

Abstract
Objectives
Behavioural and lifestyle factors, as oral hygiene and diet, are well‐established risk factors in the pathogenesis of dental caries, though displaying large differences in susceptibility across individuals. Since enamel formation already starts in utero, pregnancy course and outcome may eventually play a role in enamel strength and caries susceptibility. Therefore, we studied the association between history of pregnancy complications and the caries experience in their six‐year‐old children. The pregnancy complications included small for gestational age (SGA), spontaneous preterm birth (sPTB), gestational hypertension (GH), pre‐eclampsia (PE), individually, and a combination of those, designated as placental syndrome.
Methods
This study was embedded in Generation R, a prospective longitudinal Dutch multiethnic pregnancy cohort study. Information about pregnancy complications was obtained from questionnaires completed by midwives and obstetricians with cross‐validation in medical records. These included SGA, sPTB, GH and PE. Caries experience was assessed with the decayed, missing and filled teeth (dmft) index at a mean age of six years. The association between dental caries experience and a history of pregnancy complications was studied by using hurdle negative binomial (HNB) models.
Results
We were able to assess the dmft index in 5323 six‐year‐old children (mean age 6.2 years, SD 0.5). We did not find an association between the different pregnancy complications and dental caries experience in childhood, whether for SGA, sPTB, GH, PE, or for the combined outcome placental syndrome (HNB estimates: OR 1.02, 95%CI 0.87 ‐ 1.19; RR 0.90, 95%CI 0.78 ‐ 1.04). Further adjustment of the models with different confounders did not alter the outcome.
Conclusions
Although it is expected that prenatal stress can be a risk factor for caries development later in life, our findings do not support this hypothesis. Therefore, we believe disparities in caries experience between children are probably not explained by early life events during a critical intrauterine period of development.
Keywords: dental caries, epidemiology, paediatric dentistry, pregnancy complications
1. INTRODUCTION
Dental caries is one of the most common chronic diseases in both children and adults. 1 Behavioural and lifestyle factors, as oral hygiene and diet, are well‐established risk factors in its pathogenesis, though there are differences in susceptibility among individuals. 2 Differences in enamel strength might partly explain these disparities. It is known that children with evident hypomineralized and/or hypoplastic enamel are more prone to caries. 3 , 4 Still, subtle differences in enamel hardness might influence caries susceptibility.
Pregnancy course and outcome are important for the health and well‐being of the offspring. During conception and pregnancy, complex interaction between maternal and environmental factors influences how foetal and childhood growth and development are programmed; this is known as the Developmental Origin of Health and Disease (DOHaD) paradigm. 5 Moreover, amelogenesis starts in utero and is influenced by maternal and environmental factors. 6 The formation of a physiological phenomenon within the enamel of primary teeth, the neonatal line (NNL), is attributed to environmental and nutritional changes for a newborn. 7 The NNL resembles the moment of birth and its width seems to be dependent of the kind and duration of delivery. 8 , 9 Laboratory research has shown that this line consists of smaller enamel prisms and is less mineralized than surrounding enamel. 10
A similar phenomenon in the dental enamel is found, manifesting as Wilson bands or accentuated striae of Retzius. 11 Unlike the NNL, the presence of Wilson bands is associated with nonspecific stressors (eg neonatal asphyxia, intrauterine undernutrition, maternal diabetes) and not with the moment of birth. 11 , 12 The physiological mechanism behind the formation is unclear, but these enamel disturbances have been temporally associated with past stressors due to the incremental growth of enamel. 13
Ameloblasts are a vulnerable group of cells that can be affected by nonspecific internal or external stressors during intrauterine life. 7 This means that prenatal stress might result in a hypomineralized or more caries‐susceptible dental enamel. 14 , 15 This follows the so‐called ‘critical period model’, but other models explaining the possible association between pregnancy complications and dental caries have also been proposed in life‐course epidemiology. 16 Although a positive relationship between pregnancy complications and dental caries has been shown in different studies, the evidence remains inconclusive. 17 , 18 , 19 , 20 , 21 , 22
Four of the most common pregnancy complications are related to placental insufficiency (placental syndrome): a newborn small for gestational age; spontaneous preterm birth; gestational hypertension; and pre‐eclampsia. We hypothesized that placental insufficiency negatively affects the ameloblasts in the tooth germs. This may lead to dental enamel disturbances and greater caries susceptibility in children born from such pregnancies. In this study, we assessed the association between pregnancy complications and caries experience in the deciduous dentition of six‐year‐old children.
