

Abstract
Introduction:
Step counts represent a straight-forward method of measuring physical activity in adults with Parkinson’s disease(PD). The present study examined the absolute and relative accuracy and precision of a wrist-worn research-grade accelerometer(i.e.,ActiGraph GT3X+) for measuring step counts during over-ground and treadmill walking in adults with PD and controls without PD.
Methods:
Participants (PD: n=29; controls: n=31) wore two ActiGraph GT3X+ accelerometers, one on each wrist, and completed an over-ground walking bout followed by a treadmill walking bout at the same speed. Step counts were measured manually using a hand-held tally counter. Accuracy and precision were based on absolute and relative metrics.
Results:
The ActiGraph GT3X+ underestimated step counts in both participants with PD (4.7–11% error) and controls without PD (8.8–17% error), with a greater discrepancy in controls. The ActiGraph GT3X+ provided more accurate and precise estimates of step counts when placed on the more affected wrist and non-dominant wrist for participants with PD and controls, respectively, and was more accurate and precise during over-ground walking compared with treadmill walking for both groups.
Conclusions:
Our results suggest that placement of the device (i.e., dominant vs. non-dominant), type of activity (i.e., over-ground vs. treadmill walking), and presence of clinical conditions may impact the accuracy and precision of data when using the research-grade ActiGraph GT3X+ accelerometer for measuring step counts.
Keywords: Parkinson’s disease, accelerometry, step counts, accuracy, precision
Introduction
Parkinson’s disease (PD) is a movement disorder with motor symptoms that can be managed through physical activity engagement[1]. Researchers and clinicians have measured physical activity engagement using steps counts captured by motion sensors in PD[2,3]. There are various locations for wearing motion sensors and measuring step counts, yet one study reported that most individuals prefer a wrist-worn device[4]. Wrist-worn devices may not be accurate for measuring steps nor ideal for PD based on tremor and/or dyskinesia[5]. There is limited evidence regarding the accuracy and precision of wrist-worn accelerometry in adults with PD.
We examined the accuracy and precision of a wrist-worn research-grade accelerometer for measuring step counts during over-ground and treadmill walking in adults with PD and controls without PD. We expected that wrist-worn monitors would demonstrate accuracy and precision during over-ground walking, but not with treadmill walking[6]. We further examined the accuracy and precision of these monitors based on wrist placement, whereby we expected the placement of the device on the less affected wrist would result in better accuracy and precision estimates than the more affected wrist in PD[5].
Methods
Participants
Participants were recruited locally. Interested persons contacted research staff and were provided with a description of the study followed by a brief screening for inclusion criteria: (1)age 50–74; (2)neurologist confirmed diagnosis of idiopathic PD(i.e.,presence of bradykinesia plus rigidity and/or resting tremor); (3)mild-to-moderate disability with bilateral symptoms(i.e.,Hoehn and Yahr stage 2 or 3); and (4)ambulatory without assistance. Participants were excluded if motor symptoms were due to neuroleptic medication or a stroke or were non-responsive to dopaminergic medications. Participants without PD(i.e.,controls) were characterized by the absence of major cardiovascular, neuromuscular, and pulmonary disease, and were matched to participants with PD based on age(±5years) and sex. Controls were screened for the following inclusion criteria: (1)age 50–74 years and (2) ambulatory without assistance. We enrolled 66 participants, and 60 completed all relevant study procedures(PD=29; controls=31) for this analysis.
Device-Measured Step Counts
Participants wore two, position specific ActiGraph GT3X+ accelerometers; one per wrist. The accelerometers were initialized at a sampling frequency of 100Hz and ActiLife software downloaded raw accelerometer data and reintegrated data into step counts per 60-second epoch based on the ActiLife algorithm and using the low frequency extension filter for improving sensitivity to slow movements. Step count data were imported into Microsoft Excel for processing(i.e., trained research staff calculated total step counts by summing the total steps over 1-minute epochs per walking bout) and step counts were expressed as total steps taken per 6-minute walking bout.
