

Abstract
Allogeneic hematopoietic stem cell transplantation (HSCT) remains a potentially curative and useful strategy in high-risk relapsing chronic lymphocytic leukemia (CLL). Minimal residual disease (MRD) assessment at 12 months (M12) post-HSCT is predictive of relapse. This phase II study aimed to achieve M12 MRD negativity (MRDneg) using an MRD-driven immune-intervention (Md-PII) algorithm based on serial flow-cytometry blood MRD, involving cyclosporine tapering followed in case of failure by donor lymphocytes infusions. Patients had high-risk CLL according to the 2006 European Society for Blood and Marrow Transplantation consensus, in complete or partial response with lymphadenopathy <5 cm and comorbidity score ≤2. Donors were HLA-matched sibling or matched unrelated (10/10). Fortytwo enrolled patients with either 17p deletion (front-line, n=11; relapse n=16) or other high-risk relapse (n=15) received reduced intensity-conditioning regimen before HSCT and were submitted to Md-PII. M12- MRDneg status was achieved in 27 of 42 patients (64%) versus 6 of 42 (14.2%) before HSCT. With a median follow-up of 36 months (range, 19-53), 3-year overall survival, non-relapse mortality and cumulative incidence of relapse are 86.9% (95% Confidence Interval [CI]: 70.8-94.4), 9.5% (95% CI: 3.7-23.4) and 29.6% (95% CI: 17.3-47.7). Incidence of 2-year limited and extensive chronic graft versus host disease (cGVHD) is 38% (95% CI: 23-53) and 23% (95% CI: 10-36) including two cases post Md-PII. Fifteen patients converted to MRDneg either after cyclosporine A withdrawal (n=12) or after cGvHD (n=3). As a time-dependent variable, MRDneg achievement at any time-point correlates with reduced relapse (Hazard ratio [HR] 0.14 [range, 0.04-0.53], P=0.004) and improvement of both progression free (HR 0.18 [range, 0.06-0.6], P<0.005) and overall (HR 0.18 [range, 0.03-0.98], P=0.047) survival. These data highlight the value of MRD-driven immune-intervention to induce prompt MRD clearance in the therapy of CLL (clinicaltrials gov. Identifier: NCT01849939).
Introduction
Until recently, patients with refractory chronic lymphocytic leukemia (CLL) or who relapse early after purine analogs and rituximab-based chemoimmunotherapy or those harboring 17p deletion (del(17p)) and/or TP53 mutations were considered high-risk patients with reduced overall survival (OS). Better understanding of the molecular and genetic aspects of CLL brought novel and highly active strategies such as targeting kinases downstream of the Bcell receptor (BCR) pathway.1-3 These therapies have profondly modified the CLL therapeutic landscape, thanks to improved efficacy and better tolerability. However, the disease is still incurable and allogeneic hematopoietic stem cell transplantation (HSCT) remains a valid option in selected high-risk patients.4,5
Prospective studies have shown that allogeneic HSCT can offer long progression free survival (PFS) and even a cure in 35% to 45% of high-risk patients. Reduced intensity conditioning (RIC) HSCT can be proposed to older patients and patients with comorbidities who represent the bulk of the CLL population. However disease recurrence, recorded in 22% to 46% patients, is still a major issue.6-9 Pre-transplantation refractoriness and bulky disease is associated with higher risk of post-transplantation progression.9,10 The level of post-transplantation minimal residual disease (MRD) is widely associated with the risk of further progression. In several studies, a negative MRD (MRDneg) status at 6 to 12 months translated into a progression incidence below 10%.11-14 Moreover, the MRDneg status may be reached by post-transplantation immunomodulation such as cyclosporine A (CsA) tapering or donor lymphocyte infusion (DLI).15 These data led us to conduct a prospective study evaluating an approach of RIC HSCT followed by a preemptive MRD-driven immune-intervention with the aim to achieve a MRDneg status at 12 months post-transplantation.
Methods
Study design
The ICLL03 RICAC-PMM (Reduced Intensity Conditioning Allogeneic Transplantation for CLL with Preemptive MDR Management), a joint FILO (French Innovative Leukemia Organization) and SFGM-TC (Société Francophone de Greffe de Moelle et de Thérapie Cellulaire) multicenter phase II trial evaluated the efficacy and safety of a preemptive immune-intervention based on MRD assessment in high-risk CLL. Eligible patients were 18 to 70 years old, with CLL (Matutes score 4 or 5) or lymphocytic lymphoma, and high-risk features according to the 2006 European Society for Blood and Marrow Transplantation (EBMT) consensus16 (see Online Supplementary Appendix). Patients had to be in complete or partial response with lymphadenopathy <5 cm and a comorbidity score ≤2. Donors were HLA-matched sibling or unrelated (10/10).17 All responsible Institutional Review Boards in accordance with the Declaration of Helsinki approved the protocol including the study-specific informed consent form. The study was declared to the French Authorities (reference ID-RCB 2011- A00906-35) and registered on clinicaltrials gov. Identifier: NCT01849939.
