

Abstract
Aim
To provide a systematic review on studies examining problematic smartphone (PSU) use in children and adolescents, and its impact on quality of life, life satisfaction, and well‐being.
Methods
An extensive literature search was conducted in Google Scholar, Scopus and Pubmed.
Results
The search yielded k = 9 articles for which inclusion criteria were met. Five studies examined health‐related or overall quality of life, two assessed life satisfaction, and two evaluated well‐being in relation to PSU. Negative associations between PSU and the outcome variables were reported almost consistently, with one study yielding only a trend for a negative correlation of PSU with life satisfaction, and one study finding no significant correlation regarding quality of life. Comparability between studies was impeded by the scarcity of studies which met inclusion criteria and by the use of different measures.
Conclusion
More research is needed regarding PSU and the outcome variables in children and adolescents. Also, a distinct and consistent theoretical conceptualisation of PSU is required to replicate findings, and to enhance comparability between studies. Based on the trend reported here, the development of customised, early on interventions for children and adolescents at risk of PSU is warranted.
Keywords: adolescents, children, life satisfaction, quality of life, problematic smartphone use
Abbreviations
- HRQOL
Health related quality of life
- MPAS
Mobile Phone Addiction Scale
- MPPUS‐10
Mobile Phone Problem Use Scale
- QoL
Quality of life
- PSU
Problematic smartphone use
- SAPS
Smartphone Addiction Proneness Scale
- SAS – SV
Smartphone Addiction Scale–Short Version
- WHO
World Health Organization
Key Notes.
Given the increasing smartphone use in children and adolescents, this systematic review aimed to provide an overview over the impact of problematic smartphone use (PSU) on quality of life, life satisfaction and well‐being.
Nine studies met inclusion criteria, and most report a negative association between PSU and the outcome variables.
A consistent definition of PSU and well‐designed studies are needed for the development of early interventions.
1. INTRODUCTION
While prevalence rates of problematic smartphone use (PSU) in children and adolescents vary widely from 5% 1 to about 50%, 2 the overall number of smartphone owners has continuously increased worldwide. 3 Furthermore, the vulnerability in children and adolescents for PSU is assumed to be higher than in adults, 4 , 5 a fact that highlights the high relevance of the topic particularly in minors. Although research regarding risk factors for problematic smartphone use in children and adolescents remains somewhat inconclusive to date, a recent systematic review 6 has found female gender, strict parenting, low self‐esteem as well as gaming and social networking to serve as crucial predictors of PSU. Good friendships as well as academic motivation and success, in turn, may constitute protective factors.
In addition to risk factors, a growing body of reviews finds PSU (e.g. constantly checking for notifications or excessive usage 7 , 8 ) to be associated with negative consequences, 7 , 9 , 10 such as decreased sleep quality (in various age samples 10 , 11 ; in children/adolescents 12 and mental disorders like anxiety or depression 7 , 10 , 11 ). Mental disorders can also be linked to related constructs like problematic social networking site use. 13 , 14 In children and adolescents, excessive screen time in general also seems to be related to physical health effects (e.g. decreased sleep quality 15 , 16 ) and psychological health effects (e.g. depressive symptoms or ADHD 15 , 16 ).
Despite this wide array of findings, less studies or literature reviews can be found for the link between PSU and quality of life (QoL), health‐related quality of life (HRQOL), life satisfaction or well‐being in children and adolescents. Generally, data show that adolescents’ overall well‐being has started to decrease at the time smartphones became ubiquitous. 17 In line with this, PSU has been found to be negatively associated with psychological well‐being among university students 18 ; and greater life satisfaction in children and adolescents has—in turn—been linked to a combination of low screen time and high physical activity. 19
The theoretical concepts of QoL, HRQOL, life satisfaction and subjective well‐being are connected. QoL is defined by the World Health Organization (WHO) “as an individual's perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns” 20 , p. 1. HRQOL, in turn, includes the elements of overall quality of life that are particularly related to physical or mental health. 21 While one component of subjective well‐being covers positive and negative affect, 22 the second component, life satisfaction, is construed as a cognitive process in which a person globally evaluates his or her life. 23 Furthermore, psychological well‐being may be defined as the absence of symptoms of mental illness. 24
Despite the considerable body of literature on PSU, the underlying concept is defined quite broadly and at times—depending on the theoretical background of those proposing it—contradictorily. 7 , 9 To date, there is still no consensus on the question if excessive usage constitutes an addiction or if it should better be termed problematic usage (not meeting clinical criteria). On the one hand, symptoms commonly associated with addiction (e.g. overuse, withdrawal, daily‐life disturbance) have been observed in relation to problematic smartphone use, 25 leading some research groups to compare PSU to behavioural addictions like Internet gaming disorder. 4 , 8 , 26 On the other hand, some researchers conclude that evidence is not sufficient to assume the existence of smartphone addiction, 9 and hence, the term PSU is preferred over addiction. 27 In sum, according research is partly impeded by the use of inconclusive terminology as well as by different operationalisations of the concept and, thus, different measures. 6
Moreover, findings on how PSU affects QoL, well‐being or satisfaction with life in children and adolescents are still scarce. While there is some literature regarding the link between PSU and QoL/HRQOL or life satisfaction and well‐being, no review exists to date integrating studies explicitly examining PSU and these constructs in children and adolescents, particularly. This, however, would be of great practical relevance for the development of customised, early on interventions for afflicted minors. Thus, this systematic review aims to provide an overview over studies on the association between PSU and QoL, HRQOL, life satisfaction and well‐being in children and adolescents.
