

Abstract
Hemophagocytic lymphohistiocytosis (HLH) is an immune-regulatory disorder characterized by excessive production of inflammatory cytokines. The treatment recommendations of the HLH- 1994 and HLH-2004 protocols have long been used in HLH therapy, but some patients still do not respond well to or have unacceptable side effects from conventional therapies. It is believed that cytokine-targeted strategies that directly target disease-driving pathways will be promising options for HLH. This prospective study aimed to investigate the efficacy and safety of ruxolitinib, a Janus kinase 1/2 inhibitor, as a front-line therapy in children with secondary HLH. Twelve newly diagnosed patients without previous treatment were enrolled in this study with a median follow-up of 8.2 (range, 7.1-12.0) months, including eight cases of Epstein-Barr virus associated HLH (EBV-HLH), two cases of autoinflammatory disorder (AID)- associated HLH, and two cases of unknown etiology. Patients received oral ruxolitinib dosed on 2.5 mg, 5 mg or 10 mg twice daily depending on the body weight for 28 consecutive days. The overall response rate at the end of treatment (day 28) was 83.3% (ten of 12), with 66.7% (eight of 12) in complete response (CR), 8.3% (one of 12) in partial response (PR), and 8.3% (one of 12) in HLH improvement. Among the patients achieving CR, 87.5% (seven of eight) maintained CR condition more than 6 months, and one patient with EBV-HLH relapsed following CR. For the EBV-HLH subgroup, all eight patients responded to ruxolitinib, with a CR rate of 75% and a PR rate of 25%. Two patients with AID-associated HLH had quite different responses, with one showing reversal of the HLH abnormalities soon and the other showing no improvement, as did the two cases of unknown etiology. Patients who had no response or discontinued ruxolitinib all responded well to the subsequent HLH-1994 regimen. The expected 6-month event-free survival rate was 58.3±10.2%. No serious adverse effects were reported. Our study provides further support for the possibility of ruxolitinib targeted therapy for secondary HLH in children. This study was registered in the Chinese Clinical Trials Registry Platform (http://www.chictr.org.cn/) as clinicaltrials gov. Identifier: ChiCTR2000029977.
Introduction
Hemophagocytic lymphohistiocytosis (HLH) is an immune disorder characterized by uncontrolled T-lymphocyte and macrophage activation and excessive production of inflammatory cytokines. Patients present with multiple clinical features, including fever, lymphadenopathy or hepatosplenomegaly, cytopenia, coagulopathy, and potentially life-threatening multisystem organ dysfunction. If left untreated, HLH can result in a high risk of death.1
Currently, HLH-1994 or HLH-2004 regimen is the standard HLH treatment strategy. In this regimen, etoposide and dexamethasone, with or without cyclosporine A, are used to treat active HLH. Long-term results of the HLH-1994 regimen showed that patients had a 5-year survival of 54±6%;2 compared with the HLH-1994 data, the HLH-2004 protocol did not improve HLH outcome significantly with a 5-year survival of 61%,3 which indicates that HLH treatment has not progressed significantly in the past few decades. Furthermore, based on the HLH-1994 or HLH-2004 regimen, intense cytotoxic chemotherapy can induce serious myelosuppressive or broadly immunosuppressive effects leading to severe infection and even death. In addition, the long-term side effect of etoposide in the regimen, secondary tumor risk, also deserves more attention.4-6 Therefore, prospective clinical trials investigating novel pharmacologic treatments for HLH are urgently needed. Recently, interleukin- 1 (IL-1) inhibitors, interferon-γ (IFN-γ) monoclonal antibody and others have been suggested as possible treatment options, with varying clinical effects.7,8
Excessive production of cytokines, including IFN-γ, IL-10 and IL-6, contributes greatly to the pathogenesis of HLH. These overproduced cytokines bind to a broad array of specific receptors and activate the downstream JAK-STAT dependent signal pathway, which finally promotes the transcription of numerous downstream proinflammatory genes.9,10 Based on their essential roles in transmitting cytokine-induced signals, JAK inhibition might serve as a valid therapeutic approach in HLH. Recently, ruxolitinib (RUX), an oral selective JAK1/2 inhibitor, has shown promise in mouse models of primary and secondary HLH.11-13 When RUX is administered, cytokine production and tissue damage are decreased, leading to improved survival in mice. These data have led to interest in the use of RUX clinically for HLH treatment. Recently, RUX was used to treat refractory HLH patients in several case studies.14-16 There are also reports that RUX was used as a first-line treatment in one adult and one childhood HLH patient, and led to clinical remission.17, 18 In addition, a phase I clinical trial (clinicaltrails gov. Identifier: NCT02400463) using RUX in newly diagnosed adult HLH patients is ongoing and has published its preliminary data from the first five enrolled patients, which suggests that RUX is active and safe in that setting.19
However, since the etiology of HLH is complex and the severity of illness varies, the clinical outcome of RUX in the treatment of HLH still needs further investigation to identify the optimal dose and duration. Meanwhile, the specific subtypes of HLH which might show better sensitivity to RUX and the association between treatment response and risk stratification are still unclear. Therefore, we performed an open-label, single-arm, pilot study to investigate the efficacy and safety of RUX as a first-line agent in pediatric HLH and try to clarify the above uncertainties.
