

To the Editor,
Coronavirus disease 2019 (COVID‐19) had caused a reported 2.9 million deaths worldwide by April 3rd, 2021. 1 The impact of nonpharmacological interventions worldwide has been difficult to measure because testing capabilities, demographics, comorbidities, health infrastructure, and response differ across countries and territories. Crude death rates have been used to compare the response of each country to COVID‐19 2 ; however, this measure does not account for age, which is a strong predictor of mortality in COVID‐19, with some studies showing a risk of death 120 times higher in the population older than 65 years. 3 , 4 , 5 Population age‐structure varies widely between countries, with the percentage of the population ≥65 years old increasing with income, 6 while 18% of people in high‐income countries are ≥65 years, in low‐income countries this percentage is 3%. 6 Therefore, crude rates do not allow appropriate comparisons of mortality among countries with different age‐structures. We compare mortality between 51 countries, as well as 50 states in the US and the District of Columbia that adopted different control strategies. We use data on deaths by 10‐year age groups from COVerAGE‐DB, 7 published and updated daily, population data from the United Nations, and the World Health Organization standard population for direct standardization by age. 8 , 9 In addition, we report rates at similar timeframes (~100 days from the 50th confirmed case) to provide meaningful comparisons of community transmission.
In the US, the age‐adjusted mortality rate at approximately 100 days is 16 times greater in the US state with the largest mortality (New Jersey), compared to the states with the lowest age‐adjusted mortality rate (Alaska) (Figure 1 and Table S1). These patterns were present in different world countries, the age‐adjusted mortality rate in Uruguay was 0.5, while in Peru was 47.6 at approximate 100 days of COVID‐19 transmission (95 times higher). Countries in Europe (UK, Belgium, Ukraine, and Spain), Latin America (Ecuador, Peru, Mexico, Brazil, and Chile), Israel, and the United States, resulted in the highest age‐adjusted mortality rates worldwide during the first 100 days of transmission (Figure 1 and Table S2). These data suggest that the measures to curb the transmission of the severe acute respiratory syndrome coronavirus 2 pandemic during the first 100 days might be a factor for the different mortality rates across regions and countries worldwide.
Figure 1.
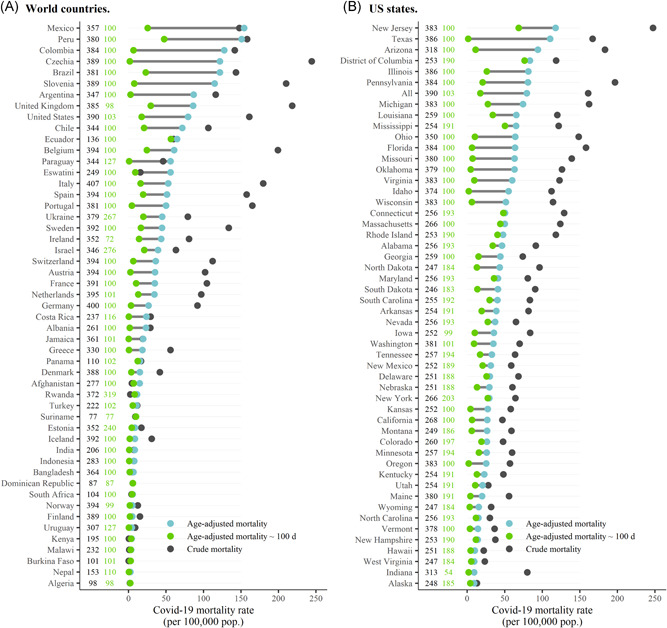
COVID‐19 crude, age‐adjusted, and age‐adjusted approximately 100 days mortality rates in 51 countries, 50 U.S. states, and the District of Columbia, by November 23, 2020. Both Panels A, B: Black Numbers in the left column represent the days between the 50th confirmed case and the last date with data for cumulative crude and age‐adjusted death rate calculation. Green numbers in the right column represent the closest days to 100 days with reported data since the 50th confirmed case for age‐adjusted approximately 100 days death rate. Panel B, Crude rates for Illinois is 525.2 (not shown). COVID‐19, coronavirus disease 2019
Our report has several limitations. The data were collected by an ongoing online effort to estimate age‐specific mortality in 5‐ and 10‐year age groups (lead by the Max Planck Institute for Demographic Research), 7 depending on openly available government sources. Case and death definitions may vary between countries, with different testing capacities. Age is not the only factor related to COVID‐19 severity. 10 Finally, the improvement of clinical management may reduce mortality risk over time. Further analyses could include comorbidities in the adjustment methods to compare countries.
