An official website of the United States government
Here's how you know
Official websites use .gov
A
.gov website belongs to an official
government organization in the United States.
Secure .gov websites use HTTPS
A lock (
) or https:// means you've safely
connected to the .gov website. Share sensitive
information only on official, secure websites.
As a library, NLM provides access to scientific literature. Inclusion in an NLM database does not imply endorsement of, or agreement with,
the contents by NLM or the National Institutes of Health.
Learn more:
PMC Disclaimer
|
PMC Copyright Notice
Outcomes of patients who participate in randomized controlled trials compared to similar patients receiving similar interventions who do not participate
Some people believe that patients who take part in randomised controlled trials (RCTs) face risks that they would not face if they opted for non‐trial treatment. Others think that trial participation is beneficial and the best way to ensure access to the most up‐to‐date physicians and treatments. This is an updated version of the original Cochrane review published in Issue 1, 2005.
Objectives
To assess the effects of patient participation in RCTs ('trial effects') independent both of the effects of the clinical treatments being compared ('treatment effects') and any differences between patients who participated in RCTs and those who did not. We aimed to compare similar patients receiving similar treatment inside and outside of RCTs.
Search methods
In March 2007, we searched The Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, EMBASE, The Cochrane Methodology Register, SciSearch and PsycINFO for potentially relevant studies. Our search yielded 7586 new references. In addition, we reviewed the reference lists of relevant articles.
Selection criteria
Randomized studies and cohort studies with data on clinical outcomes of RCT participants and similar patients who received similar treatment outside of RCTs.
Data collection and analysis
At least two review authors independently assessed studies for inclusion, assessed study quality and extracted data.
Main results
We identified 30 new non‐randomized cohort studies (45 comparisons): no new RCTs were found. This update now includes five RCTs (yielding 6 comparisons) and 80 non‐randomized cohort studies (130 comparisons), with 86,640 patients treated in RCTs and 57,205 patients treated outside RCTs. In the randomised studies, patients were invited to participate in an RCT or not; these comparisons provided limited information because of small sample sizes (a total of 412 patients) and the nature of the questions they addressed. When the results of RCTs and non‐randomized cohorts that reported dichotomous outcomes were combined, there were 98 comparisons; there was also heterogeneity (P < 0.00001, I2 = 42.2%) between studies. No statistical significant differences were found for 85 of the 98 comparisons. Eight comparisons reported statistically significant better outcomes for patients treated within RCTs, and five comparisons reported statistically significant worse outcomes for patients treated within RCTs. There was significant heterogeneity (P < 0.00001, I2 = 58.2%) among the 38 continuous outcome comparisons. No statistically significant differences were found for 30 of the 38 comparisons. Three comparisons reported statistically significant better outcomes for patients treated within RCTs, and five comparisons reported statistically significant worse outcomes for patients treated within RCTs.
Authors' conclusions
This review indicates that participation in RCTs is associated with similar outcomes to receiving the same treatment outside RCTs. These results challenge the assertion that the results of RCTs are not applicable to usual practice.
Plain language summary
Outcomes of patients who participate in randomized controlled trials compared to similar patients receiving similar interventions who do not participate
This updated review assessed whether there were harmful or beneficial effects from participating in randomized controlled trials (RCTs). The outcomes of patients who participated in RCTs were compared with outcomes of patients who were eligible for the trial and received similar clinical interventions, but did not participate. Comparisons were included both of 'experimental' treatment inside and outside of RCT and of 'control' treatment comparisons. On average, the outcomes of patients participating and not participating in RCTs were similar, suggesting that participation in RCTs, independent of the effects of the clinical interventions being compared, is likely to be comparable.
Background
The efforts of trialists, ethics committees, and funding agencies to inform potential participants (for example, patients) of the risks of participating in randomized controlled trials (RCTs) appear to be motivated in part by the 'conventional wisdom' that those who participate in RCTs face special risks that they would not face if they declined to participate and received their health care in the usual way. Thus we see statements describing trial participants as being 'conscripted' to 'sacrifice' themselves in the service of the 'collective' ‐ 'guinea pigs' to be sacrificed for the benefit of future patients (Sackett 2001). A journal editor expressed her view thus: "If the ethical commitment to protect the participants from the risks of participating in RCTs "is attenuated, even for so good a cause as benefits to future patients, the implicit assumptions of the doctor‐patient relationship are violated" (Angell 1984). And the dean of a medical school took up this argument: "The risk of such attenuation by the RCT is great" (Hellman 1991).
Conversely, some researchers and patients believe that participation in RCTs is beneficial, as well as being the most equitable and ethical way to compare the effects of treatments when there is uncertainty. Some patient advocates, especially those with HIV and cancer, demand access to clinical trials.
Anecdotal evidence is sometimes cited to support both of these opposing viewpoints. More often, assumptions are made without reference to empirical evidence. Previous reviews of the evidence of harmful or beneficial effects of participating in RCTs have been limited by the difficulty in identifying and interpreting the available evidence, which, because it comes almost entirely from non‐randomized cohort studies, is subject to the same biases as non‐randomized cohort studies of clinical interventions.
There are now at least four published reviews of evidence that might help us resolve this disagreement (Stiller 1994; Braunholtz 2001; ECRI 2002; Peppercorn 2004), but their conclusions have varied. Peppercorn and colleagues concluded that the glass is half or more empty: "Despite the widespread belief that enrolment in clinical trials leads to improved outcomes among cancer patients, there are insufficient data to conclude that such a trial effect exists." On the other hand, Braunholtz et al concluded that the glass is at least half full: "While the evidence is not conclusive, it is more likely that clinical trials have a positive rather than a negative effect on the outcome of patients."
Previous reviews have compared all patients treated within trials with all patients treated outside trials, regardless of any differences in the clinical intervention received or differences in patient populations. This previous approach means that we can not know if any differences observed reflect the effects of participating in RCTs (a trial effect), differences in the clinical interventions used within and outside RCTs (treatment effects), or an effect of differences between the patients who participate in RCTs and those who do not.
In this updated review (originally published in Issue 1, 2005) we have built on earlier work by systematically searching for relevant studies, critically appraising them, and abstracting and analysing data for comparisons that can inform judgements about the potential beneficial and harmful effects of participating in RCTs. We will periodically update the resulting review as new data become available and in response to feedback.
Objectives
The aim of this review is to address the following question: Do the outcomes of patients who participate in randomized controlled trials differ from those of similar patients, treated similarly, who do not participate? We attempted to control for differences in the clinical interventions that were received by only including analyses that compare patients receiving the same clinical intervention within and outside RCTs. That is, experimental treatment inside an RCT versus similar treatment outside of the RCT, or the control intervention inside an RCT versus similar control treatment outside of the RCT.
This question is addressed through comparisons of participants in RCTs with:
1. patients who choose not to participate, including:
1a. eligible patients who refuse to participate for any reason;
1b. eligible patients who refuse to participate because of a strong preference for one of the interventions being evaluated;
1c. participants in patient preference trials who choose not to be randomized because of a strong preference for one of the interventions being evaluated.
2. patients not invited to participate, including:
2a. uninvited eligible patients of participating clinicians;
2b. eligible patients of non‐participating clinicians.
3. patients randomized to be invited/informed that they are participating in a study versus those not invited/informed (including Zelen design where patients are randomized before consent, and then only those who are randomized to the experimental treatment are asked to consent to participate).
4. eligible patients who do not participate and do not fit into one of the above categories. This might include, for example a mixed group where it is not possible to obtain sufficient data to categorise individuals, controls from the same or nearby hospitals that are captured in large health care databases, area‐wide population controls, 'not‐quite‐eligible' patients at the same centres, 'administratively' not eligible patients.
Methods
Criteria for considering studies for this review
Types of studies
Cohort studies that include at least one of the comparisons specified above. For comparisons 2a, 2b and 4 we included any RCTs that were found in which participation or the possibility of participating in a clinical trial was randomly allocated, including participation in N of 1 trials (individualised and controlled 'trial of therapy') and cluster randomized trials.
Types of data
We collected data as reported by investigators for comparisons using concurrent controls. We also attempted to collect or calculate relative risks or hazard ratios.
Types of methods
We included comparisons of patient participation in an RCT versus non‐participation.
Types of outcome measures
The main outcome measures of interest were mortality, morbidity (excluding surrogate outcome measures), and clinically important changes in outcomes measured on continuous scales (such as self reported pain, quality of life and function).
Search methods for identification of studies
In March 2007, we searched:
MEDLINE, the search strategy is presented in Appendix 1;
EMBASE, the search strategy is presented in Appendix 2;
The Cochrane Central Register of Controlled Trials (CENTRAL), The Cochrane Library Issue 1 2007, the search strategy is shown in Appendix 3;
PsycInfo, the search strategy is presented in Appendix 4;
We checked the reference lists of the relevant articles that we retrieved. We followed up on abstracts of studies by attempting to find a full report by searching in PubMed.
Data collection and analysis
Two review authors independently assessed all retrieved citations. Any study that either review author considered potentially relevant was retrieved.
Two review authors independently assessed the relevance of all retrieved articles using the eligibility criteria specified above. Disagreements were resolved by discussion. A third review author was consulted about any disagreements that could not be resolved. We have listed references to all those studies for which there were disagreements or initial uncertainties in the Characteristics of excluded studies table, together with the reasons for our decisions to exclude them.
Methodological quality
Two review authors using the following criteria independently assessed the validity of the comparisons made in the included studies:
Selection bias
This criterion was scored as:
Met = concealed random allocation to participate or not in a clinical trial;
Partially met = control for one or more prognostic factors (we noted how many prognostic factors have been controlled for);
No imbalance = no control for prognostic factors because there was no imbalance;
Not met = imbalance in prognostic factors and failure to control for prognostic factors;
Unclear = sufficient information could not be obtained.
Detection bias
This criterion was scored as:
Met = outcomes measured in the same way in both participants and non‐participants;
Partially met = similar standards of measurement for participants and non‐participants;
Not met = different standards of measurement for participants and non‐participants;
Unclear = sufficient information could not be obtained.
Exclusion bias
We recorded the number of losses to follow up for each group (loss/total):
Loss in RCT treatment group;
Loss in RCT control group;
Loss in non‐ participants treatment group;
Loss in non‐ participants control group;
then grouped them for analysis into:
No losses to follow up;
1% to 20% losses to follow up;
>20% losses to follow up;
unclear if there were any losses to follow up.
Differences in care
Differences in the care provided to participating and non‐participating patients were recorded as a possible explanation for differences in outcomes. We regarded this as reflecting an effect of participating in a trial rather than as a 'performance' bias. Differences in the care provided might be due to differences in adherence to a protocol by participating clinicians; baseline differences between clinicians who participate and do not participate in clinical trials; or a Hawthorne effect (changes in behaviour due to being observed).
We also regarded the possible impact of psychologically mediated effects due to the informed consent process as a possible explanation for differences in outcomes rather than as a bias.
We attempted to control for differences in the clinical interventions received by including only those analyses comparing patients receiving similar treatments.
Because they might explain differences in outcomes, we recorded whether the investigators had noted changes in behaviour attributed to being observed, or different expectations, attributable to the informed consent process.
In addition to recording our assessments of the methodological quality of the included studies, we collected data describing relevant details of the included studies including the study design, types of participating patients, the types of participating clinicians, the clinical interventions that were evaluated and the main outcome measures reported.
Two review authors completed data collection forms independently for all included studies. These were compared and discrepancies were resolved by discussion, including a third review author, when necessary.
Analysis
We prepared tables summarising the results of all the relevant comparisons included, grouped as described under 'Objectives'. Additionally, comparisons were also grouped based on the risk of selection, detection and exclusion bias into controlled comparisons, partially controlled comparisons and poorly controlled comparisons. The main outcome for each of the included studies was collected, an additional outcome group included mortality only. We have reported the main outcome measures in these summary tables. For each result we recorded or calculated, if possible, a relative risk (RR) or hazard ratio with a 95% confidence interval, using adjusted estimates when these were available. In order to summarise all the dichotomous results in one summary table, we took the natural logarithm of the unadjusted RR and calculated the associated SE. For similar comparisons and outcomes we conducted a chi‐square test of heterogeneity. In order to calculate a pooled estimate for continuous outcomes, the results from individual studies were standardized (in order to return them to the same metric) and a standardized mean difference (SMD) was used to calculate the pooled estimate. For relative risk analysis we used the Mantel‐Haenszel approach available in RevMan. We calculated summary statistics using a random‐effect model using the inverse of the variance for each study to weigh its treatment effect in the pooled analysis. We did not calculate a pooled estimate if statistically significant heterogeneity was found (defined as P < 0.10). For clinically diverse comparisons or statistically heterogeneous results we described the variation in the estimates and key explanatory factors, if possible relating the explanatory factors to observed differences in estimates of the effects of participation. The main explanatory factors that we considered were:
· the risk of selection bias;
· the risk of detection bias;
· the risk of exclusion bias;
· differences in the care provided to patients (including differences between participating and non‐participating clinicians, adherence to a protocol by participating clinicians, and a possible Hawthorne effect);
· a possible effect due to the informed consent process;
· differences in the need for skills or experience (e.g. trials of surgical procedures versus drug trials).
We described the number of comparisons and the total number of patients compared from different clinical areas (e.g. cardiology and oncology) and the consistency of the evidence across different clinical areas.
Results
Description of studies
The update search identified 7586 potentially relevant references. After an initial screen of titles and abstracts, full articles were obtained for 231 of these. Thirty reported relevant data and a further 51 suggested to us that the investigators might have relevant data.
We identified 30 new non‐randomized cohort studies (45 comparisons), no new RCTs were found. This update now includes five RCTs (yielding six comparisons) and 80 non‐randomized cohort studies (130 comparisons), with 86,640 patients treated in RCTs and 57205 patients treated outside RCTs. The included studies are described in the Characteristics of included studies table. In each of five randomized studies with a total of 412 patients, investigators randomized patients to be invited to participate in an RCT or not. Based on published data alone, we could include 45 new comparisons. We have listed 51 studies as 'awaiting assessment' because they cannot currently be included or excluded in this review based on the information available to us.
In 38 studies (with 61 comparisons), patients in RCTs were compared with patients who refused to participate in RCTs without a specified reason. In 20 studies (with 34 comparisons), patients in RCTs were compared with patients who refused to participate in RCTs because of treatment preferences. In 11 partially randomized patient preference studies (with 22 comparisons), patients randomized to treatment were compared with patients who chose not to be randomized because of a treatment preference. In six studies (with nine comparisons), patients treated in RCTs were compared with patients who were not invited to participate in the RCTs. In two studies (with two comparisons), patients treated within the context of an RCT were compared with patients treated by other clinicians who did not enter any of their patients to the trial. In one study (with one comparison) non‐randomized patients were not invited to the trial because of administrative error or the researcher was absent. In one study (with one comparison) the reason for not including the eligible non‐randomized patients in trial is unclear, and finally, in one study (with one comparison) eligible non‐randomized patients were given the active treatment to give the clinicians training.
Patients received the following clinical interventions: surgery or other procedures (33 comparisons), drugs (28 comparisons), radiotherapy (15 comparisons), counselling or education (nine comparisons), usual care (45 comparisons), and active monitoring/ watchful waiting (six comparisons).
There were comparisons in the following clinical specialties: oncology (31 comparisons), cardiology (22 comparisons), other internal medicine subspecialties (27 comparisons), obstetrics and gynaecology (29 comparisons), psychology or drug abuse (15 comparisons), and paediatrics (12 comparisons).
Each comparison is represented using the main outcome as reported by the investigators, and this main outcome is noted in the Characteristics of included studies table.
Mortality was reported in 21 studies (with 37 comparisons). In two of these studies (with nine comparisons), mortality was not the main outcome, from these two studies we used the reported main outcome in the summary analysis and the mortality results in the mortality analysis only.
Risk of bias in included studies
We categorised six randomized comparisons as 'well controlled', 42 comparisons that reported no imbalance or controlled for prognostic factors as 'controlled', 29 comparisons that reported one or two differences as 'partially controlled', and 59 comparisons that reported several statistically significant differences or which did not report characteristics of the patients within and outside the RCTs as 'poorly controlled'.
Outcomes were measured in the same way within and outside the RCTs in 111 comparisons, similarly in twelve comparisons, and differently or not reported in 10 comparisons.
No patients were reported as having been excluded in 55 comparisons. In 49 comparisons, between one and 20% of patients were lost to follow up, and over 20% of patients were lost to follow up in 16 comparisons. It was unclear if there were any losses to follow up in 16 comparisons.
Effect of methods
Randomized studies
The five studies (six comparisons) in which patients were randomized to be invited to participate in an RCT or not (Table 1) provide limited information because of their small sample sizes and the nature of the questions they addressed.
1. Patients randomized to trial participation or not.
Study id
Patients
Outcome measure
Inside trial (n)
Outside trial (n)
RR or SMD
Bergmann 1994
Oncology patients
Pain score on a 100 point scale after given pain killer
mean ‐22 (31), n=18
mean ‐5 (34), n=25
SMD ‐0.5 (‐1.12 to 0.11)
Cooper 1997a
women w/heavy menstrual bleeding
Lack of satisfaction with surgical resection treatment
23 of 93
6 of 21
RR 0.87 (0.40 to 1.86)
Cooper 1997b
Women w/heavy menstrual bleeding
Lack of satisfaction with medical treatment
69 of 94
11 of 19
RR 1.27 (0.85 to 1.90)
Dahan 1986
Insomnia patients
# spontaneously reported side effects after placebo pills
4 of 30
none of 30
RR 9.0 (0.51 to 160.2)
Mahon 1996
Patients with irreversible chronic airflow limitation
Change in 6 min walk distance (m)
12 (29) m, n=12
3 (53) m, n=9
SMD‐0.21 (‐1.08 to 0.66)
Mahon 1999
Patients with irreversible chronic airflow limitation
Two studies randomized a total of 82 patients to N of 1 trials compared with standard practice (Mahon 1996; Mahon 1999).
One study with 60 patients measured spontaneously reported side effects by patients informed that they were in an RCT compared with those who were not informed (Dahan 1986).
One study with 227 patients reported satisfaction among patients randomized to an RCT compared with patients randomized to a patient preference trial who had a treatment preference (Cooper 1997a; Cooper 1997b).
The fifth study with 43 patients reported pain reduction among patients randomized to an RCT compared with patients who were not invited to participate (Bergmann 1994).
None of these studies found statistically significant differences in outcomes between patients treated within and outside RCTs. Because of the heterogeneity of questions addressed in these studies, we did not consider it appropriate to make a quantitative synthesis of their results.
Non‐randomized cohort studies
The 80 non‐randomized cohort studies (130 comparisons) included a total of 86,362 patients participating in RCTs compared with 57,071 patients treated outside RCTs. Ninety‐eight comparisons used dichotomous outcomes, 12 of them with adjusted results, 38 comparisons were of continuous outcomes.
Main outcome (dichotomous)
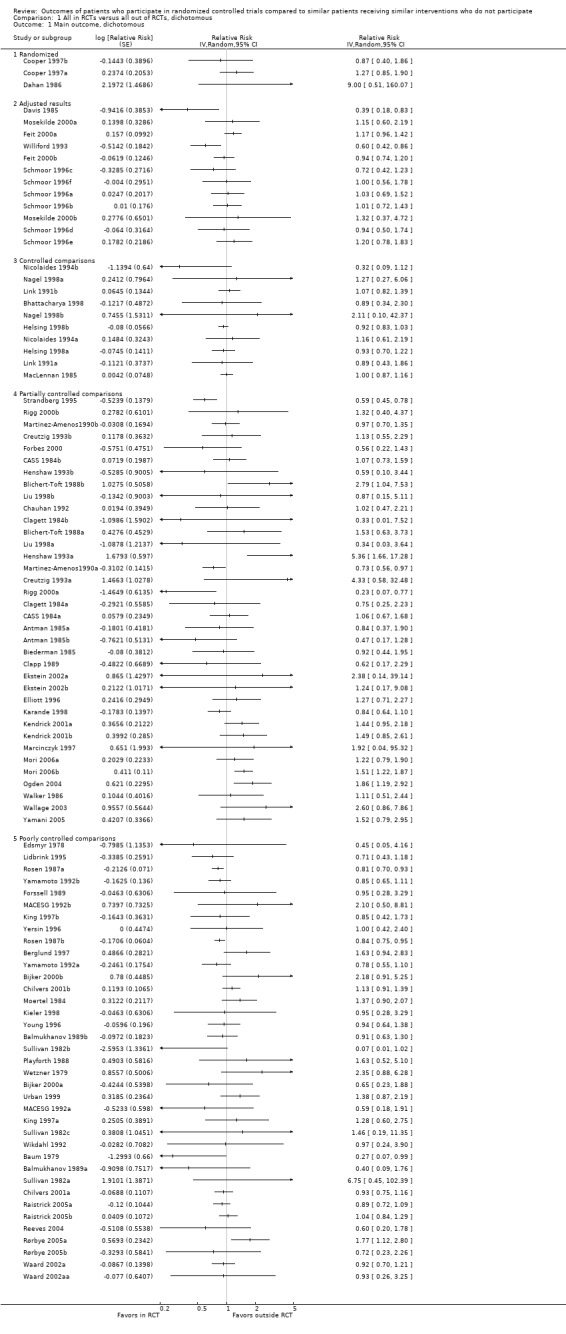
The results of all the comparisons in which dichotomous outcomes were used are summarised and presented in Analysis 1.1. There is statistically significant heterogeneity (overall P < 0.00001, and overall I2 = 42.2%). The summary estimate for the comparisons with dichotomous outcomes is not presented, the confidence interval around the pooled result ranged from 0.93 to 1.06.
Comparison 1 All in RCTs versus all out of RCTs, dichotomous, Outcome 1 Main outcome, dichotomous.
In 85 of the 98 comparisons, no statistically significant differences in outcomes were found. The results of the 13 comparisons (two adjusted comparisons and 11 unadjusted comparisons) in which statistically significant differences were found are as follows.
The two adjusted comparisons reported statistically significantly better outcomes for patients treated in RCTs than similar patients receiving similar treatments outside RCTs. One partially controlled adjusted comparison found that lung cancer patients in an RCT had a lower risk of dying inside RCT (RR 0.39, 95% CI 0.18 to 0.83) (Davis 1985). One poorly controlled comparison that adjusted for treatment (total parenteral nutrition or not) found that malnourished surgical patients in the RCT had a lower risk of complications (RR 0.60, 95% CI 0.42 to 0.86) (Williford 1993). Six unadjusted comparisons reported statistically significantly better outcomes for patients treated in RCTs than similar patients receiving similar treatments outside RCTs. Three were partially controlled and found better blood pressure control inside the RCT (RR 0.73, 95% CI 0.56 to 0.97) (Martinez‐Amenos1990a), a lower 18 year mortality after a health check without further intervention (RR 0.59, 95% CI 0.45 to 0.78) (Strandberg 1995) and a lower 30 day mortality after surgery in high risk patients (RR 0.23, 95% CI 0.07 to 0.77) (Rigg 2000a). Three poorly controlled comparisons found lower relapse rates for lymphocytic leukaemia in children receiving maintenance chemotherapy (RR 0.27, 95% CI 0.07 to 0.99) (Baum 1979), and more successful pregnancies after oocyte retrieval with different anaesthetics (RR 0.81, 95% CI 0.70 to 0.93 and RR 0.84, CI 0.75 to 0.95) (Rosen 1987a; Rosen 1987b).
Five unadjusted studies reported statistically significant better outcomes outside RCTs. Four were partially controlled comparisons. One found a higher risk of breast cancer recurrence among women who had received mastectomies within an RCT compared with women similarly treated outside the RCT (RR 2.79, 95% CI 1.04 to 7.53) (Blichert‐Toft 1988b). One found that medical abortion was more acceptable to women in a preference trial than in the RCT (RR 5.36, 95% CI 1.66 to 17.28) (Henshaw 1993a). One found better satisfaction with the use of nasal tube for endoscopy outside of RCT than inside (RR 1.51, 95% CI 1.22 to 1.87 )(Mori 2006b), one found greater rate of success for treating plantar fascitis (foot disorder) with sham electrohydraulic high‐energy shock‐wave treatment outside of the RCT than inside the RCT (RR 1.86, 95% CI 1.19 to 2.92) (Ogden 2004).
One poorly controlled unadjusted comparison reported significantly higher satisfaction among women with medical abortion outside of an RCT than women who received medical abortion inside an RCT (RR 1.77, 95% CI 1.12 to 2.80) (Rørbye 2005a).
Main outcome (continuous)
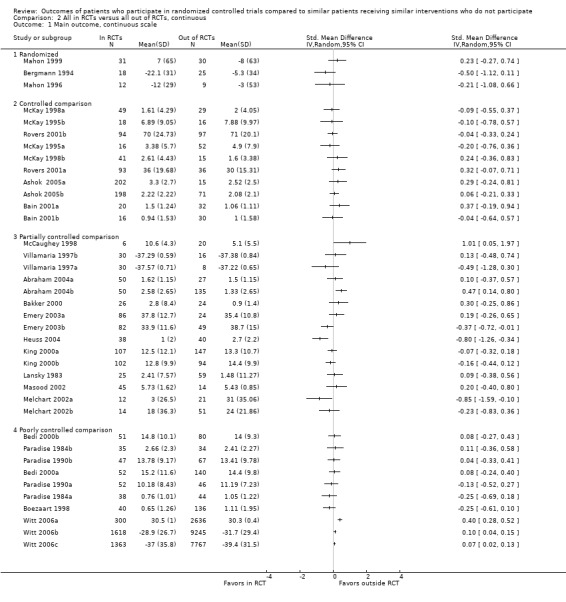
The results of the 38 comparisons in which continuous outcomes were used are presented in Analysis 2.1. There was moderate heterogeneity (overall P < 0.00001, overall I2 = 58.2%). The summary estimate for the comparisons with continuous outcomes is not presented, the confidence interval around the pooled SMD ranged from ‐0.05 to 0.11.
Comparison 2 All in RCTs versus all out of RCTs, continuous, Outcome 1 Main outcome, continuous scale.
In 30 of the 38 comparisons, no statistically significant differences in outcomes were found. The results of the eight comparisons (five partially and three poorly controlled unadjusted comparisons) in which statistically significant results were found were as follows.
Three partially controlled comparisons reported statistically significant better outcomes for patients treated in RCT than similar patients receiving similar treatment outside of the RCT. One study with two comparisons found that both couples who received pre‐IVF counselling and couples who did not receive additional counselling pre‐IVF in the RCT had lower anxiety than similar couples given or not given pre‐IVF counselling outside of the RCT (SMD ‐0.37, 95% CI ‐0.72 to ‐0.01) (Emery 2003a), (SMD ‐0.80, 95% CI ‐1.26 to ‐0.34) (Emery 2003b). In one study of endoscopy patients who were given sedation inside RCT, they scored less troublesomeness than the patients who were sedated outside of the RCT (SMD ‐0.85, 95% CI ‐1.59 to ‐0.10) (Melchart 2002a).
Two partially controlled comparisons and three poorly controlled comparisons found statistically significant worse outcomes in patients treated in RCTs. In one study the patients found the procedure more troublesome when given a placebo during endoscopy inside the RCT compared with similar patients given nothing during endoscopy outside the RCT (SMD 0.47, 95% CI 0.14 to 0.80) (Abraham 2004b). In one study of young girls who were given growth hormone, they grew more outside the RCT than those who were treated inside the RCT (SMD 1.01, 95% CI 0.05 to 1.97) (McCaughey 1998). In three large, poorly controlled unadjusted studies looking at the effect of acupuncture for osteoarthritis of the knee or hip, or chronic low back pain, or chronic neck pain patients reported less pain, higher reduction in pain and lower WOMAC score when treated with acupuncture outside RCT than similar patients treated with acupuncture in RCT (osteoarthritis patients, SMD 0.40, 95% CI 0.28 to 0.52) (Witt 2006a) (chronic low back pain, SMD 0.10, 95% CI 0.04 to 0.15) (Witt 2006b) (chronic neck pain, SMD 0.07, 95% CI 0.02 to 0.13) (Witt 2006c). The three acupuncture trials included 22,929 patients and accounted for 79% weight of the total weight of continuous data analysis.
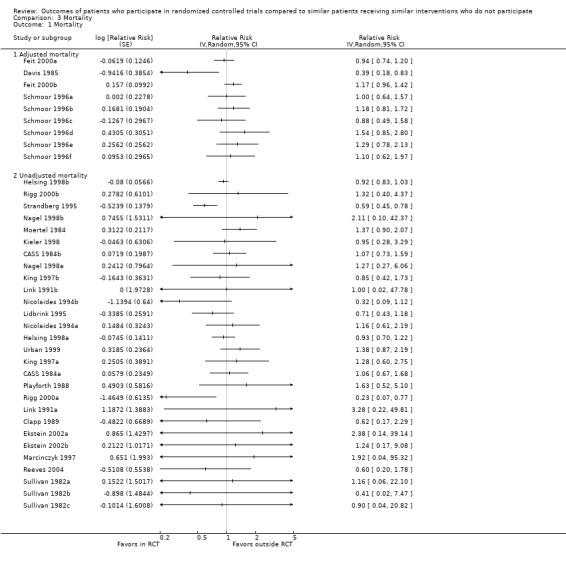
Mortality; subgroup analysis
In twenty‐one studies with 37 comparisons, mortality was reported as an outcome. The mortality results are summarised and presented in Analysis 3.1. There is statistically significant heterogeneity (overall P < 0.03, and overall I2 = 33.7%). The summary estimate for the mortality comparisons is not presented, the confidence interval around the pooled estimate ranged from 0.88 to 1.08.
In 34 of the 37 comparisons, no statistically significant differences in outcomes were found. Three comparisons (one adjusted comparison and two unadjusted comparisons) in which statistically significant differences were found are as follows.
One adjusted mortality comparison found a statistically significant lower risk of dying for patients treated within RCTs (Davis 1985).
Two unadjusted mortality comparisons found a statistically significant lower risk of dying for patients treated within RCTs (Rigg 2000a; Strandberg 1995).
None of the subgroup analyses that we conducted helped to explain the observed heterogeneity in the results of the comparisons we included. We conducted separate analyses for the different types of patients treated outside RCTs (patients who refused to participate in RCTs without a specified reason, patients who refused to participate in an RCT because of a treatment preference, etc.), different types of treatments (surgery or procedures, drugs, etc.), different clinical areas (oncology, cardiology, etc.), and differences in study quality (selection bias, detection bias, and exclusion bias). These subgroup analyses are available from us on request.
Due to insufficient information, we were unable to conduct subgroup analyses examining differences in the clinical care provided to patients or differences in the informed consent process.
Discussion
Our review does not provide strong evidence of either a harmful or a beneficial trial effect. As we found significant heterogeneity among the results of the included comparisons, which we were not able to explain, these overall findings may not apply to particular circumstances yet to be identified.
The five randomized studies that we found comparing outcomes within and outside RCTs provide limited evidence, but they do demonstrate that it is possible to address questions about the effects of participating in RCTs using randomized designs. Interpretation of the 80 non‐randomized cohort studies is limited by the quality and size of the comparisons and the wide variations in participants, clinical interventions and outcomes in these comparisons. Most of the 130 non‐randomized cohort comparisons did not yield statistically significant differences, 11 found better outcomes in RCTs and ten found better outcomes outside RCTs.
Do the outcomes of patients who participate in RCTs differ from those of similar patients who do not participate? Three previous reviews have addressed this question. Braunholtz 2001 identified 14 articles reporting data from 21 trials, and concluded that, if anything, randomized trials tend to have beneficial effects rather than harmful effects on the patients who participate in them.
Peppercorn included seven of the 14 articles in the Braunholtz review and an additional 17 (Peppercorn 2004). However, only eight of their studies compared trial patients with non‐trial patients who met the same eligibility criteria, and it is only possible to separate treatment effects from trial effects in three of these. As Peppercorn et al. classified studies as 'positive' ("outcomes among trial patients were better with P<0.05") and 'negative (P>0.05), they were unable to distinguish studies that exclude any important trial benefit ('true‐negatives') from 'indeterminate' studies that are simply too small to detect either important benefit or important harm.
