

Abstract
Objectives
The outbreak of the COVID‐19 pandemic required rapid public compliance with advice from health authorities. Here, we ask who was most likely to do so during the first wave of the pandemic.
Design
Quota‐sampled cross‐sectional and panel data from eight Western democracies (Denmark, France, Germany, Hungary, Italy, Sweden, the United Kingdom, and the United States).
Methods
We fielded online public opinion surveys to 26,508 citizens between 19 March and 16 May. The surveys included questions about protective behaviour, perceptions of the pandemic (threat and self‐efficacy), as well as broader attitudes towards society (institutional and interpersonal trust). We employ multilevel and fixed‐effects regression models to analyse the relationship between these variables.
Results
Consistent with prior research on epidemics, perceptions of threat turn out as culturally uniform determinants of both avoidant and preventive forms of protective behaviour. On this basis, authorities could foster compliance by appealing to fear of COVID‐19, but there may be normative and practical limits to such a strategy. Instead, we find that another major source of compliance is a sense of self‐efficacy. Using individual‐level panel data, we find evidence that self‐efficacy is amendable to change and exerts an effect on protective behaviour. Furthermore, the effects of fear are small among those who feel efficacious, creating a path to compliance without fear. In contrast, two other major candidates for facilitating compliance from the social sciences, interpersonal trust and institutional trust, have surprisingly little motivational power during the first wave of the COVID‐19 pandemic.
Conclusions
To address future waves of the pandemic, health authorities should thus focus on facilitating self‐efficacy in the public.
Keywords: COVID‐19, protective behaviour, efficacy, trust, fear
Statement of contribution.
What is already known on this subject?
Health‐related fear correlates with protective behaviour during epidemics including the COVID‐19 pandemic.
Prior evidence from the COVID‐19 pandemic is based on single‐country studies and cross‐sectional designs.
What does this study add?
Cross‐national evidence that fear during COVID‐19 pandemic motivated protective behaviour.
Cross‐national survey evidence that interpersonal trust and government trust had limited motivational effect on protective behaviour.
Cross‐national, causal evidence that a clear understanding of health advice motivated protective behaviour, even in the absence of fear.
Background
In most societal crises, political leaders ask citizens to ‘keep calm and carry on’ while they seek to resolve the crisis themselves. Such an approach is not viable during an epidemic. Because pathogens travel between citizens, the growth of the epidemic is fundamentally tied to citizen behaviour (Anderson, Heesterbeek, Klinkenberg, & Hollingsworth, 2020). Citizens cannot carry on with their lives as usual; rather, they need to engage in rapid physical distancing to slow the spread of pathogens (Lewnard & Lo, 2020). Accordingly, during the outbreak of the coronavirus pandemic in 2020, governments across the globe launched interventions to facilitate the public's compliance with advice regarding avoidant (e.g., physical distancing) and preventive behaviours (e.g., increased hand‐washing).
The intensity of these interventions ranged from the use of soft power in the form of information campaigns and leadership to the use of force such as strict curfews and mandatory quarantines for large sections of the population. In democratic societies, however, there are always normative and practical limits to the use of force; repressive interventions interfere with concerns for democratic rights. Furthermore, the public's compliance with health advice in democratic societies is difficult to effectively police without a massive up‐scaling of public surveillance. Thus, in a democracy, compliance with public advice and policy is a function of citizen discretion, and, hence the authorities must rely on persuasion and voluntary compliance (Tyler & Jackson, 2014). Influence via communication requires an understanding of the psychology that this communication should tap into (Bonell et al. 2020; Van Bavel et al. 2020; West, Michie, Rubin, & Amlôt, 2020). For democratic governments' success in handling both the ongoing COVID‐19 pandemic and potential future pandemics, it is key to understand the psychological correlates that motivated citizens to comply with public health advice in the initial drastic phase of the COVID‐19 pandemic.
The present manuscript identifies and investigates key individual‐level psychological correlates and causes of self‐reported protective behaviour during the first wave of the COVID‐19 pandemic across eight Western democracies. This analysis is based on large online surveys resembling the populations of interest (N = 26,508). Building on a general theoretical framework for understanding protective behaviour, protective motivation theory, the study provides insights on the correlates and causes of protective behaviour which apply to most Western democracies and, hence, on the factors that efficient health communication from governments, health authorities, and the media needs to target in order to efficiently generate compliance among the public during new waves of the pandemic or in future pandemics.
Protective motivations during a pandemic
The outbreak of the pandemic was followed by the rapid spread of information about the threat of the coronavirus and how to cope with the virus via protective behaviours (Amidon, Nielsen, Pugfelder, Richards, & Stephens, 2021). The framework of protection motivation theory is particularly useful for understanding behaviour and motivations in such situations as individual responses to these two components of risk communication constitutes the theory's core focus. Protection motivation theory stipulates that people's motivation to comply with risk‐relevant recommendations – including in the domain of health – is a function of appraisals of the threat confronting the individual and appraisals of the individual's ability to cope with threat through compliance with recommendations (Maddux & Rogers, 1983; Rogers, 1975).
The role accorded to feelings of threat in protection motivation theory is shared with ‘numerous theories in social and health psychology’ (Sheeran, Harris, & Epton, 2014). Consistent with this, individuals who perceive themselves to be more at risk have been found to be more compliant with protective advice in epidemics more generally (Brug, Aro, & Richardus, 2009) and measures of fear of the coronavirus have been found to be major determinants of protective behaviour compliance during the COVID‐19 pandemic (Brouard, Vasilopoulos, & Becher, 2020; Harper, Satchell, Fido, & Latzman, 2020; Kachanoff, Bigman, Kapsaskis, & Gray, 2020).
Yet, according to protection motivation theory, individuals need to feel not only threatened but also efficacious for efficient protective behaviour. Following Bandura (1982), self‐efficacy is understood as a belief in the self's personal ability to engage in behaviour that protects them from a given threat, here infection with the coronavirus. Self‐efficacy therefore requires mastery of both knowledge about the coronavirus and the capability to comply with behavioural recommendations (Rippetoe & Rogers, 1987). While knowledge is sometimes assessed separately from assessments of capability, knowledge may be particularly important for self‐efficacy when confronted with a novel threat such as a new virus. Consistent with the proposed role of self‐efficacy, several strands of research demonstrate that this factor is an important predictor of protective behaviour including in epidemics (Bish & Michie, 2010; Ruiter, Abraham, & Kok, 2001; Teasdale, Yardley, Schlotz, & Michie, 2012).
