

Abstract
Purpose:
To provide tobacco product use patterns for US adults by sociodemographic group.
Design:
A secondary analysis of Tobacco Use Supplement to the Current Population Survey (2014–15), National Health Interview Survey (2015), and Population Assessment of Tobacco and Health (2015–16).
Setting:
United States.
Sample:
Three nationally representative samples of adults (N = 28,070–155,067).
Measures:
All possible combinations of cigarette, Electronic Nicotine Delivery Systems (ENDS), other combustible product, and smokeless tobacco use, defined as current use every day or some days.
Analysis:
Weighted population prevalence and proportion among tobacco users of exclusive, dual, and polyuse patterns by sex, race/ethnicity, education, income, and age.
Results:
Exclusive cigarette use was the most prevalent pattern (10.9–12.8% of US population). Dual and polyuse were less prevalent at the population level (2.6–5.2% and 0.3–1.3%, respectively) but represented 16.7–25.5% of product use among tobacco users. Cigarette plus ENDS use was similar by sex, but men were more likely to be dual users of cigarettes plus other combustibles or smokeless tobacco. Among race/ethnic subgroups, non-Hispanic (NH) Whites were most likely to use cigarettes plus ENDS, while NH Blacks were most likely to use cigarettes plus other combustibles. Dual and polyuse were generally less common among adults with higher education, income, and age.
Conclusion:
Differences in product use patterns by sociodemographic group likely represent different risk profiles with important implications for resulting health disparities.
Keywords: polytobacco, patterns of tobacco use, multiple tobacco products, dual use, health disparities, inequities
Purpose
Tobacco use continues to be a leading behavioral risk factor for cancer, chronic disease, and premature death.1 As the tobacco market landscape rapidly changes, patterns of use, including dual use (use of 2 products) and polyuse (use of 3 or more products), are evolving. Although the long-term health consequences of dual and polyuse are not well understood,2,3 the concurrent use of multiple tobacco products influences nicotine dependence,4–7 frequency of product use,5,8,9 and cessation intentions.7,10
The majority of adult dual and polyuse consists of cigarette smoking in combination with one or more other tobacco products.11 Cigarette smokers may use non-combustible products, such as Electronic Nicotine Delivery Systems (ENDS) or smokeless tobacco, as a way to quit smoking.12–17 However, dual and polyuse have been linked to greater nicotine dependence than exclusive product use among adults4,5 and youth,6,7 potentially impacting cessation intentions and success.7,10 Moreover, cigarette smokers who are dual/polyusers may smoke as many or more cigarettes per day as exclusive cigarette smokers,5,8,9,18 thereby increasing their risk of poor health outcomes by using additional tobacco products.
Since tobacco products fall on a risk continuum,19 there are likely differential health effects for specific product combinations. Concurrent use of multiple combustible products, such as cigarettes and cigars, may be as or more hazardous than exclusive use of either product. Dual users of cigarettes and smokeless tobacco may be at greater risk of cardiovascular disease than exclusive cigarette smokers.20 Exclusive ENDS use may be less harmful than exclusive cigarette use,21 although there is controversy on the nature of these risks.22 Furthermore, ENDS and cigarette dual use likely presents a different risk profile than exclusive use of either product.
In addition, as there are well-established sociodemographic disparities in the use of specific tobacco products and related health outcomes,23 there are likely important differences in dual and polyuse by sex, race/ethnicity, socioeconomic status, and age. However, existing research on disparities in dual and polyuse among adults is subject to important limitations.2 Studies often do not distinguish between dual and polyuse or disaggregate product combinations by sociodemographic group,24–28 limiting our ability to measure the prevalence of specific product groupings and potential impact on health disparities. Importantly, given their relatively recent emergence, some recent studies on dual and polyuse do not include information on ENDS.27,28 Including ENDS is critical to capturing current patterns of multiple product use, as dual use of cigarettes plus ENDS was the most common product combination among adult tobacco users between 2012–20144,11 and is likely more common currently, given increasing ENDS use among young adults in recent years.29 Additionally, estimates of dual and polyuse that include ENDS provide important context for understanding evolving tobacco and nicotine product use patterns, particularly as youth, who increasingly use ENDS,30 age into adulthood.
Recent studies on sociodemographic differences in dual and polyuse employ a variety of surveys, including the National Survey on Drug Use and Health (NSDUH),27 National Adult Tobacco Survey (NATS),4,10 Population Assessment of Tobacco and Health (PATH),24 National Health Interview Survey (NHIS),28 and GfK’s KnowledgePanel.25,26 Although each of these surveys are designed to be nationally representative, prevalence estimates of tobacco product use obtained from each survey vary based on survey methodology.31,32 Moreover, the wide range of dual and polyuse definitions used across studies makes evidence summation challenging. The objective of this study is to provide recent US prevalence estimates of patterns of tobacco product use, including specific types of dual and polyuse, for US adults by sex, race/ethnicity, socioeconomic status, and age. To increase the utility of our estimates, we apply the same product use definitions to 3 large nationally representative surveys collected over a similar period, enabling us to produce a range of comparable national estimates of exclusive, dual, and polyuse.
Methods
Design
We used recent waves of 3 publicly available, nationally representative surveys: Tobacco Use Supplement to the Current Population Survey (TUS-CPS), 2014–2015; NHIS, 2015; and PATH, Wave 3 (2015–2016). Supplemental Table 1 compares methodology and tobacco product definitions for these surveys. We chose these waves to produce recent estimates that were temporally comparable across surveys. We did not include other national surveys with information on tobacco use because they lacked information on ENDS (NSDUH) or combustible products besides cigarettes (Behavioral Risk Factor Surveillance System), did not have sufficient sample size for stratified analysis by sociodemographic subgroup (National Health and Nutrition Examination Survey), or did not have data from the relevant time period (NATS).
Sample
Briefly, TUS-CPS is a cross-sectional survey of the civilian, non-institutionalized US population age 18 and older conducted by the US Census Bureau as a supplement to the Current Population Survey every 3–4 years beginning in 1992–1993.33 TUS-CPS respondents answer interviewer questions about tobacco use using either Computer Assisted Telephone Interviewing (CATI; about two-thirds of the sample) or Computer Assisted Personal Interviewing (CAPI). NHIS is a cross-sectional survey of US households and non-institutionalized group quarters conducted annually since 1960 by the National Center for Health Statistics at the Centers for Disease Control and Prevention.34 NHIS respondents answer interviewer questions on their health status and behaviors, including tobacco use, using CAPI. Although most NHIS surveys are conducted in-person, telephone interviews are used if the respondent requests a telephone interview, as a follow-up to complete an in-person interview, or when travel logistics make completing an in-person interview by the required deadline challenging.34 PATH is a longitudinal study of the civilian, non-institutionalized US population age 12 and older conducted by the National Institutes of Health and the Food and Drug Administration beginning in 2013–2014.35 PATH respondents directly enter answers to a series of detailed questions about tobacco use using Audio Computer-Assisted Self-Interviewing (ACASI). For this analysis, we selected the 2015–16 cross-sectional Wave 3 PATH survey and restricted the sample to age 18 and older.