Transplantation modalities
Conditioning regimen was fludarabine, 30 mg/m2/day, from day (D) D-5 to D-1, intravenous busulfan 3.2 mg/kg/day from D- 4 to D-3 and ATG (thymoglobuline) 2.5 mg/kg/day from D-3 to D-2.18 Stem cell source was G-CSF mobilized peripheral blood cells. Graft-versus-host disease (GvHD) prophylaxis was based on CsA with a short course of methotrexate in case of minor donor/recipient ABO mismatch.
Response and minimal residual disease evaluation
Response evaluation was performed according to 2008 iwCLL criteria including computed tomography scan (CT-scan)19 before and 3 months (M3), 6 months (M6) and 12 months (M12) after transplantation.
MRD analysis was centrally performed on blood and/or bone marrow by 10-color multiparameter flow cytometry.20-22 MRDneg definition was <1 CLL cell detectable per 10,000 leukocytes (<1.10-4).19 MRD (MRDpos) definition was ≥1 CLL cell detectable per 10,000 leukocytes. Clusters of <20 events were considered as undetectable MRD (UD). Blood MRD evaluation was planned before transplantation, then monthly until M6, at M9 and M12. Once achieved, the blood MRDneg status was confirmed 1 month later in both blood and bone marrow.
Preemptive immune-intervention
Preemptive immune-intervention was applied in the absence of significant GvHD, defined by either acute GvHD (aGVHD) ≥grade 2 or extensive chronic GvHD (cGvHD). The algorithm based on response and blood MRD assessment included acceleration of CsA tapering and withdrawal followed in case of failure by escalating DLI. The algorithm also included extension of CsA treatment in case of early achievement of MRD status (Online Supplementary Appendix; Figure A)
Chimerism and graft-versus-host disease assessment
Chimerism studies were performed on peripheral blood at M1, M2, M3, M6, and M12 post HSCT by multiplex fluorescent polymerase chain reaction using Short Tandem Repeat analysis. (Online Supplementary Appendix). The diagnosis of GvHD was made according to published criteria.23,24
Trial objectives and statistical analysis
The primary objective was to evaluate the efficacy of a preemptive immune-intervention to achieved MRDneg at M12. The probabilities of OS, and PFS were calculated using the Kaplan- Meier estimator. The probability of non-relapse mortality (NRM) and relapse/progression were calculated using the Fine and Gray approach, considering death as competing risks. In order to evaluate the impact on outcomes of MRDneg achievement, we performed time dependent analyses considering MRDneg occurrence as a time-dependent event. Outcome data were estimated by the Mantel-Byar method and graphically illustrated by Simon-Makuch plots25,26 (Online Supplementary Appendix).
Results
Patients’ characteristics, donor type and protocol adherence
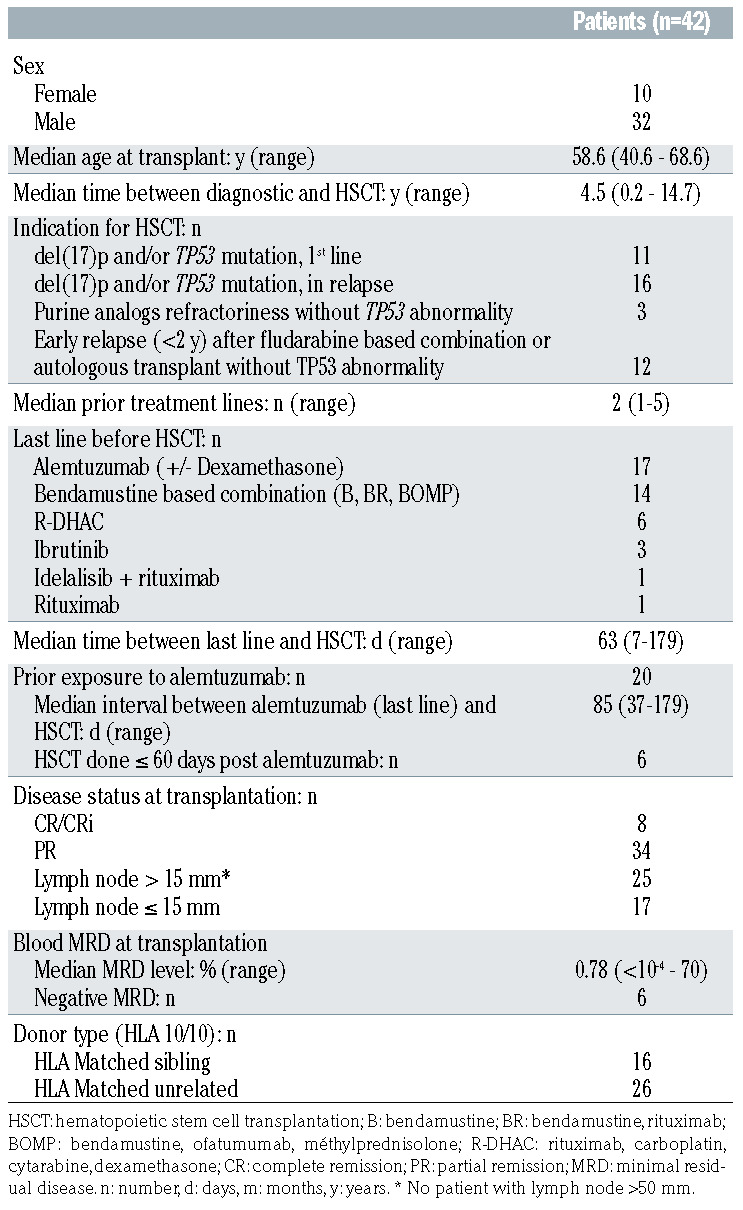
