

Abstract
Background:
Healthcare is changing from a focus on acute care health issues to one of managing chronic conditions. This change has resulted in the development of home health-care systems as a way of managing chronic conditions outside the hospital. The aim of this study was to analyze the concept of home healthcare using a hybrid model.
Materials and Methods:
This hybrid concept analysis consisted of three phases: theoretical, fieldwork, and analytical. Science Direct, PubMed, ProQuest, and Scopus were searched with related terms in the theoretical phase. In the fieldwork phase, six professionals with experience in home healthcare were interviewed and after each interview, qualitative content analysis was conducted. During the final phase, descriptions and themes from the first two phases were combined.
Results:
In the theoretical phase, the definition of home healthcare included descriptions answering the Who, What, When, Where, and Why questions. In the fieldwork phase, the results were divided into three areas: 1-comprehensive care; 2-extent of services; and 3-outcomes. The final analysis phase of this study indicated that the home health-care concept is a comprehensive, professional, and holistic care system accompanied by medical services and professionals whose goals are to support an individual's health and provide care in their home. Healthcare provided in one's home was found to preserve a patient's dignity and reduce health-care costs.
Conclusions:
The definition of the home healthcare concept establishes a foundation for developing a comprehensive home health-care system. This concept analysis for home healthcare could be a guide for future studies.
Keywords: Concept analysis, home care services, home nursing, Iran
Introduction
It is estimated that in the next 20 years fundamental changes in global public health will be occurring, as the focus of care moves toward noncontagious diseases. Thus, health-care systems are gradually transitioning from a focus on acute care in hospitals to the management of chronic health conditions in patients' home and community.[1] By the year 2050, approximately 27 million individuals in the world will need help with managing chronic health conditions, such care can best be accomplished through a home health-care system.[1,2] Three underlying factors account for this shift: 1) the focus of health conditions changing from contagious diseases to the prevention and management of noncontagious diseases; 2) an increase in the number of older adults; and 3) the increased need for rehabilitation, so individuals can function as independently as possible.[3] While people age, many are living with multiple chronic health conditions which, with support, can be managed at home through family caregivers, resulting in an increase in referrals to home health-care agencies from hospitals and physician's offices.[2]
Home health-care systems are able to support most medical needs for individuals of all ages in their place of residence. This system of care can provide services ranging from supplying and teaching a patient and/or caregivers how to use mobility aids to more complex services, such as physical and mental assessments, medical interventions such as wound care, medication education and monitoring as well as pain management and speech, physical, and occupational therapies.[1,4] Home healthcare also benefits the patient through preserving their privacy, dignity, and comfort.[5] Providing care in one's residence is a crucial component of managing chronic conditions, as patients can learn ways to manage their health on a daily basis with the appropriate resources.[2]
The Iranian health-care system is facing several challenges, such as a lack of human resources and a shortage of hospital beds. Even with limited resources, a community-based home health-care system could support managing many of the country's health-care needs.[6] However, despite a growing trend of home healthcare, the concept of such a system may be vague and implemented in a variety of ways in different countries.[7] The World Health Organization defines home healthcare as a system of care for patients in their home to assist them in the prevention or postponement of their need for long term or acute medical care.[8] This generic definition lacks the detailed descriptions of the scope of care, the target groups that would benefit from this model of care, this care's functions, and the expected and measurable outcomes. A review of studies conducted in this area does not provide the guidance needed for developing a system that would best meet Iran's home health-care needs. A more precise analysis of the concept of home healthcare is therefore required so that a clearer understanding of the characteristics of such a system, its antecedents, and its outcomes may be achieved. Exploring the home health-care concept and its distinguishing characteristics may assist countries to assess, plan, implement, and evaluate a system that meets each patient's needs and the resources that are available.[7,9] In this regard, the present study was done with the aim of clarifying the concept of home healthcare by using a hybrid model.