2. METHODS
2.1. Study design and sample
This study was embedded in the birth cohort Generation R; a prospective cohort study from foetal life until young adulthood in the city of Rotterdam, the Netherlands. Generation R aims to identify early environmental and genetic determinants of growth, development and health. 23 We received approval for this study by the Medical Ethics Committee of the Erasmus Medical Centre, Rotterdam, the Netherlands (MEC‐2007‐413). All participants gave written informed consent. In total, 9778 women were included in the study, of whom 8880 (90.1%) were included before pregnancy. They gave birth to 9745 live‐born children in total. Of those, 6690 children (68.7%) visited the research centre at the age of six, and caries experience was assessed in 5323 children (54.6%) (Figure 1).
Figure 1.
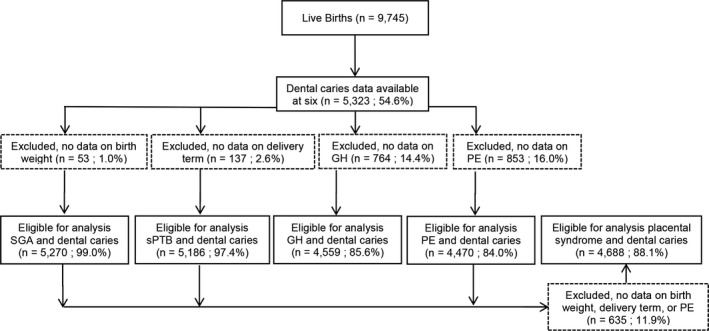
Flowchart of participants
2.2. Pregnancy complications
Information about pregnancy complications was obtained from questionnaires filled in by midwives and obstetricians with cross‐validation in medical records. 24 A child was small for gestational age if their birthweight was below the 10th percentile of their respective reference curve. 25 Spontaneous preterm birth was defined as the spontaneous onset of delivery before 37 weeks of gestation and gestational hypertension as new onset hypertension (systolic blood pressure ≥ 140 mm Hg and/or diastolic blood pressure ≥ 90 mm Hg) after 20 weeks of gestation. A mother had pre‐eclampsia if she suffered from gestational hypertension plus the concurrent presence of proteinuria (≥0.3 g of protein in a 24‐hour urine specimen, ≥2+ [1g/L] from a voided specimen, or ≥ 1+ [0.3g/L] from a catheterized specimen) according to international criteria that were in effect at time of inclusion. 26 , 27 Diagnosis of placental syndrome was based upon the presence of one or more of the abovementioned pregnancy complications. 28
2.3. Dental caries
We took intra‐oral photographs of all children who visited the research centre at the age of six years. Those photographs were taken either with the Poscam USB intra‐oral (Digital Leader PointNix) or with the Sopro 717 (Acteon) autofocus camera. The complete dentition was captured in ten intra‐oral photographs on average taken from the occlusal, buccal, palatal and lingual side of the teeth with a maximal scene illumination of 30 lux. Trained employees and PhD students took the photographs of brushed and dried (with a cotton wool roll) teeth. Since the teeth were only dried by cotton wool rolls and not with air, the minimal level of caries, we were able to assess was a ‘international caries detection and assessment system’‐score of two. Afterwards, all photographs were assessed for dental caries by using the decayed, missing and filled teeth (dmft) index by one examiner who was a paediatric dentist in training. Using this method to evaluate caries in children is a valid and reliable method, as shown by Elfrink et al. 29 Within our cohort, the intra‐ (10% of all photographs were re‐assessed by the same examiner after six weeks) and inter‐observer reliability (10% of all photographs were re‐assessed by a second paediatric dentist), for scoring dental caries on intra‐oral photographs and compared to clinical examination reached a perfect and an almost perfect agreement (quadratic weighted Cohen's kappa = 0.98, and kappa = 0.89 respectively). 30
2.4. Covariates