Given the use of de-identified publicly available datasets, the University of Michigan Institutional Review Board deemed this project not regulated as human subjects research.
Measures
Following standard practice, we defined current cigarette smokers as respondents who had smoked at least 100 cigarettes in their lifetime (established use) and smoked cigarettes every day or some days at the time of the survey. For the remaining products (ENDS, traditional cigars, cigarillos, filtered cigars, tobacco pipe, hookah, snus, dissolvable tobacco, and other smokeless tobacco), we defined current use as use every day or some days. To differentiate patterns of products used, we classified products into 4 groups: cigarettes, ENDS, other combustibles (traditional cigars, cigarillos, filtered cigars, pipes, hookah), or smokeless tobacco (snus, dissolvable tobacco, other smokeless tobacco). These groupings are similar to the Tobacco Product Use Patterns (T-PUPs) model developed by El-Toukhy and Choi,36,37 who recommend 3 groups—cigarettes, non-cigarette combustibles, and non-combustibles (i.e., smokeless tobacco and ENDS)—to reflect a decreasing risk continuum from cigarettes to non-combustibles.19 Although some other combustible products, such as cigars, may be equally or more harmful than cigarettes,38 they are generally used less frequently than cigarettes,39 which is why they are placed in a separate category on the T-PUPs risk continuum.36 Kasza et al. used 3 different groupings to examine multiple product transitions: combustibles (i.e., cigarettes, cigars), ENDS, and other non-combustibles (i.e., smokeless).40 We used 4 product groupings (cigarettes, ENDS, other combustibles, and smokeless) because we felt it was important to separate cigarettes from other combustibles and ENDS from smokeless. Additionally, 4 groups still resulted in a manageable number of product combinations while providing sufficient sample size to examine dual and polyuse.
We created a mutually exclusive, 16 category patterns-of-use variable based on all possible combinations of our 4 product groupings, including non-use, exclusive product use, dual product use (2 product groups), or poly product use (3 or more products groups). Respondents who were missing information on the 16-category variable (due to missing information on current use of any of the 4 product groups) were excluded from the analysis (0.3% PATH; 1.6% TUS-CPS; 6.3% NHIS).
To examine sociodemographic differences, we included sex (male, female), race/ethnicity (non-Hispanic (NH) White, NH Black, NH Other, Hispanic), education (< high school, high school degree/GED, some college, college degree or higher), annual household income (<$50,000, $50,000–$99,999, $100,000+), and age (18–24, 25–34, 35–54, 55+). We restricted the education analysis to respondents age 25+ since 18–24 year-olds may not have had the opportunity to graduate from high school or college yet. We selected cut-points for education, income, and age based on common collapsed response categories in the 3 public datasets and strata sample size.
Analysis
For each survey, we calculated weighted prevalence of tobacco product use patterns both for the population overall and among tobacco users, accounting for the complex survey design of each sample. We stratified by sociodemographic subgroups to examine potential disparities across patterns of use. Among users of other combustibles, we also examined the proportion using each type of other combustible product to provide context for interpreting results within the other combustibles category. We did not provide a similar breakdown for the smokeless category since there were only 2 component questions in TUS and PATH and only a single question about smokeless products in NHIS. To assess the impact of our current use definition, we conducted a sensitivity analysis examining 3 additional current use definitions based on past 30 days use (1+, 10+ or 25+ days in the past 30 days).
For PATH, we used the Wave 3 single-wave weight to estimate weighted prevalence. For TUS-CPS, we combined the 3 samples taken between 2014–2015 and divided the resulting weights by 3 to estimate weighted prevalence.33 We used Balanced Repeated Replication with replicate weights for variance estimation for both PATH and TUS-CPS, with Fay’s adjustment set to 0.3.41 For NHIS, we used the Final Annual weight to estimate weighted prevalence and Taylor Series Linearization42 for variance estimation. Due to the large number of potential comparisons in prevalence of the 16 category patterns-of-use variable across 17 sociodemographic strata and 3 surveys, we used confidence interval overlap as a guide when assessing differences in point estimates. All analyses were conducted using Stata version 15.43
Results
TUS-CPS had the largest analytic sample size (n = 155,067), followed by NHIS (n = 31,680) and PATH (n = 28,070). Since all 3 surveys are nationally representative, the weighted distributions of sociodemographic characteristics were generally similar, with approximately 48% male, 70% aged 35 or older, and 65% NH White (Table 1). However, there were differences by socioeconomic status across surveys, with a higher weighted proportion of NHIS respondents in the highest income category compared to TUS-CPS and PATH.
Table 1.
Sample characteristics for the Tobacco Use Supplement to the Current Population Survey (2014–2015), National Health Interview Survey (2015), and Population Assessment of Tobacco and Health (2015–2016).
| TUS-CPS (n = 155,067) |
NHIS (n = 31,680) |
