

Abstract
Introduction
COVID‐19 forced e‐learning processes to develop abruptly and posed challenges to the educational infrastructure. Emergency Remote Teaching was designated to distinguish the new educational scheme. This concept involves production of online activities that may return to face‐to‐face format as soon as the isolation period ends.
Objective
From March through September of 2020, this systematic review attempted to elucidate experiences, benefits, and challenges enforced in dental education due to the pandemic, the learning technologies, and methods used to maintain education.
Methods
A literature search was conducted on Cochrane, Embase, Lilacs, Livivo, PubMed, Scopus, and Web of Science databases. Gray literature was also contemplated. Studies in which online teaching methods were described and dental learners were the subjects during pandemic were included.
Results
Learning technology, pedagogical model, knowledge gain, and dental learners’ satisfaction and attitudes toward remote learning were assessed. The Joanna Briggs Institute JBI Critical Appraisal Checklist for Case Reports was applied as the methodological quality assessment to the 16 included studies. Assessments were related to demographic and historical characteristics of the participants, the intervention procedure, pre‐ and post‐intervention descriptions, and identification of unanticipated events. All studies described the use of learning technology to ensure education continuity, and 15 studies highlighted the pedagogical model applied. Eight studies investigated knowledge gain while 12 searched the learners’ satisfaction with online technologies.
Conclusion
The evidence suggests that learning technologies can support continuity in dental education. Reported problems include poor knowledge of faculty members on how to deal with technology, Internet connection, and content transition to online education.
Keywords: coronavirus, Covid‐19, dental education, dentistry, e‐learning, emergency remote teaching, systematic review
1. INTRODUCTION
In December 2019, a novel type of pneumonia was reported in Wuhan, China. The viral agent was identified as a beta coronavirus, and the respective infection was named as “Coronavirus Disease 2019 (COVID‐19).” 1 The pandemic and subsequent mitigation measures have acquired great proportions and its impact on society has become increasingly significant. With regard to education, more than 990 million learners in all levels have been affected, which corresponds to 56.6% of total enrolled learners of the world. 2
Unlike many other careers, dentistry is a fusion of three educational components: theory, laboratory, and clinical practice. During the COVID‐19 pandemic, dentists were classified in the very high risk category because of the potential of exposure to coronavirus through aerosol‐generating procedures. 3 Despite the fact that a number of online dental academic programs were available, this pandemic forced e‐learning processes to develop abruptly and posed unprecedented challenges to the dental educational infrastructure.
Online learning is used as an alternative to keep learners engaged in order to minimize the consequences of social isolation policies on academic activities. 4 , 5 Technologies such as virtual reality simulators and augmented reality, which are tools for training learners through interaction with a total or partially three‐dimensional environment, have facilitated the introduction of these strategies in some dental schools, especially for preclinical disciplines. 6 , 7
Hence, the term Emergency Remote Teaching (ERT) was designated to distinguish new educational activities during the pandemic from distance education that already existed in some schools. This concept involves production of totally online activities that may return to face‐to‐face format as soon as the isolation period ends. Thus, the main objective is not to create a new educational model, but to minimize quarantine effects making content accessible to learners during this time. 4 , 8 , 9
In this systematic review, ERT experiences were evaluated, including benefits and challenges enforced in dental education due to the pandemic, as well as the learning technologies and educational methods that can ensure continuity in the education of dental learners at any level.
2. METHODS
2.1. Protocol and registration
This systematic review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) checklist. 10 The protocol was registered in the PROSPERO database (University of York) (http://www.crd.york.ac.uk/PROSPERO)11 under number CRD42020213610.
2.2. Study design
A systematic review that analyzed education in dentistry during the COVID‐19 pandemic was performed to answer the question: “Which are the experiences, benefits and concerns with dental education during the Covid‐19 pandemic?”
2.3. Eligibility criteria
2.3.1. Inclusion criteria
Retained articles were those studies whose objective was to evaluate any method of remote education during the COVID‐19 pandemic for dental learners at any level.
2.3.2. Exclusion criteria
The following exclusion criteria were applied:
Reviews, editorials, letters, personal opinions, book chapters and conference abstracts.
Studies in which no online curricular teaching method was described.
Studies in which dental learners were not the participants.
Studies in which the main objective was to describe learners’ perceptions and anxiety about remote education without clearly describe the adopted intervention.
Data collected before Covid‐19 pandemic.
Studies written in non‐Latin alphabets.
2.4. Information sources and search strategy
Individual search strategies for each of the following bibliographic databases were developed: Cochrane, Embase, Lilacs, Livivo, PubMed, Scopus and Web of Science. A gray literature search was taken using Google Scholar, ProQuest, and Open Grey (Online Appendix 1). A filter restricting to 2019–2020 years was applied to all databases, except Cochrane Database. The end search date was September 21, 2020 across all databases. Manual searches of reference lists of relevant articles and theses and dissertations were also performed.
All references were managed by reference manager software (Mendeley, Elsevier) and duplicate hits were removed.
2.5. Study selection
The selection was completed in two phases. In phase one, two reviewers (GNMS and HECS) independently reviewed the titles and abstracts of all identified electronic database citations. Articles that did not meet the inclusion criteria were discarded. In phase two, the same reviewers applied the inclusion criteria to the full text of the articles. Both phases were completed using the Rayyan QCRI website (https://rayyan.qcri.org). The references list of selected studies was critically assessed by both examiners (GNMS and HECS). Any disagreement in the first or second phase was resolved by discussion until consensus between the two authors was attained. When a consensus was not reached, a third author (AFL) was involved to make a final decision.
2.6. Data collection process and data items
One author (GNMS) collected the required data from the selected articles. A second author (HECS) cross‐checked all the collected information. Again, any disagreement was resolved by consensus or the third author (AFL) decision. For each of the included studies, items recorded were as follows: author, year of publication, country, educational institution, learning technology, subjects, pedagogical model, main results, and conclusions. If the required data were not complete, attempts were made to contact the authors to retrieve any pertinent missing information.