All included covariates were chosen based on the previous literature. 26 , 30 Height and weight of the mother were measured at intake and were used to calculate the Body Mass Index (BMI, kg/m2). Hence, most women had their BMI measured prenatally, but some were measured postnatally or during the first trimester of pregnancy when not much weight gain was expected. Information on other covariates (including ethnicity, maternal educational level, parity, breastfeeding, smoking) was obtained by using a postnatal questionnaire. The ethnicity of the child was based on the ethnicity of both parents, where the mother's ethnicity was used if both parents were born outside the Netherlands (Western or non‐Western). At the child's age of six, the mothers were asked about their educational level (high, mid‐high, mid‐low and low). At enrolment, we asked about the number of children they already had (nullipara or primipara/multipara). We also asked whether they breastfed the participating child (six months exclusive breastfeeding, four months exclusive breastfeeding, four months partially breastfeeding, or never) and about the mothers’ smoking habits (never, smoked until pregnancy was known, or continued smoking during pregnancy). When the children were six years of age, we asked about their oral health behaviour, including their age at first dental visit (0‐3 years, >3 years, or never), toothbrushing frequency (twice or more per day, or once per day), and whether they had visited the dentist in the previous year (yes or no).
2.5. Statistical analyses
Descriptive characteristics were summarized as means and standard deviations (SDs) for continuous variables. For categorical variables, we calculated absolute numbers with their corresponding percentages. These calculations used the Statistical Package of Social Sciences version 21.0 for Windows (IBM Corp).
We used hurdle models to study the association between pregnancy complications and dental caries at the age of six years. Dmft data have generally strongly positive skewed distributions with a large stack of zero counts. Hurdle models overcome this problem, and moreover, they avoid the loss of information due to categorization of the outcome variable for binomial logistic regression. 31 The output of a hurdle model consists of two parts: the zero hurdle part and the count hurdle part. Consequently, each predictor in the model has two coefficients. The exponent of the coefficients can be interpreted as Odds Ratios (ORs) in the zero hurdle part and as Risk Ratios (RRs) in the count hurdle part. We studied the association between the pregnancy complications and dental caries in three different models, adding covariates to each consecutive model. In model 1, we adjusted for the child's age and sex. In model 2, variables related to oral health behaviour variables were added. Finally, we adjusted for maternal educational level, smoking during pregnancy, child's ethnicity, parity, breastfeeding, age of mother at intake and mother's BMI at intake.
For modelling, we used of the statistical software R version 3.4.1 for Windows (R core team, Vienna, Austria). Within R, we used the hurdle() function of the ‘pscl’‐package. 32 For the count part of the model, we fitted both a Poisson distribution and a negative binomial distribution for all first models. Afterwards, we chose the best distribution for the consecutive models based on the highest log likelihood value. Missing data were imputed by multiple imputation, using functions from the ‘mice'package. 33 The number of imputed datasets was set at ten and the results of modelling were pooled by using the pool()function following Rubin's rules. 33 A power calculation was performed using the web‐based power calculator OpenEpi. 34 The significance level of this study and the power calculation was set at the level of 0.05.
The STROBE Guidelines were used in reporting on this observational study. 35
3. RESULTS
The participating children (n = 5,323) were (on average) six years of age at the moment of dental caries assessment (mean 6.2 years, SD 0.5). Table S1 shows the most important population characteristics of all participants. Of all children, 3,783 children (71.1%) were born from an uncomplicated pregnancy course, 508 (9.5%) were small for gestational age, 238 (4.5%) children had a spontaneous preterm birth, 196 (3.7%) were born from a mother with gestational hypertension and 107 (2.0%) from a mother with pre‐eclampsia. The total caries prevalence was a little more than 30%, and there were no significant differences between the groups with a pregnancy complication and those without.