Between September 2012 and February 2015, 43 patients fulfilling the 2006 EBMT consensus criteria were recruited in 16 French centers; due to donor comorbidities, one patient included was not eventually transplanted. The present analysis includes the remaining 42 patients (32 male and 10 female). Patients’ characteristics are depicted in the Table 1. Before HSCT, patients had received a median of two lines of treatment (range, 1-5); the last one being alemtuzumab for 17 patients, immunochemotherapy for 21 and BCR inhibitors for four. Details of previous lines of treatment per patients are reported in the Online Supplementary Table S1. Eight patients were in CR/CRi (including six with blood MRDneg status) and 34 in PR pre-transplantation. Donors were HLA-identical siblings (n=16) or HLAmatched (10/10) unrelated donors (n=26).
The trial profile of the immune-intervention applied in this study and the representative protocol adherence is shown in the Online Supplementary Appendix (Online Supplementary Figure 1B). One patient died before D30. Among the 41 remaining patients, seven were not treated strictly according to study protocol: four patients had an unplanned early CsA withdrawal for primary (n=1) or secondary (n=1) graft failure or mixed chimerism (n=2). One of these last two patients relapsed at 13 months, whereas the second, who later received DLI, was still in mixed chimerism without relapse at 18 months. For two patients, CsA was tapered early, despite MRDneg status, due to renal failure in one patient. Finally CsA was reduced at D120 instead of D90 for one patient with D90 MRDpos status.
Table 1.
Patients’ characteristics
Post-transplantation response and outcomes
Engraftment occurred in 40 of the 42 transplanted patients while two presented graft failure. In the latter patients, both in PR at transplantation, the last line were alemtuzumab plus dexamatasone, interrupted 49 days before transplant in one patient and ibrutinib interrupted 9 days before transplant in the other. Assessment of the response according to the iwCLL criteria between 3 and 6 months found CR/CRi and PR for 13 (31%) and 26 (62%) patients, respectively. Response was not evaluated for three patients because of early death (n=1) or graft rejection (n=2). Response was classified as partial when there was lymph node >15 mm persistence (n=6), spleen enlargement (n=4), both (n=3) or incomplete evaluation (n=13) (Online Supplementary Table S2).
Seventeen patients developed grade 1 (n=8), 2 (n=6) and 3 (n=3) aGvHD. Limited and extensive cGvHD occurred in 15 and nine of the 39 patients who engrafted and were still alive at D100, translating into a cumulative incidence at 2 years of cGvHD of 61% (95% Confidence Interval [CI]: 54-68), including limited and extensive cGvHD in 38% (95% CI: 23-53) and in 23% (95% CI: 10%-36%) patients respectively. Two cases of primary cGvHD were diagnosed following planned immune-intervention: one was a limited cGVHD after DLI administration for early progression at D35 and one was an extensive cGvHD after cessation of CsA due to D90 MRD positivity.
Seven of the 42 patients died. Causes of death were extensive cGvHD (n=2), pulmonary aspergillosis plus Pneumocystis jiroveci pneumonia associated with limited cGvHD (n=1) and early cytomegalovirus infection (n=1) in a patient who received alemtuzumab in the last weeks prior to transplantation. The three remaining deaths were related to disease progression with Richter transformation. Moreover three patients presented severe complications, namely two polyradiculopathy and one Epstein–Barr virusinduced lymphoproliferative disease.
