

Abstract
Objective
The use of telemedicine has dramatically increased due to the coronavirus disease 2019 pandemic. Many neurosurgeons are now using telemedicine technologies for preoperative evaluations and routine outpatient visits. Our goal was to standardize the telemedicine motor neurologic examination, summarize the evidence surrounding clinical use of telehealth technologies, and discuss financial and legal considerations.
Methods
We identified a 12-member panel composed of spine surgeons, fellows, and senior residents at a single institution. We created an initial telehealth strength examination protocol based on published data and developed 10 agree/disagree statements summarizing the protocol. A blinded Delphi method was utilized to build consensus for each statement, defined as > 80% agreement and no significant disagreement using a 2-way binomial test (significance threshold of p < 0.05). Any statement that did not meet consensus was edited and iteratively resubmitted to the panel until consensus was achieved. In the final round, the panel was unblinded and the protocol was finalized.
Results
After the first round, 4/10 statements failed to meet consensus (< 80% agreement, and p = 0.031, p = 0.031, p = 0.003, and p = 0.031 statistical disagreement, respectively). The disagreement pertained to grading of strength of the upper (3/10 statements) and lower extremities (1/10 statement). The amended statements clarified strength grading, achieved consensus (> 80% agreement, p > 0.05 disagreement), and were used to create the final telehealth strength examination protocol.
Conclusion
The resulting protocol was used in our clinic to standardize the telehealth strength examination. This protocol, as well as our summary of telehealth clinical practice, should aid neurosurgical clinics in integrating telemedicine modalities into their practice.
Keywords: Telemedicine, Neurosurgery, Telehealth, Neurologic exam, Delphi method
INTRODUCTION
Telemedicine, also known as telehealth, involves the communication of medical information through electronic systems for the delivery of health care, education, and health administration [1]. Potential benefits of telemedicine technologies include providing access to care for patients without a local provider, reducing patient wait and travel times, and decreasing health care costs. Telemedicine has been steadily increasing in use, especially as associated technologies continue to improve [1,2]. In 2016, the Department of Health and Human Services (HHS) estimated that 60% of health care institutions in the United States used some sort of telemedicine modality, although use remained relatively limited due to lack of patient interest as well as concerns surrounding billing, regulatory and medicolegal matters [1,3]. The coronavirus disease 2019 (COVID-19) pandemic and associated social distancing measures have brought renewed attention to the use of telemedicine in the United States. The HHS has subsequently relaxed regulatory requirements for telemedicine to encourage its use during the pandemic and reduce patient exposure to health care facilities [4]; telemedicine is now an integral part of many health care systems across the country. The use of telemedicine for clinical care will likely remain prevalent throughout the United States given the long-term need for social restrictions [5].
As a result, neurosurgeons are now faced with the reality of using telemedicine modalities to provide outpatient care, such as in a neurosurgical spine clinic, to minimize the risk of virus transmission. Although new federal policies have increased the accessibility of telemedicine technologies, a number of challenges remain. Primary amongst these is the lack of standardized tele-neurologic examination maneuvers, which is crucial in assessing and following neurosurgical patients. While previous studies have highlighted the reliability of the neurologic exam performed over telehealth technologies, they frequently require the use of an assistant [6-9]. Thus, as patients increasingly attend telehealth visits from their home in order to avoid health care facilities, there is a significant need for a standardized in-home neurologic exam. An additional challenge to the implementation of telehealth technologies in neurosurgical clinics is the lack of familiarity with the clinical evidence surrounding their use as well as unique financial and liability considerations.
To help address these concerns, we (1) describe a standard tele-neurologic examination, based on available evidence in the literature and (2) create a consensus-based tele-strength examination protocol, as this is one of the most challenging parts of a tele-neurologic examination. We then highlight the utility of our protocol through a clinical case of a lumbar disc herniation leading to foot drop that was observed during a telehealth visit using our examination maneuvers. Finally, we discuss the clinical evidence surrounding outpatient neurosurgical telehealth visits, financial and legal considerations, and COVID-19 specific changes.
MATERIALS AND METHODS
1. Literature Review, Quantifying Telehealth Visits
We first performed a literature search to find all spine surgery and neurosurgery articles pertaining to the telehealth neurological examination, as well as billing and coding practices for telemedicine. We found that there were not enough articles to formulate a formal meta-analysis, and therefore used our literature search to create protocol for the Delphi method. Regarding billing, it was not possible to obtain a meta-analysis for 2 reasons: (1) there was an overall lack of published data addressing the billing of the telemedicine in neurosurgery and (2) the COVID-19 pandemic resulted in Centers for Medicare and Medicaid Services (CMS) waiver 1135 (starting March 6, 2020; corona virus waiver) that temporarily reduced restrictions surrounding telehealth care. Thus, the current uncertainty of the permanence of this waiver, combined with the paucity of literature pertaining to neurosurgery clinic visits, precluded a systematic review of telehealth billing. Instead, we summarize current billing practices in the discussion. To better understand the role of telehealth in our patient population, we quantified the number of patients seen in-clinic since the start of the pandemic on a day-by-day basis.
