

Abstract
Aim
To explore the relationship between demographic factors, acute coronary syndrome‐related factors, perceived control and health‐related quality of life during admission, 3 months and 6 months after discharge, in patients with acute coronary syndrome.
Methods
Participants were recruited for this longitudinal study after admission for acute coronary syndrome in three university hospitals in the Tokyo metropolitan area, Japan. Self‐administered questionnaires included demographic data, perceived control, health‐related quality of life, acute coronary syndrome symptoms, fatigue, depression and anxiety.
Results
Participants (N = 137) had an average age of 62.8 (SD 11.6) years and 80.3% were male. As a result of Path analysis, higher perceived control (β = 0.258, p = .001), lower anxiety (β = −0.226, p = .009) and lower fatigue (β = −0.231, p = .010), were significantly related to better health‐related quality of life (General health). Only annual income was significantly related to perceived control (β = 0.187, p = .029). Eighty‐two (59.9%) participants at 3 months and 54 (39.4%) participants at 6 months completed the questionnaires. Perceived control (F = 7.074, p = .001) and General health (χ2 = 10.22, p = .006) significantly increased over the 6 months. Perceived control during admission was significantly related with health‐related quality of life at 3 months. Perceived control at 3 months was significantly related with health‐related quality of life at 6 months.
Conclusion
Perceived control was an important factor for health‐related quality of life of the Japanese patients with acute coronary syndrome. It is necessary to investigate whether nursing interventions to enhance perceived control lead to improvement of health‐related quality of life.
Keywords: acute coronary syndrome, health‐related quality of life, Japanese, longitudinal study, perceived control
1. INTRODUCTION
Ischemic heart disease is the leading cause of death globally (World Health Organization, 2018) and the second leading cause of death in Japan. The rate of treatment of cardiovascular disease was the second highest after mental health problems in Japan (Ministry of Health Labor and Welfare, 2018). Although the age‐adjusted mortality rate of patients with heart disease is decreasing, crude death rate is increasing due to the aging population in Japan. Coronary heart disease is a chronic condition that develops after acute coronary syndrome (ACS). People diagnosed with ACS experience a significant reduction in their health‐related quality of life (HRQoL) (Seo et al., 2015).
In Japan, factors associated with HRQoL of patients with cardiovascular disease have not been quantitatively well investigated. QoL of the general population was significantly lower among people with lower income, those over 60 years old and people who were less educated (Shiroiwa et al., 2016). Mobility, symptoms, emotional well‐being, and fatigue were negatively related to HRQoL; employment status, income and disease information were important factors to maintain HRQoL; and a decrease in household income was associated with an increase in anxiety and depression, and decrease in HRQoL of Japanese patients with multiple sclerosis (Kikuchi et al., 2011). Miyazaki (2020) reported negative feelings were associated with lower HRQoL of patients with heart failure.
Sasaki, Inoue, Yatomi, Suzuki, and Suzuki (2006) described perceived control as an indicator of recovery from severe injury in a qualitative study, and they recommended enhancing perceived control of critically ill patients to improve their outcomes. Perceived control is a belief that a person has the resources to cope with negative events in a way that positively influences the outcome (Moser et al., 2009). In a large study with noninstitutionalized adults (N = 6,210) over 9 years in the United States, greater perceived control at baseline was predictive of less decline in health (a composite of acute conditions, chronic health conditions, and the number of functional limitations) and better social support (Gerstorf, Rocke, & Lachman, 2011). Patients with coronary heart disease, heart failure or myocardial infarction (MI), reported higher levels of perceived control had lower levels of anxiety and depression (Moser et al., 2009). Patients with high perceived control at baseline who had MI were less depressed, less anxious, less hostile, and had better psychosocial adjustment at a 6‐month follow‐up than those with low perceived control (Moser & Dracup, 1995). After ACS, higher perceived control was an independent predictor of lower in‐hospital complications (McKinley et al., 2012). However, the association between perceived control during hospitalization and HRQoL after discharge in patients with ACS has not been reported.
The purpose of study was to explore associations among demographic factors, ACS‐related factors, perceived control and HRQoL during admission, 3 months and 6 months after discharge in Japanese patients who were hospitalized for ACS. If perceived control is associated with HRQoL in patients with ACS, nurses may be able to provide care to enhance perceived control and improve HRQoL.
1.1. Research framework and definitions
Figure 1 is the framework of this study. Sociodemographic factors related to perceived control are based on the model from Robinson and Lachman (2017, p. 217), which includes age, gender, ethnicity and socio‐economic status (education, employment and income). Men tend to have a higher perceived control than women on average although this difference is less significant among college‐educated adults. Lower education and income have been associated with a lower level of perceived control (Robinson & Lachman, 2017).
FIGURE 1.
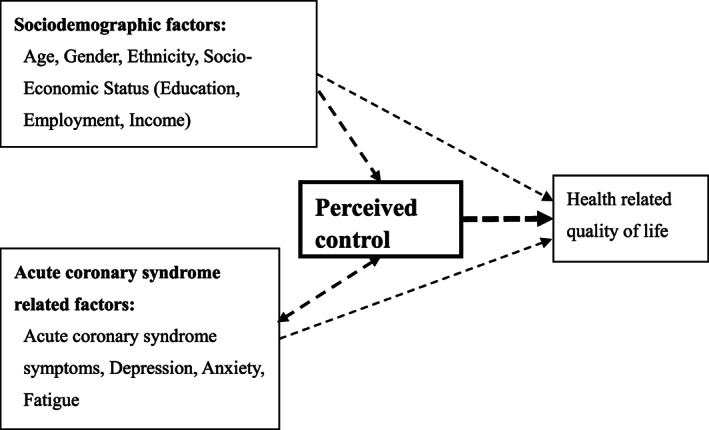
Research framework
ACS‐related factors included ACS symptoms, depression, anxiety and fatigue. Loss of perceived control is often related to anxiety, depression and death (Fatemi & Langer, 2017). Killip, New York Heart Association classification or N‐terminal pro‐brain natriuretic peptide that measure severity of conditions were not measured for all patients in the study hospitals; therefore, no severity measure was included.
Depression and anxiety are important factors that should be included in the study of patients after hospitalization for any cardiac disease. Depression is a serious mental illness which may include sadness and anhedonia (American Psychiatric Association, 2018b). Anxiety is the condition having anticipation of a future concern and is associated with tension and avoidance behavior (American Psychiatric Association, 2018a). Depression has consistently been linked to a poor prognosis in patients with coronary heart disease, including ACS, although patient populations and study designs differ (Frasure‐Smith & Lesperance, 2006). Both anxiety and depression are associated with increased risk of mortality in patients with coronary heart disease (Celano et al., 2015).