ECRI 2002 (Emergency Care Research Institute) found 10 comparisons of survival or quality of life between patients treated within and outside RCTs of treatments for life threatening illnesses (eight were cancer treatments). They concluded, "some evidence shows that patients in phase II/III trials survive longer than similar patients who are not in trials. One cannot have great confidence in these results, however, due to the small evidence base."
Our review differs from previous reviews in a number of ways, including the scope, the comprehensiveness of the search, the analysis and, importantly, the question that we asked: Do the outcomes of patients who participate in RCTs differ from those of similar patients receiving similar treatments who do not participate? Our results suggest that on average they do not.
An important corollary of this finding is that it counters the suggestions that the results of RCTs cannot be applied to usual clinical practice. Extrapolations of the results from RCTs to patients who are different to the patients who participated in the RCT, or to interventions that are different to those of the RCT, are different issues.
In summary, all of the three previous reviews and our review (now including results from over 140,000 patients) suggest that participating in a randomised controlled trial is likely to result in similar outcomes to having similar treatment outside of the trial. It is likely that there are more relevant studies than those included in this review, as indicated by the number of studies awaiting assessment, and the difficulty we and others have encountered searching for these studies in MEDLINE and other bibliographic databases. Additionally, we did not search dissertation data bases. Twelve of the 30 new studies included in update were published before the previous search data.
What we have attempted in this review and update has been to isolate the 'trial effect' of participating in RCTs. This is a question of effect where only well designed and conducted RCTs will provide conclusive answer. We have only five small randomised controlled trials where patients have been randomised to be asked to participate in a RCT or not. Due to the sparseness of data, we have in an attempt to further inform the issue of trial effect, included cohorts. We have attempted to only compare similar patients inside and outside of the RCTs, and we have attempted to only compare similar interventions inside and outside of the RCTs. Even so, these cohorts are non‐randomized studies and vulnerable to bias. There is an increasing focus on the importance of following patients outside of trials and the number of cohorts that are available for inclusion seems to be increasing. This is a welcome improvement; however, we think that we have now reached the level of information for this particular issue where only new RCTs is likely to give us more confidence in the conclusion. Therefore, updates of this review will only consider RCTs.
It is important to protect people from unnecessary risks and harms and it is essential that people are informed and warned of the risk to which they may be exposed, both in clinical trials and in routine care. When there is collective uncertainty about the effects of clinical interventions, randomised trials provide the best means of resolving that uncertainty (Kunz 2002).
Patients who are given the option of participating in a clinical trial should routinely be told what is known about the potential benefits and harms of the interventions being compared in the trial as well as whatever other options they have.
Authors' conclusions
Implication for methodological research.
Randomized comparisons with adequate sample sizes are needed to provide reliable evidence of potential differences in outcomes of patients who participate in randomised trials compared with similar patients receiving similar interventions who do not participate.
Protocol first published: Issue 4, 2001
Review first published: Issue 1, 2005
Date
Event
Description
15 May 2008
New citation required but conclusions have not changed
The list of authors has changed.
15 May 2008
New search has been performed
This review has been updated (new search in March 2007) from a previously published review (Vist 2005). Thirty new studies with 45 comparisons have been included in this update. A total of 85 studies with 136 comparisons are included. These studies report on 86,640 patients who have been randomised to treatment within RCTs compared with 57,205 similar patients who received similar treatment outside of the trial.
We would like to thank Dave Sackett for initiating the effort that has resulted in this review, for his contributions to the protocol and for his generous support. We would like to thank Marit Johansen for the search strategy. We would like to thank Kåre Birger Hagen, PJ Devereraux and Doris Tove Kristoffersen for their contributions to the first (previous) version of this review.
We would like to thank the following for providing additional information about their studies: Albert SM, Antman K, Barrett BJ, Bennett JM, Black SB, Brehm SS, Berglund G, Bergmann JF, Bijker N, Blichert‐Toft M, Boros L, Cairncross JG, Carroll KM, Chadwick DW, Chauhan SP, Chilvers C, Clagett GP, Cohen CJ, Collins K, Cooper JS, Cooper KG, Cottin V, Creutzig U, Davis S, DiMagno EP, van Eys J, Ferrone PJ, Forbes GM, Frisell J, Glimelius B, Gluud C, Guillemin F, Hauth JC, Helsing M, Hellberg D, Henderson JM, Hutter AM, Jensen LP, Jonker JJC, Karrison T, King SB, Kjar D, Kronmal RA, Licht RW, Lidbrink E, Liu WF, Madsen JK, Mahon JL, Malangoni MA, Marcocci C, McKay JR, Mourits MP, Moynihan C, Mundy GR, Naylor CD, Neuwirth MG, O'Fallon JR, Paradise JL, Pinchera A, Playforth MJ, Pollock AV, Rokke PD, Rosen MA, Rovers MM, Rychtarik RG, Schmidt B, Schmoor C, Sha BE, Shelhamer JH, Stegmayr BG, Stiller CA, Stone JM, Takolander R, Tannock IF, Vestergaard P, Ward B, Weijer C, Weisdorf DJ, Wyse DG, Yersin B, Yu VL.
Appendices
Appendix 1. MEDLINE search strategy
Randomized Controlled Trials/
Random Allocation/
random$.tw.
or/1‐3
(outside adj3 (trial? or randomi?ed or rct? or program)).tw.
((nonentry or non entry or nonenter$ or non enter$ or "not enter$" or nonenrol$ or non enrol$ or "not enrol$" or nonparticip$ or non particip$ or "not particip$") adj3 (trial? or randomi?ed or rct?)).tw.
((nonentry or non entry or nonenter$ or non enter$ or "not enter$" or nonenrol$ or non enrol$ or "not enrol$" or nonparticip$ or non particip$ or "not particip$") adj3 patient?).tw.
8. ((nonrandom$ or non random$) adj3 (patient? or group? or case? or serie? or study or studies or trial?)).tw.
((nonentry or non entry or nonenter$ or non enter$ or "not enter$" or nonenrol$ or non enrol$ or "not enrol$" or nonparticip$ or non particip$ or "not particip$") adj3 patient?).tw.
8. ((nonrandom$ or non random$) adj3 (patient? or group? or case? or serie? or study or studies or trial?)).tw.
(exclud$ adj3 randomi?ation).tw.
((non participant? or nonparticipant?) adj3 group?).tw.
(patient? adj3 prefer$).tw.
((treatment or method?) adj3 prefer$).tw.
(treatment adj3 (select$ or choose or chose or chosen or choice)).tw.
((own or patient? or by) adj choice).tw.
((standard or usual) adj practice).tw.
((refus$ or decline$) adj3 (participat$ or random$)).tw.
((non or "not" or lack$ or withh$ or without or refus$ or decline$) adj3 consent).tw.
(outside adj3 (trial? or randomi?ed or rct? or program)).tw.
((nonentry or non entry or nonenter$ or non enter$ or "not enter$" or nonenrol$ or non enrol$ or "not enrol$" or nonparticip$ or non particip$ or "not particip$") adj3 (trial? or randomi?ed or rct?)).tw.
((nonentry or non entry or nonenter$ or non enter$ or "not enter$" or nonenrol$ or non enrol$ or "not enrol$" or nonparticip$ or non particip$ or "not particip$") adj3 patient?).tw.
((nonrandom$ or non random$) adj3 (patient? or group? or case? or serie? or study or studies or trial?)).tw.
(exclud$ adj3 randomi?ation).tw.
((non participant? or nonparticipant?) adj3 group?).tw.
(patient? adj3 prefer$).tw.
((treatment or method?) adj3 prefer$).tw.
(treatment adj3 (select$ or choose or chose or chosen or choice)).tw.
((own or patient? or by) adj choice).tw.
((standard or usual) adj practice).tw.
((refus$ or decline$) adj3 (participat$ or random$)).tw.
((non or "not" or lack$ or withh$ or without or refus$ or decline$) adj3 consent).tw.
MeSH descriptor Randomized Controlled Trials, this term only
MeSH descriptor Random Allocation, this term only
(random*):ti or (random*):ab
(outside NEAR/3 (trial* or randomized or randomised or rct* or program)):ti or (outside NEAR/3 (trial* or randomized or randomised or rct* or program)):ab
(nonentry or non NEXT entry or nonenter* or non NEXT enter* or not NEXT enter* or nonenrol* or non NEXT enrol* or not NEXT enrol* or nonparticip* or non NEXT particip* or not NEXT particip*) NEAR/3 (trial* or randomized or randomised or rct*):ti or (nonentry or non NEXT entry or nonenter* or non NEXT enter* or not NEXT enter* or nonenrol* or non NEXT enrol* or not NEXT enrol* or nonparticip* or non NEXT particip* or not NEXT particip*) NEAR/3 (trial* or randomized or randomised or rct*):ab
(nonentry or non NEXT entry or nonenter* or non NEXT enter* or not NEXT enter* or nonenrol* or non NEXT enrol* or not NEXT enrol* or nonparticip* or non NEXT particip* or not NEXT particip*) NEAR/3 patient*:ti or (nonentry or non NEXT entry or nonenter* or non NEXT enter* or not NEXT enter* or nonenrol* or non NEXT enrol* or not NEXT enrol* or nonparticip* or non NEXT particip* or not NEXT particip*) NEAR/3 patient*:ab
(nonrandom* or non NEXT random*) NEAR/3 (patient* or group* or case* or serie* or study or studies or trial*):ti or (nonrandom* or non NEXT random*) NEAR/3 (patient* or group* or case* or serie* or study or studies or trial*):ab
(exclud* NEAR/3 (randomization or randomisation)):ti or (exclud* NEAR/3 (randomization or randomisation)):ab
(non NEXT participant* or nonparticipant*) NEAR/3 group*:ti or (non NEXT participant* or nonparticipant*) NEAR/3 group*:ab
(patient* NEAR/3 prefer*):ti or (patient* NEAR/3 prefer*):ab
(treatment or method*) NEAR/3 prefer*:ti or (treatment or method*) NEAR/3 prefer*:ab
(treatment NEAR/3 (select* or choose or chose or chosen or choice)):ti or (treatment NEAR/3 (select* or choose or chose or chosen or choice)):ab
(own or patient* or by) NEXT choice:ti or (own or patient* or by) NEXT choice:ab
(standard or usual) NEXT practice:ti or (standard or usual) NEXT practice:ab
(refus* or decline*) NEAR/3 (participat* or random*):ti or (refus* or decline*) NEAR/3 (participat* or random*):ab
(non or lack* or with* or without or refus* or decline*) NEAR/3 consent:ti or (non or lack* or with* or without or refus* or decline*) NEAR/3 consent:ab
(follow NEXT up) NEAR/3 register*:ti or (follow NEXT up) NEAR/3 register*:ab
(zelen):ti or (zelen):ab
(#1 OR #2 OR #3)
(#4 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17)
(outside adj3 (trial? or randomi?ed or rct? or program)).tw.
((nonentry or non entry or nonenter$ or non enter$ or "not enter$" or nonenrol$ or non enrol$ or "not enrol$" or nonparticip$ or non particip$ or "not particip$") adj3 (trial? or randomi?ed or rct?)).tw.
((nonentry or non entry or nonenter$ or non enter$ or "not enter$" or nonenrol$ or non enrol$ or "not enrol$" or nonparticip$ or non particip$ or "not particip$") adj3 patient?).tw.
((nonrandom$ or non random$) adj3 (patient? or group? or case? or serie? or study or studies or trial?)).tw.
(exclud$ adj3 randomi?ation).tw.
((non participant? or nonparticipant?) adj3 group?).tw.
(patient? adj3 prefer$).tw.
((treatment or method?) adj3 prefer$).tw.
(treatment adj3 (select$ or choose or chose or chosen or choice)).tw.
((own or patient? or by) adj choice).tw.
((standard or usual) adj practice).tw.
((refus$ or decline$) adj3 (participat$ or random$)).tw.
((non or "not" or lack$ or withh$ or without or refus$ or decline$) adj3 consent).tw.
Randomised trial with concurrent eligible patients outside of the RCT. The eligible but non‐RCT patients were not in the RCT because of patients preference for no sedation (135 patients) or patients refused (27 patients). Adult ambulatory patients scheduled to undergo diagnostic upper endoscopy. There was no losses to follow up.
Data
Characteristics of non‐RCT patients compared to RCT patients who received the same treatment not presented. 50 RCT patients who received sedation and 27 non‐RCT patients who received same treatment.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The Sedation patients received standard parenteral sedation (titrated doses of midazolam and/or meperidine). The placebo group received saline and the non‐RCT group nothing.
Outcomes
Clinical outcomes were assessed in all patients and they were followed up for 24 hours. Main outcome in this study was patient self reported satisfaction.
Randomised trial with concurrent eligible patients outside of the RCT. The eligible but non‐RCT patients were not in the RCT because of patients preference for no sedation (135 patients) or patients refused (27 patients). Adult ambulatory patients scheduled to undergo diagnostic upper endoscopy. There was no losses to follow up.
Data
Characteristics of non‐RCT patients compared to RCT patients who received the same treatment not presented. 50 RCT patients who received placebo and 135 non‐RCT patients who received nothing.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The Sedation patients received standard parenteral sedation (titrated doses of midazolam and/or meperidine). The placebo group received saline and the non‐RCT group nothing.
Outcomes
Clinical outcomes were assessed in all patients and they were followed up for 24 hours. Main outcome in this study was patient self reported satisfaction.
Randomised trial with concurrent eligible patients outside of the RCT. The eligible but non‐RCT patients were not in the RCT because of patients refusal (24 patients) or patients not invited by their physician (24 patients). Patients with intermediate or high grade sarcoma. No losses to follow up.
Data
Characteristics of non‐RCT patients compared to RCT patients who received the same treatment not presented. Twenty RCT patients received doxorubin treatment and 21 non‐RCT patients, 7 men and 14 women.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients in a registry. The experimental RCT arm patients were treated with doxorubicin. The control RCT patients were under observation.
Outcomes
Clinical outcomes were assessed in all patients. Patients were followed for up to 4 years. Main outcome reported in this study was disease free survival.
Notes
No statistically significant difference was shown between the two RCT treatments.
Randomised trial with concurrent eligible patients outside of the RCT. The eligible but non‐RCT patients were not in the RCT because of patients refusal (24 patients) or patients not invited by their physician (24 patients). Patients with intermediate or high grade sarcoma. No losses to follow up.
Data
Characteristics of non‐RCT patients compared to RCT patients who received the same treatment not presented. Twenty‐two RCT patients were under observation and 27 non‐RCT patients.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients in a registry. The experimental RCT arm patients were treated with doxorubicin. The control RCT patients were under observation.
Outcomes
Clinical outcomes were assessed in all patients. Patients were followed for up to 4 years. Main outcome reported in this study was disease free survival.
Notes
No statistically significant difference was shown between the two RCT treatments.
Randomised trial with patient preference arm. Patients who refused randomization were treated according to their choice. Women who attend termination of pregnancy at 10‐13 weeks gestation. No losses to follow up before discharge from hospital.
Data
Characteristics of choice patients presented and compared to RCT patients who received the same treatment were presented in Ashok 2002. RCT medical abortion group were mean (SD) 26 (7) years, 202 women. Preference medical abortion group were mean 29 (7) years, 15 women.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The experimental RCT arm patients underwent medical abortion. The control RCT patients underwent surgical abortion.
Outcomes
Clinical outcomes were assessed in all women, they were followed up until discharge from hospital. Main outcome of this study was anxiety after procedure.
Notes
The two randomised treatments were not statistically significantly different.
Randomised trial with patient preference arm. Patients who refused randomization were treated according to their choice. Women who attend termination of pregnancy at 10‐13 weeks gestation. No losses to follow up before discharge from hospital.
Data
Characteristics of choice patients presented and compared to RCT patients who received the same treatment were presented in Ashok 2002. RCT surgical abortion group were mean (SD) 25 (7) years, 198 women. Preference medical abortion group were mean 26 (6) years, 71 women.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The experimental RCT arm patients underwent medical abortion. The control RCT patients underwent surgical abortion.
Outcomes
Clinical outcomes were assessed in all women, they were followed up until discharge from hospital. Main outcome of this study was anxiety after procedure.
Notes
The two randomised treatments were not statistically significantly different.
Randomised trial with patient preference arm. Patients who refused randomization were treated according to their choice. Women with dysfunctional uterine bleeding suitable for endometrial ablation. No losses to follow up.
Data
Characteristics of choice patients presented and compared to RCT patients who received the same treatment. RCT local anaesthesia group were mean (SD) 43 (5) years, 20 women. Preference local anaestesia group were mean 44 (6) years, 32 women.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The experimental RCT arm patients underwent local anaesthesia. The control RCT patients underwent general anaesthesia.
Outcomes
Clinical outcomes were assessed in all women, they were followed up until discharge from hospital. The main outcome of this study was pain.
Notes
The two randomised treatments were not statistically significantly different.
Randomised trial with patient preference arm. Patients who refused randomization were treated according to their choice. Women with dysfunctional uterine bleeding suitable for endometrial ablation. No losses to follow up.
Data
Characteristics of choice patients presented and compared to RCT patients who received the same treatment. RCT general anaesthesia group were mean (SD) 42 (3) years, 16 women. Preference general anaesthesia group were mean 43 (5) years, 30 women.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The experimental RCT arm patients underwent local anaesthesia. The control RCT patients underwent general anaesthesia.
Outcomes
Clinical outcomes were assessed in all women, they were followed up until discharge from hospital. The main outcome of this study was pain.
Notes
The two randomised treatments were not statistically significantly different.
Randomised trial with concurrent eligible patients outside of the RCT. The eligible but non‐RCT patients were not in the RCT because of patients preference for no medication (31 patients). Patients with panic disorder who had had more than 3 attacks during the last three weeks. Nine (26 %) of the 35 RCT cognitive therapy patients dropped out and seven (23%) of the 31 non‐RCT cognitive therapy patients were lost to follow up.
Data
Characteristics of non‐RCT patients compared to RCT patients who received the same treatment not presented. The majority of patients were female (74% combined groups) and of average age of 34 (SD 8) years.
Comparisons
Two RCT arms, the experimental arm was compared with similarly treated non‐RCT patients. The experimental group received 12 week of cognitive therapy. The control arm was placebo.
Outcomes
Clinical outcomes were assessed in all patients who were followed up. Patients were followed for up for 12 weeks. Main outcome reported in this study was frequency of panic attacks.
Randomised trial with concurrent eligible patients outside of the RCT. We do not know why the non‐RCT patients were not in the RCT. Women with uterine cervix cancer stage II and III. Unclear if there was losses to follow up.
Data
Charateristics of the RCT radiatiotheraphy in combination with metronidazole group were 56 women, age unknown. Non‐RCT radiatiotheraphy in combination with metronidazole group were 124 women, age unknown.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The experimental arm patients received rradiatiotheraphy in combination with metronidazole. The control patients received radiation alone.
Outcomes
Clinical outcomes were assessed in all patients, patients were followed for 2 weeks after last treatment. Main outcome in this study was lack of clearance.
Notes
The experimental arm of the RCT was more effective than control.
Randomised trial with concurrent eligible patients outside of the RCT. We do not know why the non‐RCT patients were not in the RCT. Women with uterine cervix cancer stage II and III. Unclear if there was losses to follow up.
Data
Characteristics of the RCT radiation alone group were 52 women, age unknown. Non‐RCT radiation alone group were 163 women, age unknown.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The experimental arm patients received radiatiotheraphy in combination with metronidazole. The control patients received radiation alone.
Outcomes
Clinical outcomes were assessed in all patients, patients were followed for 2 weeks after last treatment. Main outcome in this study was lack of clearance.
Notes
The experimental arm of the RCT was more effective than control.
Randomised trial with concurrent eligible patients outside of the RCT. Children whose parents or physician refused randomization were treated according to their choice. Children with acute lymphocytic leukemia who had been on continuous chemotherapy for a minimum of three years, regardless of the therapy regimen. No losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT maintenance chemotherapy children were 22 boys and 22 girls, age uncertain. Non‐RCT maintenance chemotherapy patients were 16 boys and 8 girls, age uncertain.
Comparisons
Two RCT arms, the experimental arm was compared with similarly treated eligible non‐RCT patients. The experimental arm children were given continuation of maintenance chemotherapy for another three years. Chemotherapy was discontinued in the control group.
Outcomes
Clinical outcomes were assessed in all the children, they were followed up approximately 25 months. Main outcome in this study was relapse.
Notes
The experimental treatment was more beneficial than the control treatment.
Randomised trial with concurrent preference trial outside of the RCT. The non‐RCT patients were not in the RCT because they refused randomization, but consented to be followed in a preference trial. 18 to 70 years old primary care patients who meet the Research Diagnostic Criteria for major depression as assessed by the GP. The RCT counseling group lost 8 (23%) patients to follow up, the preference counseling group lost 32 (23%) patients to follow up.
Data
Characteristics of preference trial patients presented and compared to RCT patients who received the same treatment. RCT counseling patients were on average approximately 38 years, approximately 23% men. Preference counseling patients were mean 36 (10 SD) years, 36 men and 104 women.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients in a preference trial. The experimental RCT arm the patients were given counseling, the control RCT arm patients were prescribed antidepressants.
Outcomes
Clinical outcomes were assessed in all of the patients, they were followed up for 8 weeks. Main outcome in this study was BDI score at 8 weeks.
Randomised trial with concurrent preference trial outside of the RCT. The non‐RCT patients were not in the RCT because they refused randomization, but consented to be followed in a preference trial. 18 to 70 years old primary care patients who meet the Research Diagnostic Criteria for major depression as assessed by the GP. The RCT antidepressants group lost 6 (12%) patients to follow up, the preference antidepressants group lost 24 (30%) patients to follow up.
Data
Characteristics of preference trial patients presented and compared to RCT patients who received the same treatment. RCT patients prescribed antidepressants were on average approximately 38 years, approximately 23% men. Preference patients prescribed antidepressants were on mean 38 (13 SD) years, 21 men and 59 women.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients in a preference trial. The experimental RCT arm the patients were given counseling, the control RCT arm patients were prescribed antidepressants.
Outcomes
Clinical outcomes were assessed in all of the patients, they were followed up for 8 weeks. Main outcome in this study was BDI score at 8 weeks.
Randomised trial with eligible non‐randomised patients outside of the trial. Patients not in the RCT were not in because they refused randomization, but allowed monitoring. Patients below 75 years of age, curative treatment for a primary tumor and inclusion within 2 months after curative or adjuvant therapy. No patients were lost to follow up in the RCT control group, and 13 patients were lost to follow up in the non‐RCT monitoring group.
Data
Characteristics of non‐randomised patients presented and compared to RCT patients who received the same treatment. RCT control patients were on average 54 years. Non‐RCT patients were on average 54 years.
Comparisons
Two RCT arms, the control arm patients were compared with similarly treated eligible non‐RCT patients. The experimental group took part in a 'starting again' rehabilitation program. The control patients were monitored with survey.
Outcomes
Outcomes were assessed in all patients, they were followed up for 1 year. Main outcome in this study was bad quality of life.
Randomised cross over trial with some patients randomized to not be informed about the trial. Patients with mild or moderate cancer pain which did not need narcotic analgesic. No losses to follow up.
Data
Characteristics of RCT informed patients presented and compared to RCT non‐informed patients who received the same treatment. RCT informed patients were on average 58 (37 to 82) years, 4 men and 14 women. RCT un‐informed patients were on average 63 (42 to 92) years, 10 men and 15 women.
Comparisons
Two RCT arms, all patients received both treatment arms and both arms were compared with similarly treated un‐informed RCT patients. The experimental arm received naproxen. The control arm received a placebo. Only the experimental arm results are presented.
Outcomes
Clinical outcomes were assessed in all patients, they were followed up for 2 days. Main outcome in this study was pain score.
Notes
The experimental treatment was more effective than control.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not invited to take part in the RCT because they lived more than 20 miles from the hospital. Women with dysfunctional uterine bleeding, <50 years of age and weight < 100 kg. 5 (14%) women were lost to follow up in the RCT inpatient group, 16 (19%) women were lost to follow up in the non‐RCT inpatient group.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT patients were mean 41 (5) years. Non‐RCT patients were mean 40 (5) years.
Comparisons
Two RCT arms, the control arm patients were compared with similarly treated eligible non‐RCT patients. The experimental arm patients were treated as day cases and discharged from hospital on the same day. The control patients were treated as inpatients.
Outcomes
Clinical outcomes were assessed in all patients, patients were followed for 1 year. Main outcome in this study was severe pain.
Notes
No difference was shown between the two RCT treatments.
Randomised trial with concurrent eligible non‐randomised patients outside of the trial. Patients not in the RCT were not in because they refused randomization, but allowed monitoring. Young patiens with anorexia nervose with 19% weight loss. Lossess to follow up not reported.
Data
Characteristics of non‐randomised patients presented and compared to RCT patients who received the same treatment. The 14 RCT control patients were mean 17 (4) years, 36 (6) kg. The 18 Non‐RCT patients were on average 16 (2) years, 36 (7) kg.
Comparisons
Two RCT arms, the control arm patients were compared with similarly treated eligible non‐RCT patients. The experimental group were given amitriptyline and the control group were given placebo.
Outcomes
Clinical outcomes were assessed in all patients, they were followed up for 5 weeks. Main outcome in this study was less than 30% response.
Notes
No difference was shown between the two RCT treatments.
Randomised trial with concurrent eligible patients in registry outside of the RCT. The eligible but non‐RCT patients were not in the RCT because of patients preference for treatment (41 patients) or physicians preference for treatment (114 patients). Diagnosis of ductal carcinoma in situ, maximum diameter of 5 cm, age < 70 years. 4% loss to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. Breast conserving treatment +radiotherapy RCT patients were 133 women, age unknown. Breast conserving treatment +radiotherapy treated non‐ RCT patients were 29 women, age unknown.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Experimental: Breast conserving treatment + radiotherapy. Control: breast conserving treatment.
Outcomes
Clinical outcomes were assessed in all the patients. Patients in the RCT were followed for an average of 51 months and non‐RCT patients were followed for an average of 39 months. Main outcome was number of events.
Notes
The experimental treatment was significantly more beneficial than the control treatment.
Randomised trial with concurrent eligible patients in registry outside of the RCT. The eligible but non‐RCT patients were not in the RCT because of patients preference for treatment (41 patients) or physicians preference for treatment (114 patients). Diagnosis of ductal carcinoma in situ, maximum diameter of 5 cm, age < 70 years. 4% loss to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. Breast conserving treatment RCT patients were 135 women, age unknown. Breast conserving treatment non‐RCT patients were 93 women, age unknown.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Experimental: Breast conserving treatment + radiotherapy. Control: breast conserving treatment.
Outcomes
Clinical outcomes were assessed in all the patients. Patients in the RCT were followed for an average of 51 months and non‐RCT patients were followed for an average of 39 months. Main outcome was number of events.
Notes
The experimental treatment was significantly more beneficial than the control treatment.
Randomised trial with concurrent eligible patients outside of the RCT, for part of the study period, a Zelen design were applied where only those randomized to breast preservation were asked to consent. The non‐RCT patients were not in the RCT because of preference for one of the treatments. Women with invasive mammary carcinoma of 69 years or younger and with the possibility of a satisfactory cosmetic result by exicion of the tumor. The breast preserving RCT group lost 21 (6%) to follow up, the non‐RCT breast preserving group lost 30 (33%) to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. Breast preserving RCT patients were 334 women, age unknown. Breast preserving non‐RCT patients were 90 women, age unknown.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Experimental: breast conservation. Control: Mastectomy.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 6 years. Main outcome was recurrence after 1.75 years.
Randomised trial with concurrent eligible patients outside of the RCT, for part of the study period, a Zelen design was applied where only those randomized to breast preservation were asked to consent. The non‐RCT patients were not in the RCT because of preference for one of the treatments. Women with invasive mammary carcinoma of 69 years or younger and with the possibility of a satisfactory cosmetic result by exicion of the tumor. Mastectomy RCT group lost 22 (7%) to follow up, non‐RCT mastectomy group lost 19 (20%) to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. Mastectomy RCT patients were 328 women, age unknown. Mastectomy non‐ RCT patients were 95 women, age unknown.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Experimental: breast conservation. Control: Mastectomy.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 6 years. Main outcome was recurrence after 1.75 years.
Randomised trial with concurrent preference trial outside of the RCT. The non‐RCT patients were not in the RCT because they refused randomisation because of preference for treatment. Adult ASA I and II patients who presented for cataract surgery with regional anaesthesia. No lossess to follow up.
Data
Characteristics of non‐randomised patients partially presented but not compared to RCT patients who received the same treatment. The 40 patients in the RCT placebo group was compared to the 136 patients in the non‐RCT patients who did not want anxiolytic drugs.
Comparisons
Six RCT arms, five arms with different anxiolytics and one placebo arm. The placenbo arm was compared with similarly treated eligible patients outside of the trial.
Outcomes
Clinical outcomes were assessed in all patients. patients were followed until just after the procedure. Main outcome was anxiety during operation
Notes
The RCT treatemtns were not statistically different.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because of patient refusal (28%) and physician refusal (69% patients were not invited) but were followed up in a register. Patients with mild or moderate stable angina pectoris or free of angina but with a documented history of myocardial infarction, both sexes <65 years of age. Outcomes were assessed by cardiologists. The RCT lost 1 patient to follow up, and 10 patients were lost in the nonrandomized groups in total.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. Surgery RCT patients were mean 52 (7) years, 353 male and 37 female. Surgery non‐RCT patients were mean 51 (8) years, 518 male and 52 female.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Experimental: coronary artery bypass surgery. Control: medically treated patients were given medication only.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for an average of 10 years. Main outcome was 5 year mortality.
Notes
The two RCT treatment arms were not statistically different.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because of patient refusal (28%) and physician refusal (69% patients were not invited) but were followed up in a register. Patients with mild or moderate stable angina pectoris or free of angina but with a documented history of myocardial infarction, both sexes <65 years of age. Outcomes were assessed by cardiologists. The RCT lost 1 patient to follow up, and 10 patients were lost in the nonrandomized groups in total.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. Medically treated RCT patients were mean 51 (8) years, 351 male and 39 female. Medically treated non‐ RCT patients were mean 51 (8) years, 674 male and 71 female.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Experimental: coronary artery bypass surgery. Control: medically treated patients were given medication only.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for an average of 10 years. Main outcome was 5 year mortality.
Notes
The two RCT treatment arms were not statistically different.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they refused randomization. Women with singleton pregnancy with intact membranes, AFI equal to or larger than 5.0 cm and no fetal hearth rate tracing abnormalities on admission. No losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT non infusion patients were on average 22 years. Non‐RCT non infusion patients were on average 23 years.
Comparisons
Two RCT arms, the control arm patients were compared with similarly treated eligible non‐RCT patients. The experimental arm patients were treated with prophylactic saline amnioinfusion. The control patients were not infused.
Outcomes
Clinical outcomes were assessed in all women, they were followed up until delivery. Main outcome in this study was incidence of recurrent variable decelerations/bradycardia.
Notes
No significant differences were detected between the two RCT arms.
Randomised trial with patient preference arm. Patients who refused randomization were treated according to their choice. Patients who met research diagnostic criteria for major depression. Missing data for 4 (8%) patients in RCT counseling and 11 (8%) of choice counseling.
Data
Characteristics of choice patients presented and compared to RCT patients who received the same treatment. RCT counseling patients were mean 37 (11 SD) years, 16 men and 36 women. Choice counseling patients were mean 36 (10 SD) years, 36 men and 104 women.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The counseling group received 6 sessions of counseling. The other group was given antidepressant drug treatment.
Outcomes
Clinical outcomes were assessed in all patients, they were followed up for 1 year. Main outcome in this study was remission.
Randomised trial with patient preference arm. Patients who refused randomization were treated according to their choice. Patients who met research diagnostic criteria for major depression. Missing data for 1 (2%) patient in the RCT antidepressant group and 2 (3%) patients in the choice antidepressant group.
Data
Characteristics of choice patients presented and compared to RCT patients who received the same treatment. RCT antidepressant patients were mean 38 (12 SD) years, 8 men and 43 women. Choice antidepressant patients were mean 38 (13 SD) years, 21 men and 59 women.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The counseling group received 6 sessions of counseling. The other group was given antidepressant drug treatment.
Outcomes
Clinical outcomes were assessed in all patients, they were followed up for 1 year. Main outcome in this study was remission.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because of preference for treatment. Patients with asymptomatic cervical bruit and abnormal ocular pneumoplethysmography. No losses to follow up.
