

Abstract
This paper examines the immediate and long-term effects of public smoking bans on smoking prevalence, smoking regularity, smoking intensity, and secondhand tobacco smoke exposure. We supplement the extensive literature on the effects of various types of tobacco control legislation on smoking behavior in developed countries by studying the provincial smoking bans and more recent national ban of a middle-income country, Argentina. We focus on the difference between full and partial smoking bans, and take advantage of the time and province variation in ban implementation in order to determine the causal effects of each type of ban. We find that full bans reduce national smoking prevalence over time, especially among younger demographic groups, but have no significant impact on intensity of smoking among smokers. Full bans also benefit nonsmokers, as they are associated with a significant reduction in environmental tobacco smoke exposure. Partial bans do not significantly impact smoking prevalence, and are found to increase smoking intensity among individuals who smoke every day. These findings provide support for ratification of full bans by all provinces according to the National Tobacco Control Law of 2011.
1. Introduction
Tobacco consumption represents the leading preventable cause of death and disease worldwide and one of the most significant global public health concerns, accounting for almost eight million deaths annually (World Health Organization WHO, 2019). Guided by strong international evidence of the detrimental short- and long-term health impacts of tobacco consumption and secondhand smoke, many developed nations have passed legislation in recent decades aimed at discouraging smoking initiation, reducing consumption among smokers, and reducing exposure to environmental tobacco smoke (ETS). The policy mechanisms include increased taxation, restrictions on advertising and distribution, the introduction of educational programs, and bans on smoking in public places. It is important to analyze the potential impacts of each of these various policy changes on both short- and long-term smoking behavior and health in order to determine the most effective methods of reducing consumption (DeCicca et al., 2018).
This paper focuses on the effects of sub-national and national public smoking bans on tobacco consumption behavior in Argentina. While many nations have seen declines in smoking prevalence, rates of tobacco consumption have remained particularly high in Argentina, with over 30 percent of the population smoking in 2005 (Ministerio de Salud [Ministry of Health]). The only South American nations with greater smoking prevalence are Chile and Bolivia. This prevalence is largely attributed to the low tobacco prices and recent economic growth that have made cigarettes more affordable (Rodríguez-Iglesias et al., 2015). Despite the health and financial burden associated with high smoking rates, Argentina has lagged behind its neighbors in tobacco control; as of February 2021, it remains the only nation in South America that has not ratified the 2003 WHO Framework Convention on Tobacco Control (FCTC), an international treaty that establishes guidelines and principles of tobacco control. However, between 2004 and 2010, thirteen of Argentina’s 23 provinces passed province-level legislation that restricted public smoking to varying degrees. It was not until 2011 that Argentina passed its first national tobacco control law, which extended a comprehensive public smoking ban to all 23 provinces (O’Neill Institute et al., 2011). By 2017, national smoking rates among Argentinians 15 years of age and older had fallen to nearly 16 percent (WHO, 2019).
Policy evaluation of public smoking bans is complicated because of the competing incentive mechanisms a ban places on individual decision making. While bans are aimed at protecting the health of nonsmokers by limiting exposure, their short- and long-term impacts on individual smoking behavior are not, theoretically, straightforward. In fact, recent literature in economics has explored the policy impact within different countries, and results have varied greatly. This paper extends the analysis to Argentina and is the first to analyze the impact of provincial bans and provincial ratification of its 2011 National Tobacco Control Law. Previous studies in Argentina have predicted the effects of the policy implementation, but our work is the first to use recently released survey data on cigarette consumption and health-related behaviors to quantify the observed effects. We conduct a comprehensive analysis of the impacts of the national and province-level policies by examining smoking prevalence, smoking regularity, smoking intensity, and secondhand smoke exposure. We uncover causal policy effects using variation in the implementation of smoking bans by provinces across different years. Because cigarettes can be addictive, individuals may not reduce consumption immediately after smoking is restricted in public places. By accounting for the years elapsed since implementation in a particular province, we quantify the immediate and long-term effects of the policy on habitual smoking behavior.
While many studies observe large declines in both smoking prevalence and intensity among specific demographic groups after the implementation of bans, we attribute to the bans only slight reductions in consumption on average, and even an increase among some individuals. While full and partial smoking bans have no immediate effect on smoking prevalence among the general population, a reduction in prevalence is associated with a full ban that has been in place for several years. One may attribute this finding to the slow responsiveness to incentives among individuals engaged in addictive consumption behaviors.
It is also possible that the observed smoking reduction the longer a ban has been in place is the result of community- rather than individual-level behaviors. That is, individuals in a community might be impacted by improvements in enforcement of the ban over time or by changes in attitudes toward smoking that develop over time. The pattern of reduction is especially pronounced among young and wealthy males. Additionally, the reduction in prevalence is associated with a decline in the number of individuals starting to smoke, rather than an increase in the number of individuals quitting smoking. Hence, these findings suggest that the smoking bans gradually discourage take up of smoking, which generally occurs at younger ages. An observed reduction in smoking among high-income individuals suggests that the constraints placed on smoking locations may reduce the allure or prestige of smoking. In estimation, we control for permanent differences in provinces but we cannot account for province-specific time trends that could capture such community changes or enforcement.1
Interestingly, there is evidence that the way a ban is implemented can influence smoking behaviors. While we find that a full provincial ban has no significant effect on the quantity of cigarettes smoked by individual smokers, a partial provincial ban that allows smoking in designated areas increases smoking intensity among everyday smokers. We conjecture that this increase may be partially due to reinforced peer effects as the concentration of smokers in designated smoking area increases (Fowler and Christakis, 2008; Gilleskie and Li, 2018). We do not have the data to test this hypothesis about peer effects, yet we encourage future researchers to explore these concerns based on our findings from Argentina’s experience.
The high prevalence of tobacco consumption and the lack of smokefree legislation in some jurisdictions ranked Argentina among the highest in the region for indoor public place air pollution in the early 2000s (Navas-Acien, et al., 2004). We find pronounced positive effects of public smoking bans on self-reported ETS exposure as bans were implemented in the first decade of the 21st century. Full public smoking bans are associated with a significant decline in nonsmokers’ exposure to secondhand smoke, especially among young, wealthy males. Similar to early studies of the ban effectiveness using measured concentrations of particulate matter (Schoj et al., 2010), our findings provide empirical evidence of the benefits associated with full public smoking bans and the potential harm caused by partial smoking bans, and suggest that provincial policymakers should work to implement the full smoking bans outlined in the National Tobacco Control Law.
In Section 2, we discuss the relevant literature in economics on the impact of public smoking bans, both globally and within Argentina. This section includes information on recent tobacco legislation in Argentina. Section 3 presents our empirical framework for analyzing smoking behaviors based on a theoretical model of smoking decision making (described in Appendix B). In Section 4 we introduce the repeated cross-sectional data source and summarize the dependent variables, individual-specific explanatory variables, and province-specific policy variables. The results of empirical analyses are discussed in Section 5, and Section 6 concludes.
2. Review of Relevant Smoking Literature
2.1. Economic Analyses of Tobacco Control Policies
Over the past few decades, there have been a number of theoretical and empirical analyses of the impacts of various types of tobacco control policies on smoking behavior. Several researchers have attempted to quantify the price elasticity of demand for cigarettes in order to predict the potential impact of cigarette tax increases. An early analysis by Lewit and Coate (1982) determined that the price elasticity of demand in the United States in the mid-1970s ranged from −0.40 to −1.30. This study was one of the first to provide strong evidence that the passage of excise taxes could significantly reduce smoking levels. Later studies modified Lewit and Coate’s approach and analyzed how other factors affect the price elasticity of demand of cigarettes, and therefore the potential effectiveness of taxation. Wasserman et al. (1991) examined price changes and demand shifts in the context of other tobacco control regulations and determined that previous analyses may have overestimated the price elasticity of demand. Their more robust analysis found a price elasticity of demand ranging from −0.02 in 1974 to −0.23 in 1985.
Subsequent studies incorporated the effects of addiction on demand. Becker and Murphy (1988) developed the first dynamic rational addiction model, a now widely referenced model based on the idea that past consumption is very strongly correlated with current consumption. Their model and empirical work indicate that addicts do not respond strongly to temporary and short-term price changes. Gilleskie and Strumpf (2005) found evidence that adolescents with a recent history of cigarette consumption are likely to be less sensitive to cigarette price changes in the short-run than those who have never smoked.2 They showed that price increases through taxation have a greater aggregate effect in the long run than in the short run as individuals reduce consumption and move to the nonsmoking, price-sensitive group.
While much of the literature consistently predicts that pecuniary mechanisms such as cigarette prices and taxes reduce cigarette demand with differential effects on smokers and non-smokers, the economics literature on non-pecuniary mechanisms (such as restrictions on smoking in particular locations) is less definitive and underexplored. The vacillating findings on the effects of smoking bans, for example, are based on data from a number of countries in which public smoking bans have been implemented, including the United Kingdom (UK), Germany, Ireland, Switzerland, and the United States (US). The difference-in-difference model is a popular method of empirical analysis, for it allows the researcher to mimic an experimental study by comparing the effect of a treatment (i.e., a smoking ban) in an “experimental” group to a “control” group that does not face the treatment. When there is time and location variation in the implementation of tobacco control policies, difference-in-difference models allow the comparison of individuals within the states under legislation to those in the “control” states over time. Jones et al. (2015) estimated several difference-in-difference fixed effects models using panel data on tobacco consumption in the UK, and found no significant change in smoking prevalence or cigarette consumption on an aggregate level after a public smoking ban was implemented, although significant changes were found amongst specific demographic groups. Anger et al. (2011) also used a difference-in-difference model to determine that public smoking bans did not have a significant effect on overall tobacco consumption in Germany; however, the bans significantly reduced consumption among those who frequent bars and pubs. Boes et al. (2015) conducted a similar analysis on smoking bans in Switzerland and concluded that they did significantly reduce smoking rates, but these reductions only began to emerge one year after the ban. This finding indicates the importance of accounting for time since the passage of the law.
In some of the earliest work on this subject, Chaloupka (1992), using instrumental variable procedures to account for the endogeneity of past and future consumption, finds that the passage of basic public smoking bans (i.e., clean indoor air laws) significantly reduced average cigarette consumption among males in the US, but it had no significant effect on women’s consumption. Tauras’s (2006) examination of the effects of smoke-free air laws and cigarette prices on adult cigarette consumption used cross-sectional data collected by the US Centers for Disease Control and Prevention (CDC) where smoking bans are characterized by a three-point scale representing varying strengths of enforcement. Separately modeling smoking prevalence and smoking intensity, Tauras estimates a negative ban elasticity of demand of −0.072, implying that bans could significantly reduce consumption. Although public smoking bans reduced average smoking intensity by up to 5.18 percent, he found that they had very little impact on smoking prevalence. Carton et al. (2016) find that indoor smoking bans imposed between 2002 and 2010 in the US contribute a two- to three-percent reduction in smoking prevalence. Using longitudinal data and a dynamic model of behavior, Matsumoto (2017) finds that indoor smoking bans in the US reduce smoking initiation but have little effect on the quitting behavior of smokers. Additionally, Matsumoto provides evidence that individuals may anticipate passage of such local restrictions based on other, within-state ban introductions and, consequently, alter their smoking behavior prior to local implementation.