PATH (n = 28,070) |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 95% CI |
95% CI |
95% CI |
||||||||||
| n | % | LB | UB | n | % | LB | UB | n | % | LB | UB | |
| Sex | ||||||||||||
| Men | 69,355 | 48.1 | 48.0 | 48.2 | 14,198 | 48.3 | 47.5 | 49.0 | 13,741 | 47.9 | 47.8 | 48.0 |
| Women | 85,712 | 51.9 | 51.9 | 52.0 | 17,482 | 51.7 | 51.0 | 52.5 | 14,303 | 52.1 | 52.0 | 52.2 |
| Age group | ||||||||||||
| 18–24 | 10,483 | 13.0 | 12.9 | 13.0 | 2,747 | 12.5 | 11.8 | 13.2 | 8,435 | 12.4 | 12.2 | 12.6 |
| 25–34 | 25,359 | 17.7 | 17.7 | 17.7 | 5,409 | 17.4 | 16.8 | 18.1 | 5,813 | 17.5 | 17.0 | 18.1 |
| 35–54 | 53,464 | 34.2 | 34.1 | 34.2 | 10,137 | 34.1 | 33.3 | 34.9 | 7,748 | 33.3 | 32.6 | 34.0 |
| 55+ | 65,761 | 35.2 | 35.1 | 35.3 | 13,387 | 36.0 | 35.1 | 36.9 | 6,072 | 36.8 | 36.3 | 37.3 |
| Race/ethnicity | ||||||||||||
| Non-Hispanic White | 113,288 | 64.8 | 64.8 | 64.9 | 19,737 | 65.1 | 64.2 | 65.9 | 16,246 | 65.6 | 65.5 | 65.8 |
| Non-Hispanic Black | 15,451 | 11.7 | 11.6 | 11.7 | 4,092 | 11.5 | 10.9 | 12.1 | 4,060 | 11.2 | 11.1 | 11.3 |
| Hispanic | 16,370 | 15.6 | 15.6 | 15.7 | 5,262 | 15.7 | 15.0 | 16.4 | 5,226 | 15.5 | 15.4 | 15.6 |
| Non-Hispanic Other | 9,958 | 7.9 | 7.8 | 7.9 | 2,589 | 7.8 | 7.4 | 8.2 | 2,106 | 7.7 | 7.5 | 7.8 |
| Education level (25+ years of age) | ||||||||||||
| Less than high school diploma | 14,609 | 10.8 | 10.7 | 11.0 | 4,045 | 12.6 | 12.0 | 13.1 | 2,506 | 11.2 | 10.7 | 11.7 |
| High school diploma or GED | 40,334 | 27.0 | 26.8 | 27.3 | 7,098 | 23.9 | 23.2 | 24.7 | 5,258 | 27.4 | 26.8 | 27.9 |
| Some college | 40,560 | 27.4 | 27.3 | 27.6 | 8,573 | 29.2 | 28.5 | 30.0 | 6,514 | 30.2 | 29.6 | 30.8 |
| College degree | 49,081 | 34.7 | 34.5 | 35.0 | 9,089 | 34.3 | 33.3 | 35.2 | 5,274 | 31.3 | 30.9 | 31.7 |
| Household income level | ||||||||||||
| <$50,000 | 76,171 | 49.7 | 49.4 | 50.0 | 16,816 | 42.7 | 41.8 | 43.6 | 16,244 | 53.5 | 52.5 | 54.5 |
| $50,000–99,999 | 47,186 | 29.7 | 29.4 | 29.9 | 8,745 | 30.7 | 29.8 | 31.5 | 5,861 | 26.7 | 25.8 | 27.6 |
| $100,000+ | 31,710 | 20.7 | 20.4 | 20.9 | 6,119 | 26.7 | 25.7 | 27.6 | 3,910 | 19.8 | 18.8 | 20.8 |
| Patterns of tobacco/nicotine product use | ||||||||||||
| Non-user | 127,579 | 82.7 | 82.6 | 82.9 | 25,105 | 79.7 | 79.0 | 80.3 | 15,693 | 74.6 | 73.9 | 75.2 |
| Exclusive use | 23,119 | 14.4 | 14.2 | 14.5 | 5,271 | 16.4 | 15.8 | 17.0 | 8,906 | 18.9 | 18.4 | 19.5 |
| Cigarettes | 17,740 | 10.9 | 10.8 | 11.0 | 3,897 | 11.4 | 10.9 | 11.9 | 6,089 | 12.8 | 12.3 | 13.3 |
| ENDS | 1,014 | 0.7 | 0.6 | 0.7 | 317 | 1.3 | 1.1 | 1.4 | 726 | 1.4 | 1.3 | 1.6 |
| Other combustibles | 2,352 | 1.6 | 1.6 | 1.7 | 635 | 2.3 | 2.1 | 2.6 | 1,416 | 3.1 | 2.9 | 3.3 |
| Smokeless | 2,013 | 1.2 | 1.1 | 1.2 | 422 | 1.4 | 1.2 | 1.6 | 675 | 1.6 | 1.5 | 1.8 |
| Dual use | 3,937 | 2.6 | 2.5 | 2.6 | 1,147 | 3.4 | 3.2 | 3.7 | 2,715 | 5.2 | 4.9 | 5.4 |
| Cigarettes + ENDS | 2,142 | 1.3 | 1.3 | 1.4 | 543 | 1.6 | 1.4 | 1.8 | 904 | 1.8 | 1.7 | 2.0 |
| Cigarettes + other combustibles | 1,093 | 0.8 | 0.7 | 0.8 | 388 | 1.1 | 0.9 | 1.3 | 1,049 | 2.0 | 1.8 | 2.1 |
| Cigarettes + smokeless | 377 | 0.2 | 0.2 | 0.2 | 110 | 0.4 | 0.3 | 0.5 | 233 | 0.5 | 0.4 | 0.6 |
| ENDS + other combustibles | 122 | 0.1 | 0.1 | 0.1 | 31 | 0.1 | 0.1 | 0.2 | 366 | 0.6 | 0.5 | 0.7 |
| ENDS + smokeless | 41 | 0.0 | 0.0 | 0.0 | 12 | 0.0 | 0.0 | 0.1 | 35 | 0.1 | 0.0 | 0.1 |
| Other combustibles + smokeless | 162 | 0.1 | 0.1 | 0.1 | 63 | 0.2 | 0.1 | 0.3 | 128 | 0.2 | 0.2 | 0.3 |
| Polyuse | 432 | 0.3 | 0.3 | 0.3 | 157 | 0.5 | 0.4 | 0.7 | 756 | 1.3 | 1.2 | 1.4 |
| Cigarettes + ENDS + other combustibles | 229 | 0.2 | 0.1 | 0.2 | 89 | 0.3 | 0.2 | 0.4 | 416 | 0.7 | 0.6 | 0.8 |
| Cigarettes + ENDS + smokeless | 71 | 0.1 | 0.0 | 0.1 | 20 | 0.1 | 0.0 | 0.1 | 71 | 0.1 | 0.1 | 0.2 |
| Cigarettes + other combustibles + smokeless | 92 | 0.1 | 0.1 | 0.1 | 34 | 0.1 | 0.1 | 0.2 | 121 | 0.2 | 0.2 | 0.3 |
| ENDS + other combustibles + smokeless | 6 | 0.0 | 0.0 | 0.0 | 4 | 0.0 | 0.0 | 0.0 | 42 | 0.1 | 0.0 | 0.1 |
| All 4 groups | 34 | 0.0 | 0.0 | 0.0 | 10 | 0.0 | 0.0 | 0.1 | 106 | 0.2 | 0.1 | 0.2 |
n = unweighted sample size; % = weighted percentage.
LB = Lower Bound; UB = Upper Bound.
ENDS = Electronic Nicotine Delivery Systems.
Current use definitions: 100+ lifetime cigarettes and now smoke every day or some days; now use every day or some days for other products.
Missing patterns of tobacco product use information: TUS: 1.6% (n = 2,468); NHIS: 5.8% (n = 1,963); PATH: 0.3% (n = 78).
Overall Patterns of Exclusive, Dual, and Polytobacco Use
The population prevalence of tobacco use ranged from 17.3% in TUS-CPS to 25.4% in PATH (Table 1). Exclusive cigarette use was the most prevalent product use pattern across all 3 surveys (TUS-CPS 10.9%; NHIS 11.4%; PATH 12.8%), followed by exclusive use of other combustibles (TUS-CPS 1.6%; NHIS 2.3%; PATH 3.1%). Dual use ranged from 2.6% (TUS-CPS) to 5.2% (PATH) across surveys. In TUS-CPS and NHIS, the most common dual use pattern was cigarettes plus ENDS (1.3% and 1.6%, respectively), followed by cigarettes plus other combustibles (0.8% and 1.1%, respectively). Use of cigarettes plus other combustibles was slightly more prevalent than cigarettes plus ENDS in PATH (2.0% and 1.8%, respectively). Dual use combinations without cigarettes were rare across surveys (0.2–0.9%), as was polyuse (0.3–1.3%). Among tobacco users, exclusive product use represented the majority of use across surveys (74.5–83.3%; Supplemental Table 2). However, dual and polyuse combined accounted for 16.7–25.5% of product use among tobacco users.
