

Abstract
Raised blood pressure (BP) remains the biggest single risk factor contributing to the global burden of disease and to global mortality. Although a substantial number of people who have hypertension are either oblivious of it, not treated, or being managed but remain uncontrolled. May Measurement Month (MMM) is a global initiative led by the International Society of Hypertension (ISH) with the goal of increasing awareness of high BP and serving as a spur to establish screening programmes worldwide. An opportunistic cross-sectional survey of volunteers aged ≥18 years was carried out in May 2019. Measurement of BP and collection of relevant health information were performed according to a standardized protocol for MMM. Screening sites were set up in churches, mosques, health facilities, pharmacies, recreational parks, sports facilities, shopping centres, marketplaces, universities, workplaces, and community centres across four regions of Ghana. A total of 7102 participants gave their consent and were screened during MMM 2019. After multiple imputation, of all 7102 participants 1836 (25.9%) had hypertension. Of all 1836 participants with hypertension, 36.5% were aware of their status and 30.0% were on anti-hypertensive medication. Of 550 participants on antihypertensive medications, 46.1% had controlled BP (systolic BP <140 mmHg and diastolic BP <90 mmHg). Also, of all 1836 participants with hypertension, 13.8% had their BP controlled. Again, the proportion of participants with hypertension of those not receiving anti-hypertensive treatment was 1286 (19.6%). Data obtained from this project demonstrates that there is still a significant number of people with hypertension who are unaware of having it, are untreated, or are on treatment but remain uncontrolled. It also highlights the significance of BP screening campaigns as a tool to identify persons with elevated BP.
Keywords: Hypertension, Blood pressure, Screening, Treatment, Control
Introduction
Hypertension is the leading risk factor contributing to the global burden of disease and to global mortality.1 It is also an important global health challenge due to its high prevalence and resulting morbidities.2 It is estimated to result in about 11 million deaths globally. It also accounts for 57 million disability-adjusted life years annually and a major risk factor for coronary heart disease and ischaemic as well as haemorrhagic stroke.3
The World Health Organization estimates that in Ghana—a country in Sub-Saharan Africa, Non-Communicable Diseases account for an estimated 34% deaths and 31% of disease burden. Also, HIV, Malaria among other diseases contribute significantly towards overall disease burden. However, hypertension has been a major cause of cardiovascular disease morbidity and mortality over the last four decades.4 Nevertheless, its awareness, treatment, and control are poor.5,6 Researchers have observed that physical inactivity, use of alcohol, poor diets, obesity, among other risk factors were associated with the increasing prevalence of hypertension.7 The upsurge in these risk factors across several African countries have contributed to the high burden of the condition.8
It has also been observed that just about half of the population with hypertension are aware of having it.9 Therefore, identifying persons with high blood pressure (BP) through screening campaigns, making them aware of their condition and starting them on treatment is of critical importance for promotion of population health and reduction of disease burden. Ghana participated in the worldwide hypertension awareness campaign, May Measurement Month (MMM19), in an effort to increase national awareness about hypertension.
Methods
A convenience sampling method assisted by volunteers was employed for the MMM BP screening study. The study was coordinated by a team of health professionals from various institutions in the country. Ethical approval was obtained from the ethics review committee of the Ghana Health Service. About 75 sites were set up in churches, mosques, health facilities, pharmacies, recreational parks, sports facilities, shopping centres, marketplaces, universities, workplaces, and community centres across four regions of the country. Representatives from the participating regions who were trained health professionals organized training sessions on how to measure BP via video demonstrations for all the screening volunteers. Limited financial support also came from individual donors. Media publicity in a number of radio stations as well as TV stations were organized. Large banners were also displayed in public places to help with publicity.
