

Abstract
Adults are thought to show a sleep-stress spiral in which greater stress worsens sleep quality, which amplifies stress, which leads to worse sleep. This study examined whether adolescents show a similar spiral, and if so, whether coping self-efficacy—believing one can cope with stress—interrupts the spiral. Temporal dynamics of perceived stress, sleep quality, and coping self-efficacy were tracked in 381 9th graders (49% female, mean age 14.43, age range 14–16) using daily surveys across two school weeks (3184 observations). Though expected associations were evident between individuals, only a unidirectional path was found within individuals from sleep quality to perceived stress via coping self-efficacy. This challenges the conventional bidirectional understanding of sleep-stress relations and suggests coping self-efficacy as an intervention target.
Keywords: stress, sleep, coping self-efficacy, temporal, Bayesian, dynamic structural equation models
Introduction
For many, adolescence is a time of increased stress (Gunnar, Wewerka, Frenn, Long, & Griffs, 2009; Hollenstein & Lougheed, 2013) and worse sleep (Roberts, et al., 2009), a potent combination that increases risk for mental health problems (Owens & Adolescent Sleep Working Group, 2014; Short, Booth, Omar, Ostlundh, & Arora, 2020). Prior research in adults suggests bidirectional links between perceived stress and sleep that can create a downward spiral in well-being (Kahn, Sheppes, & Sadeh, 2013). It is not yet clear, however, whether and how this downward spiral plays out day to day in the lives of adolescents. Moreover, it is crucial to understand what factors might disrupt this spiral and buffer adolescents against negative emotional and behavioral consequences. Because new school settings are a valuable test-bed to understand how stress related to transitions and peer dynamics interacts with poorer sleep (Roberts, et al., 2009), the present study examined 9th graders in the United States to assess whether a similar spiral is evident, and if so, to see whether students’ beliefs in their ability to cope with stress can interrupt this spiral.
The Stress-Sleep Link in Adolescence
Adolescence often involves a number of stressful changes, including the transition to high school (Lee, et al., 2019; Rudolph et al., 2001). However, the impacts of these changes are not uniform. Past research indicates that perceived stress in adolescents increases with age (Hampel & Petermann, 2006) and is greater for females (Hampel & Petermann, 2006; Wiklund, et al., 2012), lower-SES students (Dowd, Palermo, Chyu, Adam, & McDade, 2014; Finkelstein, Kubzansky, Capitman, & Goodman, 2007; Huynh & Chiang, 2018), and Black relative to White students (DeSantis, et al., 2007; Dowd, Palermo, Chyuu, Adam, & McDade, 2014; Valois, Zullig, & Hunter, 2015). Adolescence is also associated with decreased sleep quality (Bartel, Gradisar, & Williamson, 2015; Crowley, Acebo, & Carskadon, 2007; Sadeh & Gruber, 2002), due in part to increased academic and social responsibilities, late-night screen use, and the mismatch between work and school schedules and circadian rhythm delay (Carskadon & Wolfson, 2003; Owens & Adolescent Sleep Working Group, 2014) coupled with early school start times. Sleep quality has strong associations with adolescent depression (Alfano, Zakem, Costa, Taylor, & Weems, 2009) and is impaired in low-SES (Huynh & Chiang, 2018) and minority students experiencing discrimination (Majeno, et al., 2018; Wang & Yip, 2020). One important question is whether changes in stress precede sleep or vice versa.
Both cross-sectional and experimental research in adults suggests a bidirectional spiral between stress and sleep (Kahn, Sheppes, & Sadeh, 2013). Cross-sectional diary studies find that higher levels of stress, negative affect, and anxiety are associated with a lower percentage of the night spent asleep (Åkerstedt, et al., 2007), longer time to fall asleep, shorter total sleep time, and worse sleep quality (Kalmbach, et al., 2014). Experimental stress induction studies have shown that stressful anticipation leads to poor sleep quality and reduced total sleep time (Gross & Borkovec, 1982; Guastella & Moulds, 2007). Experimental sleep deprivation causes next-day heightened negative reactivity (Goldstein & Walker, 2014; Ben Simon et al., 2020) and negative attentional bias (Krause, et al., 2017); increased anger, stress, and frustration in the face of challenges (Minkel, et al., 2012); and an exaggerated stress response during an anxiety-provoking task (Yang et al., 2012). In general, studies in adults find stronger associations between negative affect and self-reported sleep quality compared to objective sleep measures such as actigraph-measured sleep efficiency (Konjarski, et al., 2018).
Far less is known about the association between sleep and stress in adolescents. Cross-sectionally, academic stress (Yan, Lin, & Su, 2018) and racial/ethnic discrimination–related stress (Majeno, et al., 2018) appear to be correlated with sleep quality in adolescence. In terms of the pathway from stress to sleep, researchers have focused on perceived stress, referring to an individual’s perception that demands on them outstrip their resources (Blascovich & Mendes, 2010), and on subjective perceptions of sleep quality. This line of research found that perceived stress impairs subsequent sleep quality among high schoolers (Baum, et al., 2014). For the pathway from sleep to perceived stress, a qualitative meta-analysis found that poor sleep quality was associated with anxiety and depression symptoms in children and teens in both community and clinical samples (Gregory & Sadeh, 2012). A large cognitive-behavioral and mindfulness-based sleep intervention showed that behavioral issues could be reduced by improving sleep quality (Blake, et al., 2017). One recent longitudinal study in a 7th grade cohort (Kortesoja, et al., 2020) indicated that emotional and behavioral difficulties preceded poor and shortened sleep duration three and five years later. This effect was larger than the effect in the reverse direction, suggesting an asymmetric bidirectional relationship over a timescale of several years. Another study, a brief three-day ecological momentary assessment, also found bidirectional evidence: Higher self-reported stress measured five times a day was associated with shorter subsequent sleep duration, and shorter sleep duration and lower sleep efficiency (the percentage of time in bed spent asleep, considered a quantitative corollary of sleep quality) were associated with higher next-day perceived stress (Doane & Thurston, 2014). Over the longer term, poor sleep can have serious consequences, including the development of depressive symptoms, higher risk-taking behaviors, and increased risk of suicide (Lee, et al., 2012; Owens & Adolescent Sleep Working Group, 2014; Palmer, et al., 2018). However, the authors are not aware of any prior study that simultaneously examines both temporal orders at once through a daily diary study lasting more than three days, making it difficult to determine whether the bidirectional stress-sleep spiral seen in adults is evident in adolescents’ daily lives.
Coping Self-Efficacy: Interrupting the Downward Spiral?
If there is indeed a stress-sleep spiral in adolescence, one crucial question is how its downward course might be interrupted. Given that there are two steps in the spiral, one approach would be to intervene on adolescents’ sleep. However, it is notoriously difficult for adolescents to alter their sleep timing, given structured school schedules and social demands, or to access and complete sleep therapies (Moseley & Gradisar, 2009; Meltzer, et al., 2010; Owens, 2014).
A second approach would be to intervene on the side of subjective perceptions of stress. In particular, one key source of stress is an individual’s perception that they are unable to manage ongoing challenges and demands (Compas et al., 1991). The cognitive theory of stress and coping suggests that people make a primary appraisal of how a stressor will their well-being, as well as a secondary appraisal of their own coping resources (Folkman, 1984). When people believe that they cannot manage their stress, they experience additional stress engendered by the sense that they cannot manage the demands they are facing (Benight & Bandura, 2004). In contrast, even under conditions of high stress, people who believe that they are able to manage stress perceive the stress as being less toxic (Bandura, 1986; Schwarzer & Jerusalem, 1992). This belief that one is able to manage one’s own stress is known as coping self-efficacy (Bandura, 1993). In a similar vein, theories of personal agency in the stress process (Pearlin, et al., 1981; Thoits, 2006) argue that individuals with a sense of control, confidence, and optimism about having the resources to cope are more likely to respond effectively to stress because they select situations and roles in which they believe they have agentic control.
There is mounting research in the field about how altering mindsets relating to stress can powerfully shift stress-related health outcomes (Jamieson, Crum, Goyer, Marotta, & Akinola, 2018). In one study of adolescents, coping self-efficacy was shown to be positively related to well-being via reduced use of maladaptive coping strategies (Cicognani, 2011). In inner-city adolescents, having a sense of personal control over stressors mediates the relationship between a variety of stress domains and depressive symptom severity (Deardoff, Gonzales, & Sandler, 2003). Given the potential stress-modulating effects of coping self-efficacy, it is noteworthy that coping skills and self-efficacy more broadly dip during adolescence (Cracco, Goossens, & Braet, 2017; Hampel & Petermann, 2006; Schunk & Meece, 2005), with lower coping self-efficacy associated with greater depression symptom severity (Rudolph, Kurlakowsky, & Conley, 2001; Thompson, et al., 2010), socioeconomic status (Finkelstein, Kubzansky, Capitman, & Goodman, 2007; Waschbusch, Sellers, LeBlanc, & Kelley, 2003), sex (Bacchini & Magliulio, 2003; Schunk & Meece, 2005; Valois, Zullig, & Hunter, 2015), and certain ethnic and racial groups (Schunk & Meece, 2005; Valois, Zullig, & Hunter, 2015; Wang & Yip, 2020). Coping self-efficacy appears to mediate the relationship between lower socioeconomic status and perceived stress (Finkelstein, Kubzansky, Capitman, & Goodman, 2007; Glassock, Andersen, Labriola, Rasmussen, & Hansen, 2013) as well as the association between early childhood abuse and attention-deficit hyperactivity disorder (Singer, Humphreys, & Lee, 2016). Self-efficacy also seems to impact perceived stress as well as sleep. A large longitudinal study of 15-year-olds found that the effects of baseline perceived school-related stress on life satisfaction over four years were moderated by higher general self-efficacy at baseline (Burger & Samuel, 2017). General self-efficacy was also found to moderate the effects of a cognitive-behavioral and mindfulness-based sleep intervention in a large adolescent sample, such that the intervention was most effective for individuals with moderate to high self-efficacy (Blake, et al., 2018). One finding in the context of adult social anxiety disorder suggests that it is not the specific coping strategy used that predicts improvement, but the extent of self-efficacy reported for people’s ability to cope with stressors (Goldin et al., 2012). This supports work by Bonanno and Burton (2013) suggesting that regulatory flexibility rather than efficacy of a single coping strategy in the face of stressors is more predictive of well-being. However, the role of coping self-efficacy in the context of adolescents’ daily life perceived stress and sleep processes has not yet been examined.
Current Study
In light of the conflicting literature in adults and the paucity of research in adolescent samples, the goal of this study is to understand the bidirectional associations among daily reports of perceived stress, sleep quality, and coping self-efficacy in adolescents. For this study, daily diaries were administered to 9th grade adolescents across two weeks of school. Hypotheses concerning temporal associations from one night to the next school day and from one school day to that night were tested. For the first hypothesis, a negative bidirectional association between perceived stress and sleep quality was expected (Baum, et al., 2014; Gregory & Sadeh, 2012). Second, a negative bidirectional daily association between coping self-efficacy and perceived stress was predicted (Bandura, Reese, & Adams, 1982; Tamir, et al., 2007). Third, based on exploratory findings in a held-out sample, it was predicted that sleep quality would be positively associated with next-day coping self-efficacy but that coping self-efficacy would not be associated with next-night sleep quality, due to other factors (e.g., social and academic pressures, school start time) that exert a stronger influence on sleep quality in high schoolers.
The model tested also included demographic covariates known to have robust associations with perceived stress, sleep quality, and coping self-efficacy in order to determine whether temporal associations held above and beyond group differences. Specifically, the model adjusted for age and pubertal status as indices of developmental stage, depression status, maternal college education as an index of socioeconomic status (SES), sex, and race. School was also included as a covariate to adjust for any between-school differences in the sample. No specific a priori hypotheses were pre-registered as to how each of these adjustment covariates would be associated with perceived stress, sleep quality, and coping self-efficacy, given the complexity of covariation once all variables were included in the model.
Several key features of this study’s approach bear emphasis. First, most adolescent studies focus on just one half of the stress-sleep spiral, whereas this study tests both directions using a powerful new temporal modeling approach known as dynamic structural equation modeling (DSEM; Hamaker, et al., 2018). Second, this study uses a repeated design and considers all three hypothesized elements—sleep quality, perceived stress, and coping self-efficacy—to determine how these associations play out over time during a school week. Third, this study focuses on subjective sleep quality in order to capture the contribution of students’ holistic perceptions of sleep.
Methods
Sample
As part of the Texas Longitudinal Study of Adolescent Stress Resilience: Daily Diary Sample (TLSASR:DDS) (Yeager, et al., 2016), data were collected from 9th-graders in five diverse schools in Austin, Texas, after approval from the University of Texas at Austin Institutional Review Board. About 1,200 students were recruited. The present study consists of all 556 control group participants who did not receive a randomized intervention trial, who provided their written consent to participate in the study, and who answered questions about implicit theories and internalizing symptoms (see Lee et al., 2019, for details).
As a first step, exploratory models were developed with a subset of the data using one school (n = 175 from 15 classrooms; 92 females, 83 males). Based on those exploratory findings, confirmatory hypotheses were pre-registered on the Open Science Framework: https://osf.io/3tdeq/register/564d31db8c5e4a7c9694b2be. For the present study, hypotheses were tested on held-out data from the remaining four schools. A limited number of constructs and a small number of hypotheses were chosen to prevent false positives while performing confirmatory analyses on the remaining three schools. The results were also replicated using multiple analytic methods, and ultimately the method that best matched the structure of the data was chosen after unblinding the data.
