

Abstract
The unique situational challenges of the COVID‐19 pandemic have demanded creative modifications to the delivery of genetic services. Institutions across the country have adapted workflows to continue to provide quality care while minimizing the need for physical visits. As the first epicenter of the pandemic in the country, New York City healthcare workers and residents had to make rapid, unprecedented changes to their way of life. This article describes the workflow adaptations of genetic counselors across various clinical settings at New York Presbyterian/Columbia University Irving Medical Center, the largest provider of genetics care in New York City, during the height of the COVID‐19 pandemic. The authors observe how the adaptations impacted clinical care and the genetic counselors. Our lived experience and account can provide guidance for others during the current and future pandemics.
Keywords: genetic counselors, genetic services, lived experience, service delivery models, telemedicine
What is known about this topic
Prior to 2020, telemedicine was used to provide genetic services but the frequency of use varied across disciplines and regions. In response to the COVID‐19 pandemic, several genetics clinics around the country have adopted the use of telemedicine for patient appointments, which has exposed benefits and limitations of the adaptation for both providers and patients alike.
What this paper adds to the topic
In addition to addressing the impact that the sudden work changes brought about by COVID‐19 had on our genetic counselors’ mental health, the paper outlines protocols that were quickly implemented to operate different specialty genetics clinics using creativity, teamwork, and revision. Furthermore, it proposes strategies to facilitate improved communication and well‐being among staff during emergencies.
1. INTRODUCTION
The COVID‐19 pandemic caused by the SARS‐CoV‐2 virus brought about unprecedented change in the lives of millions of people. In genetics clinics all over the country, the pandemic led to major transformations in the delivery of care and forced the adaptation of existing (and development of new) workflows to continue providing quality care while minimizing the need for physical visits. The first symptomatic COVID‐19 patient in New York City (NYC) was reported on March 1, 2020, and transferred to New York Presbyterian/Columbia University Irving Medical Center (CUIMC) for care. Three weeks later, the city was named the North American epicenter of the pandemic with COVID‐19 infection rates doubling every three days (Chapell, 2020). On March 22, 2020, the ‘New York State on PAUSE’ order went into effect, which mandated that all non‐essential workers remain home (NY Governor, 2020a). In anticipation of the lockdown, our institution moved all non‐essential personnel (which included most genetic counselors) to work remotely on March 16. Clinical research activities for all but two genetic studies were suspended as they had no direct benefit to the research participants. Within a matter of days, our entire staff of 40 genetic counselors (GCs) throughout CUIMC made drastic adaptations, converting our entirely in‐person care delivery model into a telemedicine format. While the pandemic has been a shared global challenge, NYC residents faced unique trials that shaped not only our work practices during this time but the perceived quality of patient care as well. The focus of this article is to describe emergency workflow adaptations to genetic counseling taken at our institution during the height of the pandemic in NYC, from March‐May 2020. To support our observations, we present data from the general genetics clinic on provider reported stress and coping, both with work and personal issues impacted by COVID‐19. Our experience and account can serve as guidance in how we provide care, for others and ourselves, during the current and future pandemics.
2. IMPACT ON STAFF WELL‐BEING
To gauge the well‐being of our staff while working remotely, from March 16‐ May 1, 2020, GCs in the general genetics, cardiogenetics, and oncogenetics clinics were invited to complete weekly anonymous online surveys. The surveys asked respondents to state their agreement or disagreement with four statements related to anxiety about work, personal and family health, and ability to work remotely during the pandemic. Results of the survey from 33 respondents after weeks one, four, and eight of working remotely are shown in Figure 1a‐d. The survey also contained an open‐ended question to allow suggestions on how to improve workflows.
FIGURE 1.
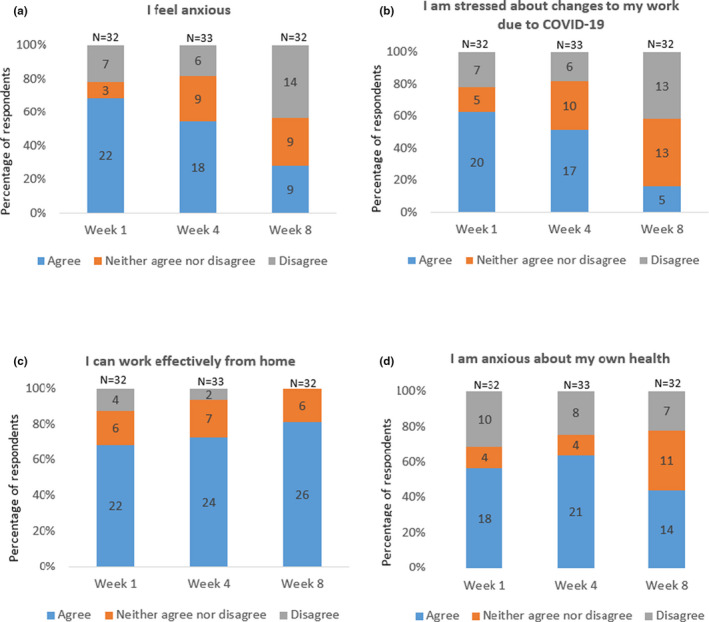
(a‐d) Anonymous survey responses of general genetics clinic staff to different questions related to their stress, anxiety, and ability to work remotely during the first eight weeks of the COVID‐19 pandemic in NYC (March 16‐ May 1, 2020). N = 32 for surveys at week one and week eight and N = 33 for survey at week four. (a) Survey responses to the statement ‘I feel anxious’. (b) Survey responses to the statement ‘I am stressed about changes to my work due to COVID‐19’. (c) Survey responses to the statement ‘I can effectively work from home’. (d) Survey responses to the statement ‘I am anxious about my own health’
The staff reported strongest feelings of anxiety and stress related to changes in work during week one (Figure 1a). This was similar at four weeks but had dropped by eight weeks. Confidence in ability to work effectively from home increased over time (Figure 1b) and stress related to work changes due to COVID‐19 decreased by week eight (Figure 1c). Anxiety related to personal health concerns (Figure 1d) brought about by COVID‐19 peaked at about four weeks.