2.7. Methodological quality assessment of included studies
The Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Case Reports was adapted and applied as the methodological quality assessment. 12 Regarding JBI quality appraisal, two reviewers (GNMS and HECS) scored eight items as Yes, No, Unclear, and Not Applicable for 16 included articles. Any disagreement was resolved by consensus or a third author (AFL) decision.
2.8. Outcomes of interest
Included manuscripts were synthesized in a qualitative and quantitative description focused on two major axes, “the learning technology” and “the pedagogical model,” and two minor axes, “knowledge gain” and “dental learners’ satisfaction and attitudes toward remote learning.”
2.9. Synthesis of results
A meta‐analysis was planned since the data from the included studies were considered relatively homogeneous.
3. RESULTS
3.1. Study selection
In phase one, 754 studies were retrieved from the seven electronic databases. In addition, 100 studies were retrieved from Google Scholar and three from ProQuest. No additional study was found across Open Grey. Afterward, duplicate articles were removed, resulting in 649 remaining different studies. Then, a comprehensive evaluation of the abstracts was conducted and 618 articles were excluded from databases. No additional articles were identified from the reference lists of these studies, resulting in 31 studies at the end of phase one. Therefore, 31 manuscripts were elected to conduct a full‐text review and later 15 studies were excluded (Online Appendix 2). Finally, 16 studies were selected for inclusion per study parameters (Figure 1).
FIGURE 1.
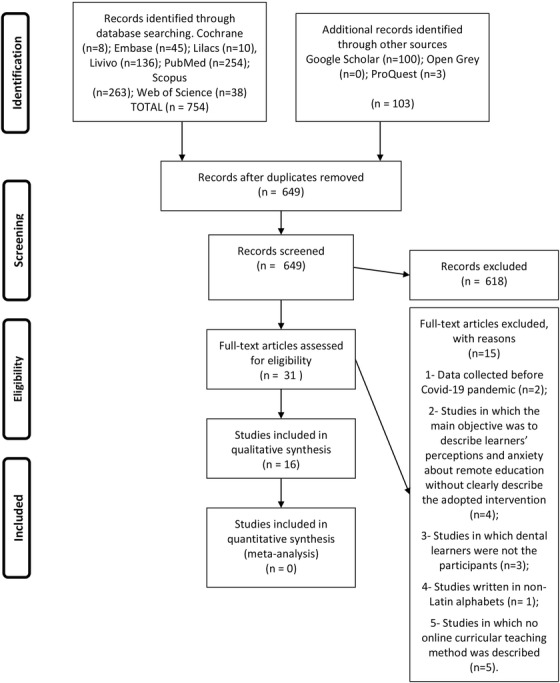
Flow diagram of literature search and selection criteria
3.2. Study characteristics
The 16 included studies were published in three different types of journals: dental sciences, 13 , 14 multidisciplinary scientific publications, 15 , 16 , and educational publications. 17 , 18 , 19 , 20 , 21 , 22 , 23 , 24 , 25 , 26 , 27 , 28 The studies were conducted in nine different countries: Brazil, 15 Canada, 28 China, 16 Costa Rica, 13 France, 17 Nepal, 14 Peru, 18 Serbia, 24 and the United States. 19 , 20 , 21 , 22 , 23 , 25 , 26 , 27 Fifteen studies were published in English and one in Portuguese. 15 Sample size ranged from 10 17 to 45013 participants. A summary of the study's descriptive characteristics can be found in Table 1.
TABLE 1.
Summary of descriptive characteristics of included studies (n = 16)
| Author(s)/ year/ country/ institution | Learning technology | Subjects | Pedagogical model | Results | Conclusion |
|---|---|---|---|---|---|
|
Aguilar‐Gálvez et al. (2020) Peru University Científica del Sur |
Virtual learning object | 13 undergraduate dental students | Asynchronous teaching material to learn the diagnosis for dental caries. |
VLO group correctly answered 90% of the questions. The virtual synchronous class group correctly answered 40% of the same questions. The opinions about VLO were favorable. |
This new virtual proposal application is recommended. |
|
Chavarría‐Bolaños et al. (2020) Costa Rica University of Costa Rica |
Metics platform | 450 undergraduate dental students |
Synchronous and asynchronous meetings with several didactic activities like interdisciplinary seminars, video demonstrations, clinical case discussions, diagnosis, and treatment plans of virtual simulated patients. Training in a virtual environment was provided. |
26% of the courses could be totally virtualized, while 32% were unfeasible. All students had access to a virtual environment using either a laptop, a cell phone, a tablet, or a desk computer. |
Strategies and changes will be analyzed for reinsertion into the clinical activities Feedback from the students the teachers is essential. |
|
Galibourg et al. (2020) France Paul Sabatier University |
Autonomous simulation equipment, including a micromotor and Zoom | 10 undergraduate dental students |
Two 30‐minute sessions of practical work in restorative dentistry and prosthodontics guided by the live teacher's explanations and videos. |
Learning motor skills, keeping human connection through interaction with teachers, and allowing students to spend time practicing, either during remote‐training sessions or independently were pointed advantages. | Future work should consider the educational and clinical benefit of this technology and its use postpandemic. |
|
Gardner et al. (2020) USA University of Texas |
Virtual dental clinic | 35 third‐year dental students and 45 fourth‐year students. |
Small‐group learning through synchronous videoconferencing, case presentations and discussion, article reviews, and videos of procedures in dentistry. |
Fourth‐ years students, felt that sessions promoted their critical thinking and solidification of concepts learned earlier. Third‐years students felt that they learned less during the sessions than they did through traditional education. | Groups felt that prosthodontics/restorative dentistry, practice management, oral pathology, and general practice should continue online in the future. This allows students to benefit from multimodal learning. |
|
Gyurko et al. (2020) USA Tufts University School of Dental Medicine |
Touch surgery virtual reality mobile application and Zoom | Predoctoral and post clinical dental learners, divided into groups of about 20. |
The mobile application allowed learners to experience a step‐by‐step periodontal procedure. Periodontal synchronous sessions via Zoom and presentation of clinical cases by learners. Knowledge retention was assessed by question/ answer pre and post‐activity. |
The case presentation provided real‐life examples for the virtual reality application. The schedule of 60 minutes was too short to cover all planned activities. Some of the questions could have been answered simultaneously. |
Future virtual rotations may include the use of augmented reality and individual learner participation to “perform” the surgical procedures. Physical participation in actual live periodontal surgeries will still be necessary. |
|
Kakadia et al. (2020) USA Harvard School of Dental Medicine |
Zoom | 34 predoctoral dental students. |
Students were equally split into two synchronous sessions, in Zoom breakout rooms. A clinical case was disseminated to each student session one hour before the class starts. Six minutes were allotted per station for oral examinations based on the clinical case given. |
OSCE was similarly successful to traditional OSCE, and all respondents felt they were able to fully showcase their knowledge. Half of the respondents thought that even future OSCEs should be performed online. There were problems related to technical difficulties. | Considering the overall success of the online OSCE and positive feedback from students and examiners/staff, there may be value in moving traditionally in‐person assessments online, even post‐pandemic. |
