

Abstract
Objectives
This study was conducted to develop and evaluate a theoretical model to explain the relationships among participation in individual and social activities, compliance with prevention guidelines, and the perception of fatalism and fear of COVID‐19.
Methods
Cross‐sectional survey of 1,067 participants who were >18 years of age living in different provinces of Turkey recruited between August 15, 2020 and October 15, 2020. We used covariant structural analysis to assess the relationships of the constructs of the theoretical model.
Results
Significant fits were detected for Model 1 (χ2 = 924,389, p < .001, comparative fit index or CFI = 0.944), and for Model 2 (χ2 = 2,253,751, p < .001, CFI = 0.926). The predetermination and luck subdimensions reduce the fear of COVID‐19, while the pessimism subdimension and compliance with preventive measures increase the fear.
Conclusion
In public health crises such as COVID‐19, it is important to plan scientific knowledge‐based public education; take initiatives in accordance with the cultural, social, economic, religious, and local characteristics of the societies; and conduct public health studies covering the whole society.
Keywords: pandemic, prevention, public health systems, risk factors
1. INTRODUCTION
Known since December 2019, COVID‐19 disease continues as a global public health crisis with over 68,000,000 cases and 1.5 million deaths (World Health Organization [WHO], 2020a; WHO, 2020b). This process in which we continue to learn more about the disease and its control every day, successful management of the epidemic and the prevention of disease have become important public health topics. To protect against COVID‐19, the World Health Organization (WHO) makes recommendations such as following personal hygiene rules, maintaining physical distance from other people, and using personal protective equipment such as masks in environments where transmission is a risk (WHO, 2020c). Previous literature reports that several factors affect compliance with these rules for protection against COVID‐19. For example, the belief that COVID‐19 precautions will be effective in preventing disease and the fear of COVID‐19 increase compliance with the restrictions (Clark et al., 2020; Harper et al., 2020). In a study conducted in Australia, individuals adhered to COVID‐19 precautions to support the authorities rather than sanction pressure or being sick due to COVID‐19 (Murphy et al., 2020).
The importance of not only biological factors but also human behavior in the spread of the COVID‐19 virus is well known (Belot et al., 2020). Culture, an element that shapes human behavior, plays an important role in the transmission, diagnosis, and treatment of COVID‐19; therefore, culturally appropriate interventions should be planned to prevent disease (Bruns et al., 2020). One factor affecting compliance with the rules of protection against COVID‐19 is the perception of fatalism. In a study conducted in the United States, the association of COVID‐19 with death and the perception of fatalism negatively affected the intention of the society to exhibit preventive behaviors such as social distancing and hand washing (Jimenez et al., 2020). Individuals who believe that COVID‐19 is contagious were more reluctant to comply with social distancing rules; this has been called the fatalism effect (Akesson et al., 2020). In the United States, participants ignored complying with the preventive measures because they believed that they were destined to be infected with the virus, and this behavior was associated with fatalism (Papageorge et al., 2020). To encourage adherence to preventive measures, a study in Iran recommended reducing fatalistic beliefs and focused on individuals living in rural areas (Shahnazi et al., 2020).
Although the COVID‐19 outbreak is global, interventions should be planned according to the countries and even regions (Bachem et al., 2020). The overall restrictions that are applied in each country are important to prevent the spread of the COVID‐19 virus; however, they have not been sustainable for humans, as we are social beings. For this reason, it is important to determine the factors that affect the behavior of an individual and the society under extraordinary conditions to both manage the current pandemic and to be prepared for possible future pandemics. In the fight against COVID‐19, the importance of increasing the rate of compliance with preventive measures and public awareness about the disease must be emphasized to plan effective public health practices (Jimenez et al., 2020).
There are a limited number of studies investigating participation in individual and social activities during epidemics and their determinants. This study can help understand the determinants of participation in individual and social activities and solution suggestions that should be developed in these situations. Findings guiding public health interventions can be revealed by determining the compliance of the society with the measures during the pandemic and then by explaining the associated factors. From this viewpoint, this study was conducted with the aim of developing and evaluating a theoretical model that could explain the relationships among compliance behaviors for preventive measures against COVID‐19, participation in individual and social activities, and the perception of fatalism and fear of COVID‐19.
2. DEVELOPMENT OF THE MODEL
In the first phase of this study, Guideline on Compliance with Preventive Measures Against COVID‐19 has been prepared. Then, the theoretical model was drawn showing the predicted relationships among participation in individual and social activities, compliance guide score for COVID‐19 preventive measures, Fatalism Scale score, and COVID‐19 Fear Scale score (Figure 1).
FIGURE 1.
