

EUS-guided gastroenterostomy (GE) was alternative treatment with respect to conventional therapies for oncological gastric outlet obstruction (GOO) during the COVID-19 pandemic in Italy.
This is the case of a patient with obstructing duodenal diffuse large B-cell lymphoma (DLBCL) causing GOO. Malignant duodenal stenosis was treated by the wireless EUS-GE simplified technique: in a single step, EUS-GE was performed, directly puncturing with a hot-cautery device the jejunal loop and using a fully-covered lumen-apposing metal stent (LAMS). A pneumatic stent dilation was finally performed to consolidate the newly-created fistula. The patient was able to tolerate oral feeding and discharged 2 days after. An adequate nutritional state persists after 8 months, with patency of the stent.
In the context of the COVID-19 crisis in Italy, EUS-GE was preferred to surgery for GOO with a rapid hospital discharge and prompt oncological treatment resumption.
COVID-19 outbreak dramatically changed patients' management in Italy, especially for oncological patients, due to their higher risk of becoming critically ill contracting the virus. Oncologists have to reassess the surgical procedures need, considering nonsurgical management whenever possible.[1]
In this period, a 53-year-old male presented with GOO. Upper-GI endoscopy revealed a large duodenal bulb Forrest 3 ulcer [Figure 1], with second duodenum stenosis [Figure 2], positive for DLBCL. Two cycles of specific chemotherapy were given. Finished second cycle, the patient developed a mild form of COVID-19 disease with pharyngeal swabs positive for 90 days.
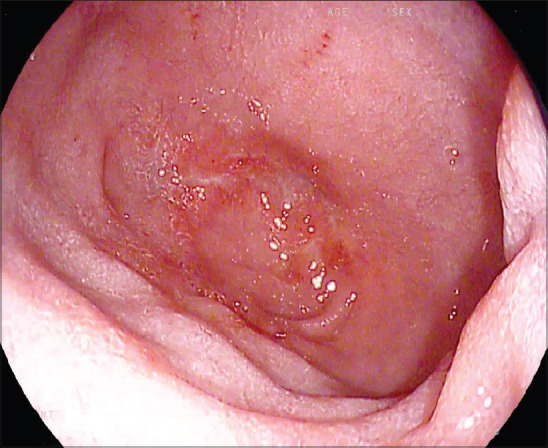
Figure 1.

Endoscopic aspect of duodenal bulb ulcer, resulted at histology diffuse large B cell-lymphoma
Figure 2.
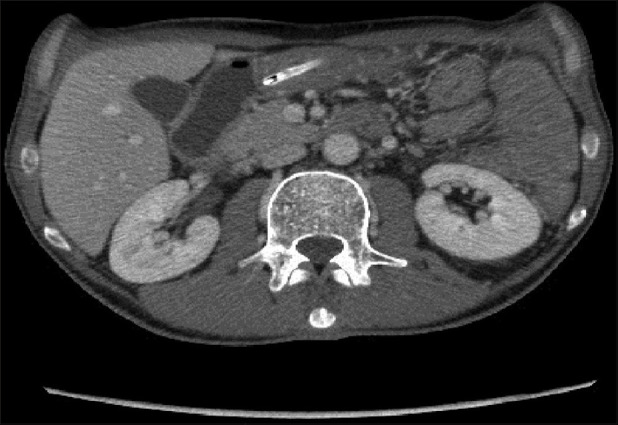
Computed tomography-scan view of second duodenum stenosis due to the lymphoma (with naso-gastric tube inserted)
Given GOO presence in COVID-19 patient, EUS-GE was considered. The procedure was performed in a negative-pressure endoscopic room under oro-tracheal intubation. Under endoscopic and fluoroscopic control a guide-wire was advanced through the duodenal stenosis to the first jejunal loop; a 7-French pig-tail nasojejunal tube (N-JT) was advanced through the guidewire and left in situ. A linear echoendoscope (EG38-J10UT-Pentax, Hamburg, Germany) was used and 500 mL of saline was injected into N-JT under continuous EUS-control, to distend the first jejunal loop at Treitz ligament. With adequate loop distension and clear lumen evidence, methylene blue dye was injected through the N-JT for subsequent GE patency assessment. EUS-GE was performed in a single step directly puncturing with a hot-cautery device jejunal loop, positioning a fully-covered LAMS (LAMS; HotAxios-Boston Scientific) 2 cm in caliber, 1 cm length, to connect gastric wall with first jejunal loop [Figure 3].[2] Methylene blue dye outlet was immediately seen; iodinate contrast injection into N-JT confirmed stomach-jejunum connection [Video 1]. Pneumatic stent dilation up to 18 mm was performed [Video 2]. 24 h contrast X-ray confirmed LAMS correct positioning and patency [Figure 4]. Two days after, the patient was able to tolerate oral feeding and was discharged. An adequate nutritional state persists after 8 months, with patency of the stent [Figures 5, 6 and Video 3]. Being the lymphoma in complete remission, a surgical/more definitive strategy will be discussed.
Figure 3.
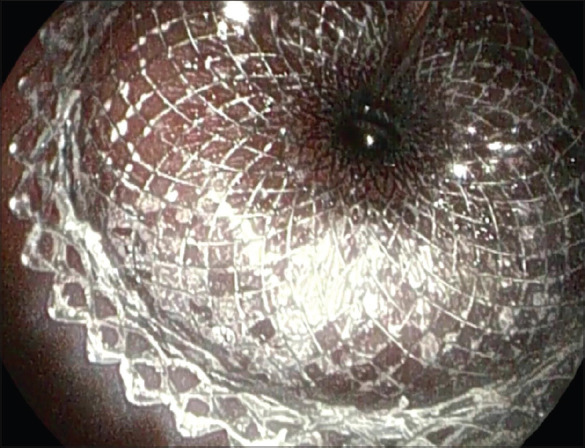
Endoscopic view just after second flange positioning of lumen apposing metal stent between the stomach and the first jejunal loop
Figure 4.

24-h contrast X-ray after EUS-gastroenterostomy: Lumen apposing metal stent correct positioning and patency
Figure 5.
8-month endoscopic control after EUS-gastroenterostomy: Complete duodenal bulb ulcer regression
Figure 6.

8-month endoscopic control after EUS-gastroenterostomy: Lumen apposing metal stent correct positioning and patencyLumen apposing metal stent correct positioning and patency
GOO increases malnutrition risk and significantly impacts on life quality and oncological regimens adherence. In the context of the COVID-19 crisis in Italy, EUS-GE was preferred to surgery for GOO with a rapid hospital discharge and prompt oncological treatment resumption.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that his name and initials will not be published and due efforts will be made to conceal his identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Videos Available on: www.eusjournal.com
REFERENCES
- 1.Asokan I, Rabadia SV, Yang EH. The COVID-19 pandemic and its impact on the cardio-oncology population. Curr Oncol Rep. 2020;22:60. doi: 10.1007/s11912-020-00945-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bronswijk M, van Malenstein H, Laleman W, et al. EUS-guided gastroenterostomy: Less is more! The wireless EUS-guided gastroenterostomy simplified technique (WEST) VideoGIE. 2020;5:442. doi: 10.1016/j.vgie.2020.06.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.