From the perspective of protection motivation theory, an added psychological effect of self‐efficacy is to increase the effects of threat appraisals (Maddux & Rogers 1983; Sheeran et al., 2014). Consistent with this, meta‐analyses of research on protective behaviour against mundane threats (e.g., smoking, sunburn, stress) provide supportive evidence (Sheeran et al., 2014). However, experimental research using simulations of immediate and large‐scale threats such as pandemics and terrorist attacks finds that self‐efficacy is more predictive of compliance than feelings of threat and that self‐efficacy beliefs can generate compliance even if personal fear is low (Pearce, Lindekilde, Parker, & Rogers, 2019; Teasdale et al., 2012). Thus, in large‐scale crises where the salience of the threat is omnipresent such as a pandemic, self‐efficacy may potentially not increase but decrease the relevance of a personal sense of threat. As emphasized by Teasdale et al. (2012) prior to the outbreak of the coronavirus pandemic: ‘Coping appraisals appear to be an important, and hitherto underresearched, predictor of how people may behave in pandemics'’. Given these conflicting theoretical possibilities, it is not only important to assess the separate effects of fear and self‐efficacy but also their potential interactive effects.
While appraisals of threat and self‐efficacy have a prominent role in the psychological literature, it is also important to note that research on protective behaviour in prior epidemics suggests that threat and self‐efficacy may not be sufficient for high levels of protective behaviour (Brug et al., 2004; Leung et al., 2005). Accordingly, we also assess two other psychological predictors that may be important in the context of collectively mobilizing events such as the outbreak of a pandemic (Johnson, Dawes, Fowler, & Smirnov, 2020): interpersonal trust in fellow citizens and institutional trust in society's institutions. These forms of trust have been highlighted as major theoretical determinants of compliance with collective rules and recommendations (Ostrom, 1998; Tyler & Jackson, 2014) including in relation to the COVID‐19 pandemic (Johnson et al., 2020). Interpersonal trust entails the perception that fellow citizens are willing to follow similar norms and institutional trust entails the perception that institutions are willing to enforce the norms (Ostrom, 1998). Some prior work on protective behaviour during epidemics has indeed found that compliance is higher among individuals with higher degrees of trust (Rubin, Amlôt, Page, & Wessely, 2009; but see Fong and Chang, 2011). Also, initial work during the COVID‐19 pandemic found that geographical areas in the United States and Italy with higher levels of trust were more likely to engage in social distancing (Brodeur, Grigoryeva, & Kattan, 2020; Durante, Guiso, & Gulino, 2020). Again, it is relevant to consider both the main effects of interpersonal trust and institutional trust and their interactive effects with appraisals of threat. Thus, individuals who do not feel threatened may still engage in protective behaviour as a contribution to the collective project of halting infection spread (Johnson et al., 2020) and, hence, feelings of threat may be less important for compliance among individuals high in trust.
The present study
While some evidence already exists of the predictors of behaviour during the COVID‐19 pandemic, none of these published studies have considered how these alternative non‐threat‐related psychological factors may interact with feelings of threat to shape protective behaviour. This is particularly important because prior evidence suggests that in extremely salient crises – such as the COVID‐19 pandemic – trust in the self (i.e., self‐efficacy) or others may make feelings of threat less rather than more predictive of compliant behaviour. Consequently, the aim of this study is to empirically assess the following two research questions: First, to what extent are feelings of threat, self‐efficacy, interpersonal trust, and institutional trust positively associated with protective behaviours during the outbreak of the COVID‐19 pandemic? Second, to what extent and in what direction, does feelings of threat interact with self‐efficacy, interpersonal trust, and institutional trust in predicting protective behaviours during the outbreak of the COVID‐19 pandemic? In addition to the theoretical contributions underlying these two research questions, the present study also contributes to the existing literature in two other ways: First, the present study seeks to establish generalizable findings by utilizing large‐scale representative surveys in eight countries during the first wave of the COVID‐19 pandemic (N = 26,508). Second, while most of the results remain correlational, we are able to use a longitudinal component in the data to increase causal leverage.
Materials and methods
Data
We fielded surveys in eight countries during the first wave of the COVID‐19 pandemic: Denmark, France, Germany, Hungary, Italy, Sweden, the United Kingdom (UK), and the United States of America (USA). The sampled set of countries were chosen to represent the diversity of national responses to the COVID‐19 pandemic as well as the diversity in the severity of the local epidemic (see further discussion below). In each of the eight countries, the survey firm Epinion sampled adult respondents using online panels. To increase representativity, survey respondents were quota‐sampled to match the population margins on age, gender, and geographic location of each of the eight countries in our study. All participants provided informed consent, and the study was conducted in accordance with the guidelines of the Danish National Committee of Health Research Ethics for survey research that do not involve human biological material. All data and required code are publicly available in a repository at the webpage of the Open Science Framework: osf.io/asczn. We utilize two samples during the first wave of the COVID‐19 pandemic. First, a cross‐sectional sample collected between 19 March and 3 April including 26,508 respondents overall (Table S1 provides country‐specific starting dates). Second, a panel sample that includes 10,569 respondents who were observed at least twice for a total of 24,720 observations in the period between 13 March and 16 May. In this sample, we observe key measures over time and are able to increase causal leverage (see Appendix S1 for further details on the samples and the data collection process).
Measures
Following prior research on behaviour during epidemics (Bish & Michie, 2010), we assess two types of protective behaviour: avoidant and preventive. Avoidant behaviours include physical distancing, such as avoiding crowds or hugging and kissing people outside your close family. Preventive behaviours include hygienic precautions (e.g., hand‐washing or coughing into ones sleeve).
To assess avoidant behaviours, respondents were asked: (1) Did you shake someone's hand yesterday? (2) Did you hug or kiss someone outside your closest family yesterday? (3) Were you in a room with more than 10 people yesterday? (4) Did you use public transport yesterday? (5) Were you careful yesterday to keep your distance from elderly and chronically ill people? And (6) to what degree were you careful yesterday to keep your distance from people outside your closest family? To assess preventive behaviours, respondents were asked: (1) When you coughed and/or sneezed yesterday, did you do this in your sleeve each time? And (2) how many times do you estimate that you washed your hands or used hand sanitizer yesterday?
For each type of behaviour, we add together these items to form indexes of avoidant and preventive behaviour, respectively. Each index is scaled to vary between 0 and 1 with higher values reflecting a higher degree of protective behaviour. In addition to these outcomes, we also obtained a measure that directly asked respondents whether they changed their behaviour during the COVID‐19 pandemic in order to avoid spreading the infection. For the cross‐sectional sample, we report analyses with this measure as an alternative outcome in the supplementary materials (see Appendix S2). All analyses replicate those presented in the main text.