Methods
Patients
Patients who were enrolled in this study fulfilled the following criteria: (i) met HLH-2004 diagnostic criteria;20 (ii) had a new diagnosis of HLH; (iii) had no prior chemotherapy treatment for HLH before screening; (iv) were male or female, less than 18 years of age and (v) signed an informed consent form before participating in the study. Patients who had any one of the following were ineligible: serious renal dysfunction (creatinine clearance <15 mL/min or glomerular filtration rate <15 mL/min), liver cirrhosis with a Model for End-stage Liver Disease (MELD) score >20, heart function above grade II (New York Heart Association), presence of a malignancy, parasitic infection, or a history of severe allergic, anaphylactic, or other hypersensitivity reactions to chemicals.
Epstein-Barr virus-associated HLH (EBV-HLH) patients were defined as patients who met the HLH diagnosis criteria and whose EBV infection was confirmed by identifying increased EBV-DNA copy numbers (500 copies/L) in the peripheral blood or plasma (cell-free). Anti-EBV serological pattern showed the EBV status. In brief, EBNA-IgG-negative and EBCA-IgG (or IgM)-positive antibodies would indicate the first exposure to EBV, while positive EBNA-IgG, EBCA-IgG and EBCA-IgM antibodies would indicate EBV reactivation from a previous infection. Autoinflammatory disorder (AID)-HLH patients were defined as patients who met HLH diagnosis criteria and had excessive systemic inflammation, leading to recurrent fever, rashes, and IL-6 overproduction and no evidence of infection, tumor or specific antibody involvement.
Patients were categorized into high- and low-risk groups. High risk was defined as any central nervous system involvement or accordance with at least three of the following criteria: i) age ≤2 years; ii) serious non-laboratory manifestations: severe hepatosplenomegaly, active bleeding, or icterus; iii) absolute neutrophil count <0.5×109/L; iv) soluble CD25 >25,000 pg/mL; v) ferritin >2,000 g/L; vi) a >10-fold increase in IFN-γ from normal levels; and vii) alanine aminotransferase (ALT) >200 U/L. Patients who do not meet the above criteria are considered low risk
Study design and ruxolitinib treatment protocol
The study was registered in the Chinese Clinical Trials Registry Platform (clinicaltrials gov. Identifier: ChiCTR2000029977) and approved by the Ethics Committee of Beijing Children’s Hospital. This is a single-arm, open-label, pilot study to investigate the efficacy and safety of RUX as a front-line therapy in children with secondary HLH. Twelve patients were enrolled in this study. Patients in this study received oral RUX phosphate tablets on a 28-day cycle for one cycle. The dose was 2.5 mg, 5 mg or 10 mg twice daily depending on the body weight (≤10 kg, ≤20 kg or >20 kg, respectively). Therapy was changed immediately when there was no response after 3 days of treatment or at any time during treatment due to disease progression, relapse or toxic effects requiring drug discontinuation. The data cutoff for the primary analysis occurred when all patients completed day 28 of or discontinued therapy.
Study end points
The primary efficacy endpoint was the overall response (OR) rate at day 28 of the last dose, including the proportion of patients achieving a complete response (CR), a partial response (PR) and HLH improvement. Secondary efficacy endpoints included the 6-month event-free survival (EFS, defined as the time from initial RUX treatment to the first occurrence of disease progression, relapse or death; for non-responders, EFS was defined as date of enrollment plus 1 day). Other end points included the durability of response, symptom reduction, dynamic changes of key biomarkers during treatment, the relationship between treatment response and risk stratification, and safety. In addition, for patients who discontinued and changed therapy regimens, we also counted the subsequent treatment responses and outcomes.
Assessment of treatment
Efficacy was evaluated 7, 14 and 28 days after initiating RUX therapy. The assessment of treatment was mainly based on the criterion previously described in studies for pediatric HLH.8, 21 A complete response was defined as normalization of all of the quantifiable symptoms and laboratory markers of HLH, including no fever (body temperature <37.5°C), no cytopenia (absolute neutrophil count ≥1.0×109/L and platelet count ≥100×109/L with the absence of granulocyte colony-stimulating factor (G-CSF) and transfusion support must be documented for ≥4 days), no evidence of coagulopathy (fibrinogen levels >1.50 g/L), normal levels of soluble CD25, ferritin and triglyceride, normal spleen size as measured by abdominal ultrasound, and no neurological and CSF abnormalities attributed to HLH. A partial response was defined as normalization of ≥3 of the aforementioned HLH abnormalities (including CNS abnormalities) and no progression of other aspects of HLH disease pathology. HLH improvement was defined as at least a 50% improvement in ≥3 HLH abnormalities from baseline. At least a 50% worsening in two or more signs or laboratory abnormalities was considered progressive disease. Three or more symptoms and laboratory markers developing into abnormalities after achieving complete response was defined as relapse.