Depression and anxiety were also associated with higher levels of fatigue in patients with ACS. Fatigue is a state of tiredness and diminished functioning. Fatigue has been implicated as a prodromal symptom of ACS in women (McSweeney et al., 2010). In a study of 472 patients with ACS, lack of energy was reported by 80% of the sample immediately following hospitalization (Shaffer et al., 2012). In addition, fatigue has been identified as a long‐term consequence of MI, affecting patients for at least 2 years (Alsen & Brink, 2013).
Perceived control is a person's belief that they can determine their own internal state and that they can influence the environment, which leads to positive changes or lessening of negative impacts (Fatemi & Langer, 2017). A cause‐and‐effect relationship has been supported with higher levels of perceived control leading to better well‐being (Fatemi & Langer, 2017).
This study focuses on HRQoL of patients with ACS as an outcome. HRQoL is an individual's or a group's perceived physical and mental health over time (Centers for Disease Control and Prevention, 2018). HRQoL can be defined as the effect of illness, treatment, and overall health on a person's QoL. HRQoL spans not only physical health, but also mental dimensions of overall well‐being (Ferrans, Zerwic, Wilbur, & Larson, 2005). In this study, the Short Form (SF)‐12, which includes physical and mental health, was used to measure HRQoL.
2. METHODS
2.1. Design and participants
This is a longitudinal study, which included patients from three hospitals in the Tokyo metropolitan area, Japan. The study hospitals are teaching hospitals with 700 ~ 800 beds and have specialized cardiovascular units. These hospitals were selected as a convenience sample of patients with ACS. In all hospitals, no specific nursing care to enhance perceived control was provided.
Inclusion criteria of participants were adults (21 years old or older), hospitalized with a primary diagnosis of ACS (acute MI or unstable angina), alert and oriented, and hemodynamically stable. Anyone under 21 years old was excluded due to low incidence of primary ACS. Exclusion criteria included patients who were unable to complete the questionnaires independently (e.g., dementia), on dialysis, active cancer or cancer treatment in the last 6 months, or anyone with a life expectancy less than 6 months.
2.2. Sample size
Sample size was calculated using G*Power. Necessary sample size was estimated to be 120 in order to detect r = 0.25 with alpha (two‐tailed) = .05, beta = 0.2. We used r = 0.25 because Ozawa and Ikeda (2016) reported rs = 0.21 ~ 0.26 (p = .005 ~ 0.026, n = 113) for the correlation coefficients between perceived control and items on the SF‐36 for patients with risk of heart failure in Japan.
3. DATA COLLECTION
Each participant was recruited during admission for ACS. All participants provided written informed consent. A self‐administered questionnaire was completed during admission by those who agreed to participate. The questionnaires included demographic data and standard tools for the measurement of perceived control, HRQoL, ACS symptoms, fatigue, depression, and anxiety. All instruments were administered in Japanese. Questionnaires except demographics along with a self‐addressed stamped envelope were mailed to each participant's home address at 3 and 6 months after discharge. Patients' diagnoses were collected from the medical records. The study period was December 2015 to December 2019.
4. MEASUREMENT
Perceived control was measured using the Control Attitudes Scale‐Revised (Moser et al., 2009). The scale includes eight questions related to perceived control over health conditions. Participants answer each question from 1 (totally disagree) to 5 (totally agree). The total score ranges from 8–40, where a higher score indicates higher levels of perceived control.
HRQoL was measured using the SF‐12. The 12‐item Likert‐type scale includes eight subscales: Physical functioning, Role‐physical, Bodily pain, General health, Vitality, Social functioning, Role‐emotional, and Mental health. All subscales are used to calculate two summary measures: physical health and mental health. The SF‐12 uses norm‐based scoring for all of the subscales employing a linear T‐score transformation with a mean of 50 ± 10 (range 0–100) with higher scores indicating better HRQoL. Comparisons across subscales enable researchers to identify which subscales are most affected by various disease states since each subscale has the same mean and standard deviation. The SF‐12 is a shortened version of the SF‐36 for which reliability and validity are well established as well as norms across different populations (McHorney, Ware, & Raczek, 1993). The SF‐12 is widely recognized for its reliability and validity in a variety of populations and has been used successfully in patients with MI (Melville, Lari, Brown, Young, & Gray, 2003). It is also widely used in Japanese (i Hope International, 2012).
The ACS Symptom Checklist is a 13‐item instrument which is used to measure symptoms in patients with ACS. Participants answer yes/no whether they have 13 common symptoms of ACS, including Chest Pressure, Shoulder Pain, Sweating, Palpitations, Chest Discomfort, Upper Back Pain, Short of Breath, Arm Pain, Unusual Fatigue, Nausea, Lightheaded, Chest Pain and Indigestion. The ACS Symptom Checklist does not have a summary score or severity score. Each symptom is analyzed individually. This is a validated checklist with symptoms that were derived from a large patient sample and can be completed within 1 min (Devon, Rosenfeld, Steffen, & Daya, 2014).
The Fatigue Symptom Inventory (FSI) is a 14‐item self‐report instrument, which measures fatigue. It includes questions of intensity, duration of fatigue and interference with activities of daily living over the past week. The first four items measure severity of fatigue (0 = not at all fatigued; 10 = as fatigued as I could be). Items 5–11 are regarded as the FSI Interference Scale which is used to measure interference with activities of daily living from 0–10 (0 = no interference; 10 = extreme interference). The items in the scale are summed and divided by the total number of questions to generate an interference score. A higher interference score indicates more interference with activities of daily living. Remaining items ask the participant about the timing and duration of fatigue. The FSI has excellent reliability with coefficient alphas >.90 (Hann, Denniston, & Baker, 2000; Hann et al., 1998), and is a publicly available tool that does not require permission to use (“Fatigue Symptom Inventory,” 2010).
Depression was measured using the Patient Health Questionnaire 9 (PHQ‐9), which includes nine items, and has been used successfully in cardiovascular disease (Eckhardt, Devon, Piano, Ryan, & Zerwic, 2014; Fink et al., 2012; Lee, Lennie, Heo, & Moser, 2012). The total score ranges from 0–27 with higher scores indicating worse depression. The scale has been translated into a variety of languages including Japanese using an internationally accepted translation methodology, and is freely downloadable (Pfizer, n.d.). Total score of 0–4 is regarded as no depression, 5–9 as mild depression, 10–14 as moderate depression, 15–19 as moderate to severe, and 20–27 as severe depression (Muramatsu, 2014). Scores of 10 or more are typically considered clinically significant requiring treatment.