To examine key correlates of protective behaviour, we assessed (1) appraisals of threat, (2) self‐efficacy, (3) interpersonal trust, and (4) institutional trust.
To measure appraisals of threat, we focus on individual‐level worries related to the coronavirus. Specifically, we create an index that adds together three items that directly measure the extent to which our respondents are concerned about the consequences of the coronavirus: To what degree are you concerned about the consequences of the coronavirus … (1) for yourself? (2) for your family? and (3) for your close friends? Respondents answered on 4‐point scale from ‘not at all’ to ‘to a high degree’. Together, the three items form a reliable scale, α = .83, scaled to range from 0 to 1, with higher values indicating higher worry.
To measure self‐efficacy, we rely on a five‐item scale.1 As noted, self‐efficacy requires mastery of both knowledge about how specific measures can protect against COVID‐19 and a feeling of being capable of following protective advice (Bandura, 1982; Rippetoe & Rogers, 1987). While the first four items in our self‐efficacy scale tap into the knowledge dimension of mastery, the fifth item taps into the capability dimension. The first four items ask: To what degree do you feel that you know enough about …(1) how to avoid being infected and/or infecting others with the coronavirus? (2) the symptoms of the coronavirus? (3) what you should do if you fall ill with the coronavirus? (4) what you as a citizen should do in relation to the coronavirus? On these questions, respondents answered on a 4‐point scale from ‘not at all’ to ‘to a high degree’. The fifth item asked: To what extent do you agree or disagree with the following statement: I'm certain I can follow official advice to ‘distance myself’ from others if I want to. Here, respondents answered on a 5‐point scale from ‘disagree completely’ to ‘agree completely’. The five items form a reliable scale as measured by alpha (α = .79). For the final index, we add together the five times and scale it to range from 0 to 1 with higher values indicating more efficacy.2
To measure interpersonal and institutional trust, we use standard measures. On interpersonal trust, we ask respondents: ‘Do you think that most people by and large are to be trusted, or that you cannot be too careful when it comes to other people?’. On institutional trust, we ask: ‘On a scale from 0 to 10, how much confidence do you personally have in the government?’.
In the analyses, we also include a battery of demographic control variables (see below). Table S10 provides descriptive statistics for all variables in our pooled sample, while Tables S11‐S18 provide the descriptives by country.
In the panel sample, not all measures were available. As discussed below, the panel sample focuses on the potential causal effect of self‐efficacy on protective behaviour. To this end, we have one repeated measure of self‐efficacy available (specifically, the question: ‘To what degree do you feel that you know enough about what you as a citizen should do in relation to the coronavirus?’) and three repeated measures of protective behaviour are available: (1) avoiding crowds, (2) washing hands, and (3) the alternative outcome that more broadly assess whether respondents changed their behaviour in order to avoid spreading the infection. We summarize these three measures into a modified index of protective behaviour (see Appendix S2 for details).
Statistical analysis
To answer the research questions, we use the cross‐sectional sample and regress protective behaviour on each psychological predictors (perceived worry, self‐efficacy, interpersonal trust, and institutional trust) separately, while controlling for a battery of covariates (age, sex, education, occupation, income, and vote choice). In this benchmark model, data are pooled from all countries and we use multilevel modelling to account for the fact that observations are nested within countries. Specifically, we fit models with random intercepts for country and time. Moreover, the slopes of the psychological correlates are allowed to vary by country (given that likelihood ratio tests show that random slope models fit the data better compared to the random intercepts‐only models). The models provide the overall correlations between protective behaviour and each psychological predictor across all countries, as well as country‐specific deviations from the overall patterns.3
In addition, we use the panel sample to estimate the causal impact of a change in self‐efficacy on protective behaviour using individual‐level linear fixed‐effects models. Individual‐level fixed‐effects control for stable individual differences (i.e., time‐invariant confounders) in protective behaviour by only using within‐individual variation in self‐efficacy and protective behaviour. Instead of comparing protective behaviour among individuals with high versus low levels of self‐efficacy, we estimate how protective behaviour changes when a respondent reports changes in their self‐efficacy compared to an earlier interview. To account for potential time trends in protective behaviour, we also include time fixed effects. To correct for clustering in self‐efficacy, we cluster standard errors by individual and time. The two‐way fixed‐effects estimator gives an unbiased estimate of the causal impact of self‐efficacy on protective behaviour on the assumption that the protective behaviour of individuals had followed parallel trends in the absence of changes in efficacy (Angrist & Pischke, 2008). In the supplementary materials, we provide tests that support that this assumption is valid here (see Appendix S2 for details).
In the analyses, all measures are scaled to range from 0 to 1. Accordingly, the size of the estimated correlations (in the cross‐sectional sample) and effects (in the panel sample) reported below reflect the change in the outcome variable when we compare individuals at the minimum and maximum values of each of the independent variables. All reported p‐values are from two‐sided tests.
Results
Descriptive levels of protective behaviour across countries
Before turning to examining the proposed research questions, we begin by providing descriptive results regarding the pandemic context of the sampled countries as well as the level of protective behaviour in each country. To this end, Figure 1 displays information about the pandemic severity, the government response, and the levels of observed preventive and avoidant behaviour for each country. To represent differences in government strategies, a dashed line plots a measure of the stringency of government responses to the COVID‐19 pandemic over the survey period (Hale, Webster, Petherick, Phillips, & Kira, 2020). This is a composite measure of the number of non‐pharmaceutical interventions taken in a specific country (e.g., school closings and curfews). The bars display the count of COVID‐19 infections per capita as an indicator of the severity of the local epidemic (also taken from Hale et al., 2020). In addition, Figure 1 plots levels of protective behaviours as a function of time. The solid black lines represent avoidant behaviour and the solid grey lines represent preventive behaviour.
Figure 1.
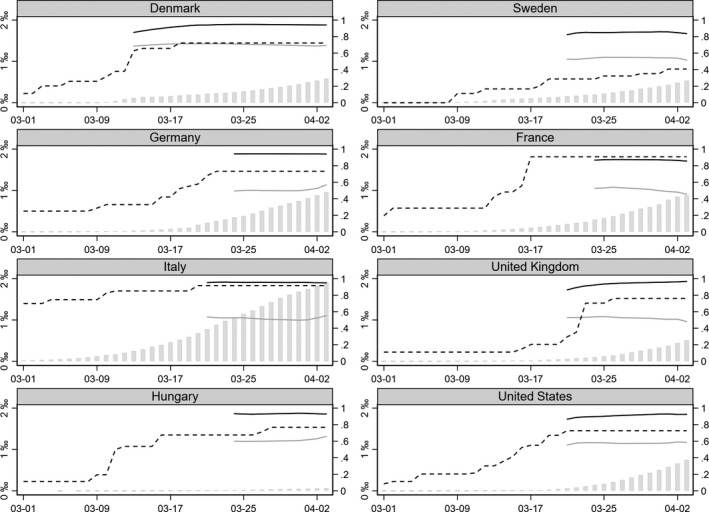
Selection of countries for data collection. Note: Solid black (avoidant behaviour) and grey (preventive) lines are the developments in the present measures of self‐reported protective behaviour. Dashed lines are the developments in policy stringency (Hale et al.,2020). Grey bars display the developments in the COVID‐19 case counts per capita.