Table 1.
The main clinical features of enrolled patients at diagnosis.

Table 2.
Response outcomes.

Side effects and complications
The safety population included all patients who received at least one dose of RUX.
Adverse events were assessed according to the National Cancer Institute Common Terminology Criteria for Adverse Events, version 3.0. (http://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/ctcaev3.pdf). In detail, we monitored the enrolled patients for any signs of toxicity and complications every day for the first week of treatment, weekly during weeks 2-4, and monthly thereafter, including routine blood tests, coagulation, infections (i.e., latent tuberculosis, adenovirus, Epstein-Barr virus, cytomegalovirus, herpes zoster, Pneumocystis jirovecii and fungal infections), cardiac function (myocardial enzyme spectrum, electrocardiogram, ultrasound cardiogram), renal function (serum creatinine, urea nitrogen, and creatinine clearance), liver function (ALT, AST, GGT, ALB, TBIL, I-BIL, D-BIL), and other adverse drug reactions such as dizziness, headache, rash, dyspnea and gastrointestinal reaction.
Statistical analysis
SPSS 20.0 software (SPSS, Chicago, IL, USA) was used for statistical analysis. All normally distributed data are represented as means ± standard deviations, and comparisons of multiple parameters between groups were performed by independent sample ttests. All data that were not distributed normally are represented as medians and ranges, and comparisons of multiple parameters between groups were performed by Wilcoxon rank sum tests. Patient survival was estimated by the Kaplan-Meier method, and differences in survival between groups were estimated by the logrank test. In all analyses, P<0.05 was considered to denote a significant difference, and P<0.01 was considered very significant. For patients who discontinued RUX within 7 days, the last known values were used as the day 7 laboratory results.
Figure 1.

Event-free survival of patients defined as the time from the initial dose of ruxolitinib to the first occurrence of disease progression, relapse or death (event).
Results
Characteristics of the patients
Twelve pediatric patients with newly diagnosed HLH were enrolled at Beijing Children’s Hospital from June 2019 to October 2019, including eight males and four females. The main clinical features of the enrolled patients at diagnosis are summarized in Table 1. The median age was 4.7 (range, 1.3-13.4) years. The median duration before HLH diagnosis was 11.5 (range, 4-92) days. From onset to diagnosis, except for patient 3 who did not receive any treatment, the patients had been typically treated with antibiotics, ganciclovir or intravenous immunoglobulin (Ig). Five subjects had been given corticosteroids for 2-4 days, but all discontinued use before they were referred to our hospital due to a lack of response. Whole-exome sequencing (WES) was performed for all patients and their parents, and no pathogenic gene mutation associated with primary HLH was found. No patient had central nervous system (CNS) involvement at enrollment. All subjects had negative evaluations for malignant tumors after bone marrow or cervical lymph node biopsy. The primary disease could not be determined in two of the 12 HLH patients; in the other ten patients, eight cases were EBV-HLH, and two cases were AID-HLH. In the EBV-HLH subgroup, two patients experienced their first exposure to EBV, five involved EBV reactivation, and one case was clearly identified as chronic active EBV (CAEBV). We classified the patients according to our stratification criteria with four patients at low risk and eight at high risk.
Figure 2.

Dynamics of hemophagocytic lymphohistiocytosis disease features during ruxolitinib treatment in eight patients who achieved complete response. (A) daily maximum temperature, within hours of receiving the first dose of ruxolitinib (RUX), most patient’s fever resolved; (B to D) The inflammatory markers soluble CD25 (sCD25), ferritin and interferon-γ (IFN-γ) cytokine level. Normal range values of sCD25, ferritin and IFN-γ are ≤6,400 pg/mL, ≤500 mg/L and ≤8 pg/mL respectively by the clinical laboratory; (E to G) absolute neutrophil count, hemoglobin concentration, absolute platelet count; (H) fibrinogen concentration; (I) triglyceride; (J) alanine aminotransferase (ALT) concentration. The dotted line on the x-axis of each graph indicate the start of RUX treatment.