Target participants were adults (≥18 years) who ideally had not had their BP measured in the previous year. Hypertension was defined as a systolic BP ≥140 mmHg or diastolic BP ≥90 mmHg (based on the mean of the second and third of three BP readings) or on treatment for hypertension. Four weeks was dedicated for the screening activities. OMRON BP monitors donated to the International Society of Hypertension (ISH) by OMRON Healthcare were used for the screening campaign. In the measurement of the three BP readings, participants were seated with their backs supported and legs resting on the ground in an uncrossed position. Data obtained were initially collated by country leads, cleaned by the MMM project team and analysed centrally by MMM project team statisticians. Multiple imputation was performed to impute the mean of the second and third BP readings where they were missing, using the global data. Details of data collection and analysis can be referred to from the Methods section of the MMM global paper.10
Results
A total of 7102 participants were screened during the study, comprising 3683 (51.9%) females and 3416 (48.1%) males with the sex of 3 (0.0%) being unknown. The mean age of participants was 38.3 years (SD 14.7 years) with the ethnicity of the vast majority (99.5%) being black. Of the total number of participants screened, 1639 (23.1%) were overweight and 1163 (16.4%) were obese. Again, of the total number of persons screened, 550 (7.7%) were on anti-hypertensive medications, 55 (0.8%) were on a statin, and 80 (1.1%) were on aspirin. Also, 1419 (20.0%) of the total number of participants screened reported that they had never had their BP measured.
| Total participants | Number (%) with hypertension | Number (%) of hypertensives aware | Number (%) of hypertensives on medication | Number (%) of those on medication with controlled BP | Number (%) of all hypertensives with controlled BP |
|---|---|---|---|---|---|
| 7102 | 1836 | 36.5% | 30.0% | 46.1% | 13.8% |
After multiple imputation, of all 7102 participants, 1836 (25.9%) had hypertension. Of all 1836 participants with hypertension, 36.5% were aware of their status and 30.0% were on anti-hypertensive medication. Of 550 participants on antihypertensive medications, 46.1% had controlled BP. Of all 1836 participants with hypertension, 13.8% had their BP controlled (systolic BP <140 mmHg and diastolic BP <90 mmHg). The proportion of participants screened who were not receiving anti-hypertensive treatment but were found to have hypertension was 19.6% (1286).
It can also be observed that compared to those of healthy weight, BP was significantly higher in overweight or obese participants, and significantly lower in underweight participants (Figure 1).
Figure 1.
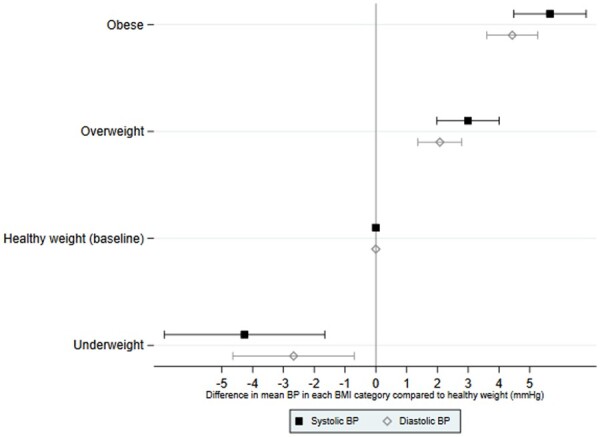
Difference in mean blood pressure in each body mass index category compared to healthy weight (mmHg).
Discussion
MMM, as a global initiative by the ISH, provides an opportunity and a large platform to employ a relatively inexpensive, volunteer-based, convenience sampling method to screening BP in an effort to increase national awareness of hypertension.
This MMM study in Ghana aimed at identifying persons with hypertension in the community and also highlighted the need to control the BPs of all who require intervention according to established guidelines.
The study identified 25.9% of total participants having hypertension. Of all hypertensive participants, 36.5% were aware of their status, 30.0% were on anti-hypertensive medication, and 46.1% of those on anti-hypertensive medications had BP controlled.
