

ABSTRACT
Objectives:
To evaluate the pooled prevalence of dental caries among Indian population through systematic review and meta-analysis.
Materials and Methods:
A keyword search was conducted in PubMed, Science Direct, Google Scholar, Cochrane, and Scopus databases using relevant key words to extract the data pertaining to dental caries in Indian population. The search criteria included manuscripts published in English language from March 2009 to March 2019 and employed standard Boolean operators. The studies which met the inclusion criteria were independently reviewed by two researchers and their quality was assessed by the Newcastle–Ottawa Scale. The overall prevalence was deduced using the random effects model with prime focus given to the site of anatomical origin. R software version 3.5.2. was used for statistical analysis.
Results:
Post screening, out of the 253 articles identified, 70 met the inclusion criteria and were used to generate the meta-analysis. Among them, only few studies investigated the prevalence of root caries (n = 1). Overall prevalence of dental caries was 54.16% (CI: 0.4966–0.5866), whereas age-specific prevalence was 62% in patients above 18 years and 52% among 3–18 years of age (P < 0.0001). Maximum overall prevalence was noted in mixed dentition (58%). Region wise prevalence was more in western India (72%). Use of decayed, missed, and filled teeth as diagnostic criteria for early childhood caries was only 29%.
Conclusions:
Besides an overall prevalence of 54.16%, there exists a remarkable variation in dental caries prevalence rates as per age, diagnostic criteria, dentition, and geographical region. Furthermore, research should be focused on the prevalence of anatomical site specific caries as well.
KEYWORDS: Dental caries, DMFT, India, prevalence
INTRODUCTION
Dental caries is a chronic disease displaying drastic variations in its prevalence across multiple factors and the obscurity of data on the same hinders the attainment of dental caries prevalence reduction goals set by WHO.[1] Considering the evolving dietary patterns in last few decades, globalization has been linked to increased consumption of sugar and growing obesity in middle and low income countries.[2] Some studies in developing countries such as India report a prevalence rate of 36.7% among 13–19 year olds while others like Saudi Arabia state prevalence to be as high as 83% among 6–8 year olds.[1,3] Untreated dental caries can cause pain and difficulties in eating and sleeping, pain, which in turn leads to emergency dental visit, hospitalization, need for invasive treatment, and systemic health problems thereby lowering the quality of life.[4] Caries of the permanent teeth was reportedly the most common oral condition as per the Global Burden of Disease Study of 2017.[5] Globally, around 2.4 billion people suffer from caries of the permanent teeth and 486 million children suffer from caries of the primary teeth.[6]
The scenario in India is no different from other developed or developing countries.[2] The available literature on the prevalence of dental caries in India shows a varied picture with prevalence of caries being very high in some areas and low in some areas.[6,7,8,9,10] In India, there are infinite number of studies done on the prevalence of dental caries.[6,7,8,9,10] However, only a few of them focused on dental caries across different age groups.[11,12,13,14] The dentist population ratio in India ranges from 1:1000 to 1:20,000 across different states.[15] Annually, 30,570 dentists are produced in India; however, only 10% of dentists serve the rural people.[16] With a poor dentist to population ratios in some areas, the chances of dental caries going undiagnosed are highly likely, contributing the regional disparity in dental caries prevalence rates.[11] Hence a true prevalence rate needs to be elucidated in order to address the growing concern of dental caries.
Further, only a few systematic reviews on dental caries have been reported among Indian population.[17,18,19,20] However, each study has its own limitations such as the use of a limited number of articles, extraction of published reports from few electronic databases, lack of complete analysis, or unavailability of recently published articles. Few systematic reviews have focused on only children or the elder population. Dental caries can be a lifelong condition which affects children, adolescents, and adults in various forms. Manifestation of dental caries in later stages of life is likely considering the increased prevalence of gingival recession and root caries as people grow older.[21] Evidence suggests that high salivary microbial counts are found in elderly populations which may facilitate the manifestation of dental caries.[22] To the best of our knowledge, there was no data on the pooled prevalence of dental caries among Indian population from different age groups, geographical region, dentition, and diagnostic criteria. Hence, the study aimed to evaluate the prevalence of dental caries across the aforementioned characteristics in the Indian population.
AIMS AND OBJECTIVE
Participants from the ages of 3–75 years and hailing from different parts of India were covered in this meta-analysis of 70 studies to elucidate the overall prevalence of dental caries as well as its distribution pattern across different age groups, geographical regions, type of dentition, and the diagnostic criteria used. The findings of which are elemental in delineating the risk factors of dental caries and vulnerable sub-populations in India along with ascertaining current gaps in the scientific literature on dental caries.
MATERIALS AND METHODS
A systematic review and meta-analysis of the literature on dental caries was conducted to determine its prevalence among the Indian population of varying age groups. The study protocol adopted was registered in PROSPERO (CRD42019132489) and followed the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines.
SEARCH STRATEGY
Research articles published between March 2009 and March 2019 were screened using databases such as PubMed, Science Direct, Google Scholar, Cochrane, and Scopus. Search strings used for electronic screening of databases included the following: prevalence, dental caries, India, DMFT, cavitated lesion, non-cavitated lesion, root caries, incisor caries, smooth surface caries, occlusal caries, proximal caries, DMF, early childhood caries, geriatric caries, premolar caries, molar caries, canine caries, coronal caries, pit and fissure caries, linear enamel caries, and age group ranging from 3 to 75 years.
INCLUSION/EXCLUSION CRITERIA
Full-text articles published in English during the last decade were screened for analysis. The inclusion criteria composed of observational studies (case–control, cohort, and cross-sectional) conducted on the prevalence of dental caries in India, on patient population aged 3–75 years. Investigations with nonspecific data, inadequately designed, editorials, letters, case reports, conference proceedings, and the grey literature, ongoing observational studies, reviews, and studies that did not report statistical tests for dental caries were excluded from the study analysis.
