

Abstract
Introduction:
Harms caused by prescription opioid analgesics (POAs) have been identified as a major international public health concern. Recent statistics show rising numbers of opioid-related deaths across Canada. However, Canadian family physicians appear to have inadequate resources to safely and effectively prescribe opioid analgesics to treat chronic non-cancer pain (CNCP).
Methods:
We completed a qualitative study of the barriers and facilitators to safe and effective prescribing of opioid analgesics for CNCP through semi-structured interviews with eight family physicians in Nova Scotia. Thematic analysis was used to identify the barriers and facilitators.
Results:
Family physicians identified challenges in prescribing opioid analgesics for CNCP: the complexity of CNCP management, addictions risks and prescribing tools, physician training, the physician–patient relationship, prescription monitoring and control, and systemic factors.
Conclusion:
Family physicians described themselves as inadequately supported in their prescribing of opioid analgesics for CNCP and could benefit from an integrated and coordinated approach to prescriber support.
Keywords: opioid, family physicians, chronic pain, addiction
Highlights
There is a complex intersection of challenges in prescribing opioid analgesics for chronic non-cancer pain (CNCP): the complexity of chronic pain management, addictions risks, physician training, the physician–patient relationship, prescription monitoring and control, and systemic factors.
Family physicians and patients need timely access to experts in pain management.
A comprehensive integrated system of support for CNCP management that provides peer-to-peer communications tools and access to a team of pain specialists is needed to support family physicians and patients.
Introduction
There were 16364 opioid-related deaths in Canada between January 2016 and March 2020.1 Nova Scotia had an estimated 57 confirmed and probable acute opioid toxicity deaths in 2019 and recorded 45 opioid overdose deaths in 2020.2
In 2018, nearly 1 in 8 Canadians were prescribed opioids.3 In 2010, about 86% of Canadian family physicians used prescription opioid analgesics (POAs) to treat chronic non-cancer pain (CNCP) in at least some patients.4 A more recent survey, conducted from May 2018 to October 2019, found that 89% of family physicians prescribed opioid analgesics to treat CNCP.5
A 2015 systematic review of 14 studies on physician adherence to prescribing guidelines for CNCP in Australia, Canada, France and the USA found that a significant proportion of physicians were not following guidelines largely because of a lack of awareness of their existence; because the guidelines were difficult to implement into practice; and because physicians were inadequately educated in pain management with POAs.6 The most current widely-adopted Canadian guideline for prescribing opioid analgesics for CNCP was released in 2017 by the McMaster University National Pain Centre.7 A 2020 survey-based study of this guideline’s impact on Canadian physicians suggested that there was a high degree of awareness of the guideline among respondents and some evidence that physicians’ practice had changed to better align with evidence for CNCP management.8
Data from Ontario from 2014–2015 indicate that the majority of opioid analgesic prescriptions were made by family physicians (38.4%), followed by dentists (16.7%).9 Family physicians’ role in prescribing a large proportion of opioids makes the details of their CNCP management practices useful for determining how to tailor policies and supports to make opioid prescribing for CNCP as safe and effective as possible in the context of continued POA-related harms. Qualitative studies internationally10-13 and in Ontario14,15 have identified key barriers and facilitators to safe and effective prescribing of opioid analgesics for CNCP by primary care physicians. These studies documented a great deal of complexity in the unique relationships between CNCP patients and their providers. They found that primary care physicians were challenged by the management of the time-consuming complexities of CNCP in the often tightly-scheduled milieu of outpatient primary care practices.12-14 A qualitative study found that through participation in video-conferenced workshops that involved structured discussion with peers and with interprofessional experts, rurally practising family physicians in Ontario gained greater confidence in prescribing opioid analgesics and developed better relationships with their CNCP patients.16
Knowledge of Canadian family physicians’ experiences in prescribing opioid analgesics for CNCP is growing due to recent research in this ever-evolving area. But no in-depth qualitative studies on prescribing for CNCP have been completed in Atlantic Canada.
A more detailed understanding of barriers and facilitators to family physicians’ safe prescribing of opioid analgesics could inform public health strategies that support effective prescribing while minimizing potential harms. Such qualitative research could also help map areas for further in-depth study.