Data collection took place in fall 2016 or 2017 and consisted of baseline survey measures collected during one class period, which took around 30 to 45 minutes to complete, followed one to two weeks later by self-reported daily diaries obtained during 10 school days (Monday through Friday) over two consecutive weeks of school.
Measures
Daily Diary.
The following measures were collected via online daily surveys in the classroom or in the school computer labs using desktops, laptops, or smartphones between 1:00 and 4:30 p.m. in a once-daily diary each weekday (Monday through Friday) across two consecutive weeks of school, totaling up to 10 diaries. Each participant completed the daily diary during the same class period throughout the two weeks to keep the time period constant within person, varying across participants depending on their class schedules. The daily survey included roughly 60 items (depending on students’ endorsed experiences), from which a subset was chosen to assess the constructs of interest.
Coping self-efficacy (CSE)
Coping self-efficacy (CSE) was measured using an averaged composite of three items (Cronbach’s alpha: 0.75; 95% CI = 0.74, 0.77): “Today I felt confident that I could handle the stresses that I experienced,” “I felt like I could handle the negative thing that happened to me today,” and “I feel overwhelmed by the negative things that happened to me today” (reverse scored) (Yeager, Lee, & Jamieson, 2016). Responses to these three items were made on a 7-point radio button scale from “Strongly disagree (1)” to “Strongly agree (7)”. The test-retest reliability from the first week to the second week of the diary was r = 0.38 (t(1390) = 15.12, p < 0.0001). These items have shown convergence with cortisol measures (Lee, et al., 2019). The association between the coping self-efficacy composite measure and an averaged composite of global scores on the Perceived Stress Scale (Cohen & Williamson, 1988) and Child Depression Inventory (Kovacs, 1992) at baseline was moderate (Pearson’s r = −0.35, t(373) = −7.24, p < 0.0001), suggesting further criterion validity.
Perceived stress (PS)
Perceived stress (PS) was operationalized using a rating on a 7-point radio button scale from “Strongly disagree (1)” to “Strongly agree (7)” in response to the daily diary question “Today I felt very stressed.” The test-retest reliability from the first week to the second week of the diary was r = 0.42 (t(1390) = 16.84, p < 0.0001). This single item has shown convergence with cortisol measures (Lee, et al., 2018), as well as relevant baseline trait measures. Mean ratings of this item across the two weeks were moderately to strongly associated (Pearson’s r = 0.49, t(343) = 10.31, p < 0.0001) with baseline ratings on the Perceived Stress Scale (Cohen & Williamson, 1988), suggesting reasonable criterion validity.
Sleep quality (SQ)
Sleep quality (SQ) was measured using a rating on a 5-point radio button scale from “Very good (5)” to “Very bad (1)” in answer to the daily diary question “How would you rate your sleep quality last night?”, which was adapted from the Pittsburgh Sleep Quality Index (Buysse, et al., 1989). This item is the gold standard for daily sleep diaries (Carney, et al., 2012). Test-retest reliability from the first week to the second week of the diary was r = 0.39 (t(1364) = 15.49, p < 0.0001). The item showed moderate association with a single item assessing “difficulty sleeping” over the past two weeks (responses from 1, “Never,” to 5, “All the time”) at baseline (Pearson’s r = −0.37, t(341) = −7.40, p < 0.0001), suggesting reasonable criterion validity.
Within-person covariates: Time of day.
Time of day of the survey response was adjusted for as a within-person covariate because the timing of responses has been shown to influence mood (Díaz-Morales, Escribano, & Jankowski, 2015). It was coded as the time since midnight at which the survey was filled out and varied between participants but remained roughly the same across different diary days for the same participant.
Within-person covariates: Diary day.
To adjust for differences due to school activities, weekend alterations to sleep schedules, or changes in responses over the course of the diary period, the model adjusted for the day of diary response. Diary day was represented as 0 through 11, indicating which day during the diary period the survey was filled out; days 6 and 7, Saturday and Sunday, were included as empty rows for the purposes of modeling auto-correlation.
Within-person covariates: Negative affect in response to daily events.
Mean intensity of negative affect in response to daily events was estimated as the mean of two rating questions. Participants were asked to write briefly about two negative things that happened today or that they thought a lot about today. Participants then rated each negative experience, answering the question “How negative would you say this experience was?” with radio button responses of “Not at all negative” (1), “Slightly negative” (2), “Moderately negative” (3), “Very negative” (4), or “Extremely negative” (5). The test-retest reliability from the first week to the second week of the diary was r = 0.39 (t(1267) = 14.87, p < 0.0001). The association between individuals’ average intensity rating of negative events and an averaged composite of baseline global scores on the Perceived Stress Scale (Cohen & Williamson, 1988) and Child Depression Inventory (Kovacs, 1992) was moderate (Pearson’s r = 0.25, t(369) = 4.89, p < 0.0001).
Between-person covariates.
Demographic covariates known to impact perceived stress, sleep quality, and coping self-efficacy were measured and included in the model in order to examine whether temporal associations among the three constructs of interest held after adjusting for between-person differences. At baseline, participants filled out the following measures via online survey in the classroom or in the school computer labs: age, sex, race, socioeconomic status, depression symptoms, and stage of pubertal development.
Socioeconomic status.
Socioeconomic status was operationalized with an item that asked participants to report their mother’s highest level of education, since students can more accurately self-report it compared to income and it shows consistent associations with academic performance (Entwisle & Astone, 1994; Mesmin, Hanselman, Buontemp, Tipton, & Yeager, 2019).
Depression symptoms.
At baseline, participants completed the full Child Depression Inventory (CDI), excluding the suicidal ideation item (Kovacs, 1992). Higher scores on the CDI index greater self-reported depressive symptoms, with scores above 19 indicating moderate to more severe symptoms according to the validated cutoff for the upper 10% of the distribution in a public school population (Smucker, Craighead, Craighead, & Green, 1986; Timbremont, Braet, & Dreessen, 2004).
Pubertal development.
Participants also self-reported their pubertal development at baseline using the Pubertal Developmental Scale, which goes from Stage 1 (pre-pubescent) to Stage 5 (adult-like genitalia, pubic hair, and growth) (Marshall & Tanner, 1969; Marshall & Tanner, 1970).
Analytical Methods
First, to identify the extent of within- and between-person variance in each variable, intra-class correlations were calculated using the ICC function in the R package merTools (Knowles, Frederick, & Whitworth, 2019). ICCs indicating that 30% or greater variance was accounted for by within-individual variation provided adequate rationale for continuing forward with a multilevel modeling approach.
Next, for each association between perceived stress (PS), sleep quality (SQ), and coping self-efficacy (CSE), variation accounted for by between-person as well as within-person effects was tested (Curran & Bauer, 2011). Analyses were performed with a dynamic structural equation model (DSEM; Hamaker, et al., 2018), which is a structural equation model composed of a series of Bayesian linear models testing between-person associations among average perceived stress, sleep quality, and coping self-efficacy, as well as within-person temporal associations (see schematic in Figure 1). Each variable served as a predictor and as an outcome in the model, and covariates were included at the between- and within-person levels of the model. Figure 2 shows the full specification of the model with both between- and within-person components. Although ideally students would have been nested within school and diary responses nested within student, there were not enough observations at the school level to reach convergence with a three-level nested model. The model therefore instead adjusted for school as a covariate at the between-person level.
Figure 1:
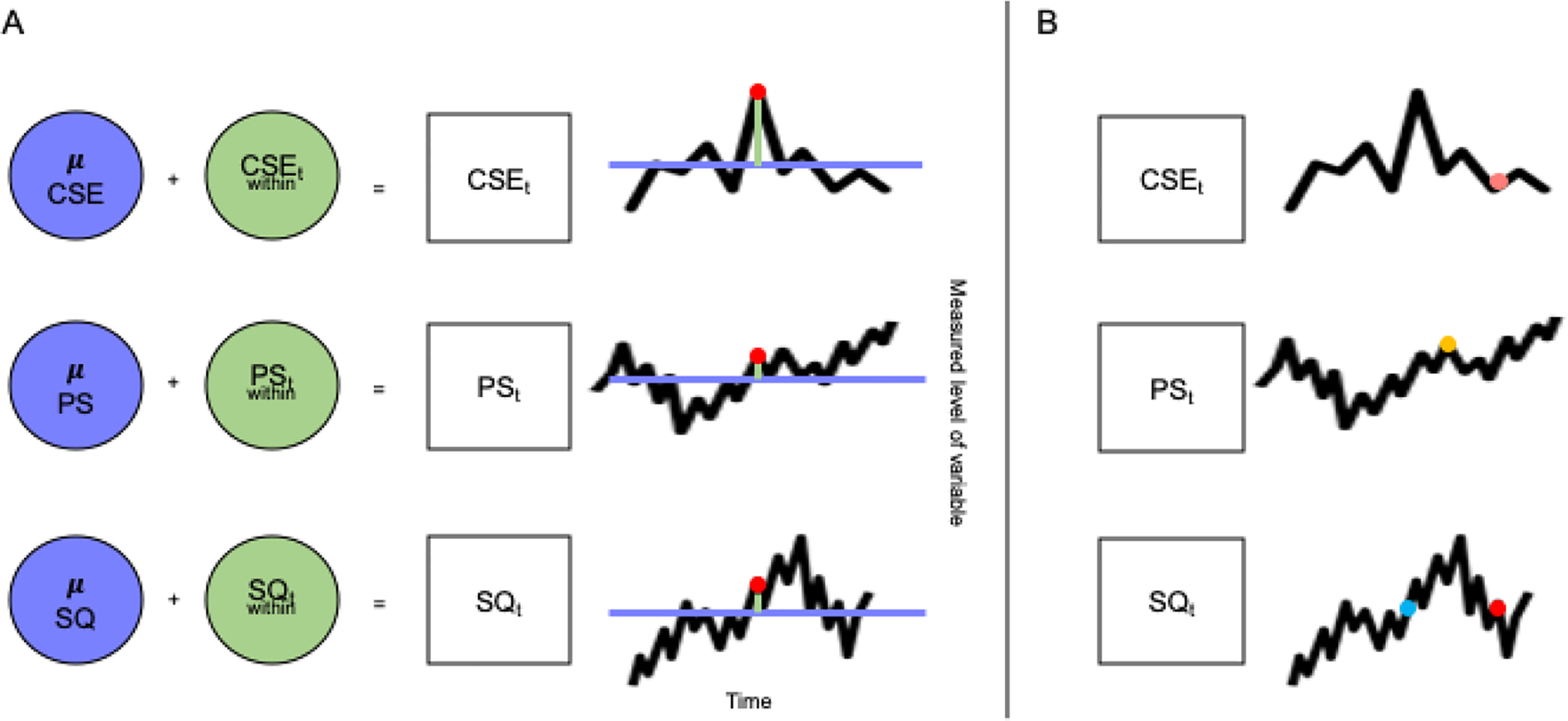
A: An Idealized Representation Breaking Down the Variables of Interest into Between-Person and Within-Person Components. Coping self-efficacy (CSE), perceived stress (PS), and sleep quality (SQ) time series measurements can be separated into between-person (purple) and within-person (pale green) components. A given measurement at timepoint t (represented by a red dot) can be decomposed into a mean across the individual’s entire time series of measurements (represented by the purple horizontal line) as well as a deviation at timepoint t from the participant’s individual mean (represented by the pale green line).
“μ” indicates the mean level of the variable, and the subscript t indicates a measurement at a given timepoint.
B: An Idealized Representation of Temporal Associations in Dynamic Structural Equation Models (DSEM). DSEM makes it possible to model how a variable, for example sleep quality, at timepoint t (represented by a red dot in the bottom time series) is predicted by 1) itself at an earlier timepoint (represented by a blue dot), called an auto-regressive association; 2) another variable at the same timepoint t (in this example, coping self-efficacy, represented by a pink dot in the top time series); or 3) another variable at an earlier timepoint (in this example, perceived stress, denoted by a yellow dot in the middle time series).
Figure 2: A Representation of Hypothesized Model Associations.