Anxiety was measured using the Generalized Anxiety Disorder 7 (GAD‐7). It is a seven‐item instrument with a total score ranging from 0–21 with higher scores indicating worse anxiety. Although anxiety and depression often co‐occur, a factor analysis confirmed that generalized anxiety disorder and depression have distinct dimensions (Spitzer, Kroenke, Williams, & Lowe, 2006). The sensitivity and specificity of the GAD‐7 in Japan were respectively reported to be 88% and 82% (Nakamura et al., 2013). A total score of 0–4 is regarded as no anxiety, 5–9 as mild anxiety, 10–14 as moderate anxiety, 15–21 as severe anxiety (Muramatsu, 2014). The scale was translated into Japanese by Muramatsu (2014), and the authors received permission to use it.
After getting permission from creators, the first author translated the Control Attitudes Scale‐Revised and ACS Checklist into Japanese, and a physician who specialized in cardiovascular internal medicine confirmed the translations. Finally, a third bilingual individual back‐translated the instruments to confirm the translation. The bilingual individual translated the FSI into Japanese and the first author confirmed the Japanese translation. Authors obtained permission to use all the above scales from creators and translators except publicly available scales.
5. ANALYSIS
The Shapiro–Wilk test was used to check normality of continuous variables. Age and total score of perceived control were normally distributed (p > .05), but each item on the Control Attitudes Scale‐Revised and FSI, other subscales of the SF‐12, and total score of depression and anxiety were not normally distributed (p < .05). Parametric methods such as mean and SD were used for normally distributed data, and non‐parametric methods such as median and range were used for non‐normally distributed data. Since total score of the Control Attitudes Scale‐Revised was normally distributed, Pearson's correlation coefficients were used to analyze the association between perceived control and each item of HRQoL, age, number of ACS symptoms, fatigue, depression and anxiety. Cronbach's alpha was used to test reliability.
Homogeneity of variance between two groups was checked by Levene's test, and Student's t test (homogenous) or Welch's t test (heterogenous) were used to compare total score of perceived control between two groups. Chi‐square test or Fisher's exact test was used to compare the ratio of gender, education, employment status and annual income between groups. Analysis of variance or Kruskal‐Wallis test was used to compare continuous variables among hospitals according to their normality.
Factors related to total score of perceived control were analyzed using linear regressions. In the first model, age, gender, education, employment, anxiety (GAD‐7) and depression (PHQ‐9), which are empirically known to be related to perceived control, were forcibly entered. In the second model, diagnosis, age, gender, education, employment, number of ACS symptoms, depression, anxiety, FSI items, and the FSI Interference score were used for the stepwise liner regression. The model that had the highest adjusted R2 in stepwise regression was selected.
Among items of SF‐12, General health was selected to analyze factors related to HRQoL because General health had the lowest median but highest correlation coefficient with perceived control in these study participants, and can include both physical and mental perceived health. Since General health was not normally distributed, Mann–Whitney U test and Spearman's correlation coefficients were used to explore the association with sociodemographic and ACS related factors. Sociodemographic and ACS related factors significantly related to General health in Mann–Whitney U test or Spearman's correlation coefficients were forcibly entered into logistic regression with the outcome variable of General health (greater than median or not). After these analyses, the relationship among sociodemographic factors, ACS related factors, perceived control and General health was analyzed using Path analysis. Comparative fit index (CFI) was used to test model fit in Path analysis. SPSS version 21 (IBM, 2016) and AMOS 26 (IBM, 2016) were used for the analyses. An alpha level of <.05 was designated for statistical significance.
Since Perceived control was normally distributed, repeated analysis of variance was used to analyze the change from admission, 3 months and 6 months. Since the other six scales were not normally distributed, Friedman test and Wilcoxon signed rank test were used to compare data points. For Wilcoxon signed rank test, Bonferroni correction was applied (an alpha level of <.05/3 = 0.017) for multiple comparison. A graph was created to see the change in the value of the scale. Ratio was calculated from the value at 3 months and 6 months divided by the during admission value: mean of perceived control and median of other scales.
Pearson's correlation coefficients were used to analyze associations between perceived control during admission, 3 months and 6 months, and ACS related factors at 3 months and 6 months, and HRQoL at 3 months and 6 months. Spearman's correlation coefficients were used to analyze the associations between General health and ACS related factors for each timing at 3 months and 6 months.
6. ETHICAL CONSIDERATIONS
This study was approved by the Institutional Review Board and the Medical Research Ethics Committee of Tokyo Medical and Dental University (approval No. M2016‐103) and Showa University (No.288). The study purpose and methods were described in detail in documents and verbally, and each participant provided written informed consent. The questionnaires included the study code number, and participants were told not to include identifiers on the return envelope or questionnaires.
7. RESULTS
7.1. Characteristics of participants
A total of 178 patients were invited, and 154 (86.5%) patients agreed to participate in the three hospitals during the study period. Among them, 137 participants completed all questions of Control Attitudes Scale‐Revised and were used for the analysis (effective response rate of 89.0%). Participants' demographics are summarized in Table 1. All participants were Japanese. Average age was 62.8 (SD 11.6, range 38–93) years and 80.3% were male. Occupation was classified as full‐time job and others (including part‐time job n = 4 and no employment n = 66), and education was classified into Bachelor's degree or higher (including graduate degree n = 4) and no college degree. There were no significant differences in demographics and other key variables among the study hospitals.
TABLE 1.
Participants characteristics measured during admission
| Statistics | Values | n | |
|---|---|---|---|
| Age | Mean (SD) | 62.8 (11.6) | 137 |
| Male gender | n (%) | 110 (80.3) | 137 |
| Bachelor's degree or higher | n (%) | 58 (42.3) | 137 |
| Full‐time job | n (%) | 67 (48.9) | 137 |
| Annual income >5 million yen | n (%) | 58 (42.3) | 137 |
| Acute myocardial infarction | n (%) | 109 (79.6) | 137 |
| Number of acute coronary syndrome symptoms | Median (range) | 5 (0‐11) | 125 |
| Average fatigue level the past 1 week | Median (range) | 4 (0‐10) | 136 |
| Fatigue interference | Median (range) | 2.7 (0‐8.9) | 129 |
| Depression | Median (range) | 4 (0‐20) | 127 |
| Anxiety | Median (range) | 2 (0‐18) | 132 |
| Total score of Perceived control | Mean (SD) | 25.4 (5.3) | 137 |
| General health (health‐related quality of life) | Median (range) | 34.5 (24.7‐63.6) | 128 |
Male patients were significantly younger (t = 3.884, p < .001), had more education (p < .001), were more likely to be employed full‐time (p < .001) and were more likely to have an annual income >5 million yen (p = .005) than female patients, but there were no differences in ACS related factors between genders. The most frequent ACS symptom was Chest Pressure (64.2%), followed by Chest discomfort (61.3%) and Chest pain (60.0%). The least frequent symptom was Indigestion (10.9%).