DATA EXTRACTION
After deduplication, the studies were screened for eligibility by two independent investigators to identify “potentially eligible” studies and the disagreements were resolved by consensus after discussion. The inter-reliability score was assessed by Cohen’s Kappa (0.00943). The information from the eligible studies were extracted which encompassed author’s name, year of publication, participants, population characteristics (age range and dentition), geographic location, type of dental caries, diagnostic criteria of dental caries, and prevalence percent of dental caries as per age group.
QUALITY ASSESSMENT
The quality of the studies that formed the basis of meta-analysis was assessed by adopting the Newcastle–Ottawa Scale (NOS) comprising three components (methodology, comparability based on study design, outcome). Based on this criterion, the study quality was graded on a 10-point scale. Studies with scores less than 5 were considered to have low methodological quality, scores of 5 to 7 indicated moderate quality, and those above 7 were considered as high quality.
DATA ANALYSIS
Statistical analyses were performed using the R software, version 3.5.2. A random effects model was employed in all meta-analysis procedures. Forest-plots were used to demonstrate the effect of each study and the summary effect size. For effect size estimates, standard errors of its logarithm were calculated from the reported or estimated CIs, assuming that the effect size was log-normally distributed. The prevalence of dental caries was extracted from individual studies and combined using the generic inverse variance method of Der Simonian and Laird random effects model. The heterogeneity of effect size among studies was quantified using I2. The influence analysis was performed by removing one study at a time to evaluate whether the pool estimates could have been altered by a single study. Subgroup analyses were conducted as per mean age, region, diagnostic criterion for estimating dental caries (DMFT), dentition, and type of dental caries. To investigate publication bias, funnel plots were constructed. The distribution of study risk estimates across the funnel plot was examined visually and Egger’s test for small study effects was performed to assess the degree of asymmetry. A P < 0.05 was considered statistically significant.
RESULTS
On electronic screening as described in Figure 1, 253 relevant publications were found. Among the databases explored, Google scholar yielded the most articles (n = 170), followed by PubMed (n = 62), science direct (n = 15), Scopus (n = 4), and Cochrane Library (n = 2). Initially, 115 duplicate records were excluded using EndNote which created a separate list of duplicate references that were reviewed by investigators for de-duplication. Subsequently, another 43 articles were excluded after scrutinizing the abstracts, thereby yielding 95 articles, the full texts of which were assessed for eligibility. Two independent reviewers on screening the remaining data, finally included 70 articles in this meta-analysis after excluding 25 articles due to studies lacking the prevalence rate of dental caries, no specification of DMFT index and age not matching with the inclusion criteria.[8,9,13,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87]
Figure 1.

Flowchart of the eligibility criteria as per PRISMA
CHARACTERISTICS OF INCLUDED STUDIES
Vast spatial distribution of studies was observed, with almost all regions of India except the northeast finding representation [Figure 2]. Prevalence of crown caries was observed in 69 studies and 8 studies reported of early childhood caries. The evaluation of dental caries was conducted through clinical examinations, in accordance with DMFT and WHO criteria mainly.
Figure 2.
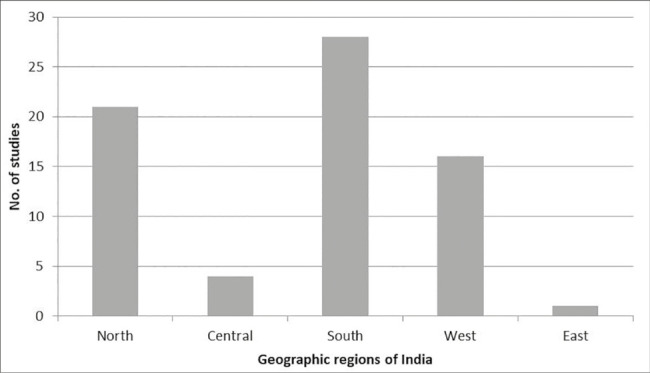
Geographical distribution pattern of the 70 studies included in the meta-analysis on prevalence of dental caries
QUALITY ASSESSMENT
The quality assessment using NOS depicted 12 studies to have low methodological quality, whereas 52 studies were of moderate methodological quality and only six studies demonstrated high methodological quality.
OVERALL PREVALENCE OF DENTAL CARIES META-ANALYSIS
The overall prevalence of the dental caries calculated using the random effects model was 54.16% (SD 0.0229, 95% CI: 0.4966–0.5866). The test for heterogeneity produced Tau square of 0.04, Q(P < 0.0001), I2 =99.57% (95% CI: 99.4121–99.7012), H square = 232.32 (95% CI: 170.1101–334.6652). Figure 3 illustrates the forest plot for each of the studies examined and the overall prevalence of dental caries in India.
Figure 3.

Forest plot depicting study specific prevalence (mean and 95% CI) for dental caries in Indian population
PREVALENCE OF DENTAL CARIES BY SUBGROUP ANALYSIS META-ANALYSIS
Studies were divided into various subgroups such as age, dentition, geographic location, estimation of caries using a diagnostic index and type of dental caries, to check for any possible heterogeneity.
Figure 4 illustrates the subgroup analysis by age which was further divided into three categories. The overall prevalence of dental caries observed in the age range of 3–18 years was 52%. The test for heterogeneity produced Tau square of 0.0330, Q(P < 0.0001), I2 =99.5365% (95% CI: 99.3520–99.6907), H square = 215.7641 (95% CI: 154.3266–323.3308). The maximum and minimum prevalence of dental caries observed in the age range of 3–18 years were 95 and 7%, respectively.[9,77]
Figure 4.

Forest plot depicting specific age-group prevalence (mean and 95% CI) for dental caries in Indian population
Similarly, the overall prevalence of dental caries observed in the age range of >18 years was 62%. The test for heterogeneity produced Tau square of 0.0519, Q(P < 0.0001), I2 = 99.5250% (95% CI: 98.8461–99.9014), H square = 210.5069 (95% CI: 86.6651–1014.4179).