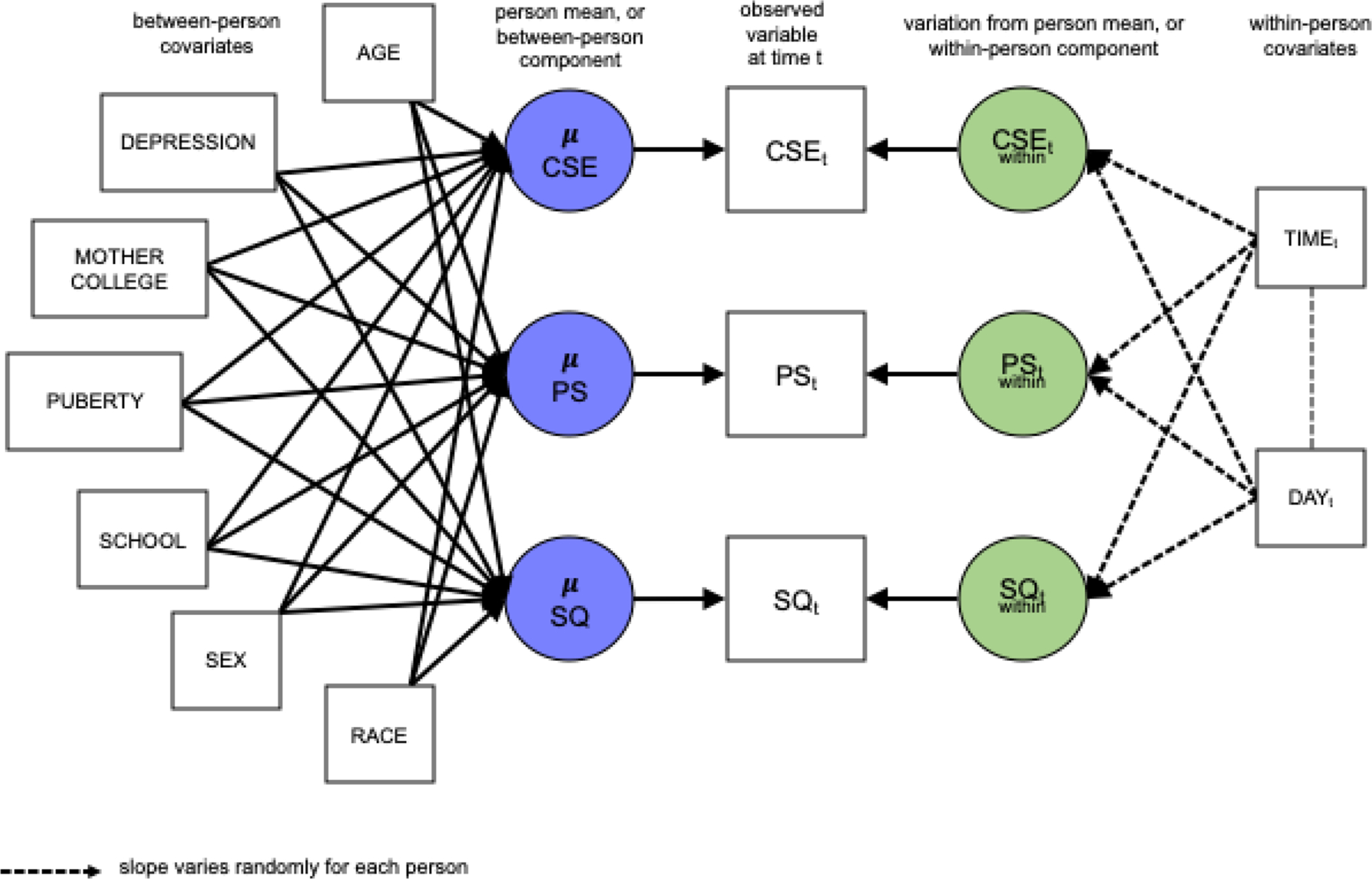
This figure visually represents the full specification of the dynamic structural equation model (DSEM). Observed variables of coping self-efficacy (CSE), perceived stress (PS), and sleep quality (SQ) measured daily across two weeks are denoted with squares, and latent variables are denoted with circles. Observed variables are constructed from latent between-person (purple) and within-person (green) components. Dotted arrows indicate that paths are allowed to vary for each individual. To test a hypothesis that a given path (represented with a line) in the DSEM is significant, the MPlus software calculates a conditional estimate given all other paths in the model and 95% Bayesian credible intervals, which indicate whether the true value of the conditional estimate is likely to include 0 (indicating no association).
“μ” indicates the mean level of the variable, and the subscript t indicates a measurement at a given timepoint.
At the within-person level, the model tested temporal associations using time-lagged variables, by modeling the effect of variable x at time t on variable y at time t+1 (one day later), controlling for all other paths in the model (see Figure 2). This meant that outcomes reflected changes from time t to time t+1. Because surveys of the previous night’s sleep quality were completed during the school day at the same time as the rest of the self-report items, it was not possible to lag the sleep quality variable by one day. At the within-person level, time of day of survey response was accounted for, given that students in different classrooms filled out surveys at slightly different times during the day. Diary day (0 through 11) was also accounted for to adjust for variation related to making responses earlier compared to later in the diary period, as well as for variation by day of the week. At the between-person level, the model adjusted for the following demographic covariates: age, depression symptoms, maternal education level, pubertal status, school, sex, and race.
DSEM, implemented in MPlus (Muthén & Muthén, 2017), uses Bayesian linear mixed models for each pathway tested, which made it possible to constrain the prior estimates for regression parameters based on the known possible distribution of outcomes. Another benefit of using Bayesian models over frequentist models is that they enable effect size point estimates with credible intervals, meaning that it is possible to report that a regression estimate lies within a certain interval with 95% certainty (McElreath, 2016).
The models used for analysis can be expressed with the following equations (Curran & Bauer, 2011):
which expresses a linear regression model predicting an outcome variable y as a function of a predictor x. In this equation, β0i and β1i represent the respective intercept and linear slope for individual i, xti represents the observed predictor value at time t for individual i, and rti represents the residual error at time t for individual i.
which, when substituted into Equation 1, reduce to yti = (γ00 + γ10xti) + (u0i + u1ixti + rti), where γ00 and γ10 represent the sample’s mean intercept and slope (i.e., the “fixed effects”), and u0i and u1i represent each individual’s deviations from these respective means (i.e., the “random effects”).
Using the MPlus software (Muthén & Muthén, 2017) with the model class “Two-level Random,” a Bayes estimator with the Gibbs algorithm for Markov chain Monte Carlo was used to implement the DSEM. Two chains on two cores for 11500 iterations, with one iteration interval for thinning, were run. MPlus’ default diffuse priors were used, following Hamaker, et al. (2018): a univariate prior with mean of zero and variance of ten for means and intercepts, and an inverse Wishart distribution with zero matrix and degrees of freedom set to the total number of variables minus one. MPlus model syntax is included in Supplementary Materials.
According to current best practices (Asparouhov, Hamaker, & Muthén, 2018), a regression coefficients was determined to be statistically significant if its 95% credible interval—which indicates the range of values within which it can be said with 95% certainty that the posterior parameter value falls (McElreath, 2016)—did not include zero, and to be statistically non-significant if it did. Although credible intervals describe parameter uncertainty (Gray, Hampton, Silveti-Falls, McConnnell, & Bausell, 2015) rather than comparing the alternative hypothesis to a null (as in frequentist hypothesis testing), it is difficult to do equivalent hypothesis testing on a DSEM. The current recommendation, used in the present study, is to “evaluate significance of individual parameters through the credibility intervals” (Asparouhov, Hamaker, & Muthén, 2018, pp. 366).
Since DSEM is well-suited to handle missingness, no participants were excluded based on a minimum usable number of surveys or missing baseline data in order to make greatest use of available data. MPlus imputed 50 data values by treating them as random effects and sampling from their conditional posteriors (for instance, neighboring time observations, individual’s autoregressive parameter, and residual variance) at each iteration of the Monte Carlo Markov Chain algorithm (Hamaker, et al., 2018).
Results
Preliminary Analyses
One subject was removed because, at age 18, they were significantly advanced in age and pubertal stage relative to the rest of the sample. The final sample from the three schools consisted of 381 9th-graders in four cohorts (two separate cohorts from the same school were collected during two different academic years). There were 188 self-identified females (49%), 174 males (45%), and 19 unreported-sex individuals in the sample, with a mean age of 14.43 (SD: 0.51, min: 14, max: 16). Mean pubertal status on the Pubertal Development Scale was 3.10 out of 5 (SD: 0.57), which matches the third Tanner stage of further penis lengthening and testes growth (boys), further breast and areola enlargement without separation (girls), darkening and coarsening pubic hair growing laterally, and 7–8 cm height increase (Marshall & Tanner, 1969; Marshall & Tanner, 1970). There were 192 white/Caucasian, 130 Hispanic/Latinx, 22 Asian/Asian-American, 19 Black/African-American, 12 multi-racial or other race, and 2 Pacific-Islander students in the sample. In the sample, 142 students reported a maternal education level of a bachelor’s degree or higher, and 75 students met the threshold for clinical depression (score >19 on the Child Depression Inventory; Kovacs, 1992).
Participation rate for baseline responses to demographic survey items was fairly high (17% of responses were missing). Participation rate for the diary surveys was high across days (mean missing days 16%, SD: 22%, min. 0%, max. 100%). Rates of missingness were nearly identical across the three variables of interest: The mean percentage of missing diary responses for the sleep quality measure was 16% (SD: 22%), the mean percentage of missing diary responses for the sleep quality measure was 17% (SD: 22%), and the mean percentage of missing diary responses for the coping self-efficacy measure was 16% (SD: 22%). Running bootstrapped tests of randomness indicated that mean rates of missingness for each demographic group lay within the 95% confidence intervals of the means in randomly shuffled samples, indicating no bias in the pattern of missingness.
Across all participants for all two weeks of diary responses, the mean daily perceived stress level reported was 3.8 (SD: 1.8), mean sleep quality was 3.3 (SD: 1.1), and mean coping self-efficacy was 5.0 (SD: 1.3). The intra-class correlation (ICC) for perceived stress was 0.45, indicating that around 55% of the variance in sleep quality was accounted for by within-individual variance. The ICC for sleep quality was 0.34, and the ICC for coping self-efficacy was 0.49. For all three variables, this indicated sufficient within-individual variation to motivate using a multilevel analytic strategy.
Within a given student’s two weeks of diary responses, the average unstandardized sleep quality rating was 2.93 on a 5-point scale [95% credible interval (CI): 2.36, 3.44], the average unstandardized perceived stress rating was 4.59 on a 7-point scale [CI: 3.81, 5.40], and the average unstandardized coping self-efficacy rating was 4.57 on a 7-point scale [CI: 3.83, 5.18].
Dynamic Structural Equation Model (DSEM) Convergence
The model was fit on 4446 observations (10 independent variables, 5 dependent variables, 9 latent variables; estimated number of parameters = 37689.980) and had a Deviance Information Criterion of −99893.230. A potential scale reduction (PSR) value of 1.096 was reached, indicating acceptable model convergence (Asparouhov & Muthén, 2010). Although ideally the PSR falls below 1.05, a larger PSR value indicates more variation in estimates across the Monte Carlo Markov chains, meaning that posterior standard deviation values and therefore credible intervals are slightly larger. Therefore, it was a trade-off between a slightly higher convergence criterion and more conservative hypothesis testing. Below, standardized posterior regression estimates are reported with 2.5% and 97.5% Bayesian credible intervals (CI).
Between-Person Results
As expected, the model confirmed that there were moderate to strong significant associations among the three constructs of interest: sleep quality (SQ), perceived stress (PS), and coping self-efficacy (CSE) (see Figure 3, Table 1). That is, students’ average levels of sleep quality, perceived stress, and coping self-efficacy across the two weeks were significantly related to one another. Across the two-week diary period, students reporting better sleep quality than average for the sample reported lower average perceived stress (−0.44 [CI: −0.56, −0.30]) and higher average coping self-efficacy (0.42 [CI: 0.29, 0.54]). Students reporting higher coping self-efficacy than average for the sample reported lower average perceived stress (−0.71 [CI: −0.78, −0.62]). There was only one significant temporal association at the between-person level: On average, higher perceived stress was associated with lower subsequent sleep quality (−1.25 [CI: −2.56, −0.03]) (see Table 1).
Figure 3: Daily Coping Self-Efficacy, Perceived Stress, and Sleep Quality Correlate as Hypothesized When Adjusting for Many Person-Level Covariates.

Between-person model results indicate cross-sectional associations among coping self-efficacy (CSE), perceived stress (PS), and sleep quality (SQ) and show significant influences of some covariates on individuals’ mean levels. Arrows reflect direction, and line widths reflect magnitude of effects, with red signifying negative associations and green signifying positive associations. Lines without arrow heads show non-directional effects.
Purple circles with “μ” indicate mean levels of variables.
Asterisks indicate significance, meaning that the Bayesian 95% credible interval for the estimate does not include 0. Only significant associations are shown.
Table 1:
Between-person results of the DSEM. Standardized posterior estimates are listed with 95% credible intervals.
| Path | Fixed Effects (Between-Person Means) | 95% Credible Interval - Lower | 95% Credible Interval - Upper | Significance Level | R2 Averaged Across Individuals | Residual Variance | 95% Credible Interval - Lower | 95% Credible Interval - Upper | Significance Level |
|---|---|---|---|---|---|---|---|---|---|
| Mean Sleep Quality (SQ) | 4.099 | 3.161 | 5.012 | *** | 0.076*** | 0.924 | 0.849 | 0.973 | *** |
| Mean Perceived Stress (PS) | 3.873 | 3.160 | 4.578 | *** | 0.188*** | 0.812 | 0.721 | 0.894 | *** |
| Mean Coping Self-Efficacy (CSE) | 4.946 | 3.957 | 5.849 | *** | 0.185*** | 0.815 | 0.721 | 0.895 | *** |
| That Day Sleep Quality → Next Day Sleep Quality | −0.073 | −1.078 | 0.967 | N.S. | 0.344*** | 0.656 | 0.458 | 0.828 | *** |
| That Day Coping Self-Efficacy → Next Night Sleep Quality | −0.706 | −2.125 | 0.663 | N.S. | 0.221*** | 0.779 | 0.524 | 0.930 | *** |
| That Day Perceived Stress → Next Night Sleep Quality | −1.248 | −2.563 | −0.027 | * | 0.181*** | 0.819 | 0.623 | 0.941 | *** |
| Prev. Night Sleep Quality → That Day Coping Self-Efficacy | 0.654 | −0.504 | 1.972 | N.S. | 0149*** | 0.851 | 0.648 | 0.960 | *** |
| That Day Coping Self-Efficacy → Next Day Coping Self-Efficacy | −0.216 | −1.639 | 1.059 | N.S. | 0.290*** | 0.710 | 0.490 | 0.878 | *** |
| That Day Perceived Stress → Next Day Coping Self-Efficacy | −0.242 | −1.844 | 1.100 | N.S. | 0.208*** | 0.792 | 0.567 | 0.934 | *** |
| Prev. Night Sleep Quality → That Day Perceived Stress | −0.459 | −1.660 | 0.583 | N.S. | 0.241*** | 0.759 | 0.570 | 0.905 | *** |
| That Day Coping Self-Efficacy → Next Day Perceived Stress | 1.079 | −0.143 | 2.343 | N.S. | 0195*** | 0.805 | 0.592 | 0.930 | *** |
| That Day Perceived Stress → Next Day Perceived Stress | 0.981 | −0.093 | 2.139 | N.S. | 0.088*** | 0.912 | 0.792 | 0.975 | *** |
| Association Between Sleep Quality and Next Day Coping Self-Efficacy | 0.423 | 0.287 | 0.544 | *** | |||||
| Association Between Same Day Sleep Quality and Next Day Perceived Stress | −0.439 | −0.559 | −0.298 | *** | |||||
| Association Between Same Day Perceived Stress and Coping Self-Efficacy | −0.705 | −0.781 | −0.615 | *** | |||||
Significance level is represented as N.S. for p > 0.05,
for p <= 0.05,
for p <= 0.01, and
for p <= 0.001.