|
Mladenovic et al. (2020) Serbia University of Pristina |
PowerPoint presentations distributed to students via e‐mail or Moodle Dent.INJURY APP Mobile application |
31 final year undergraduate dental students |
Mobile application for studying traumatic dental injury on an online work week. A questionnaire with a Likert scale via Google Forms assessed the student's satisfaction with the additional mobile learning. |
More than 90% of the students assert that the application has helped them. This type of additional learning has the advantage of being available at all times. | Mobile learning provides a high level of commitment, innovation, personalization, and autonomy. The application allowed students to explore content at their own pace, dive deeper into the most interesting topics, and reward their curiosity with instant answers. |
|
Moore et al. (2020) USA University of North Carolina |
Zoom and Echo360 |
Doctor of Dental Surgery program |
Personnel were asked to provide support to all faculty and students transitioning to online education. Sessions via Zoom and Echo360 were provided. eProctor (ExamN, by AllofE in the eMedley suite) was the assessment tool solution. |
88% of the students were satisfied or extremely satisfied with the instructors’ use of technology 77% were satisfied or extremely satisfied with Zoom platform. 67% said that nothing is limiting their ability to participate in online learning activities. |
Online classes via Zoom and Tests with eProctor tool were well received by the students. |
|
Nair et al. (2020) USA University of Iowa |
PowerPoint presentation template with prefilled patient information and additional reading material. | 20 final‐year undergraduate dental students |
A real clinical case and links with additional reading material about the patient's major health condition were sent to students. Students appraised it using the risk of ROHD assessment. This tool consists of a set of 10 open‐ended questions, about Geriatric and Special Needs Dentistry. Each assessment took approximately 45 minutes to complete. |
The students’ responses were detailed and reflected in individual decision‐making styles. Students subjectively interpreted some case information and qualified their recommendations accordingly. |
The unexpected positive result was that the application of the ROHD skillset resulted in recommended patient outcomes. Students’ self‐reported biases helped to provide context for why a particular risk stage and treatment plan was chosen. |
|
Omar et al. (2020) USA A.T. Still University |
Simulation center management solution (CAE Learning Space) was introduced as the Standardized patient encounter platform. Zoom | 60 first‐year and 41 second‐year undergraduate dental students. | Patients, students, and faculty received previous instructions. The software linked each encounter to a recorded Zoom meeting. Recorded encounters enabled the faculty to observe them and to provide feedback. This also enabled the students to revisit their encounters for self‐improvement. | Students’ feedback was positive and the majority of the encounters were successful. Technical issues related to pop‐up blockers and unstable Internet connectivity were experienced. | The incorporation of online standardized patient encounters through a web‐based platform represented a useful tool to enhance dental students’ communication skills in the preclinical years. |
|
Pani & Vieira (2020) Canada University of Western Ontario |
OWL – Online platform | 76 undergraduate dental students and two pediatric dentists |
Groups of six students were in a two‐hour live session. The session was divided into a 15‐minute case presentation and selection of simulated clinical exercises, followed by restorative exercises for a 1h 30min, and a 15‐min group discussion of the different techniques chosen. An online forum was set up to allow students to continue the debate online via the OWL platform. |
Feedback suggested that students would prefer a continuation of the model even after the current restrictions were lifted. For instructors, moving the pre‐reading and case scenario online allowed for more focused discussions and better time management. |
The integration of an online LMS to clinical and/or pre‐clinical exercises may provide a useful solution to maximize contact time in the current pandemic scenario. |
|
Patel et al. (2020) USA University of Texas |
The Simulation Team developed a series of synchronous teledentistry encounters using live actors as patients. | 93 third‐year undergraduate dental students |
Students were tasked with two eight‐minute patient encounters in which they provided differential diagnosis and care. Immediate feedback was provided by the faculty. Encounters were recorded and reviewed three weeks after when students rated their performance. |
For the pre‐survey, 64% reported some level of discomfort. Following the exercise, 23% reported continued discomfort with the idea of teledentistry. |
The survey revealed that comfort level improved. Simulation exercises provided opportunities to teach and test telehealth practices. |
|
Patterson et al. (2020) USA University School of Dentistry, Virginia University of Texas University College of Dentistry, Dallas, Texas University of Florida |
Zoom incorporating Microsoft PowerPoint lecture and Mentimeter AB platform. | 50 pediatric dental residents |
Mentimeter AB enabled multiple‐choice quiz questions during the presentation to assess information knowledge and multiple‐choice quiz questions following the presentation to assess information retention. Results of the presentation quiz outcomes were discussed in real‐time. |
Pediatric dentistry residents reported a positive learning experience. Participants correctly answered 61% of the questions queried during the presentation and 83% following the presentation. |
Response anonymity eliminates intimidation while fostering participation for small groups, whereas for larger programs the data collected assists presenters in restructuring real‐time content delivery for improved efficacy. Constructing parallel pre and post‐evaluations may enhance relevant learning outcomes. |
|
Spalding et al. (2020) Brazil Dentistry School of Science and Technology Institute of Paulista State University (ICT‐Unesp) |
PowerPoint presentation recorded in Zoom, Moodle Platform, Google Meet, Google Classroom™ and Kahoot!© | 86 first‐year undergraduate dental students |
Video classes were available in Moodle or Google classroom prior to flipped classrooms via Google Meet. Practical histologic microscopy slides were available in Moodle and Google Meet platforms, as a part of flipped classrooms. The encounters were synchronous, including debates, discussions, and clarifications of doubts. Kahoot!© quizzes enabled synchronous tests. Theoretical and practical assessments were done via Moodle. |