In conclusion, age‐adjustments are needed to compare mortality between populations with different risks and age‐structures. Even though countries may use different reporting systems or have systems in different stages of development, countries and territories should follow the International Classification of Disease Standards for mortality classification and report to the World Health Organization, using standard age groups. International efforts should be directed to strengthen mortality surveillance and help overcome the lack of human resources and data digitization and evaluation, especially in developing countries. A stronger subnational and national mortality surveillance system could foster a supranational data curation and reporting effort to improve transparency and more robust assessment of country‐ and local‐specific responses to the pandemic.
CONFLICT OF INTERESTS
The authors declare that there are no conflict of interests.
AUTHOR CONTRIBUTIONS
Christian Garcia‐Calavaro designed the analyses. Christian Garcia‐Calavaro and Angel Paternina‐Caicedo carried out the analyses and drafted the manuscript. Adrian D. Smith, Lee H. Harrison, Fernando De la Hoz‐Restrepo, Enrique Acosta, and Tim Riffe aided in interpreting the results and reviewed the manuscript for important intellectual content. Enrique Acosta and Tim Riffe provided the data for the analyses. All authors reviewed and approved the final version of the manuscript.
PEER REVIEW
The peer review history for this article is available at https://publons.com/publon/10.1002/jmv.27007
DATA AVAILABILITY STATEMENT
Data are openly available under the license CC‐By Attribution 4.0 International, in an OSF data repository (https://osf.io/mpwjq/). All data and code is available upon reasonable request to the authors EA and TR.
Supporting information
Supporting information.
REFERENCES
- 1. Dong E, Du H, Gardner L. An interactive web‐based dashboard to track COVID‐19 in real time. Lancet Infect Dis. 2020;20(5):533‐534. 10.1016/S1473-3099(20)30120-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. World Health Organization . Coronavirus disease (COVID‐19): weekly epidemiological update. World Health Organization; 2020. https://www.who.int/docs/default-source/coronaviruse/situation-reports/20201012-weekly-epi-update-9.pdf
- 3. Pollán M, Pérez‐Gómez B, Pastor‐Barriuso R, et al. Prevalence of SARS‐CoV‐2 in Spain (ENE‐COVID): a nationwide, population‐based seroepidemiological study. Lancet. 2020;396(10250):535‐544. 10.1016/S0140-6736(20)31483-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Levin AT, Hanage WP, Owusu‐Boaitey N, Cochran KB, Walsh SP, Meyerowitz‐Katz G. Assessing the age specificity of infection fatality rates for COVID‐19: meta‐analysis & public policy implications. 2020. http://www.nber.org/papers/w27597 [DOI] [PMC free article] [PubMed]
- 5. Verity R, Okell LC, Dorigatti I, et al. Estimates of the severity of COVID‐19 disease. MedRxiv. 2020. 10.1101/2020.03.09.20033357v1?rss=1 [DOI]
- 6. The World Bank . World development indicators. 2020. https://databank.worldbank.org/reports.aspx?source=World-Development-Indicators
- 7. Riffe T, Acosta E, COVerAGE‐DB team . Data resource profile: COVeAGE‐DB: a global demographic database of COVID‐19 cases and deaths. Intl J Epidermiol. 2021. 10.1101/2020.09.18.20197228v1.abstract [DOI] [Google Scholar]
- 8. Ahmad OB, Boschi‐Pinto C, Lopez AD, et al. Age standardization of rates: a new WHO standard. Geneva: World Health Organization. 2001;9(10). https://pdfs.semanticscholar.org/7e89/5b230760ac34ce3d5472fb1cbf92b08566cc.pdf
- 9. United Nations . World population prospects—population division. 2019. https://population.un.org/wpp/Download/Probabilistic/Population/
- 10. Nepomuceno MR, Acosta E, Alburez‐Gutierrez D, Aburto JM, Gagnon A, Turra CM. Besides population age structure, health and other demographic factors can contribute to understanding the COVID‐19 burden. Proc Natl Acad Sci USA. 2020;117(25):13881‐13883. 10.1073/pnas.2008760117 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting information.
Data Availability Statement
Data are openly available under the license CC‐By Attribution 4.0 International, in an OSF data repository (https://osf.io/mpwjq/). All data and code is available upon reasonable request to the authors EA and TR.