Subgroup analysis by type of dental caries depicted that the overall prevalence of crown caries was 57%, overall prevalence of dental caries was maximum in the mixed dentition (58%) followed by the primary (54%) and permanent dentition (46%). Furthermore, the overall prevalence of dental caries was observed to be higher in western India (72%) followed by northern India (57%), central India (56%), and 51% in the southern India. The lowest prevalence of dental caries, however, was observed in eastern India (36%). However, research paucity could have been the possible explanation for the low prevalence in Eastern India.
The test for heterogeneity (for type of dental caries, diagnostic criteria for estimating dental caries, dentition, region) produced Tau square of 0.0329, Q(P < 0.0001), I2 = 99.38% (95% CI: 99.11–99.58), H square = 159.52 (95% CI: 112.63–242.27).
META-ANALYSIS FOR DMFT BY SUBGROUP ANALYSIS
Random-effect model revealed the prevalence of DMFT index as a diagnostic criterion in the estimation of dental caries in the age group of 3–18 years to be 57%. In patients aged above 18 years its usage was much higher at 77%. The prevalence of DMFT index in the overall diagnosis of crown caries was observed to be 62%. In early childhood caries, the prevalence of DMFT index was comparatively low at 29%. The prevalence of DMFT index as diagnostic criterion of dental caries in primary dentition was 59%. While in mixed dentition and permanent dentition the prevalence rates of DMFT for diagnosis of dental caries were 66 and 43%, respectively. Eastern India observed the highest overall prevalence of DMFT as diagnostic criteria for estimating dental caries at 72% followed by western part of India (60%), southern (59%), and north India (58%).
The test for heterogeneity (for age, type of dental caries, dentition, region) produced Tau square of 0.0288, Q(P < 0.0001), I2 = 99.30% (95% CI: 98.9145–99.6016), H square = 143.09 (95% CI: 92.1239–250.9946).
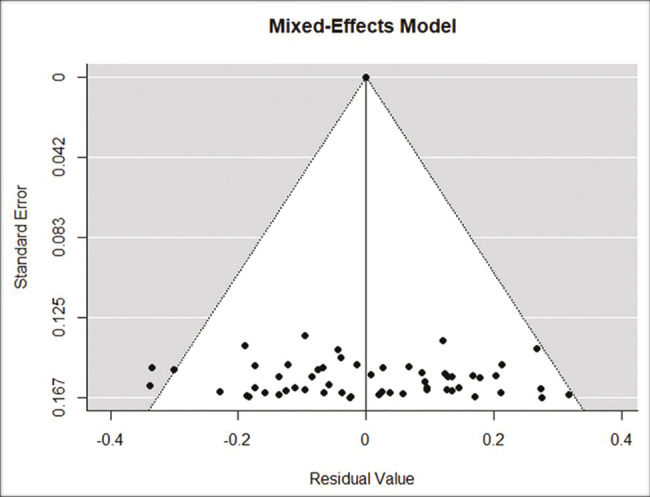
PUBLICATION BIAS AND META REGRESSION ANALYSIS
The regression test on both the random-effect (without moderators) and mixed-effect (with the 6 moderators) generated P > 0.05, indicating no funnel plot asymmetry and hence, no publication bias. The absence of publication bias in the present study is depicted by the even scattering of smaller studies at the base of the funnel in Figure 5.
Figure 5.
Funnel plot for all studies
The non-parametric rank-based test (trim and fill test) on random-effect model (without parameter model) also suggested symmetry (hence, no publication bias) and no missing studies. The Egger’s regression intercept was −5.417, 95% CI (−13.061, −2.227), t = −1.398 and P = 0.1663, indicating funnel plot symmetry and lack of publication bias.
Results of meta-regression analysis indicated that none of the included subgroups influenced the size of the average true effect. Approximately, 9.62% of the total amount of heterogeneity can be accounted for by including the 6 moderators (region, design, caries type, dentition, age, and year of study). Remaining 90.28% of variability was due to other factors not included in this study. The test for residual heterogeneity was significant (QE = 12340.4190, df = 55, P < 0.0001), possibly indicating that other moderators (such as the sample population and gender) not considered in the model were influencing the prevalence of caries.
DISCUSSION
Multitude of studies have been undertaken on the prevalence of caries among children and adolescents; however, a comprehensive insight into prevalence rates of dental caries across different age groups, type of dental caries, geographical regions, dentition, and diagnostic criterion for estimating dental caries (DMFT) has remained unexplored. Hence, this systematic review and meta-analysis set out to fill these lacunae.
As per our review and analysis, the overall prevalence of dental caries in Indian population aged between 3 and 75 years was 54.16%. This finding is in congruence with results of the National Oral Health Survey in India which noted a prevalence of 53.8%.[88]
Although most studies have focused on dental caries in populations under 18, an age-specific prevalence of 62% in patients above 18 years and 52% among 3–18 year olds (P < 0.0001) was observed. Janakiram et al. reported a mean prevalence of 49% in 5–12 year olds, with a steady increase of 60% to 84% in 15 years olds and 65–74 year group, respectively.[21] Age-specific increase in dental caries can also be attributed to poor health seeking behaviors among adults, inadequate time for self-care, substance abuse, presence of comorbidities, and absence of organized programs that target prevention and reduction of dental caries in India.[19,89,90,91,92]
In reference to prevalence of dental caries across different types of dentition, highest overall prevalence was noted in the mixed dentition (58%) category, followed by the primary (54%) type. This points towards the slow increment in prevalence of caries in the transitory period between primary and mixed dentition, as dental caries takes time to manifest as clinically detectable lesions and impact of changing dietary patterns.[93]
On assessing the geographical distribution of dental caries prevalence rates in India, the region wise prevalence was notably high in western India (72%). However, this is in dissonance with a meta-analysis by Janakiram et al. who found that the dental caries prevalence was markedly higher in North India among all age groups compared with the other parts of India.[21] This variation in inter-regional estimates can arise depending on the socio-economic parameters of the areas surveyed and the food practices pertaining to that region.[94]
The 77% prevalence of DMFT index in the diagnosis of crown caries in adults and corresponding 29% for early childhood caries emphasizes the availability and adoption of numerous newer and age-specific indices such as ICADAS, AAPD, EAPD, DEFT, and PUFA in diagnosis of caries among children. Use of DMFT index showed significant variations across other corollary parameters such as type of dental caries, dentition, and geographical region studied. The simplicity and convenient application of DMFT have made the most widely used and preferred diagnostic index for dental caries in large epidemiological surveys or in pre-operative assessments.[95]
This review has its limitations. The literature was restricted to a particular time frame, language, and could not comprehensively cover assessment of clinical symptoms, etiology, and treatment protocols associated with dental caries and thereby limiting our ability to evaluate all possible outcomes. Exclusion of studies due to incoherence in the dentition status of sampled patients further limited the number of studies analyzed. Despite these shortcomings, this systematic review and meta-analysis was able to avoid publication bias and present a cohesive understanding of dental caries prevalence among the Indian population.