Table 1 presents the outcome of the hurdle regression, fitted with a negative binomial distribution. We found no association between the separate pregnancy complications being small for gestational age, spontaneous preterm birth, gestational hypertension, pre‐eclampsia and the presence of dental caries by the age of six. Pregnancy complicated by the outcome placental syndrome was not associated with caries experience among six‐year‐olds (Model 1: OR 1.02, 95%CI 0.87 ‐ 1.19; RR 0.90, 95%CI 0.78 ‐ 1.04). Adding other confounding variables and life style factors did not alter the outcome in consecutive models.
Table 1.
Hurdle models of the relationship between pregnancy complications and the dmft index in six‐year‐old children a
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
|
Zero Part (caries yes/no) |
Count Part # of affected teeth |
Zero Part (caries yes/no) |
Count Part # of affected teeth |
Zero Part (caries yes/no) |
Count Part # of affected teeth |
|
|
Pregnancy complication (yes vs. no) |
OR [95% CI] |
RR [95% CI] |
OR [95% CI] |
RR [95% CI] |
OR [95% CI] |
RR [95% CI] |
|
SGA (508 vs. 4,762) |
1.05 [0.86 ‐ 1.28] |
0.98 [0.82 ‐ 1.18] |
1.04 [0.85 ‐ 1.27] |
0.98 [0.82 ‐ 1.18] |
0.97 [0.79 ‐ 1.19] |
0.99 [0.84 ‐ 1.17] |
|
sPTB (238 vs. 4,948) |
0.91 [0.68 ‐ 1.21] |
0.88 [0.67 ‐ 1.15] |
0.90 [0.68 ‐ 1.21] |
0.88 [0.67 ‐ 1.16] |
0.93 [0.69 ‐ 1.26] |
0.91 [0.70 ‐ 1.18] |
|
GH (196 vs. 4,363) |
1.07 [0.79 ‐ 1.46] |
0.81 [0.61 ‐ 1.07] |
1.07 [0.78 ‐ 1.45] |
0.80 [0.60 ‐ 1.07] |
1.19 [0.85 ‐ 1.65] |
0.91 [0.69 ‐ 1.19] |
|
PE (107 vs. 4,363) |
0.95 [0.62 ‐ 1.45] |
0.78 [0.52 ‐ 1.16] |
0.93 [0.61 ‐ 1.43] |
0.77 [0.52 ‐ 1.16] |
0.93 [0.59 ‐ 1.45] |
0.82 [0.56 ‐ 1.19] |
|
Placental Syndrome (950 vs. 3,738) |
1.02 [0.87 ‐ 1.19] |
0.90 [0.78 ‐ 1.04] |
1.02 [0.87 ‐ 1.19] |
0.90 [0.78 ‐ 1.04] |
1.00 [0.85 ‐ 1.18] |
0.96 [0.84 ‐ 1.09] |
In modelling the OR and RR, not being affected by pregnancy complications was used as the reference category. Model 1: Adjusted for child's age and sex. Model 2: Additionally adjusted for oral health‐related behaviour (Age at first dental visit, toothbrushing frequency, dental visit in the past year). Model 3: Additionally adjusted for child's ethnicity, age of mother at intake, BMI of mother at intake, educational level of mother, parity, breastfeeding and smoking during pregnancy.
The power calculation showed that if the ratio of unexposed to exposed is set at eight and the difference in risk of disease between the two groups is set at 1% to 10%, the level of power ranges from 3.7% to 86.2%
4. DISCUSSION
We found no association between the pregnancy complications (being small for gestational age, spontaneous preterm birth, gestational hypertension, and pre‐eclampsia) and the presence of dental caries in children, or the combined exposure placental syndrome.