Other recent studies have analyzed the effects of public smoking bans on nonsmokers’ exposure to secondhand smoke. Kuehnle and Wunder (2017), for example, studied public smoking bans passed in Germany between 2007 and 2008 and examined the effects of these bans on the self-reported health of both smokers and nonsmokers. They found improvements in self-reported health among nonsmokers in the presence of smoking bans, but deteriorations in the health of smokers. Goodman et al. (2007) investigated the concentrations of particulate matter in bars and restaurants in Dublin and conducted pulmonary function studies on workers in these venues before and after the passing of Ireland’s national public smoking ban. They found an 83 percent reduction in particulate matter in these locations and a 71 percent reduction in exhaled carbon monoxide by the workers after passage. Adda and Cornaglia (2010), conversely, found that public smoking bans not only have no significant effect on overall adult secondhand smoke exposure, but they may actually increase the exposure of nonsmokers to secondhand smoke by displacing smokers to private places. By analyzing cotinine levels to indicate exposure to cigarette smoke, they found that young children experienced greater exposure to ETS after the implementation of the public smoking ban. Perhaps related to secondhand smoke exposure, Kvasnicka et al. (2018) find that smoking bans in bars and restaurants in Germany reduced hospital admissions associated with cardiovascular health and asthma.
Despite strong international interest, there has been limited economic analysis of tobacco consumption and control in Argentina. Konfino et al. (2014) published a public health analysis that predicted the long-term health impact of Argentina’s national tobacco control law, but the prediction was based on data available before the law and did not make use of data collected after the law was passed. Guindon et al. (2018) examined the impact of real cigarette prices on smoking initiation using individual reports of age of smoking onset from cross-sectional national surveys in 2005, 2007, 2008, and 2011 (including two of the ENFR surveys we employ) and component consumer price indices to construct prices from 1980 to 2011. They find that the smoking onset hazard (i.e., likelihood of taking up smoking) among Argentinians is sensitive to price variation, but less so in periods of hyperinflation. Although not the focus of their work, they find some evidence that tobacco control policies (i.e., bans) may have reduced smoking initiation.
While individual smoking behaviors, in developed countries as well as in Argentina, appear to respond to cigarette pricing and taxation policies, there is evidence from the US of avoidance of such pecuniary pressures through cross-border purchasing, tax avoidance (through internet or Native American reservation purchases), and illegal markets in the US (e.g., Harding et al., 2012; DeCicca et al., 2013a, 2013b, 2015; and summarized thoroughly in DeCicca et al., 2018). Developing countries, perhaps at greater risk of such informal markets due to reduced regulation, may find traditional abatement methods (e.g., Pigouvian taxes) less effective. We suspect no cross-province purchasing in Argentina due to little price and tax variation in cigarettes across the region. Additionally, the market for cigarettes is almost completely supplied by two manufacturers, so tax avoidance is not common. Threats to price sensitivity are more likely to come from hyperinflation and rising incomes, which reduce the effects of taxes and increase affordability of cigarettes, respectively. As such, non-pecuniary efforts, such as smoke-free air laws that ban smoking in specific locations (e.g., workplaces, restaurants, bars and casinos) have been introduced to reduce individual smoking by making smoking inconvenient.3
2.2. Public Smoking Bans in Argentina
Prior to the implementation of Argentina’s National Tobacco Control Law of 2011, 13 of the nation’s 23 provinces and the capital city of Buenos Aires had implemented subnational tobacco control policies to restrict or ban smoking in public places. While three of these subnational policies imposed a full ban on smoking in all public places, the majority did not. Instead, these provinces implemented a limited set of restrictions, which we refer to throughout this paper as partial bans. In a province with a partial ban, smoking is permitted in particular settings among public places (e.g., in casinos but not in bars and restaurants) or in specific rooms or open-air areas within venues. It is important to acknowledge the varying levels of restrictions and clearly differentiate between partial bans and full bans, for they may affect smokers and nonsmokers differently. For example, if smoking is prohibited in the main room of a bar or restaurant but there is a designated room for smokers, it is much less likely that an individual will refrain from smoking than if there is no place to smoke (i.e., the loss of utility faced by an individual smoker attending a venue where there is no place to smoke is higher than it would be if there is a designated place). There is also the potential for peer effects that may influence smokers to smoke more by grouping them together and making the practice appear more socially acceptable. Section 4 (and Appendix B) offers more discussion of these concepts and the decisions that smokers face in the presence of smoking bans.
The National Tobacco Control Law was passed in 2011 with the intention of imposing a comprehensive public smoking ban nationally; however, the implementation of the law did not actually require that all remaining provinces enact and enforce these bans. Rather, the policy was strongly encouraged, and it was enforced only if ratified by the individual provinces. Nonetheless, the policy represents a strong change in national attitudes towards smoking, and these attitudes may have encouraged some bars and restaurants across the country to ban smoking independently. Yet, after its passage in 2011, only four provinces ratified it (and four additional provinces passed their own public smoking bans).4 A major reason for such a limited number of ratifying provinces is the fact that many already had strong policies in place; however, seven provinces with regulations weaker than those imposed by the national law and five provinces that were completely lacking regulations have yet to ratify the law. By 2013, between the subnational laws and the ratifications, 18 provinces and the capital city of Buenos Aires were covered by some level of smoking restrictions.5 Figure 1 depicts the gradual implementation of bans in Argentina (at the years of our individual-level survey data). The levels of public smoking restrictions and a description of exceptions to the law in various provinces are outlined in Appendix Table A1.
Figure 1:
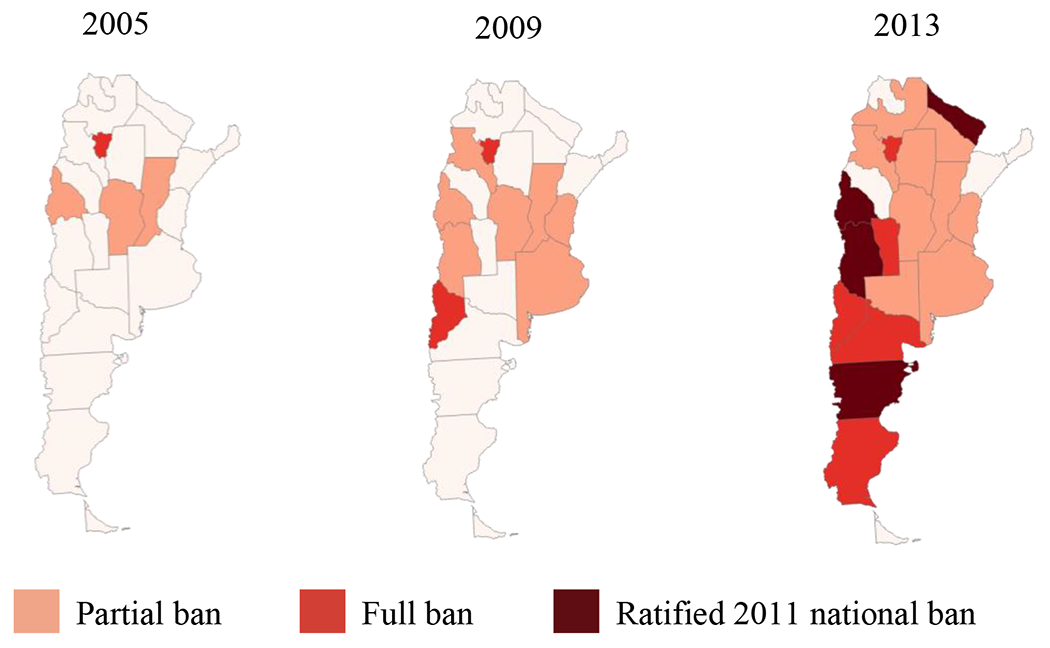
Public Smoking Bans in Argentina, by province and year
3. Empirical Framework
To motive our empirical analysis of public smoking bans on smoking behavior, we first considered the individual’s decision-making process conceptualized in the economics literature. (Appendix A provides an example of a dynamic optimization problem with regard to smoking behaviors in the presence of smoking bans.) Theory, as well as evidence from data, defines the roles of reinforcement, tolerance, and withdrawal and the dynamic nature of smoking decisions (Becker and Murphy, 1988; Matsumoto, 2014; Darden, Gilleskie and Strumpf, 2018). Theory also suggests that the presence of a public smoking ban reduces the utility an individual receives from the consumption of cigarettes. The implementation of a ban imposes both a time cost and a discomfort cost on smokers. The policy reduces the locations where, and consequently time of day when, an individual can smoke. It may relegate a smoker to areas where he gets less enjoyment from smoking. Alternatively, because smoking is often a social behavior, many individuals may receive higher utility from smoking in a social setting than they would smoking at home or alone (Fowler and Christakis, 2008; Gilleskie and Li, 2018).
The individual’s decision problem is to select an optimal level, c, of cigarette consumption today, Ct = c, to maximize his expected lifetime utility, Vc(St, εt), where St is the smoking stock (or summary of past smoking behavior). We can use the theoretical model in Appendix B that defines the time t lifetime value of each smoking alternative, Vc(St, εt) to derive the demand for cigarettes as a function of the information available to an individual at the time of decision making. That is, the probability of smoking level c is
| (1) |
where Xt represents individual demographic, socioeconomic, and health characteristics (such as gender, age, education, household size, employment, household income, health insurance, and health). His observed smoking behavior is also influenced by cigarette prices (PtC) and the presence of smoking bans in his province (Bt), among other things. In turn, his behavior influences the utility and health of nonsmokers (and smokers) who spend time in proximity to the individual.
Our data and empirical framework provide a means of quantifying these demand and exposure determinants. As mentioned previously, bans may impose time and discomfort costs that lower the utility of cigarette consumption. Hence, optimal behavior suggests that the demand for a particular quantity of cigarettes, c, falls when bans are imposed (i.e.,). We test this demand assumption as well as the conjecture that a reduction in consumption will persist over time after the passage of a ban. While a reduction persistence may be explained by a declining addictive stock (which we are unable to measure in our cross-sectional data), it is important to document differential ban effects over time. Similarly, if smoking bans alter the composition of people around the individual smoker, the disutility of the restrictions may evolve over time.