CONCLUSION
Present findings suggest that the prevalence of dental caries is a pressing health concern affecting at least half of the Indian population. Age-specific subgroup analysis highlights the need for better preventive oral care programs and awareness campaigns among adults for pertinent management of dental caries. Taking note of the regional disparities in prevalence rates can help in better targeting of interventions and health policy formulation. In addition, the lack of anatomical site-specific investigation was observed during the literature collection and research should be focused on the prevalence of anatomical site specific caries as well.
FINANCIAL SUPPORT AND SPONSORSHIP
This manuscript did not receive any funding from public or private sectors.
CONFLICTS OF INTEREST
The authors have no conflict of interests to disclose.
AUTHORS CONTRIBUTIONS
First author contributed to the concepts, design, literature search, data acquisition, screening of articles, exclusion of ineligible studies, data analysis and manuscript review stages. Second author contributed to the literature search, data acquisition, screening of articles, exclusion of ineligible studies, data analysis, statistical analysis and manuscript review. Third author contributed to the concepts, design, definition of intellectual content, data analysis and manuscript review. Fourth author contributed to the concepts, manuscript preparation, manuscript editing and manuscript review. Fifth author contributed to the design, manuscript preparation, editing and review.
ETHICAL POLICY AND INSTITUTIONAL REVIEW BOARD STATEMENT
Not applicable.
PATIENT DECLARATION OF CONSENT
Not applicable.
DATA AVAILABILITY STATEMENT
The data set used in the current study has been sourced from PubMed, Google Scholar and Science direct, Cochrane, and Scopus indexed articles. Besides the data mentioned in the article, additional data can be made available on request.
ACKNOWLEDGEMENTS
Nil.
REFERENCES
- 1.Alhabdan YA, Albeshr AG, Yenugadhati N, Jradi H. Prevalence of dental caries and associated factors among primary school children: A population-based cross-sectional study in Riyadh, Saudi Arabia. Environ Health Prev Med. 2018;23:60. doi: 10.1186/s12199-018-0750-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Alsuraim BS, Han DH. Effect of globalization on global dental caries trend. Medicine (Baltimore) 2020;99:e21767. doi: 10.1097/MD.0000000000021767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Punitha VC, Amudhan A, Sivaprakasam P, Rathanaprabu V. Role of dietary habits and diet in caries occurrence and severity among urban adolescent school children. J Pharm Bioallied Sci. 2015;7:S296–300. doi: 10.4103/0975-7406.155963. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kidd EA, Banerjee A. What is absence of caries? In: Albrektsson TO, Bratthall D, Glantz PJ, Lindhe JT, editors. Tissue Preservation in Caries Treatment. 3rd ed. Great Britain: Quintessence Publication Co. Ltd.; 2001. p. 69. [Google Scholar]
- 5.Clementino MA, Gomes MC, Pinto-Sarmento TC, Martins CC, Granville-Garcia AF, Paiva SM. Perceived impact of dental pain on the quality of life of preschool children and their families. PLoS One. 2015;10:e0130602. doi: 10.1371/journal.pone.0130602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sharma V, Gupta N, Arora V, Gupta P, Mehta N. Caries experience in permanent dentition among 11–14 years old school children in Panchkula district (Haryana) India. Int J Sci Study. 2015;3:112–5. [Google Scholar]
- 7.GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–858. doi: 10.1016/S0140-6736(18)32279-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Datta P, Datta PP. Prevalence of dental caries among school children in Sundarban, India. Epidemiology. 2013;3:2161–1165. [Google Scholar]
- 9.Reddy ER, Rani ST, Manjula M, Kumar LV, Mohan TA, Radhika E. Assessment of caries status among schoolchildren according to decayed-missing-filled teeth/decayed-extract-filled teeth index, international caries detection and assessment system, and caries assessment spectrum and treatment criteria. Indian J Dent Res. 2017;28:487–92. doi: 10.4103/ijdr.IJDR_735_16. [DOI] [PubMed] [Google Scholar]
- 10.Saravanan S, Kalyani V, Vijayarani MP, Jayakodi P, Felix J, Arunmozhi P, et al. Caries prevalence and treatment needs of rural school children in Chidambaram taluk, Tamil Nadu, South India. Indian J Dent Res. 2008;19:186–90. doi: 10.4103/0970-9290.42948. [DOI] [PubMed] [Google Scholar]
- 11.Parasuraman G, Gowtham Krishna Y, Kaviya M, Jain NA, Rajendiran P, Dutta R. A study on the prevalence of dental caries among the school-going children in Tamil Nadu. Int J Commun Med Public Health. 2017;4:3582–9. [Google Scholar]
- 12.Raja K, Radha G, Rekha R, Pallavi SK. Geriatric oral health: A literature review. Int J Dent Health Sci. 2015;2:385–95. [Google Scholar]
- 13.Khan AA, Jain SK, Shrivastav A. Prevalence of dental caries among the population of Gwalior (India) in relation of different associated factors. Eur J Dent. 2008;2:81–5. [PMC free article] [PubMed] [Google Scholar]