Methods
Approval for the study was obtained from the Dalhousie University Research Ethics Board.
We conducted semi-structured interviews with practising family physicians recruited using a snowball sampling technique (i.e. a participant was purposively selected, the initial participant suggested other contacts as potential participants, and these suggested others, and so on). The interviewer (JG) used a pre-scripted guide (available on request from the authors). The interviews were audio recorded and transcribed.
Discussion topics included
what participants considered to be the core issues and challenges with respect to prescribing opioid analgesics; and
what kinds of supports are, or would be, helpful to enable safe and effective prescribing of opioid analgesics.
Transcripts were analyzed (by JG) in the order that they were recorded using a thematic analysis approach, with Atlas.ti software version 1.5.4.17 The author began coding the interview transcripts with a framework that identified codes (with multiple corresponding quotations) as either a barrier or a facilitator to safe and effective prescribing of opioids for CNCP. A code manual was maintained to explicitly define each code, and notes were made each time a code was changed. The codes were reviewed by SK to confirm their validity. A reflexive journal was kept during analysis to maintain transparency about coder influences on the research findings. Key quotations were annotated with memos to track emergence of possible themes. Codes were sorted in Atlas.ti under theme descriptions that emerged from the codes, and the themes were consciously searched for contradictions.
We continued to conduct interviews until the data reached saturation at eight participants; at this point, no further participants were recruited for interviews. Saturation was defined by consensus between the two authors through discussion of the codes and themes when no significant new themes had emerged from the three most recently transcribed and analyzed interview transcripts.
The interviews took place from August 2016 to June 2017.
Results
Interview participants had a range of practice focuses (see Table 1 for an overview). However, interview questions concentrated on participants’ experiences in outpatient family medicine clinic settings.
Table 1. Interview parameters and participant demographics (N=8).
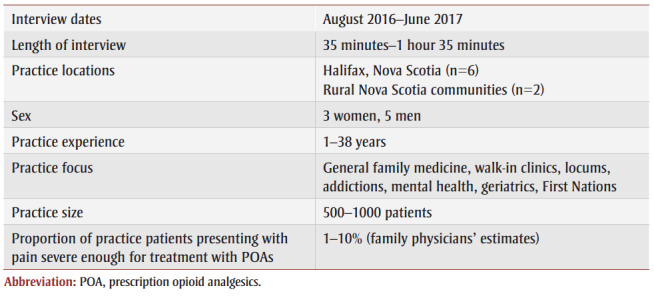 |
A total of 67 codes were developed and used during analysis to organize the data into unified themes. A set of six key themes emerged from the interview transcript text: (1) the complexity of CNCP management; (2) addictions risks and prescribing tools; (3) physician training; (4)the physician–patient relationship; (5)prescription monitoring and control; and (6) systemic factors.
(1) Complexity of CNCP management
The barriers posed by the inherent complexity of CNCP management were evident in our interviews. The family physicians often commented on their difficulty in managing patients with complaints of non-specific pain or poorly understood disorders such as fibromyalgia.
The problem is [opioids are] just not the best answer for that problem. We don’t have a good answer for chronic pain. It’s probably going to be more psychological counselling. People have very similar impairments and injuries and very different responses to them as far as pain goes. – Physician 7
One participant noted that the subjectivity of patients’ level of pain is a unique aspect of treating pain that makes it more difficult to treat than problems with visible or quantifiable findings.
And people’s experiences are really subjective too…for a lot of people, we don’t necessarily have a good solid physiologic cause of their pain. – Physician 5
The participants commented on the high comorbidity between CNCP and mental health problems. They also mentioned that, in a typical family practice, time is often a constraint to thorough CNCP management.
In the community, [a family physician] might have a 5- or a 7- or 10- or 15-minute [appointment], and they totally have inadequate time to cover it. So, it can come up where you run out of time. – Physician 6
(2) Addictions risks and prescribing tools
The participants frequently commented that a history of addiction can limit treatment options for pain because of concern that prescribing opioid analgesics could lead to unsafe use by the patient. Several also recounted experiences with “inheriting” patients who had already been prescribed opioid analgesics for CNCP at doses the physicians considered inappropriately high, some of whom had possible substance use disorders related to their POA use, and their subsequent difficulty in managing those patients.