2. Delphi Method
The Delphi Method was used to create a consensus-based tele-strength examination [10,11]. Twelve neurological surgeons (7 spine surgeons, 2 fellows, and 3 senior residents) at our institution were given a 10-item online survey (SurveyMonkey) relating to specific aspects of the tele-strength examination. Surgeons could either “agree” or “disagree” with a given statement. Responses to the initial survey were collected and analyzed. Participants were blinded to each other’s responses and to the identity of the other members of the panel. Consensus was defined ahead of time using 2 criteria: (1) > 80% agreement of the panel for a particular question and (2) an exact binomial statistical test against the expected hypothesis of 95% agreement using a 2-tailed p-value threshold of p < 0.05. All statements failing to meet consensus were analyzed, and direct feedback from disagreeing surgeons was sought. Questions failing to meet consensus were then modified and resubmitted to the expert panel in a second round of the Delphi method. After consensus for all statements was achieved, the final protocol was drafted and sent to the members of the panel. Panel members were unblinded for this portion of the Delphi method. The protocol was then finalized with direct panel member communication to each other.
3. Statistical Methods
All statistical methods were carried out in Matlab (version release 2017b, Mathworks, Inc., Natick, MA, USA) using custom software to implement the 2-sided exact binomial test, as well as the plotting function.
RESULTS
1. Rate of Telehealth Visits During the COVID-19 Pandemic
Fig. 1 demonstrates the number of patients that were seen using telehealth over an 8-week period at our spine clinic, including before the county’s COVID-19 shelter-in-place order (week 1), immediately following the shelter-in-place order (weeks 2–3), and after the shelter-in-place order until the time of writing (weeks 4–8). In order to protect patient identity, exact dates are not shown. As seen, telehealth visits increased in our spine clinic by 10 times following the shelter-in-place order (~0–1 patient per day before the pandemic compared to 10–16 patients per day after the pandemic, Fig. 1).
Fig. 1.
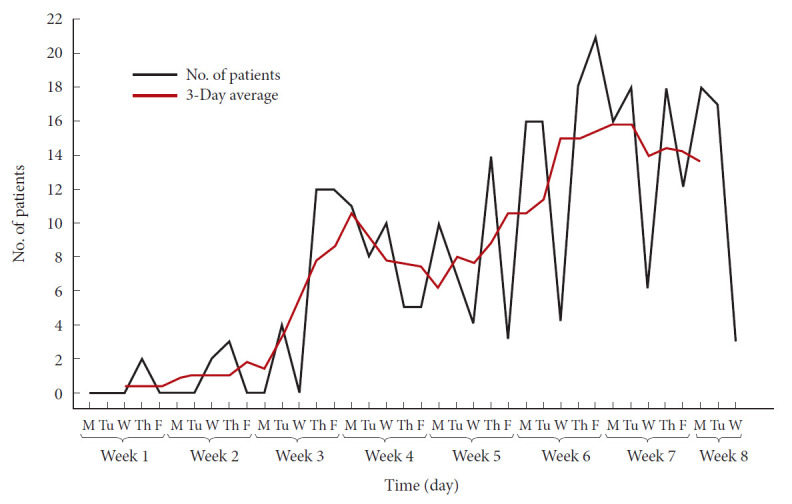
Line graph of video visits at our spine surgery clinic in the weeks following the city-mandated shelter-in-place order. Daily video visits (thin black line) and the 3-day video visit moving average are shown (thick red line).
2. Delphi Method
Fig. 2 highlights the results of the first round of the Delphi method. In the first round, 5 statements pertained to the upper extremity, 5 to the lower extremity, and 1 to the use of a weight in the exam. More specifically, statement 1 established that the physical exam should be performed with a known item with a standardized weight. Statements 2–6 described strength testing of the upper extremities, specifically the deltoids, biceps, triceps, wrist extension, grip, and hand intrinsic muscles, respectively. Statements 6–11 then pertained to strength testing of the lower extremities, specifically the iliopsoas, quadriceps, hamstrings, foot dorsiflexion, and foot plantar flexion, respectively. Following completion of the first round, statements 2, 4, 6, and 8 failed to reach consensus (p = 0.031, p = 0.031, p = 0.003, and p = 0.03, respectively).
Fig. 2.

Percentage of agreement on Delphi consensus statements regarding spine physical exam maneuvers in round 1 (A) and round 2 (B). The consensus threshold was 80% (red dashed line); 95% consensus, used as an expected outcome in 2 tailed binomial testing of significant disagreement, is indicated by the green dashed line. The green asterisk indicates statements that had significant disagreement.