- 14.Aparna A, Hegde MN, Shetty V. Evaluation of microflora of root carious lesions in different age groups: A microbiological study. Eur J Gen Dent. 2013;2:130–3. [Google Scholar]
- 15.Padminee K, Anusha R, Lakshmi K, Madan Kumar PD. Geographic disproportions in dental workforce distribution and its impact on oral disease burden: An Indian perspective. SRM J Res Dent Sci. 2020;11:76–81. [Google Scholar]
- 16.Chandu VC, Pachava S, Viswanath V. Strategies for improving accessibility to oral health care services in rural India: An insight. Int J Oral Health Med Res. 2017;4:44–6. [Google Scholar]
- 17.Agarwal P, Nayak R, Elangovan G. A predictable aesthetic rehabilitation of deciduous anterior teeth in early childhood caries. Case Rep Dent. 2018;2018:1742529. doi: 10.1155/2018/1742529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kundu H, Patthi B, Singla A, Jankiram C, Jain S, Singh K. Dental caries scenario among 5, 12 and 15-year-old children in India — A retrospective analysis. J Clin Diagn Res. 2015;9:ZE01–5. doi: 10.7860/JCDR/2015/12439.6150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mehta A. Trends in dental caries in Indian children for the past 25 years. Indian J Dent Res. 2018;29:323–8. doi: 10.4103/ijdr.IJDR_615_17. [DOI] [PubMed] [Google Scholar]
- 20.Srivastava R, Nongkynrih B, Mathur VP, Goswami A, Gupta SK. High burden of dental caries in geriatric population of india: A systematic review. Indian J Public Health. 2012;56:129–32. doi: 10.4103/0019-557X.99903. [DOI] [PubMed] [Google Scholar]
- 21.Janakiram C, Antony B, Joseph J, Ramanarayanan V. Prevalence of dental caries in India among the WHO index age groups: A meta-analysis. J Clin Diagn Res. 2018;12:8–13. [Google Scholar]
- 22.Eidt G, Waltermann EDM, Hilgert JB, Arthur RA. Candida and dental caries in children, adolescents and adults: A systematic review and meta-analysis. Arch Oral Biol. 2020;119:104876. doi: 10.1016/j.archoralbio.2020.104876. [DOI] [PubMed] [Google Scholar]
- 23.Mehta A, Bhalla S. Assessing consequences of untreated carious lesions using pufa index among 5-6 years old school children in an urban indian population. Indian J Dent Res. 2014;25:150–3. doi: 10.4103/0970-9290.135906. [DOI] [PubMed] [Google Scholar]
- 24.Ghanghas M, Manjunath BC, Kumar A, Shyam R, Phogat R, Panghal V. Validation of the hindi version of the early childhood oral health impact scale among 3-5-year-old preschool children in Rohtak City, Haryana. J Indian Soc Pedod Prev Dent. 2019;37:333–8. doi: 10.4103/JISPPD.JISPPD_128_18. [DOI] [PubMed] [Google Scholar]
- 25.Amith HV, D’Cruz AM. Prevalence of dental caries amongst 12–15 years old school going children in Warananagar, Kolhapur, Maharashtra. J Indian Assoc Public Health Dent. 2011;9:887–90. [Google Scholar]
- 26.Moses J, Rangeeth BN, Gurunathan D. Prevalence of dental caries, socio-economic old school going children of Chidambaram status and treatment needs among 5 to 15 year old school going children of Chidambaram. J Clin Diagn Res. 2011;5:146–51. [Google Scholar]
- 27.Kumar S, Tadakamadla J, Duraiswamy P, Kulkarni S. Dental caries and its socio-behavioral predictors — an exploratory cross-sectional study. J Clin Pediatr Dent. 2016;40:186–92. doi: 10.17796/1053-4628-40.3.186. [DOI] [PubMed] [Google Scholar]
- 28.Hiremath A, Murugaboopathy V, Ankola AV, Hebbal M, Mohandoss S, Pastay P. Prevalence of dental caries among primary school children of India — A cross-sectional study. J Clin Diagn Res. 2016;10:ZC47–50. doi: 10.7860/JCDR/2016/22474.8642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Marya CM, Dhingra S, Marya V, Ashokkumar BR. Relationship of dental caries at different concentrations of fluoride in endemic areas: An epidemiological study. J Clin Pediatr Dent. 2010;35:41–5. doi: 10.17796/jcpd.35.1.u6vm217421w3h521. [DOI] [PubMed] [Google Scholar]
- 30.Kumar YS, Acharya S, Pentapati KC. Prevalence of dental pain and its relationship to caries experience in school children of udupi district. Eur Arch Paediatr Dent. 2014;15:371–5. doi: 10.1007/s40368-014-0124-1. [DOI] [PubMed] [Google Scholar]
- 31.Grewal H, Verma M, Kumar A. Prevalence of dental caries and treatment needs in the rural child population of nainital district, uttaranchal. J Indian Soc Pedod Prev Dent. 2009;27:224–6. doi: 10.4103/0970-4388.57657. [DOI] [PubMed] [Google Scholar]
- 32.Grewal H, Verma M, Kumar A. Prevalence of dental caries and treatment needs amongst the school children of three educational zones of urban Delhi, India. Indian J Dent Res. 2011;22:517–9. doi: 10.4103/0970-9290.90283. [DOI] [PubMed] [Google Scholar]
- 33.Khare V, Koshy A, Rani P, Srilatha S, Kapse SC, Agrawal A. Prevalence of dental caries and treatment needs among the orphan children and adolescents of Udaipur district, Rajasthan, India. J Contemp Dent Pract. 2012;13:182–7. doi: 10.5005/jp-journals-10024-1118. [DOI] [PubMed] [Google Scholar]
- 34.Anuradha B, Laxmi GS, Sudhakar P, Malik V, Reddy KA, Reddy SN, et al. Prevalence of dental caries among 13 and 15-year-old school children in an endemic fluorosis area: A cross-sectional study. J Contemp Dent Pract. 2011;12:447–50. doi: 10.5005/jp-journals-10024-1074. [DOI] [PubMed] [Google Scholar]