Materials and Methods
An in-depth analysis of the home health-care concept was conducted in 2020 by using the hybrid concept analysis method. The hybrid concept analysis method is the exploration of an individual concept using both a theoretical phase of data collection from the research literature and a fieldwork phase through participant data collection.[10] The process is useful while the concept is still being developed and is unclear from the published literature. Thus, the value of this method over other literature reviews (systematic and scoping) is its inclusion of fieldwork data from individuals who have experience with the phenomenon. This is an important step for concepts, eventually resulting in the development of organizational structures, health policy and the health-care providers' practice. The hybrid concept analysis method is based on the disciplines of philosophy, sociology, and field research. Using inductive and deductive analyses, the hybrid concept analysis process lays the groundwork required to design research studies on an identified concept. Often, the literature provides insufficient information or multiple interpretations of a concept thus a clearer definition is needed in order to design future studies.
The model consists of three phases: 1) theoretical; 2) fieldwork; and 3) the final analysis. The theoretical phase reviews the existing literature and extracts all of the concept descriptions in order to develop an operational concept definition. While continuing to search the literature for the defining characteristics of the concept, the fieldwork phase is started. The fieldwork phase involved qualitative data collection by interviewing the participants who have had experience with the concept. It is important that phase two is started while still researching the concept in the literature, in order for the researchers to remain open to the rich experiences that participants may add to our understanding of the concept.
During the third and final phase, the data collected from the first two phases, theoretical and fieldwork, are compared and contrasted. At this time, the theoretical analyses and insights from observations and interviews are combined to develop an in-depth knowledge of the concept.[10]
Theoretical phase
Multiple databases were searched, including Science Direct, PubMed, ProQuest, Google Scholar, and Scopus using the keywords: home-based care, home healthcare, and home care. More databases were not searched, because we reached saturation on home health-care descriptions and no new descriptors were found. The time period search was 2007 to 2019 and focused on understanding, “What is the definition of home healthcare?”; “Who benefits from home healthcare services?;” and “What are the outcomes of home healthcare?” Publication inclusion criteria were for them to be Persian or English and the keywords were found in the title or the abstract. Exclusion criteria were inaccessibility to the full-text literature or the publications were unrelated to the identified concepts. The primary search was conducted independently by the first and second authors and verified by the fourth author. This phase yielded 400 publications, from which 200 were eliminated based on the exclusion criteria. The remaining 200 were reviewed, resulting in 18 publications addressing the research questions. Content analysis was used to review the articles and they were coded based on concept characteristics. The publication selection process is shown in Figure 1.
Figure 1.
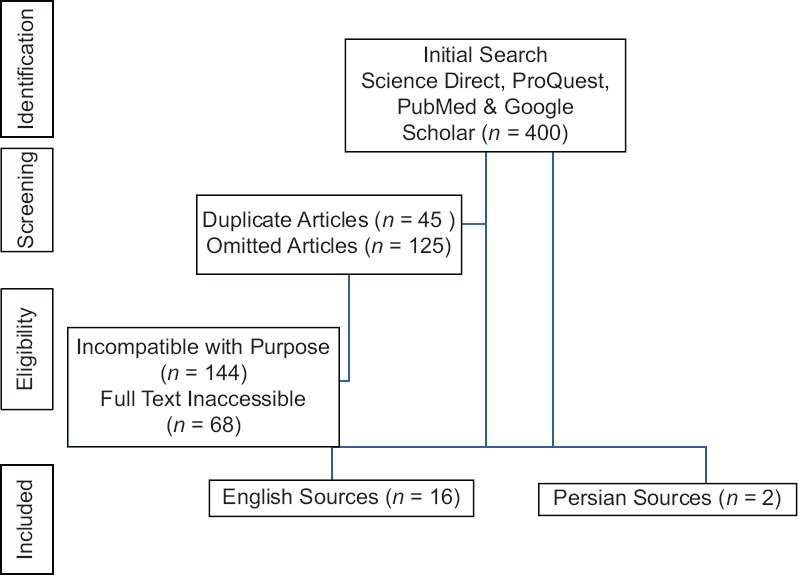
Source selection process in the theoretical phase
Fieldwork phase
The second phase focuses on enhancing and refining the content gathered from the theoretical phase.[10] Six participants were recruited using purposive convenience sampling: four nurses with two or more years of home health-care experience one policymaker with 3 years of home health-care experience, and a home health-care agency director with 5 years of experience. The interviews were conducted using open-ended semistructured questions. The questions were developed based on the literature review and included questions such as: “What is your definition of home healthcare?”, “What types of services are included in the home healthcare setting and which patients benefit the most?” The participants were encouraged to elaborate with follow-up questions, such as: “Tell me more about that.” or “Please share an example.” The interviews were conducted at a time and place convenient for the participants and informed consent was obtained. The interviews were audiorecorded and field notes were taken. The interviews were then transcribed and reviewed by the participants to verify transcription accuracy. Qualitative content analysis was conducted after each interview and informed subsequent interviews conducted with additional participants. The texts were appraised multiple times by researchers and coded into themes. The themes were examined, categorized, and subcategorized as illustrated in Figure 2.