Associations Among Between-Person Means and Covariates
At the between-person level, there were significant associations between mean levels of sleep quality, perceived stress, and coping self-efficacy and demographic covariates (see Figure 3, Supplementary Table 1). This means that several individual differences accounted for significant variation in students’ overall levels of sleep quality, perceived stress, and coping self-efficacy. Greater severity of depression as assessed by the Child Depression Inventory (Kovacs, 1992) was associated with lower average sleep quality (−0.15 [CI: −0.27, −0.03]), higher average perceived stress (0.24 [CI: 0.13, 0.35]), and lower average coping self-efficacy (−0.29 [CI: −0.40, −0.18]) across the diary period. Students whose mothers did not attend a four-year college or higher (indexing socioeconomic status: SES) reported lower average coping self-efficacy across the diary period compared to those who did (−0.14 [CI: −0.25, −0.02]). Compared to females, males reported higher average coping self-efficacy (0.21 [CI: 0.10, 0.32]) and conversely lower average perceived stress (−0.23 [CI: −0.34, −0.11]) across the diary period. Finally, there was significant variation by school in average perceived stress across the diary period (−0.19 [CI: −0.30, −0.06]). The magnitudes of all associations were low to moderate, with the largest effects for depression, maternal education, and sex. These demographic associations are considered exploratory, as specific hypotheses about the direction or magnitude of effects were not pre-registered.
Within-Person Results
The model indicated that there were significant day-to-day auto-regressive associations for all three variables of interest (see Figure 4, Table 2). This means that a given individual’s reported coping self-efficacy, perceived stress, and sleep quality on one day were significantly related to the level of the previous day’s variables, indicating stability of all three variables from day to day. Sleep quality on a given night positively predicted sleep quality on the following night (0.13 [CI: 0.08, 0.19]). Coping self-efficacy on a given day positively predicted coping self-efficacy on the next day (0.16 [CI: 0.10, 0.21]), and perceived stress on a given day positively predicted coping self-efficacy on the next day (0.14 [CI: 0.09, 0.19]).
Figure 4: Daily Sleep Quality Directly and Indirectly Impacts Subsequent Perceived Stress Via Coping Self-Efficacy, But Not the Other Way Around, Challenging Bidirectional Hypothesis.

Within-person model results indicate that there are some unidirectional within-person time-lagged associations among coping self-efficacy (CSE), perceived stress (PS), and sleep quality (SQ), but do not support a bidirectional hypothesis. Green circles indicate daily levels of variables relative to their own mean. Arrows reflect direction (e.g., from prior night to current day, from current day to next night). Line widths reflect magnitude of effects, with red signifying negative associations and green signifying positive associations. Lines without arrow heads show cross-sectional (non-directional) within-person co-variation, known as “co-movements.” Dotted lines indicate that slopes are allowed to vary by individual.
Asterisks indicate significance, meaning that the Bayesian 95% credible interval for the estimate does not include 0. Only significant associations are shown.
Table 2:
Within-person results of the DSEM. Standardized posterior estimates are listed with 95% credible intervals.
| Path | Random Effects (Within-Person Variances) | 95% Credible Interval - Lower | 95% Credible Interval - Upper | Significance Level | R2 Averaged Across Individuals | Residual Variance | 95% Credible Interval - Lower | 95% Credible Interval - Upper | Significance Level |
|---|---|---|---|---|---|---|---|---|---|
| Mean Sleep Quality (SQ) | 0.219*** | 0.781 | 0.740 | 0.821 | *** | ||||
| Mean Perceived Stress (PS) | 0.259*** | 0.741 | 0.696 | 0.778 | *** | ||||
| Mean Coping Self-Efficacy (CSE) | 0.219*** | 0.781 | 0.740 | 0.820 | *** | ||||
| That Day Sleep Quality → Next Day Sleep Quality | 0.125 | 0.075 | 0.176 | *** | |||||
| That Day Coping Self-Efficacy → Next Night Sleep Quality | 0.000 | −0.055 | 0.054 | N.S. | |||||
| That Day Perceived Stress → Next Night Sleep Quality | −0.038 | −0.094 | 0.014 | N.S. | |||||
| Prev. Night Sleep Quality → That Day Coping Self-Efficacy | 0.029 | −0.017 | 0.079 | N.S. | |||||
| That Day Coping Self-Efficacy → Next Day Coping Self-Efficacy | 0.160 | 0.101 | 0.213 | *** | |||||
| That Day Perceived Stress → Next Day Coping Self-Efficacy | −0.030 | −0.082 | 0.020 | N.S. | |||||
| Prev. Night Sleep Quality → That Day Perceived Stress | −0.059 | −0.106 | −0.015 | ** | |||||
| That Day Coping Self-Efficacy → Next Day Perceived Stress | −0.069 | −0.120 | −0.017 | ** | |||||
| That Day Perceived Stress → Next Day Perceived Stress | 0.143 | 0.089 | 0.194 | *** | |||||
| Association Between Sleep Quality and Next Day Coping Self-Efficacy | 0.083 | 0.035 | 0.128 | *** | |||||
| Association Between Same Day Sleep Quality and Next Day Perceived Stress | −0.106 | −0.153 | −0.060 | *** | |||||
| Association Between Same Day Perceived Stress and Coping Self-Efficacy | −0.423 | −0.459 | −0.384 | *** | |||||
| Association Between Day of Week and Coping Self-Efficacy | −0.017 | −0.057 | 0.021 | N.S. | |||||
| Association Between Day of Week and Perceived Stress | −0.035 | −0.072 | 0.002 | N.S. | |||||
| Association Between Time of Day and Sleep Quality | −0.003 | −0.045 | 0.037 | N.S. | |||||
| Association Between Time of Day and Coping Self-Efficacy | 0.012 | −0.035 | 0.060 | N.S. | |||||
| Association Between Time of Day and Perceived Stress | −0.006 | −0.052 | 0.041 | N.S. | |||||
| Association Between Time of Day Surveyed and Day of Week | 0.085 | 0.052 | 0.115 | *** | |||||
Significance level is represented as N.S. for p > 0.05,
for p <= 0.05,
for p <= 0.01, and
for p <= 0.001.
There were also several significant associations from one predictor at time t to a different outcome variable at time t+1 (see Figure 4 and Supplementary Table 3). These cross-lagged associations indicated that levels of one variable predicted subsequent levels of another variable, controlling for other auto-regressive associations and covariation (associations between simultaneous measurements). The model allowed intercepts and slopes to vary randomly for individuals, but the fixed effects estimates are reported here for the entire sample. Students reporting higher sleep quality for a given night relative to their own average reported significantly lower perceived stress the following day (−0.11 [CI: −0.15, −0.06]) and significantly higher coping self-efficacy the following day (0.08 [CI: 0.04, 0.13]). Students reporting higher sleep quality for a given night relative to their own average also reported significantly lower perceived stress two days later (−0.06 [CI: −0.11, −0.02]). Students reporting higher coping self-efficacy on a given day relative to their own average reported significantly lower perceived stress the next day (−0.07 [CI: −0.13, −0.02]). No other associations on the within-person level reached significance. The within-person level covariates, time of survey and day of diary, did not significantly influence any of the within-person variables, although time and day were significantly associated with each other (0.09 [CI: 0.05, 0.12]) (see Figure 4, Supplementary Table 3).
Associations Among Between-Person Covariates and Within-Person Fixed Effects
Individuals with larger within-person fixed effects showed moderate associations with several demographic covariates (see Figure 5, Supplementary Table 2). That is, particular individual characteristics were more likely to show certain day-to-day associations. Specifically, individuals with greater stability in night-to-night sleep quality were more likely to be male (0.19 [CI: 0.01, 0.37]), more likely to attend particular schools within the sample (0.23 [CI: 0.04, 0.40]), less likely to experience depression (−0.26 [CI:−0.42, −0.08]), and less likely to have a mother who had completed four years of college or higher education (−0.33 [CI: −0.53, −0.13]). Individuals with greater stability in day-to-day coping self-efficacy were more likely to report higher pubertal status (0.40 [CI: 0.20, 0.59]). No other associations among the within-person fixed effects and demographic covariates reached significance (see Supplementary Table 2). These associations are considered exploratory, as specific hypotheses about the direction or magnitude of effects were not pre-registered.
Figure 5: Stability of Students’ Coping Self-Efficacy, Perceived Stress, and Sleep Quality From Day to Day Is Related to Individual Covariates and Some Within-Person Lagged Associations.
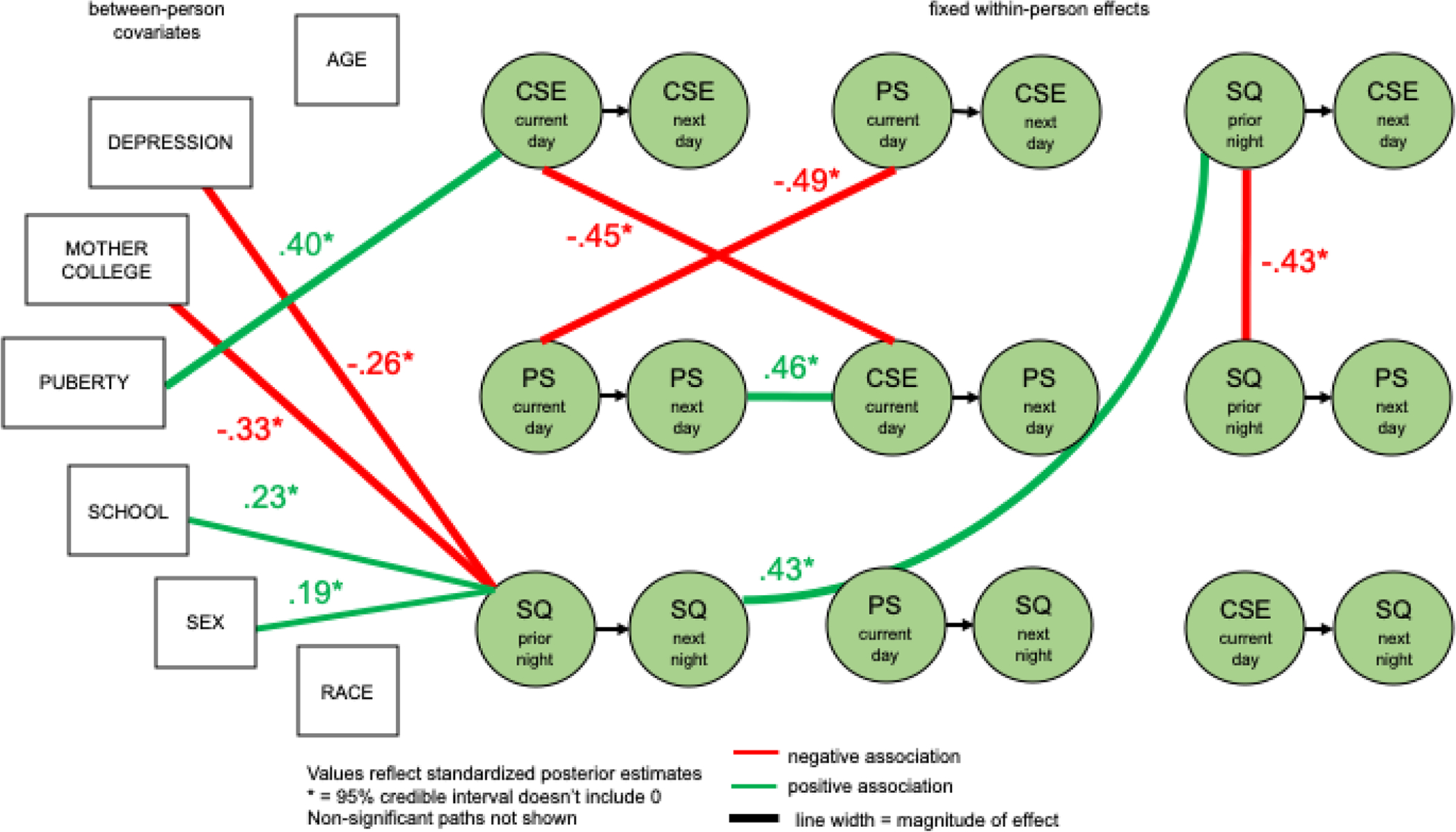
Modeling between-person covariances among within-person fixed effects indicates that the stability of an individual’s coping self-efficacy (CSE), perceived stress (PS), and sleep quality (SQ) may relate to their demographics and may make it more or less likely for their sleep quality and coping self-efficacy on one day to impact their subsequent stress. Green circles connected by black arrows indicate within-person fixed effects from time t to time t+1. Lines without arrow heads reflect cross-sectional (non-directional) effects, and line widths reflect magnitude of associations, with red signifying negative associations and green signifying positive associations.