Efficacy of ruxolitinib treatment
Table 2 shows the response outcomes in detail. Among the entire cohort, eight of 12 patients completed the 28-day treatment protocol and achieved CR, but one relapsed at the time of the fourth scheduled response assessment (day 28), and was refractory to alternative HLH-1994 regimen and finally died. Four of 12 patients discontinued the therapy after 3-7 days of treatment and were adjusted to the HLH-1994 regimen for the following reasons: two subjects had no response to RUX and progressively deteriorated; one subject had a partial response for the first 7 days of therapy but progressed soon; one achieved obvious HLH improvement over the first 5 days of treatment; however, the patient remained critically ill and developed potential CNS involvement with drowsiness, although his brain MRI and cerebrospinal fluid (CSF) exam showed no abnormalities. According to the above, for the primary endpoint, the best OR rate to RUX at the end of treatment protocol was 83.4% (ten of 12 patients), with 66.7% (eight of 12 patients) in CR, 8.3% (one of 12 patients) in PR, and 8.3% (one of 12 patients) in HLH improvement. Among the patients who achieved CR, 87.5% (seven of eight patients) maintained CR condition for >6 months. For the eight patients with EBV-HLH, the overall response was 100%, with 75% (six of eight patients) in CR and 25% (two of eight patients) in PR; however, 16.7% (one of six patients) relapsed after CR. Two AID-HLH patients had quite different responses, with one showing reversal of HLH abnormalities soon and the other showing no improvement, as did the two patients of unknown etiology. All patients who had no response or discontinued RUX responded well to the subsequent HLH-1994 regimen, achieved CR and remained off therapy except one (AID-HLH) still in treatment maintenance until data cutoff.
The EFS time was calculated from the date of RUX therapy. All patients were followed up until death or June 7, 2020 (time of data cutoff), whichever occurred first, with a median follow-up of 8.2 (range, 7.1-12.0) months. A total of five of 12 patients had an event, and the expected 6-month EFS rate was 58.3%±14.2% (Figure 1). Patients in the highrisk group showed a tendency towards a worse EFS rate than those in the low-risk group, but there was no statistical significance in this small-scale analysis (50.0±17.7% vs. 75.0±21.7%, P=0.556) (Online Supplementary Figure S1 in the Online Supplementary Appendix).
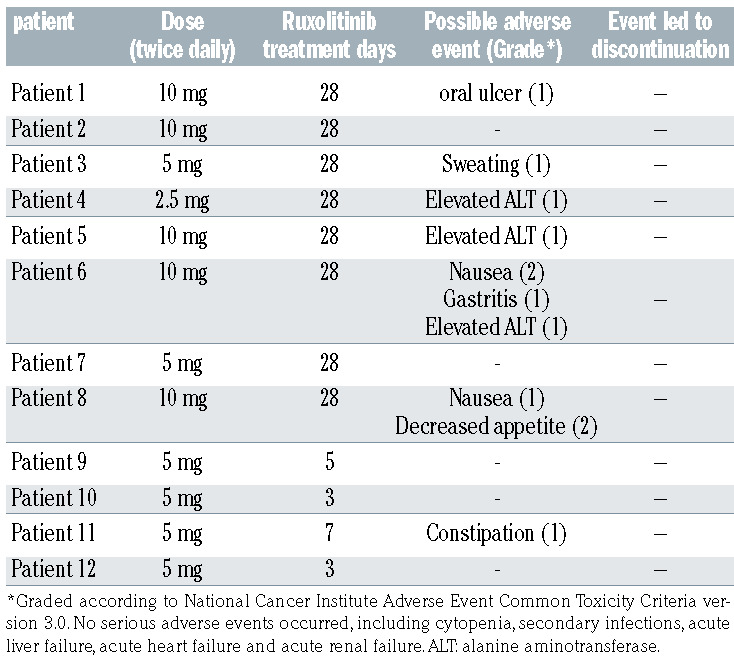
Table 3.
Adverse events observed in this study.
Changes in evaluation indicators before and after ruxolitinib therapy
We analyzed 12 HLH-associated symptoms and laboratory parameters before, and 1, 2, 4 and 8 weeks after RUX treatment. Some indicators, such as temperature and routine blood, were tested every day within the first treatment week as much as possible. Rapid resolution of various indicators was observed with continued therapy. At day 14, a complete recovery in almost all parameters was achieved in eight patients with good response (Figure 2), whereas patients with no response or progress had a persistent abnormality in many indicators (Online Supplementary Figure S2). No relationship was found between patient characteristics at diagnosis and the treatment response (Online Supplementary Table 1). We further analyzed the data before and 1 week after RUX treatment in the CR and non-CR groups respectively. There was a significant difference between the two groups in the improvement of temperature, soluble CD25, ferritin, IFN-γ and neutrophil counts, suggesting that these parameters were important indicators for evaluating the treatment response of RUX in the early phase (Figure 3). Other key cytokines, including IL-6, IL-10, TNF-a and IL-18, showed a similar trend to IFN-γ (Online Supplementary Figure S3).