7.2. Reliability of scales
Reliability of all scales was confirmed. Cronbach's alpha of the Control Attitudes Scale‐Revised was .822, SF‐12 was .858, FSI was .940, PHQ‐9 was .838, and GAD‐7 was .889. A Cronbach's alpha >.80 is indicative of a reliable scale.
7.3. Relationship between perceived control and HRQoL
Average total score of Control Attitudes Scale‐Revised was 25.4 (SD ± 5.3) at the time of hospitalization, and the median of each item was 2–4 (Table 2). Four questions including “If I do all the right things, I can successfully manage my heart condition” had the highest median of 4. The question “Regarding my heart problems, I feel lots of control” had the lowest median of 2 indicating that patients actually may not feel control over their current condition at the time of hospitalization (Table 2).
TABLE 2.
Summary scores of perceived control
| N = 137 | ||
|---|---|---|
| Total score of Control Attitudes Scale‐Revised | Mean (SD) | 25.4 (5.3) |
| 1 If I do all the right things, I can successfully manage my heart condition. | Median (range) | 4 (1‐5) |
| 2 I can do a lot of things myself to cope with my heart condition. | Median (range) | 4 (1‐5) |
| 3 When I manage my personal life well, my heart condition does not bother me as much. | Median (range) | 3 (1‐5) |
| 4 I have considerable ability to control my symptoms. | Median (range) | 3 (1‐5) |
| 5 a No matter what I do, or how hard I try, I just can't seem to get relief from my symptoms. | Median (range) | 4 (2‐5) |
| 6 I am coping effectively with my heart condition. | Median (range) | 3 (1‐5) |
| 7 Regarding my heart problems, I feel lots of control. | Median (range) | 2 (1‐5) |
| 8 a Regarding my heart problems, I feel helpless. | Median (range) | 4 (1‐5) |
Note: 1 (totally disagree) to 5 (totally agree).
Reverse scored items.
On the SF‐12, the median summary score of physical health was 47.8 (range 23.8–59.6) and the average summary score of mental health was 46.1 (SD 10.6). Participants reported better physical functioning (median 57.3; range 25.7–57.3) than any other subscale while General health was the subscale with the lowest score (median 34.5; range 24.7–63.6). Higher perceived control was significantly correlated with better Physical functioning (r = 0.307, p < .001), Role‐physical (r = 0.258, p = .003), General health (r = 0.408, p < .001), Vitality (r = 0.265, p = .002), Role‐emotional (r = 0.273, p = .002) and Summary score of physical health (r = 0.368, p < .001).
7.4. Factors related to perceived control
Mean total score of perceived control was significantly higher in patients with at least a Bachelor's degree (26.7 vs. 24.4, t = −2.640, p = .009), those employed full‐time (26.5 vs. 24.3, t = −2.490, p = .014), and those with an annual income >5 million yen (26.8 vs. 24.4, t = −2.843, p = .005) compared with others. There was no association between perceived control and diagnosis, age, gender, number of ACS symptoms, fatigue, depression, or anxiety in bivariate analyses.
Factors empirically known to be related with perceived control (age, gender, education, employment, income, anxiety, and depression) were forcibly entered into a linear regression with the outcome variable of total score of perceived control. However, no factors were significantly related to perceived control. In the stepwise linear regression, annual income >5 million yen (B = 2.207, 95% CI: 0.179–4.234, p = .033) and full‐time job (B = 2.074, 95% CI: 0.054–4.095, p = .044) were significantly related to higher levels of perceived control. The two variables explained 8.3% of the variance (Table 3).
TABLE 3.
Factors related to perceived control
| β | B (95% CI) | SE | p value | VIF | |
|---|---|---|---|---|---|
| Annual income >5million yen | .207 | 2.207 (0.179‐4.234) | 1.022 | .033 | 1.062 |
| Full‐time job | .195 | 2.074 (0.054‐4.095) | 1.019 | .044 | 1.062 |
Note: Linear regression (Stepwise): Adjusted R2 = 0.083, F = 5.806 (p = .004). Dependent variable: Total score of Control Attitudes Scale‐Revised.
Abbreviations: CI: confidence interval; VFI: variance inflation factor.
7.5. Factors related to HRQoL
Factors significantly related to General health in bivariate analyses were total score of perceived control (ρ = 0.391, p < .001), annual income >5 million yen (z = −2.208, p = .027), number of ACS symptoms (ρ = −0.195, p = .029), depression (ρ = −0.345, p < .001), anxiety (ρ = −0.382, p < .001), and FSI Interference Scale (ρ = −0.323, p < .001). The six variables were forcibly entered into the logistic regression with the outcome variable of General health (< or > the median 34.5), in which perceived control (OR = 1.175, 95% CI: 1.048–1.318, p = .006) and fatigue (OR = 0.727, 95% CI: 0.556–0.949, p = .019) were significantly related to General health. This model explained 44.3% of the overall variance (Table 4). When the five variables except perceived control were used for the logistic regression, annual income >5 million yen (OR = 3.214, 95% CI: 1.186–8.710, p = .022) and fatigue (OR = 0.743, 95%CI: 0.578–0.956, p = .021) were significantly related to General health. This model explained 35.7% of the variance. The difference of the two models indicates that perceived control explained 8.6% of the variance in General health.
TABLE 4.
Factors related to General health
| B | SE | OR (95% CI) | p value | |
|---|---|---|---|---|
| Perceived control a | 0.161 | 0.058 | 1.175 (1.048‐1.318) | .006 |
| Annual income >5million yen | 0.762 | 0.538 | 2.141 (0.746‐6.146) | .157 |
| Number of ACS symptoms | ‐0.066 | 0.110 | 0.937 (0.754‐1.163) | .553 |
| Fatigue (interference) | ‐0.319 | 0.136 | 0.727 (0.556‐0.949) | .019 |
| Depression (PHQ‐9) | ‐0.053 | 0.078 | 0.949 (0.814‐1.105) | .500 |
| Anxiety (GAD‐7) | ‐0.162 | 0.086 | 0.850 (0.718‐1.006) | .059 |
Note: Logistic regression (Enter): Nagelkerke R2 = 0.443. Hosmer and Lemeshow test (χ2 = 8.742, p = .365).
Abbreviations: ACS: acute coronary syndrome; CI: confidence interval; GAD‐7: Generalized Anxiety Disorder 7; OR: odds ratio; PHQ‐9: Patient Health Questionnaire 9.