Asterisks indicate significance, meaning that the Bayesian 95% credible interval for the estimate does not include 0. Only significant associations are shown.
Associations Among Within-Person Fixed Effects
The DSEM also revealed between-person associations among within-person fixed effects. That is, the strength of individuals’ relationships from one timepoint to another acted like individual differences, predisposing them to also experience other day-to-day relationships (see Figure 5, Supplementary Table 4). Individuals with greater stability in their day-to-day perceived stress, meaning that they either stayed high or low in perceived stress across multiple days, were then less likely to report that current-day perceived stress influenced next-day coping self-efficacy (−0.49[CI: −0.74, −0.15]). However, individuals with stable perceived stress were more likely to experience greater stability in day-to-day coping self-efficacy (0.46 [CI: 0.18, 0.68]). Individuals with greater stability in their day-to-day coping self-efficacy were less likely to report that current-day coping self-efficacy had an influence on next-day perceived stress (−0.45 [CI: −0.70, −.10]). Individuals with greater night-to-night stability in sleep quality were more likely to report that sleep quality on one night made a difference for coping self-efficacy two days later (0.43 [CI: 0.07, 0.72]). Finally, individuals whose sleep quality has a greater influence on their coping self-efficacy two days later were less likely to experience sleep quality’s influence on their perceived stress two days later (−0.43 [CI: −0.69, −0.07]). No other between-person associations among the within-person fixed effects reached significance (see Supplementary Table 4). These associations are considered exploratory, as specific hypotheses about the direction or magnitude of effects were not pre-registered.
Robustness of Results
The findings appear to be robust to the choice of analysis strategy. As pre-registered, piecewise models were initially run for each path between perceived stress, sleep quality, and coping self-efficacy using multilevel Bayesian linear models in R with the brms package (Bürkner, 2018). It was subsequently determined that the DSEM approach would be a better analytic fit for the data given the presence of simultaneous co-variation and auto-regressive paths that could only be captured by linking models in a structural equation framework. Each outcome was predicted at time t while controlling for the outcome at time t-1 as well as that day’s negative rating at time t-1, and the covariates age, depression severity, maternal education level, race, sex, and school were included in each model. Results are presented in Supplementary Table 5. In summary, bidirectional associations at the between-person level were found, where comparatively the DSEM only identified a significant between-person intercept for perceived stress to that-night sleep quality (see Table 1). Within-person associations were found from sleep quality to next-day perceived stress (−0.20 [CI: −0.28, −0.13]), sleep quality to next-day coping self-efficacy (0.15 [CI: 0.09, 0.21]), and perceived stress to next-day coping self-efficacy (0.11 [CI: 0.06, 0.15]). Although some associations appeared in the piecewise models that were not found in the DSEM, it is likely that some non-independent variance is accounted for in the DSEM by modeling the independent variance and simultaneous co-variation of perceived stress, sleep quality, and coping self-efficacy, which was not possible in piecewise linear models.
One question is whether the associations tested depend on the negative experiences of a given day. Unfortunately, technical limitations prevent this question from being fully answered at present. In DSEM, it is not currently possible to test interactions of within-person variables with time lags (M. Zyphur, personal communication, June 13, 2020). Instead, as an approximation, each cross-lagged association from the DSEM was tested in a piecewise fashion using multilevel Bayesian linear models in R with the brms package (Bürkner, 2018). Again, each outcome was predicted at time t while controlling for the outcome at time t-1 as well as that day’s negative rating at time t-1. No significant interactions in these models were found when testing the mean intensity of ratings of the day’s negative events as a moderator in the within-person time-lagged models, suggesting that these associations hold regardless of the intensity of negative events of a particular day.
Discussion
Adolescents today navigate myriad academic and social demands that can potentially disrupt sleep, from social media and bullying to standardized testing and college applications. The transition to high school can be a time of particular upheaval, as 9th-graders face novel challenges and expectations (Rudolph et al., 2001), accompanied by an uptick in sleep issues (Wolfson & Carskadon, 1998). If adolescents sleep poorly and feel unable to effectively handle their feelings of stress, this may set the stage for a destructive spiral of greater stress and worse sleep. Longitudinal studies have shown that poor sleep increases the likelihood that adolescents experiencing life stress will develop depression (Kuhlman, et al., 2020). The statistical difficulty of teasing apart these highly intertwined psychological and physiological processes has made it challenging to understand the nature of this spiral as it unfolds in the life of an adolescent. The present study aimed to understand the temporal dynamics of the stress-sleep spiral in adolescents and probe whether coping self-efficacy may provide a means to combat these negative consequences. To address this, a dynamic structural equation model was employed to examine associations among perceived stress, sleep quality, and coping self-efficacy in 9th graders from one day to the next.
The current study’s results challenge the classic conception of a bidirectional spiral between daily stress and sleep. Although associations were found between individuals’ average levels of sleep quality, perceived stress, and coping self-efficacy, there was no evidence found to support bidirectional associations in students’ daily diary reports. After taking auto-regressive associations and same-timepoint covariances into account, only unidirectional impacts were found at the between-person level from perceived stress on sleep quality, and at the within-person level from sleep quality on adolescents’ self-reported perceived stress as well as their subjective appraisals of coping self-efficacy. Coping self-efficacy also seems to play an important indirect role in sleep quality’s influence on perceived stress, such that better sleep quality on a given school night improves next-day coping self-efficacy, which subsequently decreases perceived stress one day later. Moreover, the stability of students’ day-to-day sleep quality, perceived stress, and coping self-efficacy seems related to individual differences that may serve as risk factors.
These findings highlight that adolescents’ sense of confidence in their ability to cope with challenges may be a key pathway in helping to disrupt the negative consequences of poor sleep on perceived stress and its downstream effects on their mental health. Adolescence is considered a sensitive period for brain development, in particular the executive function and regulation-related areas that aid in identifying and implementing appropriate coping strategies in challenging emotional situations (Fuhrmann, Knoll, & Blakemore, 2015; Steinberg, 2005). Adolescence also may be a sensitive period for the onset of depression, with stress, negative emotionality, and effortful control (required for adaptive coping) serving as crucial risk factors for abnormal brain maturation patterns associated with depression (Andersen & Teicher, 2008; Ellis, et al., 2017; Hankin, et al., 2015). Adolescent depression then increases risk for later adult depression, anxiety, and suicidality (Johnson, Dupuis, Piche, Clayborne, & Colman, 2017). Moreover, meta-analyses of prospective studies indicate that poor sleep in adolescents increases odds for suicidal ideation (Liu, et al., 2019; Porras-Segovia, 2019). The current study’s results showing the importance of coping self-efficacy for disrupting the link from poor sleep to perceived stress therefore have important implications for reducing the onset and severity of depression symptoms. Indeed, a meta-analysis revealed that greater use of adaptive coping is associated with decreases in depression and anxiety (Schäfer, et al., 2017). Students with confidence in their ability to deal with stressors may be more likely to attempt adaptive coping strategies on days when they have slept poorly, therefore mitigating the effects of chronic stress that may over time contribute to depression and suicidality.
This study’s approach showcases the value of a single-model dynamic structural equation in order to tease apart highly interlinked phenomena, with time-lagged analyses making it possible to address questions of temporal causality. While it is unethical and unfeasible to experimentally determine the long-term causal effects of poor sleep and high stress in students, the DSEM approach brings researchers closer to understanding how changes from one day temporally precede other fluctuations and quantifies how these effects amplify or peter out as the school week goes on. The statistical approach also holds promise for policy-oriented research in adolescents in order to identify which covariates indicate important potential target populations for intervention.
The Stress-Sleep Spiral
As expected, strong cross-sectional associations were found between sleep quality and perceived stress that remained robust after adjusting for demographic covariates. Trait differences were found based on certain demographics. More depressed students reported lower average sleep quality, and more depressed and female students reported greater perceived stress. Perceived stress also differed by school. These findings align nicely with cross-sectional work in adolescents linking perceived stress and sleep quality. For example, correlational research indicates a strong tie between stress-related measures such as mood and clinical symptoms and short or disrupted sleep (Bartel, et al., 2015). A longitudinal study in adolescents supports the idea that there are indeed bidirectional causal associations between sleep and emotional challenges, such that restricted sleep duration at baseline predicted emotional and behavioral issues five years later, and emotional and behavioral issues predicted shorter sleep duration five years later (Kortesoja, et al., 2020). However, Kortesoja and colleagues found asymmetrical bidirectionality, with a far greater effect size for sleep influencing emotional challenges.
Contrary to the hypotheses, however, the between- and within-person model results indicated unidirectional influences rather than the expected fully bidirectional relationship. At the between-person level, perceived stress was negatively associated with next-night sleep quality, while at the within-person level, sleep quality was negatively associated with next-day perceived stress. This pattern held even after adjusting for demographics, simultaneous covariance, auto-regressive effects, differences in individual means, and the intensity of negative affect reported as a result of daily events. Specifically, there was evidence that a student’s sleep quality on a given school night predicted next-day perceived stress. Sleep quality also continued to predict perceived stress two days later. These within-person results suggest that, regardless of a student’s usual levels of sleep quality and perceived stress, daily fluctuations in sleep quality relative to their own mean directly influence perceived stress for the next two school days.
Results in the direction of sleep quality to perceived stress are also consistent with prior work from sleep restriction experiments. For example, adolescents restricted to 6.5 hours of sleep for one week experienced greater feelings of tension and anxiety, hostility and oppositional behavior, and confusion, as well as lower energy (Baum et al., 2014). A brief three-day ecological momentary assessment study found that heightened daily perceived stress preceded shorter sleep duration, and worse sleep efficiency (the ratio of time asleep to time spent trying to sleep) preceded increased next-day perceived stress (Doane & Thurston, 2014). A six-day diary study found bidirectional within-person associations (van Zundert, van Roekel, Engels, & Scholte, 2015): While self-reported disturbed sleep was not related to self-reported affect, worse sleep quality was associated with greater negative affect and less positive affect the following day, and greater negative affect and lower positive affect were associated with worse sleep quality. However, these previous studies have modeled each direction in the stress-sleep spiral separately. The current study adds to this emerging picture by 1) assessing daily temporal associations in both directions simultaneously using DSEM, 2) assessing for a greater length of time than existing diary studies have, and 3) measuring perceived stress.
The Role of Coping Self-Efficacy
What role does coping self-efficacy play in the link from sleep quality to perceived stress? Strong cross-sectional associations were found between sleep quality and coping self-efficacy, and between perceived stress and coping self-efficacy, even after adjusting for demographic covariates. More depressed, female students with lower socioeconomic status (SES, indexed by maternal education) reported lower coping self-efficacy. These results align with cross-sectional results indicating significant associations for perceived stress with sense of control, sleep issues, and global and task-specific self-esteem (Schraml, Perski, Grossi, & Simonsson-Sarnecki, 2011). Further corroborating the present findings, a diary study of high school students transitioning to college showed that cortisol spikes only accompany increased perceived stress for students who report having low coping self-efficacy (Sladek, Doane, Luecken, & Eisenberg, 2016). Sladek and colleagues also found coping self-efficacy positively associated with parental education level, but not ethnicity or sex.
At the within-person level, expected bidirectional associations were not found between perceived stress and coping self-efficacy. As hypothesized, only a unidirectional association from sleep quality to next-day coping self-efficacy was identified, but not vice versa. Specifically, there was evidence that a student’s sleep quality on a given school night predicted next-day coping self-efficacy. Sleep quality did not continue to predict coping self-efficacy two days later. A student’s coping self-efficacy on a given day also predicted lower perceived stress the following day, indicating that there is an indirect effect of sleep quality on perceived stress via coping self-efficacy. These findings regarding coping self-efficacy stability align with results from a large adolescent randomized controlled trial indicating that individuals with higher general self-efficacy benefitted more from the sleep intervention (Blake, et al., 2018). A study in adults also found that adaptive coping strategies moderated the relationship between perceived stress and sleep (Sadeh, Keinan, & Daon, 2004), which aligns with the apparent indirect effect from sleep quality to perceived stress via coping self-efficacy. The within-person results suggest that, regardless of a student’s usual levels of sleep quality, perceived stress, and coping self-efficacy, daily fluctuations in sleep quality relative to students’ own means have direct and indirect influences on their perceived stress for the next two school days. The indirect pathway indicates that coping self-efficacy can serve as an important break point in the relationship between sleep quality and subsequent perceived stress.
Interpreting Unidirectional Results
One particular benefit of a DSEM analytic approach is that each estimated path adjusts for all other paths in the model. This means that, although in daily life perceived stress, sleep quality, and coping self-efficacy are interlinked in ways that can be difficult to pull apart, DSEM provides a statistical tool to examine the independent sources of variance (see Figure 1). The analysis was optimized to foreground questions about independent contributions of perceived stress, sleep quality, and coping self-efficacy, directionality, and temporal association while holding constant other associations. The significant unidirectional results therefore lend support to the idea that perceived stress and coping self-efficacy are separate constructs that, although highly related, have independent associations with daily and average sleep quality in this sample. The cross-lagged association results, which adjust for auto-regressive variance, can also hint at temporal causality.