In detail, within hours of receiving the first dose of RUX, ten of 12 patients became afebrile; however, for the patients who did not respond well to RUX, the antipyretic effect was not sustainable, and the fever recurred within 48-72 hours (Figure 2A; Online Supplementary Figure S2A). Dramatic improvements in soluble CD25 and serum ferritin were observed, falling rapidly to normal levels within approximately 1-2 weeks (Figure 2B and C); in contrast, for patients (patient 10 and 12) who were nonresponsive to RUX, soluble CD25 and serum ferritin increased to high levels (Online Supplementary Figure S2B and C). We also monitored the level of IFN-γ, a key cytokine in HLH. High inflammation was relieved in all well-responsive patients, with IFN-γ decreasing rapidly to normal levels at 2 weeks (Figure 2D). Cytopenia and coagulopathy progressively improved in all responding patients with blood transfusion support weaned off within 1 week. Platelet counts, in particular, increased to the normal range quickly within 1 week. Neutrophil count improvement varied, but all reached 1×109/L at 2 weeks and 2×109/L at 4 weeks. Hemoglobin and fibrinogen concentrations improved with slightly slower kinetics (Figure 2E and H). Triglyceride was not improved immediately with a rapid phase of improvement 1 week after starting RUX in most individuals (Figure 2I). Hepatic dysfunction resolved within 2 weeks (Figure 2J).
Figure 3.

Comparison of clinical indicators changes before and 1 week after ruxolitinib therapy in the complete response group (CR, n=8) and non-CR group (n=4) respectively. For patients who discontinued ruxolitinib (RUX) within 7 days, the last known values were used as the week-1 laboratory results. For statistical analysis, the paired sample Wilcoxon signed rank test was applied.
In addition, EBV DNA load decreased dramatically in all EBV-HLH patients (Figure 4). Among them, EBV infections were resolved in six of eight patients 1-2 weeks after RUX treatment, with cell-free (plasma) EBV DNA becoming undetectable and having no recurrence after stopping treatment until the data cutoff (June 7, 2020) except in patient 8 (CAEBV). The median time that plasma EBV DNA was maintained negative in these patients was approximately 8.7 (range, 0.5-12.0) months. Meanwhile, EBV DNA in whole blood also fell rapidly from very high levels (105-107 copies/mL) to modest levels (103-104 copies/mL), and fluctuated at these modest levels during follow-up.
Side effects
Treatment was well tolerated, with no toxicities leading to dose-reductions or interruptions of RUX observed. All possible adverse events are reported in Table 3. Although RUX has been reported to have a risk of thrombocytopenia or anemia in other settings, these side effects were not observed in our study. Cytopenia is a major clinical feature of HLH. However, patients who achieved a response to RUX had neutrophil counts, platelet counts and hemoglobin concentrations that improved gradually compared to pretreatment levels. No unusual infections were noted. Renal function was analyzed by creatinine clearance, and cardiac function tested by myocardial enzyme spectrum and ultrasound cardiogram was normal during the clinical course. Three individuals had moderately elevated ALT at 60 days after treatment, which may not have been due to RUX, as they had been off the drug for approximately 1 month. Two patients hadtwo or more grade 1-2 gastrointestinal adverse events (nausea, gastritis, decreased appetite) and were resolved soon by supportive therapies. In addition, three patients showed mild oral ulcers, sweating or constipation, and recovered without special treatment.
Discussion
HLH is a disorder characterized by high inflammatory cytokine production induced by excessive immune activation. Recently, cytokine-targeted approaches have been suggested as possible treatment options, such as emapalumab. 8, 22, 23 Rather than targeting a single cytokine, RUX can blunt numerous cytokines via inhibition of the JAK 1/2- STAT1 pathway, which makes its clinical use for HLH more rational.11-13 Currently, RUX is often recommended for refractory/relapsed HLH as a salvage treatment regimen; however, its use as a first-line agent is still based on only a small number of case reports, clinician experience or small clinical studies (clinicaltrials gov. Identifier: NCT02400463). To date, the optimal duration of RUX therapy, the utility of concurrent corticosteroids, and the effect of disease etiology or risk stratification on treatment response remain uncertain.
In this study, we explored the efficacy and safety of RUX monotherapy instead of chemotherapy for secondary HLH in children. RUX has been used for myelofibrosis,24 polycythemia, 25 and graft-versus-host disease (GvHD)26, 27 and is generally dosed between 5 mg and 25 mg twice daily, demonstrating good clinical benefits and tolerance. In addition, in patients with relapsed or refractory myeloproliferative neoplasms especially those with JAK2 or CSF3R mutations, the RUX dose can be increased to 50-200 mg twice a day, and is reasonably tolerated overall.28, 29 The pediatric dosing of RUX in HLH is unestablished. The dose in this study (2.5-10 mg) was modified with reference to the lower dose used for GvHD in children,30 which, similar to HLH, is characterized by the production of high levels of proinflammatory cytokines. In order to eliminate the probable interference of corticosteroid use, we enrolled newly diagnosed patients who had not undergone previous corticosteroid treatment or who had used but discontinued corticosteroids at least 3 days before trial screening due to a lack of response.