2. METHODS
2.1. Search strategy
The time frame of studies was set to begin after 2007, to increase the likelihood of studies examining smartphones instead of other mobile phones (i.e. without Internet access), as has been done by Elhai et al. 7 An extensive literature search was conducted in PubMed, Scopus and Google scholar regarding papers published between January 2008 and April 2020. Search parameters were PROBLEMATIC/MALADAPTIVE/EXCESSIVE/PATHOLOGICAL/DYSFUNCTIONAL in combination with SMARTPHONE/SMART PHONE/PHONE/CELLPHONE/CELL PHONE/MOBILE PHONE and ADDICTION/USE and ADOLESCENTS/CHILDREN/YOUTH as well as QUALITY OF LIFE/HEALTH RELATED QUALITY OF LIFE/LIFE SATISFACTION/WELL BEING. To ensure the inclusion of accepted articles and articles in preprint, Google Scholar alerts were enabled. Additionally, a reference search strategy was used to identify other relevant articles.
2.2. Study selection process
The authors independently examined the title, abstract and main text of each study, and at each stage of the process, studies were excluded (see Figure 1). Inclusion criteria covered original studies, which were published not earlier than 2008 in peer‐reviewed journals, which are written in English or German and focus on children and adolescents (1–20 years). The lower age limit was chosen to ensure inclusion of studies with very young children as there is a need to learn more about the impact of smartphone use particularly on young children. 6 The upper age limit corresponds to the observed circumstance that many studies on this subject include mixed age samples ranging from early puberty to late adolescence.
FIGURE 1.
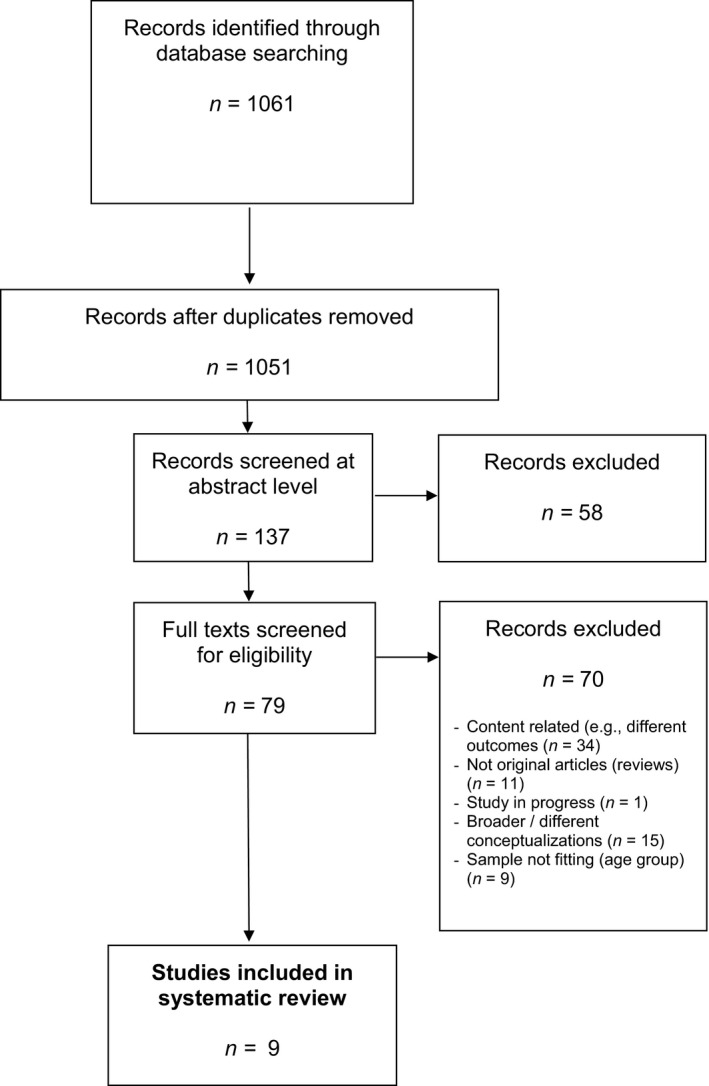
PRISMA flow diagram
Papers on university students were included if the sample's age fell into the mentioned age range. To increase comparability, articles not specifically referring to smartphones but instead to media/ technology use or screen time in general, as well as papers on the constructs of nomophobia (e.g. Ref. [28]), problematic Internet use, and problematic social networking services use were all excluded. Before reviewing full‐text articles, titles and abstracts were screened by all authors.