Data
Characteristics of non‐RCT patients not presented and compared to RCT patients who received the same treatment. RCT surgery patients were mean 64 years, 11 men and 4 women. Non‐RCT surgery patients were mean 62 years, sex unknown.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The experimental RCT arm patients underwent arteriography and prophylactic carotid endarterectomy if stenotic atherosclerosis was located at the carotid bifurcation. The control RCT patients were given aspirin, 650 mg twice a day.
Outcomes
Clinical outcomes were assessed in all patients, they were followed up for an average of 3 years. Main outcome in this study was the sum of all unfavorable outcomes including stroke, death of stroke, major angiographic and perioperative complications, asymptomatic carotid occlusion, and recurrent carotid artery stenosis.
Notes
The experimental treatment had resulted in significantly more unfavorable outcomes.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because of preference for treatment. Patients with asymptomatic cervical bruit and abnormal ocular pneumoplethysmography. The non‐RCT aspirin group lost 2 (14%) patients to follow up, no losses to follow up in the other groups.
Data
Characteristics of non‐RCT patients not presented and compared to RCT patients who received the same treatment. RCT aspirin patients were mean 63 years, 10 men and 4 women. Non‐RCT aspirin patients were mean 65 years, sex unknown.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The experimental RCT arm patients underwent arteriography and prophylactic carotid endarterectomy if stenotic atherosclerosis was located at the carotid bifurcation. The control RCT patients were given aspirin, 650 mg twice a day.
Outcomes
Clinical outcomes were assessed in all patients, they were followed up for an average of 3 years. Main outcome in this study was the sum of all unfavorable outcomes including stroke, death of stroke, major angiographic and perioperative complications, asymptomatic carotid occlusion, and recurrent carotid artery stenosis.
Notes
The experimental treatment had resulted in significantly more unfavorable outcomes.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because parents refused. Babies, 600 to 2000g birth weight, with no major organ malformation or congenital defect. Probably no losses to follow up.
Data
Characteristics of non‐RCT babies were compared to RCT babies who received the same treatment. RCT babies who received placebo were 31 gestational weeks, weight 1.3 (0.4) kg, 24 boys and 35 girls. The eligible non‐RCT babies who were given nothing, were 31 gestational weeks, weight 1.3 (0.4) kg, 48 boys and 37 girls.
Comparisons
Two RCT arms, the experiemental arm given intravenously administered immune globulin to prevent nosocomial sepsis and the RCT control arm given placebo. The placebo arm was compard to non‐RCT eligible babies given nothing.
Outcomes
Clinical outcomes were assessed in all babies, they were followed up until discharge from hospital. Main outcome in this study was mortality.
Notes
The experimental treatment was significantly better then control.
Randomised trial with patients randomised to a RCT or a patient preference trial. Patients who refused randomization were treated according to their choice. Women attending clinic because of heavy menstrual bleeding. No losses to follow up.
Data
Characteristics of choice patients presented and compared to RCT patients who received the same treatment. 31% of RCT transcervical resection patients were under 40 years. 38% of Choice transcervical resection patients were under 40 years.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The experimental group received transcervival surgical resection of the endometrium. The control patients were given medical drug treatment.
Outcomes
Clinical outcomes were assessed in all women, they were followed up for 4 months. Main outcome in this study was lack of satisfaction with treatment.
Notes
The experimental treatment was more effective than control.
Randomised trial with patients randomised to a RCT or a patient preference trial. Patients who refused randomization were treated according to their choice. Women attending clinic because of heavy menstrual bleeding. No losses to follow up
Data
Characteristics of choice patients presented and compared to RCT patients who received the same treatment. 33% of RCT medical patients were under 40 years. 37% of Choice medical patients were under 40 years.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The experimental group received transcervival surgical resection of the endometrium. The control patients were given medical drug treatment.
Outcomes
Clinical outcomes were assessed in all women, they were followed up for 4 months. Main outcome in this study was lack of satisfaction with treatment.
Notes
The experimental treatment was more effective than control.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because their parent/s declined randomisation, these patients were treated according to parental choice. The non‐RCT patients were followed‐ up identically to the RCT patients. Previously untreated AML patients less than 17 years of age. Patients were followed for 5 years. No losses to follow up.
Data
Non‐RCT patients were compared to RCT patients who received the same treatment. Of the RCT children receiving cranial irradiation 3 were under 2 years, 8 boys and 7 girls. Of the non‐RCT children receiving cranial irradiation, none were under 2 years, 6 boys and 7 girls.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Experimental: Cranial irradiation. Control: No cranial irradiation.
Outcomes
Clinical outcomes were assessed in all the patients. Main outcome was relapse.
Notes
The cranial irradiation (experimental) treatment was associated with favorable outcome.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because their parent/s declined randomisation, these patients were treated according to parental choice. The non‐RCT patients were followed‐ up identically to the RCT patients. Previously untreated AML patients less than 17 years of age. Patients were followed for 5 years. No losses to follow up.
Data
Non‐RCT patients were compared to RCT patients who received the same treatment. Of the RCT children who did not receive cranial irradiation 1 was under 2 years, 9 boys and 7 girls. Of the non‐ RCT children who did not receive cranial irradiation 3 were under 2 years, 4 boys and 8 girls.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Experimental: Cranial irradiation. Control: No cranial irradiation.
Outcomes
Clinical outcomes were assessed in all the patients. Main outcome was relapse.
Notes
The cranial irradiation (experimental) treatment was associated with favorable outcome.
Randomised trial where half the patients were randomized to not be told about the trial, these patients (No choice) were lead to believe that they were receiving standard practice. The other randomized half of the patients were told that the RCT compared a drug for insomnia and placebo, all the patients were given the same treatment, placebo pills. Patients who were in hospital for more than two days and were suffering from insomnia. No losses to follow up.
Data
Characteristics of the patients not presented. 30 placebo RCT patients and 30 no‐choice RCT patients.
Comparisons
Two RCT arms, both providing the same treatment, but the placebo group consented to take part in a RCT whereas the no‐choice group did not know about the trial.
Outcomes
Outcomes were assessed in all patients. Patients were followed for one day. Main outcome was # of spontaneously reported side effects.
Notes
The no‐choice treatment was more effective than the same treatment as placebo for hypnotic activity, results only presented as p value.
Randomised trial with concurrent eligible patients outside of the RCT. We do not know why the non‐RCT patients were not in the RCT, but their details were recorded in a population based cancer registry. Patients with resected non‐small cell lung cancer. Losses to follow up unknown.
Data
Characteristics of non‐RCT patients compared to RCT patients who received the same treatment not presented but adjusted for in the analysis.
Comparisons
Several RCT arms, the control arm patients were compared with similarly treated eligible non‐RCT patients.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 1, 2 and 3 years. Main outcome was mortality.
Randomised trial with concurrent eligible patients outside of the RCT. It is unclear why the non‐RCT patients were not in the RCT. Diagnosis of prostatic carcinoma and skeletal metastases. No losses to follow up.
Data
Some characteristics of non‐RCT patients presented next to RCT patients who received the same treatment. RCT patients were on average 68 (55 to 77) years. Ages of the non‐RCT patients were not presented.
Comparisons
Two RCT arms, the control arm patients were compared with similarly treated eligible non‐RCT patients. The experimental arm patients were treated with estramusterine. The control patients and the non‐RCT patients were treated with 2.6‐cis.
Outcomes
Clinical outcomes were assessed in all patients after 1, 2, and 3 months. Main outcome in this study was no improvement in condition after 3 months.
Notes
No statistically significant difference was shown between the two RCT treatments.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they refused. Patients with multivessel coronary artery disease eligible for stenting or bypass surgery based on agreement of cardiologist and surgeon. Unclear if there was any losses to follow up in the RCT group. Three people were lost to follow up in the non‐RCT group.
Data
Characteristics of the non‐RCT patients were presented and compared to RCT patients who received the same treatment. RCT stent patients were 61 (10) years, 462 men, 138 women. Non‐RCT stent patietns were 62 (9) years, 40 men and 10 women.
Comparisons
Two RCT arms, both arms were compared with eligible non‐RCT patients who received similar treatment. The experimental treatment was stent implantation by coronary angioplasty. The control treatment was bypass surgery.
Outcomes
Clinical outcomes were measured in all patients. Patients were followed up for 6 months. Main outcome was mortality.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they refused. Patients with multivessel coronary artery disease eligible for stenting or bypass surgery based on agreement of cardiologist and surgeon. Unclear if there was any losses to follow up in the RCT group. Two people were lost to follow up in the non‐RCT group.
Data
Characteristics of the non‐RCT patients were presented and compared to RCT patients who received the same treatment. RCT bypass patients were 61 (9) years, 460 men, 145 women. Non‐RCT bypass patients were 62 (9) years, 37 men and 9 women.
Comparisons
Two RCT arms, both arms were compared with eligible non‐RCT patients who received similar treatment. The experimental treatment was stent implantation by coronary angioplasty. The control treatment was bypass surgery.
Outcomes
Clinical outcomes were measured in all patients. Patients were followed up for 6 months. Main outcome was mortality.
Randomised population trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they refused. School children 5 to 7.9 years old. Losses to follow up were not reported.
Data
Characteristics of the 13463 eligible non‐RCT children were not presented and not compared to the 48335 RCT children who recieved similar treatment.
Comparisons
Two RCT arms, the control arm children were compared with non‐randomised children who did not receive any intervention either. The RCT experimental children were offered testing for diabetes
Outcomes
All cases of childhood diabetes were reported to the Department of Paediatrics and records were collected from them. Children were followed up for mean 7.1 years. Main outcome was getting the diagnosis of diabetes.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they refused because of preference for treatment. Couples in in‐vitro fertelisation (IVF) program, 1st IVF for the 1st child.
Data
Characteristics of the eligible non‐RCT patients were not presented or compared to the RCT patients receiving similar treatment. 100 RCT participants received pre‐IVF counselling focusing on the narrative capacities of couples, eight were lost to follow up. 24 eligible non‐RCT couples received similar treatment, six were lost to follow up.
Comparisons
Two RCT arms, both arms were compared with eligible non‐randomised couples who received similar treatment. Experimental: pre‐IVF counselling focusing on the narrative capacities of couples. Control: no counselling.
Outcomes
Outcomes were assessed in all couples. Couples were followed up for 6 weeks. Main outcome was State Trait Anxiety Inventory.
Notes
The two RCT arms were not significantly different.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they refused because of preference for treatment. Couples in in‐vitro fertelisation (IVF) program, 1st IVF for the 1st child. Three RCT control couples were lost to follow up, two non‐RCT couples were lost to follow up.
Data
Characteristics of the eligible non‐RCT patients were not presented or compared to the RCT patients receiving similar treatment. 100 RCT control participants did not receive counselling. 58 eligible non‐RCT couples received similar treatment.
Comparisons
Two RCT arms, both arms were compared with eligible non‐randomised couples who received similar treatment. Experimental: pre‐IVF counselling focusing on the narrative capacities of couples. Control: no counselling.
Outcomes
Outcomes were assessed in all couples. Couples were followed up for 6 weeks. Main outcome was State Trait Anxiety Inventory.
Notes
The two RCT arms were not significantly different.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they refused randomisation, but agreed to follow up in a registry. Patients with multivessel coronary artery disease. Losses to follow up unknown.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT percutaneous transluminal coronary angioplasty patients were mean 62 years, 668 men and 247 women. Non‐RCT percutaneous transluminal coronary angioplasty patients were mean 61 years, 880 men and 309 women.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients in a registry. The experimental RCT arm patients underwent percutaneous transluminal coronary angioplasty (PTCA). The control RCT patients underwent coronary artery bypass graft surgery (CABG).
Outcomes
Clinical outcomes were assessed in all patients, they were followed up for 7 years. Main outcome in this study was mortality.
Notes
The experimental treatment resulted in significantly higher mortality than the control treatment.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they refused randomisation, but agreed to follow up in a registry. Patients with multivessel coronary artery disease. Losses to follow up unknown.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT coronary artery bypass graft surgery patients were mean 61 years, 676 men and 238 women. Non‐RCT coronary artery bypass graft surgery patients were mean 63 years, 462 men and 163 women.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients in a registry. The experimental RCT arm patients underwent percutaneous transluminal coronary angioplasty (PTCA). The control RCT patients underwent coronary artery bypass graft surgery (CABG).
Outcomes
Clinical outcomes were assessed in all patients, they were followed up for 7 years. Main outcome in this study was mortality.
Notes
The experimental treatment resulted in significantly higher mortality than the control treatment.
Randomised controlled trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the trial because they refused randomisation. Patients undergoing outpatient colonoscopy. No losses to follow up.
Data
Characteristics of the non‐randomised patients compared to RCT patients who received the same treatment. RCT patients given intravenous were on average 49 (25 to 75) years, 29 male and 17 female. Non‐RCT patients given intravenous were on average 52 (18 to 82) years, 29 male and 59 female.
Comparisons
Two RCT arms, the control group patients were compared with the non‐randomised patients who received similar treatment. Experimental: self‐administered inhaled nitrous oxide (Entonox: 50% nitrous oxide, 50% oxygen). Control: intravenous sedation/analgesia (Midazolam and Meperidine).
Outcomes
Outcomes were assessed in all patients. The volunteers were followed for a minimum of 30 minutes after colonoscopy. Main outcome was # of adverse events.
Notes
The experimental treatment was less effective than control.
Randomised controlled trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the trial because they refused randomization (4 patients) and missed randomization (1 patient). Patients undergoing carotid endarterectomy. No losses to follow up.
Data
Characteristics of the non‐randomised patients compared to RCT patients who received the same treatment. RCT general anaesthetic patients were on average 63 (40 to 77) years, 35 male and 20 female. Non‐RCT general anaesthetic patients were on average 65 (39 to 75) years, 10 male and 4 female.
Comparisons
Two RCT arms, the control arm was compared with the non‐randomised patients who received similar treatment. Experimental: local anaesthetic. Control: general anaesthetic.
Outcomes
Outcomes were assessed in all patients. Patients were followed for the duration of hospital stay. Main outcome was perioperative neurological deficit.
Notes
The two RCT treatments were not statistically different.
Randomised controlled multi‐centre trial with some of the centers having problems recruiting patients to the trial, these centers treated patients according to patient choice. Patients with histologically or cytologically proven non‐small cell lung cancer, stage IIIB or IV. No losses to follow up.
Data
Characteristics of non‐RCT patients compared to RCT patients who received the same treatment. Chemotherapy RCT patients were on average 61 (36 to 72) years, 12 male and 10 female. Chemotherapy non‐RCT patients were on average 64 (37 to 78) years, 55 male and 42 female.
Comparisons
Two RCT arms, both of them were compared with similarly treated eligible non‐RCT patients. Experimental: Chemotherapy with carboplatin and etoposide. Control: Best supportive care.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 1 year. Main outcome was mortality.
Notes
The experimental treatment was more effective than control.
Randomised controlled multi‐centre trial with some of the centers having problems recruiting patients to the trial, these centers treated patients according to patient choice. Patients with histologically or cytologically proven non‐small cell lung cancer, stage IIIB or IV. No losses to follow up.
Data
Characteristics of non‐RCT patients compared to RCT patients who received the same treatment. Basic supportive care RCT patients were on average 65 (44 to 78) years, 18 male and 8 female. Basic supportive care non‐ RCT patients were on average 72 (66 to 78) years, 3 male and 2 female.
Comparisons
Two RCT arms, both of them were compared with similarly treated eligible non‐RCT patients. Experimental: Chemotherapy with carboplatin and etoposide. Control: Best supportive care.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 1 year. Main outcome was mortality.
Notes
The experimental treatment was more effective than control.
Randomised trial with concurrent eligible patients in a preference trial outside of the RCT. The non‐RCT patients were not in the RCT because they refused randomization because of preference for treatment. Women undergoing legal induced abortion at less than nine weeks gestation. No losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT medical induced patients were mean 25 (6) years. Preference medical induced patients were mean 24 (6) years.
Comparisons
Two RCT arms, patients in both arms were compared with similarly treated eligible preference patients. The experimental arm patients had a medical abortion with mifepristone (RU 486) and gemeprost. The control patients had surgical vacuum aspiration.
Outcomes
Clinical outcomes were assessed in all women, they were followed up for a mean of 16 days. Main outcome in this study was acceptability of procedure measured by recording the number of women who would not undergo same treatment in future.
Notes
The two RCT treatments were not statistically different.
Randomised trial with concurrent eligible patients in a preference trial outside of the RCT. The non‐RCT patients were not in the RCT because they refused randomization because of preference for treatment. Women undergoing legal induced abortion at less than nine weeks gestation. No losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT vacuum aspiration patients were mean 25 (6) years. Preference vacuum aspiration patients were mean 25 (6) years.
Comparisons
Two RCT arms, patients in both arms were compared with similarly treated eligible preference patients. The experimental arm patients had a medical abortion with mifepristone (RU 486) and gemeprost. The control patients had surgical vacuum aspiration.
Outcomes
Clinical outcomes were assessed in all women, they were followed up for a mean of 16 days. Main outcome in this study was acceptability of procedure measured by recording the number of women who would not undergo same treatment in future.
Notes
The two RCT treatments were not statistically different.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they refused because of preference for treatment. Patients undergoing an elective colonoscopy as sole endoscopic procedure. No losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT contol group were 64 (15) years old, 20 men and 9 women. Non‐RCT patients were 60 (16) years old, 20 men and 20 women.
Comparisons
Two RCT arms, the RCT control patients were compared with eligible non‐randomised patietns who received similar treatment. Experimental: self‐controlled sedation. Control: nurse‐controlled sedation.
Outcomes
Clinical outcomes were measured in all patients. Patients were followed up while they were in hospital. Main outcome was tolerability.
Notes
The two RCT treatments were equally safe, but the control was preferred.
Randomised trial with concurrent eligible patients in a preference trial outside of the RCT. The non‐RCT patients were not in the RCT because they refused. Newly presenting infertile couples less than 38 years with noprior in‐vitro fertelisation and clinically ok. RCT control group lost 13 of the 50 couples to follow up. Non‐RCT group lost 18 of the 88 couples to follow up.
Data
Characteristics of participants not presented.
Comparisons
Two RCT arms, the control arm couples were compared with eligible non‐RCT couples who received similar treatment. Experimental: in‐vitro fertelisation as first choice treatment. Control: standard infertility treatment.
Outcomes
It is unclear for how long couples were followed up. Main outcome was pregnancies.
Notes
The control arm of the RCT was better than the experimental treatment.
Randomised trial with concurrent eligible patients in a preference trial outside of the RCT. The non‐RCT patients were not in the RCT because they refused randomization because of preference for treatment. Patients with low back pain on the day of randomisation and for at least 6 weeks prior. 15 RCT patients were lost to follow up and three non‐RCT patients were lost to follow up
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT x‐ray group were median 39 years old, 90 men and 120 women. Non‐RCT x‐ray patients were median 38 years old, 22 men and 10 women.
Comparisons
Two RCT arms, both arms were compared with eligible non‐randomised patients who received similar treatment. Experimental: lumbar spine radiography in addition to usual care. Control: usual care.
Outcomes
Patients were followed up for 9 months. Main outcome was number of patients still with back pain.
Notes
The control treatment was significantly better then the experimental treatment.
Randomised trial with concurrent eligible patients in a preference trial outside of the RCT. The non‐RCT patients were not in the RCT because they refused randomization because of preference for treatment. Patients with low back pain on the day of randomisation and for at least 6 weeks prior. 12 RCT patients were lost to follow up and , two non‐RCT patients were lost to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT non‐x‐ray group were median 39 years old, 84 men and 127 women. Non‐RCT non‐x‐ray patients were median 39 years old, 12 men and 11 women.
Comparisons
Two RCT arms, both arms were compared with eligible non‐randomised patients who received similar treatment. Experimental: lumbar spine radiography in addition to usual care. Control: usual care.
Outcomes
Patients were followed up for 9 months. Main outcome was number of patients still with back pain.
Notes
The control treatment was significantly better then the experimental treatment.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they refused randomization. Pregnant women attending the participating antenatal clinics. Loss to follow up unclear for RCT group, 44 (8%) women were lost to follow up in the non‐RCT group.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT patients combined were mean 28 (5) years, these data not given for control group only. Non‐RCT patients were mean 30 (5) years.
Comparisons
Two RCT arms, the control arm patients were compared with similarly treated eligible non‐RCT patients. The experimental arm patients were given ultrasound screening. The control patients were not offered ultrasound screening.
Outcomes
Clinical outcomes were assessed in all women, they were followed up until delivery. Main outcome in this study was perinatal death.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients consisted of 97 patients who refused randomizations and 353 patients whose physician did not agree, all non‐RCT patients were followed in a registry. Patients with 2‐ or 3‐vessels coronary artery disease, both sexes. Outcomes were assessed by cardiologists. No losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. Bypass treated RCT patients were mean 61 (10) years, 53 women and 141 men. Bypass treated non‐RCT patients were mean 63 (10) years, 51 women and 219 men.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Carotid bypass surgery. Percutaneous transluminal coronary angioplasty.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 3 years. Main outcome was 3 years mortality.
Notes
The two RCT treatments were not statistically different.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients consisted of 97 patients who refused randomizations and 353 patients whose physician did not agree, all non‐RCT patients were followed in a registry. Patients with 2‐ or 3‐vessels coronary artery disease, both sexes. Outcomes were assessed by cardiologists. No losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. Percutaneous transluminal coronary angioplasty treated RCT patients were mean 62 (10) years, 50 women and 148 men. Percutaneous transluminal coronary angioplasty treated non‐ RCT patients were mean 60 (11) years, 41 women and 127 men.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Carotid bypass surgery. Percutaneous transluminal coronary angioplasty.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 3 years. Main outcome was 3 years mortality.
Notes
The two RCT treatments were not statistically different.
Randomised controlled trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were participants in a patient preference trial who refused to be randomised due to preference.The non‐RCT patients were followed up similarly to those in the RCT. Psychology. Patients with depression or depression and anxiety. 27 RCT patients who were given cognitive behavioural therapy were lost to follow up and 15 non‐RCT cognitive behavioural therapy treated patients were lost to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. Cognitive behavioural therapy RCT patients were mean 35 (11) years, 100 women and 34 men. Cognitive behavioural therapy non‐RCT patients were mean 38 (14) years, 63 women and 18 men.
Comparisons
Two RCT arms, both arms were compared with eligible non‐RCT patients who received similar treatment. The experimental treatment was cognitive behavioural therapy. The control treatment was non‐directive counselling.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 12 months. Main outcome was depression measured with Beck Depression Inventory.
Notes
The two RCT treatments were not statistically different.
Randomised controlled trial with concurrent eligible patients outside of the RCT. The non‐RCT patietns were participants in a patient preference trial who refused to be randomised due to preference.The non‐RCT patients were followed up similarly to those in the RCT. Patients with depression or depression and anxiety. 24 RCT patients who were given non‐directive counselling were lost to follow up and 14 non‐RCT non‐directive counselling treated patients were lost to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. Non‐directive counselling RCT patients were mean 33 (11) years, 91 women and 35 men. Non‐directive counselling non‐RCT patients were mean 39 (11) years, 43 women and 11 men.
Comparisons
Two RCT arms, both arms were compared with eligible non‐RCT patients who received similar treatment. The experimental treatment was cognitive behavioural therapy. The control treatment was non‐directive counselling.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 12 months. Main outcome was depression measured with Beck Depression Inventory.
Notes
The two RCT treatments were not statistically different.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they refused randomisation. Junior high school children who are 10 % or more overweight. Unclear if there was any losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. The 25 RCT control children were 13 (1) years, 11 boys and 14 girls. The not treated non‐RCT children were 13 (1) years old, 26 boys and 33 girls.
Comparisons
Two RCT arms, the control arm patients were compared with similarly treated eligible non‐RCT patients. The experimental arm patients were given a comprehensive behaviour program. The control patients were not offered anything.
Outcomes
Clinical outcomes were measured in all children, who were followed up for 12 weeks. Main outcome was % overweight.
Notes
The experimental treatment was more effective than control.
Randomised screening trial where the women not attending were classed as non‐RCT and compared with the RCT control group that were not invited to screening (until after the RCT was completed). The non‐RCT patients were not in the RCT because they did not turn up for screening. All cancers are registered with a central cancer registry. Diagnosis of breast cancer, age 40 to 65 years. No losses to follow up.
Data
Characteristics of non‐RCT patients (non‐attenders) presented and compared to RCT control patients. RCT control patients were mean 54 years, 19943 women. Non‐RCT patients were mean 54 years, 7785 women.
Comparisons
The RCT control arm was compared with the women invited to the RCT who did not participate in the screening (non‐RCT patients).
Outcomes
For both comparison groups, information was collected from a registry. Patients were followed for an average of 4 years. Main outcome was breast cancer deaths.
Notes
The experimental treatment was not significantly different from the control treatment.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they declined randomisation, but consented to follow up. Diagnosis of high‐grade osteosarcoma of an extremity with no metastases, both sexes, age < 30 years. Outcomes were assessed by oncologists. No losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. Of the RCT adjuvant chemotherapy children, 10 were over 12 years old, 13 boys and 5 girls. Of the adjuvant chemotherapy non‐RCT children, 40 were over 12 years old, 31 boys and 28 girls.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Experimental: immediate intensive adjuvant chemotherapy starting two weeks after surgery. Control: observation alone, no adjuvant chemotherapy.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for up to 6 years. Main outcomes were relapse and death.
Notes
The experimental treatment was significantly more beneficial than the control treatment.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they declined randomisation, but consented to follow up. Diagnosis of high‐grade osteosarcoma of an extremity with no metastases, both sexes, age < 30 years. Outcomes were assessed by oncologists. No losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. Of the RCT children under observation 12 were over 12 years old, 11 boys and 7 girls. Of the non‐ RCT observational children, 10 were over 12 years old, 12 boys and 6 girls.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Experimental: immediate intensive adjuvant chemotherapy starting two weeks after surgery. Control: observation alone, no adjuvant chemotherapy.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for up to 6 years. Main outcomes were relapse and death.
Notes
The experimental treatment was significantly more beneficial than the control treatment.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because of parental refusal (101), obstetrician request (35) or late arrival of the team (27). Infants born through thin meconium, after an otherwise low‐risk pregnancy. Outcomes were assessed by respiratory therapists. No losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT infants under observation were 46 boys and 46 girls. Non‐ RCT observational infants were 26 boys and 36 girls.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Experimental: observation alone, no intubation. Control: intubation, which is 'routine meconium management'.
Outcomes
Clinical outcomes were assessed in all the infants. Infants were followed for the duration of the hospital stay. Main outcome was number of respiratory symptoms.
Notes
The two treatments were not statistically significantly different.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because of parental refusal (101), obstetrician request (35) or late arrival of the team (27). Infants born through thin meconium, after an otherwise low‐risk pregnancy. Outcomes were assessed by respiratory therapists. No losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT intubation infants were 41 boys and 36 girls. Non‐RCT intubation infants were 53 boys and 48 girls.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Experimental: observation alone, no intubation. Control: intubation, which is 'routine meconium management'.
Outcomes
Clinical outcomes were assessed in all the infants. Infants were followed for the duration of the hospital stay. Main outcome was number of respiratory symptoms.
Notes
The two treatments were not statistically significantly different.
Randomised trial with concurrent eligible patients outside of the RCT. We do not know why the non‐RCT patients were not in the RCT, but they consented to follow up. Diagnosis of asymptomatic carotid stenosis, both sexes, age 17 to 79 years. Outcomes were assessed by neurologists and surgeons. No losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. 69% of the surgery RCT patients were over 65 years old, 16 women and 20 men. 63% of the surgery non‐RCT patients were over 65 years old, 6 women and 26 men.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Experimental: carotid arteriography and endarterectomy, either unilateral or bilateral at the discretion of the surgeon. Control: medically treated patients were given aspirin (80 mg/day orally). All patients received treatment as indicated for other cerebrovascular risk factors.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for an average of 24 months. Main outcome was ischaemic events.
Notes
The experimental treatment was significantly less beneficial than the control treatment.
Randomised trial with concurrent eligible patients outside of the RCT. We do not know why the non‐RCT patients were not in the RCT, but they consented to follow up. Diagnosis of asymptomatic carotid stenosis, both sexes, age 17 to 79 years. Outcomes were assessed by neurologists and surgeons. No losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. 71% of the medically treated RCT patients were over 65 years old, 14 women and 21 men. 64% of the medically treated non‐ RCT patients were over 65 years old, 25 women and 30 men.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Experimental: carotid arteriography and endarterectomy, either unilateral or bilateral at the discretion of the surgeon. Control: medically treated patients were given aspirin (80 mg/day orally). All patients received treatment as indicated for other cerebrovascular risk factors.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for an average of 24 months. Main outcome was ischaemic events.
Notes
The experimental treatment was significantly less beneficial than the control treatment.
Randomised controlled trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because of administrative reasons, there was no relaxin available or the researcher was off duty. Infertile females. No losses to follow up.
Data
Characteristics of the patients not presented. RCT placebo group included 45 women, the non‐RCT no treatment group included 73 women.
Comparisons
Two RCT arms, the control arm women were compared to similarly treated eligible but non‐randomised women. The RCT treatment women were treated with pig relaxin gel. The control women were given a placebo.
Outcomes
Clinical outcomes were measured in all women, who were followed up for 20 weeks. Main outcome was pregancies.
N of 1 trial with concurrent eligible patients randomized to standard practice. The non‐N of 1 patients were not in the trial because they were randomized to standard practice. Patients with irreversible chronic airflow limitation. N of 1 group lost 2 (14%) patients to follow up, in standard practice 3 (25%) patients were lost to follow up.
Data
N of 1 patients were compared to patients randomized to be treated in standard practice. N of 1 patients were mean 68 (7) years. Standard practice patients were mean 71 (8) years.
Comparisons
Two RCT arms, patients were randomized to N of 1 trial or standard practice. In the N of 1 trial, patients received theophylline for 10 days and placebo for 10 days in a randomized cross over design. For standard practice patients theophylline was stopped and resumed if their dyspnoea worsened.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 6 months. Main outcome was improvement (6 month distance minus baseline distance) in six minutes walking distance (m).
Notes
The walking distance was not significantly different between N of 1 and standard practice.
N of 1 trial with concurrent eligible patients randomized to standard practice. The non‐N of 1 patients were not in the trial because they were randomized to standard practice. Patients with irreversible chronic airflow limitation. N of 1 group lost 3 (9%) patients to follow up, in standard practice 4 (12%) patients were lost to follow up.
Data
N of 1 patients were compared to patients randomized to be treated in standard practice. N of 1 patients were mean 69 (8) years. Standard practice patients were mean 69 (7) years.
Comparisons
Two RCT arms, patients were randomized to N of 1 trial or standard practice. In the N of 1 trial, patients received theophylline for 10 days and placebo for 10 days in a randomized cross over design. For standard practice patients theophylline was stopped and resumed if their dyspnoea worsened.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 6 months and 1 year. Main outcome was improvement in six minutes walking distance at 6 months.
Notes
The walking distance was not significantly different between N of 1 and standard practice.
Retrospective review of a randomised trial with concurrent eligible patients outside of the RCT. The eligible non‐RCT patients were not in the RCT because of patient refusal (75), or patients were not referred by clinicians (29). Asymptomatic patients undergoing carotic endarterectomy. Unclear, but unlikely losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients similarly treated. The 54 RCT patients treated with carotid endarterectomy were mean 66 (1) years. The 104 non‐RCT patients treated with carotid endarterectomy were mean 67 (1) years.
Comparisons
Two RCT arms, the experimental arm patients were compared to similarly treated eligible but non‐randomised patients. The experimental treatment was carotid endarterectomy.
Outcomes
Clinical outcomes were measured in all patients. Patients were followed up during hospital stay. Main outcome was mortality.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because the patients refused. Hypertensive patients attending primary care centers. Losses to follow up unknown.
Data
Some characteristics of the patients presented. Individual education RCT patients were mean 60 years, 78 men and 128 women. Individual education non‐RCT patients were mean 63 years, 24 men and 45 women.
Comparisons
Three RCT arms, two arms were compared with similarly treated eligible non‐RCT patients. Experimental not compared: team education. Experimental that was compared: Individual education. Control: the group received no education.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 2 months. Main outcome was lack of blood pressure control.