Figure 4.

Eppstein-Barr virus DNA levels in the whole blood and plasma after treatment with ruxolitinib. Reported Eppstein-Barr virus (EBV) DNA values are limited to 500 copies/L by the clinical laboratory. The dotted line on the x-axis of each graph indicate the start of RUX treatment.
Our results demonstrate that RUX is effective and safe in pediatric patients with secondary forms of HLH. The rapid resolution of clinical symptoms and normalization of clinical laboratory parameters were observed. The OR rate at the end of the treatment protocol (day 28) was 83.3% (ten of 12 patients), with 66.7% (eight of 12 patients) in complete response, and all remained in CR until the data cutoff except for one who relapsed. No serious adverse effects were reported. These findings suggested that RUX may serve as a potential first-line treatment option for secondary HLH, which can greatly reduce the toxic effects compared with intense chemotherapy. In addition, for patients who need biopsy analysis, RUX instead can provide more opportunities to find the original disease cause than corticosteroid-based therapy. Our study also showed that RUX had a quick effect, and for patients for whom RUX did not work well, we can probably identify this trend within approximately 3 days. Notably, the patients who had poor response to RUX after 3-7 days of treatment all responded well to the subsequent HLH-1994 regimen. This further suggests the possibility that we can attempt to use RUX first for approximately 3 days to determine the treatment response; for patients with poor efficacy, we can then combine it with chemotherapy regimen, which may not cause delayed treatment and poor prognosis. Future studies are warranted to determine the viability of this idea. However, this does not mean that the efficacy of RUX is superior to that of HLH-1994/2004 regimen, which is also used to treat a major proportion of patients with primary HLH. Our main purpose is to sort suitable patients to avoid chemotherapy when possible, and make treatment available for patients deemed unsuitable for chemotherapy. We believe that RUX and standard chemotherapy may be two complementary first-line therapy strategies, as there are patients who cannot be solved by either RUX or chemotherapy. The key point is to find the specific HLH settings sensitive to RUX to guide better treatment in the future.
EBV-HLH accounts for approximately 60% of all pediatric HLH patients in China. EBV-HLH also accounts for a significant proportion of patients who are resistant to standard treatment and have a poor prognosis.31 No previous studies have focused on the association between etiology and RUX treatment response. In addition, current ongoing trials investigating the use of RUX in HLH have not yet enrolled EBV-HLH patients.19 Therefore, our study focused more on to the relationship between EBVHLH and RUX treatment. We enrolled eight EBV-HLH patients, the response rate was 100% (eight of eight), the CR rate was 75% (six of eight), and persistent EBV infection in plasma of these subjects resolved rapidly. This suggests the possibility of RUX for treating EBV-HLH. However, one subject relapsed soon after CR, experienced disease recurrence 1 month after the subsequent HLH-1994 therapy, and finally died. This patient had CAEBV disease that induced HLH. For CAEBV patients with HLH signs, initiating HLH-directed treatment is required to suppress the life-threatening inflammatory process that underlies HLH. In our patient, RUX could transiently control her HLH condition, but was ineffective for the CAEBV. Generally, in the absence of hematopoietic stem cell transplantation (HSCT), therapy for CAEBV, including other cytotoxic chemotherapy, can often delay the progression of disease at best, but over time, the patients become refractory and progress to an irreversible stage.
It is interesting that patients in our study were able to clear the persistent EBV DNA in the plasma (initial concentration 7.28×106-4.38×104copies/L) within 1 week after RUX treatment and had no EBV recurrence except for the CAEBV subject. We are not sure about the duration of this EBV DNA decline, since T- or natural killer (NK)-cell infection is prone to reactivation, whereas all patients in this study exhibited multiple-cell-type EBV infection predominated by the T- or NK-cell subset. There are several explanations for this decrease in EBV DNA. First, it may be related to the EBV infection being either a first infection or a reactivation. Self-limiting is possible in patients with a first EBV infection like infectious mononucleosis. In addition, emapalumab (an anti– IFN-γ monoclonal antibody) has been reported to resolve persistent EBV infection in one patient, perhaps due to relief of immune paralysis caused by IFN-γ .23 As RUX can blunt numerous cytokines, including IFN-γ, the resolution of the EBV infection in this study may also be attributed to the relief of immune paralysis after RUX treatment, which primed the body immunity and ultimately resolved the EBV infection spontaneously. Moreover, evidence suggests that host cell stress such as oxidative stress, hypoxia and inflammation can induce EBV reactivation from latency.32 All of these factors may be removed after the excessive inflammation has been controlled by RUX, leading to a switch of EBV cycle from a lytic state to a latent state. In addition, we enrolled two patients with autoinflammatory diseases-associated HLH, but these two individuals had quite different responses to RUX, with one showing reversal of the HLH abnormalities soon and the other showing no improvement. Similarly, two patients of unknown etiology also showed two different kinds of responses. The RUX dose may not have been sufficient for these non-/poor-responders in this study. Moreover, the great heterogeneity of HLH, such as the etiology, clinical features and risk stratification, may also contribute to this difference. Therefore, further study is needed to optimize the clinical use of RUX, such as identifying some sensitive biomarkers.