We subsequently progressed to the second round of the Delphi method. First, we modified the statements that did not achieve consensus and resubmitted those statements to the panel. We found that the majority of the disagreement in the first round involved how to grade strength using the known object; specifically, that a 5/5 full strength exam is not possible to test over telemedicine. With that feedback, we created new statement that defined strength grading on a 4-point scale (0, no movement; 1, movement not against gravity; 3, movement against gravity; and 4, movement against resistance, and modified the strength testing of muscle groups accordingly (Fig. 2B). After this modification, all statements achieved consensus.
Finally, we used the consensus statements from the Delphi rounds to create the finalized protocol (Fig. 3). This protocol fits on one printed page and can be used by the surgeon or advanced practitioner when completing the muscle strength physical examination over telemedicine.
Fig. 3.

A consensus-based tele-strength examination as a result of our modified Delphi method. UCSF, University of California, San Francisco.
In addition to the spine-specific motor physical examination, we also list in Table 1 a standard neurological examination. The examination techniques were extracted from both neurosurgery and neurology publications [6-9,12]. We utilized these results and clinical experience to produce a template for a general telemedicine neurologic exam in neurosurgical patients (Table 1). The general neurological examination should be used to supplement the motor examination (Fig. 3) as needed. Fig. 4 depicts a simulated patient example of the spine telemedicine motor examination being performed over an audio/visual communication system.
Table 1.
A standard tele-neurologic examination
| Exam component | Assessment strategy and comments | |
| Mental status | Can use normal examination methods | |
| Cranial nerves | ||
| II | Visual fields: can be evaluated using a shared screen or with the aid of an assistant. | |
| Visual acuity: can be measured with the aid of an assistant and/or the use of a pocket Snellen card. Online tools to measure visual acuity are available, but not yet validated. [49] | ||
| Fundoscopic exam: currently difficult to accurately performed without an assistant. Can be reported by a trained assistant. New technologies allow assistant to send picture of fundoscopic exam directly to the neurosurgeon. [50] At-home technologies for fundoscopic exams are similarly in development. [51] | ||
| III, IV, VI | EOM: can instruct patient which directions to look and observe eyes for deficits or nystagmus. Can also have patient fix eyes on camera and move head from side to site. | |
| Pupillary response: can have patient move eye closer to screen and observe response to light. If assistant is present, this can also be performed by assistant with response observed by neurosurgeon. Smart phone based technologies for measurement of pupillary light reflex are accurate, but still under development. [52] | ||
| V | Facial sensation: can ask the patient to self-assess, although assistant help is required to accurately perform. | |
| VII | Facial strength: can assess symmetry and gross movements of the face on video. | |
| VIII | Hearing: can grossly assess. | |
| IX and X | Palate: can grossly evaluate palate and phonation of patient. | |
| XI | Shoulder shrug: can assess symmetry of shoulder shrug on video. | |
| XII | Tongue: can assess that tongue is midline on video examination. | |
| Motor | ||
| Upper extremities | Strength: see Fig. 3 for consensus-driven strength exam | |
| Lower extremities | Strength: see Fig. 3 for consensus-driven strength exam | |
| Straight leg raise: an assistant can aid by passively raising the leg while observed by the neurosurgeon with moderate accuracy. [53] The patient can also be asked to raise their own leg 20 cm above the table, with any changes in breathing counted as a positive exam. This has demonstrated good reliability. [54] | ||
| Tone | Tone can be difficult to assess over telemedicine modalities, although it is possible to grossly assess. An assistant with the patient can also provide some insight into tone, albeit with poor reliability. | |
| Reflexes | Reflexes can be difficult to assess without a trained assistant. The patient or an untrained assistant can be taught how to assess plantar response while observed by neurosurgeon. | |
| Sensation | Frequently requires an assistant with the patient. Often possible to instruct an untrained assistant through a basic sensory examination. The patient can also roughly self-assess how they have been experiencing sensation in day-to-day life. | |
| Cerebellar function | Can ask patient to perform heel to shin test and rapid alternating movements while observed. Can observe patient’s gait and ask them to tandem walk if in a safe situation. | |
| Additional spine-specific components | ||
| Assessment of pain/disability | Disability and health-related quality of life: the Oswestry Disability Index and 12-item Short Form health survey can be used to measure disability successfully through telemedicine technologies. [54] | |
| Pain: a visual analogue scale and Tampa Scale of Kinesiophobia can both be successfully administered over during a telemedicine visit with good reliability. [54] | ||
| Range of motion | Spinal range of motion can be observed by directing the patient through specific maneuvers and asking them bend/twist as far as possible. Studies have shown the assessment of lumbar lateral flexion range of motion to have acceptable reliability when performed in this manner. [54] | |
Fig. 4.

A simulated patient example of the spine telemedicine motor exam performed over an audio/visual communication modality.