Notes
The RCT treatments were not statistically different.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because the patients refused. Hypertensive patients attending primary care centers. Losses to follow up unknown.
Data
Some characteristics of the patients presented. Control RCT patients were mean 61 years, 75 men and 123 women. Control non‐RCT patients were mean 65 years, 26 men and 38 women.
Comparisons
Three RCT arms, two arms were compared with similarly treated eligible non‐RCT patients. Experimental not compared: team education. Experimental that was compared: Individual education. Control: the group received no education.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 2 months. Main outcome was lack of blood pressure control.
Notes
The RCT treatments were not statistically different.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because the patients refused. Patients undergoing prostate biopsy. Unclear, but probably no losses to follow up.
Data
Patient characteristics not presented. The 45 patients in the RCT control group were given a mask with only air coming through. The 14 non‐RCT patients were not given anything.
Comparisons
Two RCT arms, the RCT control arm patients were compared to eligible non‐RCT patients who were given similar treatment. Experimental: entonox gas. Control: placebo.
Outcomes
Outcomes were assessed in all patients. Patients were followed up for 30 min after the procedure. Main outcome was pain.
Notes
The experimental treatment was more effective than control.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they did not consent to randomisation. School entry girls of height 2 SDs or more below the mean height for their age. Two (25%) girls were lost to follow up in the RCT control group, three (14%) girls were lost to follow up in the non‐RCT observation group.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT patients were mean 6 (1) years. Non‐RCT patients were mean 6 (1) years.
Comparisons
Two RCT arms, the control arm patients were compared with similarly treated eligible non‐RCT patients. The experimental arm patients were treated with growth hormone. The control patients were not treated.
Outcomes
Clinical outcomes were assessed in all girls every 6 months for 6 years. Main outcome in this study was current height minus target height (cm).
Notes
The experimental arm of the RCT was more effective than no treatment.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients refused randomization because of preference for treatment, but consented to follow up. The non‐RCT patients were followed‐ up identically to the RCT patients. Male alcoholic veterans who sought treatment. In the RCT day care, 7 (29%) patients were lost to follow up. In the non‐RCT day care, 13 (20%) patients were lost to follow up.
Data
Non‐RCT patients were compared to RCT patients who received the same treatment. RCT patients receiving day care were mean 43 (7) years. Non‐RCT patients receiving day care were mean 43 (7) years.
Comparisons
Two RCT arms, each in common use, and each of them were compared with similarly treated eligible non‐RCT patients. Control: Day care. Control: In patients.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 1 year. Main outcome was days of alcohol use during 30 days in the 12th month.
Notes
The two RCT treatments were not significantly different.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients refused randomization because of preference for treatment, but consented to follow up. The non‐RCT patients were followed‐ up identically to the RCT patients. Male alcoholic veterans who sought treatment. In the RCT in patient, 3 (13%) patients were lost to follow up. In the non‐RCT in patient, 3 (10%) patients were lost to follow up.
Data
Non‐RCT patients were compared to RCT patients who received the same treatment. RCT patients treated as in patients were mean 41 (9) years. Non‐ RCT patients treated as in patients were mean 38 (8) years.
Comparisons
Two RCT arms, each in common use, and each of them were compared with similarly treated eligible non‐RCT patients. Control: Day care. Control: In patients.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 1 year. Main outcome was days of alcohol use during 30 days in the 12th month.
Notes
The two RCT treatments were not significantly different.
Randomised trial with concurrent eligible patients outside of the RCT in a preference trial. The non‐RCT patients were not in the RCT because they did not accept randomisation, these patients were treated according to choice. The non‐RCT patients were followed‐ up identically to the RCT patients. Male veterans with current cocaine use disorder diagnosis who sought treatment. In the RCT day care, 2 (3%) patients were lost to follow up. In the non‐RCT day care, 3 (8%) patients were lost to follow up.
Data
Non‐RCT patients were compared to RCT patients who received the same treatment. RCT patients receiving day care were mean 34 (6) years. Non‐RCT patients receiving day care were mean 36 (6) years.
Comparisons
Two RCT arms, each in common use, and each of them were compared with similarly treated eligible non‐RCT patients. Control: Day care. Control: In patients.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 1 year. Main outcome was days of cocaine use during 30 days in the 12th month.
Notes
The two treatments were not significantly different.
Randomised trial with concurrent eligible patients outside of the RCT in a preference trial. The non‐RCT patients were not in the RCT because they did not accept randomisation, these patients were treated according to choice. The non‐RCT patients were followed‐ up identically to the RCT patients. Male veterans with current cocaine use disorder diagnosis who sought treatment. In the RCT in patient, 6 (11%) patients were lost to follow up. In the non‐RCT in patient, 1 (5%) patient was lost to follow up.
Data
Non‐RCT patients were compared to RCT patients who received the same treatment. RCT patients treated as in patients were mean 34 (6) years. Non‐ RCT patients treated as in patients were mean 35 (5) years.
Comparisons
Two RCT arms, each in common use, and each of them were compared with similarly treated eligible non‐RCT patients. Control: Day care. Control: In patients.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 1 year. Main outcome was days of cocaine use during 30 days in the 12th month.
Notes
The two treatments were not significantly different.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients refused randomization because of preference for treatment, but consented to follow up. The non‐RCT patients were followed‐ up identically to the RCT patients. Adult patients undergoing endoscopic investigation of upper GI tract. None were lost to follow up in the sedation groups.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT sedation patients were mean 73 (17) years, 7 women, 7 men. Non‐RCT sedation patients were mean 67 (16) years, 33 women, 32 men.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Experimental: sedation with Midazolam during endoscopy. Control: acupuncture during endoscopy.
Outcomes
Clinical outcomes were assessed in all patients. Patients were followed up for 2 hours. Main outcome was patient assessment of troublesomeness.
Notes
The experimental arm of the RCT was more effective than no treatment.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients refused randomization because of preference for treatment, but consented to follow up. The non‐RCT patients were followed‐ up identically to the RCT patients. Adult patients undergoing endoscopic investigation of upper GI tract. Two (14%) patients were lost to follow up in the RCT sedation group, none were lost to follow up in the non‐RCT sedation group.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT acupuncture patients were mean 69 (17) years, 5 women, 7 men. Non‐RCT acupuncture patients were mean 62 (16) years, 10 women, 11 men.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Experimental: sedation with Midazolam during endoscopy. Control: acupuncture during endoscopy.
Outcomes
Clinical outcomes were assessed in all patients. Patients were followed up for 2 hours. Main outcome was patient assessment of troublesomeness.
Notes
The experimental arm of the RCT was more effective than no treatment.
Zelen trial where those randomized to active treatment but refused were observed, the same as the Zelen control group. Patients with resectable but poor‐prognosis gastric carcinoma. Two (8%) patients were lost to follow up in the Zelen control group, no losses to follow up in the other group.
Data
Characteristics of Zelen patients who refused are presented and compared to Zelen control patients who received the same treatment. Zelen control patients were on average 56 (41 to 67) years, 17 men and 6 women. Patients who refused were on average 61 (55 to 66) years, 9 men and 1 women.
Comparisons
Two Zelen arms, the control arm patients were compared with similarly treated eligible Zelen patients who refused the active treatment. The experimental arm patients were treated with combined 5‐Fluorouracil and radiation therapy as a surgical adjuvant. The control patients were not treated.
Outcomes
Clinical outcomes were assessed in all patients and they were followed up for 8 years. Main outcome in this study was 5 year mortality.
Notes
The experimental Zelen arm was favored over no treatment.
Randomised controlled trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were participants in a patient preference trial who refused to be randomised due to preference.The non‐RCT patients were followed up similarly to those in the RCT. Patients undergoing endoscopy. None of the oral tube patients were lost to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. Oral tube RCT patients were median 62 (22 to 88) years, 31 women and 50 men. Oral tube non‐RCT patients were median 62 (22 to 90) years, 157 women and 168 men.
Comparisons
Two RCT arms, both arms were compared with eligible non‐RCT patients who received similar treatment. The experimental treatment was use of oral tube for endoscopy. The control treatment was nasal tube.
Outcomes
Patients were followed up during procedure. Main outcome was satisfaction.
Notes
The two RCT treatments were not statistically different.
Randomised controlled trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were participants in a patient preference trial who refused to be randomised due to preference.The non‐RCT patients were followed up similarly to those in the RCT. Patients undergoing endoscopy. Nine patients were lost to follow up in the RCT nasal tube group. 48 nasal tube non‐RCT pateints were excluded during follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. Nasal tube RCT patients were median 54 (26 to 79) years, 26 women and 51 men. Nasal tube non‐RCT patients were median 57 (16 to 88) years, 179 women and 208 men.
Comparisons
Two RCT arms, both arms were compared with eligible non‐RCT patients who received similar treatment. The experimental treatment was use of oral tube for endoscopy. The control treatment was nasal tube.
Outcomes
Patients were followed up during procedure. Main outcome was satisfaction.
Notes
The two RCT treatments were not statistically different.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were participants in a preference trial who refused to be randomized due to preference. Postmenopausal women as close to menopause as possible. In the RCT hormone replacement therapy group 54 (11%) women were lost to follow up, in the hormone replacement therapy choice group 16 (7%) women were lost to follow up.
Data
Characteristics of choice patients presented and compared to RCT patients who received the same treatment. Hormone replacement therapy RCT patients were on average 50 (45 to 57) years. Hormone replacement therapy choice patients were on average 50 (45 to 56) years.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Experimental: hormone replacement therapy. Control: no hormone replacement therapy.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for an average of 5 years. Main outcome was forearm fractures.
Notes
The experimental treatment was significantly more beneficial than the control treatment.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were participants in a preference trial who refused to be randomized due to preference. Postmenopausal women as close to menopause as possible. In the RCT no hormone replacement therapy group 55 (11%) women were lost to follow up, in the no hormone replacement therapy choice group 89 (11%) women were lost to follow up.
Data
Characteristics of choice patients presented and compared to RCT patients who received the same treatment. No hormone replacement therapy RCT patients were on average 50 (45 to 58) years. No hormone replacement therapy choice patients were on average 51 (45 to 58) years.
Comparisons
Two RCT arms, each of them were compared with similarly treated eligible non‐RCT patients. Experimental: hormone replacement therapy. Control: no hormone replacement therapy.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for an average of 5 years. Main outcome was forearm fractures.
Notes
The experimental treatment was significantly more beneficial than the control treatment.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they declined randomisation, these patients were treated according to choice. The non‐RCT patients were followed‐ up identically to the RCT patients. Pregnant women requesting early prenatal diagnosis for advanced maternal age. In the RCT early amniocentesis group, one (2%) woman was lost to follow up. In the non‐RCT early amniocentesis group, 3 (4%) women were lost to follow up.
Data
Non‐RCT patients were compared to RCT patients who received the same treatment. RCT patients receiving early amniocentesis were on average 38 years. Non‐RCT patients receiving early amniocentesis were on average 38 years.
Comparisons
Two RCT arms, each in common use, and each of them were compared with similarly treated eligible non‐RCT patients. Control: early amniocentesis. Control: chorionic villus sampling.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 1 year. Main outcome was fetal mortality.
Notes
Chorionic villus sampling resulted in much lower fetal mortality than early amniocentesis.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they declined randomisation, these patients were treated according to choice. The non‐RCT patients were followed‐ up identically to the RCT patients. Pregnant women requesting early prenatal diagnosis for advanced maternal age. In the RCT chorionic villus sampling, 10 (17%) women were lost to follow up. In the non‐RCT chorionic villus sampling, 3 (12%) women were lost to follow up.
Data
Non‐RCT patients were compared to RCT patients who received the same treatment. RCT patients receiving chorionic villus sampling were on average 38 years. Non‐ RCT patients receiving chorionic villus sampling were on average 38 years.
Comparisons
Two RCT arms, each in common use, and each of them were compared with similarly treated eligible non‐RCT patients. Control: early amniocentesis. Control: chorionic villus sampling.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 1 year. Main outcome was fetal mortality.
Notes
Chorionic villus sampling resulted in much lower fetal mortality than early amniocentesis.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients refused randomization because of preference for one of the tests. Women who requested fetal karyotyping with singleton pregnancy at 10 to 23 weeks gestation. One (0.2%) woman in the non‐RCT amniocentesis group was lost to follow up. No other losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT amniocentesis patients were on average 38 (24 to 45) years. Non‐RCT amniocentesis patients were on average 38 (23 to 45) years.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The experimental arm patients were tested with the amniocentesis technique. The control patients were tested with chorionic villus sampling.
Outcomes
Clinical outcomes were assessed in all women, they were followed up until delivery. Main outcome in this study was spontaneous fetal death.
Notes
The control treatment was safer (fewer spontaneous deaths) than the experimental treatment.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients refused randomization because of preference for one of the tests. Women who requested fetal karyotyping with singleton pregnancy at 10 to 23 weeks gestation. No losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT chorionic villus sampling patients were on average 38 (22 to 46) years. Non‐RCT chorionic villus sampling patients were on average 38 (22 to 46) years.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The experimental arm patients were tested with the amniocentesis technique. The control patients were tested with chorionic villus sampling.
Outcomes
Clinical outcomes were assessed in all women, they were followed up until delivery. Main outcome in this study was spontaneous fetal death.
Notes
The control treatment was safer (fewer spontaneous deaths) than the experimental treatment.
Randomised trial with concurrent eligible patients outside of the RCT. The eligible patients treated outside of the RCT were considered training of the investigating physicians. Patients with chronic plantar fascitis who had failed to respond after at least three attempts of interventional conservative treatment. Four patients were lost to follow up in the RCT sham group, and four patients were lost to follow up in the non‐RCT group.
Data
Characteristics of patients not presented. 148 RCT sham treatment patients were compared to 51 eligible non‐randomised patients who were treated similarly.
Comparisons
Two RCT arms, the RCT control arm patients were compared to eligible non‐RCT patients who were given similar treatment. Experimental: Electrohydraulic high‐energy shock‐wave treatment. Control: Sham shock‐wave treatment.
Outcomes
Patients were followed up for 3 months. Main outcome was success of treatment.
Notes
The experimental treatment was more effective than control treatment
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because their parent/s declined randomisation, these patients were treated according to parental choice. The non‐RCT patients were followed‐ up identically to the RCT patients. Children severely affected with recurrent throat infection. Children were followed for 3 years. In the RCT, 9 (10%) children were lost to follow up during the first year. In the non‐randomised groups, 11 (11%) children were lost to follow up during the first year.
Data
Non‐RCT patients were compared to RCT patients who received the same treatment. All children were 15 years or younger. RCT patients receiving tonsillectomy were 21 boys and 22 girls. Non‐RCT patients receiving tonsillectomy were 19 boys and 33 girls.
Comparisons
Two RCT arms, each in common use, and each of them were compared with similarly treated eligible non‐RCT patients. Control‐T: Tonsillectomy. Control‐O: Observation without surgery.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 1, 2 and 3 years. Main outcome was mean number of counting episodes per year.
Notes
The surgical treatment showed greater effectiveness than non‐surgical treatment.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because their parent/s declined randomisation, these patients were treated according to parental choice. The non‐RCT patients were followed‐ up identically to the RCT patients. Children severely affected with recurrent throat infection. Children were followed for 3 years. In the RCT, 9 (10%) children were lost to follow up during the first year. In the non‐randomised groups, 11 (11%) children were lost to follow up during the first year.
Data
Non‐RCT patients were compared to RCT patients who received the same treatment. All children were 15 years or younger. RCT patients under observation were 19 boys and 29 girls. Non‐RCT patients under observation were 29 boys and 15 girls.
Comparisons
Two RCT arms, each in common use, and each of them were compared with similarly treated eligible non‐RCT patients. Control‐T: Tonsillectomy. Control‐O: Observation without surgery.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 1, 2 and 3 years. Main outcome was mean number of counting episodes per year.
Notes
The surgical treatment showed greater effectiveness than non‐surgical treatment.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because their parent/s declined randomisation, these patients were treated according to parental choice. The non‐RCT patients were followed‐ up identically to the RCT patients. Children with persistent and/or recurrent otitis media. In the RCT, 8 (8%) children were lost to follow up during the first year. In the non‐randomised groups, 10 (9%) children were lost to follow up during the first year.
Data
Non‐RCT patients were compared to RCT patients who received the same treatment. RCT patients receiving adenoidectomy were mean 6 (2) years, 35 boys and 17 girls. Non‐RCT patients receiving adenoidectomy were mean 6 (3) years, 29 boys and 18 girls.
Comparisons
Two RCT arms, each in common use, and each of them were compared with similarly treated eligible non‐RCT patients. Control‐A: Adenoidectomy. Control‐O: Observation without surgery.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 1, 2 and 3 years. Main outcome was weeks per year with otitis media.
Notes
The surgical treatment showed greater effectiveness than non‐surgical treatment.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because their parent/s declined randomisation, these patients were treated according to parental choice. The non‐RCT patients were followed‐ up identically to the RCT patients. Children with persistent and/or recurrent otitis media. In the RCT, 8 (8%) children were lost to follow up during the first year. In the non‐randomised groups, 10 (9%) children were lost to follow up during the first year.
Data
Non‐RCT patients were compared to RCT patients who received the same treatment. RCT patients under observation were mean 5 (2) years, 33 boys and 14 girls. Non‐ RCT patients under observation were mean 6 (3) years, 41 boys and 26 girls.
Comparisons
Two RCT arms, each in common use, and each of them were compared with similarly treated eligible non‐RCT patients. Control‐A: Adenoidectomy. Control‐O: Observation without surgery.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for 1, 2 and 3 years. Main outcome was weeks per year with otitis media.
Notes
The surgical treatment showed greater effectiveness than non‐surgical treatment.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the trial because they were treated by clinicians who were not involved in the RCT and hence, these patients were not invited to take part in the trial. RCT looking at wound infection rates and mortality after colorectal operations in patients undergoing elective colorectal operations. No losses to follow up.
Data
Characteristics of the non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT patients were mean 60 years, 31 males and 30 females. Non‐RCT patients were mean 65 years, 36 males and 47 females.
Comparisons
Two RCT arms, the experimental arm patients were compared with similarly treated non‐RCT patients. The experimental arm patients received a combined oral and parenteral regimen of antimicrobial prophylaxis whereas the control patients received purely parenteral antimicrobial prophylaxis.
Outcomes
Clinical outcomes were measured in all patients. Patients were followed for 30 days. Main outcome in this study was mortality.
Notes
The experimental treatment was significantly better then control.
Randomised controlled trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were participants in a patient preference trial who refused to be randomised due to preference. The non‐RCT patients were followed up similarly to those in the RCT. Heroin users receiving treatment at a specialist addiction service. 15 of the 107 RCT patients treated with buprenorphine were lost to follow up. 28 of the 163 eligible non‐RCT patients given similar treatment were lost to follow up.
Data
Characteristics of non‐RCT patients compared to RCT patients who received the same treatment were not presented. 107 RCT patients were treated with buprenorphine, 163 eligible non‐RCT patients were given similar treatment.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The experimental arm patients received buprenorphine. The control patients received lofexidine.
Outcomes
Clinical outcomes were measured in all patients. Patients were followed up for one month. Main outcome was abstinence at one month.
Randomised controlled trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were participants in a patient preference trial who refused to be randomised due to preference. The non‐RCT patients were followed up similarly to those in the RCT. Heroin users receiving treatment at a specialist addiction service. 21 of the 103 RCT patients treated with lofexidine were lost to follow up. 18 of the 108 eligible non‐RCT patients given similar treatment were lost to follow up.
Data
Characteristics of non‐RCT patients compared to RCT patients who received the same treatment were not presented. 103 RCT patients were treated with lofexidine, 108 eligible non‐RCT patients were given similar treatment.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The experimental arm patients received buprenorphine. The control patients received lofexidine.
Outcomes
Clinical outcomes were measured in all patients. Patients were followed up for one month. Main outcome was abstinence at one month.
Randomised controlled trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the trial because they refused randomization. Patients diagnosed with single vessel disease of the LAD, including urgent patients. Unclear lossess to follow up.
Data
Characteristics of non‐RCT patients compared to RCT patients who received the same treatment were not presented. 50 RCT percutaneous transluminal coronary angioplasty patients were compared to 25 non‐randomised percutaneous transluminal coronary angioplasty patients.
Comparisons
Two RCT arms, the control arm patients were compared with similarly treated eligible non‐RCT patients. The experimental arm patients received minimally invasive direct coronary artery bypass graft. The control patients received percutaneous transluminal coronary angioplasty.
Outcomes
Patients were followed up at 3 months, 1 year, and 3 years. Main outcome was composite endpoint of cardiac‐related‐deaths at 1 year.
Randomised controlled trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the trial because the patients or their physician refused randomization, but consented to information extraction from medical records. High risk patients in major surgery. It is unclear but unlikely that there were any losses to follow up.
Data
Characteristics of the non‐randomised patients compared to RCT patients who received the same treatment. RCT epidural patients were on average 71 (38 to 90) years, 139 men and 86 women. Non‐RCT epidural patients were on average 71 (38 to 90) years, 33 men and 19 women.
Comparisons
Two RCT arms, the control arm patients were compared with non‐randomised patients who received similar treatment. Experimental: epidural block inserted preoperatively and maintained throughout and for 72 h after surgery, this in addition to general anesthetic during surgery. Control: general anesthetic during surgery and intravenous opioids.
Outcomes
Outcomes were assessed in all patients. Patients were followed for 30 days postoperatively. Main outcome was 30 days mortality.
Randomised controlled trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the trial because the patients or their physician refused randomization, but consented to information extraction from medical records. High risk patients in major surgery. It is unclear but unlikely that there were any losses to follow up.
Data
Characteristics of the non‐randomised patients compared to RCT patients who received the same treatment. RCT control patients were on average 69 (26 to 92) years, 245 men and 177 women. Non‐RCT control patients were on average 68 (30 to 93) years, 43 men and 45 women.
Comparisons
Two RCT arms, the control arm patients were compared with non‐randomised patients who received similar treatment. Experimental: epidural block inserted preoperatively and maintained throughout and for 72 h after surgery, this in addition to general anesthetic during surgery. Control: general anesthetic during surgery and intravenous opioids.
Outcomes
Outcomes were assessed in all patients. Patients were followed for 30 days postoperatively. Main outcome was 30 days mortality.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they declined randomisation. The non‐RCT patients were followed‐ up identically to the RCT patients. Patients undergoing oocyte retrieval via laparoscopy. No losses to follow up.
Data
Non‐RCT patients were compared to RCT patients who received the same treatment. Ages unknown.
Comparisons
Two RCT arms, each in common use, and each of them were compared with similarly treated eligible non‐RCT patients. Control‐N: Aneasthetic with NOx. Control‐O: Anaesthetic without NOx.
Outcomes
Clinical outcomes were assessed in all the patients. Length of followed up unknown. Main outcome was number not pregnant.
Notes
The two RCT treatments were not statistically different.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they declined randomisation. The non‐RCT patients were followed‐ up identically to the RCT patients. Patients undergoing oocyte retrieval via laparoscopy. No losses to follow up.
Data
Non‐RCT patients were compared to RCT patients who received the same treatment. Ages unknown.
Comparisons
Two RCT arms, each in common use, and each of them were compared with similarly treated eligible non‐RCT patients. Control‐N: Anaesthetic with NOx. Control‐O: Anaesthetic without NOx.
Outcomes
Clinical outcomes were assessed in all the patients. Length of followed up unknown. Main outcome was number not pregnant.
Notes
The two RCT treatments were not statistically different.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because their parent/s declined randomisation, these patients were treated according to parental choice. The non‐RCT patients were followed‐ up identically to the RCT patients. Children with persistent bilateral otitis media with effusion for 4 to 6 months. In the RCT ventilation tube, 3 (3%) children were lost to follow up. In the non‐RCT ventilation tube, 8 (22%) children were lost to follow up.
Data
Non‐RCT patients were compared to RCT patients who received the same treatment. RCT patients receiving ventilation tube were on average 18 (16 to 25) months, 55 boys and 38 girls. Non‐RCT patients receiving ventilation tube were on average 19 (14 to 22) months, 21 boys and 15 girls.
Comparisons
Two RCT arms, each in common use, and each of them were compared with similarly treated eligible non‐RCT patients. Control ventilation tube. Control watchful waiting.
Outcomes
Clinical outcomes were assessed in all the patients. Children were followed for 1 year. Main outcome was mean time with effusion.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because their parent/s declined randomisation, these patients were treated according to parental choice. The non‐RCT patients were followed‐ up identically to the RCT patients. Children with persistent bilateral otitis media with effusion for 4 to 6 months. In the RCT watchful waiting, 8 (9%) children were lost to follow up. In the non‐RCT watchful waiting, 19 (20%) children were lost to follow up.
Data
Non‐RCT patients were compared to RCT patients who received the same treatment. RCT patients under observation were on average 19 (14 to 23) months, 55 boys and 39 girls. Non‐ RCT patients under observation were on average 19 (15 to 26) months, 49 boys and 48 girls.
Comparisons
Two RCT arms, each in common use, and each of them were compared with similarly treated eligible non‐RCT patients. Control ventilation tube. Control watchful waiting.
Outcomes
Clinical outcomes were assessed in all the patients. Children were followed for 1 year. Main outcome was mean time with effusion.
Randomised controlled trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were participants in a patient preference trial who refused to be randomised due to preference.The non‐RCT patients were followed up similarly to those in the RCT. Pregnant women with fetus < 63 days gestational age. Nine % losses to follow up.
Data
Characteristics of the non‐randomised patients compared to RCT patients. Women in the RCT were on average 26 (18 to 44) years, 111 women. Women in the preference trial were on average 27 (18 to 45) years, 922 women.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The experimental arm patients received medical abortion. The control patients received surgical abortion.
Outcomes
Women were followed up for 2 weeks. Main outcome was satisfied or very satisfied at two weeks after abortion.
Notes
The control arm of the RCT gave more satisfied women compared with the experimental treatment.
Randomised controlled trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were participants in a patient preference trial who refused to be randomised due to preference.The non‐RCT patients were followed up similarly to those in the RCT. Pregnant women with fetus < 63 days gestational age. Nine % loss to follow up.
Data
Characteristics of the non‐randomised patients compared to RCT patients. Women in the RCT were on average 26 (18 to 44) years, 111 women. Women in the preference trial were on average 27 (18 to 45) years, 922 women.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The experimental arm patients received medical abortion. The control patients received surgical abortion.
Outcomes
Women were followed up for 2 weeks. Main outcome was satisfied or very satisfied at two weeks after abortion.
Notes
The control arm of the RCT gave more satisfied women compared with the experimental treatment.
Two randomised controlled trials with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the trial because the patients refused randomization because of strong preference for treatment. Women with breast cancer, node‐positive patients previously treated with mastectomy. Combined for trials a, b, c and d, losses to follow up were 4% in the RCT group and 12% in the non‐RCT group.
Data
Characteristics of the non‐randomised patients compared to RCT patients who received the same treatment. RCT a, 2, 3 x CMF patients were on average 50 (29 to 70) years, 145 women. Non‐RCT a, 2, 3 x CMF patients were on average 49 (21 to 76) years, 72 women.
Comparisons
Two RCT trials: Trial one including a, b, c and d with four arms, all of them compared with similarly treated non‐randomised patients. Trial two including e and f with two arms, both of them compared with similarly treated non‐randomised patients.
Outcomes
Outcomes were assessed in all patients. Patients were followed for 6 years. Main outcome was relapse + death, and mortality.
Two randomised controlled trials with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the trial because the patients refused randomization because of strong preference for treatment. Women with breast cancer, node‐positive patients previously treated with mastectomy. Combined for trials a, b, c and d, losses to follow up were 4% in the RCT group and 12% in the non‐RCT group.
Data
Characteristics of the non‐randomised patients compared to RCT patients who received the same treatment. RCT b, 2, 6 x CMF patients were on average 51 (25 to 80) years, 144 women. Non‐RCT b, 2, 6 x CMF patients were on average 51 (27 to 70) years, 104 women.
Comparisons
Two RCT trials: Trial one including a, b, c and d with four arms, all of them compared with similarly treated non‐randomised patients. Trial two including e and f with two arms, both of them compared with similarly treated non‐randomised patients.
Outcomes
Outcomes were assessed in all patients. Patients were followed for 6 years. Main outcome was relapse + death, and mortality.
Two randomised controlled trials with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the trial because the patients refused randomization because of strong preference for treatment. Women with breast cancer, node‐positive patients previously treated with mastectomy. Combined for trials a, b, c and d, losses to follow up were 4% in the RCT group and 12% in the non‐RCT group.
Data
Characteristics of the non‐randomised patients compared to RCT patients who received the same treatment. RCT c, 2, 3 x CMF + tamoxifen patients were on average 58 (33 to 72) years, 93 women. Non‐RCT c, 2, 3 x CMF + tamoxifen patients were on average 60 (32 to 79) years, 42 women.
Comparisons
Two RCT trials: Trial one including a, b, c and d with four arms, all of them compared with similarly treated non‐randomised patients. Trial two including e and f with two arms, both of them compared with similarly treated non‐randomised patients.
Outcomes
Outcomes were assessed in all patients. Patients were followed for 6 years. Main outcome was relapse + death, and mortality.
Two randomised controlled trials with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the trial because the patients refused randomization because of strong preference for treatment. Women with breast cancer, node‐positive patients previously treated with mastectomy. Combined for trials a, b, c and d, losses to follow up were 4% in the RCT group and 12% in the non‐RCT group.
Data
Characteristics of the non‐randomised patients compared to RCT patients who received the same treatment. RCT d, 6 x CMF + tamoxifen patients were on average 58 (34 to 71) years, 91 women. Non‐RCT d, 6 x CMF + tamoxifen patients were on average 57 (35 to 80) years, 29 women.
Comparisons
Two RCT trials: Trial one including a, b, c and d with four arms, all of them compared with similarly treated non‐randomised patients. Trial two including e and f with two arms, both of them compared with similarly treated non‐randomised patients.
Outcomes
Outcomes were assessed in all patients. Patients were followed for 6 years. Main outcome was relapse + death, and mortality.
Two randomised controlled trials with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the trial because the patients refused randomization because of strong preference for treatment. Women with breast cancer, node‐positive patients previously treated with mastectomy. Combined for group e and f, losses to follow up were 4% in both the RCT and the non‐RCT groups.
Data
Characteristics of the non‐randomised patients compared to RCT patients who received the same treatment. RCT e, 6 x CMF patients were on average 55 (28 to 71) years, 101 women. Non‐RCT e, 6 x CMF patients were on average 53 (27 to 78) years, 88 women.
Comparisons
Two RCT trials: Trial one including a, b, c and d with four arms, all of them compared with similarly treated non‐randomised patients. Trial two including e and f with two arms, both of them compared with similarly treated non‐randomised patients.
Outcomes
Outcomes were assessed in all patients. Patients were followed for 6 years. Main outcome was relapse + death, and mortality.
Two randomised controlled trials with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the trial because the patients refused randomization because of strong preference for treatment. Women with breast cancer, node‐positive patients previously treated with mastectomy. Combined for group e and f, losses to follow up were 4% in both the RCT and the non‐RCT groups.
Data
Characteristics of the non‐randomised patients compared to RCT patients who received the same treatment. RCT f, 6 x CMF + radiotherapy patients were on average 55 (29 to 69) years, 98 women. Non‐RCT f, 6 x CMF + radiotherapy patients were on average 51 (33 to 75) years, 41 women.
Comparisons
Two RCT trials: Trial one including a, b, c and d with four arms, all of them compared with similarly treated non‐randomised patients. Trial two including e and f with two arms, both of them compared with similarly treated non‐randomised patients.
Outcomes
Outcomes were assessed in all patients. Patients were followed for 6 years. Main outcome was relapse + death, and mortality.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they refused randomization. Helsinki businessmen. No losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT control patients were on average 48 (40 to 55) years. Non‐RCT patients were on average 47 (40 to 55) years.
Comparisons
Two RCT arms, the control arm patients were compared with similarly treated eligible non‐RCT patients. The experimental arm patients took part in a cardiovascular primary prevention. The control patients were given health checks without intervention.
Outcomes
The population was followed for 18 years. The main outcome in this study was mortality.