In summary, our preliminary study provides further support for the possibility of RUX-based targeted therapy in pediatric patients with secondary HLH. Since patients with known CNS involvement were not enrolled in this study, we were unable to make statements on the efficacy of ruxolitinib in the CNS. The number of patients in this study was small, and the observation time was relatively short. We are currently performing a large-scale, open-label, prospective trial on RUX monotherapy for pediatric HLH, which may answer more uncertainties and provide further evidence for RUX treatment as a firstline therapy in HLH.
Supplementary Material
Funding Statement
Funding: The authors would like to thank grants from the National Natural Science Foundation of China (No. 81800189); Beijing Municipal Administration of Hospitals’ Youth Programme (QML20181205); the Scientific Research Common Program of Beijing Municipal Commission of Education (No. KM201910025011); the Special Fund of The Pediatric Medical Coordinated Development Center of Beijing Municipal Administration (No. XTZD20180202); National Science and Technology Key Projects (No. 2017ZX09304029003); Guangdong Province Key Laboratory of Popular High Performance Computers of Shenzhen University (SZU-GDPHPCL2017) .
References
- 1.Thomas W, Veer MV, Besser M. Haemophagocytic lymphohistiocytosis: an elusive syndrome. Clin Med (Lond). 2016; 16(5):432-436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Trottestam H, Horne A, Aricò M, et al. Chemoimmunotherapy for hemophagocytic lymphohistiocytosis: long-term results of the HLH-94 treatment protocol. Blood. 2011; 118(17):4577-4584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bergsten E, Horne A, Aricó M, et al. Confirmed efficacy of etoposide and dexamethasone in HLH treatment: long-term results of the cooperative HLH-2004 study. Blood. 2017;130(25):2728-2738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Pui CH, Ribeiro RC, Hancock ML, et al. Acute myeloid leukemia in children treated with epipodophyllotoxins for acute lymphoblastic leukemia. N Engl J Med. 1991; 325(24):1682-1687. [DOI] [PubMed] [Google Scholar]
- 5.Henter JI, Elinder G, Lübeck PO, Ost A. Myelodysplastic syndrome following epipodophyllotoxin therapy in familial hemophagocytic lymphohistiocytosis. Pediatr Hematol Oncol. 1993;10(2):163-168. [DOI] [PubMed] [Google Scholar]
- 6.Kitazawa J, Ito E, Arai K, Yokoyama M, Fukayama M, Imashuku S. Secondary acute myelocytic leukemia after successful chemotherapy with etoposide for Epstein- Barr virus-associated hemophagocytic lymphohistiocytosis. Med Pediatr Oncol. 2001; 37(2):153-154. [DOI] [PubMed] [Google Scholar]
- 7.Miettunen PM, Narendran A, Jayanthan A, Behrens EM, Cron RQ. Successful treatment of severe paediatric rheumatic disease-associated macrophage activation syndrome with interleukin-1 inhibition following conventional immunosuppressive therapy: case series with 12 patients. Rheumatology (Oxford). 2011;50(2):417-419. [DOI] [PubMed] [Google Scholar]
- 8.Locatelli F, Jordan MB, Allen C, et al. Emapalumab in children with primary hemophagocytic lymphohistiocytosis. N Engl J Med. 2020;382(19):1811-1822. [DOI] [PubMed] [Google Scholar]
- 9.Villarino AV, Kanno Y, Ferdinand JR, O'Shea JJ. Mechanisms of Jak/STAT signaling in immunity and disease. J Immunol. 2015;194(1):21-27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kiu H, Nicholson SE. Biology and significance of the JAK/STAT signalling pathways. Growth Factors. 2012;30(2):88-106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Das R, Guan P, Sprague L, et al. Janus kinase inhibition lessens inflammation and ameliorates disease in murine models of hemophagocytic lymphohistiocytosis. Blood. 2016;127(13):1666-1675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Maschalidi S, Sepulveda FE, Garrigue A, Fischer A, de Saint Basile G. Therapeutic effect of JAK1/2 blockade on the manifestations of hemophagocytic lymphohistiocytosis in mice. Blood. 2016;128(1):60-71. [DOI] [PubMed] [Google Scholar]
- 13.Albeituni S, Verbist KC, Tedrick PE, et al. Mechanisms of action of ruxolitinib in murine models of hemophagocytic lymphohistiocytosis. Blood. 2019;134(2):147-159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sin JH, Zangardi ML. Ruxolitinib for secondary hemophagocytic lymphohistiocytosis: first case report. Hematol Oncol Stem Cell Ther. 2019;12(3):166-170. [DOI] [PubMed] [Google Scholar]