3. IMPACT ON WORKFLOW
Based on suggestions from the survey responses, the GCs at CUIMC made adjustments to their workflows to accommodate the switch to telemedicine. For purposes of clarity, we use the term ‘telemedicine’ in this paper to describe consults by video conference unless otherwise specified. A senior GC representative from different genetics specialties at CUIMC including general genetics (pediatric and adult), oncology, reproductive medicine, inpatient, neurology, cardiology, and clinical research described how workflows were adapted for COVID‐19 restrictions, what instigated the evolution, and lessons learned. Representatives drafted these reports in May of 2020.
4. CHANGES ACROSS INPATIENT AND OUTPATIENT GENETIC CARE AND CLINICAL GENETIC RESEARCH
4.1. Workflow changes
This section highlights the COVID‐19 workflows that GCs across our institution adopted. All our GCs shifted to providing care remotely, with the exception of one inpatient GC who was on site three times a week. The overall workflow adopted for outpatient appointments across all clinics is represented in Figure 2.
FIGURE 2.
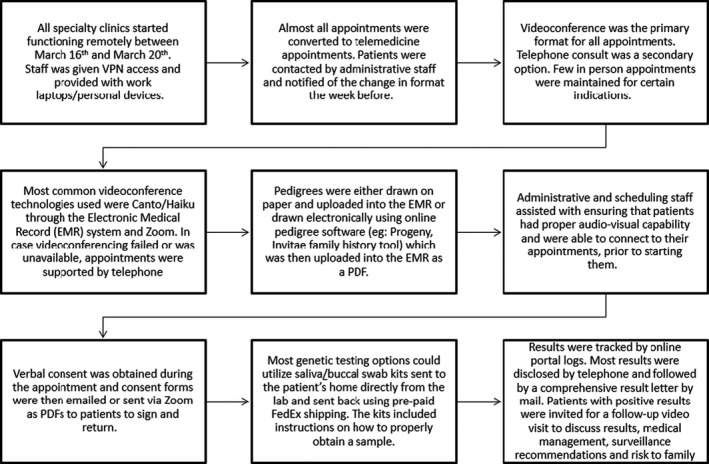
Workflow changes adopted across all outpatient genetic specialties at Columbia University Irving Medical Center
4.1.1. Switch to telemedicine
Almost all genetic counseling patient care transitioned from in‐person to telemedicine via videoconferencing as the primary mode of delivery. Canto, the video app embedded in our electronic medical record (EMR), and HIPAA‐compliant Zoom, Inc. platforms were used. If patients were unable to access these platforms, telemedicine via phone was offered as an alternative. Doximity, Inc. (Buro, 2019), a professional medical network and support service for physicians, was used to mask personal phone numbers and display the office number when calling patients. Office voicemails were checked daily remotely. In a few cases of urgent care (i.e., metabolic, inpatient care), in‐person appointments were offered.
4.1.2. Redeployment of GC staff
At the onset of the pandemic, several of our GCs were redeployed to ensure continued employment in anticipation of reduced patient volume. Ten GCs were redeployed to work for a large COVID‐19 biobank research study. One GC was redeployed to work in a different genetics clinic within the institution.
4.1.3. Inter‐staff communication
Maintaining channels of communication was key to effective remote work in order to provide consistent patient care but also ensure the well‐being of staff and team members. As COVID‐19 infection rates of medical staff at CUIMC were growing at this time, emergency phone trees and daily GC buddy check‐in systems were instigated to monitor the team's physical and mental health. In our larger GC divisions—general genetics and oncogenetics—a daily 15 min video conference staff huddle allowed the entire team to review institutional regulations on work and travel that were changing every day during this time, ensure everyone was uniformly aware of the modified workflows, and discuss ways to address issues with telemedicine that presented the day prior. Smaller divisions used less formal methods, phone calls, texts, and emails to check in.
Developing effective communication between the remote GC team and the on‐site essential workers was critical to ensure the accurate execution of all time‐sensitive procedures and testing. The GCs drafted workflows for all testing and procedures and these were shared with the essential staff on site. In prenatal genetics, a daily email was sent to the OBGYN team (administrative staff, medical assistants, nurses) and cytogenetics laboratory alerting them to scheduled prenatal diagnostic testing procedures for the day. The email alerts served as a safety measure, allowing the laboratory to track and confirm receipt of all expected prenatal chorionic villus sampling (CVS) /amniocentesis samples. In inpatient genetic care, the EMR’s instant chat function was often used to educate care teams on the floor about ways to assist the geneticists in performing virtual physical exams, coordinate genetic testing sample drop‐off, and confirm sample delivery with the inpatient GC in real time.