Patterns of Exclusive, Dual, and Polytobacco Use by Sociodemographic Subgroup
The population prevalence of exclusive cigarette use was higher for men than women in TUS-CPS, but similar for men and women in NHIS and PATH (Figure 1, Supplemental Table 3a). For example, in NHIS, 11.5% of men exclusively smoked cigarettes versus 11.2% of women. Across surveys, the population prevalence of exclusive ENDS use, exclusive other combustible use, and exclusive smokeless tobacco use was higher for men than women. Men were also more likely to be dual users of cigarettes plus other combustibles or cigarettes plus smokeless tobacco than women. The prevalence of cigarettes plus ENDS dual use was similar by sex (1.2–1.9% across surveys for both men and women), although it accounted for a higher proportion of tobacco use among female (9.7–10.6%) vs. male tobacco users (5.5–6.7%; Supplemental Table 3b). The prevalence of polyuse, which mostly consisted of concurrent use of cigarettes with 2 or more other products, was higher among men than women.
Figure 1.
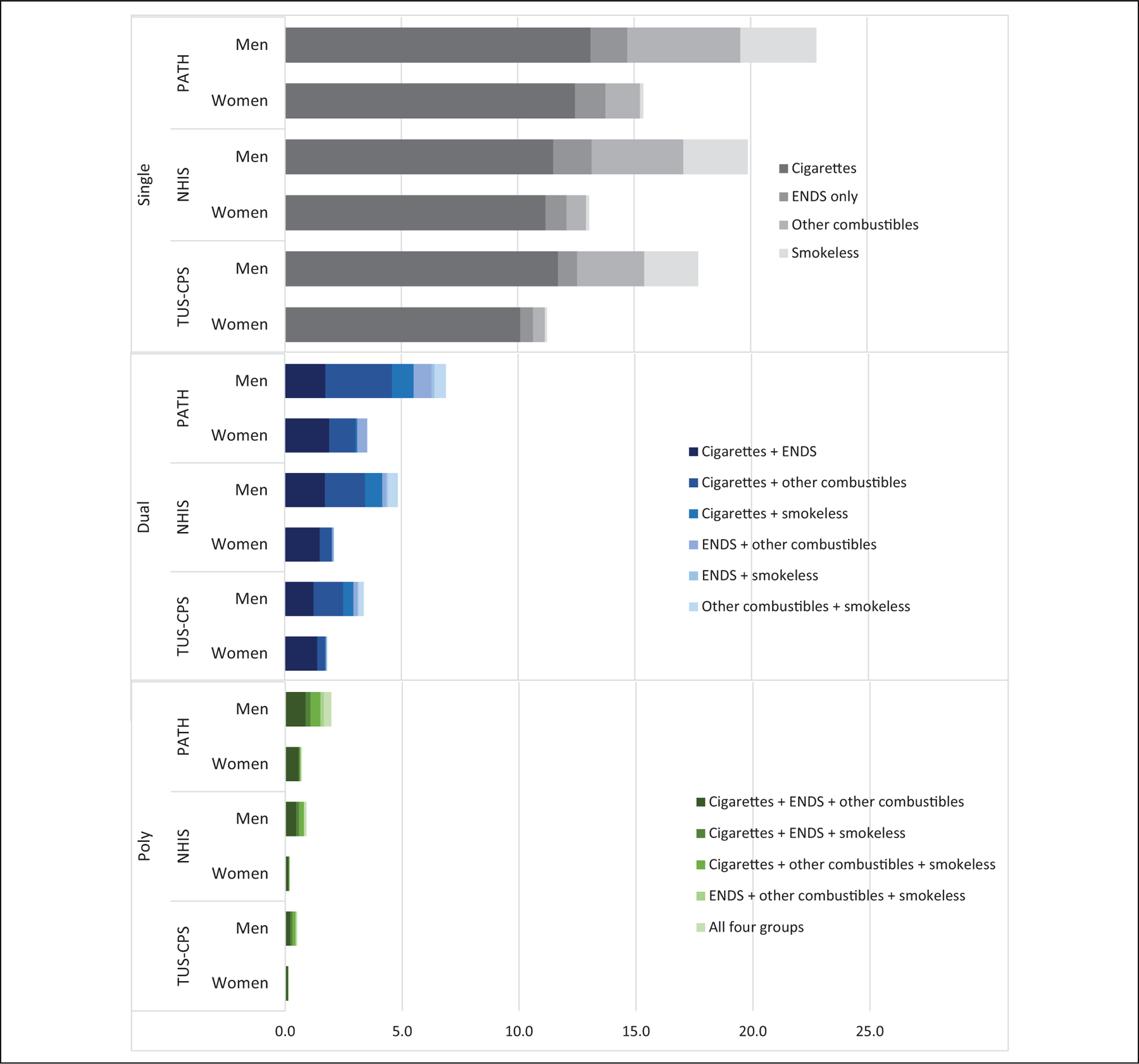
Population prevalence of single, dual, and polytobacco use by sex: TUS-CPS (2014–2015), NHIS (2015), and PATH (2015–2016).
Racial/ethnic patterns of tobacco product use were generally consistent across surveys, with slight differences in exclusive cigarette use (Figure 2, Supplemental Table 4a). Although the population prevalence of exclusive cigarette use was higher among NH Black individuals in PATH (16.3% vs. 13.1% among NH White individuals), prevalence estimates were similar for NH Black and NH White individuals in TUS-CPS (12.1% vs. 11.8%, respectively) and NHIS (12.9% vs. 12.3%, respectively). Exclusive use of the remaining product groups (ENDS, other combustibles, and smokeless tobacco) and dual use of these products with cigarettes followed similar patterns by race/ethnicity. Compared to NH Black and Hispanic individuals, NH White individuals generally had the highest prevalence of exclusive ENDS use and cigarette plus ENDS dual use in all 3 surveys. Similarly, NH White individuals had the highest prevalence of both exclusive smokeless tobacco use and cigarette plus smokeless tobacco dual use. NH Black individuals had the highest prevalence of exclusive use of other combustibles and cigarette plus other combustibles dual use. In TUS-CPS and NHIS, NH White individuals had a slightly higher prevalence of polyuse (0.4% and 0.7%) than NH Black (0.2% and 0.1%) and Hispanic individuals (0.2% and 0.2%, respectively). There were no clear differences in polyuse prevalence by race/ethnic groups in PATH (1.2–1.4%).
Figure 2.