DISCUSSION
1. Overview of Telemedicine in Surgical and Neurosurgical Clinical Practice
Routine outpatient visits, including preoperative assessment and monitoring of chronic conditions, are key areas in which telemedicine has been shown to be safe, time-saving, and cost effective. One of the leaders of telemedicine in the United States, the Department of Veterans Affairs (VA) has highlighted the applicability of telemedicine technologies for routine outpatient visits beginning in the 1990s, with continued growth since that time [13]. However, there is limited published data from the VA on their telemedicine experience with regard to surgical subspecialties. A 2018 pilot study investigating the use of telemedicine by the Connecticut VA plastic surgery department demonstrated high patient satisfaction among 41 patients who were seen using telemedicine technology [14]. Beyond the VA, preoperative assessment of patients via telemedicine has been shown to be accurate with regards to diagnosis and treatment planning in both pediatric surgery [15] and oral and maxillofacial surgery [16] with no significant difference in outcomes and reduced cost. Studies within neurology have also demonstrated the feasibility of telemedicine in the evaluation and monitoring of neurologic diseases such as epilepsy [17], movement disorders [18,19], and dementia [20,21].
While literature regarding nonneurosurgical subspecialties and neurology is more plentiful, the application of telemedicine has also been sparsely described in the neurosurgical literature. James [22] describes their experience with the formation of a pediatric neurosurgical telemedicine clinic for routine outpatient visits from 2011–2016. Subsequent analysis of the clinic’s socioeconomic impact revealed significant time and cost savings in excess of $233 per family [23]. Similarly, Mendez et al. [24] highlighted the feasibility of using a remote-presence robot for the programming of neuromodulation devices, with comparable outcomes relative to in-person visits. While the described studies are promising, additional investigations evaluating cost and clinical outcomes associated with telemedicine for outpatient care across neurosurgical subspecialties are needed.
Telemedicine technologies have also been described in the routine postoperative care of patients across surgical subspecialties for over a decade [25]. Studies from urology [26] to orthopedic surgery [27]. have demonstrated equivalent or improved efficacy and safety of telemedicine visits when compared to those in the clinic. A systematic review of telemedicine in postsurgical care found a slight increase in complications with telemedicine use (2.8% [7 of 254] vs. 0.4% [1 of 242]); however, there was also no significant difference in postoperative complications in any individual study [25]. Studies performed specifically within neurosurgery have also demonstrated the safety and cost-effectiveness of telemedicine in postoperative care [28-31]. International studies have also demonstrated reduced travel time, cost-effectiveness, and cost-saving associated with the use of Skype teleconferences (Skype Technologies S.A.R.L, Luxembourg City, Luxembourg) in the postoperative management of patients [28,31]. It is also possible that simple postoperative procedures, such as suture removal [32], may be directed using telemedicine, although further investigation is needed.
2. Financial and Legal Considerations
Prior to the COVID-19 pandemic, the use of telehealth in the United States was limited by concerns regarding reimbursement as well as federal and state regulations surrounding patient privacy, physician licensure, and liability [1,3]. There was confusion regarding what constituted a “tele-visit” as well, with different definitions, coding requirements and reimbursement rates for provider-patient electronic communication. As an example, Table 2 shows traditional current procedural terminology codes associated with telephonic, patient-initiated interactions. As providers seek to adapt to the pandemic, the HHS has expanded telemedicine coverage and relaxed regulations surrounding telemedicine in an effort to increase patient access to care without the need to travel to a health care facility [4,33,34]. While the regulatory situation remains fluid, there have been key changes that affect the clinical practice of neurosurgery.
Table 2.
Traditional telephonic CPT codes
| CPT code | Description |
|---|---|
| 99441 | 5–10 Minutes of medical discussion |
| 99442 | 11–20 Minutes of medical discussion |
| 99443 | 21–30 Minutes of medical discussion |
CPT, current procedural terminology.
A turning point in the use of telemedicine modalities for clinical care was the President’s initial declaration of a public health emergency on January 31st, 2020. Subsequently, the federal government, including the HHS and CMS began implementing policies to increase access to telehealth visits for patients. Early changes targeted the coverage of telemedicine, including telehealth visits (defined as using synchronous audio and video technologies to replace visits that usually occur in-person), Virtual Check-Ins (brief communication, including over a telephone, usually patient-initiated but can also be initiated by the provider), and E-Visits (non-face-to-face patient-initiated communications via online patient portal) (Table 3 [33]). Historically, Medicare telehealth visits and virtual check-ins were limited to established patients in rural settings, with restrictions on the frequency of visits [35,36].
Table 3.
Telehealth appointment types
| CPT code | Description |
|---|---|
| Face-to-face | |
| 99201-99205 | Outpatient new patient encounter |
| 99211-99215 | Outpatient established patient encounter |
| 99231-99233 | Subsequent hospital care |
| 99354-99357 | Prolonged service office/inpatient |
| Non-face-to-face | |
| G2012 | Brief technology-based assessment 5–10 minutes, “virtual check-in” |
| 99421-99423 | Online digital evaluation and management through online portal |
CPT, current procedural terminology.