- 15.Broglie L, Pommert L, Rao S, et al. Ruxolitinib for treatment of refractory hemophagocytic lymphohistiocytosis. Blood Adv. 2017;1(19):1533-1536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wang J, Wang Y, Wu L, et al. Ruxolitinib for refractory/relapsed hemophagocytic lymphohistiocytosis. Haematologica. 2020;105(5):e210-e212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Slostad J, Hoversten P, Haddox CL, Cisak K, Paludo J, Tefferi A. Ruxolitinib as first-line treatment in secondary hemophagocytic lymphohistiocytosis: a single patient experience. Am J Hematol. 2018;93(2):E47-e49. [DOI] [PubMed] [Google Scholar]
- 18.Zandvakili I, Conboy CB, Ayed AO, Cathcart-Rake EJ, Tefferi A. Ruxolitinib as first-line treatment in secondary hemophagocytic lymphohistiocytosis: a second experience. Am J Hematol. 2018;93(5):E123-e125. [DOI] [PubMed] [Google Scholar]
- 19.Ahmed A, Merrill SA, Alsawah F, et al. Ruxolitinib in adult patients with secondary haemophagocytic lymphohistiocytosis: an open-label, single-centre, pilot trial. Lancet Haematol. 2019;6(12):e630-e637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Henter JI, Horne A, Aricó M, et al. HLH- 2004: diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediat Blood Cancer. 2007;48(2):124-131. [DOI] [PubMed] [Google Scholar]
- 21.Marsh RA, Allen CE, McClain KL, et al. Salvage therapy of refractory hemophagocytic lymphohistiocytosis with alemtuzumab. Pediat Blood Cancer. 2013;60(1):101-109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Marsh RA, Jordan MB, Talano JA, et al. Salvage therapy for refractory hemophagocytic lymphohistiocytosis: a review of the published experience. Pediat Blood Cancer. 2017;64(4). [DOI] [PubMed] [Google Scholar]
- 23.Lounder DT, Bin Q, de Min C, Jordan MB. Treatment of refractory hemophagocytic lymphohistiocytosis with emapalumab despite severe concurrent infections. Blood Adv. 2019;3(1):47-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Verstovsek S, Mesa RA, Gotlib J, et al. A double- blind, placebo-controlled trial of ruxolitinib for myelofibrosis. N Engl J Med. 2012;366(9):799-807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Vannucchi AM, Kiladjian JJ, Griesshammer M, et al. Ruxolitinib versus standard therapy for the treatment of polycythemia vera. N Engl J Med. 2015;372(5):426-435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Przepiorka D, Luo L, Subramaniam S, et al. FDA approval summary: ruxolitinib for treatment of steroid-refractory acute graft-versushost disease. Oncologist. 2020;25(2):e328-e334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Zeiser R, Burchert A, Lengerke C, et al. Ruxolitinib in corticosteroid-refractory graftversus- host disease after allogeneic stem cell transplantation: a multicenter survey. Leukemia. 2015;29(10):2062-2068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Pemmaraju N, Kantarjian H, Kadia T, et al. A phase I/II study of the Janus kinase (JAK)1 and 2 inhibitor ruxolitinib in patients with relapsed or refractory acute myeloid leukemia. Clin Lymphoma Myeloma Leuk. 2015;15(3):171-176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Dao KT, Gotlib J, Deininger MMN, et al. Efficacy of ruxolitinib in patients with chronic neutrophilic leukemia and atypical chronic myeloid leukemia. J Clin Oncol. 2020; 38(10):1006-1018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.González Vicent M, Molina B, González de Pablo J, Castillo A, Díaz M. Ruxolitinib treatment for steroid refractory acute and chronic graft vs host disease in children: Clinical and immunological results. Am J Hematol. 2019;94(3):319-326. [DOI] [PubMed] [Google Scholar]
- 31.Wang J, Wang Y, Wu L, Zhang J, Lai W, Wang Z. PEG-aspargase and DEP regimen combination therapy for refractory Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis. J Hematol Oncol. 2016;9(1):84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Li H, Liu S, Hu J, et al. Epstein-Barr virus lytic reactivation regulation and its pathogenic role in carcinogenesis. Int J Biol Sci. 2016; 12(11):1309-1318. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.