Figure 2.
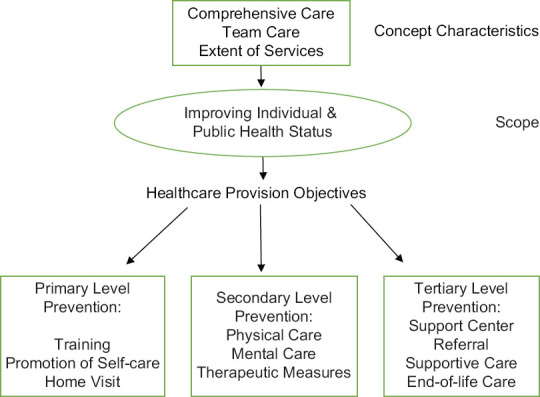
Themes related to home health-care's concept characteristics, antecedents, and outcomes
The final analytic phase
During the final analytic phase, descriptions and themes from the first two phases were combined. For this phase, the codes from the theoretical phase were extracted and compared against those of the fieldwork phase, whereas at a later stage a complete and comprehensive definition including a range of characteristics was developed.
Ethical considerations
The Ethics Committee of Iran University of Medical Sciences approved this study (Ethical code: IR.IUMS.REC.1399.117). Interested participants were informed of the study purpose and were then provided with an informed consent form to read and sign.
Results
Theoretical phase
The concept definitions require a contextual assessment addressing multiple key perspectives. A solid definition includes the descriptions answering the “who, what, when, where and why questions.” Describing a concept in this way assures the researcher that a comprehensive definition has been obtained. Thus, from the theoretical phase of data collection, we describe our findings.
Where is home healthcare provided? As may be expected, all definitions from the literature refer to home healthcare as the delivery of care in a person's home or residence. The patient could be young or old, living alone or with family members. Home is where a person spends most of their time and it is a place of comfort to live and manage everyday life. It is a familiar and safe environment and is less stressful than the hospital. Stress can delay healing so being at home can promote healing. Patients are with their friends and family, able to eat familiar foods, and are in control of their daily schedule and activities.
Who provides home healthcare? In addition to care being delivered at home, another theme found in all the literature reviewed was the presence of health-care professionals. Studies described how home healthcare is provided by professionals with a variety of education and skills, including licensed professionals as well as nontechnical staff, such as home health-care aides providing basic personal care.[11] Most of the literature talked about nurses delivering home healthcare; however, the literature was clear in that home healthcare is provided by a multiprofessional team. This team includes several disciplines, such as physicians, physiotherapists, nutritionists, rehabilitation therapists (physical, occupational, and speech), and psychiatrists.[12] The definitions of home healthcare also emphasize the importance of collaboration and communication among the various professionals for the patient to experience positive outcomes. In addition to each discipline providing their services, often a physician serves as a gatekeeper to this care. Physicians have the operational authorization to order home healthcare and they are routinely provided with reports regarding the patient's status and progress.
When is home healthcare provided? The implementation of home health-care services often occurred after an acute illness. Similarly, another study suggests that home healthcare may be a requirement after a hospital's discharge of patients with multiple conditions, acute illnesses, a new illness (such as type 2 diabetes), patients suffering from poor health needing close monitoring, or palliative/end-of-life care.[13]
In the presence of knowledgeable nurses, exacerbations of acute illnesses may be addressed in a timely manner, potential postsurgical complications may be avoided or minimized, chronic conditions and medications could be tightly managed, and rehabilitation could be shorter and tailored to the patient's functional needs at home.[14] For instance, a wound care nurse could be a key factor in the remediation of bedsores or surgical wounds in the home setting.[15] Positive outcomes of home healthcare for older adults and their caregivers could be the promotion and maintenance of independence and dignity, as well as avoiding nursing home admissions.[4] In addition, quality of life and overall improvements in the patient's health status were also listed as home healthcare's positive outcomes.[11,16]
Some studies focused on how home healthcare could meet the needs of children and adolescents with special care requirements or with chronic physical, developmental, behavioral, or emotional problems requiring complex and advanced interventions.[17] Other literature reported that patients with mental health conditions also benefit from home healthcare, as nurses and therapists could monitor medication issues and the patients felt safe and secure in their familiar home environment.[18,19] For these populations the nurses' knowledge, patient's prognosis, delivery of care, and the family needs were alleviated when services were provided in the home.