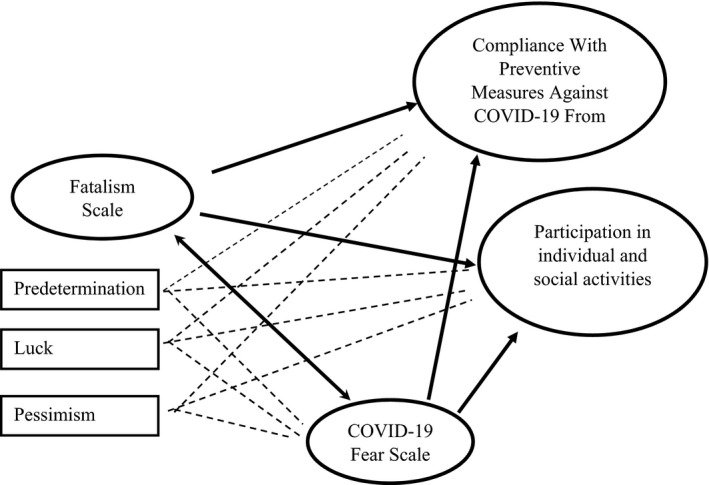
Theoretical model
3. RESEARCH QUESTIONS
What is the level of individuals’ compliance with COVID‐19 preventive measures?
What is the level of the perception of individuals’ fatalism?
What is the level of individuals’ fear of COVID‐19?
4. RESEARCH HYPOTHESES
H1.1: The perception of fatalism and its subdimensions affect behaviors to comply with the preventive measures against COVID‐19.
H1.2: The perception of fatalism and its subdimensions affect participation in individual and social activities during the pandemic.
H1.3: The perception of fatalism and its subdimensions affect the fear of COVID‐19.
H1.4: The fear of COVID‐19 affects behaviors to comply with the preventive measures for COVID‐19.
H1.5: The fear of COVID‐19 affects participation in individual and social activities during the pandemic.
H1.6: The fear of COVID‐19 affects the perception of fatalism.
H1.7: The behavior of complying with preventive measures for COVID‐19 affects participation in individual and social activities.
5. METHODS
5.1. Design and setting
This cross‐sectional study uses covariant structural analysis to verify the appropriateness of the hypotheses and structural model developed for the causal relationships among participation in individual and social activities, compliance with COVID‐19 prevention guidelines, and the perception of fatalism and fear of COVID‐19.
5.2. Sample size/setting and participants
The research sample was made up of participants > 18 years of age living in different provinces of Turkey. Sample size calculation was not made at the beginning of the study. In total, 1,067 participants attended the study between August 15, 2020, and October 15, 2020. However, among these participants, eight questionnaires with missing data were not included in the analyses, with a final sample size of 1,059 participants. The power of the research was calculated as 0.2 effect size in silico and 99% at 0.95 confidence level according to the sample size (n = 1,059).
6. INCLUSION CRITERIA
The following were the inclusion criteria: >18 years, spoke Turkish, were literate, did not have physical/psychiatric disorders that prevent verbal communication, were able to use smart phones and complete online surveys, were living in different provinces and different settlements (rural/urban).
7. EXCLUSION CRITERIA
Excluded from the study were health workers, hospital support services personnel, and teaching staff or students from health‐related departments.
7.1. Instrumentation
Data collection instructions were the Introductory Information Form, Guideline on Compliance with Preventive Measures Against COVID‐19 Form, Fatalism Scale, and COVID‐19 Fear Scale.
7.1.1. Introductory information form
This form included questions about sociodemographic characteristics and participation in individual and social activities (going to health care institutions, using transportation means, attending sporting events, going on tours, going to public places, visiting someone at their home, attending collective ceremonies or celebrations such as weddings, participation in religious activities, and experiencing regret on participating in these activities).
7.1.2. Guideline on compliance with preventive measures against COVID‐19 from
This form was created by researchers using the guidelines on protection from COVID‐19 virus prepared by the WHO, Centers for Disease Control and Prevention (CDC), and the Ministry of Health (Ministry of Health, 2020; WHO, 2020c; CDC, 2020). The draft form was then sent to three faculty members working in other fields to obtain expert opinion in terms of comprehensibility, clarity, and inclusiveness. After obtaining their opinions, some statements were rewritten for clarity, and an additional response option was added. The revised guideline contained 14 statements, all containing positive suggestions. Three response options were possible (never comply with = 1, sometimes comply with = 2, and always comply with = 3), resulting in possible scores from 14 to 42, with higher scores indicating more compliance with preventive measures against COVID‐19 (Appendix Table A1). The Cronbach's alpha coefficient of the guideline was 0.712 in this study.
7.1.3. Fatalism scale
The Fatalism Scale was a 5‐point Likert‐type scale with 20 items; five response options were possible (ranging from 1 = strongly disagree to 5 = strongly agree) (Shen et al., 2009). The scale had three subdimensions: predetermination (items 1–10), luck (items 11–14), and pessimism (items 15–20). Scale scores were totaled and divided by the number of items; higher scores indicated greater fatalistic attitudes. The scale has good Turkish validity and reliability study in Turkish, with Cronbach's alpha coefficient of 0.84 (Kızılarslan & Yıldız, 2020). In our study, the Cronbach's alpha coefficient of the scale was 0.869.
7.1.4. COVID‐19 fear scale
The newly developed COVID‐19 Fear Scale has seven items (Ahorsu et al., 2020). Possible scores range from 7 to 35; higher scores on the scale, the higher is the fear of COVID‐19. The Turkish validity and reliability study of the scale found the Cronbach's alpha coefficient of 0.88; in our study, the Cronbach's alpha was 0.877 (Bakioğlu et al., 2020).