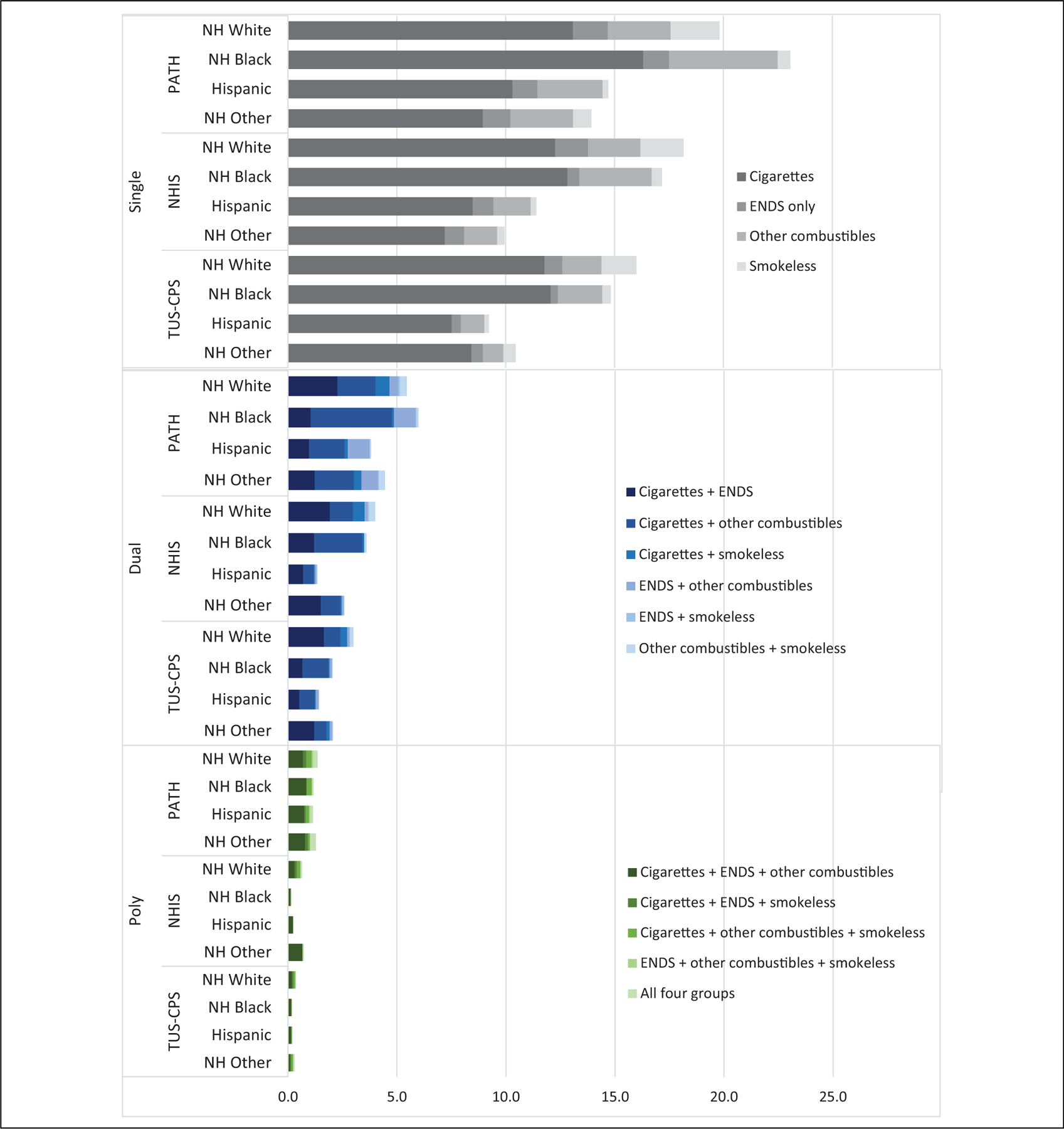
Population prevalence of single, dual, and polytobacco use by race/ethnicity: TUS-CPS (2014–2015), NHIS (2015), and PATH (2015–2016). NH = Non-Hispanic.
Patterns of tobacco product use were similar across surveys by education level (Figure 3, Supplemental Table 5a) and annual household income (Supplemental Table 6a). The population prevalence of exclusive cigarette use was less common at successively higher levels of both education and household income. Conversely, the prevalence of exclusive ENDS use was generally higher as education level went from less than high school to some college. However, college graduates had a lower prevalence of exclusive ENDS use, equal to or less than respondents without a high school degree. For example, in TUS-CPS, the prevalence of exclusive ENDS use was 0.4% for non-high school graduates, 0.7% for high school graduates, 0.9% for those with some college, and 0.4% for college graduates. Dual use of cigarettes plus ENDS was less prevalent among respondents with a college degree or higher income level than respondents without a college degree or lower income level, respectively. Although exclusive other combustibles use was more prevalent at higher education and income levels, cigarettes plus other combustibles dual use was more prevalent at lower education and income levels. Polyuse was also generally more prevalent at lower education and income levels.
Figure 3.
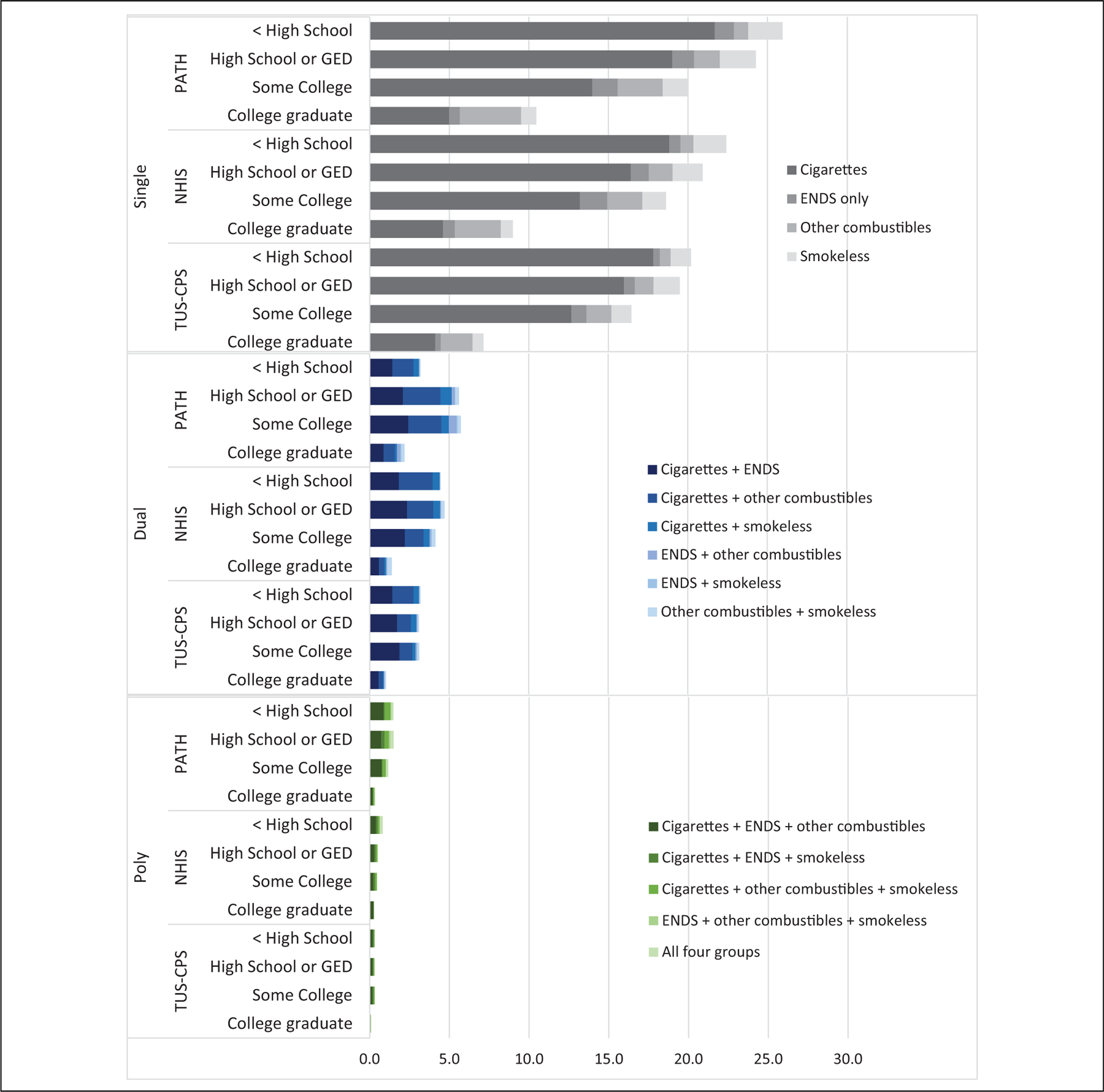
Population prevalence of single, dual, and polytobacco use by education level (ages 25 and over): TUS-CPS (2014–2015), NHIS (2015), and PATH (2015–2016).