Over-Ground Walking Protocol
Participants walked at a comfortable speed during a 6-minute bout of over-ground walking around an indoor, oval track(Supplementary Figure1). Participants were provided standardized instructions regarding comfortable walking speed that would mimic normal daily activities. One researcher provided an audible “3,2,1,Go” and “3,2,1,Stop” countdown for initiating and completing the 6-minutes, respectively, and provided time-based updates every minute(e.g.,“one minute completed, five minutes to go”).Another researcher followed the participant with a distance-measuring wheel for recording total distance traveled(feet) during the 6-minute walking bout for measuring distance and estimating walking speed for the treadmill protocol. A third researcher provided the standardized instructions and manually recorded participant step counts using a hand-held tally counter as the gold standard of direct observation.
Treadmill Protocol
Participants completed a second 6-minute walking bout on a motor-driven treadmill(Trackmaster TMX 428, Fullvision) at the same walking speed as during the over-ground walking bout. The timekeeper provided an audible “3,2,1,Go” and “3,2,1,Stop” countdown for initiating and completing the 6-minutes, respectively, whereby one researcher started the treadmill by gradually increasing the speed until the calculated walking speed was achieved within the first, five seconds.Another member of the research team manually recorded participant step counts using a hand-held tally. Participants held the handrails for the first, 10 seconds and last, 10 seconds for safety, but were then instructed to avoid using the handrails unless there was a concern for safety. Steps counted manually and by the monitors were taken for the entire duration of the 6 minutes, regardless of if the participant used the handrails periodically.
Procedures
The University’s Institutional Review Board approved all study procedures and participants provided informed consent. Participants completed a single session in the lab, whereby each participant completed a demographic and clinical characteristics questionnaire followed by the Physical Activity Readiness Questionnaire for identifying contraindications for physical activity. Participants underwent a brief examination for scoring the Movement Disorder Society version of the Motor Examination of the Unified Parkinson’s Disease Rating Scale(MDS-UPDRS-III) as a measure of disability and walking status[7]. Participants were fitted with the ActiGraph GT3X+ monitors, and completed the over-ground walking bout followed by a rest period and the treadmill walking bout. Participants were remunerated $25.
Data Analysis
Analyses were conducted using SPSS Version 26(IBM) and accuracy and precision were based on absolute and relative metrics[8]. Absolute accuracy is presented as the mean difference between manually recorded step counts and device-measured step counts. Relative accuracy is expressed as percentage error(i.e.,mean difference divided by manual step counts × 100) and the frequency of large errors per device(i.e.,number of cases with ≥5%,≥10%, and ≥25% error)[8]. Absolute precision is presented as the standard deviation(SD) of the mean difference and relative precision is presented as the coefficient of variation(CV).We further provide Bland-Altman plots for illustrating accuracy and precision with the solid line representing the mean difference between manually counted steps and device-measured steps(absolute accuracy) and the dotted line representing the 95%confidence interval(relative precision).
Results
Participant Characteristics
Demographic and clinical characteristics of participants with PD(n=29) and controls(n=31) are presented in Supplementary Table 1. There were no significant differences between groups for age, sex, height, weight or body mass index.The sample of participants with PD had a mean(SD) disease duration of 5.9(4.3) years and a MDS-UPDRS-III Motor Examination score of 22.9(15.4).
Accuracy of GT3X+
Metrics for absolute and relative accuracy are presented in Table 1 and are illustrated in Figure 1. During overground walking, step counts captured by the GT3X+ monitors deviated from the observed counts by 62 steps(9.3%error) and 32 steps(4.7%error) on the less affected wrist and more affected wrist of participants with PD, respectively and by 57 steps(8.8%error) and 61 steps(9.5%error) on the dominant wrist and non-dominant wrist of controls, respectively. The frequency of large errors(i.e.,>25%) was 5(17%) for the less affected wrist and 1(3%) on the more affected wrist in PD and 3(10%) for the dominant wrist and 6(19%) for the non-dominant wrist in controls.