7.2. Data collection
Data in the study were collected through an online questionnaire. Before rolling out the questionnaire forms, the Introductory Information Form was finalized by using it on 10 people outside of the study sample. Study participants were reached using the snowball and chaining method; potential participants who met the study criteria were initially selected from individuals in the social environment of the researchers and their colleagues.
7.3. Data analysis
Data were analyzed using SPSS 25 and AMOS 23, first using with an explanatory, then a confirmatory, and finally a structural equation model.
In the first phase of the analysis, explanatory and confirmatory factor analyses were conducted for the guideline on compliance with preventive measures against COVID‐19; the Kaiser–Meyer–Olkin value was 0.863, Bartlett test result was 1503.196 (p < .05), and Cronbach's alpha coefficient was 0.71, and these results are satisfactory. There was no limitation on the number of factors, and factors with an Eigen value >1.50 were included in the scale, and 16 questions in the guideline were removed as irrelevant. Confirmatory factor analysis was performed for the final version of 14 questions. The model obtained (Chi‐square or χ2 = 128.472, degrees of freedom or df = 77, p < .001) comprised one‐dimension. According to the results obtained from this analysis, it was determined that the guideline had a very good fit (p < .05). Therefore, the final version of the 14‐question guideline was used.
In the second phase of the analysis, structural adaptation analysis was conducted on participation in individual and social activities, compliance with the guideline on preventive measures against COVID‐19, and the perception of fatalism and fear of COVID‐19. First, two structural equation models were developed that allowed simultaneous analysis of the items of the Fatalism Scale, participation in activities, and the items of COVID‐19 Fear Scale, taking into account the prediction and measurement errors. As the goodness of fit values resulting from the initial analysis of the developed models were not within the desired limits, necessary corrections and combinations were made by considering the improvement (modification) indices. After making improvements that could be theoretically established and provided the highest contribution to the model as the correction value, the fit indices of the variables’ subdimensions were considered. Fit of the models, χ2/df, root mean square error of approximation, goodness of fit index, and standardized root mean square residual were evaluated with the comparative fit index (CFI) and incremental fit index. The regression weights of the variables were calculated by considering the standardized estimates, standard error, and critical values of the last developed models.
7.4. Ethical considerations
Before starting the study, permission was obtained from the Scientific Research Board of the Ministry of Health (15.08.2020/08‐11T14_16_03) and University's Ethics Committee (13.08.2020/2020.16.209). Permission was obtained from the authors of the scales used in the study. Information was provided about the purpose of this study at the beginning of the online questionnaire, and the option of providing informed voluntary consent was provided to the participants. The survey form was designed to not allow a participant to start the survey without selecting this option.
8. RESULTS
The average age of the 1,059 participants was 34.42 ± 12.55; 72.5% were female, 52.4% married, 64.9% university graduates, and 51.1% had a job. Of the participants, 4.2% had been diagnosed with COVID‐19 and 54.3% had a family member or neighbor who had had COVID‐19 (Table 1). During the periods when there were no activity restrictions, 52.9% went to parks and gardens, 31.3% to hospitals, 39.2% went on a festive holiday or visited the elderly, 25.7% attended weddings, 15.5% went to markets, 11.1% attended sports or went on a holiday, 8.3% went to places of worship, 15.2% used public transportation, and 31.9% of the individuals regret that they were involved in these activities.
TABLE 1.
Sociodemographic characteristics of the participants (n = 1,059)
| Age (mean ± ss ) | 34.42 ± 12.55 | |
|---|---|---|
| n | % | |
| Gender | ||
| Female | 768 | 72.5 |
| Male | 291 | 27.5 |
| Marital status | ||
| Married | 555 | 52.4 |
| Single | 504 | 47.6 |
| Education level | ||
| Literate | 25 | 2.4 |
| Primary school graduate | 54 | 5.1 |
| Secondary education graduate | 46 | 4.3 |
| High school graduate | 247 | 23.3 |
| University Graduate | 687 | 64.9 |
| Working status | ||
| Yes | 541 | 51.1 |
| No | 518 | 48.9 |
| Job | ||
| Employee | 76 | 7.2 |
| Officer | 321 | 30.3 |
| Retired | 48 | 4.5 |
| Housewife | 139 | 13.1 |
| Unemployed | 107 | 10.1 |
| Other | 368 | 34.7 |
| Living area | ||
| Province | 684 | 64.6 |
| District | 284 | 26.8 |
| Town | 18 | 1.7 |
| Village | 73 | 6.9 |
| Income level | ||
| Income lower than expenses | 241 | 22.8 |
| Income equal to expenses | 619 | 58.5 |
| Income higher than expenses | 199 | 18.8 |
| COVID−19 without diagnosis | ||
| Yes | 45 | 4.2 |
| No | 1,014 | 95.8 |
| Diagnosed with COVID−19 in the family/immediate environment | ||
| Yes | 575 | 54.3 |
| No | 484 | 45.7 |
| Total | 1,059 | 100.0 |
The mean score of compliance with preventive measures against COVID‐19 was high at 38.70 ± 3.15. The mean Fatalism Scale score of the individuals was 2.54 ± 0.57, mean predetermination subdimension was 2.81 ± 0.70, mean luck subdimension was 1.93 ± 0.80, and mean pessimism subdimension was 2.49 ± 0.73. These scores suggested a moderate level of fatalism, a high level of the subdimension of predetermination, a moderate level of the subdimension of pessimism subdimension and a low level of the subdimension of luck subdimension (Table 2).