Patterns of tobacco product use also varied by age group (Supplemental Table 7a). The population prevalence of exclusive cigarette use was highest among individuals ages 25 to 54. Exclusive ENDS use was highest among 18 to 24-year-olds and successively less prevalent with increasing age group. For example, in PATH, the population prevalence of exclusive ENDS use was 3.1% for 18 to 24-year-olds, 1.8% for 25 to 34-year-olds, 1.2% for 35 to 54-year-olds, and 0.8% for those 55 and older. Age patterns of cigarettes plus ENDS dual use differed by survey, with the highest prevalence among individuals ages 25 to 54 (TUS-CPS and PATH), or 35 to 54 more specifically (NHIS). Dual use of cigarettes plus other combustibles or cigarettes plus smokeless tobacco was lowest among individuals age 55 years and older. Polyuse was most prevalent among individuals ages 18 to 24 (TUS-CPS 0.8%; NHIS 1.1%; PATH 3.2%) and successively less prevalent for individuals ages 25 to 34, 35 to 54, and 55 and over.
Supplemental Table 8 presents a breakdown of other combustible use. Generally, cigar use was the most prevalent, followed by hookah, and tobacco pipe. In TUS-CPS and NHIS, approximately 80% of other combustible users were using traditional cigars, cigarillos, or filtered cigars. In PATH, which asks about these products separately, traditional cigar use was the most common (46.8%), followed by cigarillos (34.9%), and filtered cigars (20.2%). Hookah use among other combustible users ranged from 20.3% (TUS-CPS) to 30.8% (PATH), while tobacco pipe use ranged from 9.4% (PATH) to 12.5% (TUS-CPS).
Sensitivity Analyses
Supplemental Table 9 presents the sensitivity analysis comparing patterns of product use utilizing different current use definitions. The every day/some days definition (used in this paper) defines the most respondents as current tobacco users, although patterns are similar when defining current use as 1+ days in the past 30 days. There is a substantial difference between the prevalence of dual and polyuse comparing the less stringent definitions (every day/some days; 1+ days in past 30 days) to the more stringent definitions (10+ or 25+ days in the past 30 days). For example, the population prevalence of dual use from PATH is 5.2% using the every day/some days definition, 4.3% using 1+ days in the past 30 days, 2.0% using 10+ days in the past 30 days, and 1.1% using 25+ days in the past 30 days. The choice of current use definition will likely vary based on the goal of the analysis. The less stringent definitions capture more tobacco users, whereas the more stringent definitions may be more suitable when examining the health effects of tobacco product use.
Discussion
Our study provides estimates of adult patterns of tobacco product use, including exclusive, dual, and polytobacco use, from 3 recent nationally representative surveys (2014–2016), with a focus on differences between sociodemographic groups to provide insight into tobacco-related health disparities. Consistent with recent studies on patterns of use,10,27 exclusive cigarette use was the most common use pattern overall and across all sociodemographic subgroups. Exclusive cigarette smokers were more likely to be ages 25 to 54 (vs. 18 to 24 and 55+) and have lower (vs. higher) socioeconomic status. Exclusive ENDS use was higher among men than women, 18 to 24-year-olds than older age groups, NH White individuals than other racial/ethnic groups, and individuals with some college education compared to other education levels. Among race/ethnic subgroups, exclusive other combustible users were most likely to be NH Black, whereas exclusive smokeless tobacco users were most likely to be NH White.
Although exclusive product use represents the majority of tobacco use,10,27 the changing landscape of the tobacco market and tobacco control policies may lead to an increase in dual and polyuse, potentially impacting existing tobacco-related health disparities. In our study, cigarettes plus ENDS was the most prevalent dual use pattern in TUS-CPS and NHIS (1.3% and 1.6%, respectively). Moreover, NH White individuals were more likely than NH Black or Hispanic individuals to be dual users of cigarettes plus ENDS in all 3 surveys. If ENDS use leads to a reduction in cigarettes consumed or eventual smoking cessation,13,14,16 this finding, combined with previous evidence that NH Black and Hispanic cigarette smokers are less likely to transition to dual use with ENDS44,45 or exclusive use of ENDS,45 could lead to a potential widening of racial/ethnic disparities in tobacco-related health outcomes.
Similar to other recent studies,10,27 cigarettes plus other combustibles was the most common dual use pattern in PATH (2.0%). Men (vs. women), NH Black individuals (vs. other racial/ethnic groups), and those with lower (vs. higher) socioeconomic status were more likely to be dual users of cigarettes plus other combustibles. Depending on intensity and frequency of use, dual use of multiple combustibles may be more hazardous than exclusive use of cigarettes since some other combustibles, such as cigars, contain more toxicants that cigarettes.38,46
Dual use of cigarettes and smokeless tobacco was less common, at 0.2–0.5% across surveys. Men (vs. women), NH White individuals (vs. other racial/ethnic groups), and younger (vs. older) individuals were more likely to be cigarette plus smokeless tobacco dual users. Though some cigarette smokers use smokeless tobacco as a cessation aide,15 potentially reducing their risk of poor health outcomes, there is preliminary evidence that dual users of cigarettes plus smokeless tobacco might be at greater risk of cardiovascular disease than exclusive cigarette smokers.20 Polyuse of 3 or more product groups was more common among men (vs. women), younger (vs. older) age groups, and individuals with lower (vs. higher) socioeconomic status. Although dual and polyuse were relatively rare in the general population (2.9–6.5%), they jointly represented 16.7–25.5% of tobacco use in our study, falling within the range of dual and polyuse among tobacco users reported in other recent studies (14.2%27 to 32.5%4).
We included estimates from 3 nationally representative surveys in an attempt to capture patterns of tobacco product use in the US population, given the variation in estimates across different nationally representative surveys.47 Although there are more recent waves of data available for the 3 surveys, we chose to use data collected during a similar period to facilitate direct comparisons across surveys. We also defined product use in a consistent way across surveys, with equivalent product groupings whenever possible. Generally, the sociodemographic patterns of tobacco use were similar across surveys. However, there was considerable variation in prevalence estimates. In particular, TUS-CPS generally had lower tobacco use prevalence estimates than PATH or NHIS. This may be because the majority of TUS-CPS data are collected via telephone interview, which is potentially more susceptible to social desirability bias, or the underreporting of stigmatized behaviors such as substance use, than the in-person interviews32,48 used by NHIS. Social desirability bias is least likely when using self-interviewing methods,49 as implemented by PATH, which had the highest prevalence of any reported tobacco product use. PATH also oversampled tobacco users.35 Although the PATH weights account for this oversampling, there may be some residual bias in estimates. Additionally, some differences in reporting may stem from the disparate focus of each survey. PATH is a dedicated tobacco survey, whereas NHIS is a more general health survey and TUS is a supplement to a labor force survey.