Table 1:
Accuracy and Precision of the ActiGraph GT3X+ device worn on the wrist while walking at comfortable speed over-ground and on a treadmill in Parkinson’s disease and controls.
| Absolute Accuracy | Absolute Precision | Relative Accuracy | Relative Accuracy | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) Total Step Counts | Mean Difference in Step Counts | SD of the Mean Difference in Step Counts | Mean (SD) Percentage Error | n≥5% error | n≥10% error | n≥25% error | Coefficient of Variation | ||
| PD (n=29) | Over-Ground Walking | ||||||||
| Manually Counted | 630 (53) | ||||||||
| Less Affected Wrist ActiGraph | 569 (103) | 62 | 114 | 9.3 (16.6) | 7 | 6 | 5 | 0.08 | |
| More Affected Wrist ActiGraph | 598 (58) | 32 | 68 | 4.7 (9.1) | 6 | 5 | 1 | 0.04 | |
| Treadmill Walking | |||||||||
| Manually Counted | 663 (63) | ||||||||
| Less Affected Wrist ActiGraph | 587 (79) | 76 | 86 | 11.0 (12.0) | 15 | 10 | 3 | 0.09 | |
| More Affected Wrist ActiGraph | 597 (63) | 66 | 66 | 9.6 (9.1) | 18 | 8 | 3 | 0.07 | |
| Controls (n=31) | Over-Ground Walking | ||||||||
| Manually Counted | 621 (49) | ||||||||
| Dominant Wrist ActiGraph | 564 (76) | 57 | 83 | 8.8 (12.5) | 14 | 9 | 3 | 0.07 | |
| Non-Dominant Wrist ActiGraph | 560 (81) | 61 | 87 | 9.5 (13.4) | 11 | 10 | 6 | 0.08 | |
| Treadmill Walking | |||||||||
| Manually Counted | 647 (58) | ||||||||
| Dominant Wrist ActiGraph | 546 (101) | 1010 | 102 | 15.2 (15.4) | 20 | 16 | 8 | 0.13 | |
| Non-Dominant Wrist ActiGraph | 533 (97) | 114 | 113 | 17.0 (16.5) | 21 | 16 | 9 | 0.15 | |
Figure 1:
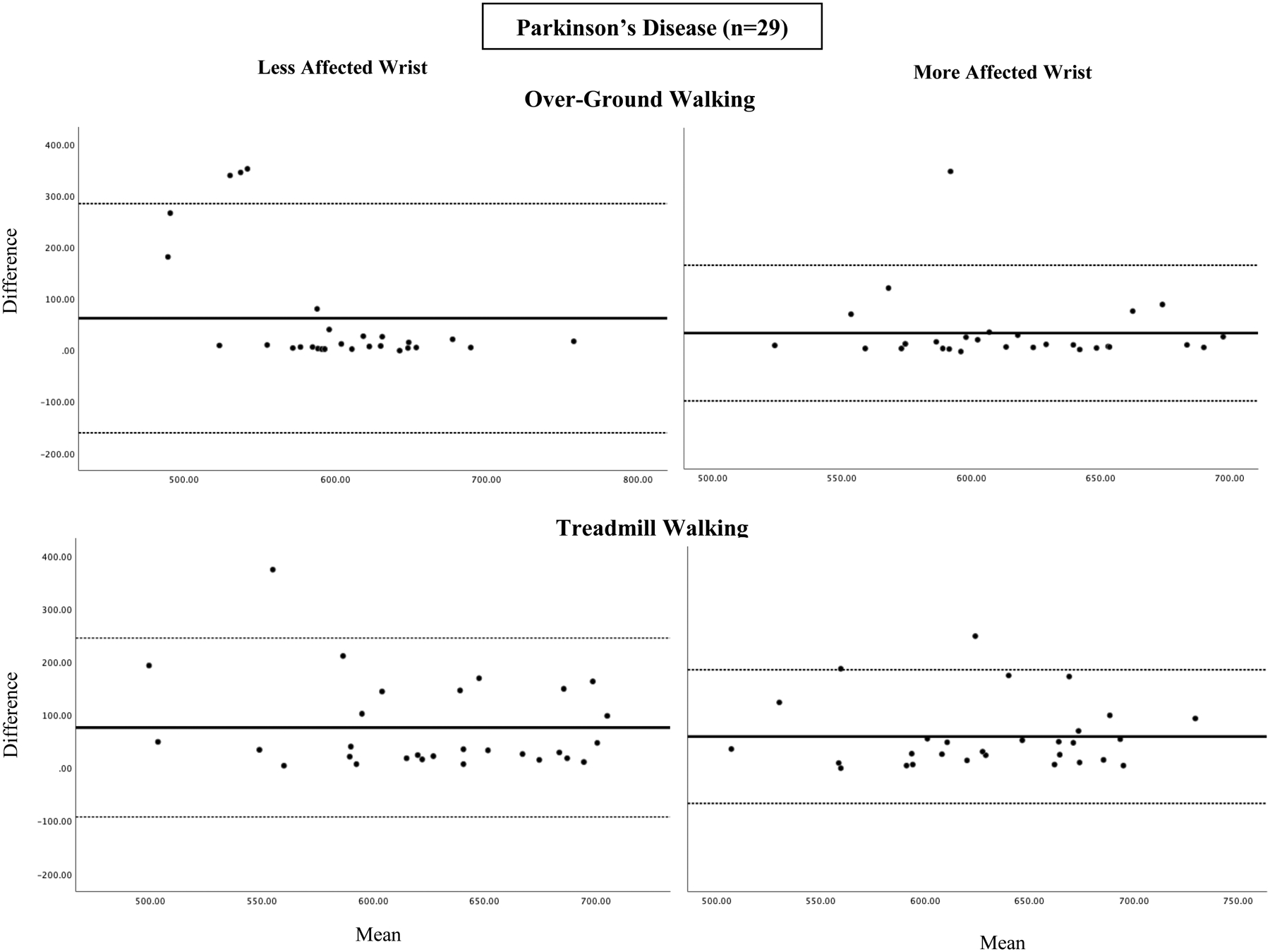