...the inheritance thing is tough. People have been on [POAs] for a long time. ‘I’ve been getting this for 20 years, my other doctor’ this and that. And it’s tough to change mindset or for them to consider coming down on it.” – Physician 6
Most participants also noted that they choose to prescribe long-acting POAs to CNCP patients. One participant referenced long-acting POAs’ decreased risk of addiction, and another participant mentioned that such medications have lower street value and are therefore less of a risk for diversion.
The majority of participants indicated that, while tools designed to screen for risk of developing addiction to POAs before initiating treatment may be helpful for some physicians, they do not use them in their practice because of time constraints and their ability to obtain a risk assessment through history taking. One participant did find a standardized opioid risk assessment tool to be helpful in their practice when used in conjunction with a functional impact scale and pain catastrophizing scale to assess a patient’s potential to benefit from opioid pain control.
All participants with a current family medicine practice used POA treatment agreements. Most of the participants commented that the agreements are useful as a way to decline a request for higher doses or larger volumes of dispensed pills than would be appropriate.
And then I always use the treatment agreements which come in handy. Because when people break the treatment agreement, I can pull it out and [say]: ‘Remember when I said if you take too much, more than I prescribed, and I said if it ran out early then I wouldn’t give you more?’ And they were like: ‘Oh yeah.’ – Physician 3
One participant noted that screening tools do not work equally well for all patient groups when describing their work with First Nations patients.
We have a lot of diabetics so we have a lot of neuropathic pain. We have a lot of people who have old injuries because physical trauma is a big problem…injuries at a rate that I think probably exceeds the average Nova Scotia population…It’s really hard to administer a questionnaire… Not necessarily just from the language…which I’m sure is one barrier for a lot of communities. But it’s also just a really oral tradition based on story telling. A lot of storytelling. And people generally don’t respond very well to a series of questions. –Physician 5
All of the participants also used random urine drug screening as part of their treatment of CNCP patients with POAs. They found these helpful for monitoring patients’ use of other substances and diversion of POA (indicated by no POA in urine). Such findings would sometimes lead to discontinuation of a patient’s prescription based on their treatment agreement. Two participants commented that, while they had access to rapid urine dip testing in their own clinics, physicians practising without this resource might find sending urine samples to labs for interpretation a barrier to effectively using that tool.
(3) Physician training
The participants said that typical undergraduate medicine and family medicine training does not focus adequately on treatment of pain. As a result, some sought further training in pain management.
…there had been no instruction whatsoever. I had no didactic training in pain management. Other than what you learn on the street. –Physician 2
Several participants commented that while some family physicians are following shifts in standards of care for treatment of CNCP, they believe some others still prescribe opioid analgesics too liberally and at too high of doses, following a common 1990s mindset in the medical community that pain was undertreated.
Opioids are overused in general. And the doses are too high many times. – Physician 1
I think the big problem for physicians is this sort of dual message that we keep getting—that physicians are part of the opiate problem and that we’re undertreating pain. And we’re getting both those messages at the same time. Sometimes from the same people. From the public and the media, those are the lines I keep hearing. The opiate problem of overprescribing seems to be the one that’s winning out right now. But it would’ve been the opposite 10 years ago. That physicians were too reluctant to prescribe opiates was the main issue 10 years ago. – Physician 7
All participants were aware of the existence of opioid analgesic prescribing guidelines, with most referring to either the 2010 McMaster University or the 2016 Centers for Disease Control and Prevention (CDC) guidelines to inform their practice. Interestingly, the majority of the participants considered the guidelines most significant as a means of explaining to patients their reason for maintaining their POA dose at a particular level. This was particularly helpful if patients were requesting a dose higher than what the physician considered appropriate. Participants found that patients were more likely to accept their response if it was supported by evidence from a guideline.
One participant stated that some of the 2016 CDC guideline recommendations, such as the daily dosing limit of 90 morphine milligram equivalents (MME) and the suggestion that patients on psychiatric medications not be prescribed POAs, would mean that some patients’ pain was undertreated. Another participant said that the available prescribing guidelines, while appropriate, are often difficult to put into practice in clinical situations for patients with history of opioid addiction.