Interpreting Individual Variation in Daily Patterns
This study’s analysis strategy also made it possible to explore variation between students in these day-today dynamics, which provides exploratory evidence about the role of individual differences. The results indicated that individuals with stable perceived stress and coping self-efficacy tended not to experience much of a shift in response to fluctuating stressors or self-beliefs about coping, regardless of the day’s experiences. These individuals may be characterized either by lingering dysfunction or by stable well-being, and more work is needed to understand different dynamics for these two groups. Another implication of these results is that individuals who already exhibit variability may be more capable of healthier shifts toward greater coping self-efficacy and lower perceived stress if nudged, compared to their peers with more trait-like stability.
Notably, however, individuals with stable sleep quality were more likely to show changes to coping self-efficacy after a night of better-than-usual sleep. For individuals whose sleep quality tended to improve subsequent coping self-efficacy, changes in their sleep quality were less likely to influence their subsequent perceived stress. This shows that students with consistent sleep quality and stronger associations between sleep quality and coping may be most capable of facing unexpected stressors with increased resilience.
Students with greater stability of sleep quality from night to night (whether consistently poor or consistently good) had lower depression severity, lower maternal education level, tended to be males, and differed by sample school. Later pubertal status was more consistent with coping self-efficacy from day to day, suggesting that physical maturity tracked with having a consistent sense of being able to cope with challenges. These demographic findings were generally consistent with the literature, which indicates that poor sleep is associated with worse depressive symptoms (Alfano, Zakem, Costa, Taylor, & Weems, 2009). A diary study on bidirectional links between negative affect and sleep found significant moderation by both sex and depressive symptoms, with girls and high depressive symptoms showing increased effect sizes (van Zundert, van Roekel, Engels, & Scholte, 2015). In the epidemiological literature on adolescent sleep disparities, evidence for sex differences is mixed, although there may be an interaction between sex and race, which unfortunately was not examined in the model (Marczyk Organek, et al. 2015). Surprisingly, the model indicated that lower maternal education was associated with more stable sleep quality, counter to findings indicating deep disparities in sleep in relation to socioeconomic status (Liang, et al., 2020). One explanation for this result could be invalidity of student responses due to lack of knowledge (Ridolfo & Maitland, 2011). Another possibility is that subjective or relative sense of status may have far greater impact on students’ perceived stress and sleep quality than objective proxies (Huynh & Chiang, 2018). It may be that high-SES parents have time to be more involved in managing school performance and bedtime schedules, potentially lowering students’ sense of self-efficacy to cope on their own. Variation in sleep could also relate to socioeconomic status in more complex ways due to parents’ work schedules, stably enforced bedtimes, work or family care burdens on students, and attitudes around homework and screen time.
Implications for Interventions
These exploratory individual differences in daily dynamics suggest two key areas for intervention. First, stabilizing and improving daily sleep quality could directly reduce perceived stress and increase the positive impact of sleep quality on subsequent coping self-efficacy. The results indicate that high-SES, high-depression females may be a target group for intervention. A second approach could be to use psychological interventions that enhance youths’ coping self-efficacy in response to their daily academic and social demands as a means to weaken the link from poor sleep quality to heightened perceived stress and decrease risk for developing mental health problems. Promising research indicates that interventions to encourage adolescents to endorse more malleable beliefs about people’s social traits (“a growth mindset of personality intervention”) can reduce depressive symptoms and improve stress resilience in adolescents’ daily stress coping (Schleider & Weisz, 2018; Yeager, Lee, & Jamieson, 2016; Yeager, 2017). These results suggest that future research should assess whether similar interventions can also improve adolescents’ mindsets about their ability to cope with stressors, leading to improved sleep quality and a cascade of positive developmental outcomes by preventing early risks for clinical depression, anxiety, and suicidal ideation.
Overall, this study’s results provide new clarity about the directionality of effects among adolescents’ daily sleep quality, perceived stress, and coping self-efficacy. It extends prior work on sleep and coping self-efficacy in adults, indicates a crucial role played by coping self-efficacy in the link between sleep and stress in adolescents, and suggests the importance of dual sleep quality and coping self-efficacy interventions among adolescents.
Strengths, Limitations, and Future Directions
This study had several notable strengths. First, state-of-the-art Bayesian DSEM analysis was employed to capture bidirectional stress-sleep temporal associations among daily measures of subjective sleep and state measures of coping self-efficacy. Second, data were collected within a large sample of ethnically and socioeconomically diverse adolescents across multiple schools, bolstering this study’s ability to provide generalizable conclusions. Third, this study controls for potential demographic covariates influencing individual differences in students’ dynamic daily experiences, including age, depression symptoms, pubertal status, race, sex, socioeconomic status, and variation between schools. Finally, the study followed best practices by exploring in a held-out subset of data before testing pre-registered confirmatory hypotheses, employing Bayesian models to reduce false positives, and completing robustness tests, such that the results can be interpreted with greater confidence.
These strengths notwithstanding, several limitations also bear mention. First, students were assessed at a single timepoint during school hours, meaning that it was only possible to capture perceived stress and coping self-efficacy assessments partway through the school day. This meant that the school environment shared common features and allowed for fairly high response rates. However, this strategy prevented assessment of experiences later in the day and at home. Diary studies, especially in an adolescent population, involve a trade-off between precision with multiple items and timepoints, and attrition with long or repetitive surveys. Future work should assess whether these patterns change if after-school perceptions of stress and coping self-efficacy are assessed.
Second, self-reported measures of sleep quality were used, but not objective measures of sleep duration and night awakenings. Thus, there was no way to determine the ground-truth of students’ reports of sleep quality relative to objective measures of unwanted wakefulness, an important contributor to sleep quality. Future work should certainly incorporate objective sleep measures; however, subjective and objective sleep measures are thought to represent separate dimensions of sleep (Kaplan, et al., 2017), and a single-item sleep quality measure is the gold standard for sleep diaries (Carney, et al., 2012). Moreover, subjective sleep measures tend to be more predictive of affect-related outcomes (Konjarski, et al., 2018; Kortesoja, et al., 2020).
Third, a single-item measure of perceived stress and a new coping self-efficacy composite measure were used to assess central constructs in the study. These measures, although face valid, may not fully capture the underlying constructs or may be subject to differences in individual interpretations of the meanings of “stress” to different students. Indeed, a moderate correlation was found between the mean of the perceived stress item and baseline ratings on the widely validated Perceived Stress Scale (Cohen & Williamson, 1988), indicating either that fluctuations in daily perceived stress are not captured by the Perceived Stress Scale or that there may be variance in perceived stress not picked up by the single item. Moreover, the composite coping self-efficacy measure was a novel measure and may not have fully captured the construct of interest. Although all measures involve trade-offs, the clear advantage of single-item measures is that they reduce burden and maintain engagement, especially in adolescent samples with limited attention. Using multiple-item measures would likely result in attrition and lower response rates if repetitive items became too tedious, which would also undermine validity. For this reason, single, face-valid items were chosen for the study design. Though unreliability is a key concern for single-item measures, this study’s results indicate that there are robust and meaningful correlations that align with theory (for example, associations between perceived stress and coping self-efficacy) even for the within-person temporal associations. This suggests that these measures have functioned as expected in this context.
Fourth, this study focused on a single school district in Texas, which makes it difficult to generalize to adolescents in other geographic locations and cultures. At the same time, this design allowed for comparison across a range of cohorts with diverse backgrounds while maintaining similar schedules for school start times. This could be considered a limitation in that it may blur important group differences. The results obtained after adjusting for demographic variables suggest the value of comparing differences among demographic and clinical groups, as certain individual differences may in fact moderate relationships among perceived stress, sleep quality, and coping self-efficacy. Future research should seek to replicate these findings in other well-powered, broad adolescent samples.
Finally, coping self-efficacy was not manipulated, so it is not possible to make fully causal claims, though the time lags in the DSEM suggest temporal causality. Future work is needed to test whether interventions that improve coping self-efficacy are indeed able to break the link between sleep and stress in adolescents. Promising results suggest that targeting mindsets about coping ability may be particularly effective (Yeager, 2017; Jamieson et al., 2018) to alter students’ responses to the combination of academic, social, and family stresses that high school adolescents face.
Conclusion
The present study examines the temporal dynamics of perceived stress and sleep quality in adolescents undergoing a challenging transition to high school and adds to the current literature by simultaneously modeling both directions in the stress-sleep spiral. Moreover, this study extends existing cross-sectional studies by examining the important role of coping self-efficacy in perpetuating or disrupting dysfunction and by identifying the temporal sequence among daily perceived stress, sleep quality, and coping self-efficacy within individual students using a new method, dynamic structural equation modeling. Contrary to general claims of a bidirectional stress-sleep spiral, this study found evidence of only unidirectional relationships. At the within-person level, a night of better sleep quality relative to an individual student’s own mean seemed to improve next-day coping self-efficacy, which then decreased perceived stress on the following day. At the between-person level, students with higher perceived stress on one day relative to their peers were likely to experience worse-than-average sleep quality. These results held after adjusting for demographic covariates and individual reports of negative daily events. These results suggest that it might be important to address adolescents’ beliefs about their ability to cope with challenges in order to mitigate the negative impacts of stress on sleep, which can lead to cascading effects on social-emotional well-being and mental health in youth.
Supplementary Material
Acknowledgements
The authors thank Michael Zyphur for statistical consulting and members of the Stanford Psychophysiology Laboratory and Sleep Health and Insomnia Program for valuable feedback.
Funding
Research reported in this publication was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the National Institutes of Health under award number R01HD084772. This research was also supported by grant P2CHD042849 awarded to the Population Research Center at the University of Texas at Austin by the Eunice Kennedy Shriver National Institute of Child Health and Human Development. M.t.B. was supported by a National Science Foundation Graduate Fellowship.
Footnotes
Pre-registration
Exploratory models were developed with a subset of the data using one school (n = 175 from 15 classrooms). Based on those exploratory findings, confirmatory hypotheses were pre-registered on the Open Science Framework: https://osf.io/3tdeq/register/564d31db8c5e4a7c9694b2be. For the present study, hypotheses were tested on held-out data from the remaining four schools in the sample. All deviations from the pre-registration are listed in Supplementary Materials.
Data Sharing Declaration
The data that support the findings of this study are available upon request from the Population Research Center at the University of Texas at Austin for researchers who agree to terms of data use, including analysis on a secure server and prohibitions against any analysis that risks exposing the identity of participating students (i.e., deductive disclosure). Requests for data should be directed to Elizabeth Johnson at ejohnson@prc.utexas.edu.
Conflicts of Interest
The authors have no conflicts of interest to report.
Ethical Approval
This study with school-age minor human participants received ethical approval from the Institutional Review Board of the University of Texas at Austin and was approved by the research committee of the participant school district and by the participant school principals.
Informed Consent
Data were collected from minors whose parents provided informed written consent and who provided informed written assent for diary response collection.