- 35.Murthy AK, Pramila M, Ranganath S. Prevalence of clinical consequences of untreated dental caries and its relation to dental fear among 12-15-year-old school children in Bangalore city, India. Eur Arch Paediatr Dent. 2014;15:45–9. doi: 10.1007/s40368-013-0064-1. [DOI] [PubMed] [Google Scholar]
- 36.Bhaskar SA, Hegde S. Molar-incisor hypomineralization: Prevalence, severity and clinical characteristics in 8- to 13-year-old children of udaipur, india. J Indian Soc Pedod Prev Dent. 2014;32:322–9. doi: 10.4103/0970-4388.140960. [DOI] [PubMed] [Google Scholar]
- 37.Sridevi T, Pranoti S, Anand S, Umesh W, Sachin G. Factors associated with early childhood caries among 3 to 6 year old children in India: A case control study. J Neonatal Perinatal Med. 2018;11:45–50. doi: 10.3233/NPM-181723. [DOI] [PubMed] [Google Scholar]
- 38.Bhayade SS, Mittal R, Chandak S, Bhondey A. Assessment of social, demographic determinants and oral hygiene practices in relation to dental caries among the children attending anganwadis of Hingna, Nagpur. J Indian Soc Pedod Prev Dent. 2016;34:124–7. doi: 10.4103/0970-4388.180415. [DOI] [PubMed] [Google Scholar]
- 39.Gaidhane AM, Patil M, Khatib N, Zodpey S, Zahiruddin QS. Prevalence and determinant of early childhood caries among the children attending the anganwadis of Wardha district, India. Indian J Dent Res. 2013;24:199–205. doi: 10.4103/0970-9290.116677. [DOI] [PubMed] [Google Scholar]
- 40.Sharma U, Gill N, Gulati A, Arora R, Bal IS, Agnihotri A, et al. Oral health behavior: Prevalence and pattern of dental caries in 11–16-year-old children of various socioeconomic strata. J Pierre Fauchard Acad (India Sect [Internet] 2016;30:36–41. Available from: https://www.sciencedirect.com/science/article/pii/S0970219916300364 . [Google Scholar]
- 41.Saimbi CS, Kaushal S, Khan MA, Avadhesh Kumar. Prevalence of caries in rural area children. J Pierre Fauchard Acad (India Section) 2010;24:62–6. [Google Scholar]
- 42.Shyam R, Manjunath BC, Kumar A, Narang R, Goyal A, Piplani A. Assessment of dental caries spectrum among 11 to 14-year-old school going children in India. J Clin Diagn Res. 2017;11:ZC78–81. doi: 10.7860/JCDR/2017/27254.10107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Shingare P, Jogani V, Sevekar S, Patil S, Jha M. Dental caries prevalence among 3–14 year old school children, Uran, Raigad district, Maharastra. J Contemp Dent. 2012;2:11–4. [Google Scholar]
- 44.Bhat PK, Aruna CN. Dietary habits, oral hygiene practices and prevalence of dental caries among 10-12 years old school children of South Bangalore. J Indian Assoc Public Health Dent. 2011;2011:78–82. [Google Scholar]
- 45.Mehta A. Assessment of dental caries experience of an adult population using caries assessment spectrum and treatment index. SRM J Res Dent Sci. 2017;8:21. [Google Scholar]
- 46.Basha S, Mohamed RN, Swamy HS, Ramamurthy PH, Sexena V. Caries incidence among obese adolescents: A 3-year prospective study. Oral Health Prev Dent. 2017;15:65–71. doi: 10.3290/j.ohpd.a37715. [DOI] [PubMed] [Google Scholar]
- 47.Shah AF, Batra M, Kabasi S, Dany SS, Rajput P. Dental caries experience among 6–12 year old school children of Budgam district, Jammu. and Kashmir state, India. Asian Pac J Health Sci. 2015;2:55–9. [Google Scholar]
- 48.Rajagopalan A, Sakthi DS, John J, Arumugham IM, Kumar RP. Dental caries experience and treatment needs among 7-17-year-old school children in Madurai, Tamil Nadu, South India. J Dent Med Sci. 2016;3:76–81. [Google Scholar]
- 49.Sharva V, Khare P, Reddy V, Jain M, Khare A, Singh P. Dental caries prevalence and treatment needs among 12- and 15-year-old school-going children of rural and Urban Areas of Bhopal District, India. J Indian Assoc Public Health Dent. 2017;15:340–3. [Google Scholar]
- 50.Peedikayil FC, Kottayi S, Kenchamba V, Jumana MK. Dental caries prevalence and treatment needs of school going children in Kannur district, Kerala. SRM J Res Dent Sci. 2013;4:51–3. [Google Scholar]
- 51.Munjal V, Gupta A, Kaur P, Garewal R. Dental caries prevalence and treatment needs in 12 and 15-year-old school children of Ludhiana city. Indian J Oral Sci. 2013;4:27–30. [Google Scholar]
- 52.Mohammadi SN, Prashant GM, Kumar PG, Sushanth VH, Imranulla M. Dental caries status in 6–14 year old schoolchildren of rural Channagiri, Davangere: A cross-sectional survey. J Indian Assoc Public Health Dent. 2015;13:389–92. [Google Scholar]
- 53.Batra M, Shah AF, Rajput P, Shah IA. Comparison of linear and zero-inflated negative binomial regression models for appraisal of risk factors associated with dental caries. J Indian Soc Pedod Prev Dent. 2016;34:71–5. doi: 10.4103/0970-4388.175521. [DOI] [PubMed] [Google Scholar]
- 54.Basavaraj P, Khuller N, Dadu M, Ingle Khuller R. Dental erosion, dental caries experience and periodontal status among battery factory workers of Ghaziabad. J Indian Assoc Public Health Dent. 2011;18(Suppl 2):827–31. [Google Scholar]