4.1.4. Sample collection and shipping
Most outpatient genetic tests were ordered remotely using buccal swab or saliva kits mailed to patients’ homes that patients then sent directly to the laboratory. To facilitate tests that were time‐sensitive and required blood samples such as maternal blood for non‐invasive prenatal testing (NIPT) and oncology genetic testing needed for urgent medical management decisions, blood draws were coordinated during a scheduled in‐person doctor appointment such as an ultrasound or chemotherapy appointment, respectively.
4.2. Challenges with workflow adjustments
This section describes the challenges of the workflow adjustments across the institution's genetic counseling services.
4.2.1. Difficulty with accessing virtual appointments
Some of our patients had trouble accessing virtual appointments for various reasons including unavailability of an electronic device, limited data bandwidth to download applications required for telemedicine, unstable internet connection, and unfamiliarity and discomfort with the virtual application. These patients were either counseled by phone or elected to postpone their visit until they could attend in person.
4.2.2. Difficulty with rapport building
Some GCs expressed concern about whether the telemedicine model allowed less opportunity for therapeutic support and rapport building. Recommended practices for telemedicine such as looking directly at the camera rather than the patient on the screen to emulate eye contact made reading non‐verbal cues or body language at the same time more challenging. Patients could also turn away or switch off their camera during a session if they wanted to, which made establishing a therapeutic connection with them harder. Additionally, patients living in NYC homes during the pandemic frequently had little privacy or help with child care and could be easily distracted.
4.2.3. Difficulty with obtaining consent
Verbal informed consent was obtained during the genetic counseling session but obtaining appropriate written informed consent for genetic testing, as required by New York State Senate (1996), was challenging. Not all patients had the technological capability to receive, sign, and return a consent form via email. Delays in receiving the signed consent from the patient were a barrier to proceeding with remote genetic testing in a timely manner. Assessing informed consent also presented challenges. Patients were asked to confirm at the beginning of the session whether they were in an appropriate space/setting to receive information and engage in decision making, but conflicts were not always disclosed. In multiple instances, patients were found multi‐tasking with other chores, working from home, or occupied with child care. In inpatient care, the ability for patients/their medical proxies to review or sign consents remotely varied widely. Several parents reviewed information on a cell phone while at bedside, which made providing electronic signatures harder. Some parents met with the inpatient GC in person specifically to sign the consent forms.
Unlike clinical care, our two active clinical research studies were set up to collect consent remotely through electronic systems such as Research Electronic Data Capture (REDCap; Harris et al., 2009). When participants were less comfortable with the remote electronic system, our research GCs offered to walk people through the electronic consent by phone. This helped to increase consent completion rates. For those who did not have access to email, we mailed paper consents. To limit the potential spread of the virus through the postal system (which was a concern early in the pandemic), the Columbia University Institutional Review Board (IRB) accepted photographs of the signed consent forms.
4.2.4. Difficulty with testing coordination
Unless ordered as a stat test, most laboratories sent buccal/saliva sample collection kits to patients by ground shipping, which generally takes five business days to arrive at the patient's home. However, the NYC postal system was experiencing delays in shipments during this time (Offenhartz, 2020). Once patients received test kits, they were often slow to submit samples to the lab, possibly due to reluctance with needing to leave their home to locate a shipping location during the stay‐at‐home order. One patient in the oncogenetics clinic reported that she had COVID‐19 and did not want to submit a saliva sample for fear of spreading infection. These delays required the GC to regularly monitor the laboratory portals and follow‐up with patients to confirm receipt of the kit and encourage sample collection.
Patients had difficulty with remote sample collection. Several instances of specimen failure occurred because the sample was not collected properly or was mislabeled. Some patients also required assistance with locating a shipping location/drop‐off box for sample return. For non‐saliva/buccal swab tests, patients were given the opportunity to have the sample collected at the outpatient commercial laboratory closest to them, at the hospital phlebotomy laboratory, or to defer having genetic testing until after the pandemic. However, traveling to have a sample collected also presented a challenge. Our patients were concerned about the potential virus exposure on public transportation, which is the primary mode of transportation for majority of NYC residents (U.S Census Bureau, 2019). As an alternative option, some genetic testing companies introduced mobile phlebotomy service. A few patients mentioned they were hesitant to invite a mobile phlebotomist into their homes but that they would consider the option if the blood draw could be done outside, on their front stoop for example.
All these challenges led to lower testing completion rates across the different specialties as seen in Table 1. Overall, most specialties saw a decline in the number of patients and testing completed as compared to pre‐COVID.
TABLE 1.