References
- Alfano CA, Zakem AH, Costa NM, Taylor LK, & Weems CF (2009). Sleep problems and their relation to cognitive factors, anxiety, and depressive symptoms in children and adolescents. Depression and Anxiety, 26, 503–512. 10.1002/da.20443 [DOI] [PubMed] [Google Scholar]
- Åkerstedt T, Kecklund G, & Axelsson J (2007). Impaired sleep after bedtime stress and worries. Biological Psychology, 76(3), 170–173. 10.1016/j.biopsycho.2007.07.010 [DOI] [PubMed] [Google Scholar]
- Andersen SL, & Teicher MH (2008). Stress, sensitive periods and maturational events in adolescent depression. Trends in Neurosciences, 31(4), 183–191. 10.1016/j.tins.2008.01.004 [DOI] [PubMed] [Google Scholar]
- Asparouhov T & Muthén B (2010). Bayesian Analysis Using Mplus: Technical Implementation. Retrieved from http://www.statmodel.com/download/Bayes3.pdf
- Asparouhov T, Hamaker EL, & Muthén B (2018). Dynamic Structural Equation Models. Structural Equation Modeling: A Multidisciplinary Journal, 25(3), 359–388. 10.1080/10705511.2017.1406803 [DOI] [Google Scholar]
- Bacchini D & Magliulo F (2003). Self-image and perceived self-efficacy during adolescence. Journal of Youth and Adolescence, 32(5), 337–349. 10.1023/A:1024969914672 [DOI] [Google Scholar]
- Bandura A (1986). The explanatory and predictive scope of self-efficacy theory. Journal of Social and Clinical Psychology, 4(3), 359–373. 10.1521/jscp.1986.4.3.359 [DOI] [Google Scholar]
- Bandura A (1993). Perceived self-efficacy in cognitive development and functioning. Educational Psychologist, 28(2), 117–148. [Google Scholar]
- Bandura A, Reese L, & Adams NE (1982). Microanalysis of action and fear arousal as a function of differential levels of perceived self-efficacy. Journal of Personality and Social Psychology, 43(1), 5–21. [DOI] [PubMed] [Google Scholar]
- Bartel KA, Gradisar M, & Williamson P (2015). Protective and risk factors for adolescent sleep: A meta-analytic review. Sleep Medicine Reviews, 21, 72–85. 10.1016/j.smrv.2014.08.002 [DOI] [PubMed] [Google Scholar]
- Baum KT, Desai A, Field J, Miller LE, Rausch J, & Beebe DW (2014). Sleep restriction worsens mood and emotion regulation in adolescents. Journal of Child Psychology and Psychiatry, 55(2), 180–190. 10.1111/jcpp.12125 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ben Simon E, Vallat R, Barnes CM, & Walker MP (2020). Sleep Loss and the Socio Emotional Brain. Trends in Cognitive Sciences, 24(6), 435–450. 10.1016/j.tics.2020.02.003 [DOI] [PubMed] [Google Scholar]
- Benight CC, & Bandura A (2004). Social cognitive theory of posttraumatic recovery: The role of perceived self-efficacy. Behaviour Research and Therapy, 42(10), 1129–1148. 10.1016/j.brat.2003.08.008 [DOI] [PubMed] [Google Scholar]
- Blake MJ, Blake LM, Schwartz O, Raniti M, Waloszek JM, Murray G, Simmons JG, Landau E, Dahl RE, McMakin DL, Dudgeon P, Trinder J, & Allen NB (2018). Who benefits from adolescent sleep interventions? Moderators of treatment efficacy in a randomized controlled trial of a cognitive-behavioral and mindfulness-based group sleep intervention for at-risk adolescents. Journal of Child Psychology and Psychiatry, 59(6), 637–649. 10.1111/jcpp.12842 [DOI] [PubMed] [Google Scholar]
- Blake MJ, Snoep L, Raniti M, Schwartz O, Waloszek JM, Simmons JG, Murray G, Blake L, Landau ER, Dahl RE, Bootzin R, McMakin DL, Dudgeon P, Trinder J, & Allen NB (2017). A cognitive-behavioral and mindfulness-based group sleep intervention improves behavior problems in at-risk adolescents by improving perceived sleep quality. Behaviour Research and Therapy, 99, 147–156. 10.1016/j.brat.2017.10.006 [DOI] [PubMed] [Google Scholar]
- Blascovich J and Mendes WB (2010). Social psychophysiology and embodiment. In Fiske ST, Gilbert DT, and Lindzey G (Eds.), The handbook of social psychology (pp. 228–267). New York: John Wiley. doi: 10.1002/9780470561119.socpsy001006 [DOI] [Google Scholar]
- Bonanno GA, & Burton CL (2013). Regulatory flexibility: An individual differences perspective on coping and emotion regulation. Perspectives on Psychological Science, 8(6), 591–612. 10.1177/1745691613504116 [DOI] [PubMed] [Google Scholar]
- Burger K, & Samuel R (2017). The role of perceived stress and self-efficacy in young people’s life satisfaction: A longitudinal study. Journal of Youth and Adolescence, 46(1), 78–90. 10.1007/s10964-016-0608-x [DOI] [PubMed] [Google Scholar]
- Buysse DJ, Reynolds CF III, Monk TH, Berman SR, & Kupfer DJ (1989). The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Research, 28(2), 193–213. 10.1016/0165-1781(89)90047-4 [DOI] [PubMed] [Google Scholar]
- Bürkner P-C. (2018). Advanced Bayesian Multilevel Modeling with the R Package brms. The R Journal, 10(1), 395–411. doi: 10.32614/RJ-2018-017. [DOI] [Google Scholar]
- Carney CE, Buysse DJ, Ancoli-Israel S, Edinger JD, Krystal AD, Lichstein KL, & Morin CM (2012). The Consensus Sleep Diary: Standardizing prospective sleep self-monitoring. Sleep, 32(2), 287–302. 10.5665/sleep.1642 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cicogagni E (2011). Coping strategies with minor stressors in adolescence: Relationships with social support, self-efficacy, and psychological well-being. Journal of Applied Social Psychology, 41(3), 559–578. [Google Scholar]
- Cohen S & Williamson G (1988). Perceived stress in a probability sample of the United States. In Spacapan S & Oskamp S (Eds.), The social psychology of health: Claremont Symposium on applied social psychology. Newbury Park, CA: Sage. [Google Scholar]
- Compas BE, Banez GA, Malcarne V, & Worsham N (1991). Perceived control and coping with stress: A developmental perspective. Journal of Social Issues, 47(4), 23–34. 10.1111/j.1540-4560.1991.tb01832.x [DOI] [Google Scholar]
- Cracco E, Goossens L, & Braet C (2017). Emotion regulation across childhood and adolescence: Evidence for a maladaptive shift in adolescence. European Child & Adolescent Psychiatry, 26(8), 909–921. 10.1007/s00787-017-0952-8 [DOI] [PubMed] [Google Scholar]
- Crowley SJ, Acebo C, & Carskadon MA (2007). Sleep, circadian rhythms, and delayed phase in adolescence. Sleep Medicine, 8(6), 602–612. 10.1016/j.sleep.2006.12.002 [DOI] [PubMed] [Google Scholar]
- Curran PJ & Bauer DJ (2011). The disaggregation of within-person and between-person effects in longitudinal models of change. Annual Review of Psychology, 62(1), 583–619. 10.1146/annurev.psych.093008.100356 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deardorff J, Gonzales NA, & Sandler IN (2003). Control beliefs as a mediator of the relation between stress and depressive symptoms among inner-city adolescents. Journal of Abnormal Child Psychology, 31(2), 205–217. [DOI] [PubMed] [Google Scholar]
- DeSantis AS, Adam EK, Doane LD, Mineka S, Zinbarg RE, & Craske MG (2007). Racial/ethnic differences in cortisol diurnal rhythms in a community sample of adolescents. Journal of Adolescent Health, 41(1), 3–13. 10.1016/j.jadohealth.2007.03.006 [DOI] [PubMed] [Google Scholar]
- Destin M, Hanselman P, Buontempo J, Tipton E, & Yeager DS (2019). Do Student Mindsets Differ by Socioeconomic Status and Explain Disparities in Academic Achievement in the United States? AERA Open, 5(3), 233285841985770. 10.1177/2332858419857706 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Díaz-Morales JF, Escribano C, & Jankowski KS (2015). Chronotype and time-of-day effects on mood during school day. Chronobiology International, 32(1), 37–42. 10.3109/07420528.2014.949736 [DOI] [PubMed] [Google Scholar]
- Doane LD, & Thurston EC (2014). Associations among sleep, daily experiences, and loneliness in adolescence: Evidence of moderating and bidirectional pathways. Journal of Adolescence, 37(2), 145–154. 10.1016/j.adolescence.2013.11.009 [DOI] [PubMed] [Google Scholar]
- Dowd JB, Palermo T, Chyu L, Adam E, & McDade TW (2014). Race/ethnic and socioeconomic differences in stress and immune function in The National Longitudinal Study of Adolescent Health. Social Science & Medicine, 115, 49–55. 10.1016/j.socscimed.2014.06.011 [DOI] [PubMed] [Google Scholar]
- Ellis RER, Seal ML, Simmons JG, Whittle S, Schwartz OS, Byrne ML, & Allen NB (2017). Longitudinal trajectories of depression symptoms in adolescence: Psychosocial risk factors and outcomes. Child Psychiatry & Human Development, 48(4), 554–571. 10.1007/s10578-016-0682-z [DOI] [PubMed] [Google Scholar]
- Entwisle DR, & Astone NM (1994). Some practical guide-lines for measuring youth’s race/ethnicity and socioeconomic status. Child Development, 65(6), 1521–1540. 10.1111/1467-8624.ep9501252881 [DOI] [Google Scholar]
- Finkelstein DM, Kubzansky LD, Capitman J, & Goodman E (2007). Socioeconomic differences in adolescent stress: The role of psychological resources. Journal of Adolescent Health, 40(2), 127–134. 10.1016/j.jadohealth.2006.10.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Folkman S (1984). Personal control and stress and coping processes: A Theoretical Analysis. Journal of Personality and Social Psychology, 46(4), 839–852. [DOI] [PubMed] [Google Scholar]
- Fuhrmann D, Knoll LJ, & Blakemore S-J (2015). Adolescence as a sensitive period of brain development. Trends in Cognitive Sciences, 19(10), 558–566. 10.1016/j.tics.2015.07.008 [DOI] [PubMed] [Google Scholar]
- Glasscock DJ, Andersen JH, Labriola M, Rasmussen K, & Hansen CD (2013). Can negative life events and coping style help explain socioeconomic differences in perceived stress among adolescents? A cross-sectional study based on the West Jutland cohort study. BMC Public Health, 13(1), 532. 10.1186/1471-2458-13-532 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldin PR, Ziv M, Jazaieri H, Werner K, Kraemer H, Heimberg RG, & Gross JJ (2012). Cognitive reappraisal self-efficacy mediates the effects of individual cognitive-behavioral therapy for social anxiety disorder. Journal of Consulting and Clinical Psychology, 80(6), 1034–1040. 10.1037/a0028555 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldstein AN, & Walker MP (2014). The role of sleep in emotional brain function. Annual Review of Clinical Psychology, 10(1), 679–708. 10.1146/annurev-clinpsy-032813-153716 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gray K, Hampton B, Silveti-Falls T, McConnell A, & Bausell C (2015). Comparison of Bayesian Credible Intervals to Frequentist Confidence Intervals. Journal of Modern Applied Statistical Methods, 14(1), 43–52. 10.22237/jmasm/1430453220 [DOI] [Google Scholar]
- Gregory AM, & Sadeh A (2012). Sleep, emotional and behavioral difficulties in children and adolescents. Sleep Medicine Reviews, 16(2), 129–136. 10.1016/j.smrv.2011.03.007 [DOI] [PubMed] [Google Scholar]
- Guastella AJ & Moulds ML (2007). The impact of rumination on sleep quality following a stressful life event. Personality and Individual Differences, 42(6), 1151–1162. 10.1016/j.paid.2006.04.028 [DOI] [Google Scholar]
- Gunnar MR, Wewerka S, Frenn K, Long JD, & Griggs C (2009). Developmental changes in hypothalamus- pituitary-adrenal activity over the transition to adolescence: Normative changes and associations with puberty. Development and Psychopathology, 21(1), 69–85. 10.1017/S0954579409000054 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamaker EL, Asparouhov T, Brose A, Schmiedek F, & Muthén B (2018). At the Frontiers of Modeling Intensive Longitudinal Data: Dynamic Structural Equation Models for the Affective Measurements from the COGITO Study. Multivariate Behavioral Research, 53(6), 820–841. 10.1080/00273171.2018.1446819 [DOI] [PubMed] [Google Scholar]
- Hampel P & Petermann F (2006). Perceived stress, coping, and adjustment in adolescents. Journal of Adolescent Health, 38(4), 409–415. 10.1016/j.jadohealth.2005.02.014 [DOI] [PubMed] [Google Scholar]
- Hankin BL, Young JF, Abela JRZ, Smolen A, Jenness JL, Gulley LD, Technow JR, Gottlieb AB, Cohen JR, & Oppenheimer CW (2015). Depression from childhood into late adolescence: Influence of gender, development, genetic susceptibility, and peer stress. Journal of Abnormal Psychology, 124(4), 803. 10.1037/abn0000089 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hollenstein T, & Lougheed JP (2013). Beyond storm and stress: Typicality, transactions, timing, and temperament to account for adolescent change. American Psychologist, 68(6), 444–454. 10.1037/a0033586 [DOI] [PubMed] [Google Scholar]
- Huynh VW & Chiang JJ (2018). Subjective social status and adolescent health: The role of stress and sleep. Youth & Society, 50(7), 926–946. 10.1177/0044118X16646028 [DOI] [Google Scholar]
- Jamieson JP, Crum AJ, Goyer JP, Marotta ME, & Akinola M (2018). Optimizing stress responses with reappraisal and mindset interventions: An integrated model. Anxiety, Stress, & Coping, 31(3), 245–261. 10.1080/10615806.2018.1442615 [DOI] [PubMed] [Google Scholar]
- Johnson D, Dupuis G, Piche J, Clayborne Z, & Colman I (2017). Adult mental health outcomes of adolescent depression: A systematic review. Depression and Anxiety, 35(8), 700–716. 10.1002/da.22777 [DOI] [PubMed] [Google Scholar]
- Kahn M, Sheppes G, & Sadeh A (2013). Sleep and emotions: Bidirectional links and underlying mechanisms. International Journal of Psychophysiology, 89(2), 218–228. 10.1016/j.ijpsycho.2013.05.010 [DOI] [PubMed] [Google Scholar]
- Kalmbach DA, Pillai V, Roth T, & Drake CL (2014). The interplay between daily affect and sleep: a 2-week study of young women. Journal of Sleep Research, 23(6), 636–645. 10.1111/jsr.12190 [DOI] [PubMed] [Google Scholar]
- Kaplan KA, Hirshman J, Hernandez B, Stefanick ML, Hoffman AR, Redline S, Ancoli-Israel S, Stone K, Friedman L, & Zeitzer JM (2017). When a gold standard isn’t so golden: Lack of prediction of subjective sleep quality from sleep polysomnography. Biological Psychology, 123, 37–46. 10.1016/j.biopsycho.2016.11.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knowles JE, Frederick C, & Whitworth A (2019). merTools: Tools for analyzing mixed effect regression models. Retrieved from https://CRAN.R-project.org/package=merTools.