More than 80% of the students had satisfactory or very satisfactory performance. More than 50% of the students had an average grade above seven using Kahoot!© quizzes. |
Digital tools and teaching platforms will not solve Brazilian educational problems. Changes in the learning and teaching conception and commitment between all people involved in this process are necessary. That is also recommended strategies focused on mental health. |
|
Tuladhar et al. (2020) Nepal Gandaki Medical College |
Zoom platform | 74 undergraduate dental students and 135 undergraduate medical students | Synchronous online classes for the theoretical portion of the curriculum. |
77.51% rated online classes as non‐effective. The majority of students rated the understanding of online classes as moderate. 58.4% suggested that the teachers need training on how to take online classes; Only 27.30% suggested continuing the online classes after the pandemic. |
Problems in Internet connectivity due to electricity cut down. Students will need a revision of some of the topics covered during the online classes once they are back to regular traditional classes. |
|
Zhong et al. (2020) China Nanjing Medical University |
Online e‐Learning platform of Nanjing Medical University Virtual Simulation Experiment Teaching Center for Dentistry |
94 third‐year undergraduate dental students |
Online oral histopathology course plus face‐to‐face laboratory learning (Online group), compared to the previous face‐to‐face course (Traditional group). Recorded theoretical lessons and scanned conventional stained slices were given through the e‐learning platform. There were prompt instructors for each online class. |
The total test score of the Online group was significantly higher than that of the Traditional group. There were no differences in the Lab test scores between the groups. Remote learning and virtual microscopy courses were well accepted by students. |
Remote learning and virtual technology have a positive impact on oral histopathology and this represents a promising tool for dental education in the future. |
Abbreviations: CAE, Civil Aviation Education; LMS, Learning management system; OSCE, Online Objective Structured Clinical Examinations; ROHD, Rapid Oral Health Deterioration; VLO, Virtual learning object.
3.3. Methodological quality assessment of included studies
All 16 selected studies were experience reports. Due to the similarity of text structure to case reports, they were evaluated by using JBI Critical Appraisal Checklist for Case Reports, 12 with a checklist adapted to the educational context. The methodological assessment ranges from low quality: one to three “yes” answers; moderate‐quality: four to six “yes” answers or high quality: seven or eight “yes” answers.
Thirteen studies 13 , 14 , 16 , 17 , 18 , 19 , 20 , 21 , 22 , 24 , 25 , 26 presented moderate methodological quality while three studies 15 , 23 , 28 showed high methodological quality.
All studies clearly reported the educational situation of the learners during the pandemic period and provided takeaway lessons. However, some selected studies presented methodological problems related to learners’ assessment methods (pre‐intervention), learning technology, or learning model application and unexpected events. Only two studies clearly described demographic and social learners’ characteristics. 13 , 14 In one study, learner population's history was missing 17 and in another, the postintervention outcomes were not described. 13 More information about methodological assessment may be found in Table 2.
TABLE 2.
Methodological quality of included studies (adapted from the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Case Reports)
| Checklist questions | Aguilar‐Gálvez et al. (2020) (18) | Chavarría‐Bolaños et al. (2020) (13) | Galibourg et al. (2020) (17) | Gardner et al. (2020) (21) | Gyurko et al. (2020) (22) | Kakadia et al. (2020) (23) | Mladenovic et al. (2020) (24) | Moore et al. (2020) (25) |
|---|---|---|---|---|---|---|---|---|
| Were learner population's demographic and social characteristics clearly described? | No | Yes | No | No | No | No | No | No |
| Was the learner population's history clearly described (considering the analyzed context)? | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes |
| Was the current educational situation of the learners in the context clearly described? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Were assessment methods and the results clearly described (pre‐intervention)? | Yes | Yes | No | No | No | Yes | No | Yes |
| Was the intervention(s) or procedure(s) / resource(s) (learning technology) or (learning model) clearly described? | Yes | Yes | Yes | Yes | Yes | Yes | No | No |
| Were the post‐intervention outcomes clearly described? | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Were unwanted or unanticipated events identified and described? | No | No | Yes | No | Yes | Yes | No | Yes |
| Does the experience report provide takeaway lessons? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Methodological quality * | Moderate | Moderate | Moderate | Moderate | Moderate | High | Moderate | Moderate |
| Checklist questions | Nair et al. (2020) (26) | Omar et al. (2020) (27) | Pani & Vieira (2020) (28) | Patel et al. (2020) (19) | Patterson et al. (2020) (20) | Spalding et al. (2020) (15) | Tuladhar et al. (2020) (14) | Zhong et al. (2020) (16) |
|---|---|---|---|---|---|---|---|---|
| Were learner population's demographic and social characteristics clearly described? | No | No | No | No | No | No | Yes | No |
| Was the learner population's history clearly described (considering the analyzed context)? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Was the current educational situation of the learners in the context clearly described? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Were assessment methods and the results clearly described (pre‐intervention)? | No | No | Yes | Yes | No | Yes | No | Yes |
| Was the intervention(s) or procedure(s) / resource(s) (learning technology) or (learning model) clearly described? | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes |
| Were the post‐intervention outcomes clearly described? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Were unwanted or unanticipated events identified and described? | No | Yes | Yes | No | No | Yes | Yes | No |
| Does the experience report provide takeaway lessons? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Methodological quality * | Moderate | Moderate | High | Moderate | Moderate | High | Moderate | Moderate |
Low quality: 1–3 “yes” answers; Moderate quality: 4–6 “yes” answers; High quality: 7 or 8 “yes” answers.