Specifically, we summarize the demand function for the number of cigarettes smoked per day and its arguments as
| (2) |
where Ct indicates the number of cigarettes consumed per period t.6 We include time-varying indicators of adoption of full and partial bans by particular provinces in Argentina to identify policy effects. In addition to indicators for the presence of both full and partial smoking bans, we include variables that quantify the number of years since full or partial ban implementation (summarized in the vector of variables, Bt). The coefficients on these variables allow for estimation of the immediate effects of the policy implementation and the effects of that policy over time.7
Fixed province effects (σp) account for variation in unobserved smoking sentiment or enforcement and other potential province-level differences that impact smoking behavior (i.e., prices of other goods). We also control for aggregate unobservables that vary over time using time fixed effects (σt). As mentioned previously, due to the lack of province-level variation in cigarette prices and only three cross-sectional data points, price data (PtC) are perfectly collinear with our year indicators. These indicators, therefore, measure the effects of price variation, along with numerous other countrywide factors that may influence cigarette consumption over time.8
Theory suggests that one’s history of smoking, or the addictive stock (St), impacts current smoking behavior. The Argentina data are cross sectional and, by design, do not record smoking behavior of the same individual at multiple points in time. Hence, we cannot control for (or empirically model) past smoking behavior. Fortunately, the data do include information on whether an individual has ever smoked in the past. We use this variable to separate current nonsmokers into never smokers and former smokers. To estimate the marginal effects of the theoretical determinants of current smoking behavior, we use the full sample (which includes those with no history of smoking) as well as restrict our sample to those individuals who have smoked at some point in the past. We also know the age at which an individual began smoking, and we control for the age of initiation when explaining the level of consumption conditional on being a current smoker. Among current smokers of the same age, those who began smoking at a younger age are likely to have more years of smoking experience (i.e., a larger addictive stock).9
The point-in-time survey also asks individuals to report their general pattern of smoking (i.e., frequency). We denote the regularity of smoking by the indicator Rt and assume that the same vector of determinants that explain demand also explain regularity of smoking. That is,
| (3) |
where regularity of smoking is never (j = 0), occasionally (j = 1), and every day (j = 2). We explore the differential impact of bans on these different types of smokers, as well as condition on these types when analyzing the bans’ effects on consumption quantities.
Because smoking bans are often implemented to reduce secondhand smoke exposure in public places, we estimate the effects of smoking bans on ETS exposure. Individual reports of regular exposure to ETS in public places (Ot) is modeled as
| (4) |
We assume exposure depends on a similar set of variables as demand: demographic, socioeconomic and health characteristics, cigarette prices, and smoking policies. Although addictive stock is not included as a determinant, we do expect that individuals who smoke will experience more ETS than nonsmokers as the former are more likely to associate with others who smoke. Therefore, we estimate the effect of public smoking bans on secondhand smoke exposure using the full sample (i.e., the general population) and the sample of nonsmokers separately.
4. Data
4.1. National Risk Factor Survey
To empirically evaluate the effects of smoking bans on individual smoking behaviors in Argentina, we use the National Risk Factor Survey (ENFR – Encuesta Nacional de los Factores de Riesgo), a stratified random survey distributed by Argentina’s National Ministry of Health in 2005, 2009, and 2013 (Ministerio de Salud).10 The ENFR project was initiated in 2005 due to a lack of national-level information on the risk factors for cardiovascular disease, a leading cause of death in Argentina. The survey is based on a questionnaire proposed by the Pan American Health Organization (PAHO) and the World Health Organization (WHO), and it has been received well by the Argentinian population with response rates of 86.7, 79.8, and 70.7 percent in the first three survey distributions, respectively. By collecting these data, the Ministry of Health desires to develop effective new health policies and improve health promotion and preventative care strategies on a national level (Ferrante et al., 2007). The questionnaires and codebooks are available for each year and contain sufficiently consistent wording of questions across survey years (with the addition of some new questions in later survey years).
The survey questions inquire about cigarette consumption behavior, including whether an individual has ever smoked, whether he or she currently smokes, age of smoking initiation, how often he or she smokes, and how many cigarettes he or she smokes per day. Using these data we construct dependent variables that describe current extensive and intensive margins of smoking (i.e., prevalence, regularity, and quantity). We also examine a binary indication of exposure to ETS. Each survey wave contains demographic, socioeconomic, and health information, including gender, age, education, household size, employment, household income, health insurance, and body mass, on over 32,000 individuals aged 18 and over from general urban areas (i.e., cities with greater than 5000 inhabitants) in all 23 provinces and the capital city of Buenos Aires.
We acknowledge some limitations of these data. First, as with many individual surveys, information is self-reported, which presents the possibility of response bias (e.g., underreported cigarette consumption). Second, the surveyed sample is repeated cross-sections of individuals in the population rather than a panel of the same individuals, making it difficult to account for the addictive and dynamic nature of cigarette consumption and to follow the same individuals through different stages of policy implementation. Third, while national data sources provide aggregated prices of cigarettes over time, province-level prices are not available (yet have been reported to vary little across regions). Additionally, the country’s reporting of consumer price index components changed in 2008. The lack of price variation at the province level and the inability to accurately deflate nominal prices prevent us from including both the price of cigarettes and a time trend in our regressions, as they would be perfectly collinear and potentially capture changes in measurement. Additionally, due to the unavailability of accurate inflation data to calculate real income, we use deviations from the mean of nominal income each year as our measure of income variation.
Despite these limitations, the ENFR presents unique advantages. Because it contains individual-level smoking data from a nationally-representative sample, we use the cross-province and cross-time variation in smoking bans to measure their impact. Furthermore, it is the most extensive and reliable dataset on health characteristics and behavior in Argentina and yields 108,489 observations over three years. The ENFR provides the best data available to make reliable estimates of the impact of public smoking bans in Argentina.
4.2. Descriptive Analysis and Construction of Key Variables
The dependent variables – smoking prevalence, smoking regularity, quantity of cigarettes smoked, and environmental tobacco smoke (ETS) exposure – are summarized in Table 1 for all individuals in all provinces and by ban status within the provinces. Approximately 52 percent of all individuals surveyed responded that they ever smoked. On average, 28 percent of individuals in any survey wave report currently smoking, and 53 percent of the individuals who report smoking in the past are current smokers. Nationally, smoking rates have declined over time: 29.91, 27.65, and 25.70 percent in 2005, 2009, and 2013, respectively.
Table 1:
Summary Statistics: Dependent Variables
| All Provinces |
No ban in province/year |
Ban in province/year |
||||||
|---|---|---|---|---|---|---|---|---|
| Variable | Sample Size | Mean | Std Dev | Mean | Std Dev | Mean | Std Dev | |
| Smoking Prevalence | ||||||||
| Ever Smoker | P(St > 0) | 108,489 | 0.524 | 0.499 | 0.533 | 0.499 | 0.515 | 0.500 |
| Current Smoker | P(Ct > 0) | 108,489 | 0.279 | 0.449 | 0.289 | 0.453 | 0.269 | 0.444 |
| Current Smoker if Ever Smoked | P(Ct > 0 | St > 0) | 56,882 | 0.533 | 0.499 | 0.542 | 0.498 | 0.523 | 0.499 |
| Smoking Regularity | ||||||||
| Nonsmoker | P(Rt = 0) | 0.716 | 0.705 | 0.727 | ||||
| Occasional Smoker | P(Rt = 1) | 108,489 | 0.080 | 0.089 | 0.071 | |||
| Everyday Smoker | P(Rt = 2) | 0.204 | 0.206 | 0.203 | ||||
| Quantity of Cigarettes Smoked per day* | ||||||||
| if a Current Smoker | Ct | Ct > 0 | 30,289 | 10.647 | 9.963 | 10.131 | 9.592 | 11.206 | 10.322 |
| if an Occasional Smoker | Ct | Rt = 1 | 8,379 | 4.211 | 5.705 | 4.162 | 5.813 | 4.273 | 5.566 |
| if an Everyday Smoker | Ct | Rt = 2 | 21,910 | 13.112 | 10.143 | 12.644 | 9.757 | 13.591 | 10.504 |
| Environmental Tobacco Smoke Exposure | ||||||||
| Regularly Exposed | P(Ot = 1) | 108,489 | 0.469 | 0.499 | 0.495 | 0.500 | 0.443 | 0.497 |
| Regularly Exposed if a Nonsmoker | P(Ot = 1 | Ct = 0) | 78,186 | 0.384 | 0.486 | 0.409 | 0.492 | 0.359 | 0.480 |
Notes: Column 2 denotes the form of the dependent variable in the estimating equation (Section 3). Column 3 specifies the size of the sample used in estimation (Section 5).
We drop 14 individuals who report being a current smoker but do not report quantity smoked.
Surveyed individuals report how often they smoke (i.e., occasionally or every day) and how many cigarettes they smoke per day. Over 70 percent of smokers in Argentina are heavy users (i.e., smoke every day). The distribution of smoking quantity per day for occasional smokers is concentrated at smaller levels than that of everyday smokers with means of 4.2 and 13.1 cigarettes per day, respectively (Figure 2).11 The data also reveal that male smokers smoke more cigarettes per day than female smokers, and older smokers smoke more than younger smokers.
Figure 2:
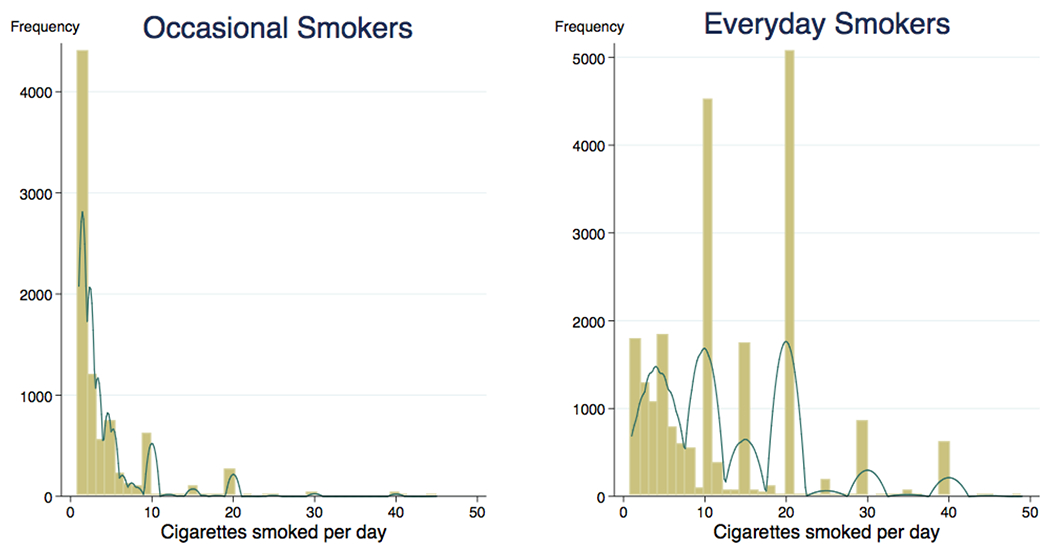
Daily smoking quantity, by smoking regularity
Finally, all individuals report whether they are regularly exposed to tobacco smoke at home and in public places (i.e., secondhand smoke).12 Approximately 46.9 percent of the population reports being regularly exposed to ETS; however, only 38.2 percent of nonsmokers report regular ETS exposure. This difference (Figure 3) may suggest that smokers spend more time around other smokers than nonsmokers do. A higher proportion of younger individuals report ETS exposure than older individuals, which may be reflect differences in propensity to frequent restaurants, bars, and other venues where smoking is most prevalent.