3. RESULTS
3.1. Sample of included studies
Overall, 1017 articles were found in the initial search process, and 44 were identified through reference search strategy. Of these, ten duplicates had to be removed. Subsequently, 1042 articles were excluded since they were not written in English or German, or did not constitute original articles, were not published in peer‐reviewed journals, or did not (exclusively) focus on children/adolescents. Also, articles, which focused on problematic Internet use, media / screen use in general, or problematic networking services use were excluded. Additionally, articles were only considered if the targeted outcome variables were explicitly assessed. Figure 1 provides a detailed description of the exclusion process.
The final sample amounted to k = 9 articles with overall n = 5928 participants. Of these, two (22.2%) were carried out in Italy and two (22.2%) in South Korea. The Philippines, Turkey, Indonesia, China and Switzerland were represented with one paper each in the review.
To measure PSU, 55.6% (k = 5) of the included studies used the Smartphone Addiction Scale–Short Version (SAS–SV), 25 while the Smartphone Addiction Proneness Scale (SAPS) 29 was applied in 22.2% (k = 2) of the studies. Finally, one study used the 10‐item version of the Mobile Phone Problem Use Scale (MPPUS‐10), 30 and another used the Mobile Phone Addiction Scale (MPAS). 31
In most of the included studies (k = 7, 77.8%), distribution of male and female participants was almost equal (50% ± 15%). One study, which compared two groups, had a higher amount of female participants (73.7%) in one of the groups, 32 while in another study the amount of male participants was 78.2%. 33 For an overview over the characteristics of included studies, see Table 1.
TABLE 1.
Characteristics and main results of included studies
| Study | Sample size | Age | Gender | Country | Measure PSU | Measure Outcome variable | Main results |
|---|---|---|---|---|---|---|---|
| Buctot et al., 2020 | N = 1447 |
M = 15.22 SD = 1.61; 13–18 years |
f = 59.9% m = 40.1% |
The Philippines | SAS‐SV | KIDSCREEN−27 |
|
|
Cha & Seo, 2018 |
N = 1824 | M = 15.6 SD =0.78 |
f = 49.0% m = 51.0% |
South Korea | SAPS | life satisfaction measured with one item |
|
| Kumcagiz, 2019 | N = 352 |
M = 16.26 SD = 2.00; 14–19 years |
f = 56.5% m = 43.5% |
Turkey | SAS‐SV | PedsQL |
|
| Kusuma et al., 2019 | N = 251 | 18–20 years |
f = 51.0% m = 49.0% |
Indonesia | SAPS | Scale of life satisfaction adopted from SWLS |
|
| Lu et al., 2018 |
1. N = 606 (Anhui province) 2. N = 705 (Qinghai province) |
1. M = 14.2 SD = 1.7 2. M = 15.9 SD = 1.7 |
1. f = 43.7% m = 56.3% 2. f = 48.2% m = 51.8% |
China | MPAS | WHOQOL‐BREF |
|
| Mascia et al., 2020 | N = 215 |
M = 12.7 SD = 0.90; 10–15 years |
f = 49.3% m = 50.7% |
Italy | SAS‐SV | My Life as a Student—questionnaire |
|
|
Roh et al., 2018 |
N = 78 |
M = 12.75 SD = 2.50; 7–17 years |
f = 21.8% m = 78.2% |
South Korea | SAS‐SV | PedsQL 4.0 |
|
| Roser et al., 2016 | N = 412 |
M = 14.0; 12–17 years |
f = 61.4% m = 38.6% |
Switzerland | MPPUS−10 | KIDSSCREEN−52 |
|
| Sarti et al., 2019 |
1. N = 19 (diagnosis of SLD group) 2. N = 19 (CNT group) |
1. M = 15.16 SD = 0.36 2. M = 15.42 SD = 0.77 |
1. f = 73.7% m = 26.3% 2. f = 52.6% m = 47.4% |
Italy | SAS‐SV | CIT |
|
N, sample size; M, mean; SD, standard deviation; f, female; m, male; CIT: Comprehensive Inventory of Thriving 54 ; CNT group: group of typically developing adolescents; KIDSCREEN‐27: Quality of Life Measure for Children and Adolescents 55 ; KIDSCREEN‐52: Quality of Life Measure for Children and Adolescents 39 ; MPAS: Mobile Phone Addiction Scale 31 ; MPPUS‐10: Mobile Phone Problem Use Scale–Short version 30 ; My Life as a Student—questionnaire 56 ; PedsQL: Pediatric Quality of Life Inventory 57 , 58 ; PSU = Problematic Smartphone Use; QoL, quality of Life; SLD group: group of adolescents with specific learning disability; SWLS: The Satisfaction With Life Scale 22 ; WHOQOL‐BREF: World Health Organization QOL—Brief Version 59 .