With a median follow-up of survivors of 36 months (range, 19-53) the 3-year OS, PFS, and NRM were 86.9% (95% CI: 70.8-94.4), 62.9% (95% CI: 45.8-75.9) and 9.5% (95% CI: 3.7-23.4) respectively. Ten patients had progression occurring after a median of 12 months (range, 1-34). The 3-year cumulative incidence of relapse was 29.6% (95% CI: 17.3-47.7) (Figure 1). Salvage therapy was delivered in patients who relapsed after donor engraftment; eight patients received ibrutinib; six of them are still in remission at the last follow-up (32 to 52 months) while two had a transient response followed by progression with Richter transformation. (Table 2).
Minimal residual disease (MRD) status at 12 months and MRD kinetics after hematopoietic stem cell transplantation
At M12, 27 patients achieved MRDneg status, including 23 patients with an undetectable MRD (MRD < limit of detection), seven patients remained MRDpos, eight patients were not evaluable because either early toxic death (n=4) or other reason including graft rejection (n=2), Eppstein- Barr virus-induced lymproliferation (n=1) and early relapse (n=1). Thus, at M12, MRDneg status was achieved in 64% (27 of 42) if we consider all patients and in 77% (27of 35) if we take into consideration all 34 patients assessed at this time point and the patient who experienced a clinical relapse at 1 month (and thus not subject to systematic MRD assessment but considered as failure) versus 14.2% before transplantation. Most patients remained MRDpos early after transplantation and progressively translated to MRDneg within the first 6 months posttransplantation. (Figure 2). Nine of the 13 (69%) D90 MRDpos patients who had no significant GvHD but who had an early CsA withdrawal according to the protocol, managed to reach a MRDneg status.
For the 39 patients who engrafted and were alive after M1, MRD kinetics followed four distinctive patterns. (Figure 3). The pattern A (n=6) is constituted of the pretransplantation MRDneg patients. Two of these patients relapsed, one at 12 and one at 19 months. The pattern B (n=11) comprised the patients who converted from pretransplantation MRDpos to post-transplantation MRDneg status within 3 months without any immune-intervention. One pattern-B patient with M12 MRD close to the positivity threshold relapsed at 13 months. The pattern C (n=15) is constituted of the patients with pre-transplantation MRDpos who remained MRDpos during the first 3 months but became MRDneg either after CsA tapering and withdrawal (n=12) or after cGvHD (n=3). Two pattern- C patients relapsed at 23 and 34 months. The pattern D (n=7) comprised the patients with a pre-transplantation MRDpos status who remained MRDpos despite cGvHD (n=1) or immune-intervention including CsA tapering and withdrawal (n=6) followed by DLI for five of them. Progression was observed in five pattern-D patients including three Richter transformations, each occurring within the first 13 months. The outcome of all four panels is represented in the Online Supplementary Table S3.
Figure 1.

Post-transplant outcome of the 42 chronic lymphocytic leukemia transplanted patients. Kaplan-Meier estimates of (A) overall survival, (B) progressionfree survival. Calculated probability of (C) non relapse mortality and (D) cumulative incidence of relapse after hematopoietic stem cell transplantation.
Impact of minimal residual disease on outcome
In Mantel-Byar analysis, evaluating MRD as a timedependent variable, achievement of the MRDneg status regardless of the time point, was predictive of an improved PFS, Hazard ratio (HR) 0.18 (range, 0.06-0.60), P=0.005, and OS, HR 0.18 (range, 0.03-0.98), P=0.047 along with a reduction of CIR, HR 0.14 (range, 0.04-0.539, P=0.004. (Figure 4).
Chimerism evaluation
The chimerism analyzed on unselected blood cells had no impact on outcome. Conversely T-cell donor engraftment (≥95% donor T cells) tended to be associated with higher PFS, HR 0.16 (range, 0.02-1.37), P=0.09, and lower relapse risk, HR 0.16 (range, 0.02-1.22) P=0.08 but had no impact on OS, P=0.18.
Discussion
Since the first descriptions, allogeneic HSCT has long been the only curative treatment for CLL. Its development has benefited greatly from the advent of reduced-intensity conditioning that can be proposed until the age of 70. The availability of new alternative therapies, including both BCR and BCL-2 inhibitors have in high-risk patients taken the place of allogeneic HSCT and delayed this strategy until later in the management of the disease. Consequently, the number of allogeneic HSCT for CLL has considerably decreased since 2015, both in the United States27 and Europe.28 BCR and BCL-2 inhibitors allow control of relapsed CLL with a response duration exceeding those reported after immunochemotherapy.29,30 However, relapses are the rule, particularly in patients with adverse molecular31,32 and/or complex karyotype.33,34 For such patients, CAR-T cells are also a hope.35,36 However, while this new option is very promising in several hematological diseases, in the 134 highly pre-treated CLL reported to date, the complete response rate remains 20 to 30%, with a median PFS of 18% at 18 months.37 This approach is associated with significant acute toxicity, but does not present, in contrast to allogeneic HSCT, a risk of GvHD. Hence, long-term results in large cohorts of CLL patients treated by CAR-T cells are currently needed, and allogeneic HSCT is still a valid option in CLL for selected patients.38
Table 2.