Figure 3:
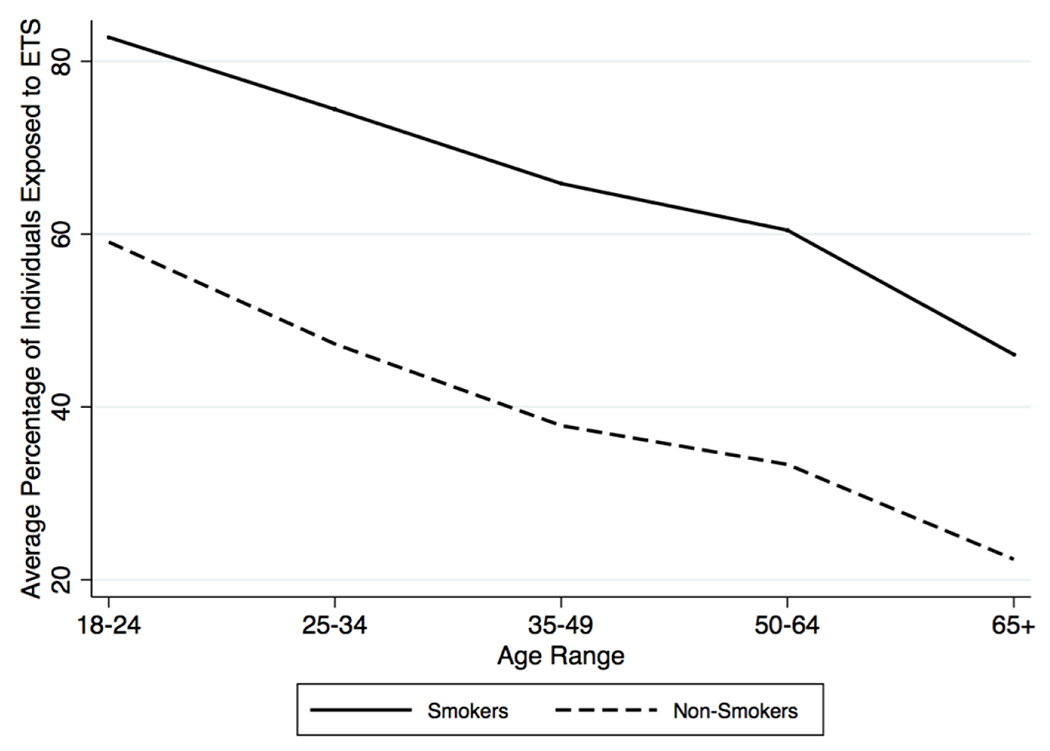
ETS Exposure, by age and smoking status
Men comprise a significantly larger proportion of smokers than nonsmokers. In fact, over a third of men currently smoke while less than a quarter of women currently smoke. Smokers also tend to be younger; the average age of smokers in the sample is 39.5, while the average age of nonsmokers is 46.2. Smokers are less likely to have completed university-level education than are nonsmokers. Although a smaller proportion are employed, nonsmokers are more likely than smokers to be female, older, and non-employed. They are also less likely to be unemployed than smokers. Indeed, the household income of nonsmokers is larger than that of smokers, and nonsmokers are more likely to have health insurance. Summary statistics for the main demographic, socioeconomic, and health variables are displayed in Table 2 for the full research sample, for current nonsmokers, and for current smokers.
Table 2:
Summary Statistics: Independent Variables
| Full Sample | Nonsmokers | Smokers | ||||
|---|---|---|---|---|---|---|
| Variable | Mean | Std Dev | Mean | Std Dev | Mean | Std Dev |
| Male | 0.435 | 0.496 | 0.398 | 0.490 | 0.530 | 0.499 |
| Age | 44.334 | 17.780 | 46.197 | 18.563 | 39.526 | 14.514 |
| Education | ||||||
| No Education | 0.020 | 0.142 | 0.023 | 0.150 | 0.014 | 0.118 |
| Completed Primary | 0.334 | 0.472 | 0.346 | 0.476 | 0.303 | 0.460 |
| Completed Secondary | 0.382 | 0.486 | 0.359 | 0.480 | 0.439 | 0.496 |
| Completed University | 0.264 | 0.441 | 0.272 | 0.445 | 0.243 | 0.429 |
| Household Size | 3.447 | 1.967 | 3.389 | 1.943 | 3.596 | 2.021 |
| Employment | ||||||
| Employed | 0.625 | 0.484 | 0.585 | 0.493 | 0.727 | 0.445 |
| Unemployed | 0.044 | 0.204 | 0.038 | 0.192 | 0.058 | 0.233 |
| Out of Labor Force | 0.331 | 0.471 | 0.377 | 0.485 | 0.215 | 0.411 |
| Income | ||||||
| Nominal Income | 1823.04 | 2130.76 | 1846.66 | 2153.76 | 1762.36 | 2069.37 |
| Normalized Income* | 0.000 | 1.000 | 0.002 | 1.001 | −0.005 | 0.998 |
| Income Missing | 0.055 | 0.227 | 0.056 | 0.229 | 0.052 | 0.221 |
| Health | ||||||
| Uninsured | 0.316 | 0.465 | 0.287 | 0.453 | 0.391 | 0.488 |
| Insurance Missing | 0.025 | 0.156 | 0.023 | 0.149 | 0.030 | 0.171 |
| Body Mass Index (BMI) | 26.120 | 4.969 | 26.284 | 4.996 | 25.702 | 4.873 |
| BMI Missing | 0.072 | 0.258 | 0.077 | 0.267 | 0.059 | 0.235 |
| Age of Smoking Initiation** | 17.674 | 5.320 | 17.956 | 5.459 | 17.426 | 5.183 |
| Initiation Age Missing | 0.016 | 0.124 | 0.018 | 0.132 | 0.014 | 0.116 |
| Full Ban | 0.124 | 0.329 | 0.125 | 0.330 | 0.121 | 0.327 |
| Partial Ban | 0.374 | 0.484 | 0.380 | 0.485 | 0.359 | 0.480 |
| Years since Full Ban*** | 2.637 | 2.430 | 2.682 | 2.440 | 2.517 | 2.400 |
| Years since Partial Ban*** | 3.566 | 2.764 | 3.588 | 2.791 | 3.508 | 2.764 |
| Samole Size | 108,489 | 78,186 | 30,303 | |||
Note:
Income normalized using mean and standard deviation by year.
Age of initiation among current non-smokers who ever smoked.
Years since ban among those person-year observations which a provincial ban exists.
For the regression analyses, we normalize the values of the independent variables such that the constant term in each regression represents the expected smoking behavior (i.e., smoking prevalence, smoking regularity, smoking quantity, ETS exposure) of a 40 year-old woman living in a household with four people in the province of Buenos Aires in 2005. She has completed secondary education, is employed, has the mean national income13 for each year (AR$858 in 2005, AR$2255 in 2009, and AR$2536 in 2013), has health insurance, and has a body mass index (BMI) of 26. Sample proportions by province and year are provided in Appendix Table A2.
4.3. Construction of Policy Variables
For each province and each year, our policy variable indicates whether the province has a full or partial smoking ban in place during the year. Ratification of bans took place at variable times over the years 2003 to 2013.14 We also create a variable measuring the number of years that a ban has been in place in a province. For example, the province of Buenos Aires initiated a partial smoking ban in 2008. Individuals living in this province and surveyed in 2005 experience no smoking ban. By the time of the 2009 survey, the ban had been in place one year. In 2013, the ban had existed for five years. The EFNR does not allow us to determine the survey respondent’s length of residency in a particular province; hence, we cannot measure the number of years that a particular individual has faced a local ban.
A concern that is often raised with the implementation of state-level tobacco control policies is the possibility of selection into tobacco control based on specific state (or voter) characteristics. That is, states with a strong (unobserved) anti-tobacco sentiment may, consequently, be observed to have low levels of tobacco consumption. Moreover, these states may be the first to implement anti-smoking policies. (California is often cited as an example in the US.) On the other hand, states may decide to pass strong tobacco control legislation in order to reduce high levels of tobacco consumption. If specific provinces in Argentina followed such trends, it is possible that those that passed legislation earlier are those that had the lowest (or highest) initial levels of consumption or exposure. To test this theory of endogenous program placement, we aggregate the individual-level Argentina data to the province level for each year and create various province-level demographic variables that may explain the presence of a partial (or full) ban. Our empirical findings, presented in Appendix Table A3, suggest that initial smoking levels and tobacco exposure rates did not influence the implementation of province-level policies.
Additionally, analyses of the type we undertake to identify policy impacts often conduct event studies depicting trends in smoking behavior pre- and post-policy implementation or test differences in average smoking prevalence across the control and treatment groups during the pre-treatment era. Recall that our smoking data comprise three points in time (2005, 2009, and 2013) and some provinces imposed bans in or prior to 2005. Nonetheless, we conduct a t-test comparing means of smoking prevalence in provinces during pre-treatment periods (i.e., during periods in which a ban did not exist within a province) across those who never imposed a smoking ban (full or partial) and those who adopted any type of ban at some point during our survey period. We cannot reject the null hypothesis with 95 percent confidence: that is, there is no evidence that the smoking rates in provinces that never adopted a smoking ban are different from those that did (t-stat = −1.435; p-value = 0.16). If we condition on looking only at adoption of full bans, we find that smoking rates are higher in provinces who eventually impose a full ban.
We depict the results from the event study in Figure 4 below. The graphs depict province-level smoking prevalence rates (top), quantities (middle), and exposure rates (bottom) by years to and from both full (solid line) and partial (dashed lines) bans. These analyses indicate that the implementation of a partial smoking ban does not impact prevalence, but both partial and full bans change the trajectory of smoking quantities and exposure. In all cases, there is a downward trend in smoking that continues (and abates slightly, but not significantly) as the bans are implemented. However, we observe a statistically significant (at the 6 percent level) effect of the bans on smoking quantity conditional on smoking (depicted in the middle graph). Average quantities of cigarettes consumed are larger in provinces that implement public smoking bans than in provinces that do not have a ban. To explore pre-policy trends, these smoking statistics are displayed for provinces that never impose a ban (dotted line).15 For smoking prevalence and smoke exposure, trends in provinces that never adopt are similar to those who eventually adopt (either the full or partial ban). The impact of the bans is explored more deeply in the rest of the paper.
Figure 4:
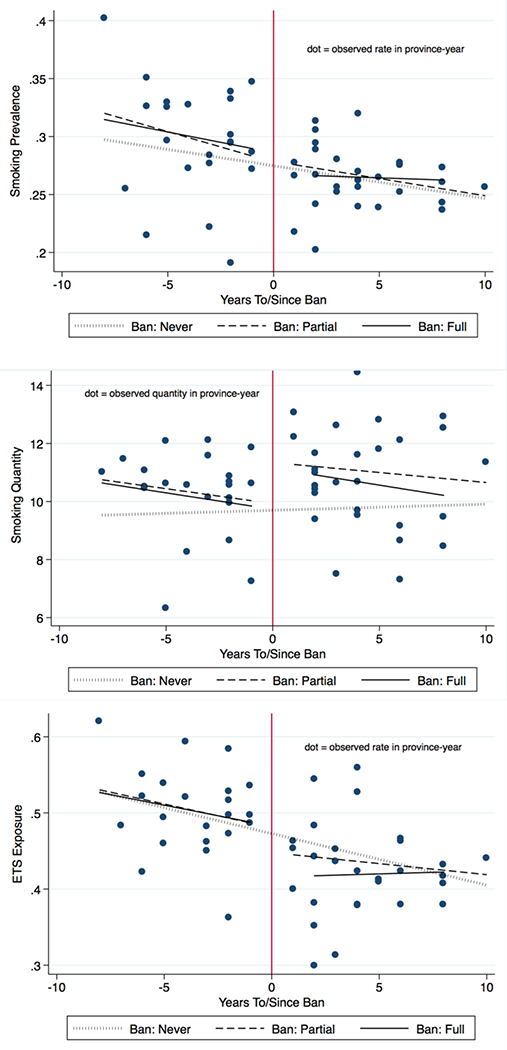
Event Study Analyses, of smoking prevalence and quantity
Note: The top graph depicts the results of an event study analysis of smoking prevalence prior to and after (partial and full) ban implementation. The middle graph explores each ban’s effect on smoking quantities conditional on smoking, while the bottom graph shows these effects on ETS exposure.