3.2. Outcomes
3.2.1. Overall QoL, HRQOL and well‐being
Three out of the total nine studies examined overall QoL, 33 , 34 , 35 two focused on HRQOL, 36 , 37 and two evaluated well‐being 32 , 38 in children and adolescents with PSU. Significant negative correlations were reported between PSU and QoL, 34 , 35 as well as between PSU and total HRQOL. 36 Overall lower QoL was also found to predict higher levels of PSU. 34
In addition to the overall constructs of QoL and HRQOL, PSU has also been found to be significantly negatively associated with several sub‐domains such as psychosocial health (i.e. emotional, social and school functioning)/QoL/well‐being, 34 , 35 , 36 , 37 physical health/QoL/well‐being, 34 , 35 , 36 social QoL (i.e. personal relationships, social support), 35 environmental QoL (i.e. freedom, physical safety, home environment) 35 and school environment (i.e. feelings about school), 36 , 37 moods and emotions (i.e. stress, depressive mood), 37 self‐perception (i.e. satisfaction with bodily appearance), 37 autonomy (i.e. the ability to organise their free time), 37 parent relations and home life (i.e. atmosphere at home, relationship with their parents), 37 as well as financial resources. 37
In the context of well‐being, PSU also seems to be associated with less perceived social support and with a decreased ability to understand and to resolve a problematic social situation. 32 Moreover, another study 38 found a significant moderation effect of PSU on the link between self‐regulation and well‐being, from which the authors conclude that a high level of smartphone addiction may weaken the effect of self‐regulation on well‐being. 38
No significant associations could be found regarding PSU and the HRQOL subscale peers and social support 36 , 37 (relationship with other adolescents), 39 and social acceptance 37 (e.g. bullying). 39 Somewhat contrary to the findings mentioned above, one study 33 yielded no significant correlation between PSU and overall QoL. In the study by Roser et al., 37 the association between PSU and physical well‐being was not significant in a more detailed analysis, whereas the study by Buctot et al. 36 found no significant correlation between PSU and autonomy and relationship with parents, thus yielding slightly different results from Roser et al. 37
3.2.2. Life satisfaction
Two 4 , 40 of the nine included studies examined life satisfaction in children and adolescents in the context of PSU, yielding slightly inconsistent results.
One of these studies 40 found a strong negative correlation between life satisfaction and the Smartphone Addiction Proneness Scale (SAPS) 29 in college students aged 18 to 20 years. 40 In contrast, the other study 4 which also used the SAPS in adolescents aged 15 years on average found no significant difference between the smartphone addiction risk group and the normal user group regarding life satisfaction. Yet, the authors reported a trend: the number of adolescents who indicated to be satisfied with their life was higher in the normal user group than in the risk group.
4. DISCUSSION
The aim of this systematic review was to assemble findings on the impact of PSU on QoL, HRQOL, life satisfaction, and well‐being in children and adolescents. Only few studies were found which explicitly examine these constructs in children and adolescents in the context of PSU: nine studies were included in this review, of which five examined overall QoL and/or HRQOL, two evaluated life satisfaction, and two assessed well‐being.
Despite the small number of included studies and despite the fact that different measures were applied, results tentatively suggest that PSU and the mentioned outcome variables are negatively associated. Hence, PSU seems to be accompanied by a lower QoL (both overall and health related) and by lower levels of life satisfaction. Also, PSU seems to influence well‐being, although this relationship does not seem to be a direct one. In both studies, which evaluated this link, 32 , 38 PSU acted as a moderating variable between self‐regulation and well‐being, and between social support and well‐being. These findings are in line with a study examining adults, which found PSU to be negatively related to psychological well‐being. 18
However, among the studies included in this review, two also yielded contradictory results regarding the main constructs. Roh et al. 33 did not find a significant correlation regarding QoL and PSU, and Cha and Seo 4 reported null findings concerning PSU and life satisfaction, although a trend towards a negative association was implied. The reason for these contradictory results may lie in methodological and sampling differences between the studies: In contrast with all other studies, which applied multiple‐item questionnaires, Cha and Seo 4 only used one item to measure life satisfaction. Whereas the participants of the other eight studies were acquired in schools or college, the study by Roh et al. 33 was conducted with children and adolescents visiting a hospital; also, it is the only one to include children under the age of 10 which might explain the contradictory results.