A strength of our study is the large number of participating mothers and children. This resulted the possibility of adjusting for many confounders. Furthermore, we are the first to study gestational hypertension and the placental syndrome in relation to dental caries experience in children. However, our study is not free of limitations. By measuring the dmft index at one time point, we were unable to draw conclusions about the association between pregnancy complications and caries development or susceptibility. Another limitation of our study was the use of photographs instead of visual examination to assess caries in children. Caries assessment from dental photographs may have underestimated the observed caries prevalence. Another limitation is the lack of adjustment for sweet consumption frequency, unlike Nirunsittirat et al and Saraiva et al. 19 , 20 This may have masked an association in our study. Furthermore, we excluded mothers without information on pregnancy complications. This may have led to selection bias, although we determined the missingness to be at random. Moreover, due to the observational setting of our study, residual confounding in the presented associations cannot be completely ruled out (eg missing information on carbohydrate intake). Finally, despite the large number of participants, the level of power for some exposures (ie gestational hypertension and pre‐eclampsia) was relatively low due to the low prevalence of these pregnancy complications.
As discussed, our hypothesis was based on the presence of the NNL and Wilson bands within the dental enamel of primary teeth. 8 , 9 , 10 , 11 , 12 The presence of NNL and Wilson bands provides evidence for the existence of a critical period in amelogenesis following the ‘critical period model’ of life‐course epidemiology. 16 Hence, this led to our hypothesis that a complicated pregnancy may lead to more caries‐susceptible enamel in children than in children born from an uncomplicated pregnancy.
Noteworthy are the findings of a previous analysis within the Generation R Study, in which Elfrink et al assessed different pre‐, peri‐ and postnatal determinants in relation to the presence of Deciduous Molar Hypomineralization (DMH) in the same study population. 36 DMH is aetiologically different than dental caries, since it is a developmental disorder of the dental enamel, but it may lead to higher caries susceptibility. 36 Next to many other determinants, Elfrink et al included being small for gestational age and pre‐eclampsia as well. They failed to find an association between these two exposures and DMH in six‐year‐old children.
As with several other studies, we did not find being small for gestational age, spontaneous preterm birth or pre‐eclampsia to be associated with dental caries in children. 19 , 21 , 22 , 37 However, Nirunsittirat et al found an inverse association between spontaneous preterm birth and childhood caries. 19 This study involved 544 four‐year‐old children from Thailand. Their population was extremely dissimilar to ours in terms of oral health behaviour and (socio)‐demographic characteristics. Since socioeconomic status is one of the most important risk factors for dental caries, these dissimilarities hamper direct comparison of our findings with theirs and might explain the different conclusions. 38
Saraiva et al observed a similar counterintuitive association between being small for gestational age and dental caries, but a higher caries prevalence in children who were born preterm. 20 They performed a study in a more comparable American population existing of 2,341 three‐ to five‐year‐olds. They explained the inverse association as a result of delayed tooth eruption or possible increased antibiotics use in children who were small for gestational age. 20 Children born small for gestational age indeed have a delayed tooth eruption and thus their teeth have a shorter exposure to cariogenic factors compared to their peers. 20 , 39 However, the effect of long‐term antibiotic use on caries prevalence has only be shown in sickle cell patients and, in the Netherlands, small for gestational age children do not have a higher use of long‐term antibiotic therapy. 40 Moreover, they did not define preterm birth as a spontaneous one and is therefore difficult to compare. 20
Furthermore, all abovementioned studies included a younger population of children. 19 , 20 , 21 , 22 , 37 Meaning a shorter exposure to cariogenic risk factors, because of caries assessment at one timepoint in all studies, may explain a part of the variability in results.