5. Results
5.1. Smoking Prevalence
Our analysis begins by examining the effects of public smoking bans at the extensive margin (i.e., current smoking prevalence, or whether or not an individual currently smokes). We measure impacts of determinants on smoking prevalence using the full sample (to reflect the general population) and the sample of those individuals with any smoking history prior to the survey. The estimated regressions follow a standard logit model with two-way fixed effects and are detailed in Table 3. In order to investigate heterogeneous effects of the smoking bans, we estimate average ban and year since implementation effects (Specification 1) and then add ban/demographics interaction terms (Specification 2).16
Table 3:
Parameter Estimates: Smoking Prevalence, Logit
| Full Sample | Sample with History of Smoking | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | Specification 1 | Specification 2 | Specification 1 | Specification 2 | ||||
| Full ban present | −0.024 | (0.058) | 0.038 | (0.056) | −0.091 | (0.070) | −0.074 | (0.077) |
| Years since full ban implementation | −0.017 | (0.009) ** | −0.019 | (0.008) ** | −0.002 | (0.016) | −0.006 | (0.017) |
| Full Ban x Male | −0.093 | (0.075) | 0.014 | (0.074) | ||||
| Full Ban x Age - 40 | 0.002 | (0.001) *** | 0.003 | (0.002) | ||||
| Full Ban x Normalized Income | −0.080 | (0.019) *** | −0.075 | (0.018) *** | ||||
| Partial ban present | −0.015 | (0.044) | 0.060 | (0.052) | 0.037 | (0.064) | 0.104 | (0.067) |
| Years since partial ban implementation | 0.015 | (0.009) ** | 0.014 | (0.009) * | 0.011 | (0.013) | 0.012 | (0.013) |
| Partial Ban x Male | −0.170 | (0.063) *** | −0.155 | (0.061) ** | ||||
| Partial Ban x Age - 40 | 0.004 | (0.002) ** | 0.003 | (0.002) | ||||
| Partial Ban x Normalized Income | −0.056 | (0.020) ** | −0.065 | (0.019) *** | ||||
| Male | 0.469 | (0.045) *** | 0.543 | (0.058) *** | 0.141 | (0.042) *** | 0.197 | (0.052) *** |
| Age - 40 | −0.010 | (0.001) *** | −0.011 | (0.001) *** | −0.020 | (0.001) *** | −0.021 | (0.001) *** |
| (Age - 40)/10 squared | −0.086 | (0.005) *** | −0.087 | (0.006) *** | −0.075 | (0.005) *** | −0.076 | (0.006) *** |
| Normalized Income | −0.015 | (0.009) | 0.016 | (0.013) | −0.028 | (0.011) ** | 0.005 | (0.014) |
| Year 2009 | −0.094 | (0.029) *** | −0.095 | (0.029) *** | −0.099 | (0.052) * | −0.100 | (0.052) * |
| Year 2013 | −0.208 | (0.060) *** | −0.206 | (0.061) *** | −0.155 | (0.089) * | −0.156 | (0.091) * |
| Constant | −0.698 | (0.045) *** | −0.719 | (0.049) *** | 0.248 | (0.066) *** | 0.242 | (0.065) *** |
| Number of observations | 108,489 | 56,882 | ||||||
Note: Specification 1 measures full and partial ban effects, on average. Specification 2 allows for heterogeneous ban effects by gender, age, and income. Each specification controls for education, household size, employment, health insurance, body mass, missing indicators (for income, health insurance, body mass) and province indicators. Standard errors (in parentheses) are clustered at the province level and account for any additional heterogeneity in ban effects.
indicates significance at 1% level;
5% level;
10% level.
A full or partial ban does not significantly affect average smoking prevalence in Argentina in the first year that it is implemented. However, there is a significant (at the 5 percent level) reduction in smoking each year after the first year of implementation of a full ban. Simulated marginal effects suggest an overall reduction in smoking prevalence of about 0.7 percent one year after the implementation of a full ban and 2.0 percent five years after the implementation of a full ban. Results from specification 2, which allows for heterogeneous effects of the bans, suggest that individuals with above-average income or who are younger than 40 years of age are less likely to smoke in a province with a full or a partial ban.17 Additionally, men are significantly less likely to smoke in provinces imposing a partial ban.
Recognizing that there are individuals who have never smoked and who may be indifferent to the ban (with regard to own smoking behavior), we estimate the impact of the bans on those individuals with some history of smoking. Table 3 indicates that, in general, the bans have no immediate or long-term effect on current smoking probabilities of individuals who have ever smoked (Specification 1). However, the partial ban reduces the probability of smoking among men and both the full and partial ban deter smoking as income rises.18
While the public smoking ban variables provide the greatest insight into the effects of tobacco control policies over time, the time indicator variables also have important implications. For all four regressions presented in Table 3, the coefficients on the indicators for the year 2009 and the year 2013 are negative and significant, and the value of the coefficient on the 2013 indicator is significantly greater than the 2009 indicator. Generally, the negative coefficients on these variables imply that unobserved aggregate factors influence smoking prevalence of all individuals over time. Because smoking prevalence is observed only three times, we are limited in the functional form specification of this aggregate impact. Nonetheless, signs and relative sizes of these coefficients suggest that there may have been a cultural shift or a change in national attitudes towards smoking, both preceding and continuing after the passage of the National Tobacco Control Act of 2011, which contributed to a reduction in prevalence. While only five of the provinces ratified national legislation of 2011 (and we have no data on enforcement of the national law), there may have been venues and cities that independently implemented bans. It is possible that the 2013 indicator accounts for some of these indirect effects of the legislation.
5.2. Smoking Regularity
After determining the effects of smoking bans on the proportion of the population that smokes, we look more closely at intensive margins of smoking. We use a multinomial logit approach (with two-way fixed effects) to capture regularity (or frequency) of smoking where the base outcome is nonsmoking and the two alternative outcomes are smoking occasionally and smoking every day. The multinomial logit estimator allows for different marginal effects of explanatory variables on each regularity outcome. Parameter estimates are provided in Table 4.
Table 4:
Parameter Estimates: Smoking Regularity, Multinomial Logit
| Full Sample | Sample with History of Smoking | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | Occasional Smoker | Everyday Smoker | Occasional Smoker | Everyday Smoker | ||||
| Full ban present | 0.114 | (0.087) | −0.000 | (0.051) | −0.008 | (0.099) | −0.097 | (0.075) |
| Years since full ban implementation | −0.029 | (0.018) | −0.015 | (0.007) ** | −0.014 | (0.011) | −0.003 | (0.021) |
| Full Ban x Male | −0.165 | (0.100) | −0.063 | (0.079) | −0.038 | (0.088) | 0.036 | (0.077) |
| Full Ban x Age - 40 | −0.001 | (0.003) | 0.004 | (0.002) ** | −0.001 | (0.004) | 0.004 | (0.002) ** |
| Full Ban x Normalized Income | −0.070 | (0.037) * | −0.078 | (0.025) *** | −0.061 | (0.038) | −0.078 | (0.022) *** |
| Partial ban present | 0.048 | (0.077) | 0.063 | (0.048) | 0.101 | (0.081) | 0.106 | (0.071) |
| Years since partial ban implementation | 0.008 | (0.011) | 0.021 | (0.009) ** | 0.007 | (0.014) | 0.016 | (0.014) |
| Partial Ban x Male | −0.194 | (0.092) ** | −0.156 | (0.058) *** | −0.182 | (0.083) ** | −0.141 | (0.056) ** |
| Partial Ban x Age - 40 | 0.000 | (0.002) | 0.004 | (0.002) * | −0.002 | (0.002) | 0.003 | (0.002) |
| Partial Ban x Normalized Income | −0.036 | (0.042) | −0.068 | (0.025) *** | −0.036 | (0.040) | −0.077 | (0.023) *** |
| Male | 0.558 | (0.090) *** | 0.541 | (0.054) *** | 0.210 | (0.076) *** | 0.191 | (0.046) *** |
| Age - 40 | −0.028 | (0.002) *** | −0.004 | (0.001) ** | −0.037 | (0.002) *** | −0.014 | (0.002) *** |
| (Age - 40)/10 squared | −0.037 | (0.006) *** | −0.109 | (0.006) *** | −0.028 | (0.006) *** | −0.097 | (0.006) *** |
| Normalized Income | −0.044 | (0.019) ** | 0.035 | (0.020) * | −0.057 | (0.026) ** | 0.026 | (0.019) |
| Year 2009 | −0.109 | (0.047) ** | −0.110 | (0.038) *** | −0.078 | (0.058) | −0.111 | (0.060) * |
| Year 2013 | −0.152 | (0.079) * | −0.254 | (0.057) *** | −0.069 | (0.087) | −0.201 | (0.096) ** |
| Constant | −2.236 | (0.076) *** | −0.941 | (0.046) *** | −1.368 | (0.077) *** | 0.018 | (0.071) |
| Number of observations | 108,489 | 56,882 | ||||||
Note: Base case among the multinomial logit outcomes is nonsmoker. Each regression controls for education, household size, employment, health insurance, body mass, missing indicators (for income, health insurance, body mass) and province indicators. Standard errors (in parentheses) are clustered at the province level and account for any additional heterogeneity in ban effects.
indicates significance at 1% level;
5% level;
10% level.
While the findings presented in Section 5.1 indicate a reduction in smoking prevalence several years after the implementation of a full ban, we explore whether the reduction varies by smoking regularity (i.e., occasional smoking or everyday smoking). Unconditional on a smoking history, there is a reduction (significant at the p<0.05 level) in everyday smoking behavior several years after the implementation of a full smoking ban, yet a slight increase in provinces with partial bans. The reduction is 0.7 percentage points one year after the implementation of a provincial full ban, and 1.4 percentage points five years after implementation. The reduction in everyday smoking, along with the (non-significant) reduction in occasional smoking behavior, corresponds to an increase in the proportion of nonsmokers by 1.9 percentage points.19 The results also suggest that individuals below age 40 and those with above-average incomes are more likely to respond to a full smoking ban, for the full sample and among those who smoke regularly.
While the full sample results presented in Table 4 indicate that a full ban is associated with a reduction in everyday smoking prevalence, they also reveal an increase in the probability of being an everyday smoker a number of years after the passage of a partial ban (e.g., 1.5 percentage points five years after the implementation). Partial bans are also associated with a 0.2 percentage point decline in the proportion of the population who smoke occasionally and a 1.3 percentage point decline in the proportion of nonsmokers five years after implementation (with the estimated coefficients being jointly, but not individually, significant). A possible explanation for this finding, though not testable in our data, is peer effects that arise when smokers are congregated in designated smoking rooms where smoking is socially acceptable and reinforced. Interactions that allow for heterogeneous partial ban impacts suggest a relative decrease in everyday smoking among men and wealthy individuals. These heterogeneous ban effects on smoking regularity are similar if we use the full sample or if we condition on those individuals with a history of smoking.