- 55.Bhardwaj VK, Vaid S, Chug A, Jhingta P, Negi N, Sharma D. Prevalence of dental caries among five-year-old school children in Shimla city, Himachal Pradesh. Eur J Gen Dent. 2012;1:34–8. [Google Scholar]
- 56.Naziya KB, Pradeep Kumar R, Arumughamm IM, Srisakthi D. Prevalence of dental caries among primary schoolchildren in Chennai – A cross-sectional study. J Adv Pharm Educ Res. 2017;7:150–2. [Google Scholar]
- 57.Rajesh SS, Venkatesh P. Prevalence of dental caries among school-going children in South India. Int J Med Sci Public Health. 2016;5:700–4. [Google Scholar]
- 58.Dixit A, Aruna DS, Sachdev V, Sharma A. Prevalence of dental caries and treatment needs among 3–5 year old preschool children in Narmada, Gujarat. IOSR J Dent Med Sci. 2015;14:97–101. [Google Scholar]
- 59.Uttarwar V, Shenoi P, Patil S, Mokhade V, Pradhan M, Bhattacharya S. Prevalence of dental caries in permanent mandibular first molars in adult patients visiting OPD of department of conservative dentistry & endodontics (18 to 44 years) a cross sectional study. Int J Sci Res. 2017;6:1934–37. [Google Scholar]
- 60.Maj Saravanan S, Lokesh S, Polepalle T, Shewale A. Prevalence, severity, and associated factors of dental caries in 3–6-year-old children–a cross-sectional study. Int J. 2014;2:5–11. [Google Scholar]
- 61.Sarvaiya B, Bhayya D, Arora R, Singh D, Pandya D. Prevalence of dental caries in relation with different fluoride levels in drinking water among school going children in Sarada Tehsil of Udaipur district, Rajasthan. NJIRM. 2012;3:118–23. doi: 10.4103/0970-4388.108929. [DOI] [PubMed] [Google Scholar]
- 62.Bansal M, Gupta N, Gupta P, Arora V, Thakar S. Reasons for extraction in primary teeth among 5-12 years school children in Haryana, India - A cross-sectional study. J Clin Exp Dent. 2017;9:e545–9. doi: 10.4317/jced.53076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Sood S, Ahuja V, Chowdhry S. Reconnoitring the association of nutritional status with oral health in elementary school-going children of Ghaziabad city, North India. J Indian Soc Pedod Prev Dent. 2014;32:197–201. doi: 10.4103/0970-4388.135824. [DOI] [PubMed] [Google Scholar]
- 64.Shanthi M, Reddy BV, Venkataramana V, Gowrisankar S, Reddy BV, Chennupati S. Relationship between drinking water fluoride levels, dental fluorosis, dental caries and associated risk factors in 9-12 years old school children of Nelakondapally mandal of Khammam district, Andhra Pradesh, India: A cross-sectional survey. J Int Oral Health. 2014;6:106–10. [PMC free article] [PubMed] [Google Scholar]
- 65.Anandakrishna L, Bhargav N, Hegde A, Chandra P, Gaviappa D, Shetty AK. Problematic eating and its association with early childhood caries among 46-71-month-old children using children’s eating behavior questionnaire (CEBQ): A cross-sectional study. Indian J Dent Res. 2014;25:602–6. doi: 10.4103/0970-9290.147101. [DOI] [PubMed] [Google Scholar]
- 66.Krishnan R, Ramesh M, Chalakkal P. Prevalence and characteristics of MIH in school children residing in an endemic fluorosis area of India: An epidemiological study. Eur Arch Paediatr Dent. 2015;16:455–60. doi: 10.1007/s40368-015-0194-8. [DOI] [PubMed] [Google Scholar]
- 67.Gopal S, Chandrappa V, Kadidal U, Rayala C, Vegesna M. Prevalence and predictors of early childhood caries in 3- to 6-year-old south indian children–A cross-sectional descriptive study. Oral Health Prev Dent. 2016;14:267–73. doi: 10.3290/j.ohpd.a35619. [DOI] [PubMed] [Google Scholar]
- 68.Pentapati KC, Siddiq H, Yeturu SK. Global and regional estimates of the prevalence of root caries - systematic review and meta-analysis. Saudi Dent J. 2019;31:3–15. doi: 10.1016/j.sdentj.2018.11.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Simratvir M, Moghe GA, Thomas AM, Singh N, Chopra S. Evaluation of caries experience in 3-6-year-old children, and dental attitudes amongst the caregivers in the ludhiana city. J Indian Soc Pedod Prev Dent. 2009;27:164–9. doi: 10.4103/0970-4388.57097. [DOI] [PubMed] [Google Scholar]
- 70.Kalita C, Choudhary B, Saikia AK, Sarma PC. Caries prevalence of school-going boys and girls according to cleaning methods and soft drink-taking frequency in different localities, in and around guwahati city. J Indian Soc Pedod Prev Dent. 2016;34:249–56. doi: 10.4103/0970-4388.186755. [DOI] [PubMed] [Google Scholar]
- 71.Sudan J, Sogi GM, Veeresha LK. Assessing clinical sequelae of untreated caries among 5-, 12-, and 15-year-old school children in Ambala district: A cross-sectional study. J Indian Soc Pedod Prev Dent. 2018;36:15–20. doi: 10.4103/JISPPD.JISPPD_97_17. [DOI] [PubMed] [Google Scholar]
- 72.Javali SB, Tippeswamy V, Prasad KVV, Preetha Shetty, Rajesh G, Shodan M. An epidemiological investigation in relative importance of factors associated with dental caries. J Pierre Fauchard Acad (India Section) 2010;24:53–61. [Google Scholar]
- 73.Singh J, Sharma A, Garg N, Lumbini P. Body mass characterization of dental diseases – A quantitative prospective study. Indian J Dent. 2012;3:68–71. [Google Scholar]
- 74.Mathur A, Mathur A, Jain M, Shah P, Pareek V, Prabu D, Kulkarni S. Dental caries experience among kindergarten school going children of India. J Ped Dent. 2011;21:1–5. [Google Scholar]