Randomised trial with concurrent eligible patients outside of the RCT. We do not know why the non‐RCT patients were not in the RCT. Children of age <18 years with proven Hodgkin's disease of pathologic I or II, no prior radiotherapy or chemotherapy. 15 (29%) children were lost to follow up in the RCT involved‐field radiotherapy group, in the non‐RCT involved‐field radiotherapy group 8 (50%) children were lost to follow up.
Data
Characteristics of patients were not presented.
Comparisons
Three RCT arms, each arm were compared with similarly treated eligible non‐RCT patients. Involved‐field radiotherapy, involved‐field radiotherapy + chemotherapy, extended‐field radiotherapy.
Outcomes
Clinical outcomes were assessed in all the children. Patients were followed for 208 weeks. Main outcomes were death and relapse.
Notes
Significant differences were found between the RCT treatments.
Randomised trial with concurrent eligible patients outside of the RCT. We do not know why the non‐RCT patients were not in the RCT. Children of age <18 years with proven Hodgkin's disease of pathologic I or II, no prior radiotherapy or chemotherapy. 43(39%) children were lost to follow up in the RCT involved‐field radiotherapy + chemotherapy group, in the non‐RCT involved‐field radiotherapy + chemotherapy group 3 (38%) children were lost to follow up.
Data
Characteristics of patients were not presented.
Comparisons
Three RCT arms, each arm were compared with similarly treated eligible non‐RCT patients. Involved‐field radiotherapy, involved‐field radiotherapy + chemotherapy, extended‐field radiotherapy.
Outcomes
Clinical outcomes were assessed in all the children. Patients were followed for 208 weeks. Main outcomes were death and relapse.
Notes
Significant differences were found between the RCT treatments.
Randomised trial with concurrent eligible patients outside of the RCT. We do not know why the non‐RCT patients were not in the RCT. Children of age <18 years with proven Hodgkin's disease of pathologic I or II, no prior radiotherapy or chemotherapy. 21 (34%) children were lost to follow up in the RCT extended‐field radiotherapy group, in the non‐RCTextended‐field radiotherapy group 10 (45%) children were lost to follow up.
Data
Characteristics of patients were not presented.
Comparisons
Three RCT arms, each arm were compared with similarly treated eligible non‐RCT patients. Involved‐field radiotherapy, involved‐field radiotherapy + chemotherapy, extended‐field radiotherapy.
Outcomes
Clinical outcomes were assessed in all the children. Patients were followed for 208 weeks. Main outcomes were death and relapse.
Notes
Significant differences were found between the RCT treatments.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because of physician preference for an early invasive approach. Patients who developed clinical cardiogenic shock within 48 hours of the onset of acute myocardial infarction. Unclear if losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT patients were mean 66 (10) years, 23 men and 9 women. Non‐RCT patients were mean 60 (16) years, 15 men and 9 women.
Comparisons
Two RCT arms, the experimental arm patients were compared with similarly treated eligible non‐RCT patients. The experimental arm patients underwent emergency angiography followed immediately by revascularization when indicated. The control patients received initial medical management.
Outcomes
Clinical outcomes were assessed in all patients, patients were followed for 1 month. Main outcome in this study was death.
Notes
No difference was shown between the two RCT treatments.
Randomised controlled trial with concurrent eligible patients outside of the trial. The non‐RCT patients were not in the trial because they refused randomisation. Cardiac surgery patients. RCT forced‐air warming group lost one (3%) patient to follow up. Non‐RCT forced‐air warming lost two (25%) patients to follow up.
Data
Characteristics of the non‐randomised patients compared to RCT patients who received the same treatment. RCT forced air warming patients were on average 68 (51 to 89) years, 23 men and 7 women. Non‐RCT forced air warming patients were on average 63 (54 to 81) years, 6 men and 2 women.
Comparisons
Two RCT arms, both arms were compared with non‐randomised patients who received similar treatment. Experimental: forced air warming. Control: usual care with warm blankets and overhead heat lamps.
Outcomes
Outcomes were assessed in all patients. Patients were followed for 3 years. Main outcome was postoperative temperature at 6 hours.
Notes
The two experimental treatments were not significantly different.
Randomised controlled trial with concurrent eligible patients outside of the trial. The non‐RCT patients were not in the trial because they refused randomisation. Cardiac surgery patients. RCT usual care lost two (7%) patients to follow up, non‐RCT usual care lost three (19%) patients to follow up.
Data
Characteristics of the non‐randomised patients compared to RCT patients who received the same treatment. RCT usual care patients were on average 69 (51 to 82) years, 23 men and 7 women. Non‐RCT usual care patients were on average 62 (46 to 81) years, 13 men and 2 women.
Comparisons
Two RCT arms, both arms were compared with non‐randomised patients who received similar treatment. Experimental: forced air warming. Control: usual care with warm blankets and overhead heat lamps.
Outcomes
Outcomes were assessed in all patients. Patients were followed for 3 years. Main outcome was postoperative temperature at 6 hours.
Notes
The two experimental treatments were not significantly different.
Randomised controlled trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were participants in a patient preference trial who refused to be randomised due to preference. The non‐RCT patients were followed up similarly to those in the RCT. Women with early fetal demise or incomplete miscarriage at a gestational age of < 16 completed weeks. RCT group lost 31 women to follow up. Non‐RCT group lost 85 women to follow up.
Data
Characteristics of the non‐randomised patients compared to RCT patients who received the same treatment. RCT expected management patients were mean 32 years, 64 women. Non‐RCT preference expectant management women were on average 33 years, 126 women.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The experimental arm patients received expectant management. The control patients received surgery.
Outcomes
Women were followed up for 6 weeks and 12 weeks. Main outcome was success at 6 weeks.
Notes
The two experimental treatments were not significantly different.
Randomised controlled trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were participants in a patient preference trial who refused to be randomised due to preference. The non‐RCT patients were followed up similarly to those in the RCT. Women with early fetal demise or incomplete miscarriage at a gestational age of < 16 completed weeks. RCT group lost 26 women to follow up. Non‐RCT group lost 124 women to follow up.
Data
Characteristics of the non‐randomised patients compared to RCT patients who received the same treatment. RCT surgery patients were mean 33 years, 58 women. Non‐RCT preference surgery women were on average 32 years, 179 women.
Comparisons
Two RCT arms, both arms were compared with similarly treated eligible non‐RCT patients. The experimental arm patients received expectant management. The control patients received surgery.
Outcomes
Women were followed up for 6 weeks and 12 weeks. Main outcome was success at 6 weeks.
Notes
The two experimental treatments were not significantly different.
Randomised controlled trial with concurrent eligible patients outside of the RCT. It is unclear why the eligible non‐RCT patients did not participate in the trial. Patients undergoing cardio‐pulmonary bypass procedures. No losses to follow up.
Data
Characteristics of non‐RCT patients compared with RCT patients who received similar treatment are not presented. 50 patients were randomised the control group. 37 eligible non‐RCT patients received similar treatment.
Comparisons
Two RCT arms, the RCT control patients were compared to similarly treated eligible non‐RCT patients.There was 50 RCT patients and 37 non‐RCT patients. Experimental adjuvant use of preincisional presternal antibiotic infiltration. Control: usual care.
Outcomes
Clinical outcomes were assessed in all patients. Follow up was until at least 24 hours post operation. Main outcome was wound colonisation.
Notes
The experimental treatment was more effective than the control treatment.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because the patients refused because of preference for treatment. Women undergoing endometrial ablation. Six randomized women were lost to follow up and four non‐randomized women were lost to follow up
Data
Characteristics of non‐RCT patients compared with RCT patients who received similar treatment are not presented. 97 women were randomised to local anaesthesia. 32 non‐RCT women received local anaesthesia due to preference.
Comparisons
Two RCT arms, both arms compared to eligible women similarly treated outside of the trial. Complete results only presented for the experimental group. Experimental treatment: Local anaesthesia during endometrial ablation. Control: General anaesthesia during endometrial ablation.
Outcomes
Clinical outcomes were assessed in all women. Follow up was until discharge from hospital. Main outcome was acceptability measured as how many would have the procedure done again.
Notes
The two experimental treatments were not similarly effective.
Randomised trial with concurrent eligible patients outside of the RCT. We do not know why the non‐RCT patients were not in the RCT. Patients who would benefit from view of the gallbladder. No losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. Cerultide RCT patients were between 29 and 83 years, 1 woman and 16 men. Ceruletide non‐RCT patients were between 19 and 71 years, 21 women and 43 men. The measuring times were different for the RCT patients and the eligible non‐RCT patients.
Comparisons
Two RCT arms, the experimental treatment was compared with similarly treated eligible non‐RCT patients. Experimental: ceruletide‐assisted cholecystography. Control: fatty meal‐ assisted cholecystography.
Outcomes
Clinical outcomes were assessed in all the patients. Patients in the RCT were followed for 40 min, patients in the non‐RCT group were followed for 30 min. Main outcome was lack of reduction in gallbladder area at 20 min.
Notes
The experimental treatment was more effective than control.
Randomised controlled trial with concurrent eligible patients outside of the trial. The non‐RCT patients were not in the trial because of patient refusal of randomisation because of strong preference for treatment. No losses to follow up.
Data
Characteristics of the non‐randomised patients compared to RCT patients who received the same treatment. RCT integrated disconnect system patients were mean 57 years, 12 men and 6 women. Non‐RCT integrated disconnect system patients were mean 44 years, 7 men.
Comparisons
Two RCT arms, the experimental treatment was compared with non‐randomised patients who received similar treatment. Experimental: integrated disconnect system, Control: UV‐box system.
Outcomes
Outcomes were assessed in all patients. RCT patients were followed for mean 11 months, non‐RCT patients were followed for mean 8 months. Main outcome was peritonitis.
Notes
The experimental RCT treatment was more effective than control.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because the patients refused. Malnourished surgical patients who required nonemergency laparotomy or noncardiac thoractomy. Losses to follow up unknown.
Data
Characteristics of the RCT patients presented and compared to the eligible non‐randomised patients. RCT patients were mean 63 (10) years, 391 men and 4 women. Non‐RCT patients were mean 62 (10) years, 196 men and 3 women.
Comparisons
Two RCT arms, both arms were combined and compared with eligible non‐RCT patients with analysis adjusted for treatment. Experimental: Total parenteral nutrition. Control: this group received no perioperative total parenteral nutrition.
Outcomes
Clinical outcomes were assessed in all the patients. Patients in were followed for 90 days. Main outcome was number of complications at 90 days.
Notes
The two RCT treatments showed similar effectiveness.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because the patients refused . Patients with pain due to osteoarthritis of the knee or the hip. RCT group lost 57 patients to follow up. Non‐RCT group lost 285 patients to follow up.
Data
Characteristics of the non‐randomised patients compared to RCT patients who received the same treatment. RCT acupuncture patients were mean 61 (10) years, 183 women, 139 men. Non‐RCT acupunture patients were on mean 62 (11) years, 1788 women, 1133 men.
Comparisons
Two RCT arms, the RCT experimental arm patients were compared to similarly treated eligible non‐RCT patients. Experimental treatment: Acupuncture. Control: delayed start of acupuncture.
Outcomes
Patient were followed up for three months. Main outcome was WOMAC severity score.
Notes
The experimental treatment was more effective than the control treatment.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because the patients refused. Patients with chronic neck pain. RCT group lost 262 patients to follow up. Non‐RCT group lost 1150 patients to follow up.
Data
Characteristics of the non‐randomised patients compared to RCT patients who received the same treatment. RCT acupuncture patients were mean 50 (13) years, 1225 women, 528 men. Non‐RCT acupunture patients were mean 51 (13) years, 7006 women, 3389 men.
Comparisons
Two RCT arms, the RCT experimental arm patients were compared to similarly treated eligible non‐RCT patients. Experimental treatment: Acupuncture. Control: delayed start of acupuncture.
Outcomes
Patient were followed up for three months. Main outcome was % reduction in neck pain.
Notes
The experimental treatment was more effective than the control treatment.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because the patients refused. Patients with chronic low back pain. RCT group lost 88 patients to follow up. Non‐RCT group lost 770 patients to follow up.
Data
Characteristics of the non‐randomised patients compared to RCT patients who received the same treatment. RCT acupuncture patients were mean 53 (14) years, 847 women, 614 men. Non‐RCT acupunture patients were mean 53 (14) years, 5061 women, 3476 men.
Comparisons
Two RCT arms, the RCT experimental arm patients were compared to similarly treated eligible non‐RCT patients. Experimental treatment: Acupuncture. Control: delayed start of acupuncture.
Outcomes
Patient were followed up for three months. Main outcome was % less pain.
Notes
The experimental treatment was more effective than the control treatment.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because some endoscopists were uncomfortable randomizing as they had considerable experience with one of the dilators. The non‐RCT patients were followed‐up identically to the RCT patients. Patients with newly diagnosed peptic strictures, both sexes, age 23 to 91 years. Outcomes were assessed by endoscopists at hospital. No losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT patients with Eder‐Puestow dilator were mean 65 (18) years, 4 women and 12 men. Non‐RCT patients with Eder‐Puestow dilator were mean 65 (12) years, 23 women and 35 men.
Comparisons
Two RCT arms, each in common use, and each of them were compared with similarly treated eligible non‐RCT patients. Control‐EP: Eder‐Puestow dilator. Control‐b: balloon dilator.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for as long as 4 years. Main outcome was recurrence of dysphagia.
Notes
The two RCT treatments were not significantly different.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because some endoscopists were uncomfortable randomizing as they had considerable experience with one of the dilators. The non‐RCT patients were followed‐up identically to the RCT patients. Patients with newly diagnosed peptic strictures, both sexes, age 23 to 91 years. Outcomes were assessed by endoscopists at hospital. No losses to follow up.
Data
Characteristics of non‐RCT patients presented and compared to RCT patients who received the same treatment. RCT patients with balloon dilator were mean 69 (11) years, 7 women and 8 men. Non‐ RCT patients with balloon dilator were mean 67 (12) years, 15 women and 19 men.
Comparisons
Two RCT arms, each in common use, and each of them were compared with similarly treated eligible non‐RCT patients. Control‐EP: Eder‐Puestow dilator. Control‐b: balloon dilator.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for as long as 4 years. Main outcome was recurrence of dysphagia.
Notes
The two RCT treatments were not significantly different.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the trial because they refused participation. Cardiac transplant patients with hypogammaglobulinemia. No losses to follow up.
Data
Characteristics of non‐RCT patiens presented and compared to RCT patients who received the same treatment. The 10 RCT control patients were mean 55 (6) years, eight men and two women.The 33 non‐randomised patients were mean 54 (10) years, 27 men and six women.
Comparisons
Two RCT arms, the control arm patients were compared with similarly treated eligible non‐RCT patients. The experiemental treatment was 150 mg/kg CytoGam intravenously over 4 hours. The control patients were monitored.
Outcomes
Clinical outcomes were assessed in all the patients, patients were followed for six months. Main outcome was cytomegalovirus infection.
Notes
The two RCT treatments were not significantly different.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because they did not accept randomisation, these patients were treated according to choice. The non‐RCT patients were followed‐ up identically to the RCT patients. Patients in a general medical ward with alcohol problems. In the RCT abstinence counseling group 9 (47%) patients were lost to follow up. In the non‐RCT abstinence counseling group, 6 (38%) patients were lost to follow up.
Data
Non‐RCT patients were compared to RCT patients who received the same treatment. RCT patients receiving abstinence counseling were on average 57 (33 to 65) years, 16 men and 3 women. Non‐RCT patients receiving abstinence counseling were on average 53 (40 to 68) years, 12 men and 4 women.
Comparisons
Two RCT arms individualized referral (experimental) and simple abstinence counseling (control) which was compared with similarly treated eligible non‐RCT patients.
Outcomes
Clinical outcomes were assessed in all the patients. Patients were followed for approximately 1 year. Main outcome was lack of abstinence.
Notes
The experimental treatment was more effective than control.
Randomised trial with concurrent eligible patients outside of the RCT. The non‐RCT patients were not in the RCT because of parental refusal (21 children), timing (22 children) and 3 others. Infants with congenital nasolacrimal duct obstruction. No losses to follow up in the RCT group, 4 eyes lost to follow up in the non‐RCT group.
Data
Characteristics of the patients not presented. Watchful waiting RCT patients included 16 affected eyes. Watchful waiting non‐RCT patients included 37 affected eyes.
Comparisons
Two RCT arms, the control treatment was compared with similarly treated eligible non‐RCT patients. Experimental: probing. Control: Watchful waiting.
Outcomes
Clinical outcomes were assessed in all the infants. Patients were followed 15 and 24 months. Main outcome was problem unresolved at 1 year.
Notes
The experimental treatment was more effective than control at 1 year.
Gunn Elisabeth Vist: study selection, data extraction, statistical analysis, drafting of written submissions, protocol and review development.
Dianne Bryant: study selection, data extraction, statistical analysis, drafting of written submissions, and review development.
Lyndsay Somerville: study selection, data extraction, statistical analysis, drafting of written submissions, review development.
Trevor Birmingham: study selection, data extraction, drafting of written submissions.
Andrew David Oxman: statistical analysis, drafting of written submissions, protocol and review development.
Sources of support
Internal sources
Norwegian Knowledge Centre for the Health Services, Norway.
University of Western Ontario, London, Canada.
External sources
The Nuffield Trust, UK.
Department of Health, UK.
Declarations of interest
None known
Unchanged
References
References to studies included in this review
Abraham 2004a {published data only}
Abraham NS,
Wieczorek P,
Huang J,
Mayrand S,
Fallone CA,
Barkun AN.
Assessing clinical generalizability in sedation studies of upper GI endoscopy.
Gastrointestinal Endoscopy 2004;60:28‐33.
[DOI] [PubMed] [Google Scholar]
Abraham 2004b {published data only}
Abraham NS,
Wieczorek P,
Huang J,
Mayrand S,
Fallone CA,
Barkun AN.
Assessing clinical generalizability in sedation studies of upper GI endoscopy.
Gastrointestinal Endoscopy 2004;60:28‐33.
[DOI] [PubMed] [Google Scholar]
Antman 1985a {published data only}
Antman K,
Amato D,
Wood W,
Carson J,
Suit H,
Proppe K,
et al.
Selection bias in clinical trials.
Journal of Clinical Oncology 1985;3:1142‐7.
[DOI] [PubMed] [Google Scholar]
Antman 1985b {published data only}
Antman K,
Amato D,
Wood W,
Carson J,
Suit H,
Proppe K,
et al.
Selection bias in clinical trials.
Journal of Clinical Oncology 1985;3:1142‐7.
[DOI] [PubMed] [Google Scholar]
Ashok 2005a {published data only}
Ashok PW,
Hamoda H,
Flett GMM,
Kidd A,
Fitzmaurice A,
Templeton A.
Psychological sequelae of medical and surgical abortion at 10‐13 weeks gestation.
Acta Obstetricia Gynecologica Scandinavica 2005;84:761‐6.
[DOI] [PubMed] [Google Scholar]
Ashok 2005b {published data only}
Ashok PW,
Hamoda H,
Flett GMM,
Kidd A,
Fitzmaurice A,
Templeton A.
Psychological sequelae of medical and surgical abortion at 10‐13 weeks gestation.
Acta Obstetrica Gynecologica Scandinavica 2005;84:761‐6.
[DOI] [PubMed] [Google Scholar]
Bain 2001a {published data only}
Bain C,
Cooper KG,
Parkin DE.
A partially randomized patient preference trial of microwave endometrial ablation using local anaesthesia and intravenous sedation or general anaesthesia: a pilot study.
Gynaecological Endoscopy 2001;10:223‐8.
[Google Scholar]
Bain 2001b {published data only}
Bain C,
Cooper KG,
Parkin DE.
A partially randomized patient preference trial of microwave endometrial ablation using local anaesthesia and intravenous sedation or general anaesthesia: a pilot study.
Gynaecological Endoscopy 2001;10:223‐8.
[Google Scholar]
Bakker 2000 {published data only}
Bakker A,
Spinhoven P,
Balkom AJLM,
Vleugel L,
Dyck R.
Cognitive therapy by allocation versus cognitive therapy by preference in the treatment of panic disorder.
Psychotherapy and Psychosomatics 2000;69:240‐3.
[DOI] [PubMed] [Google Scholar]
Balmukhanov 1989a {published data only}
Balmukhanov SB,
Beisebaev AA,
Aitkoolova ZI,
Mustaphin JS,
Philippenko VI,
Rismuhamedova RS,
et al.
Intramural and parametrial infusion of metronidazole in the radiotherapy of uterine cervix cancer: prelimenary report.
International Journal of Radiation Oncology, Biology, Physics 1989;16:1061‐3.
[DOI] [PubMed] [Google Scholar]
Balmukhanov 1989b {published data only}
Balmukhanov SB,
Beisebaev AA,
Aitkoolova ZI,
Mustaphin JS,
Philippenko VI,
Rismuhamedova RS,
et al.
Intramural and parametrial infusion of metronidazole in the radiotherapy of uterine cervix cancer: prelimenary report.
International Journal of Radiation Oncology, Biology, Physics 1989;16:1061‐3.
[DOI] [PubMed] [Google Scholar]
Baum 1979 {published data only}
Baum E,
Sather H,
Nachman J,
Seinfeld J,
Kritvit W,
Leikin S,
et al.
Relapse rates following cessation of chemotherapy during complete remission of acute lymphocytic leukemia: A report from childrens cancer study group.
Medical and Pediatric Oncology 1979;7:25‐34.
[DOI] [PubMed] [Google Scholar]
Bedi 2000a {published data only}
Bedi N,
Chilvers C,
Churchill R,
Dewey M,
Duggan C,
Fielding K,
et al.
Assessing effectiveness of treatment of depression in primary care: Partially randomised preference trial.
British Journal of Psychiatry 2000;177:312‐8.
[DOI] [PubMed] [Google Scholar]
Bedi 2000b {published data only}
Bedi N,
Chilvers C,
Churchill R,
Dewey M,
Duggan C,
Fielding K,
et al.
Assessing effectiveness of treatment of depression in primary care: Partially randomised preference trial.
British Journal of Psychiatry 2000;177:312‐8.
[DOI] [PubMed] [Google Scholar]
Berglund 1997 {published and unpublished data}
Berglund G,
Bolund C,
Gustafsson UL,
Sjoden PO.
Is the wish to participate in a cancer rehabilitation program an indicator of the need? Comparisons of participants and non‐participants in a randomized study.
Psycho‐Oncology 1997;6:35‐46.
[DOI] [PubMed] [Google Scholar]
Bergmann 1994 {published data only}
Bergmann JF,
Chassany O,
Gandiol J,
Deblois P,
Kanis JA,
Segrestaa JM,
et al.
A randomised clinical trial of the effect of informed consent on the analgesic activity of placebo and naproxen in cancer pain.
Clinical Trials and Meta‐Analysis 1994;29:41‐7.
[PubMed] [Google Scholar]
Bhattacharya 1998 {published data only}
Bhattacharya S,
Cameron IM,
Mollison J,
Parkin DE,
Abramovich DR,
Kitchener HC.
Admission‐discharge policies for hysteroscopic surgery: a randomised comparison of day case with in‐patient admission.
European Journal of Obstetrics & Gynecology and Reproductive Biology 1998;76:81‐4.
[DOI] [PubMed] [Google Scholar]
Biederman 1985 {published data only}
Biederman J,
Herzog DB,
Rivinus TM,
Harper GP,
Ferber RA,
Rosenbaum JF,
et al.
Amitriptyline in the treatment of anorexia nervosa: A double‐blind, placebo‐controlled study.
Journal of Clinical Psychopharmacology 1985;5:10‐6.
[PubMed] [Google Scholar]
Bijker 2000a {published data only}
Bijker N,
Peterse JL,
Fentiman TS,
Julien JP,
Hart AAM,
Avril A,
et al.
Effects of patient selection on the applicability of results from a randomised clinical trial (EORTC 10853) investigating breast‐conserving treatment for DCIS.
Breast conserving therapy for ductal carcinoma in situ. N Bijker. Thesis 2000.
[Google Scholar]
Bijker 2000b {published data only}
Bijker N,
Peterse JL,
Fentiman TS,
Julien JP,
Hart AAM,
Avril A,
et al.
Effects of patient selection on the applicability of results from a randomised clinical trial (EORTC 10853) investigating breast‐conserving treatment for DCIS.
Breast conserving therapy for ductal carcinoma in situ. N Bijker. Thesis. 2000.
[Google Scholar]
Blichert‐Toft 1988a {published data only}
Blichert‐Toft M,
Brincker H,
Andersen JA,
Andresen KW,
Axelsson CK,
Mouridsen HT,
et al.
A Danish randomized trial comparing breast‐conserving therapy with mastectomy in mammary carcinoma: Preliminary results.
Acta Oncologica 1988;27:671‐7.
[DOI] [PubMed] [Google Scholar]
Blichert‐Toft 1988b {published data only}
Blichert‐Toft M,
Brincker H,
Andersen JA,
Andresen KW,
Axelsson CK,
Mouridsen HT,
et al.
A Danish randomized trial comparing breast‐conserving therapy with mastectomy in mammary carcinoma: Preliminary results.
Acta Oncologica 1988;27:671‐7.
[DOI] [PubMed] [Google Scholar]
Boezaart 1998 {published data only}
Boezaart AP,
Berry RA,
Laubscher JJ,
Nell ML.
Evaluatin of anxiolysis and pain associated with combined peri‐ and retrobullar eye block for cataract surgery.
Journal of Clinical Anesthesia 1998;10:204‐10.
[DOI] [PubMed] [Google Scholar]
CASS 1984a {published data only}
CASS Principat Investigators and their Associates.
Coronary artery surgery study (CASS): A randomised trial of coronary artery bypass surgery. Comparability of entry characteristics and survival in randomized patients and nonrandomized patients meeting randomization criteria.
Journal of the American College of Cardiology 1984;3:114‐28.
[PubMed] [Google Scholar]
CASS 1984b {published data only}
CASS Principat Investigators and their Associates.
Coronary artery surgery study (CASS): A randomised trial of coronary artery bypass surgery. Comparability of entry characteristics and survival in randomized patients and nonrandomized patients meeting randomization criteria.
Journal of the American College of Cardiology 1984;3:114‐28.
[PubMed] [Google Scholar]
Chauhan 1992 {published data only}
Chauhan SP,
Rutherford SE,
Hess LW,
Morrison JC.
Prophylactic intrapartum amnioinfusion for patients with oligohydramnios: A prospective randomized study.
Journal of Reproductive Medicine 1991;37:817‐20.
[PubMed] [Google Scholar]
Chilvers 2001a {published data only}
Chilvers C,
Dewey M,
Fielding K,
Gretton V,
Miller P,
Palmer B,
et al.
Antidepressant drugs and generic counselling for treatment of major depression in primary care: randomised trial with patient preference arms.
British Medical Journal 2001;322:772‐5.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Chilvers 2001b {published data only}
Chilvers C,
Dewey M,
Fielding K,
Gretton V,
Miller P,
Palmer B,
et al.
Antidepressant drugs and generic counselling for treatment of major depression in primary care: randomised trial with patient preference arms.
British Medical Journal 2001;322:772‐5.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Clagett 1984a {published data only}
Clagett GP,
Youkey JR,
Bringham RA,
Orecchia PM,
Salander JM,
Collins GJ,
et al.
Asymptomatic cervical bruit and abnormal ocular pneumoplethysmography: A prospective study comparing two approaches to management.
Surgery 1984;96:823‐30.
[PubMed] [Google Scholar]
Clagett 1984b {published data only}
Clagett GP,
Youkey JR,
Bringham RA,
Orecchia PM,
Salander JM,
Collins GJ,
et al.
Asymptomatic cervical bruit and abnormal ocular pneumoplethysmography: A prospective study comparing two approaches to management.
Surgery 1984;96:823‐30.
[PubMed] [Google Scholar]
Clapp 1989 {published data only}
Clapp DW,
Kliegman RM,
Baley JE,
Shenker N,
Kyllonen K,
Fanaroff AA,
et al.
Use of intravenously administered immune globulin to prevent nosocomial sepsis in low birth weight infants: Report of a pilot study.
Journal of Pediatrics 1989;115:973‐8.
[DOI] [PubMed] [Google Scholar]
Cooper 1997a {published data only}
Cooper KG,
Grant AM,
Garratt AM.
The impact of using a partially randomised patient preference design when evaluating alternative managements for heavy menstrual bleeding.
British Journal of Obstetrics and Gybaecology 1997;104:1367‐73.
[DOI] [PubMed] [Google Scholar]
Cooper 1997b {published data only}
Cooper KG,
Grant AM,
Garratt AM.
The impact of using a partially randomised patient preference design when evaluating alternative managements for heavy menstrual bleeding.
British Journal of Obstetrics and Gynaecology 1997;104:1367‐73.
[DOI] [PubMed] [Google Scholar]
Creutzig 1993a {published data only}
Creutzig U,
Ritter J,
Zimmermann M,
Schellong G.
Does cranial irradiation reduce the risk of bone marrow relapse in acute myelogenous leukemia? Unexpected results of the childhood acute myelogenous leukemia study BFM‐87.
Journal of Clinical Oncology 1993;11:279‐86.
[DOI] [PubMed] [Google Scholar]
Creutzig 1993b {published data only}
Creutzig U,
Ritter J,
Zimmermann M,
Schellong G.
Does cranial irradiation reduce the risk of bone marrow relapse in acute myelogenous leukemia? Unexpected results of the childhood acute myelogenous leukemia study BFM‐87.
Journal of Clinical Oncology 1993;11:279‐86.
[DOI] [PubMed] [Google Scholar]
Dahan 1986 {published data only}
Dahan R,
Caulin C,
Figea L,
Kanis JA,
Caulin F,
Segrestaa JM.
Does informed consent influence therapeutic outcome? A clinical trial of the hypnotic activity of placebo in patients admitted to hospital.
British Medical Journal 1986;293:363‐4.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Davis 1985 {published data only}
Davis S,
Wright PW,
Schulman SF,
Hill LD,
Pinkham RD,
Johnson LP,
et al.
Participants in prospective, randomized clinical trials for resected non‐small cell lung cancer have improved survival compared with nonparticipants in such trials.
Cancer 1985;56:1710‐8.
[DOI] [PubMed] [Google Scholar]
Edsmyr 1978 {published data only}
Edsmyr F,
Esposti PL,
Johansson B,
Strindberg B.
Clinical experimental randomized study of 2.6‐CIS‐Diphenylhexamethylcyclotetrasiloxane and Estramurine‐17‐Phosphate in the treatment of prostatic carcinoma.
The Journal of Urology 1978;120:705‐7.
[DOI] [PubMed] [Google Scholar]
Ekstein 2002a {published data only}
Ekstein S,
Elami A,
Merin G,
Gotsman MS,
Lotan C.
Ballon angioplasty versus bypass grafting in the era of coronary stenting.
Israel Medical Association Journal 2002;4:583‐9.
[PubMed] [Google Scholar]
Ekstein 2002b {published data only}
Ekstein S,
Elami A,
Merin G,
Gotsman MS,
Lotan C.
Ballon angioplasty versus bypass grafting in the era of coronary stenting.
Israel Medical Association Journal 2002;4:583‐9.
[PubMed] [Google Scholar]
Elliott 1996 {published data only}
Elliott RB,
Pilcher CC,
Fergusson DM,
Stewart AW.
A population based strategy to prevent insulin‐dependent diabetes using nicotinamide.
Journal of Pediatric Endocrinology & Metabolism 1996;9:501‐9.
[DOI] [PubMed] [Google Scholar]
Emery 2003a {published data only}
Emery M,
Beran MD,
Darwiche J,
Oppizzi L,
Joris V,
Capel R,
et al.
Results from a prospective, randomized, controlled study evaluating the acceptability and effects of routine pre‐IVF counselling.
Human Reproduction 2003;18:2647‐53.
[DOI] [PubMed] [Google Scholar]
Emery 2003b {published data only}
Emery M,
Beran MD,
Darwiche J,
Oppizzi L,
Joris V,
Capel R,
et al.
Results from a prospective, randomized, controlled study evaluating the acceptability and effects of routine pre‐IVF counselling.
Human Reproduction 2003;18:2647‐53.