Comparison of outpatient volume and genetic testing completion at Columbia University Irving Medical Center between March‐April of 2019 and March‐April of 2020
| Specialty | Pre‐COVID‐19 (for months of March and April 2019) patient averages per week | During COVID‐19 (for months of March and April 2020) patient averages per week | ||||
|---|---|---|---|---|---|---|
| Number of patients | Number of patients who elected testing | Number of patients who had testing | Number of patients (% change from pre‐COVID) | Number of patients who elected testing (% change from pre‐COVID) | Number of patients who had testing (% change from pre‐COVID) | |
| General Genetics | 50 | 38 | 36 | 22 (−66%) | 17 (−55%) | 14 (−61%) |
| Oncogenetics | 23 | 20 | 20 | 29 (+21%) | 24 (+17%) | 13 (−35%) |
| Reproductive Genetics | 38 | 19 | 19 | 29 (−24%) | 15 (−21%) | 15 (−21%) |
| Neurogenetics | 30 | 19 | 19 | 19 (−37%) | 15 (−21%) | 14 (−26%) |
| Cardiogenetics | 10 | 9 | 9 | 8 (−20%) | 6 (−33%) | 5 (−45%) |
Sample collection for most of our clinical genetic research studies was altered or halted, as laboratory staff were not permitted on site to process collected biospecimens.
4.3. Advantages with workflow adjustments
This section describes the advantages of the workflow adjustments across the institution's genetic counseling services.
4.3.1. Increased availability
In some instances, the availability of patients and their family members to participate in appointments was improved because COVID‐19 altered work and school schedules. Additionally, the transition to remote work and school likely created an increased comfort with Zoom and video conferencing broadly. Thus, while patient volumes decreased during this time, so did the overall no‐show rate of scheduled patient telemedicine appointments.
4.3.2. Reduced wait time for appointments
Before the NYC PAUSE went into effect, patients in most of our clinics (other than reproductive genetics) were scheduled at least one to two months out. After the adoption of telemedicine, most referred patients were seen within one week.
4.3.3. Decreased pressure to consent to testing
Since patients were not physically in a space where they could have their sample collected immediately, they were allowed more time to process the counseling information before providing consent to testing. Prenatal GCs began seeing more patients for pre‐procedure counseling 1–2 days before the CVS/amniocentesis appointment and noted this allowed for less pressured decision‐making and more time to arrange appropriate testing.
4.3.4. Decreased physical stress
Our GCs observed that patients with issues of anxiety, including children with autism spectrum disorder, seemed more at ease with virtual appointments when in the comfort of their home. In the cardiogenetics clinic, several patients with cardiac conditions who were medically compromised or had active symptomology expressed that telemedicine appointments were easier to attend as they mitigated physical exertion and potential exposure to COVID‐19.
5. ADJUSTMENTS UNIQUE TO EACH SPECIALTY
This section highlights workflow adaptations that addressed unique demands related to each genetics sub‐specialty.
5.1. General genetics
Our general genetics clinic consists of 13 GCs and 4 geneticists who typically see pediatric and adult patients in the outpatient care setting. Prior to COVID‐19, our appointments were all conducted in person with a geneticist and a GC.
5.1.1. 3:1 GC and geneticist appointment scheduling
Each geneticist was scheduled with patients with three different GCs at a particular time slot so real‐time communication between the GC, geneticist, and administrative team was critical to the flow of the clinic. GCs utilized Microsoft Teams, Inc. (Marco et al., 2019), a HIPAA‐compliant feature included as part of Microsoft Office 365, for communication during the appointment to let a geneticist know when a patient was ready and notify the administrative staff of any changes to the appointment. The time stamped messages in this system allowed the geneticist to know the order of the next patient to be examined.
5.1.2. Limited physical examinations
Limited physical examinations were performed through video conference. For conditions such as connective tissue disorders, parents were guided by geneticists on how to measure parameters such as arm span. The geneticists relied on patient self‐report for certain features, such as cutaneous lesions, to help focus their examinations. Pictures were taken using a ‘screen grab’ feature on Canto, the video‐visit platform provided in our EMR system, which allowed for direct, secure upload to the patient's EMR without storage on the provider's device.
5.2. Metabolic genetics
Our metabolic team includes a nurse practitioner (NP), dietician, social worker, and geneticist. Metabolic patients are typically seen for appointments scheduled at regular intervals depending on the age and diagnosis of the patient.
5.2.1. Redeployment to divisions outside of genetics
Our metabolic geneticist and NP were considered for redeployment to inpatient units caring for non‐genetic patients during this time, a system our hospital utilized across departments to address changing demands of COVID‐19. To prepare for this shift, two GCs from the general genetics clinic were redeployed to the metabolic team to help identify metabolic patients requiring regular prescriptions for formula/medication or routine metabolic tests.
5.2.2. Advance prescriptions and emergency medical letters
In March, NYC hospitals saw increased hospital admissions due to COVID‐19 during this time (Thompson et al., 2020) and the hospital bed availability across NYC dropped to <17% (Hospitalization data from New York Forward, 2020). To ensure that our metabolic patients would be given appropriate care if admitted for a crisis, our GCs sent patients detailed medical emergency letters describing each patient's metabolic diagnosis, treatment plan, and the geneticist's contact information, which they were instructed to show to their provider in the even that they required urgent care. The GCs also identified and contacted patients with regular formula prescriptions to see whether they had sufficient supplies for the next three months and if not, ensured that refill orders were placed prior to the geneticist being redeployed to avoid disruption of care.
5.2.3. Urgent consults
Our metabolic geneticist and NP reported on site for urgent metabolic consults after work hours. They ensured send‐out of necessary time‐sensitive samples.