- 75.Hegde MN, Hegde P, Bhat R, Rao LN, Dahiya R. Prevalence of dental caries in anterior teeth in south Canara population – a three year epidemiological study. Indian J Appl Res. 2014;4:32–4. [Google Scholar]
- 76.Anu V, Kumar MS, Kumar PM, Babu AS. Sweet score and dental caries experience of 12–13 year old school children in Chennai. J Indian Assoc Public Health Dent. 2011;7:305. [Google Scholar]
- 77.Bharateesh JV, Kokila G. Association of root caries with oral habits in older individuals attending a rural health centre of a dental hospital in india. J Clin Diagn Res. 2014;8:ZC80–2. doi: 10.7860/JCDR/2014/8771.5165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Poorani S, Chandana CS. Prevalence of dental caries among Chennai population. J Pharm Sci Res. 2015;7:895–6. [Google Scholar]
- 79.Kaur M, Kaur S. Assessment of dental caries in subject’s age ranged 20-60 years. J Adv Med Dent Sci Res. 2018;6:12–4. [Google Scholar]
- 80.Bhardwaj VK. Dental caries prevalence in individual tooth in primary and permanent dentition among 6-12-year-old school children in Shimla, Himachal Pradesh. Int J Health Allied Sci. 2014;3:125–8. [Google Scholar]
- 81.Sharma P, Sharma K. Epidemiology of dental caries among adolescent Gaddi Rajputs of Himachal Pradesh: Spatial and altitudinal differences. Ind J Phys Anthrop Hum Genet. 2011;30:249–58. [Google Scholar]
- 82.Yashoda R, Anuradha KP, Baskar DJ, Hiremath SS. Dental caries prevalence and treatment needs among davangere preschool children. J Indian Assoc Public Health Dent. 2011;2011:193–201. [Google Scholar]
- 83.Ganesh A, Ingle N, Chaly P, Reddy C. Sugar consumption and dental caries experience in 12 and 15 year old children in Chennai. J Indian Assoc Public Health Dent. 2011;9:462–73. [Google Scholar]
- 84.Garkoti PD, Singh RK, Rawat CMS, Pandey S. Prevalence of dental caries among primary school children of Haldwani: A cross sectional study. J Evol Med Dent Sci. 2015;4:7096–100. [Google Scholar]
- 85.Kakanur M, Nayak M, Patil SS, Thakur R, Paul ST, Tewathia N. Exploring the multitude of risk factors associated with early childhood caries. Indian J Dent Res. 2017;28:27–32. doi: 10.4103/ijdr.IJDR_35_16. [DOI] [PubMed] [Google Scholar]
- 86.Yavagal PC, Singla H. Prevalence of dental caries based on personality types of 35-44 years old residents in davangere city. J Oral Biol Craniofac Res. 2017;7:32–5. doi: 10.1016/j.jobcr.2016.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Shekar C, Cheluvaiah MB, Namile D. Prevalence of dental caries and dental fluorosis among 12 and 15 years old school children in relation to fluoride concentration in drinking water in an endemic fluoride belt of Andhra Pradesh. Indian J Public Health. 2012;56:122–8. doi: 10.4103/0019-557X.99902. [DOI] [PubMed] [Google Scholar]
- 88.National Oral Health Care Program Implementation Strategies, Project of DGHS, MOH and FW. of India, Submitted by Hari Prakash and Naseem Shah. New Delhi: Department of Dental Surgery, AIIMS, Ansari Nagar; 2004. [Google Scholar]
- 89.Miglani S. Burden of dental caries in India: Current scenario and future strategies. Int J Clin Pediatr Dent. 2020;13:155–9. doi: 10.5005/jp-journals-10005-1733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Rasidi MQZBM, Gheena S. The prevalence of dental caries in 18 to 30 years individual associated with socio-economic status in an outpatient population visiting a hospital in Chennai. Biomed Pharmacol J. 2018;11:1295–1300. [Google Scholar]
- 91.Yazdanian M, Armoon B, Noroozi A, Mohammadi R, Bayat AH, Ahounbar E, et al. Dental caries and periodontal disease among people who use drugs: A systematic review and meta-analysis. BMC Oral Health. 2020;20:44. doi: 10.1186/s12903-020-1010-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Musoke D, Boynton P, Butler C, Musoke MB. Health seeking behaviour and challenges in utilising health facilities in Wakiso district, Uganda. Afr Health Sci. 2014;14:1046–55. doi: 10.4314/ahs.v14i4.36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Chankanka O, Marshall TA, Levy SM, Cavanaugh JE, Warren JJ, Broffitt B, et al. Mixed dentition cavitated caries incidence and dietary intake frequencies. Pediatr Dent. 2011;33:233–40. [PMC free article] [PubMed] [Google Scholar]
- 94.Rugg-Gunn AJ, Al-Mohammadi SM, Butler TJ. Effects of fluoride level in drinking water, nutritional status, and socio-economic status on the prevalence of developmental defects of dental enamel in permanent teeth in Saudi 14-year-old boys. Caries Res. 1997;31:259–67. doi: 10.1159/000262409. [DOI] [PubMed] [Google Scholar]
- 95.Melgar RA, Pereira JT, Luz PB, Hugo FN, Araujo FB. Differential impacts of caries classification in children and adults: A comparison of ICDAS and DMF-T. Braz Dent J. 2016;27:761–6. doi: 10.1590/0103-6440201600990. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data set used in the current study has been sourced from PubMed, Google Scholar and Science direct, Cochrane, and Scopus indexed articles. Besides the data mentioned in the article, additional data can be made available on request.