(4) Physician–patient relationship
Many of the discussions in our interviews focused on the physician–patient relationship and how trust and communication affect prescribing practices. Several participants described having patients they trusted subsequently turning out to be misusing or diverting their prescriptions. Participants noted that these were learning experiences that made them less likely to trust subsequent CNCP patients as readily.
I don’t know if trust is the right word because there’s a lot of patients that I’ve gotten burned by that I trusted. If you’re only doing urine drug screens [for people] you think are maybe misusing it, or diverting it, then you’re going to miss a lot of people. – Physician 3
One participant recounted that when they first began practice, they would have felt guilty about lowering a patient’s POA dose, but that now they do so with greater confidence. All participants described being pressured by some patients to prescribe opioid analgesics. Two participants experienced verbal aggression or threats from a patient in such a situation.
I think the patients that I’ve struggled [with] the most with are the ones that I’ve acquired on high doses of opioids. Some of them are quite intimidating. They frequently request early dispensing [or] early refills. When you discuss dose reduction, they can become agitated or angry. There’s always a reason as to why it’s not a good time to wean right now. And it’s often, sometimes, legit. It could be comorbid mental health problems that are flared up, or a distracting injury that doesn’t make it a good time to decrease it. Even when you do start to decrease it, there always seems to be something that leads to an increase…Those conversations I think are what scare a lot of physicians. They just terrify me. When I know that I’m going to be doing a urine [test] for someone that I’m quite certain is going to be diverting, I’m very nervous. – Physician 4
But he kept coming for appointments and being aggressive about it. Verbally aggressive and the problem is, he had genuine pain…I tried everything. It was very uncomfortable each visit because he is basically, in an aggressive way, saying, I’m not helping [him] with the pain. – Physician 8
All of the participants described “inheriting” patients on, in their opinion, inappropriately high doses of POAs that were prescribed by a patient’s former physician. The participants were then faced with needing to “wean” the patient down to a dose that was within the range suggested by the guideline. Participants said that this was usually poorly received by patients, and participants found it difficult to maintain their relationship with patients in the process of tapering an opioid dose.
(5) Prescription monitoring and control
All participants had experienced difficulties with diversion and misuse of medication by patients.
One patient who is on high doses of hydromorphone every day, and her urine dip is negative for hydromorphone yesterday. So, we have to figure out why that is. And that happens frequently. – Physician 7
Four participants described experiences where they thought patients were searching for a family physician who would provide them with POAs or other medications. This sometimes happened when the patients perceived the participants as new to practice or when they were working as locums.
So, there’s a lot of doctor shopping. And people trying to test you out and see if they could get Dilaudids or whatever from you. I feel like, just like a substitute teacher, you have to be extra strict when you’re starting out to kind of set the boundaries and expectations, and then you can kind of ease off with individual patients. – Physician 3
People hear that there’s a locum, and opportunists are out there, right? They’ll come in and just kind of see what they can get from you. – Physician 5
One participant suggested that the fear of receiving complaints through a regulatory body might serve as a disincentive to lower doses or discontinue prescriptions of opioid analgesics. Four participants mentioned that they find the Nova Scotia Prescription Monitoring Program (NSPMP) helpful. One participant said the NSPMP notified them that two patients might be diverting POAs.
All but one participant discussed the use of dispensing intervals to ensure safe POA use, with shorter intervals allowing the physician to regularly monitor patients face-to-face, and pre-agreed dosing intervals ensuring patients do not consume more than prescribed or divert. One participant described having a patient who takes their daily POA for CNCP under the supervision of a pharmacist to prevent them from misusing. Two participants used POA pill counts with at least some of their CNCP patients to ensure they are taking their dose as prescribed.
(6) Systemic factors
The participants explained that the Nova Scotia Pharmacare formulary rules mandate trialling some non-POA pain medications before others that may be more helpful for a particular patient. Also, the waitlists for provincially funded treatments such as physiotherapy and pain clinic services are prohibitively long, which sometimes leads them to prescribe pain medications while the patient is waiting. Similarly, the participants also stated that waitlists for mental health and addictions services are too long.
Several participants commented that stigma is a major barrier to patients receiving appropriate care.