Initially, coverage was not extended to telehealth visits with patients in their own homes [35]. On March 6, 2020, however, CMS expanded coverage for telehealth via an 1,135 waiver. The waiver removed geographic and visit frequency restrictions on reimbursement. In addition, coverage was expanded to a variety of office and hospital visits performed via telehealth technologies, including visits with patients at their homes, with equal reimbursement as a regular in-person visit. Also included in this waiver are initial patient evaluations in the hospital and emergency department as well as observation status, which previously were not eligible for telehealth coding and payment. This applies to both new and established patients for the duration of the COVID-19 public health emergency [33]. Although many private insurance payers have follow suit with similar policies, there remains variability in reimbursement guidelines between private insurance plans as well as from state to state Medicaid programs. Nevertheless, the actions taken by CMS with regards to telehealth visit reimbursements have increased the financial viability of using these technologies for patient care. It is unknown how long these waivers will last once the COVID pandemic has resolved but there has been a dramatic surge in their popularity during this crisis [33].
In an effort to increase telehealth accessibility, the Office for Civil Rights at HHS has determined that essentially any patient-facing audio/visual communication method (e.g., Zoom, Skype, Apple FaceTime) can be used for telehealth visits. While these modalities are not considered Health Insurance Portability and Accountability Act compliant by HHS, the agency has temporarily suspended enforcement of noncompliance with these rules. However, this exemption does not include the use of public facing modalities (e.g., TikTok, Facebook Live) [37]. Similarly, Medicare and Medicaid licensure requirements have been relaxed. Thus, physicians can practice, including telehealth visits, outside of the state they are licensed in, although state-specific regulations should be considered as well [38]. The Drug Enforcement Administration has also reduced restrictions, allowing providers to prescribe medications following a telehealth visit [39]. While these policies increase patient and physician access to telehealth visits, their long-term fate and the liability to the physician remain to be determined.
As the use of telemedicine visits grows, so to have concerns regarding associated physician malpractice and liability [40]. Fogel and Kvedar [41] performed a search of legal databases for medical malpractice suits associated with direct-to-consumer telemedicine and found no cases. This is likely due to the relatively low numbers of telemedicine visits [41,42]. Additionally, telehealth visits frequently involve outpatient visits that have relatively low malpractice risk [41,43]. Nevertheless, telehealth-specific malpractice considerations include the need for informed consent of the patient as well as ensuring the security and privacy of communication devices [43,44]. Measures to increase the security of a telemedicine visit vary depending on the service being used, but include the use of a password to access the visit, disallowing participants to join before the host, utilization of a virtual waiting room and preventing additional users from joining the visit once it has started. In addition, physicians should consider that essentially any telecommunication with a patient, regardless of how short, is considered professional advice [45] and establishes the patient-physician relationship, a requisite for professional liability. Thus, while telemedicine does not currently seem to be associated with increased rates of malpractice suits, neurosurgeons should take adequate precautions as we continue to learn more about telehealth practice.
3. Limitations
The most significant limitations of the protocol in Fig. 3 are (1) development at a single-center and (2) lack of prospective validation of this technique. However, given the highly extenuating circumstances involving the COVID-19 pandemic, the use of telemedicine is rapidly rising. It is thus useful to compare institutional protocols during this time, leaving the prospective validation of such protocols to future studies. Similarly, the general tele-neurologic exam in Table 1 requires additional validation, especially as cranial nerve abnormalities can be subtle and difficult to detect over visual/audio communication systems. Rather, Table 1 should serve as a guide to the literature surrounding general tele-neurologic exam maneuvers to supplement our consensus bases tele-strength protocol (Fig. 3) as needed. Despite these limitations, we believe the standardized physical examination maneuvers in our tele-neurologic examination and tele-strength protocols can act as a template for neurosurgical providers in their telehealth clinics, improving the efficacy and reliability of their tele-physical exams. To our knowledge, this is the first study to provide a consensus-based tele-strength examination.
However, there remains paucity of neurosurgical specific data surrounding the clinical applicability of these technologies as well as the performance and reliability of the tele-neurologic exam; additional research is required to determine best practices, including the sensitivity and specificity of telehealth-specific examination maneuvers. As a result, telemedicine examinations should still be interpreted with caution as their ability to replicate in-person findings has not been fully elucidated. Telemedicine is a newer modality of patient care, especially for spine surgeons, and does not completely replace in-clinic visits at this time. Rather, it should be used in the appropriate clinical scenarios, such as low-risk outpatient visits, and to protect patients from the risk associated with in-person visits to health care facilities. Future studies providing guidelines surrounding which types of patient visits are most amenable to telemedicine are warranted. Patient feedback on telemedicine visits should also be gathered and incorporated into clinical practice. Despite these limitations, telemedicine for neurosurgery will likely continue to play a role in the care of patients even after the COVID-19 pandemic has resolved, particularly as technologies continue to improve. Exciting future applications include telepathology [46], tele-surgical collaboration [47], and even the remote performance of surgical procedures [48].