What is included in home healthcare? Home healthcare applies to all ages and one of the antecedents of this care is patients' and their families' preference to receive medical attention at home.[16] The top priorities of home healthcare were supporting the patient's functional independence, health maintenance check-ups, and family inclusion during treatment and recovery.[13] In other studies, various levels of dependency determined the implementation of home healthcare.
Why is home healthcare needed? Communities are developing home health-care services, as our health-care needs are shifting from acute care to the management of chronic conditions. Challenges do exist in providing care in the home, for instance maintaining supplies and equipment as well as coordinating the health-care professionals' visits and their productivity. The outcomes of home healthcare described by the literature were significant. Home healthcare reduced the length of hospital stays, decreased the rate of hospital re-admissions, reduced the acute care bed occupancy rate and emergency room visits and extended nursing care without increasing costs, and resulted in less dependence on the health-care system.[5,10,18] Most importantly, home healthcare promotes communication between the home health-care professional staff, patients, family, and physicians and assists in assuring the quality of care.[20]
See Table 1 for a summary of the literature review. According to the studies reviewed, home healthcare is defined as a holistic, professional, and multidisciplinary care service. The services are provided by a range of health-care specialists from various community organizations. The location of care is the patient's place of residence. The purpose of care is to address post-acute or chronic conditions and promote healing or assist in managing a chronic condition. Home health-care systems address the needs of patients of all age groups with the goal of improving their quality of life.[21]
Table 1.
A summary of the study review on the concept of home healthcare
| Author/year | Characteristics | Antecedents (requirements, facilitators) | Outcome (s) |
|---|---|---|---|
| Ajlouni, et al., 2015 | Professional care or supportive care at home | Different levels of dependency | Life at home, mitigating the need to attend a health-care center such as the retirement home |
| Almoajel, 2016 | The underlying notion of home healthcare is defined as medical care with the least possible complexity | Medical team presence, health coach presence | Individual functionality improvement, preserving patient’s integrity, status check-up, family cooperation |
| Beijer, et al., 2018 | Multidisciplinary care at the patient’s residence | Requiring professional cooperation | |
| Bliss, et al., 2013 | Suffering from multiple illnesses, recuperation from a recent illness or surgery, the presence of skilled nurses in accordance with the needs of the patients. For instance, a nurse specializing in wound care | Shortened period of rehabilitation and other healthcare centers, effective medical care for bedsores, surgery wound | |
| Cire and Diamant, 2018 | Professional medical care, community support, patient-centered care at home | Authorized agencies, registered nurses, physiotherapists, & aides Effective communication between caregiver and patient. Quality referral system |
|
| Elias and Murphy, 2012 | Providing care for special need children and adolescents at home | Children and adolescents with physical, developmental, behavioral, and chronic emotional conditions who need complex medical care for survival. Knowledgeable and skillful nurses, prognosis, end-of-life care, and the needs of the families of the patients | Children and adolescents’ health status improvement |
| Foust, et al., 2012 | Helping patients to recover their health while maintaining their freedom and sufficiency in a home health-care setting | Remaining in the familiar and comfortable environment of home, preserving the integrity, sufficiency | |
| Ghaderi, 2012 | Providing services at home | Prolonged convalescence period | Less possibility for hospital infection, more effective treatment |
| Han, et al., 2013 | Covering all age groups, especially elderly individuals at their homes | Patient and family preference | Elderly citizens’ freedom, quality of life, and health status |
| Jones, et al., 2017 | Hospital referral upon discharge after an acute illness, especially in multiple illnesses or poor health status | Reduction in re-admission rate | |
| Mukamel, et al., 2014 | Requiring long-term care, patients’ and families’ needs | Patient and family satisfaction, safety and comfort | |
| Russell, et al., 2011 | A wide range of professional and supportive care that enables individuals to manage their own situations at home | A positive outcome in case of the continuous relationship between caregiver and recipient | Less risk of re-admission, less need to receive emergency medical services |
| Shahsavari, et al., 2018 | A wide range of care from basic to advanced | Patient and family needs, nursing teams from all levels of proficiency and education, doctors, physiotherapists, psychologists, and nurse aides for basic care | Reduction in re-admission rate, bed occupancy rate, reduction in ER admissions, better quality of life |