Treatment and follow-up of patients in relapse after hematopoietic stem cell transplantation.

Figure 2.

Post-transplantation minimal residual disease evaluation. At 12 months (M12), 27 of 42 (64%) patients were minimal residual disease negative (MRDneg), 7 of 42 (17%) patients remained MRD positive (MRDpos), 8 of 42 (19%) patients were not evaluable because either prior early toxic death (n=4) and 4 of 42 patients (9.5%) or other reasons including graft rejection (n=2), Eppstein-Barr virus lymproliferation (n=1) and early relapse (n=1).
Figure 3.

Patterns of minimal residual disease response of the 39 patients who engrafted and were alive after 1 month. Pattern A: patients with pre-transplant minimal residual disease negative (MRDneg) status (n=6), Pattern B: patients who converted to MRDneg within 3 months post-transplant without any immune-intervention (n=11). Pattern C : patients who converted to MRDneg upon immune-intervention (cyclosporine A [CsA] withdrawal only) or graft-versus-host disease (GvHD) (n=16) Pattern D: patients who remained MRD positive (MRDpos) during follow-up despite immune-intervention (CsA withdrawal and donor lymphocyte infusion [DLI]) or GvHD (n=7). Solid blue line: negativity limit of MRD (<0.01%). UD : undetectable MRD (MRD < limit of detection [LOD]).
We report the first trial evaluating prospectively an approach of post-transplantation MRD-driven immuneintervention for CLL. M12 MRDneg associated with a reduced risk of relapse and an improvement of disease-free survival, was chosen as the primary endpoint.10-14 We hypothesized that early CsA tapering potentially followed by DLI in case of a post-transplantation MRDpos status could increase the incidence of MRDneg status at M12 and as a consequence could reduce the risk of relapse. Conversely, for patients with a post-transplantation MRDneg status, CsA administration would be extended for a longer period to reduce the risk of chronic GvHD.
In order to minimize severe GvHD incidence, we selected the same ATG containing conditioning regimen as previously evaluated in a large multicenter study performed in a similar age population.18Overall, in this population with a median age close to 60 years, we observed less than 25% extensive cGvHD which appears lower than in previous series of HSCT in CLL and can be considered very acceptable in the context of allogeneic treatment of high-risk diseases.7-10
Moreover, only four deaths were related to either GvHD or infection and the 2-year NRM less than 10%, favorably compares with those varying from 17% to 27% reported in the main series of reduced intensity conditioning transplant in CLL.7-10 In this trial low NRM highly contribute to impressive 3-year OS close to 90%.
We show that post-transplantation MRD-driven immune-intervention is feasible in the setting of a multicenter trial. MRD evaluation was centralized and performed by a sensitive method of high-resolution ten-color flow cytometry. Results were available within 48 hours, allowing a rapid adaptation of the immunosuppressive therapy. Immune-intervention was conducted in accordance to the protocol in 83% of the evaluable patients; in the remaining patients CsA was withdrawn earlier due to graft-failure, mixed chimerism or renal failure. The immune-intervention related toxicity was low, with only two cases of GvHD occurring after CsA withdrawal or DLI applied as per protocol.
Figure 4.

Impact of minimal residual disease negative (MRDneg) status achievement on post transplant outcome according to the Mantel-Byar method illustrated by Simon-Makuch plots (MRD status as a time-dependent event). (A) overall survival, (B) progression-free survival and (C) cumulative incidence of relapse.
In an Intent-To-Treat analysis, the primary end-point of M12 MRDneg status has been achieved in 64 % of the 42 transplanted patients and in 79% of the 34 patients who actually had a M12 MRD evaluation. This result favorably compares with both prospective10 and retrospective11-14 studies reporting 48% to 71% MRDneg status at 6 to 12 months after HSCT.10-14 Particularely our results are in line with one large single-center retrospective analysis of 77 allografted CLL patients submitted to immune modulation based on MRD evaluation.6 In this latter study M12 MRD clearance was achieved in 56% overall and 84% of all patients evaluable for M12 MRD status and the 3-year relapse incidence was 26%. Our data argue for the benefit of an early preemptive immune-intervention based on MRD evaluation. Thus, early CsA withdrawal applied in D90 MRDpos patients translated into MRDneg status at M12 in 69% of them. Moreover, most patients with D90 MRDpos status and GvHD, spontaneously switched to MRDneg at M12, highlighting the role of allogeneic reaction in the control of the disease. Conversely, in this context of early preemptive immune-intervention we failed to show a benefit of DLI to convert MRD from positive to negative, but three of five patients were already in clinical progression at the time of infusion. Finally, considering the non-randomized nature of the trial, our data suggest that a MRD-driven CsA withdrawal can provide durable MRD clearance, improve GvHD leukemia effect and avoid progression.