TABLE 2.
Precaution guide, Fear Scale, Fatalism Scale, and subdimensions scale score distributions of individuals (n = 1,059)
| Scale scores | Mean ± ss | Median | Min‐max |
|---|---|---|---|
|
Guideline on Compliance With Preventive Measures Against COVID−19 From total score |
38.70 ± 3.15 | 40.0 | 18.0–42.0 |
| COVID−19 Fear Scale total score | 19.83 ± 6.11 | 20.0 | 7.00–35.0 |
| Fatalism Scale total score | 2.54 ± 0.57 | 2.55 | 1.0–5.0 |
| Predetermination subdimension | 2.81 ± 0.70 | 2.80 | 1.0–5.0 |
| Luck subdimension | 1.93 ± 0.80 | 2.0 | 1.0–5.0 |
| Pessimism subdimension | 2.49 ± 0.73 | 2.5 | 1.0–5.0 |
In the study, structural adjustment analysis was conducted to determine the relationships among the individuals' participation in individual and social activities, compliance with preventive measures against COVID‐19, Fatalism Scale score, and COVID‐19 Fear Scale score during periods of no restrictions. As a result of the analysis, two models were developed. Significant fits were determined in Model 1 (χ2 = 924,389, df = 296, p < .001) and Model 2 (χ2 = 2,253.751, df = 1,139, p < .001). Models 1 and 2 are shown in Figures 2 and 3, respectively. The data from the developed models are provided in Table 3.
FIGURE 2.
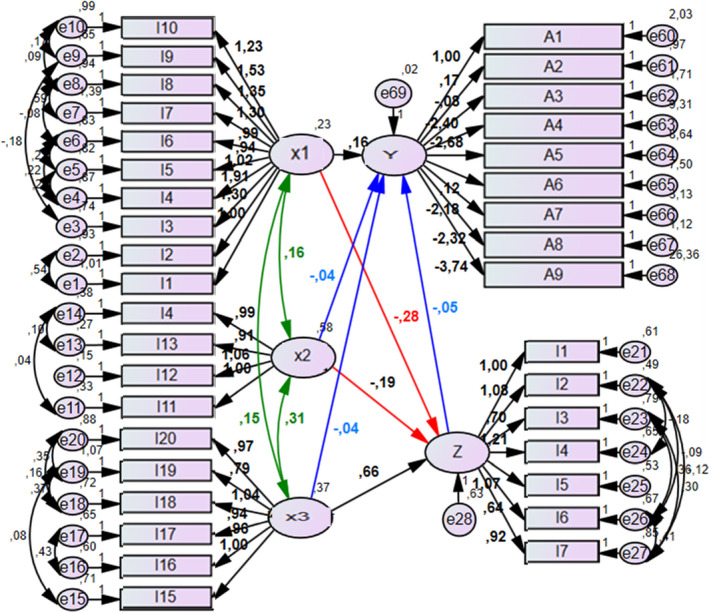
SEM model related to Model 1, x1: Predetermination, x2: Luck, x3: Pessimism, Y: Participation in activities, Z: COVID‐19 fear, A1: Going to public markets, A2: Going to health care institutions, A3: Using transportation means, A4: Attending sporting events and going on tour, A5: Going to public places, A6: Visiting someone (patient, elderly, neighbor, etc.) at home, A7: Attending collective ceremonies or celebrations such as weddings, A8: Participation in religious activities, A9: Experiencing regret on participating in these activities. [Color figure can be viewed at wileyonlinelibrary.com]
FIGURE 3.