Taking a broader view on the examined constructs, the findings of the studies included in this review undoubtedly add to research in this field. Yet, further research is needed. More studies seem to define psychological well‐being as the absence of mental illnesses, 24 and therefore, measures of well‐being are replaced by measures of different constructs like attention and learning problems (e.g. Ref. [41]), depression, and loneliness (e.g. Ref. [42]), constructs, which certainly have an influence on subjective well‐being. However, one can assume that there is more to well‐being, life satisfaction, and QoL than the absence of physical or mental illnesses.
Besides the lack of studies, a few aspects have to be considered when interpreting the present results: first, the constructs of PSU measured in the included studies are not the same. Four different measures were applied across the nine studies, with the majority (8 studies) focusing on the construct of smartphone addiction. Only one construed excessive smartphone use as problematic usage. As has been pointed out above, it is still discussed among researches, if the problematic use of smartphones can be considered as an addiction or not (e.g. Ref. [9]), and the different conceptualisations of the construct found in this review reflect the still missing consensus among researchers. However, comparability between studies and progress in this field of research would be greatly enhanced if a clear definition of the phenomenon was available.
Second, as none of the included studies applied a longitudinal study design, no assumptions about causality can be made. One of the included studies 34 describes QoL as a predictor of higher PSU scores. A study concerning PSU and depressive symptoms found a bidirectional association between the two constructs. 43 On the other hand, most research seems to hypothesise that PSU is the predecessor to negative consequences. Clearly, more longitudinal studies are needed to shed more light on the direction of effects.
Third, although this review set out to summarise findings on PSU in children and adolescents, only one study covered children aged 7 years onwards. 33 All other studies focused exclusively on adolescents. Thus, almost no research on children below the age of 10 years is available. Although adolescents can be assumed to have greater access to smartphones, in recent years also children of the age of 6–10 show increasing smartphone usage rates. 44 Accordingly, younger samples should be included in future research. This would also be of relevance to start according interventions early on.
Of similar relevance would be a cultural comparison of the outcome variables in the context of PSU, which is not possible at this point in time due to the small number of according studies. Our findings show a surplus of studies from the Asiatic region. Only three of nine studies originate from countries with western‐oriented culture. Not only do the amount of smartphone users differ across different countries, 45 studies also suggest that the use of technology and its acceptance are influenced by cultural factors such as individualism vs. collectivism. 46 Cultural differences may also be assumed regarding the concept of QoL 47 and the other outcome variables, depending on which values are considered relevant to high QoL and life satisfaction in different cultures, like, for example, individualism, high achievement goals, or the social environment or family. In line with this reasoning, a study comparing adults from China and Germany found problematic Internet use to be negatively associated with life satisfaction in both samples, whereas a negative association between PSU and life satisfaction was only found in the Chinese sample. 48
Lastly, our review only focused on the global concept of PSU. However, research suggests that not the smartphone per se, but the usage of specific smartphone applications (i.e. social networking, games) is related to problematic usage patterns. For instance, some studies found evidence of social networking services use to be particularly responsible for problematic behaviours in adolescents. 5 , 49 , 50 , 51 Similarly, entertainment seeking 50 , 52 and gaming 50 , 51 , 52 have also been linked to PSU. Hence, it would be of interest to evaluate which aspects of PSU are especially relevant when looking at negative effects on QoL, life satisfaction and well‐being. Research regarding this particular issue is still scarce, although a study by Foerster and Röösli 53 on different types of media use found that high social media use was associated with the lowest scores in several aspects of HRQOL in adolescents.
All in all, results hint at a high relevance of future research regarding the topic of PSU in relation to QoL, life satisfaction and well‐being, especially in children and adolescents, because, as has been pointed out before, these are especially vulnerable with regard to PSU, 5 and early on interventions would be important. Next to longitudinal studies examining the direction of the association of PSU with QoL and life satisfaction, studies taking a closer look at which aspects of PSU are primarily related to QoL and life satisfaction would be of special interest.
4.1. Limitations and Conclusion
This systematic review provides an initial overview over the existing literature on the association between PSU and QoL, HRQOL, life satisfaction and well‐being in adolescents, and thus, contributes to a better understanding of these intricate relationships. However, the current work also has several limitations: one limitation is the small number of studies included in this review. Thus, nine studies cover four related, yet conceptually different outcome variables. Clearly, more research is needed, particularly with regard to the question of which aspects of PSU are related to which negative outcome.