To date, one study explored the association between birthweight and repeated caries assessments. 18 In one‐year‐old Scottish children (n = 1102), Bernabé et al found the caries increment during the three year follow‐up to be the highest in children with a low birth weight (<2500 g), while not adjusting for sugar intake. 18 This design allows to draw conclusions about the gradual increase of dental caries over time, which might be more indicative for caries risk than dental caries assessment at one time point. Despite the differently defined outcome measures between our studies (low birth weight vs. being small for gestational age), it is notable that they did find a significant association without adjusting for sugar intake. Possibly, sugar intake might have masked the association between pregnancy complications and caries experience within our study, but this does not seem to hold for the association between pregnancy complications and caries increment. Part of the explanation could be the fact that the sugar intake is probably low between the age of one and four, but this remains to be investigated. 18
Although it is expected that prenatal stress in the form of placental insufficiency can be a risk factor for caries development later in life, our current study assessing this effect does not support this hypothesis following the ‘critical period model’ of life‐course epidemiology. 16 It is likely that other models in life‐course epidemiology play a more prominent role in caries development, such as the ‘accumulation of risk model’, which would better explain the association between socioeconomic position and dental caries. 16 , 38 Since caries risk is clinically the most interesting and better captured in repeated measurements than current caries experience, we would recommend future research to focus more on longitudinal caries data rather than on caries assessment at one time point. In conclusion, despite a reasonable biological basis, we found no support for an association between placental insufficiency‐related complications and caries experience by school age.
CONFLICT OF INTEREST
All authors declare to have no conflict of interest.
AUTHOR CONTRIBUTIONS
JT van der Tas wrote the manuscript, performed the analyses and conceived the idea for this study together with and under direct supervision of S. Schalekamp‐Timmermans. EB Wolvius, F. Rivadeneira, HA Moll and EAP Steegers laid the foundation for the Generation R Study cohort in which this study was embedded and was in charge of data collection and study logistics. J.T van der Tas, S. Schalekamp‐Timmermans and L. Kragt contributed to the design of the study and interpretation of the results. All authors provided critical feedback and helped shape the study, analyses and final manuscript.
Supporting information
Table S1
ACKNOWLEDGEMENTS
First of all, we gratefully acknowledge the contribution of the participants, general practitioners, hospitals, midwives and pharmacies in Rotterdam. The Generation R Study was conducted by the Erasmus Medical Center, Rotterdam, Netherlands, in close collaboration with the School of Law and Faculty of Social Sciences of Erasmus University, Rotterdam; the Municipal Health Service, Rotterdam area; the Rotterdam Homecare Foundation; and the Stichting Trombosedienst & Artsenlaboratorium Rijnmond, Rotterdam. The Erasmus Medical Center, Rotterdam; the Erasmus University, Rotterdam; and the Netherlands Organization for Health Research and Development made the first phase of the Generation R Study financially possible. For the dental part of the research, we received an additional and unrestricted grant of GABA, Therwil, Switzerland. Furthermore, VWVJ received an additional grant from the Netherlands Organization for Health Research and Development (VIDI 016.136.361) and a Consolidator Grant from the European Research Council (ERC‐2014‐CoG‐64916).