I’ve definitely spoken to many colleagues and they’re not willing to practice the way I practice because of intimidation. And they’re not willing to prescribe methadone for opioid addiction because of fear. And that’s too bad. – Physician 4
I think you have the patients that when you want to have a discussion about safety and effectiveness [they say], ‘Oh, you think I’m an addict?’ ... But that’s not why I’m having the discussion with them per se. So, you get a lot of that. And probably they’ve been treated poorly. –Physician 6
System-level facilitators included ability to prescribe cannabinoids to treat pain, collaborative care clinics, access to pain experts, and support from peers in treating complex CNCP patients. Some family physicians said they felt that colleagues in the community who are isolated from such supports could struggle more with prescribing opioid analgesics as a result.
So at least in a group practice you can get support from [colleagues]. But in the community, there’s very little other than talking to their colleagues as well. But they’re usually not in the same practice. [My colleague] is in a three-person practice but, yeah, accessing resources for [them] is very difficult. [They are] pretty much on [their] own as far as these patients go. – Physician 7
Some of the participants knew pain expert physicians to contact for support with respect to prescribing opioid analgesics, but they considered it likely that many colleagues did not have such connections. An online pain management forum for physicians was suggested as a potentially effective means of seeking opinions on difficult patient cases. However, another participant felt that such forums are not adequately private and that the embarrassment of asking for help might deter some physicians from using such a forum, but that a phone resource could be an effective alternative.
…a helpline or something like that would be helpful…As long as it’s accessible and barrier-free, and physicians aren’t going to feel judged because I think lots of physicians are in rough spots with this right now. And they’re scared. That’s a little different. So [on a forum] there’s that one extra layer of, you’re going to have to admit that mess I’ve gotten myself into. – Physician 4
Discussion
Participants identified intersecting challenges in prescribing opioid analgesics for CNCP. These challenges related to the complexity of CNCP management, addictions risks and prescribing tools, physician training, the physician–patient relationship, prescription monitoring and control, and systemic factors. Discussing the complexities evoked strong emotions in many of the interview participants.
In their 2012 ethnographic American study, Crowley-Matoka and True18 detailed the emotional challenges for clinicians who were being asked to treat pain effectively while also shouldering the widespread public attention to efforts to avoid “overprescribing” for pain.
Our findings largely agree with previous qualitative studies of family physicians prescribing opioids for CNCP elsewhere as well as in Canada. In Canada, only two such studies have been conducted, both in Ontario and both by the same research team.14,15 Three other Canadian qualitative studies have examined opioid prescribing from the perspective of Ontario pain specialists19 or with a focus on non-physician providers in long-term care settings.20,21
The findings from non-Canadian studies that corroborated our own included barriers to safe and effective prescribing for CNCP caused by the complexity of chronic pain management, addictions risks inherent to POAs, lack of training in CNCP management, delicate physician–patient relationships and systemic factors such as waitlists.22-24 Desveaux et al.14,15 also documented these barriers in their two 2019 Ontario studies.
Key facilitators to safe and effective prescribing that we identified in this study we also saw when reviewing the non-Canadian literature. These included use of prescribing guidelines and access to prescriber tools such as treatment agreements10,13 Although Krebs et al.25 found in their 2014 qualitative study that US primary care physicians viewed opioid monitoring as largely incompatible with their roles, the participants in this study considered the NSPMP to be helpful in their practice. The participants in our study also did not observe, as Krebs et al.25 had, that monitoring of patients’ POA treatment with urine screening and treatment agreements could disrupt an effective therapeutic relationship. Participants in both 2019 Ontario qualitative studies mentioned using urine screening, but they suggested that use increased tension in the physician–patient relationship15 or that urine screening was not useful.14 Buchman and Ho26 pointed out that despite the paucity of evidence for the use of POA treatment agreements, they are widely used and could undermine the therapeutic relationship between physician and patient.
Our findings are also consistent with those of Latimer et al.,27 who suggested that clinicians can improve their understanding of Mi’kmaq patients’ pain by taking the time to listen to the patient’s full “story” of the pain, since they might not use descriptors such as adjectives or numeric scales typically used by clinicians to determine their treatment plans. This information could then be used to guide the appropriate diagnosis and treatment.