5.3. Reproductive genetics
We have three clinical reproductive GCs and one reproductive geneticist who work at outpatient sites across NYC and two satellite offices. Prior to COVID‐19, patients were seen in person for their initial visits and results were disclosed primarily via telephone. With finite windows for performing aneuploidy screening and diagnostic procedures, and legal limits for decision‐making in the event of an abnormal genetic result or fetal anomaly, there was a need to maintain routine care while minimizing in‐person visits. GCs saw patients independently for the majority of indications, with the addition of the reproductive geneticist for complex diagnostic results when requested.
5.3.1. Coordination of invasive prenatal procedures
Before the pandemic, patients having invasive procedures (i.e., CVS/amniocentesis) had genetic counseling immediately prior to their procedure. During COVID, to allow patients to make preparations in advance for their commute into the hospital for the procedure, genetic counseling sessions were booked 1–2 days before the scheduled diagnostic procedure and patients signed consent forms upon their arrival for the procedure instead of during the genetic counseling appointment.
5.3.2. Limited access to OR/hospital facilities
Reduced access to the operating rooms (OR) as the hospital expanded critical care operations and mitigated spread of the virus affected the number of patients who could be accommodated for second trimester terminations. While many patients were still cared for by our Family Planning Division, GCs assisted with referrals to abortion at community‐based outpatient providers to ensure continuous, timely access when our institution lacked immediate availability. Navigating the legal limits on access for abortion is part of prenatal GC care and the team reported specific concern for patients who may need to travel during the pandemic for out‐of‐state abortions.
5.4. Oncogenetics
We have five GCs who provide cancer genetic services across three divisions (Hematology/Oncology, Digestive and Liver Disease, and Gynecological Oncology) at our main hospital and one GC who sees patients at two satellite offices. Appointments involve a physician (geneticist/oncologist/gastroenterologist) and a GC or a GC only.
5.4.1. Reduced backlog and appointment wait time
The hospital halted elective/non‐emergency surgical procedures during this time, and, as a result, our gastroenterologists were able to dedicate more of their clinical time to genetic consults in the gastrointestinal (GI) clinic. The schedule for GI clinic was reviewed to identify and triage the highest risk patients to offer them newly available slots, thereby reducing the wait time for an appointment.
5.4.2. Addressing bottlenecks in patient care
Conversely, in the Hereditary Breast and Ovarian Cancer (HBOC) clinic, there was decreased availability as the oncologists were redeployed to provide COVID‐19 care. Physical gynecologic examinations and screenings were postponed to future in‐person visits, which further added to the backlog. To address the backlog, HBOC clinic was offered more frequently (weekly rather than biweekly) and with extended hours to offer more appointments.
5.5. Neurogenetics
Neurogenetic counseling is offered by four GCs across various adult and pediatric clinics. The majority of genetic counseling occurs within specialty clinics, which include Pediatric Neuromuscular (Peds MDA), Adult Neuromuscular (Adult MDA), Motor Neuron Disease (ALS Clinic), Memory Disorders, Parkinson's Disease and Movement Disorders, and Huntington's Disease clinics. Neurogenetic counseling sessions occur within multidisciplinary clinics, during a specialty consult scheduled with a neurologist, or as a separate GC‐only appointment.
5.5.1. Multidisciplinary clinic
To facilitate multidisciplinary ALS, Adult MDA, and Peds MDA clinics remotely, the Zoom ‘breakout room’ feature was utilized to allow each clinician to see the patient during the same appointment. The clinic coordinator first invited all clinicians into one breakout room that functioned as the ‘clinic workroom’. Patients were placed into separate breakout rooms (designated as examination room 1, examination room 2, etc.) and the team ‘entered’ each ‘examination room’ to see the patient. The clinic coordinator remained in the ‘clinic workroom’ for the majority of the multidisciplinary clinic and directed different clinicians in and out of patient ‘examination rooms’.
5.5.2. Neurology examination
Modified neurological examinations were performed by neurologists through video appointments where cranial nerves were evaluated visually and other assessments of the central nervous system were done through observation of the patient performing the procedure or with the assistance of a caregiver, such as the finger‐to‐nose test. Significant gaps in the virtual assessment include important information about reflexes and overall sensitivity for degree and pattern of abnormalities.
5.6. Cardiogenetics
We have one full‐time and two part‐time cardio GCs who see patients in our cardiogenetics clinic. Patients are evaluated by a GC and a geneticist in a single visit.
5.6.1. Family appointments
The use of telemedicine allowed people in multiple locations to join a single appointment, thereby enabling more family visits than the pre‐COVID in‐person practice. We counseled and educated multiple extended family members simultaneously and offered cascade cardiogenetic testing to those at risk.
5.7. Inpatient genetics
An inpatient GC was on site three days a week and remained on pager coverage for the remaining two days during this period. The GC rarely entered the patient rooms when on site and appropriate PPE was provided by the hospital for those instances.
5.7.1. Assistance with physical examination
To limit contact with inpatients and other hospital staff, the inpatient GC contacted the floor team and asked them to upload images of the patient (profile, front facial, and full‐body) for the geneticist to perform a virtual physical examination. Nursing staff uploaded photographs of inpatients to the EMR. The geneticists discussed any relevant findings with the GCs who then contacted the patient's parents or medical proxy by phone to discuss genetic testing.