3.4. Results
In order to answer the main question of this systematic review, the following outcomes of interest were considered.
3.4.1. Major axes
The learning technology
Six studies reported the development of a new learning technology and its exclusive use. 13 , 16 , 18 , 19 , 21 , 28 Six articles described the use of commercially available platforms 14 , 15 , 20 , 23 , 25 , 26 while four studies combined new developed tools with preexistent technology. 17 , 22 , 24 , 27 Most of the adopted technologies had both computer and mobile phone interfaces. However, two programs had a mobile‐only interface. 22 , 24
In addition to general dentistry, specific theoretical themes were addressed: oral histology, 15 oral histopathology, 16 dental caries diagnosis, 18 dentistry, 21 traumatic dental injuries, 24 geriatric and special needs dentistry, 26 and pediatric dentistry. 20 , 28
The application of learning technology in laboratory activities was described in four studies. 15 , 16 , 17 , 22 Virtual microscopy has opened a new digital model of oral histology and histopathology practical learning in which conventional stained slices were scanned, and microscope images were shared over computer networks. 15 , 16 To improve motor skills in restorative dentistry and prosthodontics, a simulator that includes a micromotor was distributed to learners to perform hands‐on training at home with the aid of videoconferences. 17 To allow learners to experience a step‐by‐step periodontal procedure, a virtual reality mobile application was demonstrated in one study. 22
In addition, some studies aimed to replicate a clinical care scenario. Three of these studies provided online clinical cases so learners could develop diagnostic skills and treatment plans. 13 , 23 , 26 Also, one study provided virtual meetings between learners and simulated patients (actors), simulating clinical interaction. 19
The pedagogical model
While seven studies described exclusively synchronous activities, 14 , 17 , 20 , 21 , 22 , 23 , 28 four articles reported asynchronous learning. 16 , 18 , 24 , 26 Both modalities were presented in four studies. 13 , 15 , 19 , 27 One study did not describe the online modality of education. 25 Six studies stated that live online computer tutors were available to answer questions regarding the use of the technological tools. 13 , 15 , 16 , 23 , 25 , 27 The synchronous online classes ranged from 30 13 to 12028 min. Four studies developed online classes in small groups 21 , 22 , 23 , 28 between six 28 and 20 22 learners and rotation (polling) was applied in two of these experiences. 22 , 23
Flipped‐classroom and blended‐learning were also reported. 15 , 28 Individual activities were described in eight studies. 14 , 15 , 16 , 17 , 19 , 24 , 26 , 27
3.4.2. Minor axes
Knowledge gain
The quantity of knowledge gain was investigated in eight studies. Quizzes, 15 , 20 practical and theoretical tests, 15 , 16 electronic multiple‐choice questions and writing tests, 25 pre‐ and posttest, 18 , 22 and examinations based on the clinical cases given 23 , 26 were applied.
Two studies 22 , 23 described tests application via Zoom (https://zoom.us/). Moodle (moodle.org) and Google Meet (https://meet.google.com/) were also used in theoretical and practical tests. 15 A remote proctoring solution integrated with lockdown browser (http://www.emedley.com/eproctor/) was used in one study, 25 the application of multiple‐choice quiz questions during and following the presentation in Mentimeter AB website (www.mentimeter.com) was described in one manuscript, 20 and one article showed synchronous tests performed in Kahoot! (kahoot.com) website. 15
Regarding the synchronous tests using Kahoot!, the authors reported that more than 80% of the learners had a satisfactory or very satisfactory performance. 15 Another author described the percentage of online group total theoretical test scores was significantly higher when compared to the traditional group and there were no differences in the lab practical test scores between the two groups. 16 A study related that the 13 dental learners exposed to the technological tool correctly answered 90% of the questions evaluated, in relation to the 12 learners exposed to the virtual synchronous class group who correctly answered 40% of the same questions. 18 In addition, a manuscript reported that in a group of 19 learners, more than half correctly answered the questions at the virtual rotation end. 22 Another experience related that learners accordingly had interpreted some clinical case information and qualified their recommendations. 26 It was described in a study that participants correctly answered 61% of 13 questions queried during the presentation, and 83% of seven questions following the presentation correctly. 20
Dental learners’ satisfaction and attitudes toward remote learning
Twelve authors queried the learners’ satisfaction with the use of online technologies during the pandemic period. Nine of them 16 , 17 , 18 , 20 , 23 , 24 , 25 , 27 , 28 described respondents’ opinions as a positive, acceptable, and favorable experience.
Learners with 20 months of previous clinical experience felt that the virtual sessions promoted their critical thinking and solidification of concepts learned. However, learners with little time of clinical experience felt that they learned less during the virtual sessions than they did through traditional clinical education. 21
One article described 64% of the learners reported some level of discomfort before teledentistry had been used. Following the exercise, only 23% reported continued discomfort with the idea of leading a teledentistry visit. 19
The overall satisfaction with ERT was good. Most learners’ feedback suggested they would prefer a continuation of the model even after the current scheduling restrictions were lifted. 28 Nevertheless, a study has shown that only 27% suggested to continue the online classes even after the pandemic situation comes under control. The same research demonstrated that 77.51% of respondents rated online classes as noneffective. A majority of learners rated the understanding level of online classes as moderate and a total of 58.4% suggested that teachers need training on how to create and give online classes. 14
3.5. Risk of bias across studies
The selected studies were all descriptive and used similar methods, which reduced the possibility of misinterpretation. Results were considered homogeneous enough but did not have compatible quantitative data that would allow a meta‐analysis.