In several studies, the M12 MRDneg status was associated with lower incidence of relapse.13-15,39 As half of the progression occurred before M12 in our series, we chose to analyze the impact of MRD using MRD as a time dependent variable. We confirm here the strong correlation between an MRDneg status achievement regardless of time point and both low progression and better PFS. Interestingly, we also show that MRDneg status achievement translates into better survival. The impressive post-transplant OS closed to 90% at 3 years in this high-risk CLL population could also be explained by the possibility opened to physician of treating post-allograft relapses with ibrutinib. It should also be noted that the three patients who died from CLL-related cause had Richter's syndrome, including two escaping therapy with ibrutinib.
These data lead us to propose early additional therapy in patients who display an MRDpos status despite either MRDdriven CsA withdrawal or chronic GvHD, or in the rare patients who could experience disease despite MRDneg status achievement. Recent reports show the efficacy of ibrutinib in post-HSCT CLL relapse without limiting toxicity or GvHD, as also observed in our series.40,41 This treatment should be evaluated preemptively in patients who fail to achieve negative MRD after CsA cessation.
In conclusion, this report shows the feasibility of MRD-driven immune-intervention following ATG-based RIC allogeneic HSCT in CLL. These data highlight the importance to repeatedly monitor post-HSCT MRD to guide early CsA discontinuation in patients with D90 MRDpos and without GvHD. However, as we report the results of this study in 2020, we must emphasize that the entry criteria were based on the EBMT 2007 recommendations, which no longer represent current practice. Particularly, this is the case for untreated patients with del(17p) and/or TP53 mutation who represent 26% of the study's enrollment. A presentation of post-transplant outcome excluding these 11 patients is shown in the Online Supplementary Appendix (Online Supplementary Figure S3). Allogeneic HSCT indications have evolved in 2014 under the impulse of the European Research Initiative on CLL (ERIC) and EBMT with of a new decisional algorithm according to patient biology and prior treatment with BCR and BCL-2 inhibitors,42 the feasibility of which has just been reported in a recent analysis.43 The pre-emptive immune modulation based on post-transplant MRD, as described in our study in patients who were 90% naive of BCR and/or BCL-2 treaments, should also be effective in patients pretreated with such agents, but this will have to be demonstrated.
Supplementary Material
Acknowledgments
The study was supported by a National Grant from the Fondation ARC. Logistic support was provided through the Fonds de recherche clinique en hématologie Force Hémato. Les Laboratoires Pierre Fabre provided financial research support for the study, but did not participate in the conduct of the study or data and results analysis.
The authors thank Dr Reza Tabrizi and Dr Oumeladi Reman for their devoted implication in patient care and the clinical research assistants of the FILO group for the onsite monitoring process performed during the study.
References
- 1.Byrd JC, Furman RR, Coutre SE, et al. Targeting BTK with ibrutinib in relapsed chronic lymphocytic leukemia. N Engl J Med. 2013;369(1):32-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Furman RR, Sharman JP, Coutre SE, et al. Idelalisib and rituximab in relapsed chronic lymphocytic leukemia. N Engl J Med. 2014;370(11):997-1007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Roberts AW Davids MS Pagel JM.et al. Targeting BCL2 with venetoclax in relapsed chronic lymphocytic leukemia. N Engl J Med. 2016;374(4):311-322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gribben JG. How and when I do allogeneic transplant in CLL. Blood 2018; 132(1):31-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hallek M. Chronic lymphocytic leukemia: 2017 update on diagnosis, risk stratification, and treatment. Am J Hematol. 2017;92(9):946-965. [DOI] [PubMed] [Google Scholar]
- 6.Hahn M, Böttcher S, Dietrich S, et al. Allogeneic hematopoietic stem cell transplantation for poor-risk CLL: dissecting immune-modulating strategies for disease eradication and treatment of relapse. Bone Marrow Transplant. 2015;50(10):1279-1285. [DOI] [PubMed] [Google Scholar]
- 7.Khouri IF, Bassett R, Poindexter N, et al. Nonmyeloablative allogeneic stem cell transplantation in relapsed/refractory chronic lymphocytic leukemia. Cancer. 2011;117(20):4679-4688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Michallet M, Socié G, Mohty M, et al. Rituximab, fludarabine, and total body irradiation as conditioning regimen before allogeneic hematopoietic stem cell transplantation for advanced chronic lymphocytic leukemia: long-term prospective multicenter study. Exp Hematol. 2013;41(2):127-133. [DOI] [PubMed] [Google Scholar]