5.7.2. Demand for rapid exome sequencing
As the rate of COVID‐19 infections increased in NYC, our Neonatal and Pediatric Intensive Care Units (NICU and PICU) grew concerned about underlying undiagnosed immune disorders that could explain the cases of severe response to disease in previously healthy young individuals. NYC saw the beginning of a novel condition called Multisystem Inflammatory Syndrome in Children (MIS‐C; Godfred‐Cato et al., 2020) during this time, which describes an inflammatory disorder that presents in children who test positive for COVID‐19 (Durkin, 2020). In consultation with the Division Chiefs of the PICU, Allergy/Immunology (A/I) and Genetics, the hospital adopted a policy of performing rapid exome sequencing (ES) on all PICU patients with COVID‐19 or acute respiratory distress syndrome (ARDS). Demand for rapid ES and primary immunodeficiency (PID) panels spiked beyond the clinical capacity for a complete genetics evaluation.
Trio testing for rapid ES, which requires samples from proband and both biological parents, was challenging as hospital restrictions only allowed one parent at a time with an admitted child during this period (Health Advisory from New York Department of Health, 2020). Parents off‐site were mailed buccal/saliva collection kits, which could add days to the two‐week turnaround time for rapid ES. Multiple rapid ES tests were run as duos (i.e., proband and one biological parent) due to difficulty obtaining a second parental or familial sample in a timely matter. If the second parental sample arrived at the laboratory after sequencing was complete, it was still used in segregation analysis.
5.7.3. Education of inpatient physicians
The genetics team decided that modified genetic consultations would be best to accommodate the rising number of consults brought about by the increased demand for rapid ES and PID panels. Thus, the inpatient GCs educated A/I providers on how to appropriately order and obtain consent for these genetic tests for some patients directly and emphasized the importance of informed consent.
5.8. Clinical research
Several of our GCs serve as project managers and/or clinical research coordinators for a variety of clinical research studies recruiting patients locally and across the country. These studies collect biospecimens for genomic analyses. Most clinical research studies which include a GC were suspended during this time with the exception of two that had direct clinical benefit: a prenatal study involving enrollment of women with fetuses with congenital anomalies and a Duchenne muscular dystrophy (DMD) newborn screening study which involved recruitment of newborns.
5.8.1. Focus on alternate study processes
Our GCs who typically focus on participant recruitment instead focused their efforts on increasing the social media presence for their studies. Aware that participants may be more active on social media during the quarantine time, new written and video content was created and designed to engage participants of various age groups. The team also re‐posted COVID‐19 content relevant to the patient community from reputable sources. During this time, research GCs shifted work from recruitment to aspects of research data analysis that could be continued remotely, such as clinical confirmation of research findings. Participants were mailed saliva collection kits, and following confirmation of the variant, the results were disclosed via a video appointment with the GC and geneticist.
5.8.2. Uncertainty with life circumstances
In some cases, research participants had increased ability to complete the consent process, as they unexpectedly had more time, or all family members eligible for the study were under the same roof (working remotely, home from college, furloughed from their jobs, etc.). Others communicated an increased burden from the process as they had new challenges or uncertainties that may have contributed to disinterest in non‐urgent research.
5.8.3. Continued prenatal research
Although most genomic research was halted, our study of rapid genomic sequencing of women pregnant with fetuses with congenital anomalies was categorized as having a direct benefit to the participant and was given permission to continue. Considerations for moving forward included assessing how to obtain samples from fathers when the obstetric unit did not allow them to ultrasound visits and minimizing frequency of on‐site visits by research laboratory staff by batching samples.
6. CONCLUSION AND FUTURE STEPS
As our parks and buildings turned into makeshift hospitals (Capatides, 2020; NY Governor, 2020b), mass burial grounds were used (Kilgannon, 2020), restaurants and theaters closed (Ferre‐Sadurni, 2020; Paulson, 2020) and streets emptied, it became increasingly evident that the drastic and sudden changes coupled with the dearth of information known about the novel virus would likely bring to bear considerable mental stress on NYC patients and healthcare providers alike.
The mandate to work remotely for the first time added anxiety and disconnection, which made maintaining the GC team infrastructure and communication increasingly difficult. We saw the effects of this in our employee pulse survey. The staff members reported strongest feelings of general anxiety and stress related to changes in work at the end of week one, after the shift to telemedicine. The increase in health‐related anxiety during week four coincides with when New York was declared to have the highest number of COVID‐19 cases in the world (BBC news, 2020). The week before, face masks were made mandatory and the COVID‐19‐related death toll in NYC alone tripled overnight (Chung, 2020). At around week eight, health‐related anxiety of staff decreased slightly, but overall remained fairly high. At this time point, NYC schools had been declared closed for the remainder of the academic year, small, socially distant gatherings of 10 people were allowed, and an increasing number of children in the city were being hospitalized for MIS‐C (Godfred‐Cato et al., 2020).
One of the most important challenges faced in the overnight transition to remote work was to maintain connection with team members and prevent disjointed care. Our clinics instituted various techniques to stay connected, including daily virtual staff huddles, a health check‐in buddy system and virtual lunch rooms. We started several virtual social events including virtual group exercise classes, trivia/movie nights, happy hours, and book clubs. The general genetics clinic's social worker regularly provided resources for mental health counseling and hosted a weekly virtual meditation line as well. We continued opportunities for ongoing education and professional interaction such as genomics Grand Rounds, case conference, and journal club by switching to virtual formats. The pulse survey was a useful way to gauge how the GC team was feeling during a stressful time and identify the individual and group challenges with working remotely. Redeployment roles were assigned after careful consideration of appropriately matching the role to best accommodate GCs with limiting personal circumstances including health issues, unstable home internet connection, commutes by public transportation, small residences without designated office space and having children at home without childcare. Taking all these factors into consideration and having regular communication allowed for a successful emergency transition to working remotely during this time.