CONCLUSION
We present a standardized tele-neurological examination and consensus-based tele-strength examination that was created using a formalized Delphi method to build consensus among a panel of spine neurological surgeons. We also provide a brief overview of the clinical evidence surrounding telehealth visits in neurosurgery as well as financial and legal considerations to aid neurosurgeons venturing into telehealth practice.
Footnotes
The authors have nothing to disclose.
REFERENCES
- 1.Tuckson RV, Edmunds M, Hodgkins ML. Telehealth. N Engl J Med. 2017;377:1585–92. doi: 10.1056/NEJMsr1503323. [DOI] [PubMed] [Google Scholar]
- 2.Rockville (MD): Health Resources & Services Administration; Telehealth programs [Internet] [cited 2020 Apr 8]. Available from: https://www.hrsa.gov/about/contact/index.html. [Google Scholar]
- 3.Kahn EN, La Marca F, Mazzola CA. Neurosurgery and telemedicine in the United States: assessment of the risks and opportunities. World Neurosurg. 2016;89:133–8. doi: 10.1016/j.wneu.2016.01.075. [DOI] [PubMed] [Google Scholar]
- 4.United States Department of Health and Human Services . Secretary Azar announces historic expansion of telehealth access to combat COVID-19. Washington, DC: United States Department of Health and Human Services; 2020. [Google Scholar]
- 5.Opening up America again. Washington, DC: The White House; 2020. [Google Scholar]
- 6.Craig JJ, McConville JP, Patterson VH, et al. Neurological examination is possible using telemedicine. J Telemed Telecare. 1999;5:177–81. doi: 10.1258/1357633991933594. [DOI] [PubMed] [Google Scholar]
- 7.Meyer BC, Lyden PD, Al-Khoury L, et al. Prospective reliability of the STRokE DOC wireless/site independent telemedicine system. Neurology. 2005;64:1058–60. doi: 10.1212/01.WNL.0000154601.26653.E7. [DOI] [PubMed] [Google Scholar]
- 8.Kane RL, Bever CT, Ehrmantraut M, et al. Teleneurology in patients with multiple sclerosis: EDSS ratings derived remotely and from hands-on examination. J Telemed Telecare. 2008;14:190–4. doi: 10.1258/jtt.2008.070904. [DOI] [PubMed] [Google Scholar]
- 9.Awadallah M, Janssen F, Körber B, et al. Telemedicine in general neurology: interrater reliability of clinical neurological examination via audio-visual telemedicine. Eur Neurol. 2019;80:289–94. doi: 10.1159/000497157. [DOI] [PubMed] [Google Scholar]
- 10.Okoli C, Pawlowski SD. The Delphi method as a research tool: an example, design considerations and applications. Inf Manag. 2004;42:15–29. [Google Scholar]
- 11.Eubank BH, Mohtadi NG, Lafave MR, et al. Using the modified Delphi method to establish clinical consensus for the diagnosis and treatment of patients with rotator cuff pathology. BMC Med Res Methodol. 2016;16:56. doi: 10.1186/s12874-016-0165-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Darby JM, Shutter LA, Elmer J, et al. Reliability of the telemedicine examination in the neurologic diagnosis of death. Neurol Clin Pract. 2021;11:13–7. doi: 10.1212/CPJ.0000000000000798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Veazie S, Bourne D, Peterson K, et al. Evidence brief: video telehealth for primary care and mental health services. Washington (DC): Department of Veterans Affairs (US); 2019. [PubMed] [Google Scholar]
- 14.Douglas S, Geiger E, McGregor A, et al. Telehealth in plastic surgery: a veterans affairs hospital perspective. Plast Reconstr Surg Glob Open. 2018;6:e1840. doi: 10.1097/GOX.0000000000001840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Postuma R, Loewen L. Telepediatric surgery: capturing clinical outcomes. J Pediatr Surg. 2005;40:813–8. doi: 10.1016/j.jpedsurg.2005.01.049. [DOI] [PubMed] [Google Scholar]
- 16.Wood EW, Strauss RA, Janus C, et al. Telemedicine consultations in oral and maxillofacial surgery: a follow-up study. J Oral Maxillofac Surg. 2016;74:262–8. doi: 10.1016/j.joms.2015.09.026. [DOI] [PubMed] [Google Scholar]
- 17.Ahmed SN, Mann C, Sinclair DB, et al. Feasibility of epilepsy follow-up care through telemedicine: a pilot study on the patient’s perspective. Epilepsia. 2008;49:573–85. doi: 10.1111/j.1528-1167.2007.01464.x. [DOI] [PubMed] [Google Scholar]
- 18.Dorsey ER, Deuel LM, Voss TS, et al. Increasing access to specialty care: a pilot, randomized controlled trial of telemedicine for Parkinson’s disease. Mov Disord. 2010;25:1652–9. doi: 10.1002/mds.23145. [DOI] [PubMed] [Google Scholar]