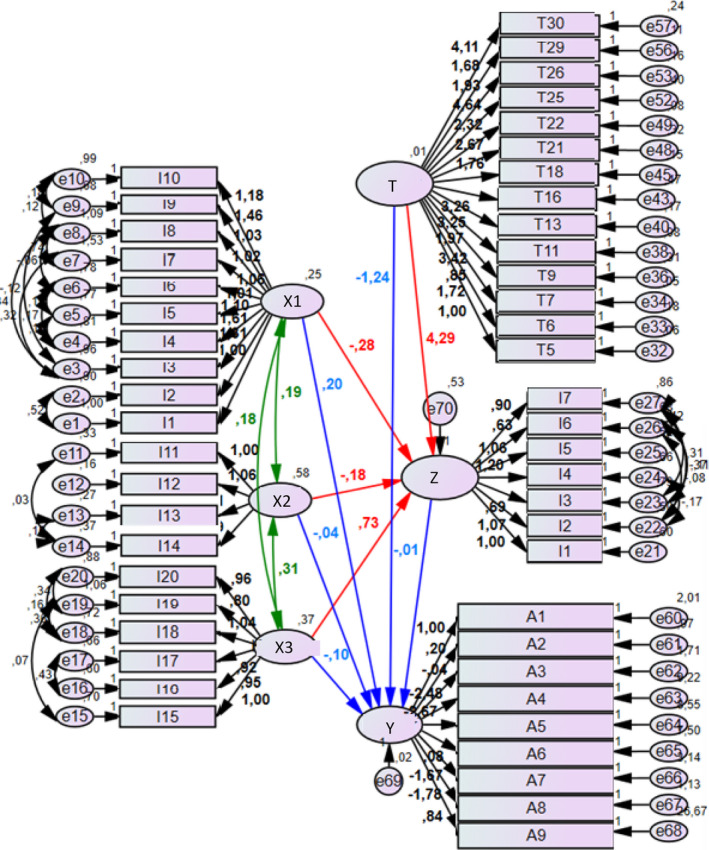
SEM model related to Model 2, x1: Predetermination, x2: Luck, x3: Pessimism, Y: Participation in activities, Z: COVID‐19 fear, T: Compliance With Preventive Measures Against COVID‐19 From, A1: Going to public markets, A2: Going to health care institutions, A3: Using transportation means, A4: Attending sporting events and going on tour, A5: Going to public places, A6: Visiting someone (patient, elderly, neighbor, etc.) at home, A7: Attending collective ceremonies or celebrations such as weddings, A8: Participation in religious activities, A9: Experiencing regret on participating in these activities. [Color figure can be viewed at wileyonlinelibrary.com]
TABLE 3.
Models and values
| χ | df | p | χ/sd | RMSEA | SRMR | IFI | CFI | GFI | TLI | |
|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | 924,389 | 296 | <0,001 | 2,305** | 0,035** | 0,110* | 0,944* | 0,944* | 0,934** | 0,937* |
| Model 2 | 2,253,751 | 1,139 | <0,001 | 1,979** | 0,030** | 0,088* | 0,926* | 0,926* | 0,920** | 0,920** |
Acceptable fit * Good fit **.
The relationships that emerged from Model 1 after the analysis following improvements are provided in Table 4. Accordingly, although other variables also had some influences, the predetermination and luck subdimensions negatively and the pessimism subdimension positively affected the fear of COVID‐19. There is a two‐way positive relationship among the subdimensions of the Fatalism Scale (p < .05). No relationship was found among participation in events, compliance with the COVID‐19 prevention guideline, and the subdimensions of the Fatalism Scale (p > .05; Table 4).
TABLE 4.
Structural equation model regression weights for Model 1 and Model 2 after the adjustments made according to the modification indexes
| Tested Path | Standardized Estimate (β) | Estimate (β) | Standard Error | Critical Value | p | ||
|---|---|---|---|---|---|---|---|
| COVID−19 fear | ← | Predetermination | −0,159 | −0,279 | 0,085 | −3,300 | .001** |
| COVID−19 fear | ← | Luck | −0,170 | −0,189 | 0,063 | −2,994 | .003** |
| COVID−19 fear | ← | Pessimism | 0,470 | 0,656 | 0,106 | 6,202 | .001** |
| Participation in activities | ← | Compliance With Preventive Measures Against COVID−19 From | −0,296 | −0,054 | 0,030 | −1,783 | .075 |
| Participation in activities | ← | Predetermination | 0,486 | 0,156 | 0,082 | 1,887 | .059 |
| Participation in activities | ← | Luck | −0,199 | −0,041 | 0,032 | −1,265 | .206 |
| Participation in activities | ← | Pessimism | −0,162 | −0,041 | 0,047 | −0,884 | .377 |
| Predetermination | <‐> | Pessimism | 0,517 | 0,151 | 0,018 | 8,253 | .001** |
| Predetermination | <‐> | Luck | 0,427 | 0,157 | 0,018 | 8,534 | .001** |
| Luck | <‐> | Pessimism | 0,665 | 0,306 | 0,026 | 11,792 | .001** |
| COVID−19 fear | ← | Predetermination | −0,160 | −0,277 | 0,091 | −3,051 | .002** |
| COVID−19 fear | ← | Luck | −0,157 | −0,177 | 0,061 | −2,895 | .004** |
| COVID−19 fear | ← | Pessimism | 0,516 | 0,729 | 0,108 | 6,767 | .001** |
| COVID−19 fear | ← |
Compliance With Preventive Measures Against COVID−19 From |
0,387 | 4,287 | 0,627 | 6,835 | .001** |
| Participation in activities | ← |
Compliance With Preventive Measures Against COVID−19 From |
−0,497 | −1,237 | 0,503 | −2,457 | .014* |
| Participation in activities | ← | COVID−19 fear | −0,050 | −0,011 | 0,023 | −0,486 | .627 |
| Participation in activities | ← | Predetermination | 0,510 | 0,199 | 0,084 | 2,378 | .017* |
| Participation in activities | ← | Luck | −0,148 | −0,038 | 0,034 | −1,102 | .271 |
| Participation in activities | ← | Pessimism | −0,299 | −0,095 | 0,065 | −1,46 | .144 |
| Predetermination | <‐> | Pessimism | 0,582 | 0,176 | 0,02 | 8,628 | .001** |
| Predetermination | <‐> | Luck | 0,499 | 0,189 | 0,021 | 9,121 | .001** |
| Luck | <‐> | Pessimism | 0,665 | 0,309 | 0,026 | 11,876 | .001** |
p* < .05. p** < .001.