Of all our clinics, our general genetics clinic saw the largest decrease in patient volume after our switch to telemedicine (Table 1). This is unsurprising given that physical examinations are often an important component of general genetics appointments but are a challenge to perform remotely. While oncogenetics saw an increase in patient volume, their test completion rate decreased overall compared with pre‐COVID, indicating the impact of challenges with testing coordination previously discussed. Overall, a clear advantage of the telemedicine system appeared to be shorter wait times for patients to receive a scheduled appointment. This is probably due to the ease of attending a telemedicine appointment from any location rather than needing to coordinate a visit to the physical clinic site. Additionally, a number of patients were also working from home during this time, further facilitating a remote model of care.
While we have an understanding of how these contingency workflow changes impacted our clinical team, we did not formally assess the patient experience. Future research should assess the patient experience of a transition to remote care, including patient satisfaction, barriers to access, and impact of telemedicine on the GC‐patient therapeutic relationship. The question of whether telemedicine allows patients to feel less pressured to consent to genetic testing and enables better decision‐making should also be explored. This information may not only impact how we provide care to patients in the future, but also drive adjustments to the competency skills (American Accreditation Council for Genetic Counseling2019) required of GC trainees.
Even if one was not personally infected by COVID‐19, the changes to our city and community were felt by patients and providers alike. Our patients were experiencing job loss and uncertainty, illness, and children home from school without childcare. It is imperative to recognize how these factors can affect both patients and staff members and develop tools to provide validation, support, and flexibility. We have drafted strategies highlighted in Table 2 that could be adopted in times of emergency to enable genetics clinics to continuously function remotely.
TABLE 2.
Strategies for genetics clinics adapting to emergencies
| 1. Strategies to improve staff communication and well‐being | 2. Strategies to maintain consistent patient care | 3. Strategies to coordinate patient consent and testing remotely |
|---|---|---|
|
|
|
Since the height of the COVID‐19 pandemic, we have transitioned to a hybrid approach of both in‐person and remote patient care. The lessons learned improved efficiency and effectiveness and will have long lasting effects on how we practice. We hope that some of the challenges and strategies shared will be useful to other genetics clinics to consider how best to provide continuity in patient care when faced with emergent city/state‐wide closures in a crisis, which rarely offer the luxuries of time, financial planning or emotional and mental adjustment.
AUTHOR CONTRIBUTIONS
Priyanka Ahimaz and Julia Wynn confirm that they had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. All of the authors provided meaningful contribution to the manuscript, gave final approval of this version to be published, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
COMPLIANCE WITH ETHICAL STANDARDS
CONFLICT OF INTEREST
Priyanka Ahimaz, Jessica Giordano, Michele Disco, Elizabeth Harrington, Elana Levinson, Erica Spiegel, Carli Andrews, Emily Griffin, Rebecca Hernan and Julia Wynn declare that they have no conflict of interest.
HUMAN STUDIES AND INFORMED CONSENT
The survey data reported here were collected as part of quality improvement measures and do not constitute research requiring IRB review. No human studies were carried out by the authors for this article.
ANIMAL STUDIES
No animal studies were carried out by the authors for this article.
DATA SHARING AND DATA ACCESSIBILITY
The data that support the findings of this study are available from the corresponding author upon reasonable request.
ACKNOWLEDGEMENTS
The authors would like to acknowledge Carrie Koval, Edwin Guzman, Katia Dergham, Leyla Tabanfar, Maureen Mulhern, Meredith Ross, Nina Harkavy, Rosa Arce, Sara Berger, Scott Robinson, and Stephanie Galloway for providing data on patient numbers and workflows undertaken.