- Konjarski M, Murray G, Lee VV, & Jackson ML (2018). Reciprocal relationships between daily sleep and mood: A systematic review of naturalistic prospective studies. Sleep Medicine Reviews, 42, 47–58. 10.1016/j.smrv.2018.05.005 [DOI] [PubMed] [Google Scholar]
- Kortesoja L, Vainikainen M-P, Hotulainen R, Rimpelä A, Dobewall H, Lindfors P, Karvonen S, & Merikanto I (2020). Bidirectional relationship of sleep with emotional and behavioral difficulties: A five-year follow-up of Finnish adolescents. Journal of Youth and Adolescence, 49(6), 1277–1291. 10.1007/s10964-020-01203-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kovacs M (1992). Children’s depression inventory. North Tonawanda, NY: Multi-Health Systems. [Google Scholar]
- Krause AJ, Simon EB, Mander BA, Greer SM, Saletin JM, Goldstein-Piekarski AN, & Walker MP (2017). The sleep-deprived human brain. Nature Reviews Neuroscience, 18(7), 404–418. 10.1038/nrn.2017.55 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kuhlman KR, Chiang JJ, Bower JE, Irwin MR, Cole SW, Dahl RE, Almeida DM, & Fuligni AJ (2020). Persistent low positive affect and sleep disturbance across adolescence moderate link between stress and depressive symptoms in early adulthood. Journal of Abnormal Child Psychology, 48(1), 109–121. 10.1007/s10802-019-00581-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee HY, Jamieson JP, Miu AS, Josephs RA, & Yeager DS (2019). An entity theory of intelligence predicts higher cortisol levels when high school grades are declining. Child Development, 0(0), 1–19. 10.1111/cdev.13116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee YJ, Cho S-J, Cho IH, & Kim SJ (2012). Insufficient sleep and suicidality in adolescents. Sleep, 35(4), 455–460. 10.5665/sleep.1722 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liang T, Munro HM, Hargreaves MK, Steinwandel MD, Blot WJ, & Buchowski MS (2020). Patterns and correlates of sleep duration in the Southern Cohort Community Study. Sleep Medicine, 10.1016/j.sleep.2020.09.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu J-W, Tu Y-K, Lai Y-F, Lee H-C, Tsai P-S, Chen T-J, Huang H-C, Chen Y-T, & Chiu H-Y (2019). Associations between sleep disturbances and suicidal ideation, plans, and attempts in adolescents: A systematic review and meta-analysis. Sleep, 42(6), zsz054. 10.1093/sleep/zsz054 [DOI] [PubMed] [Google Scholar]
- Lüdecke D (2019). sjstats: Statistical functions for regression models (Version 0.17.4). Retrieved from https://CRAN.R-project.org/package=sjstats.
- Majeno A, Tsai KM, Huynh VW, McCreath H, & Fuligni AJ (2018). Discrimination and sleep difficulties during adolescence: The mediating roles of loneliness and perceived stress. Journal of Youth and Adolescence, 47(1), 135–147. 10.1007/s10964-017-0755-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marczyk Organek KD, Taylor DJ, Petrie T, Martin S, Greenleaf C, Dietch JR, & Ruiz JM (2015). Adolescent sleep disparities: Sex and racial/ethnic differences. Sleep Health, 1(1), 36–39. 10.1016/j.sleh.2014.12.003 [DOI] [PubMed] [Google Scholar]
- Marshall WA & Tanner JM (1969). Variations in the pattern of pubertal changes in girls. Archives of Diseases in Children, 44(235), 291–303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshall WA & Tanner JM (1970). Variations in the pattern of pubertal changes in boys. Archives of Diseases in Children, 45(239), 13–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McElreath R (2016). Statistical Rethinking: A Bayesian Course with Examples in R and Stan, CRC Press. Retrieved from: https://xcelab.net/rm/statistical-rethinking/ [Google Scholar]
- Meltzer LJ, Johnson C, Crosette J, Ramos M, & Mindell JA (2010). Prevalence of Diagnosed Sleep Disorders in Pediatric Primary Care Practices. Pediatrics, 125(6), e1410–e1418. 10.1542/peds.2009-2725 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Minkel JD, Banks S, Htaik O, Moreta MC, Jones CW, McGlinchey EL, … Dinges DF (2012). Sleep deprivation and stressors: Evidence for elevated negative affect in response to mild stressors when sleep deprived. Emotion, 12(5), 1015–1020. 10.1037/a0026871 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moseley L, & Gradisar M (2009). Evaluation of a school-based intervention for adolescent sleep problems. Sleep, 32(3), 8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK and Muthén BO (2017). Mplus User’s Guide (8th ed.). Los Angeles, CA: Muthén & Muthén. Retrieved from http://www.statmodel.com/download/usersguide/MplusUserGuideVer_8.pdf [Google Scholar]
- Owens J & Adolescent Sleep Working Group (2014). Insufficient sleep in adolescents and young adults: an update on causes and consequences. Pediatrics, 34(3), e921–e932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Palmer CA, Oosterhoff B, Bower JL, Kaplow JB, & Alfano CA (2018). Associations among adolescent sleep problems, emotion regulation, and affective disorders: Findings from a nationally representative sample. Journal of Psychiatric Research, 96, 1–8. 10.1016/j.jpsychires.2017.09.015 [DOI] [PubMed] [Google Scholar]
- Pearlin LI, Lieberman MA, Menaghan EG, & Mullan JT (1981). The stress process. Journal of Health and Social Behavior, 22, 337–356. [PubMed] [Google Scholar]
- Porras-Segovia A, Pérez-Rodríguez MM, López-Esteban P, Courtet P, Barrigón M ML, López-Castromán J, Cervilla JA, & Baca-García E (2019). Contribution of sleep deprivation to suicidal behaviour: A systematic review. Sleep Medicine Reviews, 44, 37–47. 10.1016/j.smrv.2018.12.005 [DOI] [PubMed] [Google Scholar]
- Ridolfo H, & Maitland A (2011). Factors that influence the accuracy of adolescent proxy reporting of parental characteristics: A research note. Journal of Adolescence, 34(1), 95–103. 10.1016/j.adolescence.2010.01.008 [DOI] [PubMed] [Google Scholar]
- Roberts RE, Roberts CR, & Duong HT (2009). Sleepless in adolescence: Prospective data on sleep deprivation, health and functioning. Journal of Adolescence, 32(5), 1045–1057. 10.1016/j.adolescence.2009.03.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rudolph KD, Lambert SF, Clark AG, & Kurlakowsky KD (2001). Negotiating the transition to middle school: The role of self-regulatory processes. Child Development, 72(3), 929–946. 10.1111/1467-8624.00325 [DOI] [PubMed] [Google Scholar]
- Sadeh A, & Gruber R (2002). Stress and sleep in adolescence: A clinical-developmental perspective. In Carskadon MA (Ed.), Adolescent Sleep Patterns (pp. 236–253). Cambridge: Cambridge University Press. 10.1017/CBO9780511499999.017 [DOI] [Google Scholar]
- Sadeh A, Keinan G, & Daon K (2004). Effects of stress on sleep: The Moderating Role of Coping Style. Health Psychology, 23(5), 542–545. 10.1037/0278-6133.23.5.542 [DOI] [PubMed] [Google Scholar]
- Schleider J, & Weisz J (2018). A single-session growth mindset intervention for adolescent anxiety and depression: 9-month outcomes of a randomized trial. Journal of Child Psychology and Psychiatry, 59(2), 160–170. 10.1111/jcpp.12811 [DOI] [PubMed] [Google Scholar]
- Schraml K, Perski A, Grossi G, & Simonsson-Sarnecki M (2011). Stress symptoms among adolescents: The role of subjective psychosocial conditions, lifestyle, and self-esteem. Journal of Adolescence, 34(5), 987–996. 10.1016/j.adolescence.2010.11.010 [DOI] [PubMed] [Google Scholar]
- Schunk DH, & Meece JL (2005). Self-efficacy development in adolescences. In Urdan T & Pajares F (Eds.), Self-efficacy beliefs of adolescents (pp. 71–96). Greenwich: Information Age Publishing. [Google Scholar]
- Schwarzer R & Jerusalem M (1992). Self-efficacy as a resource factor in stress appraisal processes. In: Schwarzer R (Ed.), Self-efficacy: Thought control of action (pp. 195–213). Taylor & Francis Group. [Google Scholar]
- Schäfer JÖ, Naumann E, Holmes EA, Tuschen-Caffier B, & Samson AC (2017). Emotion regulation strategies in depressive and anxiety symptoms in youth: A Meta-Analytic Review. Journal of Youth and Adolescence, 46(2), 261–276. 10.1007/s10964-016-0585-0 [DOI] [PubMed] [Google Scholar]
- Short MA, Booth SA, Omar O, Ostlundh L, & Arora T (2020). The relationship between sleep duration and mood in adolescents: A systematic review and meta-analysis. Sleep Medicine Reviews, 52, 101311. 10.1016/j.smrv.2020.101311 [DOI] [PubMed] [Google Scholar]
- Singer MJ, Humphreys KL, & Lee SS (2016). Coping self-efficacy mediates the association between child abuse and ADHD in adulthood. Journal of Attention Disorders, 20(8), 695–703. 10.1177/1087054712465337 [DOI] [PubMed] [Google Scholar]
- Sladek MR, Doane LD, Luecken LJ, & Eisenberg N (2016). Perceived stress, coping, and cortisol reactivity in daily life: A study of adolescents during the first year of college. Biological Psychology, 117, 8–15. 10.1016/j.biopsycho.2016.02.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smucker MR, Craighead WE, Craighead LW, & Green BJ (1986). Normative and reliability data for the Children’s Depression Inventory. Journal of Abnormal Child Psychology, 14(1), 25–39. 10.1007/BF00917219 [DOI] [PubMed] [Google Scholar]
- Steinberg L (2005). Cognitive and affective development in adolescence. Trends in Cognitive Sciences, 9(2), 69–74. 10.1016/j.tics.2004.12.005 [DOI] [PubMed] [Google Scholar]
- Tamir M, John OP, Srivastava S, & Gross JJ (2007). Implicit theories of emotion: Affective and social outcomes across a major life transition. Journal of Personality and Social Psychology, 92(4), 731–744. 10.1037/0022-3514.92.4.731 [DOI] [PubMed] [Google Scholar]
- Timbremont B, Braet C, & Dreessen L (2004). Assessing Depression in Youth: Relation Between the Children’s Depression Inventory and a Structured Interview. Journal of Clinical Child & Adolescent Psychology, 33(1), 149–157. 10.1207/S15374424JCCP3301_14 [DOI] [PubMed] [Google Scholar]
- Thoits PA (2006). Personal agency in the stress process. Journal of Health and Social Behavior, 47(4), 309–323. 10.1177/002214650604700401 [DOI] [PubMed] [Google Scholar]
- Thompson RJ, Mata J, Jaeggi SM, Buschkuehl M, Jonides J, & Gotlib IH (2010). Maladaptive coping, adaptive coping, and depressive symptoms: Variations across age and depressive state. Behaviour Research and Therapy, 48(6), 459–466. 10.1016/j.brat.2010.01.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Valois RF, Zullig KJ, & Hunter AA (2015). Association between adolescent suicide ideation, suicide attempts and emotional self-efficacy. Journal of Child and Family Studies, 24(2), 237–248. 10.1007/s10826-013-9829-8 [DOI] [Google Scholar]
- van Zundert RMP, van Roekel E, Engels RCME, & Scholte RHJ (2015). Reciprocal associations between adolescents’ night-time sleep and daytime affect and the role of gender and depressive symptoms. Journal of Youth and Adolescence, 44(2), 556–569. 10.1007/s10964-013-0009-3 [DOI] [PubMed] [Google Scholar]
- Wang Y & Yip T (2020). Sleep facilitates coping: Moderated mediation of daily sleep, ethnic/racial discrimination, stress responses, and adolescent well-being. Child Development, 91(4). 10.1111/cdev.13324 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Waschbusch DA, Sellers DP, LeBlanc M, & Kelley ML (2003). Helpless attributions and depression in adolescents: The roles of anxiety, event valence, and demographics. Journal of Adolescence, 26(2), 169–183. 10.1016/S0140-1971(02)00134-3 [DOI] [PubMed] [Google Scholar]
- Wiklund M, Malmgren-Olsson E-B, Öhman A, Bergström E, & Fjellman-Wiklund A (2012). Subjective health complaints in older adolescents are related to perceived stress, anxiety and gender – a cross-sectional school study in Northern Sweden. BMC Public Health, 12(1), 993. 10.1186/1471-2458-12-993 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolfson AR, & Carskadon MA (1998). Sleep schedules and daytime functioning in adolescents. Child Development, 69(4), 875. 10.2307/1132351 [DOI] [PubMed] [Google Scholar]
- Yan Y-W, Lin R-M, Su Y-K, & Liu M-Y (2018). The relationship between adolescent academic stress and sleep quality: A multiple mediation model. Social Behavior and Personality: An International Journal, 46(1), 63–77. 10.2224/sbp.6530 [DOI] [Google Scholar]
- Yang H, Durocher JJ, Larson RA, DellaValla JP, & Carter JR (2012). Total sleep deprivation alters cardiovascular reactivity to acute stressors in humans. Journal of Applied Physiology, 113(6), 903–908. 10.1152/japplphysiol.00561.2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yeager DS (2017). Social and emotional learning programs for adolescents. The Future of Children, 27(1), 73–94. 10.1353/foc.2017.0004 [DOI] [Google Scholar]
- Yeager DS, Lee HY, & Jamieson J (2016). How to improve adolescent stress responses: Insights from an integration of implicit theories and biopsychosocial models. Psychological Science, 27(8), 1078–1091. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.