MMM activities especially the screening campaign has created the platform for a number of people to be screened and also be educated on hypertension and some risk factors. The results presented here however are based on an opportunistic screening campaign, and recruitment was not randomized and is therefore not nationally representative. By design, as a cross-sectional survey, true prevalence of hypertension cannot be inferred here and data on individual outcomes are unavailable. In addition, recording BP at one instance (though repeated three times) is obviously likely to involve capture of false positives who would have been provided with lifestyle advice and encouraged to see their GP for official testing. Moreover, the proportion of persons with hypertension volunteering to participate may have introduced a selection bias leading to overestimation of the true proportion of hypertensive persons.
However, despite these limitations, this study sought primarily to raise awareness. Persons found to have untreated hypertension, or uncontrolled BP on treatment, were advised and referred to health facilities for further treatment.
Acknowledgements
Our sincere gratitude to the International Society of Hypertension for the support towards a successful project. Many thanks also to the representatives of the participating regions as well as the selfless screening volunteers for their help to make MMM 19 a successful event. Without their selfless support the goal of MMM 19 would not have been achieved.
Funding
Most of the funds came from contributions of MMM Ghana team members with some little contributions from a couple of anonymous individuals.
Conflict of interest: none declared.
References
- 1.GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018; 392:1923–1994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Mills KT, Bundy JD, Kelly TN, Reed JE, Kearney PM, Reynolds K, Chen J, He J.. Global disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. Circulation 2016;134:441–450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.WHO Global Health Observatory. https://www.who.int/gho/ncd/risk_factors/blood_pressure_prevalence_text/en/ (7 October 2019).
- 4. Sanuade OA, Boatemaa S, Kushitor MK.. Hypertension prevalence, awareness, treatment and control in Ghanaian population: evidence from the Ghana demographic and health survey. PLoS One 2018;13:e0205985. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Sanuade OA, Awuah RB, Kushitor M.. Hypertension awareness, treatment and control in Ghana: a cross-sectional study. Ethn Heal 2020;25:702–716. [DOI] [PubMed] [Google Scholar]
- 6. Sarfo FS, Acheampong JW, Appiah LT, Oparebea E, Akpalu A, Bedu-Addo G.. The profile of risk factors and in-patient outcomes of stroke in Kumasi, Ghana. Ghana Med J 2014;48:127–134. PMID: 25709121 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Awuah RB, Afrifa-Anane E, Agyemang C. Cardiovascular disease, diabetes and established risk factors in low- and middle-income countries. In de-Graft Aikins A, Agyeman C, eds. Chronic Non-Communicable Diseases in Low- and Middle-Income Countries. UK: CAB International; 2016, pp. 1–13.
- 8. Addo J, Agyemang C, Smeeth L, de-Graft Aikins A, Edusei AK, Ogedegbe O.. A review of population- based studies on hypertension in Ghana. Ghana Med J 2012;46:4–11. [PMC free article] [PubMed] [Google Scholar]
- 9. Chow CK, Teo KK, Rangarajan S, Islam S, Gupta R, Avezum A, Bahonar A, Chifamba J, Dagenais G, Diaz R, Kazmi K, Lanas F, Wei L, Lopez-Jaramillo P, Fanghong L, Ismail NH, Puoane T, Rosengren A, Szuba A, Temizhan A, Wielgosz A, Yusuf R, Yusufali A, Mckee M, Liu L, Mony P, Yusuf S; PURE (Prospective Urban Rural Epidemiology) Study Investigators. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. JAMA 2013;310:959–968. [DOI] [PubMed] [Google Scholar]
- 10. Beaney T, Schutte AE, Stergiou GS, Borghi C, Burger D, Charchar F, Cro S, Diaz A, Damasceno A, Espeche W, Jose AP, Khan N, Kokubo Y, Maheshwari A, Marin MJ, More A, Neupane D, Nilsson P, Patil M, Prabhakaran D, Ramirez A, Rodriguez P, Schlaich M, Steckelings UM, Tomaszewski M, Unger T, Wainford R, Wang J, Williams B, Poulter NR; on behalf of MMM Investigators. May Measurement Month 2019: the global blood pressure screening campaign of the International Society of Hypertension. Hypertension 2020;76:333–341. [DOI] [PubMed] [Google Scholar]