Ahimaz P, Giordano J, Disco M, et al. COVID contingencies: Early epicenter experiences of different genetics clinics at a New York City institution inform emergency adaptation strategies. J Genet Couns. 2021;30:938–948. 10.1002/jgc4.1409
REFERENCES
- American Accreditation Council for Genetic Counseling . (2019). Practice Based Competencies . Retrieved December 24, 2020. https://www.gceducation.org/practice‐based‐competencies/
- BBC news . (2020). Coronavirus: New York has more cases than any country. Retrieved December 24, 2020. https://bbc.com/news/world‐us‐canada‐52239261
- Buro, J. S. (2019). App Review Series: Doximity. Journal of Digital Imaging, 32(1), 1–5. 10.1007/s10278-018-0109-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Capatides, C. (2020). Emergency field hospital erected in the middle of New York's Central Park to treat COVID‐19 patients. CBS News. Retrieved on December 24. https://www.cbsnews.com/news/coronavirus‐central‐park‐ny‐field‐hospital‐covid‐19/
- Census Bureau, U. S. (2019). American Community Survey 2019, Table S0801 . Retrieved December 24, 2020. https://data.census.gov/cedsci/table?g=0500000US36061&tid=ACSST1Y2019.S0801&hidePreview=true
- Chapell, B. (2020). Coronavirus: New York Infection Rate Is 'Doubling About Every 3 Days,' Cuomo Says. NPR. Retrieved on December 24. https://www.npr.org/sections/coronavirus‐live‐updates/2020/03/24/820891370/coronavirus‐n‐y‐infection‐rate‐is‐doubling‐about‐every‐3‐days‐cuomo‐says
- Chung, J. (2020). Coronavirus Updates: 222 COVID‐19 Deaths Reported In NYC Over 24 Hours. Gothamist. Retrieved on December 24. https://web.archive.org/web/20200329145514if_/https://gothamist.com/news/coronavirus‐updates‐222‐coronavirus‐deaths‐nyc‐over‐24‐hours
- Durkin, E. (2020). NYC Reports 52 Children with Virus‐Linked Inflammatory Syndrome . Politico. Retrieved on December 24. https://www.politico.com/states/new‐york/albany/story/2020/05/12/nyc‐reports‐52‐children‐with‐virus‐linked‐inflammatory‐syndrome‐1283503
- Ferre‐Sadurni, L. (2020). New York City Schools, Restaurants and Bars Are Shut Down Over Coronavirus . New York Times. Retrieved on December 24. https://www.nytimes.com/2020/03/15/nyregion/coronavirus‐nyc‐shutdown.html
- Godfred‐Cato, S. , Bryant, B. , Leung, J. , Oster, M. E. , Conklin, L. , Abrams, J. , Roguski, K. , Wallace, B. , Prezzato, E. , Koumans, E. H. , Lee, E. H. , Geevarughese, A. , Lash, M. K. , Reilly, K. H. , Pulver, W. P. , Thomas, D. , Feder, K. A. , Hsu, K. K. , & Plipat, N. … California MIS‐C Response Team . (2020). COVID‐19‐associated multisystem inflammatory syndrome in children‐United States, March‐July 2020. Morbidity and Mortality Weekly Report, 69, 1074–1080. 10.15585/mmwr.mm6932e2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harris, P. A. , Taylor, R. , Thielke, R. , Payne, J. , Gonzalez, N. , & Conde, J. G. (2009). Research electronic data capture (REDCap)–a metadata‐driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics, 42(2), 377–381. 10.1016/j.jbi.2008.08.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kilgannon, C. (2020). As Morgues Fill, N.Y.C. to Bury Some Virus Victims in Potter’s Field. New York Times. Retrieved on December 24. https://www.nytimes.com/2020/04/10/nyregion/coronavirus‐deaths‐hart‐island‐burial.html
- Marco, S. , Seegmiller, B. , Lazo, J. , Hall, G. , & Beard, A. (2019). HIPAA Compliance Microsoft Office 365 and Microsoft Teams. Microsoft. Retrieved on December 24, 2020. https://www.microsoft.com/en‐us/microsoft‐365/blog/wp‐content/uploads/sites/2/2019/04/HIPAA‐Compliance‐Microsoft‐Office‐365‐and‐Microsoft‐Teams.pdf
- New York Department of Health . (2020). Health Advisory:COVID‐19 Updated Guidance for Hospital Operators Regarding Visitation . Retrieved on December 24, 2020. https://opwdd.ny.gov/system/files/documents/2020/04/doh_covid19_hospitalvisitation_4.10.20.pdf
- New York Forward . (2020). COVID‐19 Regional Metrics Data‐ Hospital Capacity. Retrieved on December 24, 2020. https://forward.ny.gov/covid‐19‐regional‐metrics‐dashboard
- New York State Senate . (1996). Section 79‐L. Confidentiality of records of genetic tests . Retrieved on December 24, 2020. https://www.nysenate.gov/legislation/laws/CVR/79‐L
- NY Governor . (2020a). Amid Ongoing COVID‐19 Pandemic, Governor Cuomo Announces Completion of First 1,000‐Bed Temporary Hospital at Jacob K. Javits Convention Center . governor.ny.gov. Retrieved on December 24, 2020. https://coronavirus.health.ny.gov/new‐york‐state‐pause
- NY Governor . (2020b). Governor Cuomo signs the ‘New York State on PAUSE’ Executive Order . governor.ny.gov. Retrieved on December 24, 2020. https://coronavirus.health.ny.gov/new‐york‐state‐pause
- Offenhartz, J. (2020). "The Mail Just Stopped": Coronavirus Staffing Shortages And Budget Gaps Push Postal Service To Brink Of Collapse. Gothamist. Retrieved on December 24. https://gothamist.com/news/mail‐coronavirus‐staffing‐postal‐service‐covid‐19
- Paulson, M. (2020). Broadway, Symbol of New York Resilience, Shuts Down Amid Virus Threat. New York Times. Retrieved on December 24. https://www.nytimes.com/2020/03/12/theater/coronavirus‐broadway‐shutdown.html
- Thompson, C. N. , Baumgartner, J. , Pichardo, C. , Toro, B. , Li, L. , Arciuolo, R. , Chan, P. Y. , Chen, J. , Culp, G. , Davidson, A. , Devinney, K. , Dorsinville, A. , Eddy, M. , English, M. , Fireteanu, A. M. , Graf, L. , Geevarughese, A. , Greene, S. K. , Guerra, K. , … Fine, A. (2020). COVID‐19 Outbreak‐New York City, February 29‐June 1, 2020. Morbidity and Mortality Weekly Report, 69, 1725–1729. 10.15585/mmwr.mm6946a2 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.