4. DISCUSSION
4.1. Summary of evidence
This is the first systematic review that assessed the ERT experiences during coronavirus social distancing. The 16 included studies justified the COVID‐19 transformation to partially or totally online courses to allow learners to continue learning, faculty to stay engaged in their activities, and the dental school community to remain connected and supportive of each other throughout a quarantine period. 21 ERT has threatened conventional training opportunities but introduced some others, accelerating the reliance and significance of technology for health education. 29 , 30 , 31 Reported problems included faculty members’ limited knowledge of technology, availability and strength of learners’ Internet connection, and transition of some topics to the online version.
E‐learning, known as a kind of distance learning that uses electronic devices to promote learning, has multiple possibilities that can undoubtedly improve education 32 , 33 and growing evidence shows that it is as effective as traditional methods. 34 , 35 However, the sudden shift from traditional teaching methods did not allow sufficient time for adaptation. These hurried moves by so many institutions at once could leave the perception of e‐learning as a weak option, when in truth the transition under these circumstances will not take full advantage of the affordances and possibilities of the online method. Hence, the term ERT is defined as a temporary shift of instructional delivery to an alternate mode due to crisis environments. 8
Authors have proposed the CIPP assessment of ERT, which is more focused on the (social) context, input (educational context), and process evaluations than on the product (learning). 8 , 36
The social context assesses needs, problems, and relevant contextual conditions. First, when isolated due to imposed quarantine and travel restrictions, learners may suffer anxiety at different levels. 37 , 38 Social distancing brings fear from uncertainty, physical discomfort, loneliness, and stress that negatively affect the teaching‐learning process. 39 , 40 Computer skill level, Internet access, and electronic devices availability were significant factors in facilitating the successful acceptance of e‐learning. 41 , 42 , 43 In this context, only two of the included articles, from middle 13 ‐ and low‐income countries, 14 reported the poor technology infrastructure of the dental learners. Therefore, the challenges of adopting online learning in developing countries remain a reality due to the digital delay when compared to the developed countries. 44 One review study, 45 which has put the technological aspects of e‐learning readiness 46 (the assessment of how ready an institution is to adopt and implement e‐learning) as the main criteria for the success of the online system, indicated that 45% of e‐learning projects in developing countries are total failures, 40% are partial failures, while only 15% are successful.
The input (educational context) assesses a strategy program, action plan, and staffing arrangements to meet targeted needs and achieve goals. The Zoom platform was the preferred platform in seven of the included studies. Zoom offers several possibilities, such as synchronous and asynchronous interactions, recording lectures, chats, screen sharing, sending and receiving files, division into small groups or individual activities, and lectures to large audiences. These results are in line with other findings in the literature. In an opinion article, a maxillofacial training during the pandemic highlighted the Zoom platform, stressing the importance of audio and visual connection enabling interpersonal contact that reinforces engagement and deeper learning. 47 A systematic review demonstrated that the presence of each type of interaction, which includes learner–content, learner–learner, and learner–teacher, when meaningfully integrated, increases the learning outcomes. 48 Perceived limitations of the virtual learning strategy were the loss of collegiality and networking. In addition to difficult interactions with trainers in an “artificial” encounter where communication may be personally challenging, technical glitches and the inability to cover all disciplines are all points that need to be taken into account in planning the future dental educational experiences. 30 According to the virtualization feasibility of the dental disciplines, one included study showed that only 26% of the dental courses could be totally virtualized with no content changes, while 32% were unfeasible. 13
The process evaluations monitor, assess, and report on the implementation of plans. A previous study indicated that less than half of the participants expressed positive perceptions of e‐learning, 49 while other studies reported health learners found it gratifying. 33 , 50 According to this systematic review, most of the included articles described respondents’ experience as favorable toward ERT and the use of the Zoom platform. The main advantage was the availability of dental learners to learn at all times, 24 , 25 along with other health sciences learners. 51 Some included studies noted participants prefer a continuation of the model even after the end of current restrictions. 21 , 23 , 28 Reported problems include too short a scheduled time to cover all planned activities, 22 technical issues related to pop‐up blockers and unstable Internet connectivity. 23 , 27 Despite the difficulties, many universities recommend the incorporation of an online method in the curricula. 15 , 23
Product (learning) evaluation consists of identifying and assessing outcomes. Undoubtedly, the evaluation had the highest fluctuation in this systematic review. Contrary to what might be supposed, online classes require greater learner responsibility and leadership than passively receiving the content in face‐to‐face classes. 52 Some strategies to replace the traditional tests were developed, such as the learners' participation in online forums, 28 self‐assessment of videos recorded from previous online activities, 19 and discussion of questionnaires in real time. 20 Pre‐ and postevaluations may be considered to assess learning outcomes in online education. 20
4.2. Conclusion
The CIPP assessment of ERT concluded that, in the social context, countries with better infrastructure improved the learning process as the technology access was greater, although the learners’ levels of anxiety and fear everywhere were similar. The input (educational context) showed that ease of communication and different types of interactions between learners, teachers, and the content are the most important requirements when choosing an online learning platform. The process evaluation revealed that the respondents approved ERT and recommended e‐learning after the end of the quarantine. The product (learning) evaluation showed high fluctuation since different strategies were adopted to assess learners’ knowledge gain.
In summary, campuses have been closed due to natural disasters and other unexpected events in recent years. The data showed that most learners appreciated the technology‐based system, however, they have missed some practical activities. Exploring learners’ satisfaction toward e‐learning and seeking feedback can help institutions to improve e‐learning experience. It is hoped that this sudden shift will not be considered a detriment to education, but a learning experience to open a wide way to technology‐based education. 51
4.3. Limitations
Overall, the number of studies published on the use of e‐learning in dental education during the COVID‐19 pandemic is limited and thus contributed to the small number of studies included in this systematic review. Regarding the quality appraisal of the included studies, some methodological quality issues were found related to the learners’ demographic and social context, learning technology/ learning method, and description of unwanted events. Also, despite the varied study population groups considered for inclusion in this review, no dental assistant/ hygienist students were evaluated. This warrants the need for more studies in this area as well as diverse study populations. It is also important to consider that the learners’ perception of ERT modalities was not thoroughly assessed, although this is of great value when proposing a new educational reality.