There is substantial variation in the severity of the local epidemic across countries and, while all countries have implemented some form of stringent measures, there is also substantial variation with Sweden having the less stringent response and Italy and France the most stringent responses. Independently of both stringency and severity, however, the level of protective avoidant behaviour is exceptionally high. At the same time, we observe significantly lower, but similarly stable, levels of preventive behaviour across the countries.
Main correlations between protective behaviour and psychological predictors
To answer our first key research question, Figure 2 displays the estimated correlations between each of the protective behaviour measures and the psychological correlates.4 Worry correlates positively with both avoidant and preventive behaviour such that people who are more worried are more likely to comply with the protective advice on each measure. Whereas we observe a marked correlation between preventive behaviour and worry (), the correlation with avoidant behaviour is more moderate (). In contrast, self‐efficacy is relatively strongly correlated with both types of protective behaviour. Compared to the least efficacious, the most efficacious are hence about 11 percentage points more likely to display avoidant behaviour () and about 19 percentage points more likely to display preventive behaviour (). Against the theoretical expectation, interpersonal trust is negatively related to both types of behaviour () such that respondents who trust most other people are less likely to comply with protective advice. Finally, institutional trust has a small but statistically significant positive association with avoidant behaviour (), whereas its correlation with preventive behaviour is somewhat larger ().
Figure 2.
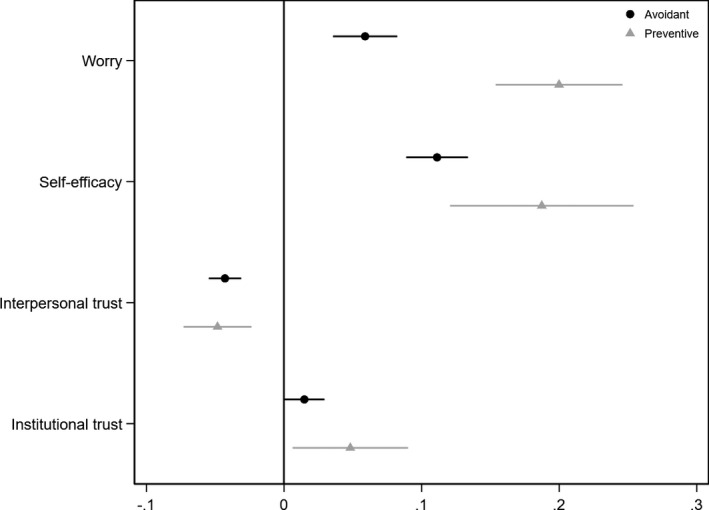
Correlations between protective behaviour and psychological correlates. Note: Correlations from our benchmark model. Filled black circles (grey triangles) show the estimated country‐specific correlations between each of the psychological variables and avoidant behaviour (preventive behaviour). Error bars are 95% confidence intervals.
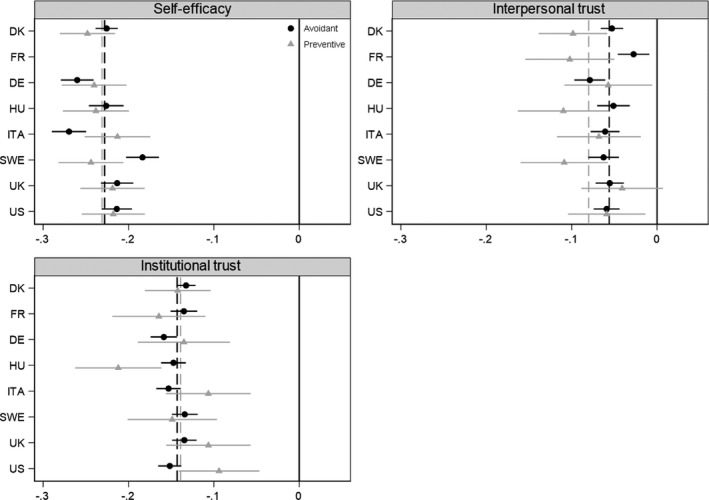
While the correlations in Figure 2 identify the average correlations with protective behaviours, they potentially mask heterogeneity across countries. To investigate this heterogeneity, we utilize the benchmark model to extract the country‐specific correlations in Figure 3. Each filled black circle (grey triangle) shows an estimated country‐specific correlation between the respective psychological variables and avoidant behaviour (preventive behaviour). The black (grey) dashed lines refer to the estimated overall associations between each of the psychological variables and avoidant behaviour (preventive behaviour) from Figure 2. If the confidence intervals overlap the dashed lines, it means that the country‐specific slope is not statistically significantly different from the overall mean slope. On the whole, Figure 3 shows that the estimated correlations are strikingly uniform across the countries.
Figure 3.
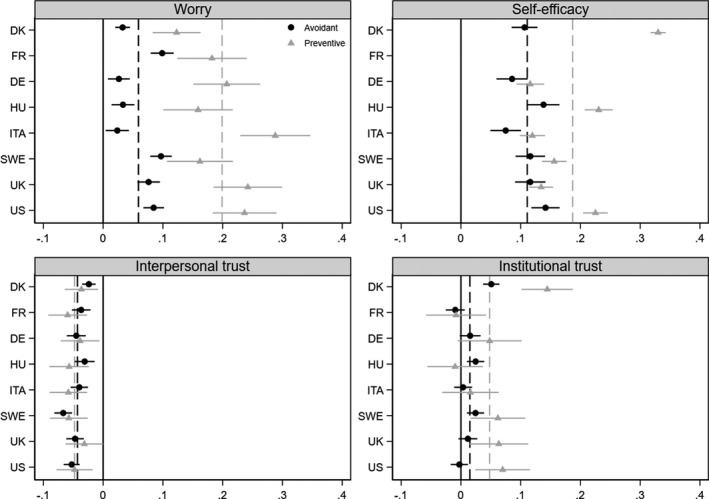
Country‐specific correlations between protective behaviour and psychological correlates. Note: Filled black circles (grey triangles) show the estimated country‐specific correlations between each of our psychological variables and avoidant behaviour (preventive behaviour). Black (grey) dashed lines refer to the estimated overall associations in Figure 2. Error bars are 95 % confidence intervals that show whether the country‐specific correlations are statistically significantly different from overall associations
Interactions between worry and alternative psychological motivations
Our second key research question focuses on the potential interactions between worry, on the one hand, and the other set of psychological correlates, on the other. We examine these potential interactions by re‐specifying the benchmark models such that they include a linear interaction between worry and each of the remaining psychological correlates, respectively. Figure 4 shows the results from these moderation analyses. The solid grey lines show predicted compliance over the range of worry at low levels on the respective moderators, the dashed lines show predicted compliance at medium levels, while solid black lines show compliance at high levels.