Bold variables indicate statistical significance (P < 0.05).
Total score of Control Attitudes Scale‐Revised.
Figure 2 shows the relationship among demographic factors, ACS related factors, perceived control and HRQoL (General health) in a Path analyses. Model fit was acceptable (CFI = 0.909). Higher perceived control was significantly related to higher General health (β = .258, p = .001). Only one variable of annual income >5 million yen was significantly related to perceived control (β = .187, p = .029). Male gender was associated with having at least a Bachelor's degree (β = −.313, p < .001). Younger age (β = −.376, p < .001) and male gender (β = −.182, p = .023) were associated with a full‐time job. Bachelor's degree or higher (β = .270, p < .001) and full‐time job (β = .241, p = .002) were associated with an annual income >5 million yen, which was associated with higher perceived control. A higher number of ACS symptoms was associated with depression (β = .196, p = .026) and fatigue (β = .25, p = .001). Depression was associated with anxiety (β = .601, p < .001) and fatigue (β = .460, p < .001). Lower anxiety (β = −.226, p = .009) and lower fatigue (β = −.231, p = .010) were associated with higher General health.
FIGURE 2.
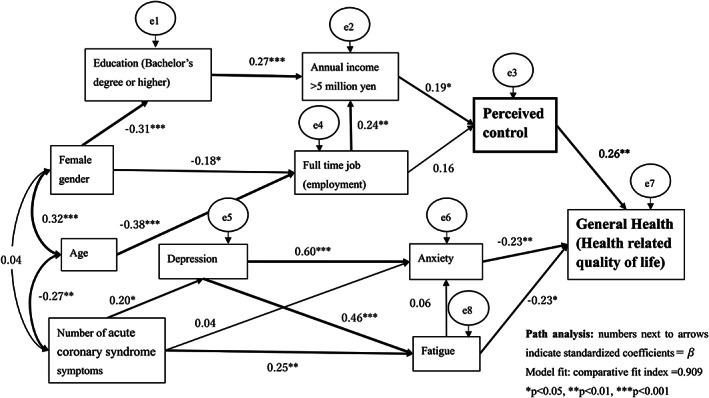
Factors related to perceived control and health‐related quality of life in Japanese patients with acute coronary syndrome
7.6. Participants at 3 months and 6 months
Among 137 patients, 82 (59.9%) at 3 months and 54 (39.4%) at 6 months completed all questions of Control Attitudes Scale‐Revised and were used for the analysis. There were no significant differences in demographics and other factors investigated during hospitalization between participants and non‐participants at 3 months or 6 months.
7.7. Change over time
Average score of perceived control was 26.7 (SD 6.2) at 3 months and 27.6 (SD 6.3) at 6 months, which indicates a significant increase from baseline (F = 7.074, p = .001). Median score of General health was 48.1 (range 24.7–63.6) at 3 months and 48.1 (range 24.7–63.6) at 6 months, which was a significant increase from baseline (χ2 = 10.22, p = .006). Number of ACS symptoms (χ2 = 38.49, p < .001), fatigue (χ2 = 22.67, p < .001), and depression (χ2 = 39.39, p = .009) significantly decreased over the 6 months. Anxiety significantly decreased at 3 months (z = −2.429, p = .015) compared to admission.
Figure 3 shows the ratio of scores for the factors at 3 months and 6 months compared to those during admission. Perceived control gradually increased, and depression and fatigue gradually decreased. General health increased, and anxiety and number of ACS symptoms decreased especially within the first 3 months after discharge.
FIGURE 3.
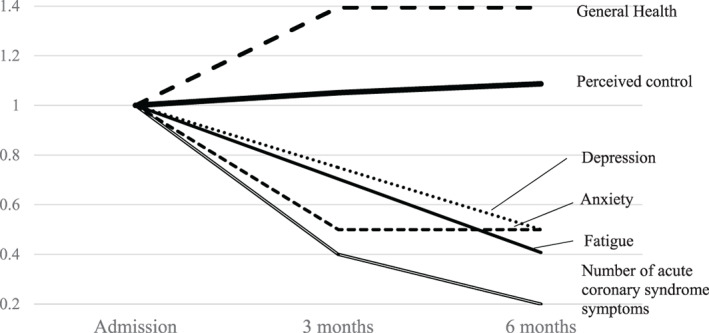
Ratio of acute coronary syndrome‐related factors, perceived control and General health compared to during hospitalization. Ratios were calculated using the average total score of perceived control and medians of other factors compared to the values of during admission
7.8. Factors of perceived control predicted after discharge
Table 5 shows association between perceived control as a predictor and outcome variables of ACS related factors and HRQoL at 3 months and 6 months after discharge. Perceived control during admission was significantly related to General health (r = 0.239, p = .035) and Vitality (r = 0.288, p = .008) at 3 months. Perceived control at 3 months was significantly related to the number of ACS symptoms (r = −0.374, p = .005), depression (r = −0.275, p = .046), anxiety (r = −0.328, p = .015), summary score of mental health (r = 0.284, p = .034), and three items of HRQoL (Role‐physical, General health, and Role‐emotional) at 6 months. Perceived control was not associated with fatigue in any time point.
TABLE 5.
Factors related to perceived control during admission, and 3 months and 6 months after discharge
| (Outcome variables) | Perceived control a (Predictor) | ||||
|---|---|---|---|---|---|
| Mean | Admission 25.4 | 3 months 26.7 | 6 months 27.6 | ||
| Median ↓ | (N = 137) | (N = 82) | (N = 54) | ||
| 3 months | Number of acute coronary syndrome symptoms | 2 | ‐0.100 | ‐0.238* | |
| Depression | 3 | 0.026 | ‐0.354** | ||
| Physical functioning | 57.3 | 0.168 | 0.342** | ||
| Role‐physical | 48.6 | 0.122 | 0.341** | ||
| Bodily pain | 57.0 | 0.067 | 0.313** | ||
| General health | 48.1 | 0.239* | 0.350** | ||
| Vitality | 49.5 | 0.288** | 0.363** | ||
| Role‐emotional | 44.0 | 0.100 | 0.327** | ||
| Summary score of physical health | 52.5 | 0.210 | 0.407*** | ||
| Summary score of mental health | 50.0 | 0.032 | 0.258* | ||
| 6 months | Number of acute coronary syndrome symptoms | 1 | ‐0.162 | ‐0.374** | ‐0.486*** |
| Depression | 2 | 0.037 | ‐0.275* | ‐0.325* | |
| Anxiety | 1 | ‐0.088 | ‐0.328* | ‐0.317* | |
| Role‐physical | 52.9 | 0.149 | 0.291* | 0.266 | |
| Bodily pain | 57 | 0.131 | 0.217 | 0.319* | |
| General health | 48.1 | 0.242 | 0.303* | 0.363** | |
| Role‐emotional | 55.5 | 0.124 | 0.287* | 0.218 | |
| Summary score of physical health | 52.2 | 0.213 | 0.260 | 0.368** | |
| Summary score of mental health | 51.6 | 0.022 | 0.284* | 0.202 | |
Note: Pearson's correlation coefficients: *p < .05, **p < .01, ***p < .001.