5.3. Smoking Quantity
In addition to participation and regularity, we observe the smoking intensity (i.e., quantity of cigarettes smoked per day) of those individuals who currently smoke.20 We explore whether partial or full bans impact amount smoked conditional on any use. Because those who smoke occasionally and those who smoke every day exhibit differences in behavior and addictive stock, we also examine the effects of restricted smoking policies on smoking quantity for these two groups of smokers separately. We use ordinary least squares (OLS) on the integer-valued outcome and OLS on its natural log to account for skewness in the outcome. To explore the sensitivity of the estimated marginal effects of the ban to distributional assumptions, we also use a generalized linear model (GLM) with a gamma distribution. We select a gamma distribution over a negative binomial distribution and Poisson distribution due to the nature of the data and the fit of each distribution.21 Lastly, we examine whether public smoking bans have had different effects at different levels of smoking intensity using a quantile regression. The results from these estimators (each with two-way fixed effects) are presented in Tables 5a and 5b, respectively.22
Table 5a:
Parameter Estimates: Smoking Quantity, OLS and GLM
| All Smokers, OLS | Occasional Smokers, OLS | Everyday Smokers, OLS | ||||
|---|---|---|---|---|---|---|
| Variables | Quantity | Ln(Quantity) | Quantity | Ln(Quantity) | Quantity | Ln(Quantity) |
| Full ban present | −0.048 (0.344) | −0.036 (0.034) | −0.578 (0.363) | −0.112 (0.068) | 0.366 (0.475) | 0.030 (0.037) |
| Years since full ban | −0.051(0.074) | 0.003 (0.009) | −0.063 (0.058) | 0.001 (0.009) | −0.077 (0.071) | −0.001 (0.007) |
| Partial ban present | 0.874 (0.252) *** | 0.058 (0.027) ** | 0.373 (0.252) | 0.035 (0.050) | 1.030 (0.326) *** | 0.064 (0.025) ** |
| Years since partial ban | 0.024 (0.061) | 0.004 (0.005) | −0.046 (0.051) | −0.006 (0.010) | 0.028 (0.075) | 0.005 (0.005) |
| Year 2009 | −0.061 (0.235) | −0.010 (0.025) | 0.130 (0.245) | 0.042 (0.046) | −0.029 (0.267) | −0.015 (0.022) |
| Year 2013 | −0.309 (0.312) | −0.009 (0.029) | 0.103 (0.307) | 0.075 (0.060) | −0.177 (0.415) | −0.005 (0.030) |
| Constant | 11.310(0.258) *** | 2.032 (0.026) *** | 2.834 (0.221) *** | 0.786 (0.047) *** | 13.157 (0.330) *** | 2.311 (0.025) *** |
| Variables | All Smokers GLM with Gamma | Occasional Smokers GLM with Gamma | Everyday Smokers GLM with Gamma | |||
| Full ban present | −0.007 (0.034) | −0.114 (0.084) | 0.029 (0.037) | |||
| Years since full ban | −0.006 (0.009) | −0.012 (0.013) | −0.007 (0.007) | |||
| Partial ban present | 0.079 (0.023) *** | 0.075 (0.060) | 0.077 (0.024) *** | |||
| Years since partial ban | 0.004 (0.006) | −0.005 (0.012) | 0.004 (0.006) | |||
| Year 2009 | −0.006 (0.022) | 0.036 (0.061) | −0.004 (0.020) | |||
| Year 2013 | −0.028 (0.032) | 0.011 (0.076) | −0.014 (0.032) | |||
| Constant | 2.387 (0.024) *** | 1.104 (0.053) *** | 2.544 (0.025) *** | |||
| Number of observations | 30,289 | 8,379 | 21,910 | |||
Note: Quantity is modeled as a continuous variable using different estimators. Among the 30,303 smokers in the sample, only 30,289 reported their smoking quantity. Each regression controls for gender, age, age of initiation, income, education, household size, employment, health insurance, body mass, missing indicators (for income, health insurance, body mass) and province indicators. Standard errors (in parentheses) are clustered at the province level.
indicates significance at 1% level;
5% level;
10% level.
Table 5b:
Parameter Estimates: Smoking Quantity, Quantile Regression
| Quantile (Quantity Smoked at each percentile) |
||||||
|---|---|---|---|---|---|---|
| Variable | 25th percentile (3) | 50th percentile (8) | 75th percentile (16) | |||
| Full ban present | −0.202 | (0.176) | −0.153 | (0.246) | −0.322 | (0.485) |
| Years since full ban | 0.021 | (0.024) | −0.017 | (0.051) | −0.002 | (0.154) |
| Partial ban present | 0.119 | (0.115) | 0.304 | (0.246) | 1.108 | (0.358)*** |
| Years since partial ban | 0.010 | (0.016) | 0.036 | (0.034) | 0.028 | (0.062) |
| Year 2009 | −0.099 | (0.083) | −0.045 | (0.113) | 0.022 | (0.204) |
| Year 2013 | 0.031 | (0.110) | −0.095 | (0.256) | −0.116 | (0.411) |
| Constant | 4.233 | (0.250)*** | 9.902 | (0.632)*** | 16.276 | (0.699)*** |
| Number of Observations | 30,289 | |||||
Note: The quantity of cigarettes smoked per day is modeled using a quantile regression. Among the 30,303 smokers in the sample, only 30,289 reported their smoking quantity. Each regression controls for gender, age, age of initiation, income, education, household size, employment, health insurance, body mass, missing indicators (for income, health insurance, body mass) and province indicators. Standard errors (in parentheses) are clustered at the province level.
indicates significance at 1% level;
5% level;
10% level.
While we found that full smoking bans are associated with a decline in smoking prevalence (Section 5.1), we observe no significant association between full bans and smoking quantity conditional on smoking. After implementation of a partial policy, however, there is a significant increase in smoking intensity among everyday smokers and, more specifically, the everyday smokers who smoke at an intensity in the top quartile of all smokers. Recall that smokers smoke about 10.6 cigarettes per day on average, with occasional smokers consuming 4.2 per day and everyday smokers consuming 13.1. The OLS estimator on levels indicates that, among all smokers, the implementation of a partial smoking ban (i.e., immediate effect) is associated with a significant increase in smoking quantity of approximately 0.874 cigarettes per day. OLS on the natural log of smoking quantity and the GLM also estimate positive and significant coefficients that correspond to similar marginal effects.23 Smoking intensity increases as the number of years since the passage of a partial ban increases, but the effect is not significant, indicating that these partial policies have strong (perverse) immediate effects on consumption but these effects do not accumulate and grow over time.
Occasional smokers are, on average, younger than everyday smokers and may be more likely to smoke in social settings with friends; as such, one might expect larger effects of public smoking bans on the smoking intensity of these individuals.24 Yet, we do not see any significant effect of either a full or partial smoking ban on smoking intensity among occasional smokers. The reason that we observe a significant increase in smoking intensity among the entire population of smokers after the implementation of a partial ban stems from the fact that everyday smokers significantly increase their consumption in the presence of such bans, and this increase drives up the unconditional (on regularity) statistic. The OLS model predicts an average increase of 1.030 cigarettes smoked per day by everyday smokers after the implementation of a partial ban. Although the utility preference-ordering in our theoretical framework (Appendix B) predicts that a partial ban would lower the utility of smoking for an individual relative to no ban (potentially through reduced opportunities to smoke), it is important to consider the compensatory incentive of addicted smokers to smoke more in settings where and when they are able to do so. Additionally, although untestable with our data, if an everyday smoker increases his time spent with other everyday smokers in designated smoking areas (due to partial bans), he may smoke more cigarettes per day than he would with non-regulated smoking location options because of the reinforcing influence of peer effects on smoking behavior. Our findings suggest that the strategy of restricting smoking locations, while perhaps meant to be a gradual way of implementing positive change, has had a contradictory effect on the smoking behavior of everyday smokers.
In addition to establishing that everyday smokers increase their smoking intensity under partial public smoking bans, we find that individuals who smoke the largest quantities of cigarettes are impacted most strongly by the partial bans (based on the quantile regression results in Table 5b where the 75th percentile corresponds to a smoking intensity of 16 cigarettes per day). The model predicts that a partial ban is associated with an increase in consumption (by about 1.108 cigarettes per day) among smokers at this level of smoking intensity. Another interesting difference highlighted by prevalence and intensity comparisons is that smoking intensity has not steadily declined over time as prevalence has. This lack of a significant aggregate time impact has important implications for smoking behavior in Argentina. As stated previously, there may have been unobserved aggregate factors over time or a general cultural shift in attitudes toward smoking that contributed to a reduction in prevalence, yet those same factors do not appear to have influenced smoking intensity, or they were offset by some other change over time that increased intensity while having a minimal effect on prevalence.
One such aggregate change could be the affordability of cigarettes over time. Due to a lack of province-level variation and a corresponding perfect multicollinearity with the time indicator variables, the price of cigarettes is not included as an explanatory variable. Additionally, due to inaccurate inflation data reporting since 2007 in Argentina, it is difficult to calculate the real price of goods. However, using quarterly household income data from Argentina’s Personal Household Survey (EPH- Encuesta Permanente de Hogares) and monthly cigarette price data from the Ministry of Agriculture, we can calculate the quarterly average number of packs of cigarettes that can be purchased (i.e., a relative measure of the affordability of cigarettes).25 This information (depicted in Figure 5) suggests that cigarettes have become more affordable over time. It is possible that this increase in affordability offsets the general downward trend in smoking behavior over time. Our conjecture presents an exciting opportunity for future studies and, potentially, important implications for policymakers in Argentina, where tobacco prices remain low and very few tobacco taxes have been implemented.26
Figure 5:
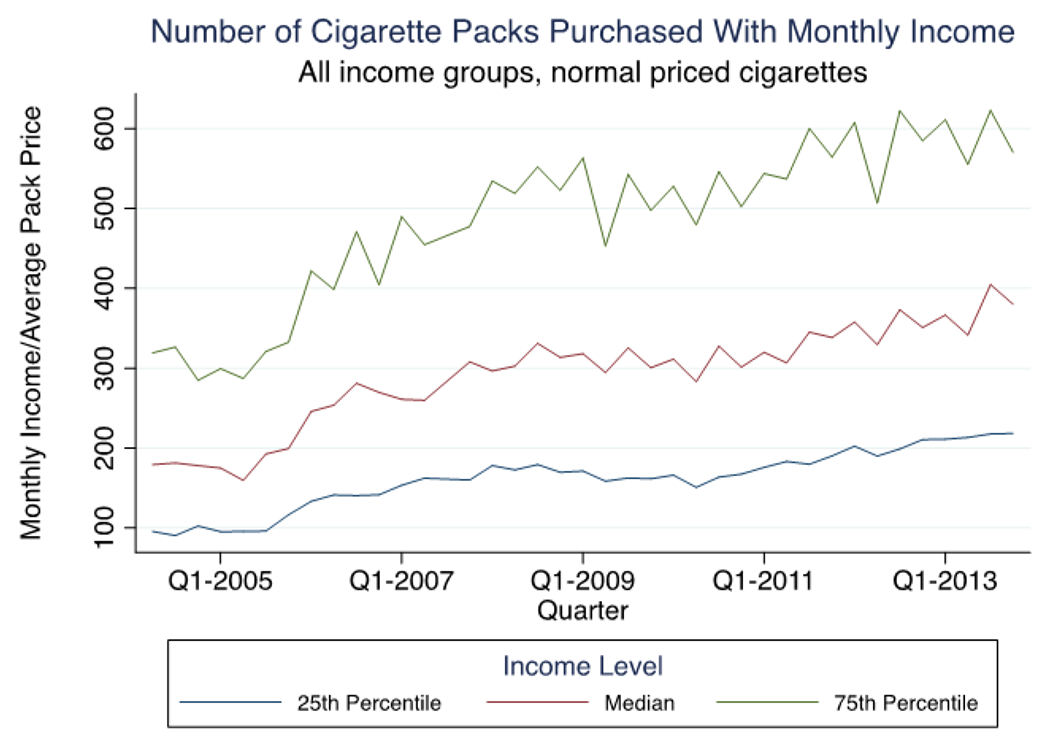
Average cigarette affordability, by income level
5.4. ETS Exposure
We conclude our investigation of the effects of public smoking bans by examining individual reports of environmental tobacco smoke (ETS) exposure, a public health concern that presents significant, and often underestimated, health risks.27 An indicator of whether or not an individual reports being regularly exposed (Ot) to environmental tobacco smoke (ETS) is the dependent variable of a standard logit model with two-way fixed effects, estimated on all individuals regardless of own smoking behavior and on current nonsmokers only. Coefficient results are presented in Table 6.