Figure 4.
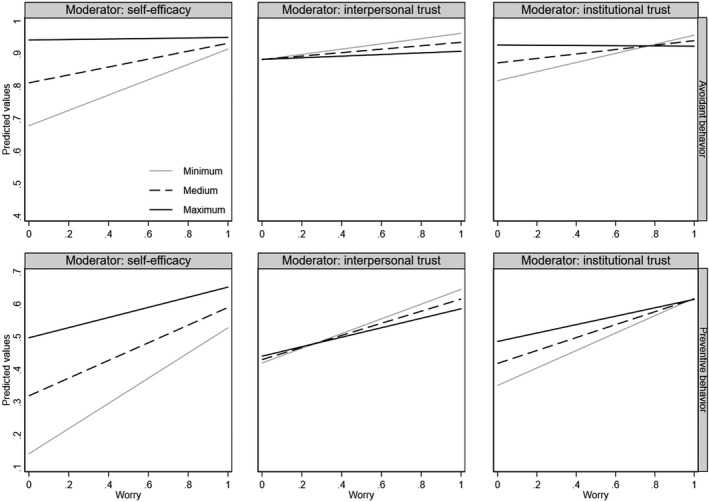
Do self‐efficacy and trust moderate the correlation between worry and protective behaviour? Note: Solid black lines show predicted values at high levels of each moderator, black dashed lines show predicted values at medium levels, and solid grey lines show predicted values at low levels
For self‐efficacy (top‐left panel), we observe a substantive and statistically significant moderation of the association between worry and avoidant behaviour (). Among those with minimal levels of self‐efficacy, worry has a substantial effect on avoidant behaviour such that the difference in predicted values among those who feel worried and those who do not is 0.24 (). Among those with maximal levels of self‐efficacy, however, this difference is statistically indistinguishable from 0. For preventive behaviour (bottom‐left panel), we observe a similar empirical pattern. The difference in preventive behaviour between those who are worried and those who are not is largest at low levels of self‐efficacy and decreases as self‐efficacy increases ().
On institutional trust, we similarly find that worry is significantly and substantively moderated by institutional trust. For avoidant behaviour (top‐right panel), we observe a substantive and statistically significant decrease in the difference between the worried and unworried () from 0.14 () at low levels of institutional trust to 0 () at high trust levels. For preventive behaviour (bottom‐right panel), we similarly observe that the difference decreases from 0.27 () at minimal levels of institutional trust to 0.13 () at maximal trust levels.
On interpersonal trust, we observe more modest moderations for both types of behaviour (). On avoidant behaviour, the difference between the worried and unworried decreases from 0.08 () at low levels of trust to 0.02 () at high level of trust. On preventive behaviour, the decrease reflects a change from 0.23 () at low trust levels to 0.15 () at high trust levels.5
Figure 5 displays the consistency of these interactions across the countries in our sample. For each country, the black filled circles (grey triangles) show the estimated country‐specific interaction between worry and each of the moderators on avoidant (preventive) behaviour. If the confidence intervals overlap the dashed black (grey) lines, the country slopes are not statistically distinguishable from overall mean slope on the specific interaction term. Overall, we find the interactions to be relatively consistent across cultures, suggesting that the substantive patterns observed in Figure 4 apply across the different countries in our sample.
Figure 5.
Country‐specific moderations. Note: Filled black circles (grey triangles) show the estimated country‐specific moderations. Error bars are 95 % confidence intervals that show whether the country‐specific moderations are statistically significantly different from overall moderations (see Figure 4)
Assessing longitudinal effects of self‐efficacy on protective behaviour
The above analyses highlight the importance of self‐efficacy for protective behaviour during the outbreak of a pandemic. To increase the causal leverage of any conclusions regarding this key variable, we utilize the panel sample and estimate the effect of self‐efficacy on protective behaviour using the two‐way fixed‐effects estimator. We observe a substantial effect of efficacy of 0.06 () (see Table S19). Additional analyses show that this effect is relatively homogeneous across countries and varies between () and () (see Figure S16).
Discussion
In this study, we asked two research questions: First, to what extent does appraisals of threat, self‐efficacy, interpersonal trust, and institutional trust predict protective behaviour during the first wave of the coronavirus pandemic? Second, does self‐efficacy and trust moderate the effects of feelings of threat on protective behaviour?
We found extremely high levels of avoidant behaviour (e.g., physical distancing) in all countries and medium to high levels of preventive behaviour (e.g., increased hand‐washing) across the countries. Most likely, this reflects that policy measures during the first wave of the pandemic were particularly targeted towards fostering avoidant behaviour in the form of distancing. In answering the first research question, we found that individual‐level variation in these protective behaviours strongly reflected individual‐level differences in threat appraisals (i.e., self‐assessed worry) and self‐efficacy but not measures of trust. In answering the second research question, we found strong evidence that individual‐level differences in self‐efficacy decreased the importance of threat as a predictor of protective behaviour and also found some evidence that the trust measures similarly negatively moderated the association between threat and protective behaviour. Finally, additional analyses using panel data suggested (1) that efficacy is amendable to change and does not just reflect a set of stable traits and (2) that changes in efficacy causally impact protective behaviour.