Despite the limited number of studies, this review may tentatively state that PSU seems to be related to decreased health‐related and overall quality of life as well as life satisfaction, and subjective well‐being in adolescents. These findings highlight the relevance of future studies, especially with longitudinal research designs, to help parents, teachers, as well as adolescents to react quickly to an emerging PSU and to help health care professionals to develop effective interventions to increase QoL, satisfaction with life and well‐being in those afflicted by PSU.
CONFLICT OF INTEREST
None of the authors have any potential conflict of interest.
Funding information
No funding was provided.
REFERENCES
- 1. Lopez‐Fernandez O. 13. Problem Mobile Phone Use in Spanish and British Adolescents: first steps towards a cross‐cultural research in Europe. The psychology of social networking, Vol. 2. Sciendo Migration; 2015:186‐201. 10.1515/9783110473858-015 [DOI] [Google Scholar]
- 2. Yen CF, Tang TC, Yen JY, et al. Symptoms of problematic cellular phone use, functional impairment and its association with depression among adolescents in Southern Taiwan. J Adolescence. 2009;32(4):863‐873. [DOI] [PubMed] [Google Scholar]
- 3. Statista.com . Number of smartphone users worldwide from 2016 to 2021 (in billions). 2020. [cited 2020 May 24] Available from https://www.statista.com/statistics/330695/number‐of‐smartphone‐users‐worldwide/
- 4. Cha SS, Seo BK. Smartphone use and smartphone addiction in middle school students in Korea: prevalence, social networking service, and game use. Health Psychol Open. 2018;5(1):1‐15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Lee H, Seo MJ, Choi TY. The effect of home‐based daily journal writing in Korean adolescents with smartphone addiction. J Korean Med Sci. 2016;31(5):764‐769. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Fischer‐Grote L, Kothgassner OD, Felnhofer A. Risk factors for problematic smartphone use in children and adolescents: a review of existing literature. Neuropsychiatrie. 2019;1‐12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Elhai JD, Dvorak RD, Levine JC, Hall BJ. Problematic smartphone use: a conceptual overview and systematic review of relations with anxiety and depression psychopathology. J Affect Disorders. 2017;207:251‐259. [DOI] [PubMed] [Google Scholar]
- 8. Van Deursen AJ, Bolle CL, Hegner SM, Kommers PA. Modeling habitual and addictive smartphone behavior: the role of smartphone usage types, emotional intelligence, social stress, self‐regulation, age, and gender. Comput Hum Behave. 2015;45:411‐420. [Google Scholar]
- 9. Panova T, Carbonell X. Is smartphone addiction really an addiction? J Behav Addict. 2018;7(2):252‐259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Thomée S. Mobile phone use and mental health. A review of the research that takes a psychological perspective on exposure. Int J Environ Res Public Health. 2018;15(12):1‐25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Yang J, Fu X, Liao X, Li Y. Association of problematic smartphone use with poor sleep quality, depression, and anxiety: a systematic review and meta‐analysis. Psychiatry Res. 2019;284:112686. [DOI] [PubMed] [Google Scholar]
- 12. Mac Cárthaigh S, Griffin C, Perry J. The relationship between sleep and problematic smartphone use among adolescents: a systematic review. Dev Rev. 2020;55:100897. [Google Scholar]
- 13. Hussain Z, Griffiths MD. Problematic social networking site use and comorbid psychiatric disorders: a systematic review of recent large‐scale studies. Front Psychiatry. 2018;9(686):1‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Marino C, Gini G, Vieno A, Spada MM. The associations between problematic Facebook use, psychological distress and well‐being among adolescents and young adults: a systematic review and meta‐analysis. J Affect Disord. 2018;226:274‐281. [DOI] [PubMed] [Google Scholar]
- 15. Lissak G. Adverse physiological and psychological effects of screen time on children and adolescents: literature review and case study. Environ Res. 2018;164:149‐157. [DOI] [PubMed] [Google Scholar]
- 16. Martin A, Pugmire J, Wells V, Riddell J, McMellon C, Skivington K, et al. Systematic literature review of the relationship between adolescents’ screen time, sleep and mental health. 2020. [cited 2020 May 24] Available from https://dera.ioe.ac.uk/35074/1/systematic‐literature‐review‐relationship‐between‐adolescents‐screen‐time‐sleep‐mental‐health.pdf