Table 6:
Parameter Estimates: Smoke Exposure, Logit
| Variable | Full Sample | Nonsmokers | ||
|---|---|---|---|---|
| Full ban present | −0.180 | (0.099) * | −0.226 | (0.101) ** |
| Years since full ban | −0.013 | (0.011) | 0.001 | (0.013) |
| Partial ban present | −0.068 | (0.076) | −0.071 | (0.079) |
| Years since partial ban | 0.003 | (0.014) | −0.001 | (0.015) |
| Year 2009 | −0.097 | (0.050) * | −0.105 | (0.054) * |
| Year 2013 | −0.347 | (0.105) *** | −0.347 | (0.117) *** |
| Constant | 0.111 | (0.073) | −0.231 | (0.080) *** |
| Number of observations | 108,489 | 78,186 | ||
Note: Each regression controls for gender, age, income, education, household size, employment, health insurance, body mass, missing indicators (for income, health insurance, body mass) and province indicators. Standard errors (in parentheses) are clustered at the province level.
indicates significance at 1% level;
5% level;
10% level.
Implementation of a full smoking ban significantly reduces exposure for all individuals (unconditional on own smoking behavior) and for nonsmokers. The full ban rapidly reduces the general exposure to secondhand smoke, as there appears to be no incremental impact in the years following implementation. It is estimated that nonsmokers are approximately 4.9 percentage points less likely to be exposed to ETS in the year that a full ban is imposed. Partial bans are not found to be significantly associated with any change in ETS exposure. These findings provide support for the benefits of full public smoking bans in Argentina.28
The aggregate time trends indicate a reduction in ETS exposure over time, with a greater reduction between 2009 and 2013 than between 2005 and 2009. This finding provides further support of the presence of unobserved cultural shifts and changes in attitudes towards smoking that likely developed during and after the passage of the National Tobacco Control Law.
6. Conclusions
This study examines the effects of public smoking bans on levels of smoking prevalence, smoking regularity, and smoking intensity in Argentina. While the investigated smoking behaviors are analyzed separately, the conditional relationships between them are explored. Furthermore, we determine the effects of smoking bans on environmental tobacco smoke exposure.
One of the key findings of our analyses is that full public smoking bans significantly reduce the prevalence of smoking over time. This reduction is associated with a decline in the number of individuals taking up smoking rather than an increase in the number of individuals who are quitting. The reduction is also associated with a decrease in the proportion of everyday smokers relative to the proportion of nonsmokers. These effects are greater among male, younger and wealthier individuals. Full bans do not have a significant impact on smoking intensity, which implies that smokers are finding other places and times to smoke. However, they do present benefits to nonsmokers, as they are associated with a significant decline in ETS exposure.
On the other hand, partial smoking bans appear to have negative effects that outweigh any benefits that they present. They do not significantly affect smoking prevalence or ETS exposure, and it is found that everyday smokers consume more cigarettes after the implementation of partial bans. These results provide evidence to support the ratification and implementation of the full bans dictated by Argentina’s National Tobacco Control Law of 2011. A conclusive analysis of the roles of peer effects and enforcement effects, in combination with this study, would provide additional evidence for stronger action (e.g., full versus partial bans) among policymakers.
Supplementary Material
Footnotes
We appreciate useful comments from David Guilkey, Klara Peter, Valentin Verdier, two editors and three anonymous referees, as well as support from the Institute for Clinical Effectiveness and Health Policy in Buenos Aires, Argentina. Additional comments are welcome at mcatal94@gmail.com or donna_gilleskie@unc.edu.
There was widespread support for smoking legislation in Argentina as early as 2005, but manufacturers – two multinational tobacco companies (Massalin Particulares (Philip Morris) and Nobleza-Piccardo (British-American Tobacco) who controlled the market – continued to promote and advertise its products until 2011. The national law implemented in 2011 prohibited advertising and sponsoring of tobacco. The fine for breaking the law is equivalent to 250 and 1,000,000 packets of the most expensive cigarettes on the market. (“Argentine law targets smoking in enclosed public spaces”. BBC News. 2 June 2011 Link). Schoj et al. (2010) provide the most convincing evidence of enforcement of provincial bans by measuring particulate matter in public venues.
Adolescence is the predominant age range at which smoking initiation occurs; 90 percent of smokers first tried cigarettes before age 19 (Centers for Disease Control and Prevention. “Youth and Tobacco Use.” http://www.cdc.gov/tobacco/data_statistics/fact_sheets/youth_data/tobacco_use/index.htm).
Burton (2020) explores the effects of local smoking bans on cigarette consumption as well as alcohol consumption, since individuals may substitute restricted behaviors with allowed behaviors, especially in bars and restaurants. She finds that bans lead to differential increases in drinking behavior by type of smoker.
Two of the four provinces that ratified the national law actually had their own provincial smoking bans in place at the time of ratification; the national law simply imposed stronger restrictions.
The progression of province-level smoking bans between 2004 and 2011 was similar to the experience at city- and state-levels in the US beginning in the 1970s (Institute of Medicine, 2010; American Lung Association). In 1973, Arizona became the first state to restrict smoking in several public places; Connecticut followed in 1974 by passing the first state law to restrict smoking in restaurants. Other states and individual cities followed suit over the next two decades, and San Luis Obispo, California became the first city in the world to ban smoking in all public buildings in 1990. By 2009, 30 states and the District of Columbia had passed comprehensive smoke-free legislation (Institute of Medicine). A number of studies have been conducted on smoke-free legislation within the US, which can serve as a useful and interesting comparison and potential check for external validity of the Argentinian results.
Cigarette consumption is skewed right and a large proportion of our sample reports zero consumption. (Section 4 provides detail from our estimation sample.) We explore how the determinants in Equation (2) explain the probability of any cigarette consumption (i.e., P(Ct > 0)), as well as the level (quantity) of cigarettes consumed conditional on having non-zero consumption (i.e., Ct | Ct > 0).
Although the National Tobacco Control Law was implemented and strongly encouraged nationally beginning in 2011, only four provinces ratified it. These four provinces are recorded as having full bans, yet any changes in national attitudes towards smoking, as well as the changes in cities and venues that followed the recommended law informally, are not picked up by the ban indicator. Rather, these unofficial effects are captured by the time indicators. This potential influence is important to consider in interpretation of the findings.
We acknowledge that we are unable to account for time-varying unobserved heterogeneity at the provincial level. We did interact the time indicators with several demographic characteristics, and find no significant differential effects of time in these dimensions.
To consider possible correlation between one’s smoking history and current smoking behavior, we estimated a Heckman selection model without an exclusion restriction (because our data do not contain one that is theoretically-justified) to jointly estimate the probability of ever smoking and the probability of currently smoking. Although the standard errors are inconsistent, we find that the correlation coefficient, which measures the correlation between the errors of the two equations, is not significantly different from zero. A similar maximum likelihood strategy to estimate the correlation between the smoking history, current smoking participation, and the level of smoking conditional on any smoking did not converge.
The 2005 survey information was collected between March and June; the 2009 survey, between October and December; and the 2013 survey, between November and December. These survey periods postdate periods of high inflation as well as an ad valorem emergency tax on cigarettes, and they conveniently span years of provincial implementation of partial and full indoor smoking bans.
Like many self-reported sources of smoking consumption, individual responses are clustered at intervals of 5 and 10 cigarettes per day. To account for this clustering, we considered mixture models of count data (e.g., heapreg in Stata) and did not find appreciably different results from those reported in Section 5.
Specifically, we measure exposure by responses of surveyed individuals to the question: “Do people regularly smoke near you?”. While there is a question about exposure to smoke in one’s home, the non-response rate to this question does not allow us to “subtract” the home exposure response from exposure generally so as to construct a measure of exposure in public places, which is what the bans address.
We do not convert the Argentine peso (ARS) to US dollars (USD) due to Argentina’s frequent exchange rate fluctuations and the existence of an unofficial exchange rate (fueled by the difficulty for locals to acquire dollars through traditional means) known as the “blue” rate. In 2005, the official exchange rate was 2.9 ARS per USD and the blue rate was 3.2 ARS per USD; in July of 2015, the official exchange rate was 8.0 ARS per USD and the blue rate was 14.0 ARS per USD. Instead, we measure deviations from the mean nominal income in each survey year.
Recall that almost two-thirds of the sampled individuals were interviewed in the last quarter of the calendar year (spring in Argentina), while the 2005 survey was conducted between March and June (autumn in Argentina). It has been suggested that season of the year may affect reported smoking through weather conditions (but we expect spring and autumn to be similar), taxing variation (but we see little variation in prices of cigarettes across provinces), and timing of quitting (e.g., New Year’s day).
We assign the average smoking rate (or quantity smoked if any or ETS exposure) of those provinces that never implemented a ban throughout our survey period in the year that corresponds to the years to/since ban in provinces that do. That is, for every “dot” in the figure (i.e., every province/year data point), we record the average smoking rate in non-ban provinces. We then regress this average on the years to/since variable to indicate the trend in smoking rates among those provinces that never implement a ban.
We estimate specifications of the models that allow for polynomials of the explanatory variables and interactions of the policy variables with individual characteristics. We simulate marginal effects (available from the authors) in order to properly account for the non-linear effects of squared or cubed variables and interactions between variables. Standard errors are clustered at the province level. The small number of provinces (23) suggests using alternative calculation of standard errors, such as wild bootstrapping. This procedure did not produce qualitatively different results.