This study adds to the current literature on patterns of tobacco product use, as all 3 surveys include information on more recently available tobacco products, such as ENDS, allowing us to characterize dual and polytobacco use based on a wider array of products not captured in previous studies.27,28 However, the timing of the surveys predates the rise in ENDS use among young adults after 201629 and likely underestimates current ENDS prevalence, both exclusively and in combination with other products. Additionally, although we used the current use definition regularly employed by the Center for Disease Control and Prevention,50 our definition did not capture frequency (e.g., # of days used in the past 30 days) or intensity (e.g., cigarettes smoked per day), which was not available for all products across surveys. Future studies incorporating intensity of product use are needed to distinguish health risks related to exclusive, dual, and polytobacco use. Furthermore, by grouping other combustibles and smokeless tobacco products, we are not capturing dual and polyuse within these categories (e.g., use of traditional cigars plus hookah), and potential sociodemographic differences in the use patterns of other combustibles in particular. As risk profiles based on dual and polyuse evolve, it is important to distinguish between products within the same category with varying risks, such as chew and dissolvable tobacco. Nonetheless, as dual and polytobacco use without cigarettes is relatively rare, our analyses provide a picture of the majority of use.
In summary, this study considers the prevalence of single, dual, and polytobacco use overall and by sociodemographic subgroup across 3 nationally representative surveys. Although exclusive product use was the most common tobacco use pattern among US adults, dual and polytobacco use represented a considerable proportion of tobacco product use and may become more prominent as product availability and regulations continue to evolve. Since unique product combinations may have important implications for tobacco-related health risks and cessation, researchers and regulators need to monitor differences in use patterns by sociodemographic subgroup to assess whether they impact tobacco-related health disparities.
Supplementary Material
SO WHAT?
What is already known on this topic?
Although there are well-established sociodemographic differences in individual tobacco product use, research on disparities in multiple product use is extremely limited.
What does this article add?
We report differences in multiple product use by sociodemographic group from 3 nationally representative surveys. Non-Hispanic (NH) Whites were more likely than NH Blacks or Hispanics to use cigarettes plus ENDS. Men, NH Blacks, and those with lower socioeconomic status (SES) were more likely to use cigarettes plus other combustibles than their counterparts. Men and those with lower SES were also more likely than women and those with higher SES to use 3 or more tobacco products.
What are the implications for health promotion practice or research?
Since tobacco products fall on a risk continuum, researchers and regulators need to monitor differences in product combinations by sociodemographic subgroup to assess how they might affect tobacco-related health disparities.
Acknowledgments
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Cancer Institute of the National Institutes of Health [grant number U54-CA229974]. The opinions expressed in this article are the authors’ own and do not reflect the views of the National Institutes of Health, the Department of Health and Human Services, or the United States government.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
- 1.US Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2014. [Google Scholar]
- 2.Pacek LR, Wiley JL, McClernon FJ. A conceptual framework for understanding multiple tobacco product use and the impact of regulatory action. Nicotine Tob Res. 2019;21(3):268–277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Stanton CA, Halenar MJ. Patterns and correlates of multiple tobacco product use in the United States. Nicotine Tob Res. 2018;20(suppl_1): S1–S4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sung HY, Wang Y, Yao T, Lightwood J, Max W. Polytobacco use and nicotine dependence symptoms among US adults, 2012–2014. Nicotine Tob Res. 2018;20(suppl_1): S88–S98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rostron BL, Schroeder MJ, Ambrose BK. Dependence symptoms and cessation intentions among US adult daily cigarette, cigar, and e-cigarette users, 2012–2013. BMC Public Health. 2016; 16(1):814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Harrell PT, Naqvi SMH, Plunk AD, Ji M, Martins SS. Patterns of youth tobacco and polytobacco usage: the shift to alternative tobacco products. Am J Drug Alcohol Abuse. 2017;43(6):694–702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ali M, Gray TR, Martinez DJ, Curry LE, Horn KA. Risk profiles of youth single, dual, and poly tobacco users. Nicotine Tob Res. 2016;18(7):1614–1621. [DOI] [PubMed] [Google Scholar]
- 8.Choi K, Inoue-Choi M, McNeel TS, Freedman ND. Mortality risks of dual- and poly-tobacco product users in the United States. Am J Epidemiol. 2019. June 21:kwz143. 10.1093/aje/kwz143 [DOI] [PMC free article] [PubMed]
- 9.Tomar SL, Alpert HR, Connolly GN. Patterns of dual use of cigarettes and smokeless tobacco among US males: findings from national surveys. Tob Control. 2010;19(2):104–109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lee YO, Hebert CJ, Nonnemaker JM, Kim AE. Multiple tobacco product use among adults in the United States: cigarettes, cigars, electronic cigarettes, hookah, smokeless tobacco, and snus. Prev Med. 2014;62:14–19. [DOI] [PubMed] [Google Scholar]
- 11.Kasza KA, Ambrose BK, Conway KP, et al. Tobacco-product use by adults and youths in the United States in 2013 and 2014. N Engl J Med. 2017;376(4):342–353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Anic GM, Holder-Hayes E, Ambrose BK, et al. E-cigarette and smokeless tobacco use and switching among smokers: findings from the National Adult Tobacco Survey. Am J Prev Med. 2018; 54(4):539–551. [DOI] [PubMed] [Google Scholar]
- 13.Pechacek TF, Nayak P, Gregory KR, Weaver SR, Eriksen MP. The potential that electronic nicotine delivery systems can be a disruptive technology: results from a national survey. Nicotine Tob Res. 2016;18(10):1989–1997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Rass O, Pacek LR, Johnson PS, Johnson MW. Characterizing use patterns and perceptions of relative harm in dual users of electronic and tobacco cigarettes. Exp Clin Psychopharmacol. 2015; 23(6):494–503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Schauer GL, Malarcher AM, Babb SD. Prevalence and correlates of switching to another tobacco product to quit smoking cigarettes. Nicotine Tob Res. 2014;17(5):622–627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Berg CJ, Haardoerfer R, Escoffery C, Zheng P, Kegler M. Cigarette users’ interest in using or switching to electronic nicotine delivery systems for smokeless tobacco for harm reduction, cessation, or novelty: a cross-sectional survey of US adults. Nicotine Tob Res. 2015;17(2):245–255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Benmarhnia T, Pierce JP, Leas E, et al. Can E-cigarettes and pharmaceutical aids increase smoking cessation and reduce cigarette consumption? Findings from a nationally representative cohort of American smokers. Am J Epidemiol. 2018;187(11): 2397–2404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Petersen A, Myers MG, Tully L, Brikmanis K, Doran N. Polytobacco use among young adult smokers: prospective association with cigarette consumption. Tob Control. 2020;29(1):43–48. [DOI] [PubMed] [Google Scholar]