| Shamsaii, 2007 | Human care and sympathy | The case of chronic mental illness such as schizophrenia | Effective treatment planning based on communication |
| Shang, et al., 2014 | Medical care provided by a team of specialist at the patient’s house | Shorter hospital stay, less medical expenses, receiving care in a familiar environment, preserving the integrity and self-sufficiency | |
| Thome, et al., 2003 | Home as the location for providing services | Multidisciplinary team (physician, nurse, physiotherapist, nutritionist, psychologist, speech therapist, occupational therapist) | Human care as a component of the health treatment process, hospital costs reduction |
| Wang, et al., 2017 | Nursing professional care, occupational therapy, speech therapy, physiotherapy, supportive care for daily routines | Requiring care after acute illnesses | Cost reduction, shortening hospital stay, quality of life improvement, first-rate basic care |
Fieldwork phase
The results of this phase were divided into three areas: (1)- comprehensive care: with subthemes of holistic and team care; (2)- extent of services: with subthemes of primary, secondary, and tertiary prevention; and (3)- outcomes of home healthcare: with subthemes of individual, family, and community health system levels.
Comprehensive care: A home health-care system must provide “comprehensive care,” which includes both holistic and team care. Holistic care was identified with most of the participants stating that a patient should be cared for as a whole person, and that this goal could best be met in the home setting. One nurse stated, ”We must look at the patient in a holistic manner. I cannot tell a patient that … I do not concern myself with your job or your children.” (nurse, 8 years' experience).
Another nurse shared, ”In a home setting, we can observe many factors that play a part in a patient's health status. For example, the physical environment of the house or the kinds of relationships in the family.this will help give better and more thorough care.” (nurse, 10 years' experience).
Team care was highlighted by the participants and they discussed how better care was provided when specialists from different fields collaborated to meet treatment goals. One nurse shared, “When I attend the patients in their homes, at times there are issues that I cannot see to by myself. That is when I call on …colleagues for help. For instance, we know that after a laryngeal surgery, vocal rehabilitation is needed. So, we ask a speech therapist to attend the patient.that is why a team of professionals must be involved in the care process” (nurse, 12 years' experience).
The Extent of Services: An important descriptor of the home health-care system by participants was for it to include a wide range of services covering all age groups and all illnesses. A participant elaborated, ”Overall, it can be applied to all diseases. Whether it is a person with a disability or someone who suffers from psychological problems.from a simple injection to more complex medical treatments.for all ages, from children to elderly persons.” (nurse, 8 years' experience).
Most participants agreed that services, such as training, prompt diagnosis, effective treatment, rehabilitation, and palliative care in home healthcare may be categorized with primary, secondary, and tertiary levels of health promotion and prevention methods.
Primary prevention measures in home health-care systems often occur in conjunction with secondary or tertiary care that has been initiated. These measures focus on the prevention of new conditions or reduce or eliminate causative risk factors. One nurse shared, ”I, for instance, know that taking primary prevention measures means that during the home visits I should advise on self-care behaviors” (nurse, 8 years' experience).
A home health-care agency director commented, “For patients with a high risk of developing diabetes or blood pressure, education is given so as to mitigate that risk” (home health-care director, 17 years' experience). In the secondary level of prevention, medical measures include early interventions for exacerbations of related sequalae. ”Every time I am assigned to give medical care to a patient with diabetes, I watch over timely medicine consumption, I check their blood sugar level, I give those instructions as to how to prevent diabetic foot.” (nurse, 12 years' experience).
Tertiary prevention includes areas of healthcare, such as rehabilitation, supportive care, and end-of-life palliative care. ”A nurse in a home care setting can tell you which centers in the community will provide you with the help that you seek and can refer you to that center” (nurse, 6 years' experience). ”.there are patients whose status is beyond any hope of recovery.in such cases, many of the patients and even their families seek to spend the last days together at home. They want to avoid spending the [precious time they have left] in a hospital environment. So, they need people to give them nursing care at home” (nurse, 4 years' experience).