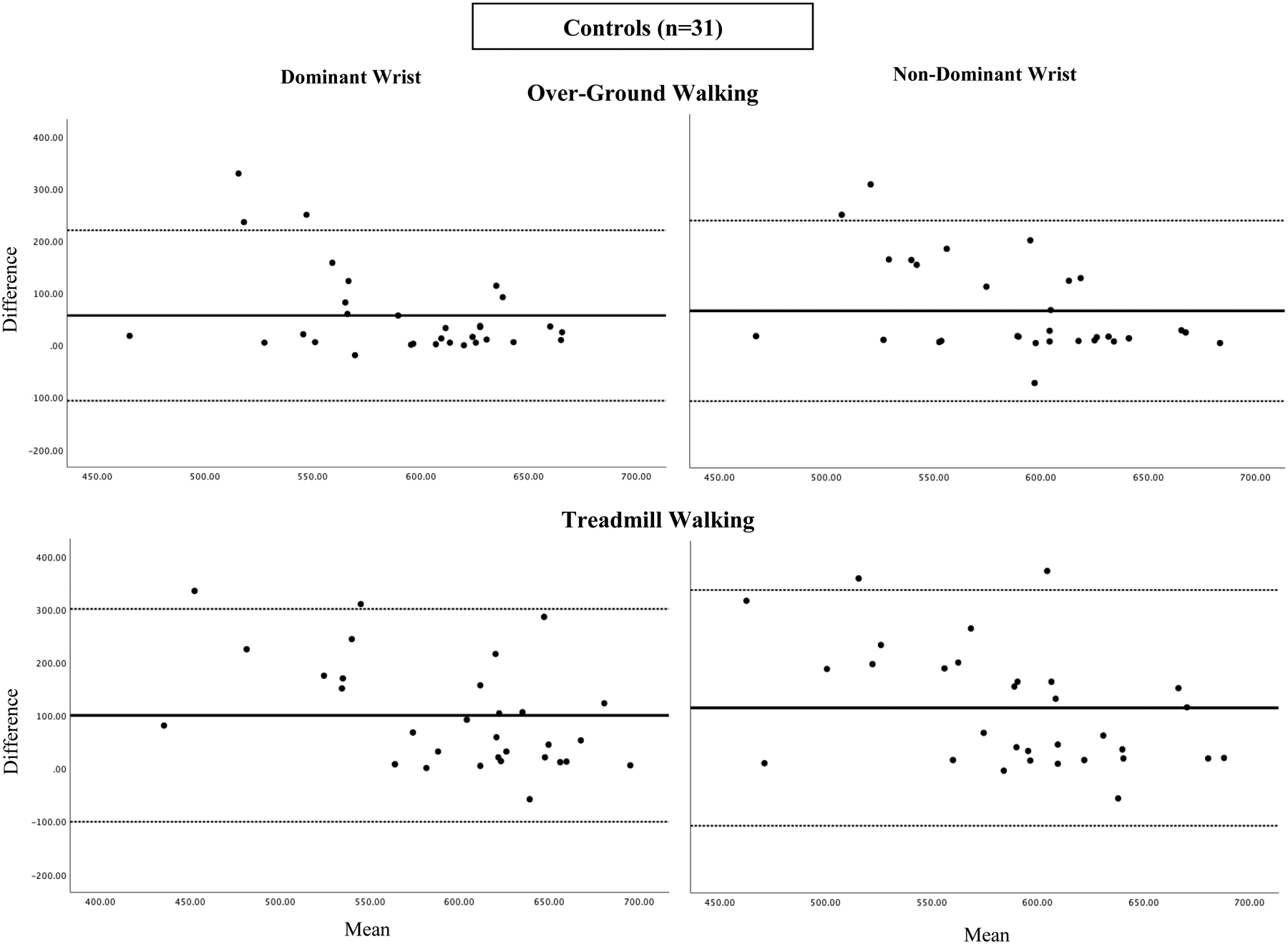
Bland-Altman Plots for over-ground and treadmill walking in participants with Parkinson’s disease (n=29) and controls (n=31).
During treadmill walking, step counts captured by the GT3X+ deviated from observed counts by 76 steps(11.0%error) and 66 steps(9.6%error) on the less affected wrist and more effected wrist in PD, respectively, and by 100 steps(15.2%error) and 114 steps(17.0%error) on the dominant wrist and non-dominant wrist in controls, respectively. The frequency of large errors (i.e.,>25%) was 3(10%) for the less affected wrist and 3(10%) on the more affected wrist in PD and 8(26%) for the dominant wrist and 9(29%) for the non-dominant wrist in controls.
Precision of GT3X+
Metrics for absolute and relative precision are presented in Table 1 and are illustrated in Figure 1. During overground walking, the SD of the mean difference between actual and observed step counts was 114(CV=0.08) and 68(CV=0.04) for the less affected wrist and more affected wrist in PD, respectively, and 83(CV=0.07) and 87(CV=0.08) for the dominant wrist and non-dominant wrist in controls, respectively. Regarding treadmill walking, the SD of the mean difference between actual and observed step counts was 86(CV=0.09) and 66(CV=0.07) for the less affected wrist and more affective wrist in PD, respectively, and 102(CV=0.13) and 113(CV=0.15) for the dominant wrist and non-dominant wrist in controls, respectively.
Discussion