Total score of Control Attitudes Scale‐Revised.
7.9. Association between General health and ACS related factors after discharge
At 3 months, General health was negatively related to the number of ACS symptoms (ρ = −0.417, p < .001), fatigue (ρ = −0.493, p < .001), depression (ρ = −0.402, p < .001), and anxiety (ρ = −0.312, p = .006). At 6 months, General health was also negatively related to number of ACS symptoms (ρ = −0.565 p < .001), fatigue (ρ = −0.601, p < .001), depression (ρ = −0.602, p < .001), and anxiety (ρ = −0.470, p < .001).
8. DISCUSSION
This study explored factors related to perceived control and HRQoL of Japanese patients with ACS. This is the first study which shows the relationship between perceived control during hospitalization and HRQoL after discharge in patients with ACS. It is also the first study that measures perceived control of Japanese patients with ACS using quantitative measures and prospectively collected data. Higher perceived control was significantly related to better HRQoL. Higher income was the most important factor for higher perceived control. Higher perceived control, lower anxiety and lower fatigue were independently and significantly related to higher General health.
The average score for perceived control in this study was significantly lower than published data using the same scale on patients with MI in the USA, which were measured during hospitalization (29.1 ± 4.6; N = 513; t = 8.090, p < .001) (Moser et al., 2009). Results from this study corroborate published findings that Japanese people showed the lowest levels of perceived control among 38 nations (N = 48,951) (Hornsey, Greenaway, Harris, & Bain, 2019). However, perceived control was found to be one of the most important factors related to HRQoL in Japanese patients with ACS.
In this study, only economic status (measured by income) predicted higher perceived control. Gender, age and education were indirectly related to perceived control through income. These results are similar to previous research (Robinson & Lachman, 2017); however, depression and anxiety were not directly or indirectly related to perceived control during admission, which was different from previous research (Fatemi & Langer, 2017).
Generally, higher income is associated with better HRQoL (Dejvorakul, Kumar, Srirojanakul, Panupichit, & Somrongthong, 2019; Kikuchi et al., 2011; Mohanty & Niyonsenga, 2019; Smith et al., 2019). de Jong‐Watt and Sherifi (2011) reported that higher income and higher perceived social support were associated with greater treatment satisfaction and HRQoL in patients with ACS in a large Canadian urban center (de Jong‐Watt & Sherifi, 2011). Wang, Huang, and Zhou (2019) reported that patients diagnosed with stable angina who had a higher monthly income had better HRQoL in China. In the current study, income was not directly related to HRQoL, but was related to perceived control. Factors such as accessibility of treatment and perceived social support (de Jong‐Watt & Sherifi, 2011), as well as lifestyle factors such as exercise and sleep (Wang et al., 2019), may be related to perceived control and/or HRQoL in Japanese patients with ACS, but it is necessary to investigate how income increases perceived control.
In order to increase perceived control of Japanese patients with ACS, helping patients understand how and when to return to work is important as income is related to perceived control. Nurses should provide education on how to adapt to life after ACS, and assure the person has adequate resources to successfully manage their disease.
Perceived control of participants in this study gradually increased after discharge, but it was still lower at 6 months compared with US patients during hospitalization (Moser et al., 2009) and almost comparable with Lebanese patients 1 month after their discharge from the hospital (28.5 ± 5.8; N = 50; t = 0.756, p = .451) (Noureddine, Dumit, & Maatouk, 2019). However, higher perceived control of Japanese patients during admission could predict higher general health at 3 months. The response rate was not high enough to detect a statistically significant association between perceived control during admission and HRQoL at 6 months, but the correlation coefficient was over 0.2 indicating that perceived control and HRQoL are at least weakly correlated. Participants with higher perceived control at 3 months were less depressed, less anxious and had better HRQoL at 6 months. These results were similar to the study in the USA (Moser & Dracup, 1995). Even though perceived control of Japanese patients with ACS was lower, it may be a predictor of better health. It is necessary to further investigate how perceived control increases HRQoL of Japanese patients with ACS.
Perceived control during admission was not related to any of the ACS related factors, but perceived control at 3 months and 6 months were correlated with them. As perceived control increased after discharge, the correlation with ACS related factors increased. Therefore, lower perceived control, rather than lower depression and anxiety, may be the reason there were no associations between perceived control and depression and anxiety during admission.
9. LIMITATIONS AND FUTURE STUDIES
This study used a convenience sample from three university hospitals in the Tokyo metropolitan area; therefore, it is difficult to generalize to all Japanese patients with ACS. While adequate for analysis during admission, the sample size was smaller at the follow up time points which limited meaningful comparisons. Although data collection was extended, we were unable to increase the response rate at 3 and 6 months. Although characteristics between participants and non‐participants at 3 months and 6 months were not different, healthier patients may have participated at follow up time points, which may cause bias. A larger, more diverse sample, including patients in other cities and rural areas, is needed to better understand the perceived control of the Japanese population with ACS. In the future, it is necessary to investigate the causal relationship between perceived control, ACS related factors and HRQoL, and to explore other factors that can increase perceived control, such as social support, accessibility to health care, and lifestyle factors, instead of focusing on income.
10. CONCLUSIONS
This study explored factors related to perceived control and HRQoL of Japanese patients with ACS. Higher perceived control, lower anxiety and lower fatigue were significantly and independently related to higher General health. Income was the most important factor related to perceived control. Perceived control and General health significantly increased, and ACS related factors significantly improved after discharge, especially within the first 3 months. Higher perceived control during admission was associated with better HRQoL at 3 months. It is necessary to investigate the causal relationship and long‐term effect of perceived control on ACS related factors and HRQoL, and to explore other factors that can increase perceived control of Japanese patients with ACS in larger samples.
CONFLICT OF INTEREST
No conflict of interest has been declared by the authors.
AUTHOR CONTRIBUTIONS
Conceptualization: AK, AE, TO and AO. Data curation: AK, TO, AO and RA. Formal analysis: AK. Funding acquisition: AK, AE. Writing original draft: AK. Writing ‐ review and editing: AE. All authors critically reviewed and approved the manuscript.
