

INTRODUCTION
The brunt of mortality related to coronavirus disease 2019 (COVID‐19) has been borne by older adults. In the United States, over 80% of all COVID‐19 deaths have been among people over the age of 65 years. 1 Likewise, Centers for Disease Control data show a dramatic age‐associated rise in case fatality rates among individuals admitted for COVID‐19, from 2.1% for those aged 18–49 to 20% for those aged 65 and older. 2 Over time, however, there has been a trend toward lower case fatality rates among individuals hospitalized for COVID‐19. 3 Whether this has held among older patients has implications for the effectiveness of changes in care among those at the highest risk for adverse outcomes from COVID‐19. We present temporal trends in COVID‐19 mortality for individuals hospitalized in the Veterans Affairs (VA) Health Care System.
METHODS
Data were obtained from the VA Corporate Data Warehouse. Hospitalizations for COVID‐19 were defined as new hospitalization in a VA hospital within 30 days after a positive COVID‐19 Polymerase Chain Reaction test or a positive COVID‐19 PCR during an ongoing hospitalization. All veterans admitted to any VA hospital across the United States from March 1 to November 30, 2020, and who were aged 65 and older at time of their positive COVID‐19 test were eligible for inclusion in this study.
Trends in 30‐day mortality by month of admission and by age category (65–74, 75–84, and 85+) were examined using the Cochran–Armitage test for trend. The impact of time on mortality was assessed using logistic regression with adjustment for age, sex, race, region, Charlson Comorbidity Index, and Systemic Inflammatory Response Syndrome criteria. Analysis was conducted in SAS, version 9.4.6. IRB approval was obtained from the Boston VA Health Care System. This work was funded by the VA, which did not have a role in study design, analysis, or reporting of results.
RESULTS
The final sample included 11,162 veterans, mean age was 76 (SD 7.8) years, and 98% were male (see Table S1 and Figure S1). Over 9 months, the average 30‐day mortality rate was 19.2%, starting at 32% in March and declining to 16.8% in November. Figure 1 shows trends in 30‐day mortality by month of admission for veterans admitted for COVID‐19 according to age category. The overall trend demonstrated a significant decline in the 30‐day mortality proportion (p < 0.001, Table S2), which remained significant for all age groups. The greatest proportion of this decline occurred between March and May. Adjusted odds ratios (95% CIs) for mortality by month of admission are 0.91 (0.89–0.93) overall and 0.907 (0.881–0.935) for those aged 65–74, 0.95 (0.92–0.98) for those aged 75–84, and 0.871 (0.84–0.91) for those 85+ years.
FIGURE 1.
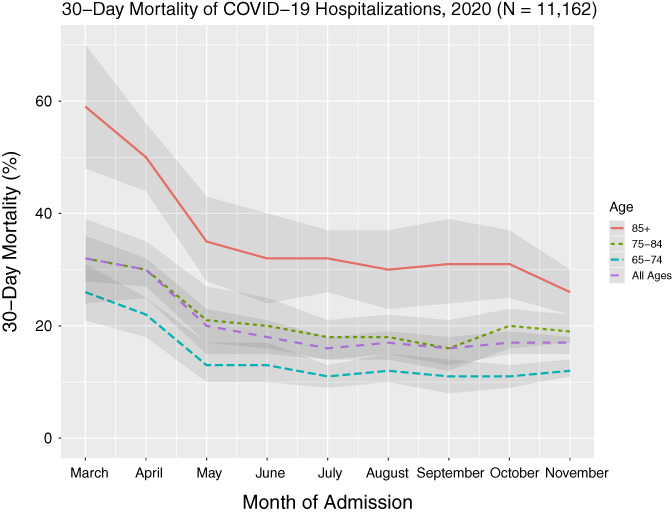
Time trend of 30‐day mortality proportion by month of admission among veterans admitted to the VAHCS with COVID‐19, March 1–November 30, 2020, according to age category. Shaded areas are 95% confidence intervals
DISCUSSION
As with the general population, in a cohort of older adults, even the oldest olds (aged 85 and older) hospitalized with COVID‐19 in the VA system have realized a significant and linear decline in 30‐day mortality. The disparity in mortality outcome among age groups also seems to have decreased, although it remains. Compared with data representing all ages from three health systems in New York, mortality rates in this national older population are approximately 1.5‐ to 2‐fold greater, although the comparator study considered in‐hospital rather than 30‐day mortality. 3 These are also similar to age‐adjusted 28‐day mortality trends in England. 4 Improvements in mortality over the first 10 months of the pandemic may reflect improved care for all hospitalized patients, for which even the oldest olds have benefitted as well. Given that older individuals do not always see the same benefit, and may even experience harm, from interventions in younger people, these data are reassuring. Which interventions may be driving these trends is unknown, as the largest declines occurred before the preliminary results of the Randomised Evaluation of COVID‐19 Therapy trial and the approval of remdesivir.5, 6, 7 The then‐growing availability of data from China and Europe, which had earlier experience with COVID‐19, likely helped guide care, such as avoiding early intubation and prone positioning. 8 It is possible that improved masking and adherence to physical distancing lowered inoculum and subsequent disease intensity. Residual confounding remains a possible explanation, even with adjustment for comorbidity in particular. Despite declines in 30‐day mortality reported, individuals aged 85 and older remain at the highest risk of mortality from COVID‐19. Focused attention to improving outcomes by specifically studying interventions for this age group remains an imperative.