van der Tas JT, Wolvius EB, Kragt L, et al. Caries experience among children born after a complicated pregnancy. Community Dent Oral Epidemiol. 2021;49:225–231. 10.1111/cdoe.12593
REFERENCES
- 1. Vos T, Lozano R, Naghavi M, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(9995):743‐800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Selwitz RH, Ismail AI, Pitts NB. Dental caries. Lancet. 2007;369:51‐59. [DOI] [PubMed] [Google Scholar]
- 3. Americano GC, Jacobsen PE, Soviero VM, Haubek D. A systematic review on the association between molar incisor hypomineralization and dental caries. Int J Paediatr Dent. 2017;27:11‐21. [DOI] [PubMed] [Google Scholar]
- 4. Elfrink ME, Schuller AA, Veerkamp JS, Poorterman JH, Moll HA, ten Cate JM. Factors increasing the caries risk of second primary molars in 5‐year‐old Dutch children. Int J Paediatr Dent. 2010;20:151‐157. [DOI] [PubMed] [Google Scholar]
- 5. Barker DJ. The foetal and infant origins of adult disease. BMJ. 1990;301:1111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Smith CE. Cellular and chemical events during enamel maturation. Crit Rev Oral Biol Med. 1998;9:128‐161. [DOI] [PubMed] [Google Scholar]
- 7. Eli I, Sarnat H, Talmi E. Effect of the birth process on the neonatal line in primary tooth enamel. Pediatr Dent. 1989;11:220‐223. [PubMed] [Google Scholar]
- 8. Canturk N, Atsu SS, Aka PS, Dagalp R. Neonatal line on fetus and infant teeth: An indicator of live birth and mode of delivery. Early Hum Dev. 2014;90:393‐397. [DOI] [PubMed] [Google Scholar]
- 9. Hurnanen J, Visnapuu V, Sillanpää M, Löyttyniemi E, Rautava J. Deciduous neonatal line: Width is associated with duration of delivery. Forensic Sci Int. 2017;271:87‐91. [DOI] [PubMed] [Google Scholar]
- 10. Sabel N, Johansson C, Kühnisch J, et al. Neonatal lines in the enamel of primary teeth—a morphological and scanning electron microscopic investigation. Arch Oral Biol. 2008;53:954‐963. [DOI] [PubMed] [Google Scholar]
- 11. FitzGerald CM, Saunders SR. Test of histological methods of determining chronology of accentuated striae in deciduous teeth. Am J Phys Anthropol. 2005;127:277‐290. [DOI] [PubMed] [Google Scholar]
- 12. FitzGerald C, Saunders S, Bondioli L, Macchiarelli R. Health of infants in an imperial roman skeletal sample: Perspective from dental microstructure. Am J Phys Anthropol. 2006;130:179‐189. [DOI] [PubMed] [Google Scholar]
- 13. Simmer JP, Papagerakis P, Smith CE, et al. Regulation of dental enamel shape and hardness. J Dent Res. 2010;89:1024‐1038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Jacobsen PE, Haubek D, Henriksen TB, Østergaard JR, Poulsen S. Developmental enamel defects in children born preterm: A systematic review. Eur J Oral Sci. 2014;122:7‐14. [DOI] [PubMed] [Google Scholar]
- 15. Costa FS, Silveira ER, Pinto GS, Nascimento GG, Thomson WM, Demarco FF. Developmental defects of enamel and dental caries in the primary dentition: A systematic review and meta‐analysis. J Dent. 2017;60:1‐7. [DOI] [PubMed] [Google Scholar]
- 16. Nicolau B, Thomson WM, Steele JG, Allison PJ. Life‐course epidemiology: Concepts and theoretical models and its relevance to chronic oral conditions. Community Dent Oral Epidemiol. 2007;35:241‐249. [DOI] [PubMed] [Google Scholar]
- 17. Yokomichi H, Tanaka T, Suzuki K, Akiyama T, Yamagata Z. Macrosomic Neonates Carry Increased Risk of Dental Caries in Early Childhood: Findings from a Cohort Study, the Okinawa Child Health Study, Japan. PLoS One. 2015;10:e0133872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Bernabé E, MacRitchie H, Longbottom C, Pitts NB, Sabbah W. Birth weight, breastfeeding, maternal smoking and caries trajectories. J Dent Res. 2016;96:171‐178. [DOI] [PubMed] [Google Scholar]
- 19. Nirunsittirat A, Pitiphat W, McKinney C, et al. Adverse birth outcomes and childhood caries: A cohort study. Community Dent Oral Epidemiol. 2016;44:239‐247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Saraiva MC, Bettiol H, Barbieri MA, Silva AA. Are intrauterine growth restriction and preterm birth associated with dental caries? Community Dent Oral Epidemiol. 2007;35:364‐376. [DOI] [PubMed] [Google Scholar]