- 19.Zeller M, Hatsukami D. The strategic dialogue on tobacco harm reduction: a vision and blueprint for action in the US. Tob Control. 2009;18(4):324–332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Teo KK, Ounpuu S, Hawken S, et al. Tobacco use and risk of myocardial infarction in 52 countries in the INTERHEART study: a case-control study. Lancet. 2006;368(9536):647–658. [DOI] [PubMed] [Google Scholar]
- 21.McNeill A, Brose LS, Calder R, Bauld L, Robson D. Evidence Review of e-Cigarettes and Heated Tobacco Products 2018. Public Health England: A report commissioned by Public Health England; 2018. [Google Scholar]
- 22.Eissenberg T, Bhatnagar A, Chapman S, Jordt SE, Shihadeh A, Soule EK. Invalidity of an oft-cited estimate of the relative harms of electronic cigarettes. Am J Public Health. 2020;110(2):161–162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Fagan P, Moolchan ET, Lawrence D, Fernander A, Ponder PK. Identifying health disparities across the tobacco continuum. Addiction. 2007;102(suppl 2):5–29. [DOI] [PubMed] [Google Scholar]
- 24.Osibogun O, Taleb ZB, Bahelah R, Salloum RG, Maziak W. Correlates of poly-tobacco use among youth and young adults: findings from the population assessment of tobacco and health study, 2013–2014. Drug Alcohol Depend. 2018;187:160–164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Rath JM, Villanti AC, Abrams DB, Vallone DM. Patterns of tobacco use and dual use in US young adults: the missing link between youth prevention and adult cessation. J Environ Public Health. 2012;2012:679134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Richardson A, Williams V, Rath J, Villanti AC, Vallone D. The next generation of users: prevalence and longitudinal patterns of tobacco use among US young adults. Am J Public Health. 2014; 104(8):1429–1436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Fix BV, O’Connor RJ, Vogl L, et al. Patterns and correlates of polytobacco use in the United States over a decade: NSDUH 2002–2011. Addict Behav. 2014;39(4):768–781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Sung HY, Wang Y, Yao T, Lightwood J, Max W. Polytobacco use of cigarettes, cigars, chewing tobacco, and snuff among US adults. Nicotine Tob Res. 2016;18(5):817–826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Dai H, Leventhal AM. Prevalence of e-cigarette use among adults in the United States, 2014–2018. JAMA. 2019;322(18):1824–1827. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Cullen KA, Ambrose BK, Gentzke AS, Apelberg BJ, Jamal A, King BA. Notes from the field: use of electronic cigarettes and any tobacco product among middle and high school students—United States, 2011–2018. MMWR Morb Mortal Wkly Rep. 2018; 67(45):1276–1277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Delnevo CD, Gundersen DA, Manderski MTB, Giovenco DP, Giovino GA. Importance of survey design for studying the epidemiology of emerging tobacco product use among youth. Am J Epidemiol. 2017;186(4):405–410. [DOI] [PubMed] [Google Scholar]
- 32.Soulakova J, Davis WW, Hartman A, Gibson J. The impact of survey and response modes on current smoking prevalence estimates using TUS-CPS: 1992–2003. Surv Res Methods. 2009;3(3): 123–137. [PMC free article] [PubMed] [Google Scholar]
- 33.US Department of Commerce, Census Bureau 2016, National Cancer Institute and Food and Drug Administration co-sponsored Tobacco Use Supplement to the Current Population Survey. Technical Documentation. Published 2016. Accessed February 3, 2020. https://www.census.gov/programs-surveys/cps/technical-documentation/complete.html
- 34.National Center for Health Statistics. Survey Description, National Health Interview Survey, 2015. 2016.
- 35.Hyland A, Ambrose BK, Conway KP, et al. Design and methods of the Population Assessment of Tobacco and Health (PATH) study. Tob Control. 2017;26(4):371–378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Choi K, Sabado M, El-Toukhy S, Vogtmann E, Freedman ND, Hatsukami D.Tobacco product use patterns, and nicotine and tobacco-specific nitrosamine exposure: NHANES 1999–2012. Cancer Epidemiol Biomarkers Prev. 2017;26(10):1525–1530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.El-Toukhy S, Choi K. A risk-continuum categorization of product use among US youth tobacco users. Nicotine Tob Res. 2016;18(7): 1596–1605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Ghosh A, Abdelwahab SH, Reeber SL, et al. Little cigars are more toxic than cigarettes and uniquely change the airway gene and protein expression. Sci Rep. 2017;7:46239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Corey CG, Holder-Hayes E, Nguyen AB, et al. US adult cigar smoking patterns, purchasing behaviors, and reasons for use according to cigar type: findings from the Population Assessment of Tobacco and Health (PATH) study, 2013–2014. Nicotine Tob Res. 2018;20(12):1457–1466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Kasza KA, Borek N, Conway KP, et al. Transitions in tobacco product use by U.S. adults between 2013(−)2014 and 2014(−)2015: findings from the PATH study wave 1 and wave 2. Int J Environ Res Public Health. 2018;15(11):2515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Judkins D Fay’s method for variance estimation. J Official Statist. 1990;6(3):223–239. [Google Scholar]
- 42.Williams RL. Taylor series linearization (TSL). In: Lavrakas PJ, ed. Encyclopedia of Survey Research Methods. Sage Publications, Inc; 2008. [Google Scholar]
- 43.Stata Statistical Software: Release 15 [computer program]. StataCorp LLC; 2017. [Google Scholar]
- 44.Kasza KA, Coleman B, Sharma E, et al. Correlates of transitions in tobacco product use by U.S. adult tobacco users between 2013(−)2014 and 2014(−)2015: findings from the PATH Study Wave 1 and Wave 2. Int J Environ Res Public Health. 2018;15(11):2556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Harlow A, Stokes A, Brooks D. Socio-economic and racial/ethnic differences in e-cigarette uptake among cigarette smokers: longitudinal analysis of the Population Assessment of Tobacco and Health (PATH) study. Nicotine Tob Res. 2018;21(10):1385–1393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.National Cancer Institute. Smoking and Tobacco Control Monograph 9: Cigars: Health Effects and Trends. US Department of Health and Human Services, National Cancer Institute; 1998. [Google Scholar]
- 47.Levy DT, Yuan Z, Li Y, Mays D, Sanchez-Romero LM. An examination of the variation in estimates of e-cigarette prevalence among U.S. adults. Int J Environ Res Public Health. 2019;16(17):3164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Tourangeau R, Yan T. Sensitive questions in surveys. Psychol Bull. 2007;133(5):859–883. [DOI] [PubMed] [Google Scholar]
- 49.Smith TW, Jibum K. A review of survey data-collection modes: with a focus on computerizations. Soc Theory Method. 2015; 30(2):185–200. [Google Scholar]
- 50.Creamer MR, Wang TW, Babb S, et al. Tobacco product use and cessation indicators among adults—United States, 2018. MMWR Morbid Mortal Weekly Rep. 2019;68(45):1013–1019. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.