- 9.Sorror ML, Storer BE, Sandmaier BM, et al. Five-year follow-up of patients with advanced chroniclLymphocytic leukemia treated with allogeneic hematopoietic cell transplantation after nonmyeloablative conditioning. J Clin Oncol. 2008;26(30):4912-4920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Dreger P, Döhner H, Ritgen M, et al. Allogeneic stem cell transplantation provides durable disease control in poor-risk chronic lymphocytic leukemia: long-term clinical and MRD results of the German CLL Study Group CLL3X trial. Blood. 2010;116(14):2438-2447. [DOI] [PubMed] [Google Scholar]
- 11.Algrin C, Golmard J-L, Michallet M, et al. Flow cytometry minimal residual disease after allogeneic transplant for chronic lymphocytic leukemia. Eur J Haematol. 2017; 98(4):363-370. [DOI] [PubMed] [Google Scholar]
- 12.Farina L, Carniti C, Dodero A, et al. Qualitative and quantitative polymerase chain reaction monitoring of minimal residual disease in relapsed chronic lymphocytic leukemia: early assessment can predict longterm outcome after reduced intensity allogeneic transplantation. Haematologica. 2009;94(5):654-662. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Logan AC, Zhang B, Narasimhan B, et al. Minimal residual disease quantification using consensus primers and high-throughput IGH sequencing predicts post-transplant relapse in chronic lymphocytic leukemia. Leukemia. 2013;27(8):1659-1665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Moreno C, Villamor N, Colomer D, et al. Clinical significance of minimal residual disease, as assessed by different techniques, after stem cell transplantation for chronic lymphocytic leukemia. Blood. 2006;107(11):4563-4569. [DOI] [PubMed] [Google Scholar]
- 15.Ritgen M, Böttcher S, Stilgenbauer S, et al. Quantitative MRD monitoring identifies distinct GVL response patterns after allogeneic stem cell transplantation for chronic lymphocytic leukemia: results from the GCLLSG CLL3X trial. Leukemia. 2008;22(7):1377-1386. [DOI] [PubMed] [Google Scholar]
- 16.Dreger P, Corradini P, Kimby E, et al. Indications for allogeneic stem cell transplantation in chronic lymphocytic leukemia: the EBMT transplant consensus. Leukemia. 2007;21(1):12-17. [DOI] [PubMed] [Google Scholar]
- 17.Sorror ML, Maris MB, Storb R, et al. Hematopoietic cell transplantation (HSCT)- specific comorbidity index: a new tool for risk assessment before allogeneic HSCT. Blood. 2005;106(8):2912-2919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Blaise D, Devillier R, Lecoroller-Sorriano AG, et al. Low non-relapse mortality and long-term preserved quality of life in older patients undergoing matched related donor allogeneic stem cell transplantation: a prospective multicenter phase II trial. Haematologica. 2015;100(2):269-274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hallek M, Cheson BD, Catovsky D, et al. Guidelines for the diagnosis and treatment of chronic lymphocytic leukemia: a report from the International Workshop on Chronic Lymphocytic Leukemia updating the National Cancer Institute–Working Group 1996 guidelines. Blood. 2008;111(12):5446-5456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Rawstron AC, Villamor N, Ritgen M, et al. International standardized approach for flow cytometric residual disease monitoring in chronic lymphocytic leukaemia. Leukemia. 2007;21(5):956-964. [DOI] [PubMed] [Google Scholar]
- 21.Rawstron AC, Böttcher S, Letestu R, et al. Improving efficiency and sensitivity: European Research Initiative in CLL (ERIC) update on the international harmonised approach for flow cytometric residual disease monitoring in CLL. Leukemia. 2013;27(1):142-149. [DOI] [PubMed] [Google Scholar]
- 22.Rawstron AC, Fazi C, Agathangelidis A, et al. A complementary role of multiparameter flow cytometry and high-throughput sequencing for minimal residual disease detection in chronic lymphocytic leukemia: an European Research Initiative on CLL study. Leukemia. 2016;30(4):929-936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Glucksberg H, Storb R, Fefer A, et al. Clinical manifestations of graft-versus-host disease in human recipients of marrow from HL-Amatched sibling donors. Transplantation. 1974;18(4):295-304. [DOI] [PubMed] [Google Scholar]
- 24.Przepiorka D, Weisdorf D, Martin P, et al. 1994 consensus conference on acute GVHD grading. Bone Marrow Transplant. 1995;15(6):825-828. [PubMed] [Google Scholar]