[DOI] [PubMed] [Google Scholar]
Feit 2000a {published data only}
Feit F,
Brooks MM,
Sopko G,
Keller NM,
Rosen A,
Krone R,
et al.
Long‐term clinical outcome in the bypass angioplasty revascularization investigation registry: Comparison with the randomized trial.
Circulation 2000;101:2795‐802.
[DOI] [PubMed] [Google Scholar]
Feit 2000b {published data only}
Feit F,
Brooks MM,
Sopko G,
Keller NM,
Rosen A,
Krone R,
et al.
Long‐term clinical outcome in the bypass angioplasty revascularization investigation registry: Comparison with the randomized trial.
Circulation 2000;101:2795‐802.
[DOI] [PubMed] [Google Scholar]
Forbes 2000 {published data only}
Forbes GM,
Collins BJ.
Niros oxide for colonoscopy: A randomized controlled study.
Gastrointestinal Endoscopy 2000;51:271‐7.
[DOI] [PubMed] [Google Scholar]
Forssell 1989 {published and unpublished data}
Forssell C,
Takolander R,
Bergqvist D,
Johansson A,
Persson NH.
Local versus general anaestesia in carotid surgery. A prospective, randomised study.
European Journal of Vascular Surgery 1989;3:503‐9.
[DOI] [PubMed] [Google Scholar]
Helsing 1998a {published and unpublished data}
Helsing M,
Bergman B,
Thaning L,
Hero U,
for the Joint Lung Cancer Study Group.
Quality of life and survival in patients with advanced non‐small cell lung cancer receiving supportive care plus chemotherapy with carboplatin and etoposide or supportive care only. A multicentre randomised phase III trial.
European Journal of Cancer 1998;34:1036‐44.
[DOI] [PubMed] [Google Scholar]
Helsing 1998b {published and unpublished data}
Helsing M,
Bergman B,
Thaning L,
Hero U,
for the Joint Lung Cancer Study Group.
Quality of life and survival in patients with advanced non‐small cell lung cancer receiving supportive care plus chemotherapy with carboplatin and etoposide or supportive care only. A multicentre randomised phase III trial.
European Journal of Cancer 1998;34:1036‐44.
[DOI] [PubMed] [Google Scholar]
Henshaw 1993a {published data only}
Henshaw RC,
Naji SA,
Templeton AA.
Comparison of medical abortion with surgical vacuum aspiration: women's preferences and acceptability of treatment.
British Medical Journal 1993;307:714‐7.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Henshaw 1993b {published data only}
Henshaw RC,
Naji SA,
Templeton AA.
Comparison of medical abortion with surgical vacuum aspiration: women's preferences and acceptability of treatment.
British Medical Journal 1993;307:714‐7.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Heuss 2004 {published data only}
Heuss LT,
Juergen D,
Schnieper P,
Tapparelli CB,
Pflimlin E,
Beglinger C.
Patient‐controlled versus nurse‐administered sedation with propofol colonoscopy. A prospective randomized trial.
American Journal of Gastroenterology 2004:511‐8.
[DOI] [PubMed] [Google Scholar]
Karande 1998 {published data only}
Karande V,
Korn A,
Morris R,
Rao R,
Balin M,
Rinehart J,
et al.
The continuous outcome and cost evaluation of a prospective randomized trial of in vitro fertilization (IVF) versus a traditional treatmetn algorithm as first choice infertility treatment.
Fertility and Sterility 1998:P‐142.
[DOI] [PubMed] [Google Scholar]
Kendrick 2001a {published data only}
Kendrick D,
Fielding K,
Bentley E,
Miller P,
Kerslake R,
Pringle M.
The role of radiography in primary care patients with low back pain of at least 6 weeks duration: a randomised (unblinded) controlled trial.
Health Technology Assessment 2001;5(30):70.
[DOI] [PubMed] [Google Scholar]
Kendrick 2001b {published data only}
Kendrick D,
Fielding K,
Bentley E,
Miller P,
Kerslake R,
Pringle M.
The role of radiography in primary care patients with low back pain of at least 6 weeks duration: a randomised (unblinded) controlled trial.
Health Technology Assessment 2001;5(30).
[DOI] [PubMed] [Google Scholar]
Kieler 1998 {published data only}
Kieler H,
Hellberg D,
Nilsson S,
Waldenstrøm U,
Axelsson O.
Pregnancy outcome among non‐participants in a trial on ultrasound screening.
Ultrasound in Obstetrics and Gynecology 1998;11:104‐9.
[DOI] [PubMed] [Google Scholar]
King 1997a {published data only}
King III SB,
Barnhart HX,
Kosinski AS,
Weintraub WS,
Lembo NJ,
Petersen JY,
et al.
Angioplasty or surgery for multivessel coronary artery disease: Comparison of eligible registry and randomized patients in the EAST trial and influence of treatment selection on outcomes.
American Journal of Cardiology 1997;79:1453‐9.
[DOI] [PubMed] [Google Scholar]
King 1997b {published data only}
King III SB,
Barnhart HX,
Kosinski AS,
Weintraub WS,
Lembo NJ,
Petersen JY,
et al.
Angioplasty or surgery for multivessel coronary artery disease: Comparison of eligible registry and randomized patients in the EAST trial and influence of treatment selection on outcomes.
American Journal of Cardiology 1997;79:1453‐9.
[DOI] [PubMed] [Google Scholar]
King 2000a {published data only}
King M,
Sibbald B,
Ward E,
Bower P,
Lloyd M,
Gabbay M,
et al.
Randomised controlled trial of non‐directive counselling, cognitive‐behaviour therapy and usual general practitioner care in the management of depression as well as mixed anxiety and depression in primary care.
Health Technology Assessment 2000;4(19):85.
[PubMed] [Google Scholar]
King 2000b {published data only}
King M,
Sibbald B,
Ward E,
Bower P,
Lloyd M,
Gabbay M,
et al.
Randomised controlled trial of non‐directive counselling, cognitive‐behaviour therapy and usual general practitioner care in the management of depression as well as mixed anxiety and depression in primary care.
Health Technology Assessment 2000;4(19).
[PubMed] [Google Scholar]
Lansky 1983 {published data only}
Lansky D,
Vance MA.
School‐based intervention for adolescent obesity: Analysis of treatment, randomly selected control, and self‐selected control subjects.
Journal of Consulting and Clinical Psychology 1983;51:147‐8.
[DOI] [PubMed] [Google Scholar]
Lidbrink 1995 {published data only}
Lidbrink E,
Frisell J,
Rosendahl I,
Rutqvist LE.
Nonattendance in the Stockholm mammography screening trial: Relative mortality and reasons for nonattendance.
Breast Cancer Research and Treatment 1995;35:267‐75.
[DOI] [PubMed] [Google Scholar]
Link 1991a {published data only}
Link MP,
Goorin AM,
Horowitz M,
Meyer WH,
Belasco J,
Baker A,
et al.
Adjuvant chemotherapy of high‐grade osteosarcoma of the extremity. Updated results of the multi‐institutional osteosarcoma study.
Clinical Orthopaedics and Related Research 1991;270:8‐14.
[PubMed] [Google Scholar]
Link 1991b {published data only}
Link MP,
Goorin AM,
Horowitz M,
Meyer WH,
Belasco J,
Baker A,
et al.
Adjuvant chemotherapy of high‐grade osteosarcoma of the extremity. Updated results of the multi‐institutional osteosarcoma study.
Clinical Orthopaedics and Related Research 1991;270:8‐14.
[PubMed] [Google Scholar]
Liu 1998a {published and unpublished data}
Liu WF,
Harrington T.
The need for delivery room intubation of thin meconium in the low risk newborn: A clinical trial.
American Journal of Perinatology 1998;15:675‐82.
[DOI] [PubMed] [Google Scholar]
Liu 1998b {published and unpublished data}
Liu WF,
Harrington T.
The need for delivery room intubation of thin meconium in the low risk newborn: A clinical trial.
American Journal of Perinatiology 1998;15:675‐82.
[DOI] [PubMed] [Google Scholar]
MACESG 1992a {published data only}
Mayo Asymptomatic Carotid Endarterectomy Study Group.
Results of a randomized controlled trial of carotid endarterectomy for asymptomatic carotid stenosis.
Mayo Clinic Proceedings 1992;67:513‐8.
[DOI] [PubMed] [Google Scholar]
MACESG 1992b {published data only}
Mayo Asymptomatic Carotid Endarterectomy Study Group.
Results of a randomized controlled trial of carotid endarterectomy for asymptomatic carotid stenosis.
Mayo Clinic Proc 1992;67:513‐8.
[DOI] [PubMed] [Google Scholar]
MacLennan 1985 {published data only}
MacLennan AH,
Kerin JFP,
Kirby C,
Grant P,
Warnes GM,
Cox LW,
et al.
The effect of porcine relaxin vaginally applied at human embryo transfer in an In vitro fertilization programme.
The Australian & New Zealand Journal of Obstetrics & Gynaecology 1985;25:68‐71.
[DOI] [PubMed] [Google Scholar]
Mahon 1996 {published data only}
Mahon J,
Laupacis A,
Donner A,
Wood T.
Randomised study of no 1 trials versus standard practice.
British Medical Journal 1996;312:1069‐74.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Mahon 1999 {published data only}
Mahon JL,
Laupacis A,
Hodder RV,
McKim DA,
Paterson NAM,
Wood TE,
et al.
Theophylline for irreversible chronic airflow limitation. A randomized study comparing n of 1 trials to standard practice.
Chest 1999;115:38‐48.
[DOI] [PubMed] [Google Scholar]
Marcinczyk 1997 {published data only}
Marcinczyk MJ,
Nicholas GG,
Reed JF,
Nastasee SA.
Asymptomatic carotid endarterectomy: Patient and surgeon selection.
Stroke 1997;28:291‐6.
[DOI] [PubMed] [Google Scholar]
Martinez‐Amenos1990a {published data only}
Martinez‐Amenos A,
Ferre MLF,
Vidal CM,
Rocasalbas JA.
Evaluation of two educative models in primary care hypertension programme.
Journal of Human Hypertension 1990;4:362‐4.
[PubMed] [Google Scholar]
Martinez‐Amenos1990b {published data only}
Martinez‐Amenos A,
Ferre MLF,
Vidal CM,
Rocasalbas JA.
Evaluation of two educative models in primary care hypertension programme.
Journal of Human Hypertension 1990;4:362‐4.
[PubMed] [Google Scholar]
Masood 2002 {published data only}
Masood J,
Shah N,
Lane T,
Andrews H,
Simpson P,
Barua JM.
Nitrous oxide (entonox) inhalation and tolerance of transrectal ultrasound guided prostate biopsy: A double‐blind randomized controlled study.
The Journal of Urology 2002;168:116‐20.
[PubMed] [Google Scholar]
McCaughey 1998 {published data only}
McCaughey ES,
Mulligan J,
Voss LD,
Betts PR.
Randomised trial of growth hormone in short normal girls.
Lancet 1998;351:940‐4.
[DOI] [PubMed] [Google Scholar]
McKay 1995a {published and unpublished data}
McKay JR,
Alterman AI,
McLellan AT,
Snider EC,
O'Brian CP.
Effect of random versus nonrandom assignment in a comparison of inpatient and day hospital rehabilitation for male alcoholics.
Journal of Consulting and Clinical Psychology 1995;63:70‐8.
[DOI] [PubMed] [Google Scholar]
McKay 1995b {published and unpublished data}
McKay JR,
Alterman AI,
McLellan AT,
Snider EC,
O'Brian CP.
Effect of random versus nonrandom assignment in a comparison of inpatient and day hospital rehabilitation for male alcoholics.
Journal of Consulting and Clinical Psychology 1995;63:70‐8.
[DOI] [PubMed] [Google Scholar]
McKay 1998a {published and unpublished data}
McKay JR,
Alterman AI,
McLellan AT,
Boardman CR,
Mulvaney FD,
O'Brian CP.
Random versus nonrandom assignment in the evaluation of treatment for cocaine abusers.
Journal of Consulting and Clinical Psychology 1998;66:697‐701.
[DOI] [PubMed] [Google Scholar]
McKay 1998b {published and unpublished data}
McKay JR,
Alterman AI,
McLellan AT,
Boardman CR,
Mulvaney FD,
O'Brian CP.
Random versus nonrandom assignment in the evaluation of treatment for cocaine abusers.
Journal of Consulting and Clinical Psychology 1998;66:697‐701.
[DOI] [PubMed] [Google Scholar]
Melchart 2002a {published data only}
Melchart D,
Steger H‐G,
Linde K,
Makarian K,
Hatahet Z,
Brenke R,
et al.
Integrating patient preferences in clinical trials: A pilot study of acupuncture versus midazolam for gastroscopy.
The Journal of Alternative and Complementary medicine 2002;8:265‐74.
[DOI] [PubMed] [Google Scholar]
Melchart 2002b {published data only}
Melchart D,
Steger H‐G,
Linde K,
Makarian K,
Hatahet Z,
Brenke R,
et al.
Integrating patient preferences in clinical trials: A pilot study of acupuncture versus midazolam for gastroscopy.
The Journal of Alternative and Complementary medicine 2002;8:265‐74.
[DOI] [PubMed] [Google Scholar]
Moertel 1984 {published data only}
Moertel CG,
Childs DS,
O'Fallon JR,
Holbrook MA,
Schutt AJ,
Reitemeier RJ.
Combined 5‐Fluorouracil and radiation therapy as a surgical adjuvant for poor prognosis gastric carcinoma.
Journal of Clinical Oncology 1984;2:1249‐54.
[DOI] [PubMed] [Google Scholar]
Mori 2006a {published data only}
Mori A,
Fushimi N,
Asano T,
Maruyama T,
Ohashi N,
Okumura H,
et al.
Cardiovascular tolerance in unsedated upper gastrointestinal endoscopy: prospective randomized comparison between transnasal and conventional oral procedures.
Digestive Endoscopy 2006;18:282‐7.
[Google Scholar]
Mori 2006b {published data only}
Mori A,
Fushimi N,
Asano T,
Maruyama T,
Ohashi N,
Okumura H,
et al.
Cardiovascular tolerance in unsedated upper gastrointestinal endoscopy: prospective randomized comparison between transnasal and conventional oral procedures.
Digestive Endoscopy 2006;18:282‐7.
[Google Scholar]
Mosekilde 2000a {published and unpublished data}
Mosekilde L,
Beck‐Nielsen H,
Sørensen OH,
Nielsen SP,
Charles P,
Vestergaard P,
et al.
Hormonal replacement therapy reduces forearm fracture incidence in recent postmenopausal women ‐ results of the Danish osteoporosis prevention study.
Maturitas 2000;36:181‐93.
[DOI] [PubMed] [Google Scholar]
Mosekilde 2000b {published and unpublished data}
Mosekilde L,
Beck‐Nielsen H,
Sørensen OH,
Nielsen SP,
Charles P,
Vestergaard P,
et al.
Hormonal replacement therapy reduces forearm fracture incidence in recent postmenopausal women ‐ results of the Danish osteoporosis prevention study.
Maturitas 2000;36:181‐93.
[DOI] [PubMed] [Google Scholar]
Nagel 1998a {published data only}
Nagel HTC,
Vanderbussche FPHA,
Keirse MJNC,
Oepkes D,
Oosterwijk JC,
Beverstock G,
et al.
Amniocentesis before 14 completed weeks as an alternative to transabdominal chorionic villus sampling: A controlled trial with infant follow‐up.
Prenatal Diagnosis 1998;18:465‐75.
[PubMed] [Google Scholar]
Nagel 1998b {published data only}
Nagel HTC,
Vanderbussche FPHA,
Keirse MJNC,
Oepkes D,
Oosterwijk JC,
Beverstock G,
et al.
Amniocentesis before 14 completed weeks as an alternative to transabdominal chorionic villus sampling: A controlled trial with infant follow‐up.
Prenatal Diagnosis 1998;18:465‐75.
[PubMed] [Google Scholar]
Nicolaides 1994a {published data only}
Nicolaides K,
Brizot MdL,
Patel F,
Snijders R.
Comparison of chorionic villus sampling and amniocentesis for fetal karyotyping at 10‐13 weeks' gestation.
Lancet 1994;344:435‐9.
[DOI] [PubMed] [Google Scholar]
Nicolaides 1994b {published data only}
Nicolaides K,
Brizot MdL,
Patel F,
Snijders R.
Comparison of chorionic villus sampling and amniocentesis for fetal karyotyping at 10‐13 weeks' gestation.
Lancet 1994;334:435‐9.
[DOI] [PubMed] [Google Scholar]
Ogden 2004 {published data only}
Ogden JA,
Alvarez RG,
Levitt RL,
Johnson JE,
Marlow ME.
Electrohydraulic high‐energy shock‐wave treatment for chronic plantar fasciitis.
Journal of Bone and Joint Surgery 2994;86:2216‐28.
[DOI] [PubMed] [Google Scholar]
Paradise 1984a {published and unpublished data}
Paradise JL,
Bluestone CD,
Bachman RZ,
Colborn DK,
Bernard BS,
Taylor FH,
et al.
Efficacy of tonsillectomy for recurrent throat infection in severely affected children. Results of parallel randomized clinical trials.
The New England Journal of Medicine 1984;310:674‐83.
[DOI] [PubMed] [Google Scholar]
Paradise 1984b {published and unpublished data}
Paradise JL,
Bluestone CD,
Bachman RZ,
Colborn DK,
Bernard BS,
Taylor FH,
Rogers KD,
Schwarzbach RH,
Stool SE,
Friday GA,
Smith IH,
Saez CA.
Efficacy of tonsillectomy for recurrent throat infection in severely affected children. Results of parallel randomized clinical trials.
The New England Journal of Medicine 1984;310:674‐83.
[DOI] [PubMed] [Google Scholar]
Paradise 1990a {published and unpublished data}
Paradise JL,
Bluestone CD,
Rogers KD,
Taylor FH,
Colborn DK,
Bachman RZ,
et al.
Efficacy of adenoidectomy for recurrent otitis media in children previously treated with tympanostomy‐tube replacement. Results of parallel randomized and nonrandomized trials.
Journal of the American Medical Association 1990;263:2066‐73.
[PubMed] [Google Scholar]
Paradise 1990b {published and unpublished data}
Paradise JL,
Bluestone CD,
Rogers KD,
Taylor FH,
Colborn DK,
Bachman RZ,
et al.
Efficacy of adenoidectomy for recurrent otitis media in children previously treated with tympanostomy‐tube replacement. Results of parallel randomized and nonrandomized trials.
Journal of the American Medical Association 1990;263:2066‐73.
[PubMed] [Google Scholar]
Playforth 1988 {published and unpublished data}
Playforth MJ,
Smith GMR,
Evans M,
Pollock AV.
Antimicrobial bowel preparation. Oral, parenteral, or both?.
Diseases Colon and Rectum 1988;31:90‐3.
[DOI] [PubMed] [Google Scholar]
Raistrick 2005a {published data only}
Raistrick D,
West D,
Finnegan O,
Thistlethwaite G,
Brearley R,
Banbery J.
A comparison of buprenorphine and lofexidine for community opiate detoxification: results from a randomized controlled trial.
Addiction 2005;100:1860‐7.
[DOI] [PubMed] [Google Scholar]
Raistrick 2005b {published data only}
Raistrick D,
West D,
Finnegan O,
Thistlethwaite G,
Brearley R,
Banbery J.
A comparison of buprenorphine and lofexidine for community opiate detoxification: results from a randomized controlled trial.
Addiction 2005;100:1860‐7.
[DOI] [PubMed] [Google Scholar]
Reeves 2004 {published data only}
Reeves BC,
Angelini GD,
Bryan AJ,
Taylor FC,
Cripps T,
Spyt TJ,
et al.
A multi‐centre randomised controlled trial of minimally invasive direct coronary bypass grafting versus percutaneous transluminal coronary angioplasty with stenting for proximal stenosis of the left anterior descending coronary artery.
Health Technology Assessment 2004;8(16):57p.
[DOI] [PubMed] [Google Scholar]
Rigg 2000a {published and unpublished data}
Rigg JRA,
Jamrozik K,
Myles PS,
Silbert B,
Peyton P,
Parsons RW,
et al.
Design of the multicenter Australian study of epidural anesthesia and analgesia in major surgery: The MASTER trial.
Controlled Clinical Trials 2000;21:244‐56.
[DOI] [PubMed] [Google Scholar]
Rigg 2000b {published and unpublished data}
Rigg JRA,
Jamrozik K,
Myles PS,
Silbert B,
Peyton P,
Parsons RW,
et al.
Design of the multicenter Australian study of epidural anesthesia and analgesia in major surgery: The MASTER trial.
Controlled Clinical Trials 2000;21:244‐56.
[DOI] [PubMed] [Google Scholar]
Rosen 1987a {published data only}
Rosen MA,
Roizen MF,
Eger II EI,
Glass RH,
Martin M,
Dandekar PV,
et al.
The effect of nitrous oxide on in vitro fertilization success rate.
Anesthesiology 1987;67:42‐4.
[DOI] [PubMed] [Google Scholar]
Rosen 1987b {published data only}
Rosen MA,
Roizen MF,
Eger II EI,
Glass RH,
Martin M,
Dandekar PV,
et al.
The effect of nitrous oxide on in vitro fertilization success rate.
Anesthesiology 1987;67:42‐4.
[DOI] [PubMed] [Google Scholar]
Rovers 2001a {published and unpublished data}
Rovers MM,
Straatman H,
Ingels K,
Wilt GJ,
Broek P,
Zielhuis GA.
Generalizability of trial results based on randomized versus nonrandomized allocation of OME infants to ventilation tubes or watchful waiting.
Journal of Clinical Epidemiology 2001;54:789‐94.
[DOI] [PubMed] [Google Scholar]
Rovers 2001b {published and unpublished data}
Rovers MM,
Straatman H,
Ingels K,
Wilt GJ,
Broek P,
Zielhuis GA.
Generalizability of trial results based on randomized versus nonrandomized allocation of OME infants to ventilation tubes or watchful waiting.
Journal of Clinical Epidemiology 2001;54:789‐94.
[DOI] [PubMed] [Google Scholar]
Rørbye 2005a {published data only}
Rørbye C,
Nørgaard M,
Nilas L.
Medical versus surgical abortion: comparing satisfaction and potential confounders in a partly randomized study.
Human Reproduction 2005;20:834‐8.
[DOI] [PubMed] [Google Scholar]
Rørbye 2005b {published data only}
Rørbye C,
Nørgaard M,
Nilas L.
Medical versus surgical abortion: comparing satisfaction and potential confounders in a partly randomized study.
Human Reproduction 2005;20:834‐8.
[DOI] [PubMed] [Google Scholar]
Schmoor 1996a {published and unpublished data}
Schmoor C,
Oleschewski M,
Schumacher M.
Randomized and non‐randomized patients in clinical trials: Experiences with comprehensive cohort studies.
Statistics in Medicine 1996;15:263‐71.
[DOI] [PubMed] [Google Scholar]
Schmoor 1996b {published and unpublished data}
Schmoor C,
Oleschewski M,
Schumacher M.
Randomized and non‐randomized patients in clinical trials: Experiences with comprehensive cohort studies.
Statistics in Medicine 1996;15(263‐71).
[DOI] [PubMed] [Google Scholar]
Schmoor 1996c {published and unpublished data}
Schmoor C,
Oleschewski M,
Schumacher M.
Randomized and non‐randomized patients in clinical trials: Experiences with comprehensive cohort studies.
Statistics in Medicine 1996;15:263‐71.
[DOI] [PubMed] [Google Scholar]
Schmoor 1996d {published and unpublished data}
Schmoor C,
Oleschewski M,
Schumacher M.
Randomized and non‐randomized patients in clinical trials: Experiences with comprehensive cohort studies.
Statistics in Medicine 1996;15:263‐71.
[DOI] [PubMed] [Google Scholar]
Schmoor 1996e {published and unpublished data}
Schmoor C,
Oleschewski M,
Schumacher M.
Randomized and non‐randomized patients in clinical trials: Experiences with comprehensive cohort studies.
Statistics in Medicine 1996;15:263‐71.
[DOI] [PubMed] [Google Scholar]
Schmoor 1996f {published and unpublished data}
Schmoor C,
Oleschewski M,
Schumacher M.
Randomized and non‐randomized patients in clinical trials: Experiences with comprehensive cohort studies.
Statistics in Medicine 1996;15:263‐71.
[DOI] [PubMed] [Google Scholar]
Strandberg 1995 {published and unpublished data}
Strandberg TE,
Salomaa VV,
Vanhanen HT,
Naukkarin VA,
Sarna AJ,
Miettinen TA.
Mortality in participants and non‐participants of a multifactorial prevention study of cardiovascular diseases: A 28 year follow up of the Helsinki businessmen study.
British Heart Journal 1995;74:449‐54.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Sullivan 1982a {published data only}
Sullivan MP,
Fuller LM,
Chen T,
Fisher R,
Fryer C,
Gehan E,
et al.
Intergroup Hodgkin's disease in children study of stages I and II: A preliminary report.
Cancer Treatment Reports 1982;66:937‐47.
[PubMed] [Google Scholar]
Sullivan 1982b {published data only}
Sullivan MP,
Fuller LM,
Chen T,
Fisher R,
Fryer C,
Gehan E,
et al.
Intergroup Hodgkin's disease in children study of stages I and II: A preliminary report.
Cancer Treatment Reports 1982;66:937‐47.
[PubMed] [Google Scholar]
Sullivan 1982c {published data only}
Sullivan MP,
Fuller LM,
Chen T,
Fisher R,
Fryer C,
Gehan E,
et al.
Intergroup Hodgkin's disease in children study of stages I and II: A preliminary report.
Cancer Treatment Reports 1982;66:937‐47.
[PubMed] [Google Scholar]
Urban 1999 {published data only}
Urban P,
Stauffer J‐C,
Bleed D,
Khatchatrian N,
Amann W,
Bertel O,
et al.
A randomized evaluation of early revascularization to treat shock complicating acute myocardial infarction.
European Heart Journal 1999;20:1030‐8.
[DOI] [PubMed] [Google Scholar]
Villamaria 1997a {published and unpublished data}
Villamaria FJ,
Baisden CE,
Hillis A,
Rajab MH,
Rinaldi PA.
Forced‐air warming is no more effective than conventional methods for raising postoperative core temperature after cardiac surgery.
Journal of Cardiothoracic and Vascular Anesthesia 1997;11:708‐11.
[DOI] [PubMed] [Google Scholar]
Villamaria 1997b {published and unpublished data}
Villamaria FJ,
Baisden CE,
Hillis A,
Rajab MH,
Rinaldi PA.
Forced‐air warming is no more effective than conventional methods for raising postoperative core temperature after cardiac surgery.
Journal of Cardiothoracic and Vascular Anesthesia 1997;11:708‐11.
[DOI] [PubMed] [Google Scholar]
Waard 2002a {published data only}
Waard MW,
Vos J,
Bonsel GJ,
Bindels PJE,
Ankum WM.
Management of miscarriage: a randomized controlled trial of expectant mangement versus surgical evaluation.
Human Reproduction 2002;17:2445‐50.
[DOI] [PubMed] [Google Scholar]
Waard 2002aa {published data only}
Waard MW,
Vos J,
Bonsel GJ,
Bindels PJE,
Ankum WM.
Management of miscarriage: a randomized controlled trial of expectant mangement versus surgical evaluation.
Human Reproduction 2002;17:2445‐50.
[DOI] [PubMed] [Google Scholar]
Walker 1986 {published data only}
Walker WS,
Raychaudhury T,
Faichney A,
Prescott RJ,
Tonkin RW,
Sang CTM,
Cameron EWJ,
Reid KG,
Walbaum PR.
Wound colonisation following cardiac surgery.
Journal Cardiovascular Surgery 1986;27:662‐6.
[PubMed] [Google Scholar]
Wallage 2003 {published data only}
Wallage S,
Cooper KG,
Graham WJ,
Parkin DE.
A randomised trial comparing local versus general anaesthesia for microwave endometrial ablation.
BJOG 2003;10:799‐807.
[PubMed] [Google Scholar]
Wetzner 1979 {published data only}
Wetzner SM,
Vincent ME,
Robbins AH.
Ceruletide‐assisted cholecystography: A clinical assessment.
Radiology 1979;131:23‐6.
[DOI] [PubMed] [Google Scholar]
Wikdahl 1992 {published and unpublished data}
Wikdahl AM,
Granbom L,
Stegmayr BG.
CAPD bag changing with integrated disconnect system gives lower incidence of peritonitis than with UV‐box system.
Advances in Peritoneal Dialysis 1992;8:276‐80.
[PubMed] [Google Scholar]
Williford 1993 {published data only}
Williford WO,
Krol WF,
Buzby GP.
Comparison of eligible randomized patients with two groups of ineligible patients: can the results of the VA total parenteral nutrition clinical trial be generalized?.
Journal of Clinical Epidemiology 1993;46:1025‐34.
[DOI] [PubMed] [Google Scholar]
Witt 2006a {published data only}
Witt CM,
Jena S,
Brinkhaus B,
Liecker B,
Wegscheider K,
Willich SN.
Acupuncture in patients with osteoarthritis of the knee or hip.
Arthritis & Rheumatism 2006;54:3485‐93.
[DOI] [PubMed] [Google Scholar]
Witt 2006b {published data only}
Witt CM,
Jena S,
Brinkhaus B,
Liecker B,
Wegscheider K,
Willich SN.
Acupuncture for patients with chronic neck pain.
Pain 2006;125:98‐106.
[DOI] [PubMed] [Google Scholar]
Witt 2006c {published data only}
Witt CM,
Jena S,
Selim D,
Brinkhaus B,
Reinhold T,
Wruck K,
et al.
Pragmatic randomized trial evaluating the clinical and economic effectiveness of acupuncture for chronic low back pain.
American Journal of Epidemiology 2006;164:487‐96.
[DOI] [PubMed] [Google Scholar]
Yamamoto 1992a {published data only}
Yamamoto H,
Hughes RW,
Schroeder KW,
Viggiano TR,
DiMagno EP.
Treatment of benign esophageal stricture by Eder‐Puestow or balloon dilators: A comparison between randomized and prospective nonrandomized trials.
Mayo Clinic Proc 1992;67:228‐36.
[DOI] [PubMed] [Google Scholar]
Yamamoto 1992b {published data only}
Yamamoto H,
Hughes RW,
Schroeder KW,
Viggiano TR,
DiMagno EP.
Treatment of benign esophageal stricture by Eder‐Puestow or balloon dilators: A comparison between randomized and prospective nonrandomized trials.
Mayo Clinic Proc 1992;67:228‐36.
[DOI] [PubMed] [Google Scholar]
Yamani 2005 {published data only}
Yamani MH,
Avery R,
Mawhorter SD,
McNeill A,
Cook D,
Ratliff NB,
et al.
The impact of cytgam on cardiac transplant recipients with moderate hypogammaglobulinemia: A randomized single‐center study.
Journal Heart and Lung Transplant 2005;24:1766‐9.
[DOI] [PubMed] [Google Scholar]
Yersin 1996 {published data only}
Yersin B,
Besson J,
Duc‐Mingot S,
Burnand B.
Screening and referral of alcoholic patients in a general hospital. A clinical trial.
European Addiction Research 1996;2:94‐101.
[Google Scholar]
Young 1996 {published data only}
Young JDH,
MacEwen CJ,
Ogston SA.
Congenital nasolacrimal duct obstruction in the second year of life: A multicentre trial of management.
Eye 1996;10:485‐91.
[DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Akaza 1995 {published data only}
Akaza H,
Hinotsu S,
Aso Y,
Kakizoe T,
Koiso K.
Bacillus Calmette‐Guerin treatment of existing papillary bladder cancer and carcinoma in situ of the bladder. Four‐year results. The Bladder Cancer BCG Study Group.
Cancer 1995;75(2):552‐9.
[DOI] [PubMed] [Google Scholar]
Albert 1997 {published and unpublished data}
Albert SM,
Sano M,
Marder K,
Jacobs DM,
Brandt J,
Albert M,
et al.
Participation in clinical trials and long‐term outcomes in Alzheimer's disease.
Neurology 1997;49:38‐43.
[DOI] [PubMed] [Google Scholar]
Amadori 1993 {published data only}
Amadori S,
Testi AM,
Arico M,
Comelli A,
Giuliano M,
Madon E,
et al.