Most participants described ways that guidelines support their safe and effective prescribing of opioid analgesics. Renthal28 pointed out that the 2016 CDC guidelines,29 pushed the “pendulum” of opioid analgesic prescribing back toward a more restrictive position. The most recent Canadian guidelines were released in 2017 by the McMaster University National Pain Centre to update their previous 2010 guideline; the 10 recommendations cover first-line therapies, POA therapy in substance use disorder, psychiatric disorders, history of substance use disorder, dosing, tapering and POA rotation.7
In a 2020 survey of Canadian family physicians, Furlan et al.5 found that two of 12 guideline-concordant practices were performed regularly by the majority of respondents. This survey, a follow-up to a similar 2010 survey, found that urine drug screening by respondents had increased from 22% in 2010 to 57% in 2018.5 These findings cannot be fully generalized to Nova Scotia, however, because the 2018 survey included only one Nova Scotian respondent.5 (Urine drug screening is described under a guidance statement rather than recommendation in the 2017 McMaster guideline, due to lack of evidence for its use.7)
While uptake, since 2010, of some guideline-based practices by Canadian family physicians might be attributable to creation and dissemination of prescribing guidelines,5 the systemic problems we identified in our study are not easily solved. Our findings suggest that while some family physicians have access to peers and experts to support their prescribing for challenging patient cases, others have to place their patients on long waitlists to obtain those supports because they do not have connections to knowledgeable peers or experts. Prolonged wait times are not confined to Nova Scotia, but have been identified across Canada; wait times for methadone maintenance therapy were between 2 weeks and 12 months across the provinces as of 2011,30 but there is a paucity of more recent published data. A 2017 study of the specialist referral experiences of family physicians in Hamilton, Ontario, found that pain management clinics were among the specialities least likely to respond to requests for consultation.31
The majority of family physicians practising in Nova Scotia do so independently in community-based practices, and many are working in rural areas. These family physicians are often isolated from the support of colleagues and experts in pain and addiction medicine that they might need to support their decisions in CNCP management—support that participants in our study often described as being key facilitators to their practice. One participant noted that the Atlantic Mentoring Network for Pain and Addiction, which provides an online forum for discussion of difficult cases with colleagues, was helpful in their practice. A similarly accessible, coordinated and integrated system-wide approach where family physicians are supported with expert knowledge would enable safer and more effective prescribing of opioid analgesics. Such an approach could involve formation of a centralized network of experts in CNCP management that are accessible to all Nova Scotian family physicians when they need a referral for a CNCP patient. This approach could be complemented by simultaneously building capacity for CNCP management through continued medical education sessions with pain experts, similar to the Project ECHO model described by Carlin et al.16 in Ontario.
Future research
The challenges identified here are likely applicable to other cities in Canada of similar size. Further research is needed to gain a more representative understanding of Nova Scotian family physician practices and whether they follow evidence-based guidelines for prescribing opioid analgesics. It would be useful to gain a better understanding of family physicians’ attitudes toward these guidelines on a broader scale and whether there is a need to support their adoption into practice.
More research is also required to effectively address the challenges Nova Scotian family physicians face when prescribing opioid analgesics for CNCP. A survey distributed to all family physicians in the province could accomplish this.
Strengths and limitations
This qualitative study achieved its aim of describing the previously undocumented challenges faced by Nova Scotian family physicians in their prescribing of opioid analgesics for CNCP. Most participants acknowledged that they had an interest in patient populations with addictions or chronic pain. Thus, our participants are not entirely representative of Nova Scotian family physicians. Several of the participants described working in a collaborative care clinic, while most Nova Scotian family physicians work independently in the community.
Despite these limitations, participants did describe experiences of their own and those of colleagues working in independent community practices that would be broadly applicable to the practice of family medicine in NS and beyond.
Conclusion
Nova Scotian family physicians identified intersecting challenges in prescribing opioid analgesics for CNCP related to the complexity of chronic pain management, their relationships with patients, prescription monitoring and control, lack of training, and systemic issues that likely affect family physicians across Canada. Options for Nova Scotian family physicians to manage patients’ CNCP are limited. More timely access to experts in pain management and addictions are needed for family physicians and patients in Nova Scotia. A coordinated and integrated system-wide approach where family physicians are supported would enable safe and effective prescribing of opioid analgesics.
