

A 46-years-old female with unresectable pancreatic adenocarcinoma previously palliated by a transpapillary biliary plastic stent placement, was referred to our unit because of the onset of gastric outlet obstruction (GOO) symptoms, along with jaundice relapse. Endoscopic assessment confirmed a neoplastic stricture of the duodenal bulb with an inaccessible major papilla. Single-session EUS-guided gastroenterostomy (GE) and biliary drainage (BD) was therefore planned.
A 7.5 Fr nasobiliary tube was introduced into the proximal jejunum, and a blue-tinged, contrasted solution was instilled to distend the jejunal lumen. After EUS confirmation of the target loop by aspirating the blue-tinged solution with a 19-gauge needle, EUS-GE was performed by a 15 mm × 10 mm cautery-assisted lumen apposing metal stent (EC-LAMS, Hot-Axios, Boston Scientific Corporation Inc., Marlborough, MA, USA) placement (Video 1).
Since the duodenal infiltration, with distance between the duodenal wall and the common bile duct up to 12 mm [Figure 1], did not allow a stable position, BD was obtained by performing an EUS-guided hepaticogastrostomy (EUS-HGS). A specifically dedicated 10 mm × 80 mm partially-covered stent (Hanarostent Biliary stent, M. I. Tech, Seoul, Rep. South Korea) was placed under endoscopic and fluoroscopic guidance. This stent was conceived as asymmetrically covered and shaped, in order to have its uncovered-tubular end into the intrahepatic ducts, and the covered-flanged end into the gastric cavity, to reduce the risk of migration (Video 2).
Figure 1.
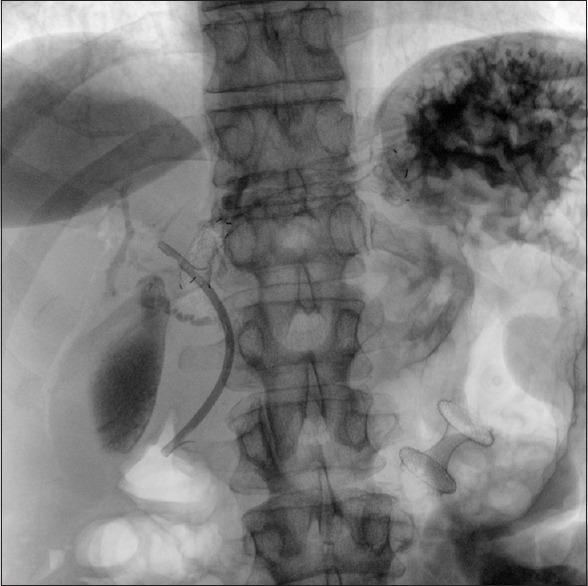
Dedicated stents for EUS-GE and -HGS: final fluoroscopic view.
No procedure-related adverse events were reported.
Successful single session management of concomitant biliary and duodenal obstruction has been described, by EUS-choledochoduodenostomy and subsequent duodenal stent placement[1].
In this case, we preferred to perform an EUS-GE followed by EUS-HGS as they have emerged as a feasible and effective novel alternative approach for palliation of concomitant biliary and GOO.[2,3,4]
Keeping the distance from the neoplastic epicenter both the approaches could offer long-lasting stents patency. As a matter of fact since specifically dedicated devices (i.e., LAMS) have been developed, we are witnessing the escalation of EUS-guided therapeutic procedures.[5] The development of dedicated stents for different indications (such as EUS-HGS) could further increase the procedural feasibility offering customized approaches to our patients.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that her name and initials will not be published and due efforts will be made to conceal her identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Videos available on: www.eusjournal.com
REFERENCES
- 1.Anderloni A, Buda A, Carrara S, et al. Single-session double-stent placement in concomitant malignant biliary and duodenal obstruction with a cautery-tipped lumen apposing metal stent. Endoscopy. 2016;48:E321–2. doi: 10.1055/s-0042-117425. [DOI] [PubMed] [Google Scholar]
- 2.Mussetto A, Fugazza A, Fuccio L, et al. Current uses and outcomes of lumen-apposing metal stents. Ann Gastroenterol. 2018;31:535–40. doi: 10.20524/aog.2018.0287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Chen YI, Itoi T, Baron TH, et al. EUS-guided gastroenterostomy is comparable to enteral stenting with fewer re-interventions in malignant gastric outlet obstruction. Surg Endosc. 2017;31:2946–52. doi: 10.1007/s00464-016-5311-1. [DOI] [PubMed] [Google Scholar]
- 4.Ogura T, Chiba Y, Masuda D, et al. Comparison of the clinical impact of endoscopic ultrasound-guided choledochoduodenostomy and hepaticogastrostomy for bile duct obstruction with duodenal obstruction. Endoscopy. 2016;48:156–63. doi: 10.1055/s-0034-1392859. [DOI] [PubMed] [Google Scholar]
- 5.Anderloni A, Leo MD, Carrara S, et al. Endoscopic ultrasound-guided transmural drainage by cautery-tipped lumen-apposing metal stent: Exploring the possible indications. Ann Gastroenterol. 2018;31:735–41. doi: 10.20524/aog.2018.0299. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.