The present study examined the accuracy and precision of the ActiGraph GT3X+ for measuring steps during over-ground and treadmill walking in adults with PD and controls without PD. The GT3X+ underestimated step counts in both groups, with a greater discrepancy in controls, and provided more accurate and precise estimates of step counts (1)when placed on the more affected wrist and non-dominant wrist for participants with PD and controls, respectively; and (2)during over-ground walking compared with treadmill walking. These results suggest that placement of the device, type of ambulatory activity, and the presence of clinical conditions may impact the accuracy and precision of data when using the research-grade ActiGraph GT3X+ accelerometer for measuring steps.
The present study indicated that the GT3X+ underestimated steps regardless of wrist placement, walking condition, and group.This is inconsistent with other studies suggesting wrist accelerometers overestimate step counts in PD[5,9], but consistent with a study in healthy adults suggesting the underestimation of step counts from a wrist worn GT3X+[10]. One possible explanation is the lower disability status of participants with PD in the current study, whereby a majority of participants with PD did not present with upper extremity motor symptoms. Another explanation could be that the ActiLife software step-counting algorithm was specifically developed for hip-worn devices, whereby one study in healthy adults reported that acceleration from wrist-worn devices is smaller in magnitude than those at the hip, and this results in fewer occurrences where the acceleration magnitude will satisfy the step threshold criteria, resulting in the underestimation of step counts[10].