The relationships that emerged from Model 2 after the analysis following improvements are provided in Table 4. Although other variables also had some influences, the predetermination and luck subdimensions negatively and the pessimism subdimension positively affected the fear of COVID‐19. Although other variables also had some influences, compliance with the COVID‐19 prevention guideline positively affected the fear of COVID‐19 and negatively affected participation in activities, and the predetermination subdimension positively affected participation in activities. There is a two‐way positive relationship among the subdimensions of the Fatalism Scale (p < .05). No relationship was found among participation in individual and social activities, fear of COVID‐19, luck subdimension, and pessimism subdimension (p > .05; Table 4).
9. DISCUSSION
Despite the precautions taken and restrictions imposed all over the world, the COVID‐19 disease continues to spread (WHO, 2020b). Setting aside compulsory and unchangeable factors such as working conditions, professions, and socioeconomic status of individuals, failure to comply with the preventive measures against COVID‐19 and the restrictions in the absence of any obstacle is an issue in need of explanation. Factors that are beyond the control of health services and that lead to poor health indicators are unaddressed cultural values. Understanding the cultural factors that affect health‐promoting behaviors is critical (Napier et al., 2014). In this study, the relationships among participation in individual and social activities, compliance with preventive measures against COVID‐19, and the perception of fatalism and fear of COVID‐19 of the participants were examined.
Findings included high scores on compliance with preventive measures against COVID‐19, and individuals mostly complied with the preventive measures. Individuals' fear of COVID‐19 and fatalism were at moderate levels. Among the subdimensions of the Fatalism Scale, the predetermination score was high, pessimism score was medium, and luck score was low (Table 2). Hence, the belief that events such as illness or death are beyond the control of a person and that they are predetermined is more common, the pessimism related to the illness and suffering is moderate, and the belief that being healthy depends on luck is less common.
According to the structural adjustment analysis conducted in the study, two models were developed in which the relationships among the fatalistic attitude of the individuals and fear of COVID‐19, guideline on compliance with the preventive measures against COVID‐19, and participation in individual and social activities were stipulated (Table 3). The structural adjustment analysis following adjustments made according to the modification indexes revealed that the predictive attitude regarding the predetermination of events decreased the fear of COVID‐19 but increased the participation in individual and social activities (Table 4). Individuals' belief that events are predetermined might have also made it unnecessary to worry and fear about COVID‐19, thereby reducing their fear of COVID‐19. Moreover, despite the COVID‐19 pandemic, participants took part in individual and social activities probably due to the belief that whatever happens will happen no matter what the person does and that the contagion may be more related to the destiny than participation in the activities. According to a study, individuals’ belief that they are destined to be infected can lead them to ignore preventive measures against COVID‐19 (Papageorge et al., 2020). Another study identified that individuals who believed that COVID‐19 is contagious were more reluctant to comply with social distancing rules—this situation has been called the fatalism effect (Akesson et al., 2020).
The importance of reducing fatalistic disposition and increasing beliefs in the effectiveness of preventive measures is emphasized to encourage protective behavior against COVID‐19 (Clark et al., 2020; Shahnazi et al., 2020). This study determined that a fatalistic attitude, which equated being healthy with luck, reduced the fear of COVID‐19 (Table 4). This may be due to the fact that individuals explained their health and longevity outside and beyond themselves through luck, an inexplicable abstract concept, denying the determinacy of the contagiousness and virulence of COVID‐19. On the other hand, this study identified that the pessimistic fatalistic attitude regarding being sick and suffering increased the fear of COVID‐19 (Table 4). Accordingly, the pessimistic attitudes of individuals lead them to see themselves as possible patients for COVID‐19, a known deadly and contagious disease. One recent study found that the pessimism and tendency to associate COVID‐19 with death negatively affected individuals' intention to comply with social distancing and exhibit protective behaviors such as hand washing (Jimenez et al., 2020). In this study, no relationship was predicted among individuals' fatalistic attitude, fear of COVID‐19, and their compliance with preventive measures against COVID‐19 (Table 4). On the other hand, adherence to COVID‐19 preventive measures increased the fear of COVID‐19 and decreased participation in activities (Table 4). One study reported that the fear of COVID‐19 was the only variable that determined compliance with preventive measures (Harper et al., 2020). Another study found that those who do not believe in conspiracy theories have a lower fear of COVID‐19 and follow preventive measures more (Jovančević & Milićević, 2020).
9.1. Limitations of the study
This study had limitations. Collecting data through online surveys might have contributed to participants' inability and/or refusal to answer, only those sensitive to the subject answering, problems accessing the questionnaire, and not understanding the importance and sensitivity of the study. However, some measures were taken by the researchers to overcome these problems, including anonymizing the questionnaire, sharing the researcher contact information, and notifying the participants that they can contact the researchers whenever they want. Another limitation was that only those with internet access could participate, limiting generalizability.