- 19.Achey M, Aldred JL, Aljehani N, et al. The past, present, and future of telemedicine for Parkinson’s disease. Mov Disord. 2014;29:871–83. doi: 10.1002/mds.25903. [DOI] [PubMed] [Google Scholar]
- 20.Loh PK, Ramesh P, Maher S, et al. Can patients with dementia be assessed at a distance? The use of Telehealth and standardised assessments. Intern Med J. 2004;34:239–42. doi: 10.1111/j.1444-0903.2004.00531.x. [DOI] [PubMed] [Google Scholar]
- 21.Wechsler LR. Advantages and limitations of teleneurology. JAMA Neurol. 2015;72:349–54. doi: 10.1001/jamaneurol.2014.3844. [DOI] [PubMed] [Google Scholar]
- 22.James HE. Pediatric neurosurgery telemedicine clinics: a model to provide care to geographically underserved areas of the United States and its territories. J Neurosurg Pediatr. 2016;18:753–7. doi: 10.3171/2016.6.PEDS16202. [DOI] [PubMed] [Google Scholar]
- 23.Hayward K, Han SH, Simko A, et al. Socioeconomic patient benefits of a pediatric neurosurgery telemedicine clinic. J Neurosurg Pediatr. 2020;25:204–8. doi: 10.3171/2019.8.PEDS1925. [DOI] [PubMed] [Google Scholar]
- 24.Mendez I, Song M, Chiasson P, et al. Point-of-Care programming for neuromodulation. Neurosurgery. 2013;72:99–108. doi: 10.1227/NEU.0b013e318276b5b2. [DOI] [PubMed] [Google Scholar]
- 25.Gunter RL, Chouinard S, Fernandes-Taylor S, et al. Current Use of telemedicine for post-discharge surgical care: a systematic review. J Am Coll Surg. 2016;222:915–27. doi: 10.1016/j.jamcollsurg.2016.01.062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Viers BR, Lightner DJ, Rivera ME, et al. Efficiency, satisfaction, and costs for remote video visits following radical prostatectomy: a randomized controlled trial. Eur Urol. 2015;68:729–35. doi: 10.1016/j.eururo.2015.04.002. [DOI] [PubMed] [Google Scholar]
- 27.Sathiyakumar V, Apfeld JC, Obremskey WT, et al. Prospective randomized controlled trial using telemedicine for follow-ups in an orthopedic trauma population: a pilot study. J Orthop Trauma. 2015;29:e139–45. doi: 10.1097/BOT.0000000000000189. [DOI] [PubMed] [Google Scholar]
- 28.Dadlani R, Mani S, Jai JG, et al. The impact of telemedicine in the postoperative care of the neurosurgery patient in an outpatient clinic: a unique perspective of this valuable resource in the developing world - an experience of more than 3000 teleconsultations. World Neurosurg. 2014;82:270–83. doi: 10.1016/j.wneu.2014.05.027. [DOI] [PubMed] [Google Scholar]
- 29.Reider-Demer M, Raja P, Martin N, et al. Prospective and retrospective study of videoconference telemedicine follow-up after elective neurosurgery: results of a pilot program. Neurosurg Rev. 2018;41:497–501. doi: 10.1007/s10143-017-0878-0. [DOI] [PubMed] [Google Scholar]
- 30.Snyder SR. Telemedicine for elective neurosurgical routine follow-up care: a promising patient-centered and cost-effective alternative to in-person clinic visits. Neurosurg Focus. 2018;44:E18. doi: 10.3171/2018.2.FOCUS1889. [DOI] [PubMed] [Google Scholar]
- 31.Thakar S, Rajagopal N, Mani S, et al. Comparison of telemedicine with in-person care for follow-up after elective neurosurgery: results of a cost-effectiveness analysis of 1200 patients using patient-perceived utility scores. Neurosurg Focus. 2018;44:E17. doi: 10.3171/2018.2.FOCUS17543. [DOI] [PubMed] [Google Scholar]
- 32.Tofte JN, Anthony CA, Polgreen PM, et al. Postoperative care via smartphone following carpal tunnel release. J Telemed Telecare. 2020;26:223–31. doi: 10.1177/1357633X18807606. [DOI] [PubMed] [Google Scholar]
- 33.Centers for Medicare & Medicaid Services . Woodlawn, Baltimore County (MD): Centers for Medicare & Medicaid Services; Physicians and other clinicians: CMS flexibilities to fight COVID-19 [Internet] [cited 2020 Apr 18]. Available from: https://www.endocrine.org/-/media/endocrine/files/membership/cms--covid-phys-fact-sheet.pdf. [Google Scholar]
- 34.Baltimore (MD): Centers for Medicare & Medicaid Services; President Trump expands telehealth benefits for edicare beneficiaries during COVID-19 outbreak [Internet] [cited 2020 Apr 18]. Available from: https://www.cms.gov/newsroom/press-releases/president-trump-expands-telehealth-benefits-medicare-beneficiaries-during-covid-19-outbreak. [Google Scholar]
- 35.Gilman M, Stensland J. Telehealth and medicare: payment policy, current use, and prospects for growth. Medicare Medicaid Res Rev. 2013;3:mmrr.003.04.a04. doi: 10.5600/mmrr.003.04.a04. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Horton K, Malcarney MB, Seiler N. Medicare payment rules and telemedicine. Public Health Rep. 2014;129:196. [Google Scholar]