Prospective comparative study of bone marrow transplantation and postremission chemotherapy for childhood acute myelogenous leukemia.
Journal of Clinical Oncology 1993;11:1046‐54.
[DOI] [PubMed] [Google Scholar]
Ashok 2002 {published data only}
Ashok PW,
Kidd A,
Flett GMM,
Fitzmaurice A,
Graham W,
Templeton A.
A randomized comparison of medical abortion and surgical vacuum aspiration at 10‐13 weeks gestation.
Human Reproduction 2002;17:92‐8.
[DOI] [PubMed] [Google Scholar]
Azurin 1971 {published data only}
Azurin JC,
Alvero M.
Cholera Incidence in a population offered Cholera vaccination: Comparison of cooperative and uncooperative groups.
Bulletin World Health Organisation 1971;44:815‐9.
[PMC free article] [PubMed] [Google Scholar]
Bahit 2003 {published data only}
Bahit MC,
Cannon CP,
Antman EM,
Murphy SA,
Gibson CM,
McCabe CH,
et al.
Direct comparison of characteristics, treatment, and outcomes of patients enrolled versus patients not enrolled in a clinical trial at centers participating in the TIMI 9 Trial and TIMI 9 Registry.
American Heart Journal 2003;145(1):109‐17.
[DOI] [PubMed] [Google Scholar]
Banach 2000 {published data only}
Banach MJ,
Ferrone PJ,
Trese MT.
A comparison of dense versus less dense diode laser photocoagulation patterns for threshold retinopathy of prematurity.
Ophthalmology 2000;107:324‐8.
[DOI] [PubMed] [Google Scholar]
Bangstad 1992 {published data only}
Bangstad HJ,
Kofoed‐Enevoldsen A,
Dahl‐Jorgensen K,
Hanssen KF.
Glomerular charge selectivity and the influence of improved blood glucose control in type 1 (insulin‐dependent) diabetic patients with microalbuminuria.
Diabetologia 1992;35(12):1165‐9.
[DOI] [PubMed] [Google Scholar]
Barnett 1992 {published and unpublished data}
Barnett BJ,
Parfrey PS,
Vavasour HM,
McDonald J,
Kent G,
Hefferton D,
et al.
Contrast nephropathy in patients with impared renal function: High versus low osmolar media.
Kidney International 1992;41:1274‐9.
[DOI] [PubMed] [Google Scholar]
Bartalena 1983 {published and unpublished data}
Bartalena L,
Marcocci C,
Chiovato L,
Laddaga M,
Lepri G,
Andreani D,
Cavallacci G,
Baschieri L,
Pinchera A.
Orbital cobalt irradiation combined with systemaic corticosteroids for Graves' ophthalmopathy: Comparison with systemic corticosteroids alone.
Journal of Clinical Endocrinology and Metabolism 1983;56:1139‐44.
[DOI] [PubMed] [Google Scholar]
Behar 1975 {published data only}
Behar J,
Sheahan DG,
Biancani P,
Spiro HM,
Storer EH.
Medical and surgical management of reflux esophagitis. A 38‐month report of a prospective clinical trial.
The New England Journal of Medicine 1975;293:263‐8.
[DOI] [PubMed] [Google Scholar]
Bertelsen 1991 {published data only}
Bertelsen K.
Protocol allocation and exclusion in two Danish randomised trials in ovarian cancer.
British Journal of Cancer 1991;64:1172‐6.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Bertelsen 1994 {published data only}
Bertelsen K,
Andersen JE.
Long‐term survival and prognostic factors in advanced epithelial ovarian cancer with special emphasis upon the effects of protocol inclusion.
International Journal of Gynecological Cancer 1994;4:180‐7.
[DOI] [PubMed] [Google Scholar]
Bifano 1994 {published data only}
Bifano EM,
Miggiani WP,
Parker PR.
Impact of transfusion guidelines on transfusion practices in premature infants.
Pediatric Research 1994;35:216A.
[Google Scholar]
Black SB,
Shinefield HR,
Ray P,
Lewis EM,
Fireman B,
Hiatt R,
et al.
Safety of combined oligosaccharide conjugate Haemophilus influenzae type b (HbOC) and whole cell diphtheria‐tetanus toxoids‐pertussis vaccine in infancy.
Pediatric Infectious Diseases Journal 1993;12:981‐5.
[DOI] [PubMed] [Google Scholar]
Boros 1985 {published and unpublished data}
Boros L,
Chuang C,
Butler FO,
Bennett JM.
Leukemia in Rochester (NY). A 17‐year experience with an analysis of the role of cooperative group (ECOG) participation.
Cancer 1985;56:2161‐9.
[DOI] [PubMed] [Google Scholar]
Bouchet 1996 {published and unpublished data}
Bouchet C,
Guillemin F,
Briancon S.
Nonspecific effects of longitudinal studies: Impact on quality of life measures.
Journal of Clinical Epidemiology 1996;49:15‐20.
[DOI] [PubMed] [Google Scholar]
Brower 2000 {published data only}
Brower RG,
Matthay MA,
Morris A,
Schoenfeld D,
Thompson BT,
Wheeler A.
Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome.
The New England Journal of Medicine 2000;342:1301‐8.
[DOI] [PubMed] [Google Scholar]
Brown 1981 {published and unpublished data}
Brown CA,
Hutter AM,
DeSanctis RW,
Gold HK,
Leinbach RC,
Robert_niles A,
Austen WG,
Buckley MJ.
Prospective study of medical and urgent surgical therapy in randomizable patients with unstable angina pectoris: Results of in‐hospital and chronic mortallity and morbidity.
American Heart Journal 1981;102:959‐64.
[DOI] [PubMed] [Google Scholar]
Brown 1999 {published data only}
Brown N,
Melville M,
Gray D,
Young T,
Skene AM,
Wilcox RG,
et al.
Relevance of clinical trial results in myocardial infarction to medical practice: comparison of four year outcome in participants of a thrombolytic trial, patients receiving routine thrombolysis, and those deemed ineligible for trombolysis.
Hearth 1999;81:598‐602.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Browne 1990 {published data only}
Browne MJ,
Potter D,
Gress J,
Cotton D,
Hiemenz J,
Thaler M,
et al.
A randomized trial of open lung biopsy versus empiric antimicrobial therapy in cancer patients with diffuse pulmonary infiltrates.
Journal of Clinical Oncology 1990;8:222‐9.
[DOI] [PubMed] [Google Scholar]
Canfield 1977 {published data only}
Canfield R,
Rosner W,
Skinner J,
McWhorter J,
Resnick L,
Feldman F,
et al.
Diphosphonate therapy of Paget's disease of the bone.
Journal of Clinical Endocrinological Metabolism 1977;44:96‐106.
[DOI] [PubMed] [Google Scholar]
Caplan 1984 {published data only}
Caplan DB,
Buchanan CN.
Treatment of lower respiratory tract infections due to pseudomonas aeruginosa in patients with cystic fibrosis.
Reviews of Infectious Diseases 1984;6:S705‐10.
[DOI] [PubMed] [Google Scholar]
Carroll 1999 {published and unpublished data}
Carroll KM,
Nich C,
McLellan AT,
McKay JR,
Rounsaville BJ.
'Research' versus 'real‐world' patients: representativeness of participants in clinical trials of treatments for cocaine dependence.
Drug and Alcohol Dependence 1999;54:171‐7.
[DOI] [PubMed] [Google Scholar]
Chadwick 1991 {published and unpublished data}
Chadwick DW.
A randomized study of antiepilectic drug withdrawl in patients in remission of epilepsy.
Boll Lega It Epil 1991;75/76:29‐36.
[Google Scholar]
Chaitman 1986 {published data only}
Chaitman BR,
Davis KB,
Kaiser GC,
Mudd G,
Wiens RD,
Ng GS,
et al.
The role of coronary bypass surgery for 'left main equivalent' coronary disease: The coronary artery surgery study registry.
Circulation 1986;74 S III:III‐17‐25.
[PubMed] [Google Scholar]
Chaitman 1990 {published data only}
Chaitman BR,
Ryan TJ,
Kronmal RA,
Foster ED,
Frommer PL,
Killip T,
et al.
Coronary artery surgery study (CASS): Comparability of 10 year survival in randomized and randomizable patients.
Journal of the American College of Cardiology 1990;16:1071‐8.
[DOI] [PubMed] [Google Scholar]
Chen 2000 {published data only}
Chen CI,
Skingley P,
Meyer RM.
A comparison of elderly patients with aggressive histology lymphoma who were entered or not entered on to a randomised phase II trial.
Leukemia and Lymphoma 2000;38:327‐34.
[DOI] [PubMed] [Google Scholar]
Clemens 1992 {published data only}
Clemens JD,
Loon FFPL,
Rao M,
Sack DA,
Ahmed F,
Chakraborty J,
et al.
Nonparticipation as a determinant of adverse health outcomes in a field of oral cholera vaccines.
American Journal of Epidemiology 1992;135:865‐74.
[DOI] [PubMed] [Google Scholar]
Cohen 1983 {published data only}
Cohen CJ,
Goldberg JD,
Holland JF,
Bruckner HW,
Deppe G,
Gusberg SB,
et al.
Improved therapy with cisplatin regimens for patients with ovarian carcinoma (FIGO Stages III and IV) as measured by surgical end‐staging (second‐look operation).
American Journal of Obstertrics and Gynecology 1983;145:955‐67.
[DOI] [PubMed] [Google Scholar]
Cooper 1999 {published data only}
Cooper JS,
Guo MD,
Herskovic A,
Macdonald JS,
Martenson JA,
Al‐Sarraf M,
et al.
Chemoradiotherapy of locally advanced esophageal cancer. Long‐term follow‐up of a prospective randomized trial (RTOG 85‐01).
Journal of the American Medical Association 1999;281:1623‐7.
[DOI] [PubMed] [Google Scholar]
Cottin 1999 {published data only}
Cottin V,
Arpin D,
Lasset C,
Cordier J‐F,
Brune J,
Chauvin F,
et al.
Small‐cell lung cancer: Patients included in clinical trials are not representative of the patient population as a whole.
Annals of Oncology 1999;10:809‐15.
[DOI] [PubMed] [Google Scholar]
Cunningham 1989 {published data only}
Cunningham AJ,
Tocco EK.
A randomized trial of group psychoeducational therapy for cancer patients.
Patient Education and Counseling 1989;14:101‐14.
[Google Scholar]
Cutlip 2001 {published data only}
Cutlip DE,
Baim DS,
Ho KKL,
Popma JJ,
Lansky AJ,
Cohen DJ,
et al.
Stent thrombosis in the modern era: A pooled analysis of multicenter coronary stent clinical trials.
Circulation 2001;103:1967‐71.
[DOI] [PubMed] [Google Scholar]
Dahlberg 1999 {published data only}
Dahlberg M,
Glimelius B,
Påhlman L.
Improved survival and reduction in local failure rates after preoperative radiotherapy. Evidence for the generalizability of the results of Swedish rectal cancer trial.
Annals of Surgery 1999;229:493‐7.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Davis 1988 {published data only}
Davis K.
The comprehensive cohort study: The use of registry data to confirm and extend a randomized trial.
Recent results in cancer research 1988;111:138‐48.
[DOI] [PubMed] [Google Scholar]
Decensi 2003 {published data only}
Decensi A,
Robertson C,
Viale G,
Pigatto F,
Johansson H,
Kisanga ER,
et al.
A randomized trial of low‐dose tamoxifen on breast cancer proliferation and blood estrogenic biomarkers.
Journal of the National Cancer Institute 2003;95(11):779‐90.
[DOI] [PubMed] [Google Scholar]
Detre 1999 {published data only}
Detre KM,
Guo P,
Holubkov R,
Califf RM,
Sopko G,
Bach R,
et al.
Coronary revascularization in diabetic patients: A comparison of the randomized and observational components of the bypass angioplasty revascularization investigation (BARI).
Circulation 1999;99:633‐40.
[DOI] [PubMed] [Google Scholar]
Deuschle 2004 {published data only}
Deuschle M,
Krumm B,
Bindeballe N,
Colla M,
Hamann B,
Lederbogen F,
et al.
Open‐label non‐randomized versus double‐blind randomized antidepressive treatment: what are the advantages of clinical decision over randomization?.
Pharmacopsychiatry 2004;37(6):299‐302.
[DOI] [PubMed] [Google Scholar]
Devine 1973 {published data only}
Devine DA,
Fernald PS.
Outcome effects of receiving a preferred, randomly assigned, or nonpreferred therapy.
Journal of Counseling and Clinical Psychology 1973;41:104‐7.
[DOI] [PubMed] [Google Scholar]
Diehl 1995 {published data only}
Diehl V,
Loeffler M,
Pfreundschuh M,
Ruehl U,
Hasenclever D,
Nister‐Backes H,
et al.
Further chemotherapy versus low‐dose involved field radiotherapy as consolidation of complete remission after six cycles of alternating chemotherapy in patients with advanced Hodgkin's disease.
Annals of Oncology 1995;6:901‐10.
[DOI] [PubMed] [Google Scholar]
Exner 1999 {published data only}
Exner DV,
Reiffel JA,
Epstein AE,
Ledingham R,
Reiter MJ,
YAo Q,
et al.
Beta‐blocker use and survival in patients with ventricular fibrillation or symptomatic ventricular tachycardia: The antiarrhytmics versus implantable defibrillators (AVID) trial.
Journal of American College of Cardiology 1999;34:325‐33.
[DOI] [PubMed] [Google Scholar]
Fossa 2002 {published data only}
Fossa SD,
Skovlund E.
Selection of patients may limit the generalizability of results from cancer trials.
Acta Oncologica 2002;41(2):131‐7.
[DOI] [PubMed] [Google Scholar]
Franz 1995 {published data only}
Franz MJ,
Monk A,
Barry B,
McClain K,
Weaver T,
Cooper N,
et al.
Effectiveness of medical nutrition therapy provided by dietitians in the management of non‐insulin‐dependent diabetes mellitus: a randomized, controlled clinical trial.
Journal of the American Dietetic Association 1995;95(9):1009‐17.
[DOI] [PubMed] [Google Scholar]
Frazee 1996 {published data only}
Frazee RC,
Roberts JW,
Symmonds RE,
Snyder SK,
Hendricks JC,
Smith RW,
et al.
Open versus stereotactic breast biopsy.
The American Journal of Surgery 1996;172:491‐5.
[DOI] [PubMed] [Google Scholar]
Frucht‐Pery 2006 {published data only}
Frucht‐Pery J,
Raiskup F,
Ilsar M,
Landau D,
Orucov F,
Solomon A.
Conjunctival autografting combined with low‐dose mitomycin C for prevention of primary pterygium recurrence.
American Journal of Ophthalmology 2006;141(6):1044‐50.
[DOI] [PubMed] [Google Scholar]
GBSG 1995 {published data only}
The German Breast Cancer Study Group (GBSG).
Therapy of small breast cancer ‐ Four‐year results of a prospective non‐randomised study.
Breast Cancer Research and Treatment 1995;34:1‐13.
[DOI] [PubMed] [Google Scholar]
Gonwa 2002 {published data only}
Gonwa TA,
Hricik DE,
Brinker K,
Grinyo JM,
Schena FP,
Sirolimus Renal Function Study Group.
Improved renal function in sirolimus‐treated renal transplant patients after early cyclosporine elimination.
Transplantation 2002;74(11):1560‐7.
[DOI] [PubMed] [Google Scholar]
Gossop 1986 {published data only}
Gossop M,
Johns A,
Green L.
Opiate withdrawl: Inpatient versus outpatient programmes and preferred versus random assignment to treatment.
British Medical Journal 1986;293:103‐4.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Groff 2004 {published data only}
Groff A,
Burns B,
Swanson J,
Swartz M,
Wagner HR,
Tompson M.
Caregiving for persons with mental illness: the impact of outpatient commitment on caregiving strain.
Journal of Nervous & Mental Disease 2004;192(8):554‐62.
[DOI] [PubMed] [Google Scholar]
Haberkern 1997 {published data only}
Haberkern CM,
Neumayr LD,
Orringer EP,
Earles AN,
Robertson SM,
Black D,
et al.
Cholecystectomy in sickle cell anemia patients: Perioperative outcome of 364 cases from the national preoperative transfusion study.
Blood 1997;5:1533‐42.
[PubMed] [Google Scholar]
Hauth 1983 {published data only}
Hauth JC,
Gilstrap LC,
Brekken AL,
Hauth JM.
The effect of 17a‐hydroxyprogesterone caproate on pregnancy outcome in an active‐duty military population.
American Journal of Obstetrics and Gynecology 1983;146:187‐9.
[DOI] [PubMed] [Google Scholar]
Hertegard 2002 {published data only}
Hertegard S,
Hallen L,
Laurent C,
Lindstrom E,
Olofsson K,
Testad P,
et al.
Cross‐linked hyaluronan used as augmentation substance for treatment of glottal insufficiency: safety aspects and vocal fold function.
Laryngoscope 2002;112(12):2211‐9.
[DOI] [PubMed] [Google Scholar]
Hjorth 1992 {published data only}
Hjorth M,
Holmberg E,
Rodjer S,
Westin J for the myeloma group of western Sweden.
Impact of active and passive exclusions on the results of a clinical trial in multiple myeloma.
British Journal of Hematology 1992;80:55‐61.
[DOI] [PubMed] [Google Scholar]
Hoh 1998 {published data only}
Hoh R,
Pelfini A,
Neese RA,
Chan M,
Cello JP,
Cope FO,
et al.
De novo lipogenesis predicts short‐term body‐composition response by bioelectrical impedance analysis to oral nutritional supplements in HIV‐associated wasting.
American Journal of Clinical Nutrition 1998;68(1):154‐63.
[DOI] [PubMed] [Google Scholar]
Holubkov 1999 {published data only}
Holubkov R,
Detre KM,
for the bypass Angioplasty revascularization investigation (BARI) researchers.
Differences in 5‐year outcome for BARI trial and registry diabetics.
Diabetes 1999;16:27‐31.
[Google Scholar]
Jack 1990 {published data only}
Jack WJL,
Chetty U,
Rodger A.
Recruitment to a prospective breast conservation trial: Why are so few patients randomised?.
British Medical Journal 1990;301:83‐5.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Jensen 1996 {published and unpublished data}
Jensen LP,
Nielsen OM,
Schroeder TV.
The importance of complete follow‐up for results after femoro‐infrapopliteal vascular surgery.
European Journal of Vascular and Endovascular Surgery 1996;12:282‐6.
[DOI] [PubMed] [Google Scholar]
Jeremic 1999 {published data only}
Jeremic B,
Shibamoto Y,
Nikolic N,
Milicic B,
Milisavljevic S,
Dagovic A,
et al.
Role of radiation therapy in the combined‐modality treatment of patients with extensive disease small‐cell lung cancer: A randomized study.
Journal of Clinical Oncology 1999;17(7):2092‐9.
[DOI] [PubMed] [Google Scholar]
Jha 1996 {published data only}
Jha P,
Deboer D,
Sykora K,
Naylor CD.
Characteristics and mortality outcomes of thrombolysis trial participants and nonparticipants: A population‐based comparison.
Journal of the American College of Cardiology 1996;27:1335‐42.
[DOI] [PubMed] [Google Scholar]
Julien 2000 {published data only}
Julien J‐P,
Bijker N,
Fentiman IS,
Peterse JL,
Delledonne V,
Rouanet P,
et al.
Radiotherapy in breast‐conserving treatment for ductal carcinoma in situ: First results of the EORTC randomised phase III trial 10853.
The Lancet 2000;355:528‐33.
[DOI] [PubMed] [Google Scholar]
Kahan 2000 {published data only}
Kahan BD,
for The Rapamune US Study Group.
Efficacy of sirolimus compared with azathioprine for reduction of acute renal allograft rejection: A randomized multicentre study.
The Lancet 2000;356:194‐202.
[DOI] [PubMed] [Google Scholar]
Kamal 2006 {published data only}
Kamal SM,
Moustafa KN,
Chen J,
Fehr J,
Abdel MA,
Khalifa KE,
et al.
Duration of peginterferon therapy in acute hepatitis C: a randomized trial.[see comment][erratum appears in Hepatology. 2006 Oct;44(4):1055].
Hepatology 2006;43(5):923‐31.
[DOI] [PubMed] [Google Scholar]
Karande 1997 {published data only}
Karande V,
Korn A,
Morris R,
Rao R,
Balin M,
Rinehart J,
et al.
A prospective randomized trial, assessing outcome and cost of IVF as a first choice treatment versus a traditional infertility treatment algorithm.
1997:S41.
[DOI] [PubMed]
Kober 1995 {published data only}
Kober L,
Torp‐Pedersen C,
on behalf of the TRACE study group.
Clinical characteristics and mortality of patients screened for entry into the trandolapril cardiac evaluation (TRACE) study.
American Journal of Cardiology 1995;76:1‐5.
[DOI] [PubMed] [Google Scholar]
Kober 2000 {published data only}
Kober L,
Thomsen PEB,
Moller M,
Torp‐Pedersen C,
Carlsen J,
Sandoe E,
et al.
Effect of dofetilide in patients with recent myocardial infarction and left‐ventricular dysfunction: A randomised trial.
The Lancet 2000;356:2052‐8.
[DOI] [PubMed] [Google Scholar]
Korvick 1992 {published and unpublished data}
Korvick JA,
Peacock JE,
Muder RR,
Wheeler RR,
Yu VL.
Addition of Rifampin to combination antibiotic therapy for Pseudomonas aeruginosa bacteria: Prospective trial using the Zelen protocol.
Antimicrobial Agents and Chemotherapy 1992;36:620‐5.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Lechner 1983 {published data only}
Lechner GW,
Elliot DW.
Comparison of weight loss after gastric exclusion and partitioning.
Archives of Surgery 1983;118:685‐92.
[DOI] [PubMed] [Google Scholar]
Lennox 1979 {published data only}
Lennox EL,
Stiller CA,
Morris Jones PH,
Kinner Wilson LM.
Nephroblastoma: Treatment during 1970‐3 and the effect on survival of inclusion in the first MRC trial.
British Medical Journal 1979;2:567‐9.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Libman 2000 {published data only}
Libman R,
Bhatnagar R,
Ding L,
Kwiatkowski T,
Barr W.
Placebo treatment in acute stroke trials : benefit or harm to patients?.
Stroke 2000;31(2):355‐7.
[DOI] [PubMed] [Google Scholar]
Licht 1997 {published and unpublished data}
Licht RW,
Gouliaev G,
Vestergaard P,
Frydenberg M.
Generalisability of results from randomised drug trials. A trial on antimanic treatment.
British Journal of Psychiatry 1997;170:264‐7.
[DOI] [PubMed] [Google Scholar]
Link 1986 {published data only}
Link MP,
Goorin AM,
Miser AW,
Green AA,
Pratt CB,
Belasco JB,
et al.
The effect of adjuvant chemotherapy on relapse‐free survival in patients with osteosarcoma of the extremity.
The New England Journal of Medicine 1986;314:1600‐6.
[DOI] [PubMed] [Google Scholar]
Madsen 1993 {published data only}
Madsen JK,
Hansen JF,
the DAVIT‐II Study Group.
Mortality of patients excluded from the Danish verapamil infarction trial II.
European Heart Journal 1993;14:177‐9.
[DOI] [PubMed] [Google Scholar]
MAGPIE 1995 {published data only}
The Eclampsia Trial Collaborative Group.
Which anticonvulsant for women with eclampsia? Evidence from the Collaborative Eclampsia Trial.
Lancet 1995;345:1455‐63.
[PubMed] [Google Scholar]
Marsa‐Vila 1991 {published data only}
Marsa‐Vila L,
Gorin NC,
Laporte JP,
Labopin M,
Dupuy‐Montbrun MC,
Fouillard L,
et al.
Prophylactic heparin does not prevent liver veno‐occlusive disease following autologous bone marrow transplantation.
European Journal of Haematology 1991;47:346‐54.
[DOI] [PubMed] [Google Scholar]
Mayers 2001 {published and unpublished data}
Mayers C,
Panzarella T,
Tannock IF.
Analysis of the prognostic effects of inclusion in a clinical trial and of myelosuppression on survival after adjuvant chemotherapy for breast carcinoma.
Cancer 2001;91:2246‐57.
[PubMed] [Google Scholar]
McAfee 2006 {published data only}
McAfee PC,
Geisler FH,
Saiedy SS,
Moore SV,
Regan JJ,
Guyer RD,
et al.
Revisability of the CHARITE artificial disc replacement: analysis of 688 patients enrolled in the U.S. IDE study of the CHARITE Artificial Disc.
Spine 2006;31(11):1217‐26.
[DOI] [PubMed] [Google Scholar]
McCusker 1982 {published data only}
McCusker J,
Wax A,
Bennett JM.
Cancer patient accessions into clinical trials. A pilot investigation into some patient and physician determinants of entry.
American Journal of Clinical Oncology 1982;5:227‐36.
[DOI] [PubMed] [Google Scholar]
Meade 2000 {published data only}
Meade TW,
Brennan PJ,
on behalf of the MRC General Practice Research Framework.
Determination of who may derive most benefit from aspirin in primary prevention: Subgroup results from a randomised controlled trial.
British Medical Journal 2000;321:13‐7.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Meier 1985 {published and unpublished data}
Meier P,
Ferguson DJ,
Karrison T.
A controlled trial of extended radical mastectomy.
Cancer 1985;55:880‐91.
[DOI] [PubMed] [Google Scholar]
Mendonca 1983 {published and unpublished data}
Mendonca PJ,
Brehm SS.
Effects of choice on behavioral treatment of overweight children.
Journal of Social and Clinical Psychology 1983;1(343‐58).
[Google Scholar]
Merlino 2001 {published and unpublished data}
Merlino JI,
Malangoni MA,
Smith CM,
Lange RL.
Prospective randomized trials affect the outcomes of intraabdominal infection.
Annals of Surgery 2001;233:859‐66.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Millat 1993 {published data only}
Millat B,
Hay J‐M,
Valleur P,
Fingerhut A,
Fagniez P‐L,
and the French Association for surgical research.
Emergency surgical treatment for bleeding duodenal ulcer: Oversewing plus vagotomy versus gastric resection, a controlled randomized trial.
World Journal of Surgery 1993;17:568‐74.
[DOI] [PubMed] [Google Scholar]
Moynihan C,
Bliss JM,
Davidson J,
Burchell L,
Horwich A.
Evaluation of adjuvant psychological therapy in patients with testicular cancer: Randomised controlled trial.
British Medical Journal 1998;316:429‐35.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Mundy 1983 {published data only}
Mundy GR,
Wilkinson R,
Heath DA.
Comparative study of available medical therapy for hypercalcemia of malignancy.
The American Journal of Medicine 1983;74:421‐32.
[DOI] [PubMed] [Google Scholar]
Narayan 1998 {published data only}
Narayan KM,
Hoskin M,
Kozak D,
Kriska AM,
Hanson RL,
Pettitt DJ,
et al.
Randomized clinical trial of lifestyle interventions in Pima Indians: a pilot study.
Diabetic Medicine 1998;15(1):66‐72.
[DOI] [PubMed] [Google Scholar]
NASCET 1991 {published data only}
North American Symptomatic Carotid Endarterectomy Trial (NASCET) Steering Committee.
North American symptomatic carotid endarterectomy trial. Methods, patient characteristics, and progress.
Stroke 1991;22:711‐20.
[DOI] [PubMed] [Google Scholar]
Naukkarinen 1989 {published data only}
Naukkarinen VA,
Strandberg TE,
Vanhanen HT,
Salomaa VV,
Sarna SJ,
Miettinen TA.
Mortality rates after multifactorial primary prevention of cardiovascular diseases.
Annals of Medicine 1989;21(6):441‐6.
[DOI] [PubMed] [Google Scholar]
Neill 1991 {published data only}
Neill MA,
Opal SM,
Heelan J,
Giusti R,
Cassidy JE,
White R,
et al.
Failure of Ciprofluxacin to eradicate convalescent fecal excretion after acute samonellosis: Experience during an outbreak in health care workers.
Annals of Internal Medicine 1991;114:195‐9.
[DOI] [PubMed] [Google Scholar]
Newman 2002 {published data only}
Newman NJ,
Scherer R,
Langenberg P,
Kelman S,
Feldon S,
Kaufman D,
et al.
The fellow eye in NAION: report from the ischemic optic neuropathy decompression trial follow‐up study.
American Journal of Ophthalmology 2002;134(3):317‐28.
[DOI] [PubMed] [Google Scholar]
Olschewski 1992 {published data only}
Olschewski M,
Schumacher M,
Davis KB.
Analysis of randomized and nonrandomized patients in clinical trials using the comprehensive cohort follow‐up study design.
Controlled Clinical Trials 1992;13:226‐39.
[DOI] [PubMed] [Google Scholar]
Peterson 2006 {published data only}
Peterson AC,
Harlin H,
Karrison T,
Vogelzang NJ,
Knost JA,
Kugler JW,
et al.
A randomized phase II trial of interleukin‐2 in combination with four different doses of bryostatin‐1 in patients with renal cell carcinoma.
Investigational New Drugs 2006;24(2):141‐9.
[DOI] [PubMed] [Google Scholar]
Phillips 1975 {published data only}
Phillips MM,
Ramsey GR,
Conn HO.
Portacaval anastomosis and peptic ulcer: a nonassociation.
Gastroenterology 1975;68(1):121‐31.
[PubMed] [Google Scholar]
Powles 1997 {published data only}
Powles R,
Raje N,
Milan S,
Millar B,
Shepherd V,
MehtaJ,
et al.
Outcome assessment of a population‐based group of 195 unselected myeloma patients under 70 years of age offered intensive treatment.
Bone Marrow Transplantation 1997;20:435‐43.
[DOI] [PubMed] [Google Scholar]
Quoix 1986 {published data only}
Quoix E,
Finkelstein H,
Wolkove N,
Kreisman H.
Treatment of small‐cell lung cancer on protocol: Potential bias of results.
Journal of Clinical Oncology 1986;4:1314‐20.
[DOI] [PubMed] [Google Scholar]
Ravindranath 1996 {published data only}
Ravindranath Y,
Yeager AM,
Chang MN,
Steuber CP,
Krischer J,
Graham‐Pole J,
et al.
Autologouos bone marrow transplantation versus intensive consolidation chemotherapy for acute myeloid leukemia in childhood.
The New England Journal of Medicine 1996;334:1428‐34.
[DOI] [PubMed] [Google Scholar]
Regan 2006 {published data only}
Regan JJ,
McAfee PC,
Blumenthal SL,
Guyer RD,
Geisler FH,
Garcia R,
et al.
Evaluation of surgical volume and the early experience with lumbar total disc replacement as part of the investigational device exemption study of the Charite Artificial Disc.
Spine 2006;31(19):2270‐76.
[DOI] [PubMed] [Google Scholar]
Rock 1992 {published data only}
Rock G,
Shumak K,
Kelton J,
Blanchette VS,
Buskard N,
Nair R,
Spasoff R.
Thrombotic thrombocytopenic purpura: outcome in 24 patients with renal impairment treated with plasma exchange. Canadian Apheresis Study Group.
Transfusion 1992;32(8):710‐4.
[DOI] [PubMed] [Google Scholar]
Rogers 1995 {published data only}
Rogers WL,
Alderman EL,
Chaitman BR,
DiSciascio G,
Horan M,
Lytle B,
et al.
Bypass angioplasty revasularization investigation (BARI): Baseline clinical and angiographic data.
American Journal of Cardiology 1995;75:9C‐17C.
[PubMed] [Google Scholar]
Rokito 1996 {published and unpublished data}
Rokito SE,
Schwartz MC,
Neuwirth MG.
Deep vein thrombosis after major reconstructive spinal surgery.
Spine 1996;21:853‐9.
[DOI] [PubMed] [Google Scholar]
Rokke 1999 {published and unpublished data}
Rokke PD,
Tomhave JA,
Jocic Z.
The role of client choice and target selection in self‐management therapy for depression in older adults.
Psychology and Aging 1999;14:155‐69.
[DOI] [PubMed] [Google Scholar]
Rychtarik 1998 {published and unpublished data}
Rychtarik RG,
McGillicuddy NB,
Connors GJ,
Whitney RB.
Participant selection biases in a randomized clinical trial of alcoholism treatment settings and intensities.