Conflicts of interest
The authors have no conflicts of interest to declare.
Authors’ contributions and statement
JG and SK conceptualized the work and both developed the methods for data collection and analysis. JG completed interviews for data collection. Both JG and SK completed the coding and analysis of the data. JG drafted the manuscript and SK provided revisions to the manuscript.
The content and views expressed in this article are those of the authors and do not necessarily reflect those of the Government of Canada.
References
- Government of Canada. Ottawa(ON): Opioid-related harms in Canada [Internet] Available from: https://health-infobase.canada.ca/substance-related-harms/opioids. [Google Scholar]
- Government of Nova Scotia. Halifax(NS): Opioid use and overdose strategy: Opioid toxicity deaths in Nova Scotia [Internet] Available from: https://novascotia.ca/opioid/#table. [Google Scholar]
- Opioid prescribing in Canada: how are practices changing. Canadian Institute for Health Information. 2019 [Google Scholar]
- Asbridge MM, MacDougall PC, Furlan AD, Tugalev O, et al. Self-reported practices in opioid management of chronic noncancer pain: a survey of Canadian family physicians. Pain Res Manag. 2013;18((4)):177–84. doi: 10.1155/2013/528645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Furlan AD, Diaz S, Carol A, MacDougall P, Allen M, et al. Self-reported practices in opioid management of chronic noncancer pain: an updated survey of Canadian family physicians. J Clin Med. 2020;9((10)):1–14. doi: 10.3390/jcm9103304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tournebize J, Gibaja V, Muszczak MA, Kahn JP, et al. Are physicians safely prescribing opioids for chronic noncancer pain. Pain Pract. 2016:370–83. doi: 10.1111/papr.12289. [DOI] [PubMed] [Google Scholar]
- Busse J, Michael G, et al. McMaster University Michael G. DeGroote National Pain Centre. Hamilton(ON): The 2017 Canadian guideline for opioids for chronic non-cancer pain [Internet] Available from: http://nationalpaincentre.mcmaster.ca/guidelines.html. [Google Scholar]
- Busse JW, Douglas J, Chauahan TS, Kobeissi B, Blackmer J, et al. Perceptions and impact of the 2017 Canadian guideline for opioid therapy and chronic noncancer pain: a cross-sectional study of Canadian physicians. Pain Res Manag. :8380171–83. doi: 10.1155/2020/8380171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ontario narcotics atlas [Internet] Health Analytics Branch. Available from: https://docplayer.net/60771965-Ontario-narcotics-atlas.html. [Google Scholar]
- Kennedy M, Henman MC, Cousins G, et al. General practitioners and chronic non-malignant pain management in older patients: a qualitative study. General practitioners and chronic non-malignant pain management in older patients: a qualitative study. Pharmacy (Basel) 2016;4((1)):15–83. doi: 10.3390/pharmacy4010015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harle CA, Bauer SE, Hoang HQ, Cook RL, Hurley RW, Fillingim RB, et al. Decision support for chronic pain care: how do primary care physicians decide when to prescribe opioids. BMC Fam Pract. 2015 doi: 10.1186/s12875-015-0264-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McRorie C, Closs SJ, House A, et al, et al. Understanding long-term opioid prescribing for non-cancer pain in primary care: a qualitative study. BMC Fam Pract. 2015;16((121)):121–83. doi: 10.1186/s12875-015-0335-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barry DT, Irwin KS, Jones ED, et al, et al. Opioids, chronic pain, and addiction in primary care. J Pain. 2010;11((12)):1442–50. doi: 10.1016/j.jpain.2010.04.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Desveaux L, Saragosa M, Kithulegoda N, Ivers NM, et al. Understanding the behavioural determinants of opioid prescribing among family physicians: a qualitative study. BMC Fam Pract. 2019;20((1)):59–50. doi: 10.1186/s12875-019-0947-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Desveaux L, Saragosa M, Kithulegoda N, Ivers NM, et al. Family physician perceptions of their role in managing the opioid crisis. Ann Fam Med. 2019:345–51. doi: 10.1370/afm.2413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carlin L, Zhao J, Dubin R, Taenzer P, Sidrak H, Furlan A, et al. Project ECHO telementoring intervention for managing chronic pain in primary care: insights from a qualitative study. Pain Med. 2018;16((9)):1140–6. doi: 10.1093/pm/pnx233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Markgraf F, Michels S, Winter M, et al, et al. ATLAS/ti version 1.5.4 [Software] Markgraf F, Michels S, Winter M, et al. 2017 [Google Scholar]