Our results further suggest that wrist placement should be considered when estimating step counts for participants with PD, whereby the more affected wrist and non-dominant wrist were more accurate for persons with PD and controls, respectively. Studies in the general population demonstrated no effect of wrist placement for commercial devices walking on a treadmill at different speeds[11,12], but one study reported less error in estimations from the non-dominant wrist for other common daily activities(e.g.,stair climbing)[11]. One possible explanation is that the affected side in persons with PD is commonly considered the non-dominant side as it often has less movement than the less affected/dominant side, and less movement would be advantageous for a detector worn on the wrist.
The GT3X+ was more accurate and precise during over-ground walking compared with treadmill walking for both groups. One explanation could be due to gait differences in walking over-ground compared with walking on a treadmill[13] or to the periodic use of handrails on the treadmill that would reduce step detection. Although, participants in this study were instructed to avoid using the treadmill handrails, 11 participants(5 PD and 6 controls) periodically used the handrails for safety. These results align with our previous study examining the accuracy and precision of commercial-grade monitors, which demonstrated accurate and precise step count estimates during over-ground walking, but not during treadmill walking[6]. This supports the application of the GT3X+ for monitoring ambulatory physical activity during free-living conditions in PD, and this is relevant for behavioral interventions targeting free-living behavior and clinical applications involving the effect of PD manifestations on ambulation.
There are important limitations to consider when interpreting our results. We included participants who did not use assistive devices for mobility, limiting the generalizability of our results among adults with higher disability. Periodic use of the safety handrails on the treadmill while walking may have contributed to the underestimation of step counts during treadmill walking. Walking impairment(e.g., axial rigidity) and tremor are common in PD and may contribute to reduced accuracy; however, participants with the largest error values and outliers identified by the Bland-Altman plots mostly had normal or slight tremor as well as similar disability levels and walking speed, but outliers were shorter in height, had a longer disease duration(Supplementary Table2). Walking conditions were performed under controlled circumstances and may not be reflective of real-world ambulation. Steps taken over the course of the day often come from shorter walking bouts(e.g., around the house) with longer perambulations as measured in this study. However, shorter walking bouts have different characteristics than longer walking and often include turning and stopping and starting; all difficult to measure with an accelerometer and more troublesome for people with PD. Future research should examine the utility of a system for measuring walking and should include assessment of this type of walking. We examined single bouts of walking with controlled speeds rather than across varying speeds that may provide additional insight into the accuracy and precision as a function of walking speeds or conditions mimicking real-world situations.
Overall, this study provided an initial evaluation of the accuracy and precision of the ActiGraph GT3X+ worn on each wrist in participants with PD and controls without PD. Our primary findings suggest that the GT3X+ worn on the wrist underestimates step counts and that estimates during over-ground walking were more precise and accurate than during treadmill walking. Our results further suggest that the GT3X+ was more accurate and precise in estimating step counts for participants with PD than controls, and the monitor worn on the more affected wrist provided more accurate and precise estimates for participants with PD. Future research should evaluate various research-grade monitors and determine optimal placement and conditions for the most accurate and precise estimation of step counts in adults with PD, as data generated from wearable devices offer exciting opportunities for more robust, reliable, and low-cost research and patient care methodologies.
Supplementary Material
Highlights.
ActiGraph GT3X+ underestimated step counts in participants with PD and controls
ActiGraph GT3X+ was more accurate and precise on the more affected wrist in PD
ActiGraph GT3X+ was more accurate and precise on the non-dominant wrist in controls
ActiGraph GT3X+ was more accurate and precise during over-ground walking
Funding:
This work was supported, in part, by the National Rehabilitation Research Resource to Enhance Clinical Trials [REACT; P2CHD086851] and by the Eunice Kennedy Shriver National Institute Of Child Health & Human Development [F31HD097903; F31HD101281], and the National Heart, Lung, and Blood Institute [T32HL105349] of the National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declaration of Interest: None.