Alcoholism: Clinical and Experimental Research 1998;22:969‐73.
[DOI] [PubMed] [Google Scholar]
Schmidt 1999 {published data only}
Schmidt B,
Gillie P,
Caco C,
Roberts J,
Roberts R.
Do sick newborn infants benefit from participation in a randomized clinical trial?.
Journal of Pediatrics 1999;134:151‐5.
[DOI] [PubMed] [Google Scholar]
Sha 1995 {published and unpublished data}
Sha BE,
Benson CA,
Pottage JC,
Urbanski PA,
Daugherty SR,
Kessler HA.
HIV infection in women: An observational study of clinical characteristics, disease progression, and survivial for a cohort of women in Chicago.
Journal of Acquired Immune Deficiency Syndrome and Human Retrovirology 1995;8:486‐95.
[PubMed] [Google Scholar]
Sharp 2004 {published data only}
Sharp DM,
Power KG,
Swanson V.
A comparison of the efficacy and acceptability of group versus individual cognitive behaviour therapy in the treatment of panic disorder and agoraphobia in primary care.
Clinical Psychology & Psychotherapy 2004;11(2):73‐82.
[Google Scholar]
Singh 1995 {published data only}
Singh BN,
Kehoe R,
Woosley RL,
Scheinman M,
Quart B,
and the Sotalol Multicenter Study Group.
Multicenter trial of sotalol compared with procainamide in the supression of inducible ventricular tachycardia: A double blind, randomized parallel evaluation.
American Hearth Journal 1995;129:87‐98.
[DOI] [PubMed] [Google Scholar]
Singhal 2003 {published data only}
Singhal A,
Fewtrell M,
Cole TJ,
Lucas A.
Low nutrient intake and early growth for later insulin resistance in adolescents born preterm.
Lancet 2003;361(9363):1089‐97.
[DOI] [PubMed] [Google Scholar]
Smith 1990 {published data only}
Smith P,
Arnesen H.
Mortality in non‐consenters in a post‐myocardial infarction trial.
Journal of Internal Medicine 1990;228:253‐6.
[DOI] [PubMed] [Google Scholar]
Sterling 1997 {published data only}
Sterling RC,
Gottheil E,
Glassman SD,
Weinstein SP,
Serota RD.
Patient treatment choice and compliance. Data from a substance abuse treatment program.
American Journal on Addictions 1997;6(2):168‐76.
[PubMed] [Google Scholar]
Stiller 1989 {published and unpublished data}
Stiller CA,
Draper GJ.
Treatment centre size, entry to trial, and survival in acute lymphoblastic leukemia.
Archives of Diseases in Childhood 1989;64:657‐61.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Stiller 1994 {published and unpublished data}
Stiller CA,
Eatock EM.
Survival from acute non‐lymhocytic leukemia, 1971‐88: A population based study.
Archives of Diseases in Childhood 1994;70:219‐23.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Stiller 1999 {published and unpublished data}
Stiller CA,
Eatock EM.
Patterns of care and survival for children with acute lymphoblastic leukemia diagnosed between 1980 and 1994.
Archives of Diseases in Childhood 1999;81:202‐8.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Stockle 1995 {published data only}
Stockle M,
Meyenburg W,
Wellek S,
Voges GE,
Rossmann M,
Gertenbach U,
Thuroff JW,
et al.
Adjuvant polychemotherapy of nonorgan‐confined bladder cancer after radical cyctectomy revisited: Long‐term results of a controlled prospective study and further clinical experience.
The Journal of Urology 1995;153:47‐52.
[DOI] [PubMed] [Google Scholar]
Stone 1994 {published and unpublished data}
Stone JM,
Page FJ,
Laidlaw CR,
Cooper I.
Selection of patients for randomised trials: A study based on the MACOP‐B vs CHOP in NHL study.
Australia and New Zealand Journal of Medicine 1994;24:536‐40.
[DOI] [PubMed] [Google Scholar]
Straatsma 2003 {published data only}
Straatsma BR,
Diener‐West M,
Caldwell R,
Engstrom RE,
Collaborative Ocular Melanoma Study Group.
Mortality after deferral of treatment or no treatment for choroidal melanoma.
American Journal of Ophthalmology 2003;136(1):47‐54.
[DOI] [PubMed] [Google Scholar]
Swartz 2001 {published data only}
Swartz M,
Swanson JW,
Wagner HR,
Burns BJ,
Hiday VA.
Effects of involuntary outpatient commitment and depot antipsychotics on treatment adherence in persons with severe mental illness.
Journal of Nervous & Mental Disease 2001;189(9):583‐92.
[DOI] [PubMed] [Google Scholar]
Thomas 1990 {published and unpublished data}
Thomas I,
Wright G,
Ward B.
The effect of condom use on cervical intaepithelial neoplasia grade I (CIN I).
Australia and New Zealand Journal of Obstetrics and Gynaecology 1990;30:236‐9.
[DOI] [PubMed] [Google Scholar]
Thompson 2000 {published data only}
Thompson BT for the ARDS network.
Ketoconazole for early treatment of acute lung injury and acute respiratory distress syndrome. A randomized controlled trial.
JAMA 2000;283:1995‐2002.
[DOI] [PubMed] [Google Scholar]
Tuppurainen 1998 {published data only}
Tuppurainen MT,
Komulainen M,
Kroger H,
Honkanen R,
Jurvelin J,
Puntila E,
et al.
Does vitamin D strengthen the increase in femoral neck BMD in osteoporotic women treated with estrogen?.
Osteoporosis International 1998;8(1):32‐8.
[DOI] [PubMed] [Google Scholar]
van Bergen 1995 {published and unpublished data}
Bergen PFMM,
Jonker JJC,
Molhoek GP,
Burgh PH,
Domburg RT,
Deckers JW,
et al.
Characteristics and prognosis of non‐participants of a multi‐centre trial of long‐term anticoagulant treatment after myocardial infarction.
International Journal of Cardiology 1995;49:135‐41.
[DOI] [PubMed] [Google Scholar]
van Eys 1987 {published and unpublished data}
Eys J,
Berry DM,
Crist W,
Doering EJ,
Fernbach DJ,
Pullen J,
et al.
Effect of Trimethprim/ Sulfamethoxazole prophylaxis on outcome of childhood lymphocytic leukemia. A pediatric oncology group study.
Cancer 1987;59:19‐23.
[DOI] [PubMed] [Google Scholar]
Vassilopoulou‐Sellin 1995 {published data only}
Vassilopoulou‐Sellin R,
Asmar L,
Hortobagyi GN,
Klein MJ,
McNeese M,
Singletary SE,
et al.
Estrogen replacement therapy after localized breast cancer: Clinical outcome of 319 women followed prospectively.
Journal of Clinical Oncology 1995;17:1482‐7.
[DOI] [PubMed] [Google Scholar]
Verdonck 1995 {published data only}
Verdonck LF,
Putten WLJ,
Hagenbeek A,
Schouten HC,
Sonneveld P,
Imhoff GW,
et al.
Comparison of chop chemotherapy with autologous bone marrow transplantation for slowly responding patients with aggressive non‐hodgkin's lymphoma.
The New England Journal of Medicine 1995;332:1045‐51.
[DOI] [PubMed] [Google Scholar]
Waard 2002b {published data only}
Waard MW,
Hartman EE,
Ankum WM,
Reitsma JB,
Bindels PJE,
Bonsel G.
Expectant management versus surgical evaluation in first trimester miscarriage: helath‐related quality of life in randomized and non‐randomized patients.
Human Reproduction 2002;17:1638‐42.
[DOI] [PubMed] [Google Scholar]
Ward 1992 {published data only}
Ward LC,
Fielding JWL,
Dunn JA,
Kelly KA,
for the British Stomach Cancer Group.
The selection of cases for randomised trials: A registry survey of concurrent trial and non‐trial patients.
British Journal of Cancer 1992;66:943‐50.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Warren 1982 {published and unpublished data}
Warren WD,
Millikan WJ,
Henderson JM,
Wright L,
Kutner M,
Smith RB,
et al.
Ten years portal hypertensive surgery ar Emory. Results and new perspectives.
Annals of Surgery 1982;195:530‐42.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Weijer 1996 {published and unpublished data}
Weijer C,
Freedman B,
Fuks A,
Robbins J,
Shapiro S,
Skrutkowska M.
What difference does it make to be treated in a clinical trial? A pilot study.
Clinical Investigations in Medicine 1996;19:179‐83.
[PubMed] [Google Scholar]
Weijmar Schultz 1996 {published data only}
Weijmar Schultz WCM,
Gianotten WL,
Meijden WI,
Wiel HBM,
Blindeman L,
Chadha S,
et al.
Behavioral approach with or without surgical intervention to the vulvar vestibulitis syndrome: A prospective randomized and non‐randomized study.
Journal of Psychosomatic Obstetrics and Gynecology 1996;17:143‐8.
[DOI] [PubMed] [Google Scholar]
Weisdorf 1997 {published and unpublished data}
Weisdorf DJ,
Verfaillie CM,
Miller WJ,
Blazar BR,
Perry E,
Shu XO,
et al.
Autologous bone marrow versus non‐mobilized peripheral blood stem cell transplantation for lymphoid malignancies: A prospective comparative trial.
American Journal of Hematology 1997;54:202‐8.
[DOI] [PubMed] [Google Scholar]
Welt 1981 {published data only}
Welt SI,
Dorminy JH,
Jelovsek FR,
Crenshaw MC,
Gall SA.
The effects of prophylactic management and therapeutics on hypertensive disease in pregnancy: preliminary studies.
Obstetrics & Gynecology 57;5(557‐65).
[PubMed] [Google Scholar]
Westerberg 2000 {published data only}
Westerberg VS,
Miller WR,
Tonigan JS.
Comparison of outcomes for clients in randomized versus open trials of treatment for alcohol use disorders.
Journal of Studies on Alcohol 2000;61:720‐7.
[DOI] [PubMed] [Google Scholar]
Whitehouse 2006 {published data only}
Whitehouse PJ,
Rajcan JL,
Sami SA,
Patterson MB,
Smyth KA,
Edland SD,
et al.
ADCS Prevention Instrument Project: Pilot testing of a book club as a psychosocial intervention and recruitment and retention strategy.
Alzheimer Disease & Associated Disorders 2006;20(Suppl 3):203‐8.
[DOI] [PubMed] [Google Scholar]
Wilhelmsen 1976 {published data only}
Wilhelmsen L,
Ljungberg S,
Wedel H,
Werko L.
A comparison between participants and non‐participants in a primary preventive trial.
Journal of Chronic Diseases 1976;29:331‐9.
[DOI] [PubMed] [Google Scholar]
Winger 1989 {published data only}
Winger MJ,
MacDonald DR,
Schold SC,
Cairncross JG.
Selection bias in clinical trials of anaplastic glioma.
Annals of Neurology 1989;26:531‐4.
[DOI] [PubMed] [Google Scholar]
Winters 1981 {published data only}
Winters WD,
Lamm DL.
Antibody responses to Bacillus Calmette‐Guerin during immunotherapy in bladder cancer patients.
Cancer Research 1981;41:2672‐6.
[PubMed] [Google Scholar]
Woodcock 2001 {published data only}
Woodcock NP,
Zeigler D,
Palmer MD,
Buckley P,
Mitchell CJ,
MacFie J.
Enteral versus parenteral nutrition: A pragmatic study.
Nutrition 17;1(1‐12).
[DOI] [PubMed] [Google Scholar]
Woodhouse 1995 {published data only}
Woodhouse SP,
Cox S,
Boyd P,
Case C,
Weber M.
High dose and standard dose adrenaline do not alter survival, compared with placebo, in cardiac arrest.
Resuscitation 1995;30(3):243‐9.
[DOI] [PubMed] [Google Scholar]
Wyse 1991 {published and unpublished data}
Wyse DG,
Hallstrøm A,
McBride R,
Cohen JD,
Steinberg JS,
Mahmarian J,
et al.
Events in the Cardiac Arrhythmia Suppression Trial (CAST): Mortality in patients surviving open label titration but not randomized to double blind therapy.
Journal of the American College of Cardiology 1991;18:20‐8.
[DOI] [PubMed] [Google Scholar]
References to studies awaiting assessment
Adriaensen 2004 {published data only}
Adriaensen MEAPM,
Kock MCJM,
Stijnen T,
Sambeek MRHM,
Urk H,
Pattynama PMT,
et al.
Peripheral arterial disease: Therapeutic confidence of CT versus digital subtraction angiography and efffects on additional imaging recommendations.
Radiology 2004;233:385‐91.
[DOI] [PubMed] [Google Scholar]
Berr 2001 {published data only}
Berr F,
Liebertruth J,
Caca K,
Giesse A,
Huster D,
Moessner J,
et al.
Photodynamic therapy (PDT) or non‐resectable cholangiocracinoma (CC)‐first results of a randomized study (abstract).
Journal of Hepatology 2001;34(1):107.
[Google Scholar]
Beutel 2005 {published data only}
Beutel ME,
Zwerenz R,
Bleichner F,
Vorndran A,
Gustson D,
Knickenberg RJ.
Vocational training integrated into inpatient psychosomatic rehabilitation‐‐short and long‐term results from a controlled study.
Disability & Rehabilitation 2005;27(15):891‐900.
[DOI] [PubMed] [Google Scholar]
Bjorklund 2004 {published data only}
Bjorklund E,
Lindahl B,
Stenestrand U,
Swahn E,
Dellborg M,
Pehrsson K,
et al.
Outcome of ST‐elevation myocardial infarction treated with thrombolysis in the unselected population is vastly different from samples of eligible patients in a large‐scale clinical trial.
American Heart Journal 2004;148:566‐73.
[DOI] [PubMed] [Google Scholar]
Brandberg 1999 {published data only}
Brandberg Y,
Malm M,
Rutqvist LE,
Jonsson E,
Blomqvist L.
A prospective randomised study (named SVEA) of three methods of delayed breast reconstruction. Study design, patients' preoperative problems and expectations.
Scandinavian Journal of Plastic & Reconstructive Surgery & Hand Surgery 1999;33(2):209‐16.
[DOI] [PubMed] [Google Scholar]
Burgers 2002 {published data only}
Burgers JA,
Arance A,
Ashcroft L,
Hodgetts J,
Lomax L,
Thatcher N.
Identical chemotherapy schedules given on and off trial protocol in small cell lung cancer: response and survival results.
British Journal of Cancer 2002;87(5):562‐66.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Campbell 2006 {published data only}
Campbell M,
Wileman S,
Grant A,
Ramsay C,
Reflux Trial Group.
The partially‐randomised patient‐preference design: lessons from the REFLUX Trial [abstract].
Clinical Trials 2006;3:203‐4.
[Google Scholar]
Chiradejnant 2003 {published data only}
Chiradejnant A,
Maher CG,
Latimer J,
Stepkovitch N.
Efficacy of "therapist‐selected" versus "randomly selected" mobilisation techniques for the treatment of low back pain: a randomised controlled trial.
Australian Journal of Physiotherapy 2003;49(4):233‐41.
[DOI] [PubMed] [Google Scholar]
Cho 2005 {published data only}
Cho AH,
Jackson GL,
Bosworth HB.
Patient Preference and Validity of Randomized Controlled Trials: Comment.
JAMA 2005;294(1):41.
[DOI] [PubMed] [Google Scholar]
COMSG 2003 {published data only}
Collaborative Ocular Melanoma Study Group.
Trends in size and treatment of recently diagnosed choroidal melanoma, 1987‐1997: findings from patients examined at collaborative ocular melanoma study (COMS) centers: COMS report no. 20.
Archives of Ophthalmology 2003;121(8):1156‐62.
[DOI] [PubMed] [Google Scholar]
Dickersin 2003 {published data only}
Dickersin K,
Munro M,
Langenberg P,
Scherer R,
Frick KD,
Weber AM,
et al.
Surgical Treatments Outcomes Project for Dysfunctional Uterine Bleeding (STOP‐DUB): design and methods.
Controlled Clinical Trials 2003;24(5):591‐609.
[DOI] [PubMed] [Google Scholar]
Dutoit 2000 {published data only}
Dutoit R,
Situ P,
Simpson T,
Fonn D.
Results of a one year clinical trial comparing monovision and bifocal contact lenses.
Optometry & Vision Science 2000:18.
[Google Scholar]
Englund 2005 {published data only}
Englund JA,
Walter EB,
Fairchok MP,
Monto AS,
Neuzil KM.
A comparison of 2 influenza vaccine schedules in 6‐ to 23‐month‐old children.
Pediatrics 2005;115(4):1039‐47.
[DOI] [PubMed] [Google Scholar]
Feldon 2004 {published data only}
Feldon SE.
Computerized expert system for evaluation of automated visual fields from the Ischemic Optic Neuropathy Decompression Trial: Methods, baseline fields, and six‐month longitudinal follow‐up.
Transactions of the American Ophthalmological Society 2004;102:269‐303.
[PMC free article] [PubMed] [Google Scholar]
Feldon 2006 {published data only}
Feldon SE,
Levin L,
Scherer RW,
Arnold A,
Chung SM,
Johnson LN,
et al.
Development and validation of a computerized expert system for evaluation of automated visual fields from the Ischemic Optic Neuropathy Decompression Trial.
BMC Ophthalmology 2006;6(34):1‐21.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Hack 2003 {published data only}
Hack TF,
Pickles T,
Bultz BD,
Ruether JD,
Weir LM,
Degner LF,
et al.
Impact of providing audiotapes of primary adjuvant treatment consultations to women with breast cancer: a multisite, randomized, controlled trial.
Journal of Clinical Oncology 2003;21(22):4138‐44.
[DOI] [PubMed] [Google Scholar]
Havel 2001 {published data only}
Havel C,
Sieder A,
Herkner H,
Domanovits H,
Schmied M,
Segel R,
et al.
Which treatment for low back pain? A factorial randomised controlled trial comparing intravenous analgesics with oral analgesics in the emergency department and a centrally acting muscle relaxant with placebo over three days.
BMC Emergency Medicine 2001;1(2).
[DOI] [PMC free article] [PubMed] [Google Scholar]
Hehr 2004 {published data only}
Hehr T,
Classen J,
Schreck U,
Glocker S,
Bamberg M,
Budach W.
Hyperfractionated accelerated radiotherapy alone and with concomitant chemotherapy to the head and neck: treated within and outside of randomized clinical trials.
International Journal of Radiation Oncology, Biology, Physics 2004;58(5):1424‐30.
[DOI] [PubMed] [Google Scholar]
Holub 2000 {published data only}
Holub Z,
Voracek J,
Wagnerova M,
Kliment L Jr.
[Hormone replacement therapy in women with surgical treatment of endometriosis and adenomyosis: prospective and follow‐up study. Part I]. [Czech].
Ceska Gynekologie 2000;65(1):16‐20.
[PubMed] [Google Scholar]
Jeffery 2003 {published data only}
Jeffery JR,
Leslie WD,
Karpinski ME,
Nickerson PW,
Rush DN.
Prevalence and treatment of decreased bone density in renal transplant recipients: a randomized prospective trial of calcitriol versus alendronate.
Transplantation 2003;76(10):1498‐502.
[DOI] [PubMed] [Google Scholar]
Juster 1995 {published data only}
Juster HR,
Heimberg RG,
Engelberg B.
Self selection and sample selection in a treatment study of social phobia.
Behaviour Research & Therapy 1995;33(3):321‐4.
[DOI] [PubMed] [Google Scholar]
Kitchener 2004 {published data only}
Kitchener HC,
Burns S,
Nelson L,
Myers AJ,
Fletcher I,
Desai M,
et al.
A randomised controlled trial of cytological surveillance versus patient choice between surveillance and colposcopy in managing mildly abnormal cervical smears.
BJOG: An International Journal of Obstetrics & Gynaecology 2004;111(1):63‐70.
[DOI] [PubMed] [Google Scholar]
Koch‐Henriksen 2006 {published data only}
Koch‐Henriksen N,
Sørensen PS,
Christensen T,
Fredriksen J,
Ravnborg M,
Jensen K,
et al.
A randomized study of two interferon‐beta treatments in relapsing‐remitting multiple sclerosis.
Neurology 2006;66:1056‐60.
[DOI] [PubMed] [Google Scholar]
Krysztopik 2002 {published data only}
Krysztopik RJ,
Jamieson GG,
Devitt PG,
Watson DI.
A further modification of fundoplication. 90 degrees anterior fundoplication.
Surgical Endoscopy 2002;16(10):1446‐51.
[DOI] [PubMed] [Google Scholar]
Kudenchuk 1998 {published data only}
Kudenchuk PJ,
Maynard C,
Cobb LA,
Wirkus M,
Martin JS,
Kennedy JW,
et al.
Utility of the prehospital electrocardiogram in diagnosing acute coronary syndromes: the Myocardial Infarction Triage and Intervention (MITI) Project.
Journal of the American College of Cardiology 1998;32(1):17‐27.
[DOI] [PubMed] [Google Scholar]
Lavertu 2001 {published data only}
Lavertu P,
Adelstein DJ,
Myles J,
Secic M.
P53 and Ki‐67 as outcome predictors for advanced squamous cell cancers of the head and neck treated with chemoradiotherapy.
Laryngoscope 2001;111(11 pt 1):1878‐92.
[DOI] [PubMed] [Google Scholar]
Linn 2003 {published data only}
Linn T,
Mann M,
Mann M,
Bretzel RG,
Boedeker RH.
Randomised prospective study for the effect of therapy on residual beta cell function in type‐1 diabetes mellitus [ISRCTN70703138].
BMC Endocrine Disorders 2003;3(5):1‐9.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Mattila 2003 {published data only}
Mattila PS,
Joki‐Erkkila V‐P,
Kilpi T,
Jokinin J,
Herva E,
Puhakka H.
Prevention of otitis media by adenoidectomy in children younger than 2 years.
Archives of Otolaryngology Head and Neck Surgery 2003;129:163‐8.
[DOI] [PubMed] [Google Scholar]
Mayberg 1991 {published data only}
Mayberg MR,
Wilson SE,
Yatsu F,
Weiss DG,
Messina L,
Hershey LA,
et al.
Carotid endarterectomy and prevention of cerebral ischemia in symptomatic carotid stenosis. Veterans Affairs Cooperative Studies Program 309 Trialist Group.
JAMA 1991;266(23):3289‐94.
[PubMed] [Google Scholar]
Miller 2003 {published data only}
Miller P,
Chilvers C,
Dewey M,
Fielding K,
Gretton V,
Palmer B,
et al.
Counseling versus antidepressant therapy for the treatment of mild to moderate depression in primary care: economic analysis.
International Journal of Technology Assessment in Health Care 2003;19(1):80‐90.
[DOI] [PubMed] [Google Scholar]
Mills 2006 {published data only}
Mills N,
Metcalfe C,
Ronsmans C,
Davis M,
Lane JA,
Sterne JAC,
et al.
A comparison of socio‐demographic and psychological factors between patients consenting to randomisation and those selecting treatment (the ProtecT study).
Contemporary Clinical Trials 2006;27:413‐9.
[DOI] [PubMed] [Google Scholar]
Mitchell 2005 {published data only}
Mitchell EA,
Didsbury PB,
Kruithof N,
Robinson E,
Milmine M,
Barry M,
et al.
A randomized controlled trial of an asthma clinical pathway for children in general practice.
Acta Pædiatrica 2005;94:226‐33.
[DOI] [PubMed] [Google Scholar]
Mohr 2006 {published data only}
Mohr P,
Rodriguez M,
Novak T,
Kopecek M,
Horacek J,
Hendrychova Y,
et al.
Repetitive transcranial magnetic stimulation and rehabilitation of cognitive functions in schizophrenia. [Czech].
Psychiatrie 2006;10(1):7‐15.
[Google Scholar]
Molkenboer 2004 {published data only}
Molkenboer JF,
Reijners EP,
Nijhuis JG,
Roumen FJ.
Moderate neonatal morbidity after vaginal term breech delivery.
Journal of Maternal‐Fetal & Neonatal Medicine 2004;16(6):357‐61.
[DOI] [PubMed] [Google Scholar]
Moore 2000 {published data only}
Moore DA,
Goodall RL,
Ives NJ,
Hooker M,
Gazzard BG,
Easterbrook PJ.
How generalizable are the results of large randomized controlled trials of antiretroviral therapy?.
HIV Medicine 2000;1(3):149‐54.
[DOI] [PubMed] [Google Scholar]
Moran 2003 {published data only}
Moran SL,
Nava G,
Behnam AB,
Serletti JM.
An outcome analysis comparing the thoracodorsal and internal mammary vessels as recipient sites for microvascular breast reconstruction: a prospective study of 100 patients.[erratum appears in Plast Reconstr Surg.2003 Sept; Note: Behnam Amir H [corrected to Behnam Amir B]].
Plastic & Reconstructive Surgery 2003;111(6):1876‐82.
[DOI] [PubMed] [Google Scholar]
Neldam 1986 {published data only}
Neldam S,
Osler M,
Hansen PK,
Nim J,
Smith SF,
Hertel J.
Intrapartum fetal heart rate monitoring in a combined low‐ and high‐risk population: a controlled clinical trial.
European Journal of Obstetrics, Gynecology, & Reproductive Biology 1986;23(1‐2):1‐11.
[DOI] [PubMed] [Google Scholar]
Nicolaides 1996 {published data only}
Nicolaides KH,
Brizot ML,
Patel F,
Snjders R.
Comparison of chorion villus sampling and early amniocentesis for karyotyping in 1,492 singleton pregnancies.
Fetal Diagnosis & Therapy 1996;11(1):9‐15.
[DOI] [PubMed] [Google Scholar]
Noël 1998 {published data only}
Noël PH,
Larme AC,
Meyer J,
Marsh G,
Correa A,
Pugh JA.
Patient choice in diabetes education curriculum. Nutritional versus standard content for type 2 diabetes.
Diabetes Care 1998;21(6):896‐901.
[DOI] [PubMed] [Google Scholar]
Näslund 1994 {published data only}
Näslund GK,
Fredrikson M,
Hellenius ML,
Faire U.
Characteristics of participating and nonparticipating men in a randomized, controlled diet and exercise intervention trial.
Scandinavian Journal of Primary Health Care 1994;12(4):249‐54.
[DOI] [PubMed] [Google Scholar]
Oude Elberink 2006 {published data only}
Oude Elberink JN,
Heide S,
Guyatt GH,
Dubois AE.
Analysis of the burden of treatment in patients receiving an EpiPen for yellow jacket anaphylaxis.
Journal of Allergy & Clinical Immunology 2006;118(3):699‐704.
[DOI] [PubMed] [Google Scholar]
Pearson 2005 {published data only}
Pearson S,
Maddern GJ,
Hewett P.
Interacting effects of preoperative information and patient choice in adaptation to colonoscopy.
Diseases of the Colon & Rectum 2005;48(11):2047‐54.
[DOI] [PubMed] [Google Scholar]
Pizer 2006 {published data only}
Pizer BL,
Weston CL,
Robinson KJ,
Ellison DW,
Ironside J,
Saran F,
et al.
Analysis of patients with supratentorial primitive neuro‐ectodermal tumours entered into the SIOP/UKCCSG PNET 3 study.
European Journal of Cancer 2006;42(8):1120‐8.
[DOI] [PubMed] [Google Scholar]
Ros 2006 {published data only}
Ros A,
Carlsson P,
Rahmqvist M,
Backman K,
Nilsson E.
Non‐randomised patients in a cholecystectomy trial: characteristics, procedures, and outcomes.
BMC Surgery 2006;6:17‐21.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Scott 2001 {published data only}
Scott RA,
Vardulaki KA,
Walker NM,
Day NE,
Duffy SW,
Ashton HA.
The long‐term benefits of a single scan for abdominal aortic aneurysm (AAA) at age 65.
European Journal of Vascular & Endovascular Surgery 2001;21(6):535‐40.
[DOI] [PubMed] [Google Scholar]
Sesso 2002 {published data only}
Sesso HD,
Gaziano JM,
VanDenburgh M,
Hennekens CH,
Glynn RJ,
Buring JE.
Comparison of baseline characteristics and mortality experience of participants and nonparticipants in a randomized clinical trial: The Physicians' Health Study.
Controlled Clinical Trials 2002;23(6):686‐702.
[DOI] [PubMed] [Google Scholar]
Thomssen 2000 {published data only}
Thomssen C,
Prechtl A,
Meisner C,
Braun M,
Harbeck N,
Schmitt M,
et al.
Efficacy of adjuvant chemotherapy in node‐negative breast cancer patients with elevated UPA and PAI‐1 tumor levels: Interim analysis of a randomized trial.
2nd European Breast Cancer Conference, Brussels, 26 30 September 2000 2000:67.
[Google Scholar]
Viola 1996 {published data only}
Viola L,
Perez V,
Tanno H,
Silva M,
Welz G,
Vilar J,
et al.
Predictive factors of non‐response to recombinant interferon alpha 2b in patients with chronic hepatitis C [AASLD abstract].
Hepatology 1996;24(4 pt 2):594A.
[Google Scholar]
Walther 2003 {published data only}
Walther B,
Johansson J,
Johnsson F,
Holstein CS,
Zilling T.
Cervical or thoracic anastomosis after esophageal resection and gastric tube reconstruction: a prospective randomized trial comparing sutured neck anastomosis with stapled intrathoracic anastomosis.
Annals of Surgery 2003;238(6):803‐14.
[DOI] [PMC free article] [PubMed] [Google Scholar]
West 2005 {published data only}
West J,
Wright J,
Tuffnell D,
Jankowicz D,
West R.
Do clinical trials improve quality of care? A comparison of clinical processes and outcomes in patients in a clinical trial and similar patients outside a trial where both groups are managed according to a strict protocol.
Quality & Safety in Health Care 2005;14(3):175‐8.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Wright 2002 {published data only}
Wright D,
Paterson C,
Scott N,
Hair A,
O'Dwyer PJ.
Five‐year follow‐up of patients undergoing laparoscopic or open groin hernia repair: A randomized controlled trial.
Annals of Surgery 2002;235(3):333‐7.
[DOI] [PMC free article] [PubMed] [Google Scholar]
Additional references
Angell 1984
Angell M.
Patients' preferences in randomized clinical trials.
New England Journal of Medicine 1984;310:1385‐7.
[DOI] [PubMed] [Google Scholar]
Braunholtz 2001
Braunholtz DA,
Edwards SJL,
Lilford RJ.
Are randomized clinical trials good for us (in the short term)? Evidence for a "trial effect".
Journal of Clinical Epidemiology 2001;54:217‐24.
[DOI] [PubMed] [Google Scholar]
ECRI 2002
Patients' reasons for particpation in clinical trials and effect of trial participation on patient outcomes.
http://www.ecri.org/Patient_Information/Patient_Reference_Guide/evidence.pdf.
Hellman 1991
Hellman S,
Hekkman DS.
Of mice but not of men: problems of the randomized clinical trial.
New England Journal of Medicine 1991;324:1585‐9.
[DOI] [PubMed] [Google Scholar]
Kunz 2002
Kunz R,
Vist G,
Oxman AD.
Randomisation to protect against selection bias in healthcare trials.
The Cochrane Database of Methodology Reviews 2002, Issue 4. Art. No.: MR000012. DOI: 10.1002/14651858.MR000012.
[DOI] [PMC free article] [PubMed]
Peppercorn 2004
Peppercorn JM,
Weeks JC,
Cook EFC,
Joffe S.
Comparison of outcomes in cancer patients treated within and outside clinical trials: conceptual framewok and structured review.
The Lancet 2004;363:263‐70.
[DOI] [PubMed] [Google Scholar]
Sackett 2001
Sackett DL.
How do the outcomes of patients treated within randomised controlled trial compare with those of similar patients treated outside these trials.
Controlled Clinical Trials 2001;22(2S):84S.
[Google Scholar]
Stiller 1994
Stiller CA.
Centralised treatment, entry to trials and survival.
British Journal of Cancer 1994;70:352‐62.
[DOI] [PMC free article] [PubMed] [Google Scholar]
References to other published versions of this review
Vist 2005
Vist GE,
Hagen KB,
Devereaux PJ,
Bryant D,
Kristoffersen D,
Oxman AD.
Systematic review to determine whether participation in a trial influences outcome.
BMJ 2005;330:1175.
[DOI: ]
[DOI] [PMC free article] [PubMed] [Google Scholar]