The interactions of the ban with normalized and linear age and income variables suggest that individuals who are older or have lower income (than average) may be more likely to smoke when smoking in public places is restricted. Note, however, that older individuals are significantly less likely to smoke unconditionally. Similarly, men are more likely to smoke than women, unconditionally.
Selection, in this case into having a history of smoking, causes concern about measurement of biased impacts. That is, permanent or time-varying unobservables that may be correlated with previous smoking behavior may also explain current smoking behavior. Unfortunately, we have little information on smoking policy variation in Argentina prior to 2003 and, hence, cannot jointly model whether or not an individual ever smoked nor the age of initiation.
This estimate aligns closely with the 2.0 percentage point reduction in smoking prevalence predicted by the logit model in Section 5.1.
While studies have focused on the health risks associated with duration of smoking rather than intensity of smoking (e.g., Darden, Gilleskie, and Strumpf, 2018), researchers have shown a positive and significant correlation between smoking intensity and risk for smoking-related illnesses. Shields and Wilkins (2013), for example, found such a relationship in their study of smoking intensity and heart disease in Canada.
Figure A1 of the Appendix presents a visualization of each of these three distributions fit to the actual smoking intensity data (conditional on being a current smoker) and plotted against these data; the gamma distribution fits most closely.
Heterogeneous ban effects were insignificant so we report results for average ban effects only.
The marginal effect with OLS on the ln(quantity) is a 5.8 percent increase in the quantity smoked; the marginal effect using GLM with the gamma assumption is an increase of 0.734 cigarettes per day.
The mean age of occasional smokers in Argentina is 36.4 years and, of everyday smokers, is 40.7 years.
The EPH, distributed quarterly since 2003, is a rotating panel dataset that contains household-level data on employment, income, and other general economic indicators.
Guindon et al. (2018) study the effect of tobacco prices on the decision to start smoking in Argentina using individual-level data, noting that periods of high inflation alter the real price impacts.
Barnoya and Glantz (2005) found that the cardiovascular health risks presented by ETS exposure are, on average, 80 to 90 percent as large as those from active smoking.
Recent work suggests that outdoor smoking bans similarly reduce exposure in Korea, with little change in prevalence of smoking (e.g., Ko, 2020).
Contributor Information
Michael A. Catalano, Zucker School of Medicine at Hofstra/Northwell, Hofstra University
Donna B. Gilleskie, Department of Economics, University of North Carolina at Chapel Hill
References
- Adda J and Cornaglia F 2010. “The effect of bans and taxes on passive smoking.” American Economic Journal: Applied Economics 2(1): 1–32. [Google Scholar]
- American Lung Association. “Tobacco Control Milestones.” Accessed April 15, 2021. https://www.lung.org/research/sotc/tobacco-timeline
- Anger S, Kvasnicka M, and Siedler T 2011. “One last puff? Public smoking bans and smoking behavior.” Journal of Health Economics 30(3): 591–601. [DOI] [PubMed] [Google Scholar]
- Barnoya J and Glantz S 2005. “Cardiovascular effects of secondhand smoke, nearly as large as smoking.” Circulation 111(20): 2684–98. [DOI] [PubMed] [Google Scholar]
- Becker GS and Murphy KM 1988. “A theory of rational addiction.” The Journal of Political Economy 96(4): 675–700. [Google Scholar]
- Boes S, Marti J, and Maclean JC 2015. “The impact of smoking bans on smoking and consumer behavior: quasi-experimental evidence from Switzerland.” Health Economics 24(11): 1502–1516. [DOI] [PubMed] [Google Scholar]
- Burton A 2020. “The Impact of Smoking Bans in Bars and Restaurants on Alcohol Consumption, Smoking, and Alcohol-Related Externalities.” Working paper. [Google Scholar]
- Carton T, Darden M, Levendix J, Lee S, and Ricket I (2016). “Comprehensive indoor smoking bans and smoking prevalence: Evidence from the BRFSS.” American Journal of Health Economics 2(4): 535–556. [Google Scholar]
- Chaloupka FJ 1992. “Clean indoor air laws, addiction and cigarette smoking.” Applied Economics 24(2): 193–205. [Google Scholar]
- Darden M, Gilleskie D, and Strumpf K 2018. “Smoking and Mortality: New Evidence from a Long Panel.” International Economic Review 59(2): 1571–1619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeCicca P, Kenkel D, and Liu F 2013a. “Who pays cigarette taxes? The impact of consumer price search.” Review of Economics and Statistics 95(2):516–529. [Google Scholar]
- DeCicca P, Kenkel D, and Liu F 2013b. “Excise tax avoidance: The case of state cigarette taxes.” Journal of Health Economics 32(6): 1130–1141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeCicca P, Kenkel D, and Liu F 2015. “Reservation prices: An economic analysis of cigarette purchases on Indian reservations.” National Tax Journal 68(1):93–120. [Google Scholar]
- DeCicca P, Kenkel D, Lovenheim M, and Nesson E 2018. “The Economics of Smoking Prevention.” in Oxford Research Encyclopedia of Economics and Finance. Oxford University Press. [Google Scholar]
- Ferrante D and Virgolini M 2007. National Risk Factor Survey 2005: main results. Revista Argentina de Cardiología 75(1): 20–29. [Google Scholar]
- Fowler J and Christakis N 2008. “Estimating peer effects on health in social networks.” Journal of Health Economics 27(5): 1400–1405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gilleskie D and Strumpf K 2005. “The behavioral dynamics of youth smoking.” The Journal of Human Resources 40(4): 822–866. [Google Scholar]
- Goodman P, Agnew M, McCaffrey M, Paul G, and Clancy L 2007. “Effects of the Irish smoking ban on respiratory health of bar workers and air quality in Dublin pubs.” American Journal of Respiratory and Critical Care Medicine 175(8): 840–845. [DOI] [PubMed] [Google Scholar]
- Gordon B and Sun B 2015. “A dynamic model of rational addiction: evaluating cigarette taxes.” Marketing Science 34(3): 452–470. [Google Scholar]
- Guindon GE, Paraje GR and Chávez R 2018. “Prices, Inflation, and Smoking Onset: The Case of Argentina.” Economic Inquiry 56(1): 424–445. [Google Scholar]
- Harding M, Leibtag E, and Lovenheim M 2012. “The heterogeneous geographic and socioeconomic incidence of cigarette taxes: Evidence from Nielsen Homescan data.” American Economic Journal: Economic Policy 4(4): 169–198. [Google Scholar]
- Institute of Medicine. Secondhand Smoke Exposure and Cardiovascular Effects: Making Sense of the Evidence. Washington, DC: The National Academies Press, 2010. [PubMed] [Google Scholar]
- Jones AM, Laporte A, Rice N, Zucchelli E, 2015. “Do public smoking bans have an impact on active smoking? Evidence from the UK.” Health Economics 24(2): 175–192. [DOI] [PubMed] [Google Scholar]
- Ko Hansoo. 2020. “The effect of outdoor smoking ban: Evidence from Korea.” Health Economics 29(3): 278–293. [DOI] [PubMed] [Google Scholar]
- Konfino J, Ferrante D, Mejia R, Coxson S, Moran A, Goldman L, and Pérez-Stable EJ 2014. “Impact on cardiovascular disease events of the implementation of Argentina’s national tobacco control law.” Tobacco Control 23(2). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kuehnle D and Wunder C 2017. “The effects of smoking bans on self-assessed health: evidence from Germany.” Health Economics 26(3):321–337. [DOI] [PubMed] [Google Scholar]
- Kvasnicka M, Siedler T, and Ziebarth NR. 2018. “The health effects of smoking bans: Evidence from German hospitalization data.” Health Economics 27(11): 1738–1753. [DOI] [PubMed] [Google Scholar]
- Lewit EM and Coate D. 1982. “The potential for using excise taxes to reduce smoking.” Journal of Health Economics 1(2), 121–145. [DOI] [PubMed] [Google Scholar]
- Matsumoto B 2014. “Lighting the fires: explaining youth smoking initiation and experimentation in the context of a rational addiction model with learning.” Working Paper. [Google Scholar]
- Matsumoto B 2017. “Estimating policy effectiveness in a dynamic context when agents anticipate policy change: the case of indoor smoking bans.” Working Paper, Bureau of Labor Statistics. [Google Scholar]
- Ministerio de Salud de la Nación. Encuesta Nacional de Factores de Riesgo [National Risk Factor Survey], Buenos Aires: Ministerio de Salud de la Nación; 2011. [Google Scholar]
- Ministerio de Salud de la Nación. Encuesta Permanente de Hogares [Permanent Household Survey], Buenos Aires: Ministerio de Salud de la Nación; 2014. [Google Scholar]
- Nakajima R 2007. “Measuring peer effects on youth smoking behaviour.” The Review of Economic Studies 74(3), 897–935. [Google Scholar]
- Navas-Acien A, Peruga A, Breysse P, Zavaleta A, Blanco-Marquizo A, Pitarque R, Acuña M, Jiménez-Reyes K, Colombo V, Gamarra G, Stillman F, and Samet J 2004. “Secondhand Tobacco Smoke in Public Places in Latin America, 2002-2003.” Journal of the American Medical Association 291 (22):2741 –2745. [DOI] [PubMed] [Google Scholar]
- Odermatt R and Stutzer A. 2015. “Smoking bans, cigarette prices and life satisfaction.” Journal of Health Economics 44: 176–194. [DOI] [PubMed] [Google Scholar]
- O’Neill Institute, Fundación Interamericana del Corazón –Argentina [The InterAmerican Heart Foundation -Argentina], and The Foundation for the Development of Sustainable Policy (FUNDEPS). 2011. “Tobacco control in Argentina: advances and pending tasks.” (2011, November). Georgetown Law. [Google Scholar]
- Powell LM, Tauras JA, and Ross H 2005. “The importance of peer effects, cigarette prices and tobacco control policies for youth smoking behavior.” Journal of Health Economics 24(5), 950–968. [DOI] [PubMed] [Google Scholar]
- Rodríguez-Iglesias G, González-Rozada M, Champagne BM, and Schoj V. 2015. “Real price and affordability as challenges for effective tobacco control policies: an analysis for Argentina.” Revista Panamericana de Salud Púiblica 37(2), 98–103. [PubMed] [Google Scholar]
- Schoj V, Sebrié EM, Pizarro ME, Hyland A, and Travers MJ 2010. “Informing effective smokefree policies in Argentina: air quality monitoring study in 15 cities (2007-2009).” Salud publica de Mexico, 52 Suppl 2(0 2), S157–S167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shields M and Wilkins K 2013. “Smoking, smoking cessation and heart disease risk: a 16-year follow-up study.” Health Reports 24(2), 12–22. [PubMed] [Google Scholar]
- Tauras J 2006. “Smoke-free air laws, cigarette prices, and adult cigarette demand.” Economic Inquiry 44(2), 333–342. [Google Scholar]
- Wasserman J, Manning WG, Newhouse JP, and Winkler JD 1991. “The effect of excise taxes and regulations on cigarette smoking.” Journal of Health Economics 10, 43–64. [DOI] [PubMed] [Google Scholar]
- World Health Organization. 2019. “Report on Global Tobacco Epidemic, 2019.” Geneva: World Health Organization. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.