We acknowledge that participation in individual and social activities and compliance with preventive measures against COVID‐19 are not independent of the factors addressed in this study and may be influenced by several variables outside the scope of this study (having to go to work, government policies, inefficient audits and measures, etc).
10. CONCLUSION
This study revealed that individuals mostly comply with preventive measures against COVID‐19 and that fatalism and fear of COVID‐19 were at moderate levels. Among the fatalism subdimensions, predetermination was at a high level, pessimism at medium level, and luck at low level. According to the results obtained from the structural fit analysis of participation in individual and social activities, compliance with preventive measures against COVID‐19, and fatalism and fear of COVID‐19, predetermination subdimension reduced the fear of COVID‐19 while increasing participation in individual and social activities, luck subdimension reduced fear of COVID‐19, and pessimism subdimension increased fear of COVID‐19. Compliance with preventive measures against COVID‐19 reduced participation in individual and social activities while increasing the fear of COVID‐19.
In line with these results, recommendations include plan public education that will provide an opinion and attitude based on scientific knowledge instead of a fatalistic attitude regarding diseases such as COVID‐19 that influence and affect the whole society. A second recommendation is to plan initiatives in accordance with the cultural, social, economic, religious, and local characteristics of the societies, although it is a global problem, and conduct public health studies covering the whole society. The guideline on compliance with preventive measures against COVID‐19 developed in this study may be used to evaluate other factors (news, social media, religion, etc.) that affect the behavior of different societies in social communicable diseases.
11. CONFLICT OF INTEREST FORM
No conflict of interest has been declared by the author(s).
AUTHOR CONTRIBUTIONS
K.Ö., G.D.BB, and A.Ç. were responsible for the study conception and design. A.Ç., and K.Ö. performed the acquisition of data. G.D.BB performed the data analysis. K.Ö., G.D.BB, and A.Ç. were responsible for the drafting of the manuscript. K.Ö., G.D.BB, and A.Ç. made revisions to the paper for important intellectual content, and supervised the study. All authors contributed equally to this study.
PERMISSIONS TO USE SCALES
Permissions for the scales used in the study were taken from related persons.
1.
TABLE A1.
Guidelines on compliance with preventive measures against COVID‐19
| Yes | Sometimes | No | |
|---|---|---|---|
| 1. If there is no handkerchief while coughing or sneezing, I cover my mouth with the inside of my elbow. | |||
| 2. I do not share any of my personal belongings. | |||
| 3. I often ventilate the environment I am in. | |||
| 4. I consume plenty of fluids to strengthen my immune system, eat a balanced diet, and pay attention to my sleep patterns. | |||
| 5. I wash my hands often with soap and water for at least 20 s. | |||
| 6. I maintain social distance (at least 1 m). | |||
| 7. I try to cancel or postpone my travels. | |||
| 8. If there is an alcohol‐containing disinfectant in the places I go, I will definitely use it. | |||
| 9. I prefer cashless or contactless payment options whenever possible. | |||
| 10. I try to use disposable materials wherever I go. | |||
| 11. I always carry alcohol‐based hand disinfectant with me and use it when necessary. | |||
| 12. I avoid meeting with people who have chronic illnesses or older people to avoid contagion. | |||
| 13. When I get together at events such as weddings, engagements, etc., I pay more attention to social distance. | |||
| 14. I warn people around me about social distancing and the use of masks. |
Özdil K, Bulucu Büyüksoy GD, Çatiker A. Fatalism, fear, and compliance with preventive measures in COVID‐19 pandemic: A structural equation modeling analysis. Public Health Nurs. 2021;38:770–780. 10.1111/phn.12898
Funding information
This research received no specific grant from any funding agency in the public, commercial, or not‐for‐profit sectors.
[Correction added on 14 July 2021, after first online publication: The surname of the last author was corrected to read as “Çatıker”.]
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available form the corresponding author [KÖ] upon reasonable request.
REFERENCES
- Ahorsu, D. K. , Lin, C.‐Y. , Imani, V. , Saffari, M. , Griffiths, M. D. , & Pakpour, A. H. (2020). The Fear of COVID‐19 Scale: Development and initial validation. International Journal of Mental Health and Addiction. 1–9. Advance online publication. 10.1007/s11469-020-00270-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Akesson, J. , Ashworth‐Hayes, S. , Hahn, R. , Metcalfe, R. D. , & Rasooly, I. (2020). Fatalism, beliefs, and behaviors during the COVID‐19 pandemic (No. w27245). Cambridge, MA: National Bureau of Economic Research. NBER Working Paper No. 27245, May. https://www.nber.org/papers/w27245 [Google Scholar]
- Bachem, R. , Tsur, N. , Levin, Y. , Abu‐Raiya, H. , & Maercker, A. (2020). Negative affect, fatalism, and perceived institutional betrayal in times of the coronavirus pandemic: A cross‐cultural investigation of control beliefs. Frontiers in Psychiatry, 11, 589914. 10.3389/fpsyt.2020.589914 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bakioğlu, F. , Korkmaz, O. , & Ercan, H. (2020). Fear of COVID‐19 and positivity: Mediating role of intolerance of uncertainty, depression, anxiety, and stress. International Journal of Mental Health and Addiction. 1–14.Advance online publication. 10.1007/s11469-020-00331-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Belot, M. , Choi, S. , Jamison, J. C. , Papageorge, N. W. , Tripodi, E. , van den Broek‐Altenburg, E. (2020). Six‐Country Survey on Covid‐19. IZA Discussion Paper No. 13230.