ACKNOWLEDGMENTS
This study was funded by Grant‐in‐Aid for Scientific Research (C) from Japan Society for the Promotion of Science (No. 15 K11607), and an Artistic and Scholarly Development Grant from Illinois Wesleyan University. Authors thank all people who collaborated with data collection: Noriko Makino, MS, RN at Tokyo Medical and Dental University, Shoko Yoshihara, MS, RN, Hitomi Sasaki, MS, RN, Satoko Washiyama, MS, RN, Shinji Koba, PhD, MD, and Eiichi Geshi, PhD, MD at Showa University.
Kondo A, Oki T, Otaki A, Abuliezi R, Eckhardt AL. Factors related to perceived control and health‐related quality of life of patients after acute coronary syndrome during admission and after discharge. Jpn J Nurs Sci. 2021;18:e12404. 10.1111/jjns.12404
Funding information Japan Society for the Promotion of Science, Grant/Award Number: 15K11607; Artistic and Scholarly Development Grant from Illinois Wesleyan University
REFERENCES
- Alsen, P. , & Brink, E. (2013). Fatigue after myocardial infarction ‐ A two‐year follow‐up study. Journal of Clinical Nursing, 22(11–12), 1647–1652. 10.1111/jocn.12114 [DOI] [PubMed] [Google Scholar]
- American Psychiatric Association . (2018a). What are Anxiety Disorders? Retrieved from https://www.psychiatry.org/patients-families/anxiety-disorders/what-are-anxiety-disorders
- American Psychiatric Association . (2018b). What is Depression? Retrieved from https://www.psychiatry.org/patients-families/depression/what-is-depression
- Celano, C. M. , Millstein, R. A. , Bedoya, C. A. , Healy, B. C. , Roest, A. M. , & Huffman, J. C. (2015). Association between anxiety and mortality in patients with coronary artery disease: A meta‐analysis. The American Heart Journal, 170(6), 1105–1115. 10.1016/j.ahj.2015.09.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention . (2018). Health‐Related Quality of Life (HRQOL). Retrieved from https://www.cdc.gov/hrqol/index.htm
- de Jong‐Watt, W. , & Sherifi, I. (2011). Patient‐centred assessment of social support, health status and quality of life in patients with acute coronary syndrome. Canadian Journal of Cardiovascular Nursing, 21(2), 21–29. [PubMed] [Google Scholar]
- Dejvorakul, S. , Kumar, R. , Srirojanakul, S. , Panupichit, N. , & Somrongthong, R. (2019). Factors predicted with quality of life among hemodialysis patients in private hospital of Thailand. Hospital Practice (1995), 47(5), 254–258. 10.1080/21548331.2019.1682879 [DOI] [PubMed] [Google Scholar]
- Devon, H. A. , Rosenfeld, A. , Steffen, A. D. , & Daya, M. (2014). Sensitivity, specificity, and sex differences in symptoms reported on the 13‐item acute coronary syndrome checklist. Journal of the American Heart Association, 3(2), e000586. 10.1161/JAHA.113.000586 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eckhardt, A. L. , Devon, H. A. , Piano, M. R. , Ryan, C. J. , & Zerwic, J. J. (2014). Fatigue in the presence of coronary heart disease. Nursing Research, 63(2), 83–93. 10.1097/NNR.0000000000000019 [DOI] [PubMed] [Google Scholar]
- Fatemi, S. M. , & Langer, E. J. (2017). 6. Perceived control and mindfulness ‐controlling the impossibility of controllability. In Reich J. W. & Infurna F. J. (Eds.), Perceived control theory, research and practice in the first 50 years (pp. 131–146). New York, NY: Oxford University Press. [Google Scholar]
- Ferrans, C. E. , Zerwic, J. J. , Wilbur, J. E. , & Larson, J. L. (2005). Conceptual model of health‐related quality of life. Journal of Nursing Scholarship, 37(4), 336–342. [DOI] [PubMed] [Google Scholar]
- Fink, A. M. , Gonzalez, R. C. , Lisowski, T. , Pini, M. , Fantuzzi, G. , Levy, W. C. , & Piano, M. R. (2012). Fatigue, inflammation, and projected mortality in heart failure. Journal of Cardiac Failure, 18(9), 711–716. 10.1016/j.cardfail.2012.07.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frasure‐Smith, N. , & Lesperance, F. (2006). Recent evidence linking coronary heart disease and depression. The Canadian Journal of Psychiatry, 51(12), 730–737. [DOI] [PubMed] [Google Scholar]
- Gerstorf, D. , Rocke, C. , & Lachman, M. E. (2011). Antecedent‐consequent relations of perceived control to health and social support: Longitudinal evidence for between‐domain associations across adulthood. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 66(1), 61–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hann, D. M. , Denniston, M. M. , & Baker, F. (2000). Measurement of fatigue in cancer patients: further validation of the Fatigue Symptom Inventory. Quality of Life Research, 9(7), 847–854. [DOI] [PubMed] [Google Scholar]
- Hann, D. M. , Jacobsen, P. B. , Azzarello, L. M. , Martin, S. C. , Curran, S. L. , Fields, K. K. , … Lyman, G. (1998). Measurement of fatigue in cancer patients: development and validation of the Fatigue Symptom Inventory. Quality of Life Research, 7(4), 301–310. [DOI] [PubMed] [Google Scholar]
- Hornsey, M. J. , Greenaway, K. H. , Harris, E. A. , & Bain, P. G. (2019). Exploring cultural differences in the extent to which people perceive and desire control. Personality and Social Psychology Bulletin, 45(1), 81–92. 10.1177/0146167218780692 [DOI] [PubMed] [Google Scholar]
- i Hope International . (2012). MOS 36‐Item Short‐Form Health Survey. Retrieved from https://www.sf-36.jp/qol/sf12.html
- IBM . (2016). IBM Support. Retrieved from http://www-01.ibm.com/support/docview.wss?uid=swg21608060
- Kikuchi, H. , Mifune, N. , Niino, M. , Ohbu, S. , Kira, J. , Kohriyama, T. , … Kikuchi, S. (2011). Impact and characteristics of quality of life in Japanese patients with multiple sclerosis. Quality of Life Research, 20(1), 119–131. 10.1007/s11136-010-9725-2 [DOI] [PubMed] [Google Scholar]
- Lee, K. S. , Lennie, T. A. , Heo, S. , & Moser, D. K. (2012). Association of physical versus affective depressive symptoms with cardiac event‐free survival in patients with heart failure. Psychosomatic Medicine, 74(5), 452–458. 10.1097/PSY.0b013e31824a0641 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McHorney, C. A. , Ware, J. E., Jr. , & Raczek, A. E. (1993). The MOS 36‐item short‐form health survey (SF‐36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Medical Care, 31(3), 247–263. [DOI] [PubMed] [Google Scholar]
