Zhang, A.D. & Ross, J.S. Regulatory review of new therapeutic agents. N. Engl. J. Med. 376, 2598 (2017). [DOI] [PubMed] [Google Scholar]
- 12. Ueno, T. , Asahina, Y. , Tanaka, A. , Yamada, H. , Nakamura, M. & Uyama, Y. Significant differences in drug lag in clinical development among various strategies used for regulatory submissions in Japan. Clin. Pharmacol. Ther. 95, 533–541 (2014). [DOI] [PubMed] [Google Scholar]
- 13. Atlas of MS (MS International Federation) <https://www.atlasofms.org/map/global/epidemiology/number‐of‐people‐with‐ms> (2020). Accessed September 15, 2020.
- 14. Lopes, A.A. et al. Screening for depression in hemodialysis patients: associations with diagnosis, treatment, and outcomes in the DOPPS. Kidney Int. 66, 2047–2053 (2004). [DOI] [PubMed] [Google Scholar]
- 15. Fukuhara, S. et al. Health‐related quality of life among dialysis patients on three continents: the Dialysis Outcomes and Practice Patterns Study. Kidney Int. 64, 1903–1910 (2003). [DOI] [PubMed] [Google Scholar]
- 16. Shimazawa, R. & Ikeda, M. Japan lags behind the UK in neurological drug approvals. Br. J. Clin. Pharmacol. 71, 473–475 (2011). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Honig, P.K. Recent trends and success factors in reducing the lag time to approval of new drugs in Japan. Clin. Pharmacol. Ther. 95, 467–469 (2014). [DOI] [PubMed] [Google Scholar]
- 18. Asano, K. , Tanaka, A. , Sato, T. & Uyama, Y. Regulatory challenges in the review of data from global clinical trials: the PMDA perspective. Clin. Pharmacol. Ther. 94, 195–198 (2013). [DOI] [PubMed] [Google Scholar]
- 19. Woodcock, J. & LaVange, L.M. Master protocols to study multiple therapies, multiple diseases, or both. N. Engl. J. Med. 377, 62–70 (2017). [DOI] [PubMed] [Google Scholar]
- 20. Barker, A.D. , Sigman, C.C. , Kelloff, G.J. , Hylton, N.M. , Berry, D.A. & Esserman, L.J. I‐SPY 2: an adaptive breast cancer trial design in the setting of neoadjuvant chemotherapy. Clin. Pharmacol. Ther. 86, 97–100 (2009). [DOI] [PubMed] [Google Scholar]
- 21. Huang, S.M. & Temple, R. Is this the drug or dose for you? Impact and consideration of ethnic factors in global drug development, regulatory review, and clinical practice. Clin. Pharmacol. Ther. 84, 287–294 (2008). [DOI] [PubMed] [Google Scholar]
- 22. Kondo, H. , Saint‐Raymond, A. & Yasuda, N. What to know about medicines with new active ingredients approved in FY 2016 / 2016 in Japan and EU: a brief comparison of new medicines approved in Japan and the EU in 2016. Ther. Innov. Regul. Sci. 52, 214–219 (2018). [DOI] [PubMed] [Google Scholar]
- 23. Teixeira, T. , Kweder, S.L. & Saint‐Raymond, A. Are the European medicines agency, US food and drug administration, and other international regulators talking to each other? Clin. Pharmacol. Ther. 107, 507–513 (2020). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Chalasani, M. , Vaidya, P. & Mullin, T. Enhancing the incorporation of the patient's voice in drug development and evaluation. Res. Involv. Engagem. 4, 10 (2018). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Brown, P. & Bahri, P. 'Engagement' of patients and healthcare professionals in regulatory pharmacovigilance: establishing a conceptual and methodological framework. Eur. J. Clin. Pharmacol. 75, 1181–1192 (2019). [DOI] [PubMed] [Google Scholar]
- 26. Kondo, T. , Hayashi, Y. , Sato, J. , Sekine, S. , Hoshino, T. & Sato, D. Evolving vision of regulatory science in the global medical community. Clin. Pharmacol. Ther. 107, 136–139 (2020). [DOI] [PubMed] [Google Scholar]
- 27. van der Graaf, P.H. Are regulators talking to each other across borders? Clin. Pharmacol. Ther. 107, 481–483 (2020). [DOI] [PubMed] [Google Scholar]
- 28. Downing, N.S. , Zhang, A.D. & Ross, J.S. Regulatory review of new therapeutic agents ‐ FDA versus EMA, 2011–2015. N. Engl. J. Med. 376, 1386–1387 (2017). [DOI] [PubMed] [Google Scholar]
- 29. Kuhler, T.C. , Bujar, M. , McAuslane, N. & Liberti, L. To what degree are review outcomes aligned for new active substances (NASs) between the European Medicines Agency and the US Food and Drug Administration? A comparison based on publicly available information for NASs initially approved in the time period 2014 to 2016. BMJ Open 9, e028677 (2019). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Joppi, R. , Bertele, V. , Vannini, T. , Garattini, S. & Banzi, R. Food and Drug Administration vs European Medicines Agency: Review times and clinical evidence on novel drugs at the time of approval. Br. J. Clin. Pharmacol. 86, 170–174 (2020). [DOI] [PMC free article] [PubMed] [Google Scholar]