Positive Outcomes of a Home Health-care System: Another benefit of home healthcare described by participants was the positive outcomes for patients when receiving home healthcare. Positive outcomes were discussed at three levels, individual, family, and community. On the individual level, the positive outcomes were related to receiving care in the comforting, convenient, and safe environment of their home, strengthening their self-esteem, providing freedom, decreasing medical expenses, and avoiding unnecessary care. One participant stated, “When patients receive care at their own houses there is less need for commuting, and at times they can see to a problem just by a phone call. All of this reduces their expenses” (health policymaker, 24 years' experience).
Another participant stated, “A patient will receive medical care in the peaceful environment of their own home…when a nurse frequents a patient's home, the patient learns what needs to be done so he or she will cooperate more and takes on more responsibility. In this way, as time goes by, they can practice self-care while being watched over…” (nurse, 12 years' experience).
On the family level there are fewer expenditures for medical treatment, a decreased need to take off from work, less stress in the process of caring for their loved one, and feeling more confident in providing care as they continue to receive training and instruction as to what they should be doing. One nurse shared, “Since the care is given in the presence of the family members, it becomes possible to include them in the treatment…this will enable the family to become self-sufficient” (nurse, 12 years' experience).
Another nurse elaborated, saying, ”Economically speaking, it becomes much more practical for families to receive home care for their patients. It is not only about the cost of treatment. Once a family member is admitted to a hospital, others must take [leave] from work which in the long run will add up to an even bigger number” (nurse, 8 years' experience).
For the community, a health policymaker elaborated that, “The hospital beds will become unoccupied again… [decrease] in emergency room [use]… as issues can be easily taken care of in a home setting. But since [at this time] they do not have access to such a system they will need to go to the hospital.” (health policymaker, 24 years' experience).
Therefore, ”if you combine all the positive [outcomes a home healthcare] system, the society as a whole will benefit from it all” (nurse, 12 years' experience).
Final analytic phase
The results from the final analytic phase of this study suggest that the concept of home healthcare refers to professional medical care addressing individual, family, and societal needs, includes a wide range of services, and focuses on all levels of preventive strategies, resulting in the improvement of society's health status. In this hybrid concept analysis, the findings from the theoretical phase are supported by the field-research phase findings. This analysis provides a clearer understanding of the home health-care system concept. This concept may be achieved and defined as a comprehensive, professional, and holistic medical care system that includes services provided by teams of specialists for the purpose of promoting individual care at all three levels of prevention. Home health-care services are provided at one's place of residence while preserving the patient's dignity, comfort, safety, and overall quality of life. In addition, home healthcare reduces expenditures at all levels and supports patients and families to become self-sufficient, decreasing health system burdens.
Discussion
The results of the present study suggest that home healthcare is to include comprehensive and holistic medical teamwork. The definition, however, does not include a direct association between home healthcare and professional human caring. This may be because from the viewpoint of the participants, the two concepts of “professional” and “human” are implied from the word “care” which, of course, at all times is the essence of nursing. Another issue discussed in the fieldwork phase of this study was the idea of preventive strategies used in home healthcare. This theme was not discussed in the literature review phase and only one home health-care study discussed a range of primary to advanced care.[11] According to the participants, however, all three levels of prevention strategies may be applied in the home health-care setting. According to the participants' interpretation of preventive care, such care is an antecedent of the concept of the home health-care system. In many studies, the home health-care setting focused on the patient's need for long-term care, wound care, or rehabilitation.