5. CONCLUSION
The experiences showed that the ERT is a good option to ensure multimodal and active education during the COVID‐19 period since e‐learning is well‐received by dental learners. Some benefits are to decrease anxiety and to promote mutual support while in mandated quarantine. The identified problems include poor technological infrastructure in both learners’ and institutions’ environment and difficulty in replacing clinical activities.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
Supporting information
Supporting information
Supporting information
Santos GNM, da Silva HEC, Leite AF, et al. The scope of dental education during COVID‐19 pandemic: A systematic review. J Dent Educ. 2021;85:1287–1300. 10.1002/jdd.12587
REFERENCES
- 1. Dong E, Du H, Gardner L. COVID‐19 dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Lancet Inf Dis. 2020;19:533‐534. [Google Scholar]
- 2.COVID‐19 educational disruption and response. UNESCO. 2020 Available at: https://en.unesco.org/covid19/educationresponse. Accessed October 15 2020.
- 3. Iyer P, Aziz K, Ojcius DM. Impact of COVID‐19 on dental education in the United States. J Dent Educ. 2020;84(6):718‐722. [DOI] [PubMed] [Google Scholar]
- 4. Joye C, Moreira M, Rocha S. Distance education or emergency remote educational activity: in search of the missing link of school education in times of COVID‐19. Res Soc Dev. 2020;9(7):e521974299. [Google Scholar]
- 5. Krasna M, Bratina T. E‐learning materials for social science students. Probl Educ 21st Cent. 2014;61:77‐87. [Google Scholar]
- 6. Towers A, Field J, Stokes C, Maddok S, Martin N. A scoping review of the use and application of virtual reality in pre‐clinical dental education. Br Dent J. 2019;226(5):358‐366. [DOI] [PubMed] [Google Scholar]
- 7. Al‐Mussawi RMA, Farid F. Computer‐based technologies in dentistry: types and applications. J Dent. 2016;13(3):215‐222. [PMC free article] [PubMed] [Google Scholar]
- 8. Hodges CB, Moore S, Lockee BB, Trust T, Bond MA. The difference between emergency remote teaching and online learning. Educause Rev. 2020:1‐14. [Google Scholar]
- 9. Reich J, Buttimer C, Fang A, Hillaire G, Hirsch K, Larke L, et al. Remote learning guidance from state education agencies during the COVID‐19 pandemic: a first look. 2020.
- 10. Moher D, Liberati A, Tetzlaff J, Altman D, Group P. Preferred reporting items for systematic reviews and meta‐analyses: the PRISMA statement. Open Med. 2009;3:e123‐30. [PMC free article] [PubMed] [Google Scholar]
- 11. University of York: Centre for Reviews and Dissemination. 2020. crd.york.ac.uk. Accessed October 8, 2020.
- 12. Moola S, Munn Z, Tufanaru C. Systematic reviews of etiology and risk. In: Aromataris E, Munn Z, eds. Joanna Briggs Institute Rewiewer's Manual for Evidence Synthesis. Adelaide, Australia: The Joanna Briggs Institute; 2017:1‐5. [Google Scholar]
- 13. Chavarría‐Bolaños D, Gómez‐Fernández A, Dittel‐Jiménez C, Montero‐Aguilar M. E‐learning in dental schools in the times of COVID‐19: a review and analysis of an educational resource in times of the COVID‐19 pandemic. Odovtos‐International J Dent Sci. 2020;22:69‐86. [Google Scholar]
- 14. Tuladhar SL, Pradhan D, Parajuli U, Manandhar P, Subedi N. Study on the effectiveness of online classes for undergraduate medical and dental students of Gandaki Medical College during COVID 19 pandemic period in Nepal. Orthod J Nepal. 2020;10(2):36‐40. [Google Scholar]
- 15. Spalding M, Rauen C, de Vasconcellos LMR, da Cruz Vegian MR, Miranda KC, Bressane A. Desafios e possibilidades para o ensino superior: uma experiência brasileira em tempos de COVID‐19. Res Soc Dev. 2020;9(8):e534985970. [Google Scholar]
- 16. Zhong Y, Sun W, Zhang W, Liu L, Xu Y, Jiang Y. Application of remote online learning in oral histopathology teaching: an acute response to the COVID‐19 pandemic. Res Sq. 2020. 10.21203/rs.3.rs-51823/v1 [DOI] [Google Scholar]
- 17. Galibourg A, Delrieu J, Monsarrat P, Joniot S, Maret D, Nasr K. E‐dental practicum: a way to maintain student hands‐on training during disruptive crises. J Dent Educ. 2021;85(Suppl. 1):1148‐1151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Aguilar‐Gálvez D, Noal FC, de Araujo FB, Arriola‐Guillén LE. Virtual learning object: an asynchronous solution for virtual learning in dentistry post COVID‐19. J Dent Educ. 2021;85(Suppl. 1):1123‐1125. [DOI] [PubMed] [Google Scholar]
- 19. Patel SA, Halpin RM, Olson GW, Franklin A. Global pandemic and the rise of teledentistry. J Dent Educ. 2021;85(Suppl. 1):1158‐1159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Patterson K, Ritwik P, Kerins C, Adewumi A. Real‐time measurement for effectiveness of novel educational endeavors during the COVID‐19 pandemic. J Dent Educ. 2021;85(Suppl. 1):1020‐1021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Gardner AL, Halpin R, Saeed SG. Virtual dental clinic. J Dent Educ. 2021;85(Suppl. 1):883‐884. [DOI] [PubMed] [Google Scholar]
- 22. Gyurko R, Neste C, Dragan IF. Transitioning clinical rotations to a virtual experience: problem, solution, and results. J Dent Educ. 2021;85(Suppl. 1):896‐898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Kakadia R, Chen E, Ohyama H. Implementing an online OSCE during the COVID‐19 pandemic. J Dent Educ. 2021;85(Suppl. 1):1006‐1008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Mladenovic R, Bukumiric Z, Mladenovic K. Influence of a dedicated mobile application on studying traumatic dental injuries during student isolation. J Dent Educ. 2021;85(Suppl. 1):1131‐1133. [DOI] [PubMed] [Google Scholar]