- Crowley-Matoka M, True G, et al. No one wants to be the candy man: ambivalent medicalization and clinician subjectivity in pain management. Cult Anthropol. 2012:689–712. [Google Scholar]
- Chang Y, Zhu KL, Florez ID, et al, et al. Attitudes toward the Canadian guideline for safe and effective use of opioids for chronic non-cancer pain: a qualitative study. J Opioid Manag. 2016;12((6)):377–87. doi: 10.5055/jom.2016.0357. [DOI] [PubMed] [Google Scholar]
- Kaasalainen S, Coker S, Dolovich E, et al, et al. Pain management decision making among long-term care physicians and nurses. West J Nurs Res. 2007;29((5)):561–80. doi: 10.1177/0193945906295522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaasalainen S, Brazil K, Coker S, et al, et al. An action-based approach to improving pain management in long-term care. Can J Aging. 2010;29((4)):503–17–80. doi: 10.1017/S0714980810000528. [DOI] [PubMed] [Google Scholar]
- Baldacchino A, Gilchrist G, Fleming R, Bannister J, et al. Guilty until proven innocent: a qualitative study of the management of chronic non-cancer pain among patients with a history of substance abuse. Addict Behav. 2010:270–2. doi: 10.1016/j.addbeh.2009.10.008. [DOI] [PubMed] [Google Scholar]
- Esquibel AY, Borkan J, et al. Doctors and patients in pain: conflict and collaboration in opioid prescription in primary care. Pain. 2014;155((12)):2575–82. doi: 10.1016/j.pain.2014.09.018. [DOI] [PubMed] [Google Scholar]
- Spitz A, Moore AA, Papaleontiou M, Granieri E, Turner BJ, Reid MC, et al. Primary care providers’ perspective on prescribing opioids to older adults with chronic non-cancer pain: a qualitative study. BMC Geriatr. 2011;11((35)):1–9. doi: 10.1186/1471-2318-11-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krebs EE, Bergman AA, Coffing JM, Campbell SR, Frankel RM, Matthias MS, et al. Barriers to guideline-concordant opioid management in primary care—a qualitative study. J Pain. 2014;5((11)):1148–55. doi: 10.1016/j.jpain.2014.08.006. [DOI] [PubMed] [Google Scholar]
- Buchman DZ, Ho A, et al. What's trust got to do with it. J Med Ethics. 2014;40((10)):673–7. doi: 10.1136/medethics-2013-101320. [DOI] [PubMed] [Google Scholar]
- Latimer M, Simandl D, Finley A, et al, et al. Understanding the impact of the pain experience on Aboriginal children’s wellbeing: viewing through a two-eyed seeing lens. First Peoples Child & Family Review [Internet] 2014;9((1)):22–37. Available from: https://fpcfr.com/index.php/FPCFR/article/view/183. [Google Scholar]
- Renthal W, et al. Seeking balance between pain relief and safety: CDC issues new opioid-prescribing guidelines. JAMA Neurol. 2016;73((5)):513–4. doi: 10.1001/jamaneurol.2016.0535. [DOI] [PubMed] [Google Scholar]
- Dowell D, Haegerich TM, Chou R, et al. CDC guideline for prescribing opioids for chronic pain—United States, 2016. Dowell D, Haegerich TM, Chou R. 2016;315((15)):1624–45. doi: 10.1001/jama.2016.1464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luce J, Strike C, et al. Canadian Executive Council on Addictions. Ottawa(ON): A cross-Canada scan of methadone maintenance treatment policy developments [Internet] Available from: https://www.ceca-cect.ca/pdf/CECA%20MMT%20Policy%20Scan%20April%202011.pdf. [Google Scholar]
- Neimanis I, Gaebel K, Dickson R, et al, et al. Referral processes and wait times in primary care. Can Fam Physician. 2017;63((8)):619–24. [PMC free article] [PubMed] [Google Scholar]