Several years prior to the coronavirus pandemic, Teasdale et al. (2012) used protection motivation theory to argue that self‐efficacy could be ‘an important, and hitherto under‐researched, predictor of how people may behave in pandemics’'. Overall, the present findings provide direct evidence for this assertion during the outbreak of an actual pandemic. Furthermore, the findings extend previous studies of protective motivations by suggesting that self‐efficacy may be even more important in the face of exceptionally salient threats such as a pandemic. Thus, prior research on protection motivation in the context of mundane threats (e.g., smoking, sunburn, and stress) suggests that self‐efficacy enhances the effects of threat appraisals (Sheeran et al., 2014). In contrast, we found that high levels of self‐efficacy made individual‐level feelings of threat almost irrelevant for engagement in the protective behaviours promoted by authorities worldwide during the COVID‐19 pandemic, providing a pathway to compliance without fear.6
This finding might be key for health communication during both the current and future pandemics. Thus, the risk profile of many diseases including COVID‐19 is highly asymmetric with some individuals being more at risk (Jordan, Adab, & Cheng, 2020). As physical distancing and other protective measures are most effective if most parts of society comply (Anderson et al. 2020), such asymmetries imply that health communication that exclusively focuses on personal risk and threat may not motivate sufficiently high levels of protective behaviour. Instead, the present findings suggest that an alternate and more effective focus for health communication is self‐efficacy. A focus on promoting self‐efficacy rather than fear may also be normatively desirable. While an increased sense of threat may increase compliance, it can entail mental health costs (Ornell, Schuch, Sordi, & Kessler, 2020) and increase the acceptance of undemocratic treatments of other groups (Marcus, Theiss‐Morse, Sullivan, & Wood, 1995).
The fact that individual differences in trust were not strongly associated with compliance during the outbreak of the COVID‐19 pandemic also has important theoretical implications. In particular, it is relevant to note that people high in interpersonal trust were less likely to engage in protective behaviours compared to people low in interpersonal trust across all countries. While unexpected, this effect is consistent with some prior findings on the relationship between trust and protective behaviour during epidemics (Fong & Chang, 2011; Lear, 1995). While trust may increase other forms of protective behaviour, the trusting mindset seems to make it psychologically difficult to treat others as infection threats (see Aarøe, Osmundsen, and Petersen, 2016). For institutional trust, the inconsistent and weak correlations between protective behaviour and institutional trust may be viewed as welcome news. According to the present data, political views and polarization does not necessarily jeopardize compliance in the outbreak of a massive global crisis like a pandemic, although it may naturally influence compliance at later stages (see Gollwitzer et al., 2020).
These conclusions notwithstanding three important limitations of the present study should be noted. First, results from the cross‐sectional analyses are limited in terms of causality, and while the applied two‐way fixed‐effects estimator controls away all time‐invariant unobserved heterogeneity, it does not control for time‐varying factors that may still bias our estimates. Future research should seek to corroborate our findings relying on more longitudinal and experimental designs including to assess how the interaction between threat appraisals and self‐efficacy may change as a function of the magnitude of the crisis. Second, the study relied on high‐quality online panels for recruiting in our participants and not random probability sampling. Accordingly, the samples may be systematically different to the national population, for example in terms of digital literacy. This sampling bias may increase due to non‐response. In the present study, response rates for the individual countries vary between 18 and 38 % and may imply that the samples are biased towards those most interested in or concerned about the pandemic. Third, it is relevant to note that social desirability may bias the present findings. At the same time, several recent studies have assessed whether or not participants over‐report compliance when asked about protective behaviour in the context of the COVID‐19 pandemic. Most of these studies find no evidence to suggest that self‐reports of protective behaviour are tainted by social desirability bias (Galasso et al., 2020; Larsen, Nyrup, & Petersen, 2020; Munzert & Selb, 2020). Furthermore, the exceptional high levels of reported avoidant behaviour are consistent with studies from the United States using actual behavioural measures (Lee et al., 2020) . These observations suggest that social desirability may not be a major factor in the context of the present studies.7
Conclusion
The present findings demonstrate that self‐efficacy was both necessary and sufficient for protective behaviour during the first wave of the COVID‐19 pandemic and constitutes a pathway to compliance with pandemic health advice not driven by personal fear. Seemingly, the salience of the emergency created an unprecedented motivation to obtain and act on health advice, while ignoring other common psychological considerations including those related to fear as well as trust in fellow citizens and political institutions. Accordingly, the findings suggest that a major focus during the current and future pandemics should be on providing clear information about protective behaviour and formulating guidelines that facilitate a sense of self‐efficacy in the public. To facilitate society‐wide protective behaviour during a massive crisis such as the first wave of COVID‐19 pandemic, the establishment of a strong sense of self‐efficacy is key.
Conflict of interest
All authors declare no conflict of interest.
Author contributions
Frederik Jørgensen (Conceptualization; Data curation; Formal analysis; Methodology; Writing – original draft; Writing – review & editing). Alexander Bor (Conceptualization; Data curation; Formal analysis; Methodology; Writing – original draft; Writing – review & editing). Michael Bang Petersen (Conceptualization; Data curation; Funding acquisition; Project administration; Writing – original draft; Writing – review & editing).
Supporting information
Appendix S1. Materials and methods.
Appendix S2. Supporting results.
Acknowledgements
This study was funded by grant CF20‐0044 from the Carlsberg Foundation to Michael Bang Petersen.
Footnotes
Due to a programming error, we did not observe self‐efficacy in France. Consequently, French respondents are left out of models including this measure.
Although the scale covers both aspects in the theoretical definition of self‐efficacy, we would ideally have observed more items that directly measure the capability dimension. Empirically, however, there is significant evidence that the utilized scale in fact measures a single latent trait of self‐assessed mastery. First, the findings are not an artefact of the scale construction. Hence, we rerun our analyses while including only the capability item as a measure of self‐efficacy (i.e., the agreement with the statement: I'm certain I can follow official advice to ‘distance myself’ from others if I want to). These analyses show that all results replicate those in the main manuscript (see Appendix S2 for details). Note, we are unable to repeat this analysis for the longitudinal results because we, unfortunately, do not measure both dimensions of self‐efficacy repeatedly. Second, beyond the evidence provided by the satisfactory alpha‐value, we conducted a polychoric PCA, which demonstrates that the five items clearly load on only one dimension. Specifically, the first component in the polychoric PCA has an eigenvalue of 3.20, while the second component's eigenvalue is 0.80. Third, to assess the consequence that the scale includes more items reflecting knowledge than capability, we also created an alternative scale where the items for each component were equally weighted (i.e., 50 % each). This alternative scale is highly correlated with our preferred scale (r =.91), suggesting again that the used scale does indeed reflect one single trait of self‐efficacy.
The supplementary materials include results from a full model that includes all psychological predictors as well as all demographics in the same model. All analyses replicate those presented in the main text (see Appendix S2).
For correlates between protective behaviour and demographic variables, see Figure S1).
Following the advice of (Hainmueller et al. 2019), we test the robustness of these linear interactions in Appendix S2. Figure S14 shows the binned estimator that provides no evidence for non‐linearities in the interactions. Figure S15 shows the more flexible kernel estimator. Although it should be noted that there is some tendency for a curvilinear interaction between worry and self‐efficacy on preventive behaviour, it is crucial that this observed curvilinearity is driven by very few observations. For more than 95 per cent of the observations, we observe a linear negative moderation (please see the distribution on the self‐efficacy moderator in Appendix S1). Altogether, this corroborates the robustness of the results.