Another antecedent of home healthcare is supporting the relationship between the caregiver and the recipient when addressing mental health issues, supportive care, and end-of-life care. The participants interviewed in this study agreed that one of the most positive outcomes of care in the home setting is the communication and promotion of self-esteem facilitating the preservation of a patient's integrity.[22] In reviewing the studies items such as receiving care in a peaceful and safe environment and lower costs were given special attention. According to the interviews, this is because the participants put more emphasis on a patient's individual outcomes such as being with family during their last days and avoiding the incurrence of unnecessary care. In a recent study, being with family members and not needing multiple physician appointments at medical centers were mentioned as the main preferences for home healthcare.[4] The participants expanded on this idea by explaining that having end-of-life care in the hospital might not be of any benefit to the patients. In one study, it was discussed that unnecessary routine care at the end-of-life may cause more suffering for the patient.[23] Regarding positive outcomes on the family level, the findings from the reviews and participant interview data do support each other. This topic has received special attention in a couple of studies, suggesting that one of the benefits of home healthcare is a reduction in costs through avoiding unnecessary care.[21,24] From this analysis, home healthcare should be described as a comprehensive, professional, and holistic care system accompanied by medical services and professionals whose goals are supporting of the individual's health and providing care at their place of residence. The focus of care includes preventative interventions, in addition to strategies to manage chronic health conditions.
The strength of this study is the use of a concept analysis method going beyond the published literature. Adding fieldwork provides a richer understanding of the concept, as well as ideas for future directions. This study's limitations are the views of physicians, patients, and their families who engage with home healthcare were not interviewed. The participants' viewpoints only included those of nurses and policymakers. In future studies, a more diverse sample would be useful to insure all dimensions of the concept are analyzed.
Conclusion
This article facilitated a clearer understanding of the home health-care concept, including the system, outlook, importance, and applicability.[25] Home healthcare continues to be developed in countries around the world, as the monitoring and managing of chronic conditions becomes more prevalent for populations. Our findings in this paper serve as a foundation for further inquiry and investigation. This analysis of home healthcare provides information to be used by policymakers, organizational leaders, and educators to assure a health-care delivery system that would benefit the health of communities and countries.[26,27]
Financial support and sponsorship
Tabriz University of Medical Sciences
Conflicts of interest
Nothing to declare.
Acknowledgements
The authors would like to express their gratitude to all whom participated in the present study (approved project no. 98-4-99-16806).
References
- 1.Beer JM, Mcbride SE, Mitzer TL, Rogers WA. Understanding challenges in the front lines of home healthcare: A human-systems approach. Appl Ergon. 2014;45:1687–99. doi: 10.1016/j.apergo.2014.05.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mukamel DB, Fortinsky RH, White A, Harrington C, White LM, Ngo-Metzger Q. The policy implications of the cost structure of home health agencies. Medicare Medicaid Res Rev. 2014;4:1–21. doi: 10.5600/mmrr2014-004-01-a03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Dieckmann JL. Burlington: Jones & Bartlett Learning; 2015. Home Healthcare: A Historical Perspective and Overview. Handbook of Home Healthcare Administration; pp. 10–14. [Google Scholar]
- 4.Ajlouni MT, Dawani H, Diab SM. Home Healthcare (HHC) Managers perceptions about challenges and obstacles that hinder HHC services in Jordan. Glob J Health Sci. 2015;7:121–9. doi: 10.5539/gjhs.v7n4p121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Shang J, Poghosyan L, Dowding D, Stone P. The prevalence of infections and patient risk factors in home healthcare: A systematic review. Am J Infect Control. 2014;42:479–84. doi: 10.1016/j.ajic.2013.12.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Nasrabadi AN, Almasian M, Heydari H. Exploration of the administrative aspects of the delivery of home health care services: A qualitative study. Asia Pac Fam Med. 2018;17:1–7. doi: 10.1186/s12930-018-0038-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Thome B, Dykes AK, Hallberg IR. Home care with regard to definition, care recipients, content and outcome: Systematic literature review. J Clin Nurs. 2003;12:860–72. doi: 10.1046/j.1365-2702.2003.00803.x. [DOI] [PubMed] [Google Scholar]
- 8.Busse R, Blumel M, Scheller-Kreinsen D, Zentner A. Tackling chronic disease in Europe: Strategies, interventions and challenges. World Health Org. 2010. Available from: https://www.euro.who.int/__data/assets/pdf_file/0008/96632/E93736.pdf .