- 17. Twenge JM, Martin GN, Campbell WK. Decreases in psychological well‐being among American adolescents after 2012 and links to screen time during the rise of smartphone technology. Emotion. 2018;18(6):765‐780. [DOI] [PubMed] [Google Scholar]
- 18. Tangmunkongvorakul A, Musumari PM, Thongpibul K, et al. Association of excessive smartphone use with psychological well‐being among university students in Chiang Mai, Thailand. PloS one. 2019;14(1):1‐13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Matin N, Kelishadi R, Heshmat R, et al. Joint association of screen time and physical activity on self‐rated health and life satisfaction in children and adolescents: the CASPIAN‐IV study. Int Health. 2017;9(1):58‐68. [DOI] [PubMed] [Google Scholar]
- 20. WHO . Health Statistics and Information Systems. HOQOL: Measuring Quality of Life. 2020. [cited 2020 May 24] Available from https://www.who.int/healthinfo/survey/whoqol‐qualityoflife/en/ [Google Scholar]
- 21. Centers for Disease Control and Prevention . Measuring healthy days: Population assessment of health‐related quality of life. Atlanta: CDC; 2000:4‐6. [Google Scholar]
- 22. Diener E, Emmons RA. The independence of positive and negative affect. J Pers Soc Psychol. 1984;47(5):1105‐1117. [DOI] [PubMed] [Google Scholar]
- 23. Diener ED, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale. J Pers Assess. 1985;49(1):71‐75. [DOI] [PubMed] [Google Scholar]
- 24. Ryff CD. Psychological well‐being in adult life. Curr Dir Psychol Sci. 1995;4(4):99‐104. [Google Scholar]
- 25. Kwon M, Kim DJ, Cho H, Yang S. The smartphone addiction scale: development and validation of a short version for adolescents. PLoS One. 2013;8(12):1‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Demirci K, Orhan H, Demirdas A, Akpinar A, Sert H. Validity and reliability of the Turkish Version of the Smartphone Addiction Scale in a younger population. Klinik Psikofarmakoloji Bülteni‐Bulletin Clin Psychopharmacol. 2014;24(3):226‐234. [Google Scholar]
- 27. Billieux J, Philippot P, Schmid C, Maurage P, De Mol J, Van der Linden M. Is dysfunctional use of the mobile phone a behavioural addiction? confronting symptom‐based versus process‐based approaches. Clin Psychol Psychother. 2015;22(5):460‐468. [DOI] [PubMed] [Google Scholar]
- 28. Gezgin DM, Çakır Ö. Analysis of nomofobic behaviors of adolescents regarding various factors. J Hum Sci. 2016;13(2):2504‐2519. [Google Scholar]
- 29. Kim D, Lee Y, Lee J, Nam JK, Chung Y. Development of Korean smartphone addiction proneness scale for youth. PLoS One. 2014;9(5):1‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Foerster M, Roser K, Schoeni A, Röösli M. Problematic mobile phone use in adolescents: derivation of a short scale MPPUS‐10. Int J Public Health. 2015;60(2):277‐286. [DOI] [PubMed] [Google Scholar]
- 31. Hong FY, Chiu SI, Huang DH. A model of the relationship between psychological characteristics, mobile phone addiction and use of mobile phones by Taiwanese university female students. Comput Human Behav. 2012;28(6):2152‐2159. [Google Scholar]
- 32. Sarti D, Bettoni R, Offredi I, et al. Tell me a story: socio‐emotional functioning, well‐being and problematic smartphone use in adolescents with specific learning disabilities. Front Psychol. 2019;10:1‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Roh D, Bhang SY, Choi JS, Kweon YS, Lee SK, Potenza MN. The validation of Implicit Association Test measures for smartphone and Internet addiction in at‐risk children and adolescents. J Behav Addict. 2018;7(1):79‐87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Kumcagiz H. Quality of life as a predictor of smartphone addiction risk among adolescents. Technology, Knowledge and Learning. 2019;24(1):117‐127. [Google Scholar]
- 35. Lu LI, Xu D‐D, Liu H‐Z, et al. Mobile phone addiction in tibetan and han chinese adolescents. Perspect Psychiatr Care. 2018:55(3):438‐444. [DOI] [PubMed] [Google Scholar]
- 36. Buctot DB, Kim N, Kim JJ. Factors Associated with Smartphone Addiction Prevalence and its Predictive Capacity for Health‐Related Quality of Life among Filipino Adolescents. Child Youth Serv Rev. 2020;104758:1‐12. [Google Scholar]
- 37. Roser K, Schoeni A, Foerster M, Röösli M. Problematic mobile phone use of Swiss adolescents: is it linked with mental health or behaviour? Int J Public Health. 2016;61(3):307‐315. [DOI] [PubMed] [Google Scholar]