While efficacious individuals may not need to feel personally threatened in order to comply, it is possible to ask whether they do need to feel that society as such is threatened by COVID‐19? To assess this, we conducted additional analyses, reported in Appendix S2, which replicated the findings using a measure of feelings of societal threat. Hence, during first wave of the COVID‐19 pandemic, efficacious individuals did not need to feel that they or society was threatened in order to comply.
Nonetheless, in Appendix S2, we seek to directly limit any confounding from social desirability bias using the personality trait of agreeableness. The personality trait of agreeableness is a trait that is frequently discussed as a potential target of social desirability bias (Graziano and Tobin 2002). Independently of the larger research question of how much agreeableness is tainted by social desirability, it is clear that people who report that they lack agreeableness are willing to disclose socially undesirable traits. We make use of this fact and subset our analyses to the bottom half of the agreeableness scale and find that results replicate among individuals who are not unwilling to disclose undesirable behaviours and attitudes.
Data availability statement
Replication data and code are publicly available here at Open Science Framework: https://osf.io/asczn/.
References
- Aarøe L., Osmundsen M., Petersen M. B. (2016). Distrust As a Disease Avoidance Strategy: Individual Differences in Disgust Sensitivity Regulate Generalized Social Trust. Frontiers in Psychology, 7, 1–14. 10.3389/fpsyg.2016.01038 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Amidon, T. R. , Nielsen, A. C. , Pugfelder, E. H. , Richards, D. P. , & Stephens, S. H. (2021). Visual risk literacy in “flatten the curve” covid‐19 visualizations. Journal of Business and Technical Communication, 35(1), 101–109. 10.1177/1050651920963439 [DOI] [Google Scholar]
- Anderson, R. M. , Heesterbeek, H. , Klinkenberg, D. , & Hollingsworth, T. D. (2020). How will country‐based mitigation measures influence the course of the covid‐19 epidemic? The Lancet, 395, 931–934. 10.1016/S0140-6736(20)30567-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Angrist, J. D. , & Pischke, J.‐S. (2008). Mostly harmless econometrics: An empiricist's companion. Princeton, NJ: Princeton University Press. [Google Scholar]
- Bandura, A. (1982). Self‐efficacy mechanism in human agency. American Psychologist, 37, 122–147. 10.1037/0003-066X.37.2.122 [DOI] [Google Scholar]
- Bavel, J. J. V. , Baicker, K. , Boggio, P. S. , Capraro, V. , Cichocka, A. , Cikara, M. , … Willer, R. (2020). Using social and behavioural science to support covid‐19 pandemic response. Nature Human Behaviour, 4, 460–471. 10.1038/s41562-020-0884-z [DOI] [PubMed] [Google Scholar]
- Bish, A. , & Michie, S. (2010). Demographic and attitudinal determinants of protective behaviours during a pandemic: a review. British Journal of Health Psychology, 15, 797–824. 10.1348/135910710X485826 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bonell, C. , Michie, S. , Reicher, S. , West, R. , Bear, L. , Yardley, L. , … Rubin, G. J. (2020). Harnessing behavioural science in public health campaigns to maintain “social distancing” in response to the covid‐19 pandemic: key principles. Journal of Epidemiology and Community Health, 74(8), 617–619. 10.1136/jech-2020-214290 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brodeur, A. , Grigoryeva, I. , & Kattan, L. (2020). Stay‐at‐home orders, social distancing and trust. IZA Discussion Paper No. 13234, Available at SSRN: https://ssrn.com/abstract=3602410 [DOI] [PMC free article] [PubMed]
- Brouard, S. , Vasilopoulos, P. , & Becher, M. (2020). Sociodemographic and psychological correlates of compliance with the covid‐19 public health measures in France. Canadian Journal of Political Science, 53, 253–258. 10.1017/S0008423920000335 [DOI] [Google Scholar]
- Brug, J. , Aro, A. R. , Oenema, A. , De Zwart, O. , Richardus, J. H. , & Bishop, G. D. (2004). Sars risk perception, knowledge, precautions, and information sources, the Netherlands. Emerging Infectious Diseases, 10, 1486. 10.3201/eid1008.040283 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brug, J. , Aro, A. R. , & Richardus, J. H. (2009). Risk perceptions and behaviour: towards pandemic control of emerging infectious diseases. International Journal of Behavioral Medicine, 16(1), 3–6. 10.1007/s12529-008-9000-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Durante, R. , Guiso, L. , & Gulino, G. (2020). Asocial capital: Civic culture and social distancing during COVID‐19. Journal of Public Economics, 194(104342), 1–17. 10.1016/j.jpubeco.2020.104342 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fong, E. , & Chang, L.‐Y. (2011). Community under stress: Trust, reciprocity, and community collective efficacy during sars outbreak. Journal of Community Health, 36, 797–810. 10.1007/s10900-011-9378-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galasso, V. , Pons, V. , Profeta, P. , Becher, M. , Brouard, S. , & Foucault, M. (2020). Gender differences in covid‐19 attitudes and behavior: Panel evidence from eight countries. Proceedings of the National Academy of Sciences, 117, 27285–27291. 10.1073/pnas.2012520117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gollwitzer, A. , Martel, C. , Brady, W. J. , Pärnamets, P. , Freedman, I. G. , Knowles, E. D. , & Van Bavel, J. J. (2020). Partisan differences in physical distancing are linked to health outcomes during the covid‐19 pandemic. Nature Human Behaviour, 4, 1186–1197. http://doi.or/10.1038/s41562‐020‐00977‐7 [DOI] [PubMed] [Google Scholar]
- Graziano, W. G. , & Tobin, R. M. (2002). Agreeableness: Dimension of personality or social desirability artifact? Journal of Personality, 70, 695–728. 10.1111/1467-6494.05021 [DOI] [PubMed] [Google Scholar]
- Hainmueller, J. , Mummolo, J. , & Xu, Y. (2019). How much should we trust estimates from multiplicative interaction models? Simple tools to improve empirical practice. Political Analysis, 27, 163–192. 10.1017/pan.2018.46 [DOI] [Google Scholar]