- 9.Ghaderi H, Shafiee H, Amery H, Vafaeinasab MR. The cost-effectiveness analysis of hospital compared to at homeCVA patients. J Healthc Manag. 2012;3-4:7–15. [Google Scholar]
- 10.Rodgers BL, Knafi KA. Philadelphia: Saunders; 2000. Concept Development in Nursing: Foundations, Techniques, and Applications. [Google Scholar]
- 11.Shahsavari H, Nasrabadi AN, Almasian M, Heydari H, Hazini A. Exploration of the administrative aspects of the delivery of home healthcare services: A qualitative study. Asia Pac Fam Med. 2018;17:1–7. doi: 10.1186/s12930-018-0038-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cire AA, Diamant A. Dynamic Scheduling of Home Healthcare Patients to Medical Providers. 2018 doi: 10.2139/ssrn. 3210339. [Google Scholar]
- 13.Almoajel A. Perception and knowledge of healthcare professionals toward home healthcare in Riyadh. Life Sci J. 2016;1:106–12. [Google Scholar]
- 14.Heydari H. Home-based palliative care: A missing link to patients' care in Iran. J Hayat. 2018;24:97–101. [Persian] [Google Scholar]
- 15.Bliss D, Westra BL, Savik K, Hou Y. Effectiveness of wound, ostomy and continence–certified nurses on individual patient outcomes in home healthcare. Home Healthcare Nurs. 2014;32:31–8. doi: 10.1097/NHH.0000000000000012. [DOI] [PubMed] [Google Scholar]
- 16.Han SJ, Kim H K, Storfjell J, Kim MJ. Clinical outcomes and quality of life of home healthcare patients. Asian Nurs Res. 2013;7:53–60. doi: 10.1016/j.anr.2013.03.002. [DOI] [PubMed] [Google Scholar]
- 17.Elias ER, Murphy NA. Home care of children and youth with complex healthcare needs and technology dependencies. Pediatrics. 2012;5:996–05. doi: 10.1542/peds.2012-0606. [DOI] [PubMed] [Google Scholar]
- 18.Jones CD, Wald HL, Boxer RS, Masoudi FA, Burke RE, Capp R, et al. Characteristics associated with home healthcare referrals at hospital discharge: Results from the 2012 national inpatient sample. Health Ser Res, 2017;52:879–94. doi: 10.1111/1475-6773.12504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Shamsaii F, Cheraghi F, Ghaleealiha A. Effects of home psychiatric nursing care in treatment of schizophrenic patients. J Ilam Univ Med Sci. 2007;15:32–8. [Persian] [Google Scholar]
- 20.Russell D, Rosati RJ, Rosenfeld P, Marren JM. Continuity in home healthcare: Is consistency in nursing personnel associated with better patient outcomes? J Healthc Qual. 2011;33:33–9. doi: 10.1111/j.1945-1474.2011.00131.x. [DOI] [PubMed] [Google Scholar]
- 21.Wang Y, Leifheit-Limson EC, Fine J, Pandolfi MM, Gao Y, Liu F, et al. National trends and geographic variation in availability of home healthcare: 2002–2015. J Am Geri Soc. 2017;65:1434–40. doi: 10.1111/jgs.14811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Johnston B, Lawton S, McCaw C, Law E, Murray J, Gibb J, et al. Living well with dementia: Enhancing dignity and quality of life, using a novel intervention, Dignity Therapy. Int J Older People Nurs. 2016;11:107–20. doi: 10.1111/opn.12103. [DOI] [PubMed] [Google Scholar]
- 23.Yekefallah L, Ashktorab T, Manochehri H, Alavimajd H. Intensive care nurses' reaction to futile cares: A phenomenological study. J Holist Nurs Midwifery. 2016;26:107–17. [Google Scholar]
- 24.Rostami S, Esmaeali R, Jafari H, Shorofi SA. Perception of futile care of nurses in intensive care units. Iranian J Medl Ethics Hist Med. 2017;10:155–64. [Google Scholar]
- 25.Ghafari S, Mohammadi F. Concept analysis of nursing care: A hybrid model. J Mazandaran Univ Med Sci. 2012;21:153–64. [Persian] [Google Scholar]
- 26.Foust JB, Vuckovic N, Henriquez E. Hospital to home health care transition: Patient, caregiver, and clinician perspectives. West J Nurs Res. 2012;3:194–12. doi: 10.1177/0193945911400448. [DOI] [PubMed] [Google Scholar]
- 27.Beijer U, Vingare EL, Eriksson HG, Umb Carlsson Õ. Are clear boundaries a prerequisite for well-functioning collaboration in home health care.A mixed methods study? Scan J Caring Sci. 2018;32:128–37. doi: 10.1111/scs.12438. [DOI] [PubMed] [Google Scholar]