- McKinley, S. , Fien, M. , Riegel, B. , Meischke, H. , Aburuz, M. E. , Lennie, T. A. , & Moser, D. K. (2012). Complications after acute coronary syndrome are reduced by perceived control of cardiac illness. The Journal of Advanced Nursing, 68(10), 2320–2330. 10.1111/j.1365-2648.2011.05933.x [DOI] [PubMed] [Google Scholar]
- McSweeney, J. C. , O'Sullivan, P. , Cleves, M. A. , Lefler, L. L. , Cody, M. , Moser, D. K. , … Zhao, W. (2010). Racial differences in women's prodromal and acute symptoms of myocardial infarction. American Journal of Critical Care., 19(1), 63–73. 10.4037/ajcc2010372 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Melville, M. R. , Lari, M. A. , Brown, N. , Young, T. , & Gray, D. (2003). Quality of life assessment using the short form 12 questionnaire is as reliable and sensitive as the short form 36 in distinguishing symptom severity in myocardial infarction survivors. Heart, 89(12), 1445–1446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ministry of Health Labor and Welfare . (2018). Demographic statistics Monthly year meter (Abstract). Retrieved from https://www.mhlw.go.jp/toukei/saikin/hw/jinkou/geppo/nengai18/index.html
- Miyazaki, H. (2020). Factors affecting well‐being in patients with heart failure ‐focus on optimism, depression, health‐related QOL, and social interaction. Journal of School of Nursing and Social Services, Health Sciences University of Hokkaido, 16(1), 3–11 (in Japanese). [Google Scholar]
- Mohanty, I. , & Niyonsenga, T. (2019). A longitudinal analysis of mental and general health status of informal carers in Australia. BMC Public Health, 19(1), 1436. 10.1186/s12889-019-7816-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moser, D. K. , & Dracup, K. (1995). Psychosocial recovery from a cardiac event: The influence of perceived control. Heart & Lung, 24(4), 273–280. [DOI] [PubMed] [Google Scholar]
- Moser, D. K. , Riegel, B. , McKinley, S. , Doering, L. V. , Meischke, H. , Heo, S. , … Dracup, K. (2009). The control attitudes scale‐revised: Psychometric evaluation in three groups of patients with cardiac illness. Nursing Research, 58(1), 42–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muramatsu, K. (2014). An up‐to‐date letter in the Japanese version of PHQ, PHQ‐9, PHQ‐15. Niigata Seiryo University Clinical Psychological Research, 7, 35–39 (in Japanese). [Google Scholar]
- Nakamura, S. , Kato, K. , Yoshida, A. , Fukuma, N. , Okumura, Y. , Ito, H. , & Mizuno, K. (2013). Prognostic value of depression, anxiety, and anger in hospitalized cardiovascular disease patients for predicting adverse cardiac outcomes. American Journal of Cardiology, 111(10), 1432–1436. 10.1016/j.amjcard.2013.01.293 [DOI] [PubMed] [Google Scholar]
- Noureddine, S. , Dumit, N. Y. , & Maatouk, H. (2019). Patients' knowledge and attitudes about myocardial infarction. Nursing & Health Sciences, 22(1), 49–56. 10.1111/nhs.12642 [DOI] [PubMed] [Google Scholar]
- Ozawa, M. , & Ikeda, K. (2016). Relationship between health related quality of life and the learning needs in patients at risk of heart failure. Journal of Japan Health Medicine Association, 25(1), 34–46 (in Japanese). [Google Scholar]
- Pfizer, I . (n.d.). Instructions for Patient Health Questionnaire (PHQ) and GAD‐7 measures. Retrieved from https://www.ons.org/sites/default/files/PHQandGAD7_InstructionManual.pdf
- Robinson, S. A. , & Lachman, M. E. (2017). 9. Perceived control and behavior change ‐a personalized approach. In Reich J. W. & Infurna F. J. (Eds.), Perceived control theory, research and practice in the first 50 years (pp. 201–227). New York, NY: Oxford University Press. [Google Scholar]
- Sasaki, Y. , Inoue, T. , Yatomi, Y. , Suzuki, K. , & Suzuki, N. (2006). Sense‐of‐control as an index of Total recovery during the acute recovery phase of critically injured patients and nursing support for such patients: A secondary analysis. Nursing Research (Kango Kenkyu), 39(6), 509–520 (in Japanese). [Google Scholar]
- Seo, J. , Lee, Y. , Kang, S. , Chun, H. , Pyun, W. B. , Park, S. H. , … Chung, I. M. (2015). Poor health‐related quality of life and proactive primary control strategy may act as risk factors for acute coronary syndrome. Korean Circulation Journal, 45(2), 117–124. 10.4070/kcj.2015.45.2.117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shaffer, J. A. , Davidson, K. W. , Schwartz, J. E. , Shimbo, D. , Newman, J. D. , Gurland, B. J. , & Maurer, M. S. (2012). Prevalence and characteristics of anergia (lack of energy) in patients with acute coronary syndrome. The American Journal of Cardiology, 110(9), 1213–1218. 10.1016/j.amjcard.2012.06.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiroiwa, T. , Fukuda, T. , Ikeda, S. , Igarashi, A. , Noto, S. , Saito, S. , & Shimozuma, K. (2016). Japanese population norms for preference‐based measures: EQ‐5D‐3L, EQ‐5D‐5L, and SF‐6D. Quality of Life Research, 25(3), 707–719. 10.1007/s11136-015-1108-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith, G. L. , Lopez‐Olivo, M. A. , Advani, P. G. , Ning, M. S. , Geng, Y. , Giordano, S. H. , & Volk, R. J. (2019). Financial burdens of cancer treatment: A systematic review of risk factors and outcomes. Journal of the National Comprehensive Cancer Network, 17(10), 1184–1192. 10.6004/jnccn.2019.7305 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spitzer, R. L. , Kroenke, K. , Williams, J. B. , & Lowe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD‐7. Archives of Internal Medicine, 166(10), 1092–1097. 10.1001/archinte.166.10.1092 [DOI] [PubMed] [Google Scholar]
- Wang, Y. , Huang, L. , & Zhou, L. X. (2019). Correlation between exercise, personal income level and health‐related quality of life in patients with newly diagnosed stable angina. Military Medical Research, 6(1), 36. 10.1186/s40779-019-0226-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization . (2018, May 24). The Top 10 Global Causes of Deaths. Retrieved from https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death