- 21. Shulman JD. Is there an association between low birth weight and caries in the primary dentition? Caries Res. 2005;39:161‐167. [DOI] [PubMed] [Google Scholar]
- 22. Tanaka K, Miyake Y. Low birth weight, preterm birth or small‐for‐gestational‐age are not associated with dental caries in young Japanese children. BMC Oral Health. 2014;14:38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Kooijman MN, Kruithof CJ, van Duijn CM, et al. The generation R study: Design and cohort update 2017. Eur J Epidemiol. 2016;31:1243‐1264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Coolman M, de Groot CJM, Jaddoe VW, Hofman A, Raat H, Steegers EAP. Medical record validation of maternally reported history of preeclampsia. J Clin Epidemiol. 2010;63:932‐937. [DOI] [PubMed] [Google Scholar]
- 25. Gaillard R, de Ridder MAJ, Verburg BO, et al. Individually customised foetal weight charts derived from ultrasound measurements: The generation R study. Eur J Epidemiol. 2011;26:919‐926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Mol BWJ, Roberts CT, Thangaratinam S, Magee LA, de Groot CJM, Hofmeyr GJ. Pre‐eclampsia. Lancet. 2016;387:999‐1011. [DOI] [PubMed] [Google Scholar]
- 27. Sohn W, Burt B, Sowers M. Carbonated soft drinks and dental caries in the primary dentition. J Dent Res. 2006;85:262‐266. [DOI] [PubMed] [Google Scholar]
- 28. Brosens I, Pijnenborg R, Vercruysse L, Romero R. The, “great obstetrical syndromes” are associated with disorders of deep placentation. Am J Obstet Gynecol. 2011;204:193‐201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Elfrink ME, Veerkamp JS, Aartman IH, Moll HA, Ten Cate JM. Validity of scoring caries and primary molar hypomineralization (DMH) on intraoral photographs. JM Eur Arch Paediatr Dent. 2009;10:5‐10. [DOI] [PubMed] [Google Scholar]
- 30. van der Tas JT, Kragt L, Veerkamp JJS, et al. Ethnic disparities in dental caries among six‐year‐old children in the netherlands. Caries Res. 2016;50:489‐497. [DOI] [PubMed] [Google Scholar]
- 31. Hofstetter H, Dusseldorp E, Zeileis A, Schuller AA. Modeling caries experience: Advantages of the use of the hurdle model. Caries Res. 2016;50:517‐526. [DOI] [PubMed] [Google Scholar]
- 32. Zeileis A, Kleiber C, Jackman S. Regression models for count data in R. J Stat Softw. 2008;27:1‐25. [Google Scholar]
- 33. van Buuren S, Groothuis‐Oudshoorn K. Mice: Multivariate imputation by chained equations in r. J Stat Softw. 2011;45:1‐67. [Google Scholar]
- 34. Openepi: Open source epidemiologic statistics for public health [online]. 2012. http://www.openepi.com/SampleSize/SSCohort.htm Accessed 05/05/2020
- 35. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. J Clin Epidemiol. 2008;61:344‐349. [DOI] [PubMed] [Google Scholar]
- 36. Elfrink MEC, Moll HA, Kiefte‐de Jong JC, et al. Pre‐ and Postnatal Determinants of Deciduous Molar Hypomineralisation in 6‐Year‐Old Children. The Generation R Study. PLoS One. 2014;9:e91057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Sayyed T, Kandil M, Bashir O, Alnaser H. The relationship between term pre‐eclampsia and the risk of early childhood caries. J Matern Fetal Neonatal Med. 2014;27:62‐65. [DOI] [PubMed] [Google Scholar]
- 38. Schwendicke F, Dörfer CE, Schlattmann P, Page LF, Thomson WM, Paris S. Socioeconomic inequality and caries: A systematic review and meta‐analysis. J Dent Res. 2014;94:10‐18. [DOI] [PubMed] [Google Scholar]
- 39. Aktoren O, Tuna EB, Guven Y, Gokcay G. A study on neonatal factors and eruption time of primary teeth. Community Dent Health. 2010;27:52‐56. [PubMed] [Google Scholar]
- 40. Fukuda JT, Sonis AL, Platt OS, Kurth S. Acquisition of mutans streptococci and caries prevalence in pediatric sickle cell anemia patients receiving long‐term antibiotic therapy. Pediatr Dent. 2005;27:186‐190. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1