- 25.Mantel N, Byar DP. Evaluation of responsetime data involving transient states: an illustration using heart-transplant data. J Am Stat Assoc. 1974;69:81-86. [Google Scholar]
- 26.Simon R, Makuch RW. A non-parametric graphical representation of the relationship between survival and the occurrence of an event: application to responder versus nonresponder bias. Stat Med. 1984;3(1):35-44. [DOI] [PubMed] [Google Scholar]
- 27.Kharfan-Dabaja MA, Kumar A, Hamadani M, et al. Clinical practice recommendations for use of allogeneic hematopoietic cell transplantation in chronic lymphocytic leukemia on behalf of the guidelines committee of the American Society for Blood and Marrow Transplantation. Biol Blood Marrow Transplant. 2016;22(12):2117-2125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Tournilhac O, van Gelder N, Dreger P, et al. The 10-years EBMT landscape of allogeneic hematopoietic cell transplantation (alloHCT) for chronic lymphocytic leukemia. 46th Annual Meeting of the European Society for Blood and Marrow Transplantation. Madrid, 2020 [Google Scholar]
- 29.Chanan-Khan A, Cramer P, Demirkan F, et al. Ibrutinib combined with bendamustine and rituximab compared with placebo, bendamustine, and rituximab for previously treated chronic lymphocytic leukaemia or small lymphocytic lymphoma (HELIOS): a randomised, double-blind, phase 3 study. Lancet Oncol. 2016;17(2):200-211. [DOI] [PubMed] [Google Scholar]
- 30.Deng R, Gibiansky L, Lu T. Bayesian population model of the pharmacokinetics of venetoclax in combination with rituximab in patients with relapsed/refractory chronic lymphocytic leukemia: results from the Phase III MURANO Study. Clin Pharmacokinet. 2019;58(12):1621-1634. [DOI] [PubMed] [Google Scholar]
- 31.O'Brien S, Furman RR, Coutre S, et al. Single-agent ibrutinib in treatment-naïve and relapsed/refractory chronic lymphocytic leukemia: a 5-year experience. Blood. 2018;131(17):1910-1919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Mato AR, Thompson M, Allan JN, et al. Real-world outcomes and management strategies for venetoclax-treated chronic lymphocytic leukemia patients in the United States. Haematologica. 2018;103(9):1511-1517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Jain P, Thompson PA, Keating M, et al. Longterm outcomes for patients with chronic lymphocytic leukemia who discontinue ibrutinib. Cancer. 2017;123(12):2268-2273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Anderson M, Tam C, Lew TE, et al. Clinicopathological features and outcomes of progression of CLL on the BCL2 inhibitor venetoclax. Blood. 2017;129(25):3362-3370. [DOI] [PubMed] [Google Scholar]
- 35.Porter DL, Hwang W-T, Frey NV, et al. Chimeric antigen receptor T cells persist and induce sustained remissions in relapsed refractory chronic lymphocytic leukemia. Sci Transl Med. 2015;7(303):303ra139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Turtle CJ, Hay KA, Hanafi LA, et al. Durable molecular remissions in chronic lymphocytic Leukemia treated with CD19-specific chimeric antigen receptor-modified T cells after failure of ibrutinib. J Clin Oncol. 2017;35(26):3010-3020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Lemal R. Tournilhac O. State-of-the-art for CAR T-cell therapy for chronic lymphoid leukemia in 2019. J Immunother Cancer. 2019;7(1):202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Dreger P, Ghia P, Schetelig J, et al. High-risk chronic lymphocytic leukemia in the era of pathway inhibitors: integrating molecular and cellular therapies. Blood. 2018;132(9): 892-902. [DOI] [PubMed] [Google Scholar]
- 39.Krämer I, Stilgenbauer S, Dietrich S, et al. Allogeneic hematopoietic cell transplantation for high-risk CLL: 10-year follow-up of the GCLLSG CLL3X trial. Blood. 2017;130(12):1477-1480. [DOI] [PubMed] [Google Scholar]
- 40.Link CS, Teipel R, Heidenreich F, et al. Durable responses to ibrutinib in patients with relapsed CLL after allogeneic stem cell transplantation. Bone Marrow Transplant. 2016;51(6):793-798. [DOI] [PubMed] [Google Scholar]
- 41.Ryan CE, Sahaf B, Logan AC, et al. Ibrutinib efficacy and tolerability in patients with relapsed chronic lymphocytic leukemia following allogeneic HSCT. Blood. 2016;128(25):2899-2908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Dreger P, Schetelig J, Andersen N, et al. Managing high-risk CLL during transition to a new treatment era: stem cell transplantation or novel agents? Blood. 2014;124(26): 3841-3849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Hoffmann A, Dietrich S, Hain S, et al. Allogeneic transplantation in high-risk chronic lymphocytic leukemia: a single-center, intent-to-treat analysis. Haematologica. 2019;104(7):e304-e306. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.