FUNDING DISCLOSURES
ARO is supported by VA CSRD CDA2 IK2CX001800‐01A1.
CONFLICT OF INTEREST
The authors have no conflicts of interest to report.
AUTHOR CONTRIBUTIONS
Benjamin Seligman and Ariela R. Orkaby designed the study with input from David R. Gagnon. Brian Charest developed the cohort, and Brian Charest and Benjamin Seligman conducted the analysis. Benjamin Seligman drafted the manuscript. All authors reviewed and revised the manuscript.
FUNDING INFORMATION
VA, Grant/Award Number: CSRD CDA2 IK2CX001800‐01A1.
SPONSOR'S ROLE
The sponsor had no role in the design, analysis, and reporting of results of this study.
Supporting information
Data S1 Cohort characteristics and details from results: contains information on cohort construction and characteristics as well as detailed results from statistical test for trend.
Figure S1 Diagram outlining creation of analytic cohort of older adults admitted for COVID‐19 in the Veterans Affairs Health Care System.
Table S1. Baseline characteristics of 11,162 veterans aged ≥65 years admitted with COVID‐19 to the Veterans Affairs Health Care System, March 1–November 30, 2020.
Table S2. Cochran–Armitage test of trend results for change in 30‐day mortality among veterans admitted to the VAHCS with COVID‐19, March 1–November 30, 2020, by age category.
ACKNOWLEDGMENTS
Seligman B, Charest B, Gagnon DR, Orkaby AR. Trends in 30‐day mortality from COVID‐19 among older adults in the Veterans Affairs system. J Am Geriatr Soc. 2021;69:1448–1450. 10.1111/jgs.17127
Funding information VA, Grant/Award Number: CSRD CDA2 IK2CX001800‐01A1
REFERENCES
- 1. Centers for Disease Control and Prevention . CDC COVID data tracker. https://covid.cdc.gov/covid-data-tracker/#demographics. Accessed January 22, 2021.
- 2. Centers for Disease Control and Prevention . COVID‐NET: COVID‐19 associated hospitalization surveillance network. https://gis.cdc.gov/grasp/COVIDNet/COVID19_5.html. Accessed January 14, 2021.
- 3. Horwitz LI, Jones SA, Cerfolio RJ, et al. Trends in COVID‐19 risk‐adjusted mortality rates. J Hosp Med. 2021;16(2):90‐92. 10.12788/jhm.3552. [DOI] [PubMed] [Google Scholar]
- 4. Jones S, Mason N, Palser T, Swift S, Petrilli CM, Horwitz LI. Trends in risk‐adjusted 28‐day mortality rates for patients hospitalized with COVID‐19 in England. J Hosp Med. 2021;16(Issue 2021‐Feb ONLINE 1st):E1‐E4. 10.12788/jhm.3599. [DOI] [PubMed] [Google Scholar]
- 5. Horby P, Lim WS, Emberson J, et al. Effect of dexamethasone in hospitalized patients with COVID‐19 – Preliminary report. medRxiv. 2020. 10.1101/2020.06.22.20137273. [DOI] [Google Scholar]
- 6. Food and Drug Administration. Coronavirus (COVID‐19) Update : FDA issues emergency use authorization for potential COVID‐19 treatment|FDA. 2020; https://www.fda.gov/news‐events/press‐announcements/coronavirus‐covid‐19‐update‐fda‐issues‐emergency‐use‐authorization‐potential‐covid‐19‐treatment. Accessed January 14, 2021.
- 7. The RECOVERY Collaborative Group . Dexamethasone in hospitalized patients with Covid‐19. N Engl J Med. 2021;384(8):693‐704. 10.1056/NEJMoa2021436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID‐19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054‐1062. 10.1016/S0140-6736(20)30566-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1 Cohort characteristics and details from results: contains information on cohort construction and characteristics as well as detailed results from statistical test for trend.
Figure S1 Diagram outlining creation of analytic cohort of older adults admitted for COVID‐19 in the Veterans Affairs Health Care System.
Table S1. Baseline characteristics of 11,162 veterans aged ≥65 years admitted with COVID‐19 to the Veterans Affairs Health Care System, March 1–November 30, 2020.
Table S2. Cochran–Armitage test of trend results for change in 30‐day mortality among veterans admitted to the VAHCS with COVID‐19, March 1–November 30, 2020, by age category.