- Hale, T. , Webster, S. , Petherick, A. , Phillips, T. , & Kira, B. (2020). Oxford covid‐19 government response tracker. Blavatnik School of Government, 25. https://covidtracker.bsg.ox.ac.uk/ [DOI] [PubMed] [Google Scholar]
- Harper, C. A. , Satchell, L. P. , Fido, D. , & Latzman, R. D. (2020). Functional fear predicts public health compliance in the covid‐19 pandemic. International Journal of Mental Health and Addiction, 1–14. 10.1007/s11469-020-00281-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson, T. , Dawes, C. , Fowler, J. , & Smirnov, O. (2020). Slowing COVID‐19 transmission as a social dilemma: Lessons for government officials from interdisciplinary research on cooperation. Journal of Behavioral Public Administration, 3(1).1–13. 10.30636/jbpa.31.150 [DOI] [Google Scholar]
- Jordan, R. E. , Adab, P. , & Cheng, K. K. (2020). Covid‐19: risk factors for severe disease and death. BMJ, 368, 1–2. 10.1136/bmj.m1198 [DOI] [PubMed] [Google Scholar]
- Kachanoff, F. , Bigman, Y. , Kapsaskis, K. , & Gray, K. (2020). Measuring realistic and symbolic threats of COVID‐19 and their unique impacts on well‐being and adherence to public health behaviors. Preprint at Social Psychological and Personality Science, 1–14. 10.1177/1948550620931634 [DOI] [Google Scholar]
- Larsen, M. , Nyrup, J. , & Petersen, M. B. (2020). Do survey estimates of the public's compliance with covid‐19 regulations suffer from social desirability bias? Journal of Behavioral Public Administration, 3(2), 1–9. 10.30636/jbpa.32.164 [DOI] [Google Scholar]
- Lear, D. (1995). Sexual communication in the age of aids: The construction of risk and trust among young adults. Social Science & Medicine, 41, 1311–1323. 10.1016/0277-9536(95)00010-5 [DOI] [PubMed] [Google Scholar]
- Lee, M. , Zhao, J. , Sun, Q. , Pan, Y. , Zhou, W. , Xiong, C. , & Zhang, L. (2020). Human mobility trends during the early stage of the covid‐19 pandemic in the United States. PLoS One, 15, e0241468. 10.1371/journal.pone.0241468 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leung, G. M. , Ho, L.‐M. , Chan, S. K. , Ho, S.‐Y. , Bacon‐Shone, J. , Choy, R. Y. , … Fielding, R. (2005). Longitudinal assessment of community psychobehavioral responses during and after the 2003 outbreak of severe acute respiratory syndrome in Hong Kong. Clinical Infectious Diseases, 40, 1713–1720. 10.1086/429923 [DOI] [PubMed] [Google Scholar]
- Lewnard, J. A. , & Lo, N. C. (2020). Scientific and ethical basis for social‐distancing interventions against covid‐19. The Lancet. Infectious Diseases, 20, 631–633. 10.1016/S1473-3099(20)30190-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maddux, J. E. , & Rogers, R. W. (1983). Protection motivation and self‐efficacy: A revised theory of fear appeals and attitude change. Journal of Experimental Social Psychology, 19, 469–479. 10.1016/0022-1031(83)90023-9 [DOI] [Google Scholar]
- Marcus, G. E. , Theiss‐Morse, E. , Sullivan, J. L. , & Wood, S. L. (1995). With malice toward some: How people make civil liberties judgments. Cambridge: Cambridge University Press. [Google Scholar]
- Munzert, S. , & Selb, P. (2020). Can we directly survey adherence to non‐pharmaceutical interventions?. Survey Research Methods, 14, 205–209. 10.18148/srm/2020.v14i2.7759 [DOI] [Google Scholar]
- Ornell, F. , Schuch, J. B. , Sordi, A. O. , & Kessler, F. H. P. (2020). “Pandemic fear” and covid‐19: mental health burden and strategies. Brazilian Journal of Psychiatry, 42, 232–235. 10.1590/1516-4446-2020-0008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ostrom, E. (1998). A behavioral approach to the rational choice theory of collective action: Presidential address, American political science association, 1997. American Political Science Review, 92(1), 1–22. 10.2307/2585925 [DOI] [Google Scholar]
- Pearce, J. M. , Lindekilde, L. , Parker, D. , & Rogers, M. B. (2019). Communicating with the public about marauding terrorist firearms attacks: Results from a survey experiment on factors influencing intention to “run, hide, tell” in the United Kingdom and Denmark. Risk Analysis, 39, 1675–1694. 10.1111/risa.13301 [DOI] [PubMed] [Google Scholar]
- Rippetoe, P. A. , & Rogers, R. W. (1987). Effects of components of protection‐motivation theory on adaptive and maladaptive coping with a health threat. Journal of Personality and Social Psychology, 52, 596. 10.1037//0022-3514.52.3.596 [DOI] [PubMed] [Google Scholar]
- Rogers, R. W. (1975). A protection motivation theory of fear appeals and attitude change. The Journal of Psychology, 91(1), 93–114. 10.1080/00223980.1975.9915803 [DOI] [PubMed] [Google Scholar]
- Rubin, G. J. , Amlôt, R. , Page, L. , & Wessely, S. (2009). Public perceptions, anxiety, and behaviour change in relation to the swine u outbreak: cross sectional telephone survey. BMJ, 339, b2651. 10.1136/bmj.b2651 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruiter, R. A. , Abraham, C. , & Kok, G. (2001). Scary warnings and rational precautions: A review of the psychology of fear appeals. Psychology and Health, 16, 613–630. 10.1080/08870440108405863 [DOI] [Google Scholar]
- Sheeran, P. , Harris, P. R. , & Epton, T. (2014). Does heightening risk appraisals change people's intentions and behavior? A meta‐analysis of experimental studies. Psychological Bulletin, 140, 511. [DOI] [PubMed] [Google Scholar]
- Teasdale, E. , Yardley, L. , Schlotz, W. , & Michie, S. (2012). The importance of coping appraisal in behavioural responses to pandemic flu. British Journal of Health Psychology, 17(1), 44–59. 10.1037/a0033065 [DOI] [PubMed] [Google Scholar]
- Tyler, T. R. , & Jackson, J. (2014). Popular legitimacy and the exercise of legal authority: Motivating compliance, cooperation, and engagement. Psychology, Public Policy, and Law, 20(1), 78. 10.1037/a0034514 [DOI] [Google Scholar]
- West, R. , Michie, S. , Rubin, G. J. , & Amlôt, R. (2020). Applying principles of behaviour change to reduce sars‐cov‐2 transmission. Nature Human Behaviour, 4, 451–459. 10.1038/s41562-020-0887-9 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1. Materials and methods.
Appendix S2. Supporting results.
Data Availability Statement
Replication data and code are publicly available here at Open Science Framework: https://osf.io/asczn/.