References
- [1].Lauzé M, Daneault JF, Duval C, The Effects of Physical Activity in Parkinson’s Disease:A Review, J. Parkinsons Dis 6(4) (2016) 685–698. doi: 10.3233/jpd-160790 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Tokuçoğlu F, Monitoring Physical Activity with Wearable Technologies, Noro Psikiyatr Ars 55(Suppl 1) (2018) S63–s65. doi: 10.29399/npa.23333 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Cohen S, Bataille LR, Martig AK, Enabling breakthroughs in Parkinson’s disease with wearable technologies and big data analytics, Mhealth 2 (2016) 20.doi: 10.21037/mhealth.2016.04.02 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Alley S, Schoeppe S, Guertler D, Jennings C, Duncan MJ, Vandelanotte C, Interest and preferences for using advanced physical activity tracking devices: results of a national cross-sectional survey, BMJ open 6(7) (2016) e011243. doi: 10.1136/bmjopen-2016-011243 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Kim DW, Hassett LM, Nguy V, Allen NE, A Comparison of Activity Monitor Data from Devices Worn on the Wrist and the Waist in People with Parkinson’s Disease, Movement disorders clinical practice 6(8) (2019) 693–699. doi: 10.1002/mdc3.12850 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Lai B, Sasaki JE, Jeng B, Cederberg KL, Bamman MM, Motl RW, Accuracy and Precision of Three Consumer-Grade Motion Sensors During Overground and Treadmill Walking in People With Parkinson Disease: Cross-Sectional Comparative Study, JMIR rehabilitation and assistive technologies 7(1) (2020) e14059. doi: 10.2196/14059 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Goetz CG, Tilley BC, Shaftman SR, Stebbins GT, Fahn S, Martinez-Martin P, Poewe W, Sampaio C, Stern MB, Dodel R, Dubois B, Holloway R, Jankovic J, Kulisevsky J, Lang AE, Lees A, Leurgans S, LeWitt PA, Nyenhuis D, Olanow CW, Rascol O, Schrag A, Teresi JA, van Hilten JJ, LaPelle N, Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): scale presentation and clinimetric testing results, Mov. Disord 23(15) (2008) 2129–70. doi: 10.1002/mds.22340 [DOI] [PubMed] [Google Scholar]
- [8].Balto JM, Kinnett-Hopkins DL, Motl RW, Accuracy and precision of smartphone applications and commercially available motion sensors in multiple sclerosis, Mult Scler J Exp Transl Clin 2 (2016) 2055217316634754. doi: 10.1177/2055217316634754 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Wallén MB, Nero H, Franzén E, Hagströmer M, Comparison of two accelerometer filter settings in individuals with Parkinson’s disease, Physiol. Meas 35(11) (2014) 2287–96. doi: 10.1088/0967-3334/35/11/2287 [DOI] [PubMed] [Google Scholar]
- [10].John D, Morton A, Arguello D, Lyden K, Bassett D, “What Is a Step?” Differences in How a Step Is Detected among Three Popular Activity Monitors That Have Impacted Physical Activity Research, Sensors (Basel) 18(4) (2018). doi: 10.3390/s18041206 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Chen MD, Kuo CC, Pellegrini CA, Hsu MJ, Accuracy of Wristband Activity Monitors during Ambulation and Activities, Med. Sci. Sports Exerc 48(10) (2016) 1942–9. doi: 10.1249/mss.0000000000000984 [DOI] [PubMed] [Google Scholar]
- [12].Chow JJ, Thom JM, Wewege MA, Ward RE, Parmenter BJ, Accuracy of step count measured by physical activity monitors: The effect of gait speed and anatomical placement site, Gait Posture 57 (2017) 199–203. doi: 10.1016/j.gaitpost.2017.06.012 [DOI] [PubMed] [Google Scholar]
- [13].Lee SJ, Hidler J, Biomechanics of overground vs. treadmill walking in healthy individuals, J Appl Physiol (1985) 104(3) (2008) 747–55. doi: 10.1152/japplphysiol.01380.2006 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.