- 38. Mascia ML, Agus M, Penna MP. Emotional intelligence, self‐regulation, smartphone addiction: which relationship with student well‐being and quality of life? Front Psychol. 2020;11(375):1‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Ravens‐Sieberer U, Gosch A, Rajmil L, et al. The KIDSCREEN‐52 quality of life measure for children and adolescents: psychometric results from a cross‐cultural survey in 13 European countries. Value Health. 2008;11:645‐658. [DOI] [PubMed] [Google Scholar]
- 40. Kusuma JF, Sahede I, Sunaryo AT, Fahmi AZ, Nurtjahjo FE. Smartphone Addiction and Life Satisfaction among College Students [cited 2020 May 24]. 14th International Conference on Language, Innovation, Culture and Education (ICLICE) & 3rd International Research Conference on Management, Leadership & Social Sciences (IRCMALS) 2019. Seoul, South Korea. 2019. https://icsai.org/procarch/14iclice3ircmals/14ICLICE‐025‐019.pdf
- 41. Tariq K, Tariq R, Ayesha AH, Shahid M. Effects of smartphone usage on psychological wellbeing of school going children in Lahore, Pakistan. JPMA. J Pak Med Assoc. 2019;69(7):955‐958. [PubMed] [Google Scholar]
- 42. Lapierre MA, Zhao P, Custer BE. Short‐term longitudinal relationships between smartphone use/dependency and psychological well‐being among late adolescents. J Adolescent Health. 2019;65(5):607‐612. [DOI] [PubMed] [Google Scholar]
- 43. Jun S. The reciprocal longitudinal relationships between mobile phone addiction and depressive symptoms among Korean adolescents. Comput Human Behav. 2016;58:179‐186. [Google Scholar]
- 44. Bitkom Research . Kinder und Jugend in der digitalen Welt. 2020. [cited 2020 May 24] Available from https://www.bitkom.org/sites/default/files/file/import/170512‐Bitkom‐PK‐Kinder‐und‐Jugend‐2017.pdf
- 45. Pew Research Center . Smartphone ownership and internet usage continues to climb in emerging economies. 2016. [cited 2020 May 24] Available from http://www.pewglobal.org/2016/02/22/smartphone‐ownership‐and‐internet‐usage‐continues‐to‐climb‐in‐emerging‐economies/
- 46. Nath R, Murthy NR. A study of the relationship between Internet diffusion and culture. Journal of International Information Management. 2004;13(2):5. [Google Scholar]
- 47. Hofstede G. The cultural relativity of the quality of life concept. Acad Manage Rev. 1984;9(3):389‐398. [Google Scholar]
- 48. Lachmann B, Sindermann C, Sariyska RY, et al. The role of empathy and life satisfaction in internet and smartphone use disorder. Front Psychol. 2018;9(398):1‐11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Haug S, Castro RP, Kwon M, Filler A, Kowatsch T, Schaub MP. Smartphone use and smartphone addiction among young people in Switzerland. J Behav Addict. 2015;4(4):299‐307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Jeong SH, Kim H, Yum JY, Hwang Y. What type of content are smartphone users addicted to? SNS vs. games. Comput Hum Behav. 2016;54:10–17. [Google Scholar]
- 51. Lee SJ, Lee C, Lee C. Smartphone addiction and application usage in Korean adolescents: effects of mediation strategies. Soc Behav Personal. 2016;44(9):1525‐1534. [Google Scholar]
- 52. Bae SM. The relationship between the type of smartphone use and smartphone dependence of Korean adolescents: National survey study. Child Youth Serv Rev. 2017;81:207‐211. [Google Scholar]
- 53. Foerster M, Röösli M. A latent class analysis on adolescents media use and associations with health related quality of life. Comput Hum Behav. 2017;71:266‐274. [Google Scholar]
- 54. Su R, Tay L, Diener E. The development and validation of the Comprehensive Inventory of Thriving (CIT) and the Brief Inventory of Thriving (BIT). Appl Psychol Health Well Being. 2014;6(3):251‐279. [DOI] [PubMed] [Google Scholar]
- 55. Ravens‐Sieberer U, Auquier P, Erhart M, et al. The KIDSCREEN‐27 quality of life measure for children and adolescents: psychometric results from a cross‐cultural survey in 13 European countries. Qual Life Res. 2007;16(8):1347‐1356. [DOI] [PubMed] [Google Scholar]
- 56. Soresi S, Nota L. La mia vita da Studente. Firenze: ITER–Institute of Training Education and Research; 2003. [Google Scholar]
- 57. Varni JW, Seid M, Rode CA. The PedsQL™: measurement model for the pediatric quality of life inventory. Med Care. 1999;126‐139. [DOI] [PubMed] [Google Scholar]
- 58. Varni JW, Seid M, PedsQL KPS. PedsQL™ 4.0: reliability and validity of the pediatric quality of life inventory™ version 4.0 generic core scales in healthy and patient populations. Medical Care. 2001;39(8):800–812. [DOI] [PubMed] [Google Scholar]
- 59. Whoqol Group . Development of the World Health Organization WHOQOL‐BREF quality of life assessment. Psychol Med. 1998;28(3):551‐558. [DOI] [PubMed] [Google Scholar]