- Bruns, D. P. , Kraguljac, N. V. , & Bruns, T. R. (2020). COVID‐19: Facts, cultural considerations, and risk of stigmatization. Journal of Transcultural Nursing, 31(4), 326–332. 10.1177/1043659620917724 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Center for Disease Control and Prevention (CDC) . (2020). Personal and Social Activities. https://www.cdc.gov/coronavirus/2019‐ncov/daily‐life‐coping/personal‐social‐activities.html
- Clark, C. , Davila, A. , Regis, M. , & Kraus, S. (2020). Predictors of COVID‐19 voluntary compliance behaviors: An international investigation. Global Transitions, 2, 76–82. 10.1016/j.glt.2020.06.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harper, C. A. , Satchell, L. P. , Fido, D. , & Latzman, R. D. (2020). Functional fear predicts public health compliance in the COVID‐19 pandemic. International Journal of Mental Health and Addiction, 1–14.Advance online publication. 10.1007/s11469-020-00281-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jimenez, T. , Restar, A. , Helm, P. J. , Cross, R. I. , Barath, D. , & Arndt, J. (2020). Fatalism in the context of COVID‐19: Perceiving coronavirus as a death sentence predicts reluctance to perform recommended preventive behaviors. SSM Popul Health, 11, 100615. 10.1016/j.ssmph.2020.100615 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jovančević, A. , & Milićević, N. (2020). Optimism‐pessimism, conspiracy theories and general trust as factors contributing to COVID‐19 related behavior ‐ A cross‐cultural study. Personality and Individual Differences, 167, 110216. 10.1016/j.paid.2020.110216 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kızılarslan, V. , & Yıldız, E. (2020). Kaderci̇li̇k Ölçeği̇ni̇n Türkçe Geçerli̇li̇k ve Güveni̇li̇rli̇ği̇ Çalışması. Turkish Validity and Reliability Study of the Fatalism Scale. Yüksek Lisans Tezi. Atatürk Üni̇versi̇tesi̇, Sağlik Bi̇li̇mleri̇ Ensti̇tüsü. Erzurum.
- Murphy, K. , Williamson, H. , Sargeant, E. , & McCarthy, M. (2020). Why people comply with COVID‐19 social distancing restrictions: Self‐interest or duty? Australian & New Zealand Journal of Criminology, 53(4), 477–496. 10.1177/0004865820954484 [DOI] [Google Scholar]
- Napier, A. , Ancarno, C. , Butler, B. , Calabrese, J. , Chater, A. , Chatterjee, H. , Guesnet, F. , Horne, R. , Jacyna, S. , Jadhav, S. , Macdonald, A. , Neuendorf, U. , Parkhurst, A. , Reynolds, R. , Scambler, G. , Shamdasani, S. , Smith, S. Z. , Stougaard‐Nielsen, J. , & Thomson, L. (2014). Culture and health. The Lancet, 384(9954), 1607–1639. 10.1016/S0140-6736(14)61603-2 [DOI] [PubMed] [Google Scholar]
- Papageorge, N. W. , Zahn, M. V. , Belot, M. , van den Broek‐Altenburg, E. , Choi, S. , Jamison, J. C. , & Tripodi, E. (2021). Socio‐demographic factors associated with self‐protecting behavior during the COVID‐19 pandemic. J Popul Econ, 34, 691–738. 10.1007/s00148-020-00818-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Republic of Turkey, Ministry of Health . (2020) Novel coronavirus disease. (COVID‐19). https://covid19bilgi.saglik.gov.tr/tr/
- Shahnazi, H. , Ahmadi‐Livani, M. , Pahlavanzadeh, B. , Rajabi, A. , Hamrah, M. S. , & Charkazi, A. (2020). Assessing preventive health behaviors from COVID‐19: A cross sectional study with health belief model in Golestan Province, Northern of Iran. Infectious Diseases of Poverty, 9(1), 157. 10.1186/s40249-020-00776-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shen, L. , Condit, C. M. , & Wright, L. (2009). The psychometric property and validation of a fatalism scale. Psychology & Health, 24(5), 597–613. 10.1080/08870440801902535 [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization (WHO) (2020a). Coronavirus disease (COVID‐19) dashboard. https://covid19.who.int/
- World Health Organization (WHO) (2020b). WHO Timeline COVID‐19. Retrieved from https://www.who.int/news‐room/detail/27‐04‐2020‐who‐timeline‐‐‐covid‐19
- World Health Organization (WHO) . (2020c). Coronavirus disease (COVID‐19) advice for the public. Retrieved from https://www.who.int/emergencies/diseases/novel‐coronavirus‐2019/advice‐for‐public
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available form the corresponding author [KÖ] upon reasonable request.