- 37.Washington, DC: United States Department of Health and Human Services; Notification of enforcement discretion for telehealth remote communications during the COVID-19 nationwide public health emergency [Internet] [cited 2020 Apr 18]. Available from: https://www.hhs.gov/hipaa/for-professionals/special-topics/emergency-preparedness/notification-enforcement-discretion-telehealth/index.html. [Google Scholar]
- 38.Washington, DC: United States Department of Health and Human Services; Waiver or modification of requirements under section 1135 of the social security act [Internet] [cited 2020 Apr 18]. Available from: https://www.phe.gov/emergency/news/healthactions/section1135/Pages/covid19-13March20.aspx. [Google Scholar]
- 39.Arlington (VA): Drug Enforcement Administration; COVID-19 Information Page [Internet] [cited 2020 Apr 18]. Available from: https://www.deadiversion.usdoj.gov/coronavirus.html. [Google Scholar]
- 40.Jena AB, Seabury S, Lakdawalla D, et al. Malpractice risk according to physician specialty. N Engl J Med. 2011;365:629–36. doi: 10.1056/NEJMsa1012370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Fogel AL, Kvedar JC. Reported cases of medical malpractice in direct-to-consumer telemedicine. JAMA. 2019;321:1309–10. doi: 10.1001/jama.2019.0395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Jena AB, Chandra A, Lakdawalla D, et al. Outcomes of medical malpractice litigation against US physicians. Arch Intern Med. 2012;172:892–4. doi: 10.1001/archinternmed.2012.1416. [DOI] [PubMed] [Google Scholar]
- 43.Nittari G, Khuman R, Baldoni S, et al. Telemedicine practice: review of the current ethical and legal challenges. Telemed J E Health. 2020;26:1427–37. doi: 10.1089/tmj.2019.0158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Kramer GM, Kinn JT, Mishkind MC. Legal, regulatory, and risk management issues in the use of technology to deliver mental health care. Cogn Behav Pract. 2015;22:258–68. [Google Scholar]
- 45.Rovit RL, Simon AS, Drew J, et al. Neurosurgical experience with malpractice litigation: an analysis of closed claims against neurosurgeons in New York State, 1999 through 2003. J Neurosurg. 2007;106:1108–14. doi: 10.3171/jns.2007.106.6.1108. [DOI] [PubMed] [Google Scholar]
- 46.Horbinski C, Fine JL, Medina-Flores R, et al. Telepathology for intraoperative neuropathologic consultations at an academic medical center: a 5-year report. J Neuropathol Exp Neurol. 2007;66:750–9. doi: 10.1097/nen.0b013e318126c179. [DOI] [PubMed] [Google Scholar]
- 47.Shenai MB, Tubbs RS, Guthrie BL, et al. Virtual interactive presence for real-time, long-distance surgical collaboration during complex microsurgical procedures: technical note. J Neurosurg. 2014;121:277–84. doi: 10.3171/2014.4.JNS131805. [DOI] [PubMed] [Google Scholar]
- 48.Wirz R, Torres LG, Swaney PJ, et al. An experimental feasibility study on robotic endonasal telesurgery. Neurosurgery. 2015;76:479–84. doi: 10.1227/NEU.0000000000000623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Yeung WK, Dawes P, Pye A, et al. eHealth tools for the self-testing of visual acuity: a scoping review. NPJ Digit Med. 2019;2:82. doi: 10.1038/s41746-019-0154-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Nazari Khanamiri H, Nakatsuka A, El-Annan J. Smartphone fundus photography. J Vis Exp. 2017;(125):55958. doi: 10.3791/55958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Holekamp NM. Moving from clinic to home: what the future holds for ophthalmic telemedicine. Am J Ophthalmol. 2018;187:xxviii–xxxv. doi: 10.1016/j.ajo.2017.11.003. [DOI] [PubMed] [Google Scholar]
- 52.McAnany JJ, Smith BM, Garland A, et al. iPhone-based pupillometry: a novel approach for assessing the pupillary light reflex. Optom Vis Sci. 2018;95:953–8. doi: 10.1097/OPX.0000000000001289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Truter P, Russell T, Fary R. The validity of physical therapy assessment of low back pain via telerehabilitation in a clinical setting. Telemed J E Health. 2014;20:161–7. doi: 10.1089/tmj.2013.0088. [DOI] [PubMed] [Google Scholar]
- 54.Palacín-Marín F, Esteban-Moreno B, Olea N, et al. Agreement between telerehabilitation and face-to-face clinical outcome assessments for low back pain in primary care. Spine (Phila Pa 1976) 2013;38:947–52. doi: 10.1097/BRS.0b013e318281a36c. [DOI] [PubMed] [Google Scholar]