- 25. Moore Z, Stallard J, Tittemore A, Lee JY. The COVID‐19 pandemic: opportunity for integration of educational technology. J Dent Educ. 2021;85(Suppl. 1):1160‐1162. [DOI] [PubMed] [Google Scholar]
- 26. Nair R, Marchini L, Johnsen D, Xie X. Implementation of an online treatment planning exercise focused on vulnerable patient groups. J Dent Educ. 2021;85(Suppl. 1):941‐943. [DOI] [PubMed] [Google Scholar]
- 27. Omar H, Archer L, Schroeder K, Robinson B. Web‐based standardized patient encounters for preclinical dental students during COVID‐19 pandemic. J Dent Educ. 2021;85(Suppl. 1):1167‐1169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Pani S, Vieira L. Integrating online learning management systems to dental simulation clinics—an example of blended learning in pediatric dentistry. J Dent Educ. 2021;85(Suppl. 1):1163‐1166. [DOI] [PubMed] [Google Scholar]
- 29. Basilaia G, Kvavadze D. Transition to online education in schools during a SARS‐ CoV‐2 coronavirus (COVID‐19) pandemic in Georgia. Pedagog Res. 2020;5(4):1‐9. [Google Scholar]
- 30. Elledge R, Williams R, Fowell C, Green J. Maxillofacial education in the time of COVID‐19: the West Midlands experience. Br J Oral Maxillofac Surg. 2020. 10.1016/j.bjoms.2020.07.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Fang C, Wang G, Huang B. Can information technology promote the development of students’ cognitive abilities? An estimate based on the net effect of educational value added instruments. Open Edu Res. 2019;25(4):100‐110. [Google Scholar]
- 32. Sadeghi R, Sedaghat MM, Sha Ahmadi F. Comparison of the effect of lecture and blended teaching methods on students’ learning and satisfaction. J Adv Med Educ Prof. 2014;2(4):146‐150. [PMC free article] [PubMed] [Google Scholar]
- 33. Huynh R. The role of E‐learning in medical education. Acad Med. 2017;92(4):430. [DOI] [PubMed] [Google Scholar]
- 34. Hattar S, AlHadidi A, Sawair FA, Abd Alraheam I, El‐Ma'aita A, Wahab FK. Impact of COVID‐19 pandemic on dental academia. Students’ experience in online education and expectations for a predictable practice. Res Sq. 2020. 10.21203/rs.3.rs-54480/v1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Santos GNM, Leite AF, De Figueiredo PTS, et al. Effectiveness of E‐learning in oral radiology education: a systematic review. J Dent Educ. 2016;80(9):1126‐1139. [PubMed] [Google Scholar]
- 36. Stufflebeam DL, Zhang G. The CIPP Evaluation Model: How to Evaluate for Improvement and Accountability. New York: Guilford Publications; 2017. [Google Scholar]
- 37. Sahu P. Closure of universities due to coronavirus disease 2019 (COVID‐19): impact on education and mental health of students and academic staff. Cureus. 2020;12(4):e7541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Gillett‐Swan J. The challenges of online learning: supporting and engaging the isolated learner. J Learn Des. 2017;10(1):20‐30. [Google Scholar]
- 39. Karen JBT, Cathy MDT. Philippine teachers’ practices to deal with anxiety amid COVID‐19. J Loss Trauma. 2020;25(6‐7):573‐579. [Google Scholar]
- 40. Xiang TT, Yang Y, Li W, et al. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry. 2020;7(3):228‐229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Asiry MA. Learning styles of dental students. Saudi J Dent Res. 2016;7:13‐17. [Google Scholar]
- 42. Alhabeeb A, Rowley J. Critical success factors for eLearning in Saudi Arabian universities. Int J Educ Manag. 2017;31(2):131‐147. [Google Scholar]
- 43. Lorenzo G. A research review about online learning: are students satisfied? Why do some succeed and others fail? What contributes to higher retention rates and positive learning outcomes. Internet Learn. 2015;1(5):45‐55. [Google Scholar]
- 44. Eltahir ME. E‐learning in developing countries: is it a panacea? A case study of Sudan. IEEE Access. 2019;7:97784‐97792. [Google Scholar]
- 45. Al‐Araibi AAM, Naz'ri Bin Mahrin M, Yusoff RCM. Technological aspect factors of E‐ learning readiness in higher education institutions: Delphi technique. Educ Inf Technol. 2019;24(1):567‐590. [Google Scholar]
- 46. Bowles M. What is electronic learning? Relearning to e‐Learn: Strategies for Electronic Learning and Knowledge. Carlton: Melbourne University Press; 2004:3‐19. [Google Scholar]
- 47. Carlson ER. COVID‐19 and educational engagement. J Oral Maxillofac Surg. 2020;78:1049‐1051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Bernard RM, Abrami PC, Borokhovski CE, et al. A meta‐analysis of three types of interaction treatments in distance education. Rev Educ Res. 2009;79(3):243‐289. [Google Scholar]
- 49. Schulz P, Sagheb K, Affeldt H, et al. Acceptance of e‐learning devices by dental students. Med 20. 2013;2(2):e6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Ruiz JG, Mintzer MJ, Leipzig RM. The impact of e‐learning in medical education. Acad Med. 2006;81(3):207‐212. [DOI] [PubMed] [Google Scholar]
- 51. Puljak L, Civljak M, Haramina A, et al. Attitudes and concerns of health sciences students in Croatia regarding complete switch to e‐learning during COVID‐19 pandemic: a survey. BMC Med Educ. 2020;20(1):416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Regmi K, Jones L. A systematic review of the factors—enablers and barriers–affecting e‐learning in health sciences education. BMC Med Educ. 2020;20(1):91. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting information
Supporting information